
CEACAM6’s Role as a Chemoresistance and Prognostic Biomarker for Pancreatic Cancer: A Comparison of CEACAM6’s Diagnostic and Prognostic Capabilities with Those of CA19-9 and CEA

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Patients’ Selection and Samples Collection
2.2. Proteomic Analysis of Tissue Samples
2.3. Tissue Lysates Preparation and Western Blot
2.4. Enzyme Linked Immunosorbent Assay (ELISA) and Chemiluminescent Microparticle Immunoassay (CMIA)
2.5. Statistics
3. Results
3.1. Proteomic Identification of CEACAM6 as Potential PDAC Biomarker
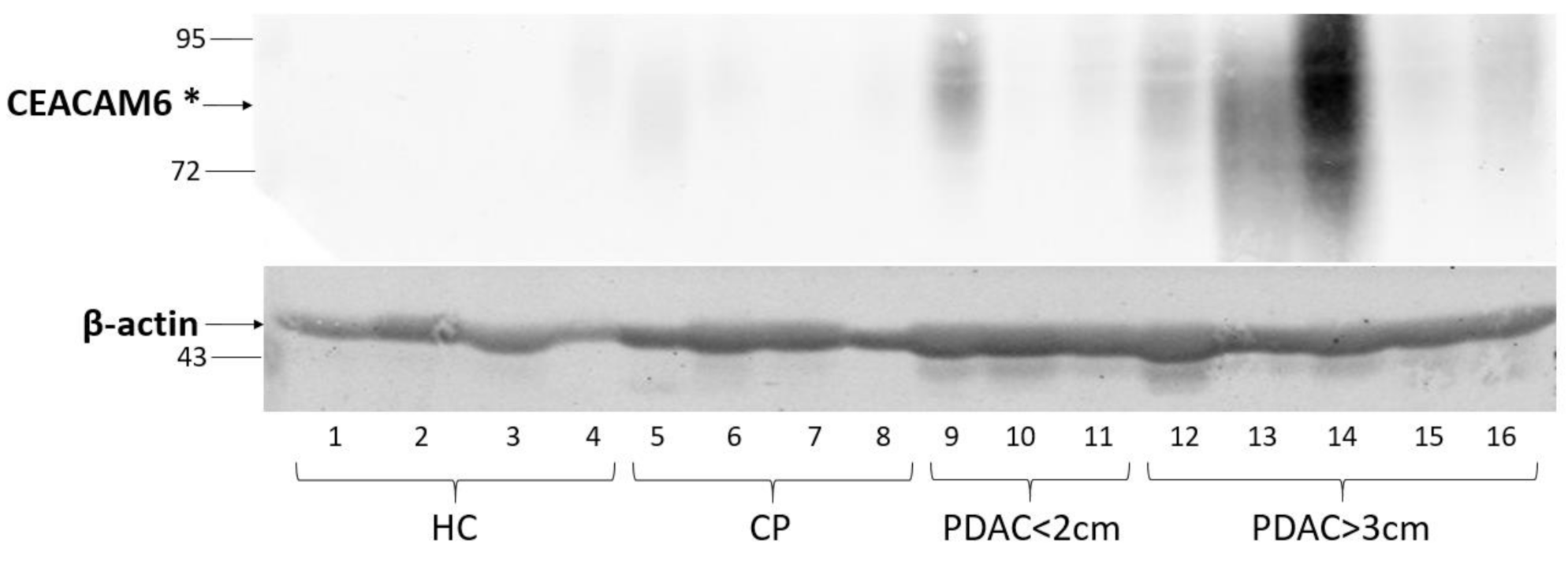
3.2. CEACAM6 Expression in PDAC Tissue Specimens
3.3. Evaluation of CEACAM6, CEA and CA19-9 Concentrations in Patients’ Blood Serum, Diagnostic Capability of CEACAM6
3.4. Comparative Analysis of CEACAM6 as a Prognostic Biomarker
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Commission. European Cancer Information System. Available online: https://ecis.jrc.ec.europa.eu/explorer.php?$0-0$1-All$2-All$4-1,2$3-0$6-0,14$5-2008,2008$7-7$CEstByCountry$X0_8-3$X0_19-AE27$X0_20-No$CEstBySexByCountry$X1_8-3$X1_19-AE27$X1_-1-1$CEstByIndiByCountry$X2_8-3$X2_19-AE27$X2_20-No$CEstRelative$X3_8-3$X3_9-AE27$X3_19-AE27$CEstByCountryTable$X4_19-AE27 (accessed on 15 February 2021).
