
Non-Albumin Proteinuria (NAP) as a Complementary Marker for Diabetic Kidney Disease (DKD)


Abstract
1. Introduction
2. What NAP Reflects in DKD
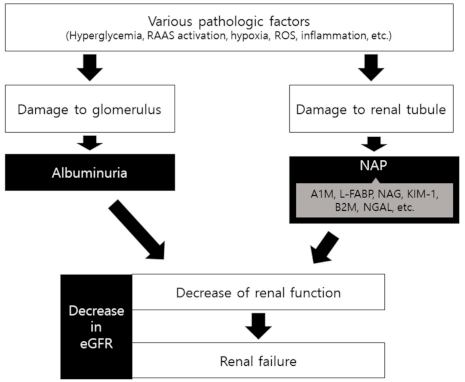
2.1. Pathogenesis and Structural Changes of DKD
2.2. Albuminuria and NAP
2.2.1. Albuminuria
2.2.2. NAP and Tubular Injury
3. Clinical Significance of NAP in DKD
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tuttle, K.R.; Bakris, G.L.; Bilous, R.W.; Chiang, J.L.; de Boer, I.H.; Goldstein-Fuchs, J.; Hirsch, I.B.; Kalantar-Zadeh, K.; Narva, A.S.; Navaneethan, S.D.; et al. Diabetic kidney disease: A report from an ADA Consensus Conference. Diabetes Care 2014, 37, 2864–2883. [Google Scholar] [CrossRef]
- Association, A.D. 11. Microvascular Complications and Foot Care: Standards of Medical Care in Diabetes-2021. Diabetes Care 2021, 44, S151–S167. [Google Scholar] [CrossRef]
- Fox, C.S.; Matsushita, K.; Woodward, M.; Bilo, H.J.; Chalmers, J.; Heerspink, H.J.; Lee, B.J.; Perkins, R.M.; Rossing, P.; Sairenchi, T.; et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes: A meta-analysis. Lancet 2012, 380, 1662–1673. [Google Scholar] [CrossRef]
- Nauta, F.L.; Scheven, L.; Meijer, E.; van Oeveren, W.; de Jong, P.E.; Bakker, S.J.; Gansevoort, R.T. Glomerular and tubular damage markers in individuals with progressive albuminuria. Clin. J. Am. Soc. Nephrol. CJASN 2013, 8, 1106–1114. [Google Scholar] [CrossRef]
- Mogensen, C.E. Microalbuminuria, blood pressure and diabetic renal disease: Origin and development of ideas. Diabetologia 1999, 42, 263–285. [Google Scholar] [CrossRef]
- De Nicola, L.; Gabbai, F.B.; Liberti, M.E.; Sagliocca, A.; Conte, G.; Minutolo, R. Sodium/glucose cotransporter 2 inhibitors and prevention of diabetic nephropathy: Targeting the renal tubule in diabetes. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2014, 64, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Alicic, R.Z.; Rooney, M.T.; Tuttle, K.R. Diabetic Kidney Disease: Challenges, Progress, and Possibilities. Clin. J. Am. Soc. Nephrol. CJASN 2017, 12, 2032–2045. [Google Scholar] [CrossRef]
- Boronat, M.; García-Cantón, C.; Quevedo, V.; Lorenzo, D.L.; López-Ríos, L.; Batista, F.; Riaño, M.; Saavedra, P.; Checa, M.D. Non-albuminuric renal disease among subjects with advanced stages of chronic kidney failure related to type 2 diabetes mellitus. Ren. Fail. 2014, 36, 166–170. [Google Scholar] [CrossRef] [PubMed]
- Klimontov, V.V.; Korbut, A.I. Albuminuric and non-albuminuric patterns of chronic kidney disease in type 2 diabetes. Diabetes Metab. Syndr. 2019, 13, 474–479. [Google Scholar] [CrossRef]
- Fiseha, T.; Tamir, Z. Urinary Markers of Tubular Injury in Early Diabetic Nephropathy. Int. J. Nephrol. 2016, 2016, 4647685. [Google Scholar] [CrossRef]
- Kamijo-Ikemori, A.; Sugaya, T.; Kimura, K. Novel urinary biomarkers in early diabetic kidney disease. Curr. Diabetes Rep. 2014, 14, 513. [Google Scholar] [CrossRef]
