
High Levels of TNF-α and TIM-3 as a Biomarker of Immune Reconstitution Inflammatory Syndrome in People with HIV Infection

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. IRIS Diagnosis
2.3. Soluble Levels Measurements in Plasma Samples by Enzyme-Linked Immunosorbent Assay (ELISA)
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Study Populations
3.2. sTIM-3 Increased in HIV+IRIS Patients at IRIS Onset
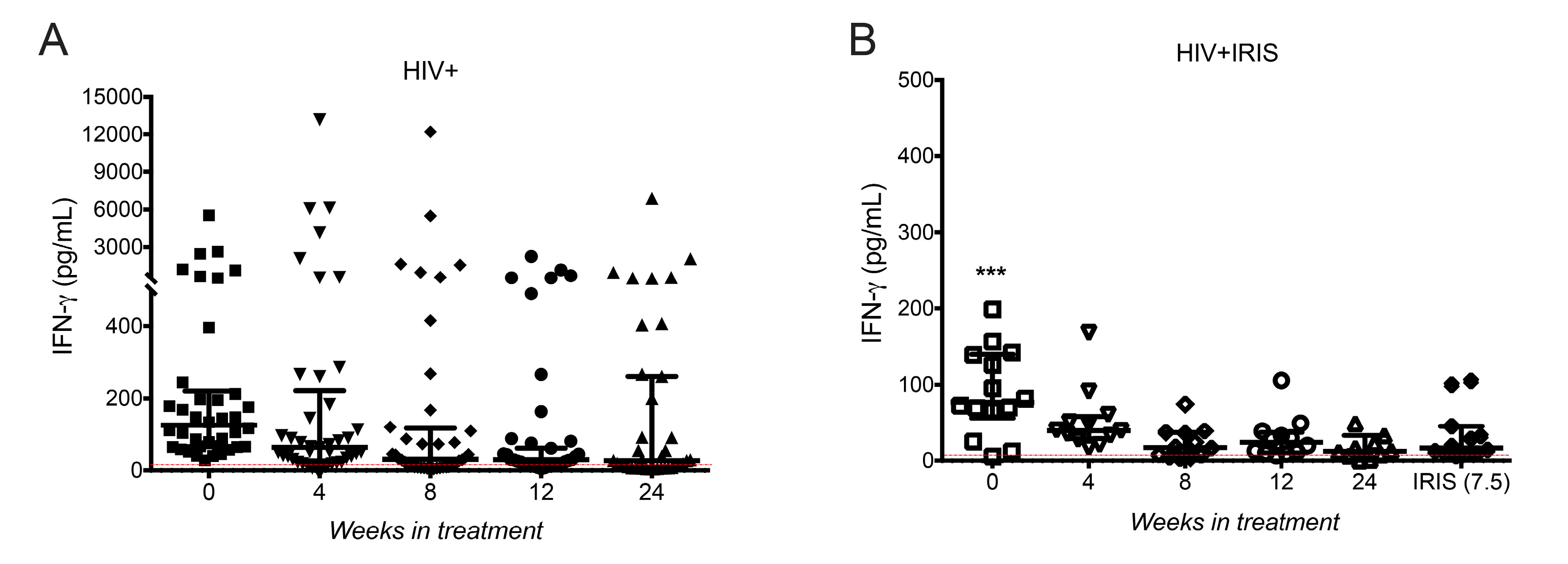
3.3. IFN-γ Levels Did Not Increase in HIV+IRIS Patients at IRIS Onset
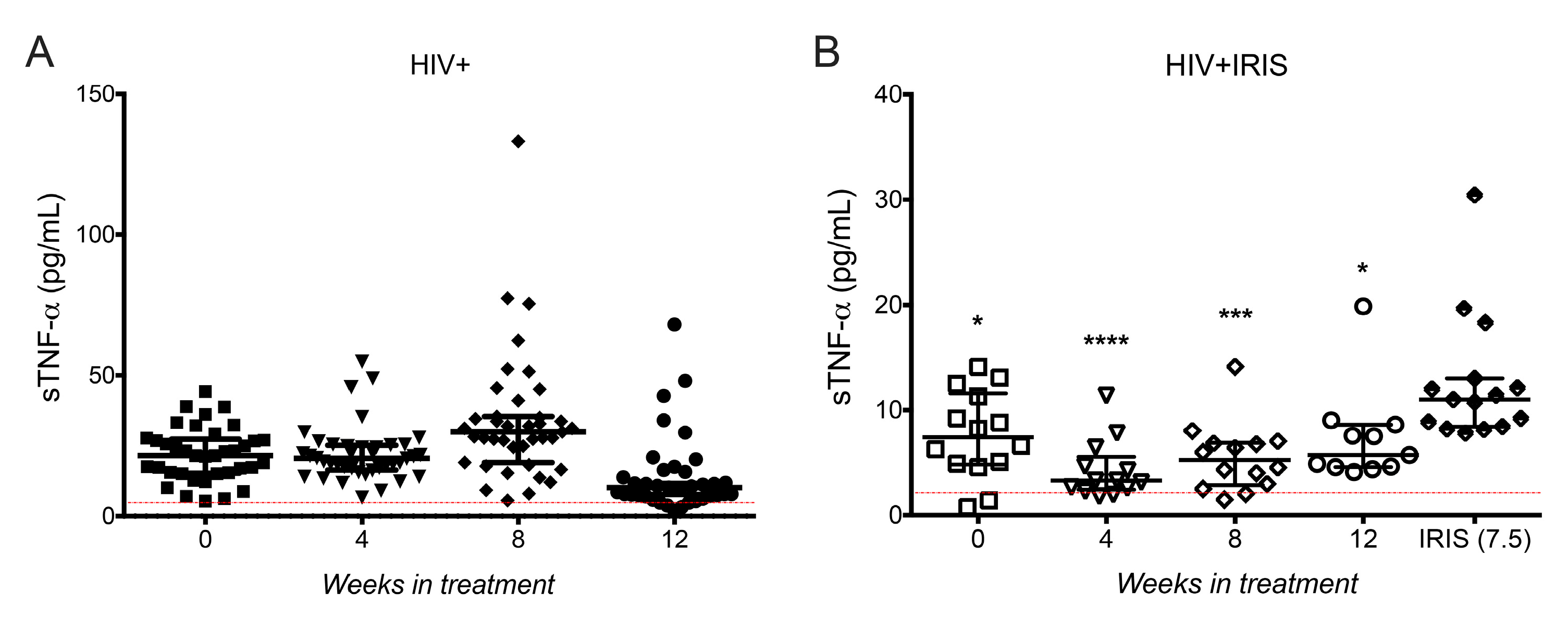
3.4. sTNF-α Was Increased at IRIS Onset
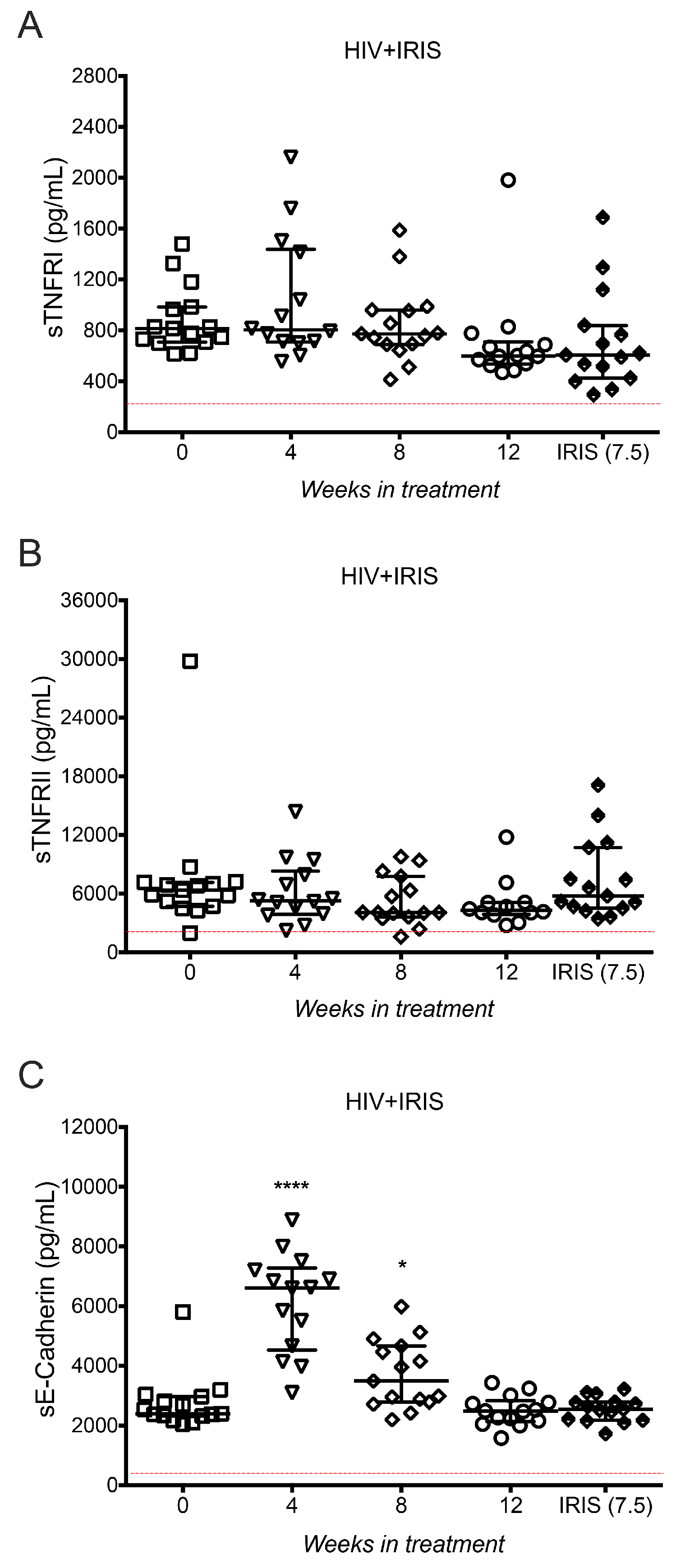
3.5. TNF-α Receptors and E-cadherin Were Not Affected at IRIS Events
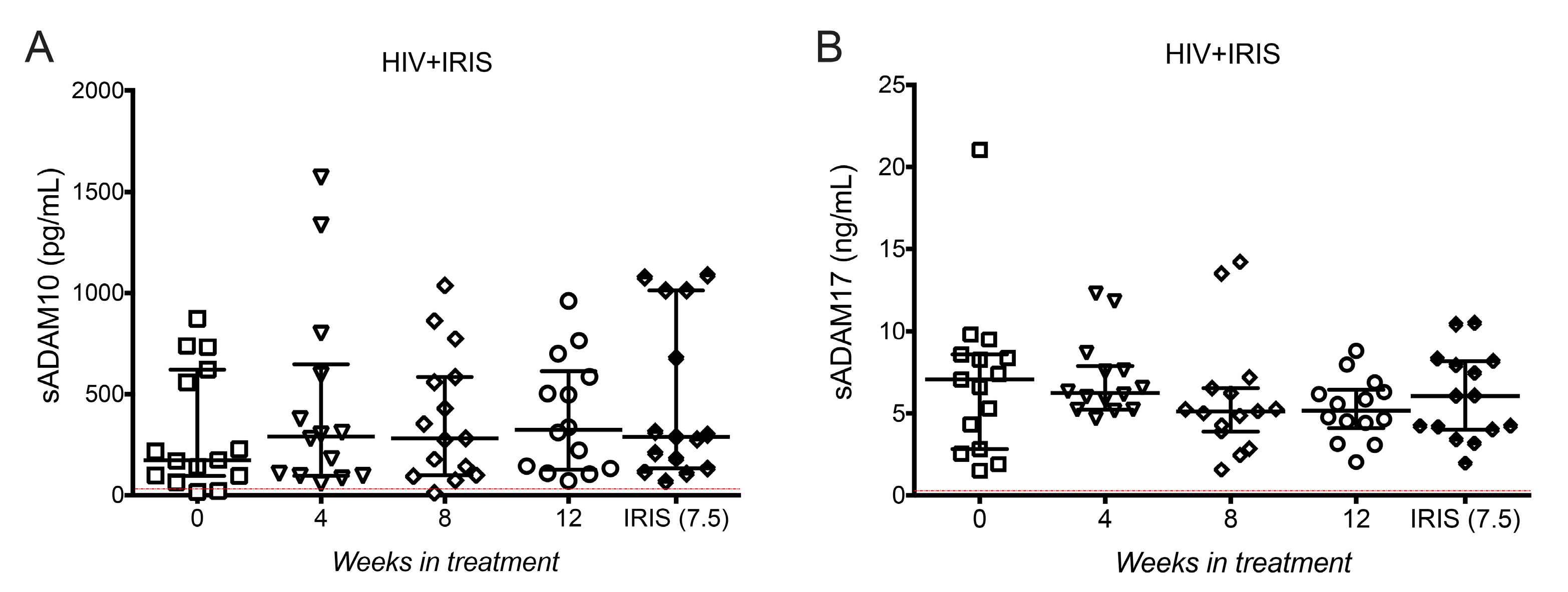
3.6. ADAM10 and ADAM17 Did Not Increase at the Onset of IRIS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sereti, I.; Rodger, A.J.; French, M.A. Biomarkers in Immune Reconstitution Inflammatory Syndrome: Signals from Pathogenesis. Curr. Opin. HIV AIDS 2010, 5, 504–510. [Google Scholar] [CrossRef]
- Antonelli, L.R.; Mahnke, Y.; Hodge, J.N.; Porter, B.O.; Barber, D.L.; Dersimonian, R.; Greenwald, J.H.; Roby, G.; Mican, J.; Sher, A.; et al. Elevated Frequencies of Highly Activated CD4+ T Cells in HIV+ Patients Developing Immune Reconstitution Inflammatory Syndrome. Blood 2010, 116, 3818–3827. [Google Scholar] [CrossRef]
- Murdoch, D.M.; Venter, W.D.F.; Feldman, C.; Van Rie, A. Incidence and Risk Factors for the Immune Reconstitution Inflammatory Syndrome in HIV Patients in South Africa: A Prospective Study. AIDS 2008, 22, 601–610. [Google Scholar] [CrossRef]