- Ferlay, J.; Partensky, C.; Bray, F. More Deaths from Pancreatic Cancer than Breast Cancer in the EU by 2017. Acta Oncol. 2016, 55, 1158–1160. [Google Scholar] [CrossRef] [PubMed]
- Canto, M.I.; Harinck, F.; Hruban, R.H.; Offerhaus, G.J.; Poley, J.-W.; Kamel, I.; Nio, Y.; Schulick, R.S.; Bassi, C.; Kluijt, I.; et al. International Cancer of the Pancreas Screening (CAPS) Consortium Summit on the Management of Patients with Increased Risk for Familial Pancreatic Cancer. Gut 2013, 62, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Yoneyama, T.; Ohtsuki, S.; Honda, K.; Kobayashi, M.; Iwasaki, M.; Uchida, Y.; Okusaka, T.; Nakamori, S.; Shimahara, M.; Ueno, T.; et al. Identification of IGFBP2 and IGFBP3 As Compensatory Biomarkers for CA19-9 in Early-Stage Pancreatic Cancer Using a Combination of Antibody-Based and LC-MS/MS-Based Proteomics. PLoS ONE 2016, 11, e0161009. [Google Scholar] [CrossRef] [PubMed]
- Dutta, S.K.; Girotra, M.; Singla, M.; Dutta, A.; Otis Stephen, F.; Nair, P.P.; Merchant, N.B. Serum HSP70: A Novel Biomarker for Early Detection of Pancreatic Cancer. Pancreas 2012, 41, 530–534. [Google Scholar] [CrossRef] [PubMed]
- Tumas, J.; Baskirova, I.; Petrenas, T.; Norkuniene, J.; Strupas, K.; Sileikis, A. Towards a Personalized Approach in Pancreatic Cancer Diagnostics Through Plasma Amino Acid Analysis. Anticancer Res. 2019, 39, 2035–2042. [Google Scholar] [CrossRef]
- Peng, J.; Sun, B.-F.; Chen, C.-Y.; Zhou, J.-Y.; Chen, Y.-S.; Chen, H.; Liu, L.; Huang, D.; Jiang, J.; Cui, G.-S.; et al. Single-Cell RNA-Seq Highlights Intra-Tumoral Heterogeneity and Malignant Progression in Pancreatic Ductal Adenocarcinoma. Cell Res. 2019, 29, 725–738. [Google Scholar] [CrossRef]
- Pedersen, K.; Bilal, F.; Bernadó Morales, C.; Salcedo, M.T.; Macarulla, T.; Massó-Vallés, D.; Mohan, V.; Vivancos, A.; Carreras, M.-J.; Serres, X.; et al. Pancreatic Cancer Heterogeneity and Response to Mek Inhibition. Oncogene 2017, 36, 5639–5647. [Google Scholar] [CrossRef]
- Neuzillet, C.; Tijeras-Raballand, A.; Ragulan, C.; Cros, J.; Patil, Y.; Martinet, M.; Erkan, M.; Kleeff, J.; Wilson, J.; Apte, M.; et al. Inter- and Intra-Tumoural Heterogeneity in Cancer-Associated Fibroblasts of Human Pancreatic Ductal Adenocarcinoma. J. Pathol. 2019, 248, 51–65. [Google Scholar] [CrossRef]
- United European Gastroenterology Report: Pancreatic Cancer Across Europe—Taking a United Stand. Available online: https://ueg.eu/files/630/9cc138f8dc04cbf16240daa92d8d50e2.pdf (accessed on 22 February 2021).