- Al-Hazmi, S.F.; Gad, H.G.M.; Alamoudi, A.A.; Eldakhakhny, B.M.; Binmahfooz, S.K.; Alhozali, A.M. Evaluation of early biomarkers of renal dysfunction in diabetic patients. Saudi Med. J. 2020, 41, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.S.; Song, S.H.; Kim, I.J.; Kim, W.J.; Jeon, Y.K.; Kim, B.H.; Kwak, I.S.; Lee, E.K.; Kim, Y.K. Nonalbuminuric proteinuria as a biomarker for tubular damage in early development of nephropathy with type 2 diabetic patients. Diabetes Metab. Res. Rev. 2014, 30, 736–741. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Oh, S.Y.; Kim, E.H.; Lee, M.J.; Jeon, Y.K.; Kim, B.H.; Kim, J.M.; Kim, Y.K.; Kim, S.S.; Kim, I.J. Addition of nonalbumin proteinuria to albuminuria improves prediction of type 2 diabetic nephropathy progression. Diabetol. Metab. Syndr. 2017, 9, 68. [Google Scholar] [CrossRef] [PubMed]
- DCCT/EDIC Research Group. Effect of intensive diabetes treatment on albuminuria in type 1 diabetes: Long-term follow-up of the Diabetes Control and Complications Trial and Epidemiology of Diabetes Interventions and Complications study. Lancet Diabetes Endocrinol. 2014, 2, 793–800. [Google Scholar] [CrossRef]
- de Boer, I.H.; Sun, W.; Cleary, P.A.; Lachin, J.M.; Molitch, M.E.; Steffes, M.W.; Zinman, B. Intensive diabetes therapy and glomerular filtration rate in type 1 diabetes. N. Engl. J. Med. 2011, 365, 2366–2376. [Google Scholar] [CrossRef]
- UK Prospective Diabetes Study Group. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet 1998, 352, 854–865. [Google Scholar] [CrossRef]
- Patel, A.; MacMahon, S.; Chalmers, J.; Neal, B.; Billot, L.; Woodward, M.; Marre, M.; Cooper, M.; Glasziou, P.; Grobbee, D.; et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N. Engl. J. Med. 2008, 358, 2560–2572. [Google Scholar] [CrossRef]
- Melmed, S.; Polonsky, K.S.; Larsen, P.R.; Kronenberg HMMelmed, S.; Polonsky, K.S.; Larsen, P.R.; Kronenberg, H.M. Williams Textbook of Endocrinology, 12th ed.; Saunders: Philadelphia, PA, USA, 2011. [Google Scholar]
- Cooper, M.E. Interaction of metabolic and haemodynamic factors in mediating experimental diabetic nephropathy. Diabetologia 2001, 44, 1957–1972. [Google Scholar] [CrossRef]
- Thomas, M.C.; Tikellis, C.; Burns, W.M.; Bialkowski, K.; Cao, Z.; Coughlan, M.T.; Jandeleit-Dahm, K.; Cooper, M.E.; Forbes, J.M. Interactions between renin angiotensin system and advanced glycation in the kidney. J. Am. Soc. Nephrol. JASN 2005, 16, 2976–2984. [Google Scholar] [CrossRef]
- Forbes, J.M.; Cooper, M.E.; Oldfield, M.D.; Thomas, M.C. Role of advanced glycation end products in diabetic nephropathy. J. Am. Soc. Nephrol. JASN 2003, 14, S254–S258. [Google Scholar] [CrossRef]
- Saraheimo, M.; Teppo, A.M.; Forsblom, C.; Fagerudd, J.; Groop, P.H. Diabetic nephropathy is associated with low-grade inflammation in Type 1 diabetic patients. Diabetologia 2003, 46, 1402–1407. [Google Scholar] [CrossRef] [PubMed]
- Pan, H.Z.; Zhang, L.; Guo, M.Y.; Sui, H.; Li, H.; Wu, W.H.; Qu, N.Q.; Liang, M.H.; Chang, D. The oxidative stress status in diabetes mellitus and diabetic nephropathy. Acta Diabetol. 2010, 47 (Suppl. 1), 71–76. [Google Scholar] [CrossRef]
- Tervaert, T.W.; Mooyaart, A.L.; Amann, K.; Cohen, A.H.; Cook, H.T.; Drachenberg, C.B.; Ferrario, F.; Fogo, A.B.; Haas, M.; de Heer, E.; et al. Pathologic classification of diabetic nephropathy. J. Am. Soc. Nephrol. JASN 2010, 21, 556–563. [Google Scholar] [CrossRef] [PubMed]
- Fioretto, P.; Mauer, M. Histopathology of diabetic nephropathy. Semin. Nephrol. 2007, 27, 195–207. [Google Scholar] [CrossRef] [PubMed]