- Shelburne, S.A.; Visnegarwala, F.; Darcourt, J.; Graviss, E.A.; Giordano, T.P.; White, A.C.; Hamill, R.J. Incidence and Risk Factors for Immune Reconstitution Inflammatory Syndrome during Highly Active Antiretroviral Therapy. AIDS 2005, 19, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Meintjes, G.; Lawn, S.D.; Scano, F.; Maartens, G.; French, M.A.; Worodria, W.; Elliott, J.H.; Murdoch, D.; Wilkinson, R.J.; Seyler, C.; et al. Tuberculosis-Associated Immune Reconstitution Inflammatory Syndrome: Case Definitions for Use in Resource-Limited Settings. Lancet Infect. Dis. 2008, 8, 516–523. [Google Scholar] [CrossRef]
- Rallón, N.; García, M.; García-Samaniego, J.; Cabello, A.; Álvarez, B.; Restrepo, C.; Nistal, S.; Górgolas, M.; Benito, J.M. Expression of PD-1 and Tim-3 Markers of T-Cell Exhaustion Is Associated with CD4 Dynamics during the Course of Untreated and Treated HIV Infection. PLoS ONE 2018, 13, e0193829. [Google Scholar] [CrossRef] [PubMed]
- Golden-Mason, L.; Palmer, B.E.; Kassam, N.; Townshend-Bulson, L.; Livingston, S.; McMahon, B.J.; Castelblanco, N.; Kuchroo, V.; Gretch, D.R.; Rosen, H.R. Negative Immune Regulator Tim-3 Is Overexpressed on T Cells in Hepatitis C Virus Infection and Its Blockade Rescues Dysfunctional CD4+ and CD8+ T Cells. J. Virol. 2009, 83, 9122–9130. [Google Scholar] [CrossRef] [PubMed]
- Saitoh, H.; Ashino, Y.; Chagan-Yasutan, H.; Niki, T.; Hirashima, M.; Hattori, T. Rapid Decrease of Plasma Galectin-9 Levels in Patients with Acute HIV Infection after Therapy. Tohoku J. Exp. Med. 2012, 228, 157–161. [Google Scholar] [CrossRef]
- Espinosa, E.; Ormsby, C.E.; Vega-Barrientos, R.S.; Ruiz-Cruz, M.; Moreno-Coutiño, G.; Peña-Jiménez, Á.; Peralta-Prado, A.B.; Cantoral-Díaz, M.; Romero-Rodríguez, D.P.; Reyes-Terán, G. Risk Factors for Immune Reconstitution Inflammatory Syndrome under Combination Antiretroviral Therapy Can Be Aetiology-Specific. Int. J. STD AIDS 2010, 21, 573–579. [Google Scholar] [CrossRef]