- Beauchemin, N.; Draber, P.; Dveksler, G.; Gold, P.; Gray-Owen, S.; Grunert, F.; Hammarström, S.; Holmes, K.V.; Karlsson, A.; Kuroki, M.; et al. Redefined Nomenclature for Members of the Carcinoembryonic Antigen Family. Exp. Cell Res. 1999, 252, 243–249. [Google Scholar] [CrossRef]
- Kuespert, K.; Pils, S.; Hauck, C.R. CEACAMs: Their Role in Physiology and Pathophysiology. Curr. Opin. Cell Biol. 2006, 18, 565–571. [Google Scholar] [CrossRef]
- Gebauer, F.; Wicklein, D.; Horst, J.; Sundermann, P.; Maar, H.; Streichert, T.; Tachezy, M.; Izbicki, J.R.; Bockhorn, M.; Schumacher, U. Carcinoembryonic Antigen-Related Cell Adhesion Molecules (CEACAM) 1, 5 and 6 as Biomarkers in Pancreatic Cancer. PLoS ONE 2014, 9, e113023. [Google Scholar] [CrossRef]
- Horst, A.K.; Ito, W.D.; Dabelstein, J.; Schumacher, U.; Sander, H.; Turbide, C.; Brümmer, J.; Meinertz, T.; Beauchemin, N.; Wagener, C. Carcinoembryonic Antigen-Related Cell Adhesion Molecule 1 Modulates Vascular Remodeling in Vitro and in Vivo. J. Clin. Investig. 2006, 116, 1596–1605. [Google Scholar] [CrossRef]
- Obrink, B. CEA Adhesion Molecules: Multifunctional Proteins with Signal-Regulatory Properties. Curr. Opin. Cell Biol. 1997, 9, 616–626. [Google Scholar] [CrossRef]
- Duxbury, M.S.; Matros, E.; Clancy, T.; Bailey, G.; Doff, M.; Zinner, M.J.; Ashley, S.W.; Maitra, A.; Redston, M.; Whang, E.E. CEACAM6 Is a Novel Biomarker in Pancreatic Adenocarcinoma and PanIN Lesions. Ann. Surg. 2005, 241, 491–496. [Google Scholar] [CrossRef]
- Zińczuk, J.; Zaręba, K.; Romaniuk, W.; Kamińska, D.; Nizioł, M.; Baszun, M.; Kędra, B.; Guzińska-Ustymowicz, K.; Pryczynicz, A. Expression of Chosen Carcinoembryonic-Related Cell Adhesion Molecules in Pancreatic Intraepithelial Neoplasia (PanIN) Associated with Chronic Pancreatitis and Pancreatic Ductal Adenocarcinoma (PDAC). Int. J. Med. Sci. 2019, 16, 583–592. [Google Scholar] [CrossRef]
- Strickland, L.A.; Ross, J.; Williams, S.; Ross, S.; Romero, M.; Spencer, S.; Erickson, R.; Sutcliffe, J.; Verbeke, C.; Polakis, P.; et al. Preclinical Evaluation of Carcinoembryonic Cell Adhesion Molecule (CEACAM) 6 as Potential Therapy Target for Pancreatic Adenocarcinoma. J. Pathol. 2009, 218, 380–390. [Google Scholar] [CrossRef]
- Duxbury, M.S.; Ito, H.; Benoit, E.; Waseem, T.; Ashley, S.W.; Whang, E.E. A Novel Role for Carcinoembryonic Antigen-Related Cell Adhesion Molecule 6 as a Determinant of Gemcitabine Chemoresistance in Pancreatic Adenocarcinoma Cells. Cancer Res. 2004, 64, 3987–3993. [Google Scholar] [CrossRef]
- Chen, J.; Li, Q.; An, Y.; Lv, N.; Xue, X.; Wei, J.; Jiang, K.; Wu, J.; Gao, W.; Qian, Z.; et al. CEACAM6 Induces Epithelial-Mesenchymal Transition and Mediates Invasion and Metastasis in Pancreatic Cancer. Int. J. Oncol. 2013, 43, 877–885. [Google Scholar] [CrossRef]
- Tuck, M.K.; Chan, D.W.; Chia, D.; Godwin, A.K.; Grizzle, W.E.; Krueger, K.E.; Rom, W.; Sanda, M.; Sorbara, L.; Stass, S.; et al. Standard Operating Procedures for Serum and Plasma Collection: Early Detection Research Network Consensus Statement Standard Operating Procedure Integration Working Group. J. Proteome Res. 2009, 8, 113–117. [Google Scholar] [CrossRef]
- Ger, M.; Kaupinis, A.; Nemeikaite-Ceniene, A.; Sarlauskas, J.; Cicenas, J.; Cenas, N.; Valius, M. Quantitative Proteomic Analysis of Anticancer Drug RH1 Resistance in Liver Carcinoma. Biochim. Biophys. Acta Proteins Proteom. 2016, 1864, 219–232. [Google Scholar] [CrossRef]
- Cheng, T.-M.; Murad, Y.M.; Chang, C.-C.; Yang, M.-C.; Baral, T.N.; Cowan, A.; Tseng, S.-H.; Wong, A.; Mackenzie, R.; Shieh, D.-B.; et al. Single Domain Antibody against Carcinoembryonic Antigen-Related Cell Adhesion Molecule 6 (CEACAM6) Inhibits Proliferation, Migration, Invasion and Angiogenesis of Pancreatic Cancer Cells. Eur. J. Cancer 2014, 50, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Roser, M.; Ritchie, H. Cancer. Available online: https://ourworldindata.org/cancer (accessed on 8 February 2021).