- Krolewski, A.S. Progressive renal decline: The new paradigm of diabetic nephropathy in type 1 diabetes. Diabetes Care 2015, 38, 954–962. [Google Scholar] [CrossRef]
- Retnakaran, R.; Cull, C.A.; Thorne, K.I.; Adler, A.I.; Holman, R.R. Risk factors for renal dysfunction in type 2 diabetes: U.K. Prospective Diabetes Study 74. Diabetes 2006, 55, 1832–1839. [Google Scholar] [CrossRef]
- Gilbert, R.E.; Cooper, M.E. The tubulointerstitium in progressive diabetic kidney disease: More than an aftermath of glomerular injury? Kidney Int. 1999, 56, 1627–1637. [Google Scholar] [CrossRef]
- Gilbert, R.E. Proximal Tubulopathy: Prime Mover and Key Therapeutic Target in Diabetic Kidney Disease. Diabetes 2017, 66, 791–800. [Google Scholar] [CrossRef] [PubMed]
- DeFronzo, R.A.; Hompesch, M.; Kasichayanula, S.; Liu, X.; Hong, Y.; Pfister, M.; Morrow, L.A.; Leslie, B.R.; Boulton, D.W.; Ching, A.; et al. Characterization of renal glucose reabsorption in response to dapagliflozin in healthy subjects and subjects with type 2 diabetes. Diabetes Care 2013, 36, 3169–3176. [Google Scholar] [CrossRef] [PubMed]
- Körner, A.; Eklöf, A.C.; Celsi, G.; Aperia, A. Increased renal metabolism in diabetes. Mechanism and functional implications. Diabetes 1994, 43, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Meyer, C.; Stumvoll, M.; Nadkarni, V.; Dostou, J.; Mitrakou, A.; Gerich, J. Abnormal renal and hepatic glucose metabolism in type 2 diabetes mellitus. J. Clin. Investig. 1998, 102, 619–624. [Google Scholar] [CrossRef] [PubMed]
- Zhan, M.; Usman, I.M.; Sun, L.; Kanwar, Y.S. Disruption of renal tubular mitochondrial quality control by Myo-inositol oxygenase in diabetic kidney disease. J. Am. Soc. Nephrol. JASN 2015, 26, 1304–1321. [Google Scholar] [CrossRef] [PubMed]
- Lindenmeyer, M.T.; Kretzler, M.; Boucherot, A.; Berra, S.; Yasuda, Y.; Henger, A.; Eichinger, F.; Gaiser, S.; Schmid, H.; Rastaldi, M.P.; et al. Interstitial vascular rarefaction and reduced VEGF-A expression in human diabetic nephropathy. J. Am. Soc. Nephrol. JASN 2007, 18, 1765–1776. [Google Scholar] [CrossRef] [PubMed]
- Yacoub, R.; Campbell, K.N. Inhibition of RAS in diabetic nephropathy. Int. J. Nephrol. Renov. Dis. 2015, 8, 29–40. [Google Scholar] [CrossRef]
- Vallon, V. The proximal tubule in the pathophysiology of the diabetic kidney. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2011, 300, R1009–R1022. [Google Scholar] [CrossRef]
- Forrester, S.J.; Kawai, T.; O’Brien, S.; Thomas, W.; Harris, R.C.; Eguchi, S. Epidermal Growth Factor Receptor Transactivation: Mechanisms, Pathophysiology, and Potential Therapies in the Cardiovascular System. Annu. Rev. Pharmacol. Toxicol. 2016, 56, 627–653. [Google Scholar] [CrossRef]
- Parving, H.H. Microalbuminuria in essential hypertension and diabetes mellitus. J. Hypertens. Suppl. Off. J. Int. Soc. Hypertens. 1996, 14, S89–S93. [Google Scholar] [CrossRef]
- Satchell, S.C.; Tooke, J.E. What is the mechanism of microalbuminuria in diabetes: A role for the glomerular endothelium? Diabetologia 2008, 51, 714–725. [Google Scholar] [CrossRef] [PubMed]