- Yeni, P.G.; Hammer, S.M.; Hirsch, M.S.; Saag, M.S.; Schechter, M.; Carpenter, C.C.J.; Fischl, M.A.; Gatell, J.M.; Gazzard, B.G.; Jacobsen, D.M.; et al. Treatment for Adult HIV Infection: 2004 Recommendations of the International AIDS Society-USA Panel. J. Am. Med. Assoc. 2004, 292, 251–265. [Google Scholar] [CrossRef]
- Ocaña-Guzman, R.; Tellez-Navarrete, N.A.; Preciado-Garcia, M.; Ponce-Gallegos, M.A.; Buendia-Roldan, I.; Falfán-Valencia, R.; Chavez-Galan, L. Multidrug-Resistant Tuberculosis Patients Expressing the HLA-DRB1*04 Allele, and after Treatment They Show a Low Frequency of HLA-II+ Monocytes and a Chronic Systemic Inflammation. Microb. Pathog. 2021, 153, 104793. [Google Scholar] [CrossRef] [PubMed]
- Tandon, R.; Chew, G.M.; Byron, M.M.; Borrow, P.; Niki, T.; Hirashima, M.; Barbour, J.D.; Norris, P.J.; Lanteri, M.C.; Martin, J.N.; et al. Galectin-9 Is Rapidly Released during Acute HIV-1 Infection and Remains Sustained at High Levels despite Viral Suppression Even in Elite Controllers. AIDS Res. Hum. Retrovir. 2014, 30, 654–664. [Google Scholar] [CrossRef] [PubMed]
- Jost, S.; Moreno-Nieves, U.Y.; Garcia-Beltran, W.F.; Rands, K.; Reardon, J.; Toth, I.; Piechocka-Trocha, A.; Altfeld, M.; Addo, M.M. Dysregulated Tim-3 Expression on Natural Killer Cells Is Associated with Increased Galectin-9 Levels in HIV-1 Infection. Retrovirology 2013, 10, 74. [Google Scholar] [CrossRef]
- Zhao, J.; Shiratori, B.; Chagan-Yasutan, H.; Matsumoto, M.; Niki, T.; Tanaka, M.; Takahashi, Y.; Usami, O.; Ashino, Y.; Hattori, T. Secretion of IFN-γ Associated with Galectin-9 Production by Pleural Fluid Cells from a Patient with Extrapulmonary Tuberculosis. Int. J. Mol. Sci. 2017, 18, 1382. [Google Scholar] [CrossRef]