- Duxbury, M.S.; Ito, H.; Zinner, M.J.; Ashley, S.W.; Whang, E.E. CEACAM6 Gene Silencing Impairs Anoikis Resistance and in Vivo Metastatic Ability of Pancreatic Adenocarcinoma Cells. Oncogene 2004, 23, 465–473. [Google Scholar] [CrossRef] [PubMed]
- Duxbury, M.S.; Ito, H.; Ashley, S.W.; Whang, E.E. CEACAM6 Cross-Linking Induces Caveolin-1-Dependent, Src-Mediated Focal Adhesion Kinase Phosphorylation in BxPC3 Pancreatic Adenocarcinoma Cells. J. Biol. Chem. 2004, 279, 23176–23182. [Google Scholar] [CrossRef] [PubMed]
- Duxbury, M.S.; Ito, H.; Benoit, E.; Zinner, M.J.; Ashley, S.W.; Whang, E.E. Overexpression of CEACAM6 Promotes Insulin-like Growth Factor I-Induced Pancreatic Adenocarcinoma Cellular Invasiveness. Oncogene 2004, 23, 5834–5842. [Google Scholar] [CrossRef]
- Duxbury, M.S.; Ito, H.; Ashley, S.W.; Whang, E.E. C-Src-Dependent Cross-Talk between CEACAM6 and Alphavbeta3 Integrin Enhances Pancreatic Adenocarcinoma Cell Adhesion to Extracellular Matrix Components. Biochem. Biophys. Res. Commun. 2004, 317, 133–141. [Google Scholar] [CrossRef]
- Duxbury, M.S.; Ito, H.; Benoit, E.; Ashley, S.W.; Whang, E.E. CEACAM6 Is a Determinant of Pancreatic Adenocarcinoma Cellular Invasiveness. Br. J. Cancer 2004, 91, 1384–1390. [Google Scholar] [CrossRef]
- Yan, L.; Wang, Y.; Wang, Z.-Z.; Rong, Y.-T.; Chen, L.-L.; Li, Q.; Liu, T.; Chen, Y.-H.; Li, Y.-D.; Huang, Z.-H.; et al. Cell Motility and Spreading Promoted by CEACAM6 through Cyclin D1/CDK4 in Human Pancreatic Carcinoma. Oncol. Rep. 2016, 35, 418–426. [Google Scholar] [CrossRef]
- LeBlanc, J.K.; Chen, J.-H.; Al-Haddad, M.; Luz, L.; McHenry, L.; Sherman, S.; Juan, M.; Dewitt, J. Can Endoscopic Ultrasound Predict Pancreatic Intraepithelial Neoplasia Lesions in Chronic Pancreatitis?: A Retrospective Study of Pathologic Correlation. Pancreas 2014, 43, 849–854. [Google Scholar] [CrossRef]
- Rosty, C.; Geradts, J.; Sato, N.; Wilentz, R.E.; Roberts, H.; Sohn, T.; Cameron, J.L.; Yeo, C.J.; Hruban, R.H.; Goggins, M. P16 Inactivation in Pancreatic Intraepithelial Neoplasias (PanINs) Arising in Patients with Chronic Pancreatitis. Am. J. Surg. Pathol. 2003, 27, 1495–1501. [Google Scholar] [CrossRef]
- Sindhu, R.S.; Parvathy, G.; Fysal, K.; Jacob, M.K.; Geetha, S.; Krishna, B.; Natesh, B.; Rajan, R. Clinical Profile of PanIN Lesions in Tropical Chronic Pancreatitis. Indian J. Gastroenterol. Off. J. Indian Soc. Gastroenterol. 2015, 34, 436–441. [Google Scholar] [CrossRef]
- Ludwig, O.J.; Cortese, C.M.; Collins, B.T.; Agarwal, B. Immunostaining As Adjunct to Cytologic Assessment of Endoscopic Ultrasound Guided Fine Needle Aspiration (EUS-FNA) Specimens for Diagnosis of Pancreatic Adenocarcinoma. Gastrointest. Endosc. 2007, 65, AB119. [Google Scholar] [CrossRef]