- Afkarian, M.; Sachs, M.C.; Kestenbaum, B.; Hirsch, I.B.; Tuttle, K.R.; Himmelfarb, J.; de Boer, I.H. Kidney disease and increased mortality risk in type 2 diabetes. J. Am. Soc. Nephrol. JASN 2013, 24, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Pugliese, G. Updating the natural history of diabetic nephropathy. Acta Diabetol. 2014, 51, 905–915. [Google Scholar] [CrossRef] [PubMed]
- Kramer, H.J.; Nguyen, Q.D.; Curhan, G.; Hsu, C.Y. Renal insufficiency in the absence of albuminuria and retinopathy among adults with type 2 diabetes mellitus. JAMA 2003, 289, 3273–3277. [Google Scholar] [CrossRef] [PubMed]
- MacIsaac, R.J.; Tsalamandris, C.; Panagiotopoulos, S.; Smith, T.J.; McNeil, K.J.; Jerums, G. Nonalbuminuric renal insufficiency in type 2 diabetes. Diabetes Care 2004, 27, 195–200. [Google Scholar] [CrossRef]
- Molitch, M.E.; Steffes, M.; Sun, W.; Rutledge, B.; Cleary, P.; de Boer, I.H.; Zinman, B.; Lachin, J. Development and progression of renal insufficiency with and without albuminuria in adults with type 1 diabetes in the diabetes control and complications trial and the epidemiology of diabetes interventions and complications study. Diabetes Care 2010, 33, 1536–1543. [Google Scholar] [CrossRef] [PubMed]
- Thomas, M.C.; Macisaac, R.J.; Jerums, G.; Weekes, A.; Moran, J.; Shaw, J.E.; Atkins, R.C. Nonalbuminuric renal impairment in type 2 diabetic patients and in the general population (national evaluation of the frequency of renal impairment cO-existing with NIDDM [NEFRON] 11). Diabetes Care 2009, 32, 1497–1502. [Google Scholar] [CrossRef] [PubMed]
- Mottl, A.K.; Kwon, K.S.; Mauer, M.; Mayer-Davis, E.J.; Hogan, S.L.; Kshirsagar, A.V. Normoalbuminuric diabetic kidney disease in the U.S. population. J. Diabetes Its Complicat. 2013, 27, 123–127. [Google Scholar] [CrossRef]
- Ekström, B.; Peterson, P.A.; Berggård, I. A urinary and plasma alpha1-glycoprotein of low molecular weight: Isolation and some properties. Biochem. Biophys. Res. Commun. 1975, 65, 1427–1433. [Google Scholar] [CrossRef]
- Petrica, L.; Vlad, A.; Gluhovschi, G.; Zamfir, A.; Popescu, C.; Gadalean, F.; Dumitrascu, V.; Vlad, D.; Popescu, R.; Velciov, S.; et al. Glycated peptides are associated with proximal tubule dysfunction in type 2 diabetes mellitus. Int. J. Clin. Exp. Med. 2015, 8, 2516–2525. [Google Scholar]
- Hong, C.Y.; Hughes, K.; Chia, K.S.; Ng, V.; Ling, S.L. Urinary alpha1-microglobulin as a marker of nephropathy in type 2 diabetic Asian subjects in Singapore. Diabetes Care 2003, 26, 338–342. [Google Scholar] [CrossRef]
- Petrica, L.; Petrica, M.; Vlad, A.; Jianu, D.C.; Gluhovschi, G.; Ianculescu, C.; Firescu, C.; Dumitrascu, V.; Giju, S.; Gluhovschi, C.; et al. Proximal tubule dysfunction is dissociated from endothelial dysfunction in normoalbuminuric patients with type 2 diabetes mellitus: A cross-sectional study. Nephron Clin. Pract. 2011, 118, c155–c164. [Google Scholar] [CrossRef]
- Suzuki, K.; Babazono, T.; Murata, H.; Iwamoto, Y. Clinical significance of urinary liver-type fatty acid-binding protein in patients with diabetic nephropathy. Diabetes Care 2005, 28, 2038–2039. [Google Scholar] [CrossRef] [PubMed]