- Barber, D.L.; Andrade, B.B.; McBerry, C.; Sereti, I.; Sher, A. Role of IL-6 in Mycobacterium Avium—Associated Immune Reconstitution Inflammatory Syndrome. J. Immunol. 2014, 192, 676–682. [Google Scholar] [CrossRef]
- Tadokera, R.; Meintjes, G.; Skolimowska, K.H.; Wilkinson, K.A.; Matthews, K.; Seldon, R.; Chegou, N.N.; Maartens, G.; Rangaka, M.X.; Rebe, K.; et al. Hypercytokinaemia Accompanies HIV-Tuberculosis Immune Reconstitution Inflammatory Syndrome. Eur. Respir. J. 2011, 37, 1248–1259. [Google Scholar] [CrossRef] [PubMed]
- Möller-Hackbarth, K.; Dewitz, C.; Schweigert, O.; Trad, A.; Garbers, C.; Rose-John, S.; Scheller, J. A Disintegrin and Metalloprotease (ADAM) 10 and ADAM17 Are Major Sheddases of T Cell Immunoglobulin and Mucin Domain 3 (Tim-3). J. Biol. Chem. 2013, 288, 34529–34544. [Google Scholar] [CrossRef] [PubMed]
- Black, R.A.; Rauch, C.T.; Kozlosky, C.J.; Peschon, J.J.; Slack, J.L.; Wolfson, M.F.; Castner, B.J.; Stocking, K.L.; Reddy, P.; Srinivasan, S.; et al. A Metalloproteinase Disintegrin That Releases Tumour-Necrosis Factor-∅ from Cells. Nature 1997, 385, 729–733. [Google Scholar] [CrossRef]
- Porteu, F.; Nathan, C. Shedding of Tumor Necrosis Factor Receptors by Activated Human Neutrophils. J. Exp. Med. 1990, 172, 599–607. [Google Scholar] [CrossRef]
- Maretzky, T.; Reiss, K.; Ludwig, A.; Buchholz, J.; Scholz, F.; Proksch, E.; de Strooper, B.; Hartmann, D.; Saftig, P. ADAM10 Mediates E-Cadherin Shedding and Regulates Epithelial Cell-Cell Adhesion, Migration, and β-Catenin Translocation. Proc. Natl. Acad. Sci. USA 2005, 102, 9182–9187. [Google Scholar] [CrossRef]
- Müller, M.; Wandel, S.; Colebunders, R.; Attia, S.; Furrer, H.; Egger, M. Immune Reconstitution Inflammatory Syndrome in Patients Starting Antiretroviral Therapy for HIV Infection: A Systematic Review and Meta-Analysis. Lancet Infect. Dis. 2010, 10, 251–261. [Google Scholar] [CrossRef]