- Farina, A.; Dumonceau, J.-M.; Frossard, J.-L.; Hadengue, A.; Hochstrasser, D.F.; Lescuyer, P. Proteomic Analysis of Human Bile from Malignant Biliary Stenosis Induced by Pancreatic Cancer. J. Proteome Res. 2009, 8, 159–169. [Google Scholar] [CrossRef]
- Sharma, N.; Srivastava, S.; Kern, F.; Xian, W.; Yeoh, K.G.; Ming, T.; McKeon, F.; Ho, K.Y. CEACAM 6, a Novel Marker for the Diagnosis of Barrett’s Esophagus. Dis. Esophagus Off. J. Int. Soc. Dis. Esophagus 2017, 30, 1–5. [Google Scholar] [CrossRef]
- Katz, S.C. Phase 1b Study of CAR2Anti-CEA CAR-T Cell Hepatic Infusions for Pancreatic Carcinoma Patients With CEA + Liver Metastases (AntiCEA_CART); ClinicalTrials.Gov Identifier: NCT03818165; Sponsor: Sorrento Therapeutics, Inc.; Start Date: 1 February 2019. Available online: https://clinicaltrials.gov/ct2/show/NCT03818165 (accessed on 7 June 2021).
- Pandey, R.; Zhou, M.; Islam, S.; Chen, B.; Barker, N.K.; Langlais, P.; Srivastava, A.; Luo, M.; Cooke, L.S.; Weterings, E.; et al. Carcinoembryonic Antigen Cell Adhesion Molecule 6 (CEACAM6) in Pancreatic Ductal Adenocarcinoma (PDA): An Integrative Analysis of a Novel Therapeutic Target. Sci. Rep. 2019, 9, 18347. [Google Scholar] [CrossRef]
- Ieta, K.; Tanaka, F.; Utsunomiya, T.; Kuwano, H.; Mori, M. CEACAM6 Gene Expression in Intrahepatic Cholangiocarcinoma. Br. J. Cancer 2006, 95, 532–540. [Google Scholar] [CrossRef]
- Wang, Z.; Luo, C.; Wang, H.; Yan, X.; Liu, W.; Meng, Z. CEACAM6 Is Associated with Osteosarcoma Metastasis and Facilitates Epithelial-Mesenchymal Transition in Osteosarcoma Cells. OncoTargets Ther. 2018, 11, 3159–3166. [Google Scholar] [CrossRef]
- Zhu, R.; Ge, J.; Ma, J.; Zheng, J. Carcinoembryonic Antigen Related Cell Adhesion Molecule 6 Promotes the Proliferation and Migration of Renal Cancer Cells through the ERK/AKT Signaling Pathway. Transl. Androl. Urol. 2019, 8, 457–466. [Google Scholar] [CrossRef]
- Jantscheff, P.; Terracciano, L.; Lowy, A.; Glatz-Krieger, K.; Grunert, F.; Micheel, B.; Brümmer, J.; Laffer, U.; Metzger, U.; Herrmann, R.; et al. Expression of CEACAM6 in Resectable Colorectal Cancer: A Factor of Independent Prognostic Significance. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2003, 21, 3638–3646. [Google Scholar] [CrossRef]
- Kim, K.S.; Kim, J.-T.; Lee, S.-J.; Kang, M.A.; Choe, I.S.; Kang, Y.H.; Kim, S.-Y.; Yeom, Y.I.; Lee, Y.-H.; Kim, J.H.; et al. Overexpression and Clinical Significance of Carcinoembryonic Antigen-Related Cell Adhesion Molecule 6 in Colorectal Cancer. Clin. Chim. Acta. 2013, 415, 12–19. [Google Scholar] [CrossRef]