- Kamijo-Ikemori, A.; Sugaya, T.; Yasuda, T.; Kawata, T.; Ota, A.; Tatsunami, S.; Kaise, R.; Ishimitsu, T.; Tanaka, Y.; Kimura, K. Clinical significance of urinary liver-type fatty acid-binding protein in diabetic nephropathy of type 2 diabetic patients. Diabetes Care 2011, 34, 691–696. [Google Scholar] [CrossRef]
- Nielsen, S.E.; Sugaya, T.; Hovind, P.; Baba, T.; Parving, H.H.; Rossing, P. Urinary liver-type fatty acid-binding protein predicts progression to nephropathy in type 1 diabetic patients. Diabetes Care 2010, 33, 1320–1324. [Google Scholar] [CrossRef] [PubMed]
- Panduru, N.M.; Forsblom, C.; Saraheimo, M.; Thorn, L.; Bierhaus, A.; Humpert, P.M.; Groop, P.H. Urinary liver-type fatty acid-binding protein and progression of diabetic nephropathy in type 1 diabetes. Diabetes Care 2013, 36, 2077–2083. [Google Scholar] [CrossRef] [PubMed]
- Price, R.G. Measurement of N-acetyl-beta-glucosaminidase and its isoenzymes in urine methods and clinical applications. Eur. J. Clin. Chem. Clin. Biochem. J. Forum Eur. Clin. Chem. Soc. 1992, 30, 693–705. [Google Scholar]
- Assal, H.S.; Tawfeek, S.; Rasheed, E.A.; El-Lebedy, D.; Thabet, E.H. Serum cystatin C and tubular urinary enzymes as biomarkers of renal dysfunction in type 2 diabetes mellitus. Clin. Med. Insights Endocrinol. Diabetes 2013, 6, 7–13. [Google Scholar] [CrossRef]
- Mohammadi-Karakani, A.; Asgharzadeh-Haghighi, S.; Ghazi-Khansari, M.; Hosseini, R. Determination of urinary enzymes as a marker of early renal damage in diabetic patients. J. Clin. Lab. Anal. 2007, 21, 413–417. [Google Scholar] [CrossRef]
- Kim, S.R.; Lee, Y.H.; Lee, S.G.; Kang, E.S.; Cha, B.S.; Kim, J.H.; Lee, B.W. Urinary N-acetyl-β-D-glucosaminidase, an early marker of diabetic kidney disease, might reflect glucose excursion in patients with type 2 diabetes. Medicine 2016, 95, e4114. [Google Scholar] [CrossRef] [PubMed]
- Hong, N.; Lee, M.; Park, S.; Lee, Y.H.; Jin, S.M.; Kim, J.H.; Lee, B.W. Elevated urinary N-acetyl-β-D-glucosaminidase is associated with high glycoalbumin-to-hemoglobin A1c ratio in type 1 diabetes patients with early diabetic kidney disease. Sci. Rep. 2018, 8, 6710. [Google Scholar] [CrossRef]
- Kim, S.R.; Lee, Y.H.; Lee, S.G.; Kang, E.S.; Cha, B.S.; Lee, B.W. The renal tubular damage marker urinary N-acetyl-β-D-glucosaminidase may be more closely associated with early detection of atherosclerosis than the glomerular damage marker albuminuria in patients with type 2 diabetes. Cardiovasc. Diabetol. 2017, 16, 1–11. [Google Scholar] [CrossRef]
- Lee, M.; Hong, N.; Lee, Y.H.; Kang, E.S.; Cha, B.S.; Lee, B.W. Elevated N-acetyl-β-d-glucosaminidase, a urinary tubular damage marker, is a significant predictor of carotid artery atherosclerosis in type 1 diabetes, independent of albuminuria: A cross-sectional study. J. Diabetes Its Complicat. 2018, 32, 777–783. [Google Scholar] [CrossRef]
- Bonventre, J.V. Kidney injury molecule-1 (KIM-1): A urinary biomarker and much more. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. Eur. Ren. Assoc. 2009, 24, 3265–3268. [Google Scholar] [CrossRef]
- Nauta, F.L.; Boertien, W.E.; Bakker, S.J.; van Goor, H.; van Oeveren, W.; de Jong, P.E.; Bilo, H.; Gansevoort, R.T. Glomerular and tubular damage markers are elevated in patients with diabetes. Diabetes Care 2011, 34, 975–981. [Google Scholar] [CrossRef]