- Khaitan, A.; Unutmaz, D. Revisiting Immune Exhaustion during HIV Infection. Curr. HIV/AIDS Rep. 2011, 8, 4–11. [Google Scholar] [CrossRef]
- Valiathan, R.; Asthana, D. Increase in Frequencies of Circulating Th-17 Cells Correlates with Microbial Translocation, Immune Activation and Exhaustion in HIV-1 Infected Patients with Poor CD4 T-Cell Reconstitution. Immunobiology 2016, 221, 670–678. [Google Scholar] [CrossRef]
- Goovaerts, O.; Massinga-Loembé, M.; Ondoa, P.; Ceulemans, A.; Worodria, W.; Mayanja-Kizza, H.; Colebunders, R.; Kestens, L. Increased KLRG1 and PD-1 Expression on CD8 T Lymphocytes in TB-IRIS. PLoS ONE 2019, 14, e0215991. [Google Scholar] [CrossRef] [PubMed]
- Espinosa, E.; Romero-Rodríguez, D.P.; Cantoral-Díaz, M.-T.; Reyes-Terán, G. Transient Expansion of Activated CD8+ T Cells Characterizes Tuberculosis-Associated Immune Reconstitution Inflammatory Syndrome in Patients with HIV: A Case Control Study. J. Inflamm. 2013, 10, 21. [Google Scholar] [CrossRef]
- Boulware, D.R.; Bonham, S.C.; Meya, D.B.; Wiesner, D.L.; Park, G.S.; Kambugu, A.; Janoff, E.N.; Bohjanen, P.R. Paucity of Initial Cerebrospinal Fluid Inflammation in Cryptococcal Meningitis Is Associated with Subsequent Immune Reconstitution Inflammatory Syndrome. J. Infect. Dis. 2010, 202, 962–970. [Google Scholar] [CrossRef] [PubMed]
- Streeck, H.; Kwon, D.S.; Pyo, A.; Flanders, M.; Chevalier, M.F.; Law, K.; Jülg, B.; Trocha, K.; Jolin, J.S.; Anahtar, M.N.; et al. Epithelial Adhesion Molecules Can Inhibit HIV-1-Specific CD8+ T-Cell Functions. Blood 2011, 117, 5112–5122. [Google Scholar] [CrossRef] [PubMed]