- Ru, G.-Q.; Han, Y.; Wang, W.; Chen, Y.; Wang, H.-J.; Xu, W.-J.; Ma, J.; Ye, M.; Chen, X.; He, X.-L.; et al. CEACAM6 Is a Prognostic Biomarker and Potential Therapeutic Target for Gastric Carcinoma. Oncotarget 2017, 8, 83673–83683. [Google Scholar] [CrossRef]
- Deng, X.; Liu, P.; Zhao, Y.; Wang, Q. Expression Profiling of CEACAM6 Associated with the Tumorigenesis and Progression in Gastric Adenocarcinoma. Genet. Mol. Res. 2014, 13, 7686–7697. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HC | CP | PDAC < 2 cm | PDAC > 3 cm | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Line No. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 |
| CEACAM6 | 1.0 | 0.6 | 0.5 | 2.4 | 11.7 | 1.8 | 1.4 | 1.1 | 19.9 | 1.2 | 6.4 | 15.6 | 69.4 | 110.3 | 14.9 | 24.0 |
| β-actin | 1.0 | 1.8 | 1.9 | 0.7 | 1.3 | 2.3 | 2.2 | 1.4 | 2.8 | 2.7 | 2.3 | 3.8 | 2.4 | 2.8 | 2.1 | 2.2 |
| Parameter | PDAC | CP | HC | p |
|---|---|---|---|---|
| No. of patients | 142 | 66 | 31 | |
| Gender | <0.001 | |||
| Female No. (%) | 71 (50.0) | 15 (22.7) | 17 (54.8) | |
| Male No. (%) | 71 (50.0) | 51 (77.3) | 14 (45.2) | |
| Age (years) Median (IQR) | 66.0 (13.8) | 49.0 (12.0) | 56.0 (11.0) | <0.001 |
| BMI * Median (IQR) | 25.4 (5.5) | 22.5 (4.4) | 27.3 (9.7) | <0.001 |
| Diabetes mellitus | 0.009 | |||
| Present No. (%) | 32 (22.5) | 27 (40.9) | 5 (16.1) | |
| Absent No. (%) | 110 (77.5) | 39 (59.1) | 26 (83.9) |
| Biomarker | PDAC | CP | HC | p |
|---|---|---|---|---|
| CEA * (mkg/L) Median (IQR) | 2.9 (3.8) | 2.6 (2.7) | 1.4 (0.8) | <0.001 |
| CEACAM6 (ng/mL) Median (IQR) | 2.1 (2.4) | 3.3 (2.3) | 1.1 (1.8) | <0.001 |
| CA19-9 ** (kU/L) Median (IQR) | 176.0 (1386.9) | 7.6 (22.1) | 3.6 (5.1) | <0.001 |
| Parameter | CEA Effect Size (p-Value) | CEACAM6 Effect Size (p-Value) | Ca19-9 Effect Size (p-Value) |
|---|---|---|---|
| Demographical | |||
| Gender | 0.01 (0.1) ** | −0.01 (0.8) ** | 0.00 (0.3) ** |
| Age | 0.04 (0.46) * | 0.09 (0.13) * | −0.05 (0.42) * |
| Diabetes mellitus | 0.01 (0.1) ** | 0.01 (0.06) ** | 0.00 (0.9) ** |
| BMI | −0.04 (0.47) * | 0.01 (0.85) * | 0.04 (0.51) * |
| Oncological | |||
| T 1 | 0.05 (0.001) ** | 0.04 (0.008) ** | 0.05 (0.001) ** |
| N 2 | −0.01 (0.9) ** | 0.00 (0.5) ** | 0.05 (0.002) ** |
| M 3 | 0.07 (0.00005) ** | 0.02 (0.03) ** | 0.03 (0.004) ** |
| G 4 | −0.01 (0.9) ** | 0.00 (0.6) ** | −0.01 (0.7) ** |
| R 5 | 0.00 (0.5) ** | 0.00 (0.3) ** | 0.01 (0.1) ** |
| Stage | 0.06 (0.002) ** | 0.00 (0.3) ** | 0.04 (0.01) ** |
| LNR 6 | −0.05 (0.59) * | −0.05 (0.56) * | 0.13 (0.14) * |
| Perineural invasion | 0.10 (0.000004) ** | 0.05 (0.0008) ** | 0.03 (0.02) ** |
| Perivascular invasion | 0.09 (0.000007) ** | 0.06 (0.0005) ** | 0.02 (0.02) ** |