- Kim, S.S.; Song, S.H.; Kim, I.J.; Yang, J.Y.; Lee, J.G.; Kwak, I.S.; Kim, Y.K. Clinical implication of urinary tubular markers in the early stage of nephropathy with type 2 diabetic patients. Diabetes Res. Clin. Pract. 2012, 97, 251–257. [Google Scholar] [CrossRef]
- Ucakturk, A.; Avci, B.; Genc, G.; Ozkaya, O.; Aydin, M. Kidney injury molecule-1 and neutrophil gelatinase associated lipocalin in normoalbuminuric diabetic children. J. Pediatric Endocrinol. Metab. JPEM 2016, 29, 145–151. [Google Scholar] [CrossRef]
- Conway, B.R.; Manoharan, D.; Manoharan, D.; Jenks, S.; Dear, J.W.; McLachlan, S.; Strachan, M.W.; Price, J.F. Measuring urinary tubular biomarkers in type 2 diabetes does not add prognostic value beyond established risk factors. Kidney Int. 2012, 82, 812–818. [Google Scholar] [CrossRef] [PubMed]
- Atoh, K.; Itoh, H.; Haneda, M. Serum indoxyl sulfate levels in patients with diabetic nephropathy: Relation to renal function. Diabetes Res. Clin. Pract. 2009, 83, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Guarda, N.S.; Bollick, Y.S.; de Carvalho, J.A.M.; Premaor, M.O.; Comim, F.V.; Moresco, R.N. High Serum Uric Acid Is Associated with Tubular Damage and Kidney Inflammation in Patients with Type 2 Diabetes. Dis. Markers 2019, 2019, 6025804. [Google Scholar] [CrossRef] [PubMed]
- Halimi, J.M.; Matthias, B.; Al-Najjar, A.; Laouad, I.; Chatelet, V.; Marlière, J.F.; Nivet, H.; Lebranchu, Y. Respective predictive role of urinary albumin excretion and nonalbumin proteinuria on graft loss and death in renal transplant recipients. Am. J. Transplant. Off. J. Am. Soc. Transplant. Am. Soc. Transpl. Surg. 2007, 7, 2775–2781. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.; Lee, Y.H.; Kang, E.S.; Cha, B.S.; Lee, B.W. Glucometabolic characteristics and higher vascular complication risk in Korean patients with type 2 diabetes with non-albumin proteinuria. J. Diabetes Its Complicat. 2019, 33, 585–591. [Google Scholar] [CrossRef]
- Bae, J.; Lee, Y.H.; Kang, E.S.; Cha, B.S.; Lee, B.W. Proteinuria is Associated with Carotid Artery Atherosclerosis in Non-Albuminuric Type 2 Diabetes: A Cross-Sectional Study. J. Clin. Med. 2020, 9, 136. [Google Scholar] [CrossRef] [PubMed]
- Fraser, S.D.; Roderick, P.J.; McIntyre, N.J.; Harris, S.; McIntyre, C.; Fluck, R.; Taal, M.W. Assessment of proteinuria in patients with chronic kidney disease stage 3: Albuminuria and non-albumin proteinuria. PLoS ONE 2014, 9, e98261. [Google Scholar] [CrossRef] [PubMed]
- Katayev, A.; Zebelman, A.M.; Sharp, T.M.; Samantha, F.; Bernstein, R.K. Prevalence of isolated non-albumin proteinuria in the US population tested for both, urine total protein and urine albumin: An unexpected discovery. Clin. Biochem. 2017, 50, 262–269. [Google Scholar] [CrossRef]
- Sakatsume, M.; Kubota, R.; Ogawa, A.; Narita, I.; Matsuda, T.; Shiba, K.; Gejyo, F. Rapid and sensitive electrophoresis of urinary protein clearly reveals the pathophysiological feature of renal diseases. Nephrology 2007, 12, 191–196. [Google Scholar] [CrossRef]
- Methven, S.; MacGregor, M.S.; Traynor, J.P.; Hair, M.; O’Reilly, D.S.; Deighan, C.J. Comparison of urinary albumin and urinary total protein as predictors of patient outcomes in CKD. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2011, 57, 21–28. [Google Scholar] [CrossRef]