- Clayton, K.L.; Douglas-Vail, M.B.; Rahman, A.K.M.N.; Medcalf, K.E.; Xie, I.Y.; Chew, G.M.; Tandon, R.; Lanteri, M.C.; Norris, P.J.; Deeks, S.G.; et al. Soluble T Cell Immunoglobulin Mucin Domain 3 Is Shed from CD8 + T Cells by the Sheddase ADAM10, Is Increased in Plasma during Untreated HIV Infection, and Correlates with HIV Disease Progression. J. Virol. 2015, 89, 3723–3736. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | All, n = 61 | HIV+, n = 46 (75%) | HIV+IRIS, n = 15, (25%) |
|---|---|---|---|
| Age (median) IQR | 34 (29–39) | 32 (29–39) | 36 (29–40) |
| CD4 count cells/ml, median (IQR) | |||
| Week 0 | 55 (31–105) | 54 (31–124) | 58 (25–101) |
| Week 4 post-ART | 151 (79–215) | 132 (75–214) | 165 (146–217) |
| Week 8 post-ART | 159 (117–252) | 158 (122–256) | 160 (113–215) |
| Week 12 post-ART | 164 (102–231) | 166 (104–247) | 160 (100–230) |
| Week 24 post-ART | 199 (152–274) | 204 (148–274) | 179 (161–274) |
| CD4/CD8 ratio, median (IQR) | |||
| Baseline | 0.07 (0.04–0.13) | 0.07 (0.04–0.13) | 0.08 (0.03–0.13) |
| Week 4 post-ART | 0.14 (0.09–0.25) | 0.14 (0.10–0.25) | 0.13 (0.08–0.28) |
| Week 8 post-ART | 0.17 (0.1–0.25) | 0.17 (0.11–0.24) | 0.14 (0.09–0.25) |
| Week 12 post-ART | 0.17 (0.11–0.26) | 0.18 (0.12–0.27) | 0.15 (0.11–0.22) |
| Week 24 post-ART | 0.21 (0.14–0.29) | 0.21 (0.14–0.28) | 0.20 (0.12–0.31) |
| HIV Viral load, Log10 copies/ml, median (IQR) | |||
| Baseline | 5.57 (5.1–5.8) | 5.5 (5.1–5.8) | 5.8 (5.2–6.0) |
| Week 4 post-ART | 2.8 (2.6–3.1) | 2.8 (2.6–3.1) | 2.8 (2.5–3.1) |
| Week 8 post-ART | 2.2 (1.6–2.6) | 2.2 (1.8–2.6) | 2.0 (1.6–2.6) |
| Week 12 post-ART | 1.8 (1.6–2.6) | 1.9 (1.6–2.6) | 1.7 (1.6–2.6) |
| Week 24 post-ART | 1.6 (1.6–1.6) | 1.6 (1.6–1.6) | 1.6 (1.6–1.6) |
| Parameters | n = 15 |
|---|---|
| Time to IRIS onset, weeks, median (IQR) | 7.5 (4.1–19.0) |
| Manifestations related with IRIS | |
| Mycobacteria, n (%) | 4 (27%) |