| Tumour diameter | 0.1 (0.1) * | 0.1 (0.09) * | 0.2 (0.00) * |
| Tumour localization | 0.00 (0.3) ** | −0.02 (0.9) ** | 0.00 (0.4) ** |
| Bilirubin concentration | 0.05 (0.4) * | 0.01 (0.83) * | −0.04 (0.46) * |
| Parameter | Radical Treatment | Palliative Treatment |
|---|---|---|
| No. of patients | 73 | 69 |
| Stage | ||
| IA | 4 | 4 |
| IB | 8 | 0 |
| IIA | 11 | 1 |
| IIB | 33 | 8 |
| III | 17 | 21 |
| IV | 0 | 35 |
| Adjuvant chemotherapy | 58 | 57 |
| Gemcitabine | 23 | 19 |
| Folfirinox | 13 | 8 |
| Gemcitabine and Folfirinox | 22 | 30 |
| Refused/did not tolerate | 11 | 11 |
| Missing data | 4 | 1 |
| Overall Survival (Months) | Disease-Free Survival (Months) | ||||||
|---|---|---|---|---|---|---|---|
| Negative * | Positive ** | p | Negative * | Positive ** | p | ||
| Radical treatment | CEA median (IQR) | 15.6 (22.8) | 15.4 (16.6) | 0.3 | 8.7 (17.3) | 7.9 (11.0) | 0.38 |
| CEACAM6 median (IQR) | 17.0 (21.3) | 12.6 (14.1) | 0.017 | 8.7 (14.4) | 7.0 (19.0) | 0.094 | |
| CA19-9 median (IQR) | 16.4 (18.8) | 13.3 (21.8) | 0.64 | 8.1 (16.4) | 9.2 (11.9) | 0.23 | |
| Palliative treatment | CEA median (IQR) | 11.7 (13.6) | 13.6 (9.9) | 0.71 | |||
| CEACAM6 median (IQR) | 11.8 (7.9) | 13.5 (12.6) | 0.87 | ||||
| CA19-9 median (IQR) | 13.6 (16.4) | 12.0 (10.5) | 0.12 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kurlinkus, B.; Ger, M.; Kaupinis, A.; Jasiunas, E.; Valius, M.; Sileikis, A. CEACAM6’s Role as a Chemoresistance and Prognostic Biomarker for Pancreatic Cancer: A Comparison of CEACAM6’s Diagnostic and Prognostic Capabilities with Those of CA19-9 and CEA. Life 2021, 11, 542. https://doi.org/10.3390/life11060542
Kurlinkus B, Ger M, Kaupinis A, Jasiunas E, Valius M, Sileikis A. CEACAM6’s Role as a Chemoresistance and Prognostic Biomarker for Pancreatic Cancer: A Comparison of CEACAM6’s Diagnostic and Prognostic Capabilities with Those of CA19-9 and CEA. Life. 2021; 11(6):542. https://doi.org/10.3390/life11060542
Chicago/Turabian StyleKurlinkus, Benediktas, Marija Ger, Algirdas Kaupinis, Eugenijus Jasiunas, Mindaugas Valius, and Audrius Sileikis. 2021. "CEACAM6’s Role as a Chemoresistance and Prognostic Biomarker for Pancreatic Cancer: A Comparison of CEACAM6’s Diagnostic and Prognostic Capabilities with Those of CA19-9 and CEA" Life 11, no. 6: 542. https://doi.org/10.3390/life11060542
APA StyleKurlinkus, B., Ger, M., Kaupinis, A., Jasiunas, E., Valius, M., & Sileikis, A. (2021). CEACAM6’s Role as a Chemoresistance and Prognostic Biomarker for Pancreatic Cancer: A Comparison of CEACAM6’s Diagnostic and Prognostic Capabilities with Those of CA19-9 and CEA. Life, 11(6), 542. https://doi.org/10.3390/life11060542