- Smith, E.R.; Cai, M.M.; McMahon, L.P.; Wright, D.A.; Holt, S.G. The value of simultaneous measurements of urinary albumin and total protein in proteinuric patients. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. Eur. Ren. Assoc. 2012, 27, 1534–1541. [Google Scholar] [CrossRef]
- Kim, S.S.; Song, S.H.; Kim, I.J.; Jeon, Y.K.; Kim, B.H.; Kwak, I.S.; Lee, E.K.; Kim, Y.K. Urinary cystatin C and tubular proteinuria predict progression of diabetic nephropathy. Diabetes Care 2013, 36, 656–661. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, S.S.; Kim, I.J.; Lee, M.J.; Jeon, Y.K.; Kim, B.H.; Song, S.H.; Kim, Y.K. Nonalbumin proteinuria is a simple and practical predictor of the progression of early-stage type 2 diabetic nephropathy. J. Diabetes Its Complicat. 2017, 31, 395–399. [Google Scholar] [CrossRef]
- Han, E.; Cho, Y.; Kim, K.W.; Lee, Y.H.; Kang, E.S.; Cha, B.S.; Lee, B.W. Hepatic fibrosis is associated with total proteinuria in Korean patients with type 2 diabetes. Medicine 2020, 99, e21038. [Google Scholar] [CrossRef]
- Lee, B.W.; Lee, Y.H.; Park, C.Y.; Rhee, E.J.; Lee, W.Y.; Kim, N.H.; Choi, K.M.; Park, K.G.; Choi, Y.K.; Cha, B.S.; et al. Non-Alcoholic Fatty Liver Disease in Patients with Type 2 Diabetes Mellitus: A Position Statement of the Fatty Liver Research Group of the Korean Diabetes Association. Diabetes Metab. J. 2020, 44, 382–401. [Google Scholar] [CrossRef] [PubMed]
- Pilz, S.; Rutters, F.; Nijpels, G.; Stehouwer, C.D.; Højlund, K.; Nolan, J.J.; Balkau, B.; Dekker, J.M. Insulin sensitivity and albuminuria: The RISC study. Diabetes Care 2014, 37, 1597–1603. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.S.; Bril, F.; Cusi, K.; Newsome, P.N. Modulation of Insulin Resistance in Nonalcoholic Fatty Liver Disease. Hepatology 2019, 70, 711–724. [Google Scholar] [CrossRef] [PubMed]
- Dekkers, C.C.J.; Petrykiv, S.; Laverman, G.D.; Cherney, D.Z.; Gansevoort, R.T.; Heerspink, H.J.L. Effects of the SGLT-2 inhibitor dapagliflozin on glomerular and tubular injury markers. Diabetes Obes. Metab. 2018, 20, 1988–1993. [Google Scholar] [CrossRef]
- Greco, E.V.; Russo, G.; Giandalia, A.; Viazzi, F.; Pontremoli, R.; De Cosmo, S. GLP-1 Receptor Agonists and Kidney Protection. Medicina 2019, 55, 233. [Google Scholar] [CrossRef] [PubMed]
- Ninčević, V.; Omanović Kolarić, T.; Roguljić, H.; Kizivat, T.; Smolić, M.; Bilić Ćurčić, I. Renal Benefits of SGLT 2 Inhibitors and GLP-1 Receptor Agonists: Evidence Supporting a Paradigm Shift in the Medical Management of Type 2 Diabetes. Int. J. Mol. Sci. 2019, 20, 5831. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Class | Description | Inclusion Criteria |
|---|---|---|
| I | Mild or nonspecific LM changes and EM-proven GBM thickening | Biopsy does not meet any of the criteria mentioned below for class II, III, or IV |
| GBM > 395 nm in female and >430 nm in male individuals 9 years of age and older 1 | ||
| IIa | Mild mesangial expansion | Biopsy does not meet criteria for class III or IV |
| Mild mesangial expansion in >25% of the observed mesangium | ||
| IIb | Severe mesangial expansion | Biopsy does not meet criteria for class III or IV |