| Mycobacterium tuberculosis | 2 |
| Mycobacterium avium complex | 2 |
| Herpesviruses, n (%) | 7 (47%) |
| Herpes Zoster | 4 |
| Herpes Simplex Virus | 2 |
| Cytomegalovirus | 1 |
| Other dermatological manifestations, n (%) | 3 (20%) |
| Molluscum contagiosum | 1 |
| Eosinophilic folliculitis | 2 |
| Lymphadenopathy not specified, n(%) | 1 (6%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramon-Luing, L.A.; Ocaña-Guzman, R.; Téllez-Navarrete, N.A.; Preciado-García, M.; Romero-Rodríguez, D.P.; Espinosa, E.; Reyes-Terán, G.; Chavez-Galan, L. High Levels of TNF-α and TIM-3 as a Biomarker of Immune Reconstitution Inflammatory Syndrome in People with HIV Infection. Life 2021, 11, 527. https://doi.org/10.3390/life11060527
Ramon-Luing LA, Ocaña-Guzman R, Téllez-Navarrete NA, Preciado-García M, Romero-Rodríguez DP, Espinosa E, Reyes-Terán G, Chavez-Galan L. High Levels of TNF-α and TIM-3 as a Biomarker of Immune Reconstitution Inflammatory Syndrome in People with HIV Infection. Life. 2021; 11(6):527. https://doi.org/10.3390/life11060527
Chicago/Turabian StyleRamon-Luing, Lucero A., Ranferi Ocaña-Guzman, Norma A. Téllez-Navarrete, Mario Preciado-García, Dámaris P. Romero-Rodríguez, Enrique Espinosa, Gustavo Reyes-Terán, and Leslie Chavez-Galan. 2021. "High Levels of TNF-α and TIM-3 as a Biomarker of Immune Reconstitution Inflammatory Syndrome in People with HIV Infection" Life 11, no. 6: 527. https://doi.org/10.3390/life11060527
APA StyleRamon-Luing, L. A., Ocaña-Guzman, R., Téllez-Navarrete, N. A., Preciado-García, M., Romero-Rodríguez, D. P., Espinosa, E., Reyes-Terán, G., & Chavez-Galan, L. (2021). High Levels of TNF-α and TIM-3 as a Biomarker of Immune Reconstitution Inflammatory Syndrome in People with HIV Infection. Life, 11(6), 527. https://doi.org/10.3390/life11060527