| Severe mesangial expansion in >25% of the observed mesangium | ||
| III | Nodular sclerosis (Kimmelstiel–Wilson lesion) | Biopsy does not meet criteria for class IV |
| At least one convincing Kimmelstiel–Wilson lesion | ||
| IV | Advanced diabetic glomerulosclerosis | Global glomerular sclerosis in >50% of glomeruli |
| Lesions from classes I through III |
| Lesion | Criteria | Score |
|---|---|---|
| Interstitial lesions | ||
| IFTA | No IFTA | 0 |
| <25% | 1 | |
| 25% to 50% | 2 | |
| >50% | 3 | |
| Interstitial inflammation | Absent | 0 |
| Infiltration only in relation to IFTA | 1 | |
| Infiltration in areas without IFTA | 2 | |
| Vascular lesions | ||
| Arteriolar hyalinosis | Absent | 0 |
| At least one area of arteriolar hyalinosis | 1 | |
| More than one area of arteriolar hyalinosis | 2 | |
| Presence of large vessels | Yes/No | |
| Arteriosclerosis 1 | No intimal thickening | 0 |
| Intimal thickening less than thickness of media | 1 | |
| Intimal thickening greater than thickness of media | 2 |
| Stage | Albuminuria | eGFR |
|---|---|---|
| I. Hyper-filtration | Possibly increased | Increased |
| II. Silent | Returns to normal | Returns to normal |
| III. Incipient | Increased | Persistent |
| IV. Overt | Progressed | Decreased |
| V. End stage renal disease | Various within morbid range | Progressed |
| Index | Design | Subjects | Characteristics | Variable Correlated with the Index |
|---|---|---|---|---|
| NAPCR [13] | Cross-sectional | 118 | Type 2 DM, eGFR ≥ 60 | UACR, L-FABP, KIM-1, NGAL |
| NAPCR [78] | Longitudinal, observational | 237 | Type 2 DM, eGFR ≥ 30 | Baseline UACR Annual decline of eGFR during median 29 months |
| NAPCR [79] | Longitudinal, observational | 73 | Type 2 DM, eGFR ≥ 60 | Annual decline of eGFR, development of CKD stage 3 or greater during median 50 months |
| NAPCR [14] | Longitudinal, observational | 325 | Type 2 DM, eGFR ≥ 30 | Decline of eGFR, progression of CKD stage during median 4.3 years |
| Isolated NAP [71] | Cross-sectional | 883 | Type 2 DM, Not on RRT | (vs. normal UACR and UPCR) proportion of female, lower BMI, eGFR, glucometabolic parameters, beta cell function, vascular disease (vs. albuminuria group) higher eGFR |
| UPCR [72] | Cross-sectional | 2047 | Type 2 DM, eGFR ≥ 15,UACR<30 | Carotid artery intima-media thickness |
| Isolated NAP [80] | Cross-sectional | 1108 | Type 2 DM, eGFR ≥ 15 | Hepatic fibrosis |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bae, J.; Won, Y.J.; Lee, B.-W. Non-Albumin Proteinuria (NAP) as a Complementary Marker for Diabetic Kidney Disease (DKD). Life 2021, 11, 224. https://doi.org/10.3390/life11030224
Bae J, Won YJ, Lee B-W. Non-Albumin Proteinuria (NAP) as a Complementary Marker for Diabetic Kidney Disease (DKD). Life. 2021; 11(3):224. https://doi.org/10.3390/life11030224
Chicago/Turabian StyleBae, Jaehyun, Young Jun Won, and Byung-Wan Lee. 2021. "Non-Albumin Proteinuria (NAP) as a Complementary Marker for Diabetic Kidney Disease (DKD)" Life 11, no. 3: 224. https://doi.org/10.3390/life11030224
APA StyleBae, J., Won, Y. J., & Lee, B.-W. (2021). Non-Albumin Proteinuria (NAP) as a Complementary Marker for Diabetic Kidney Disease (DKD). Life, 11(3), 224. https://doi.org/10.3390/life11030224