
Body Mass Index Influence for the Personalization of the Monoclonal Antibodies Therapy for Psoriasis


Abstract
:1. Introduction
2. Materials and Methods
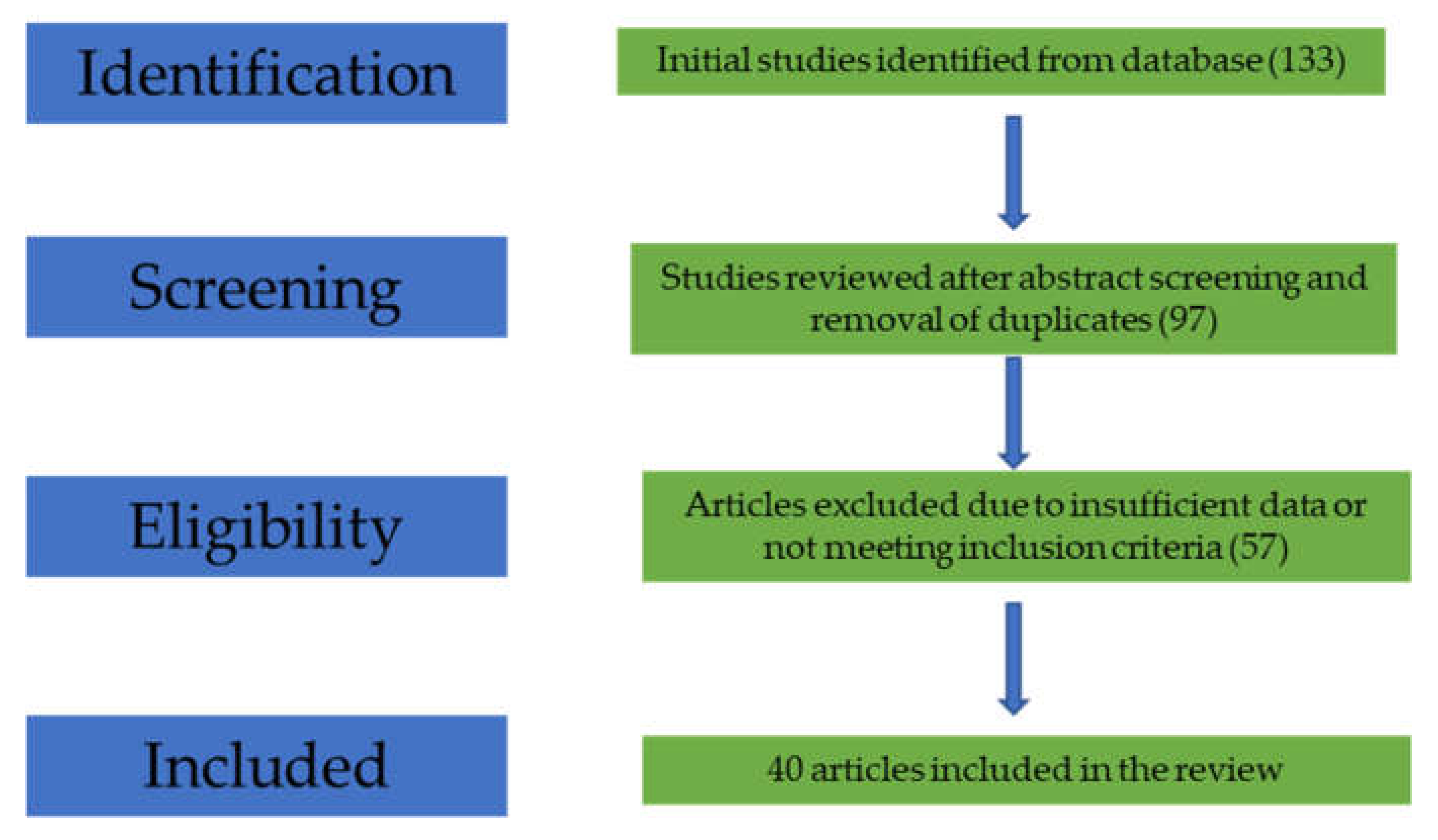
2.1. Selection of Studies
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. End-Points
2.5. Study Characteristics
3. Results
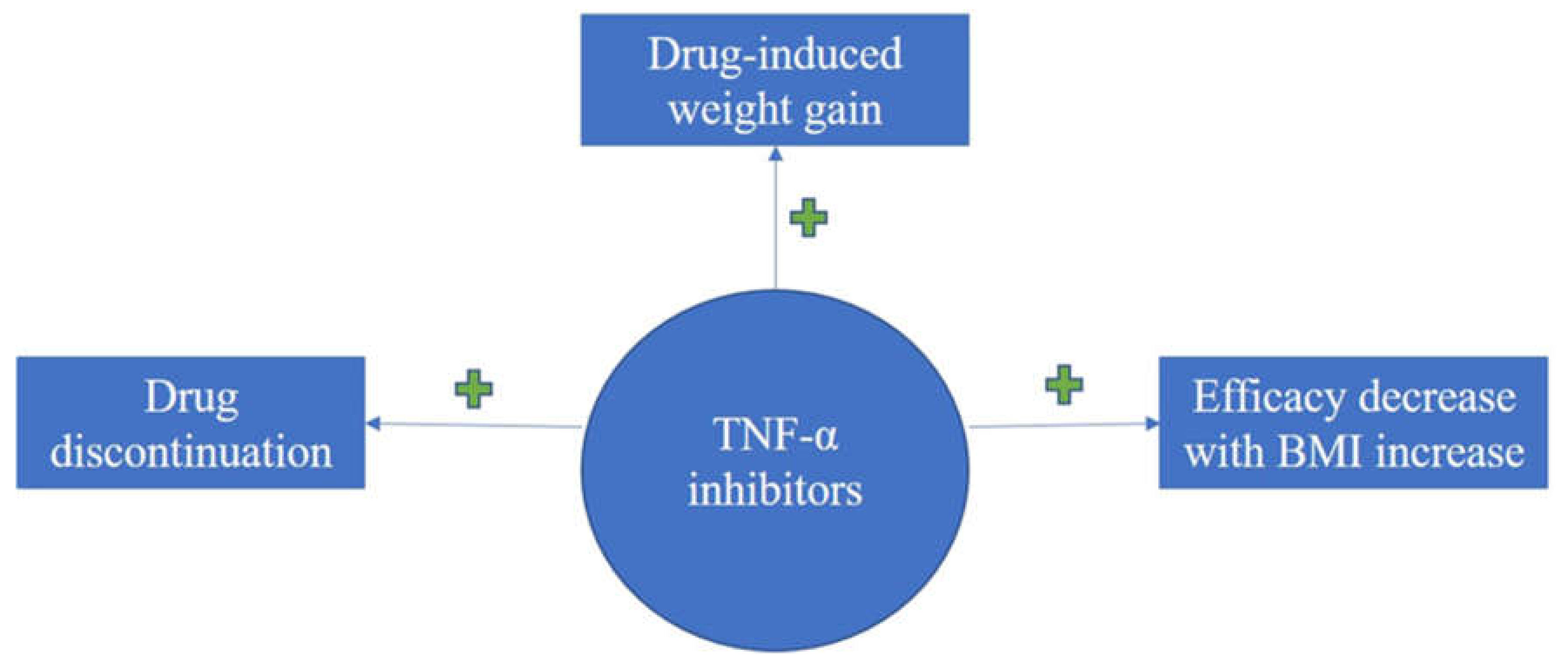
3.1. TNF-α Inhibitors (TNFI) and BMI

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TNFI | Structure and Mechanism | Effect on BMI/Weight Gain | Influence of BMI on Drug Efficacy | Commentary |
|---|---|---|---|---|
| Infliximab | mouse-derived chimeric IgG1; neutralizes both soluble, and membrane-bound TNF-α | Significant, gradual increase [8,10,13,14,15,16,17,18,19,20,21,22,23,24] | Increased BMI promotes drug discontinuation [11,12,26] Failing therapy [12] Steady decrease of PASI-75 with increasing BMI [21] Increased BMI leads to reduced efficacy and delayed response [27] | Weight-dependent dosing shows to increase efficacy [8,10] |
| Etanercept | prototypic recombinant fusion protein; inhibits only soluble TNF-α | Non-uniform [10,19] weight increase [16,17,18,23,24] Non-statistically significant weight increase [10,25] BMI increased more in subjects with normal weight at baseline [19] | Pharmacokinetic interactions due to wider adipose tissue [10,26] Drug discontinuation [11,12,26] BMI increase affects early clinical response [21] | Weight-dependent dosing not implemented to date [28]; should be taken in consideration to counteract pharmacokinetic issues Significant weight gain might call for the use of etanercept only in normal BMI individuals [8] |
| Adalimumab | phage display-derived, fully monoclonal antibody | Significant mass increase [10,18,19] | Pharmacokinetic interactions due to wider adipose tissue [10,26] Highest drug discontinuation [26] Strong diminished drug efficacy with BMI increase [8] No significant relationship between efficacy and body weight [22] | Conflicting studies call for further research to draw definitive conclusions |
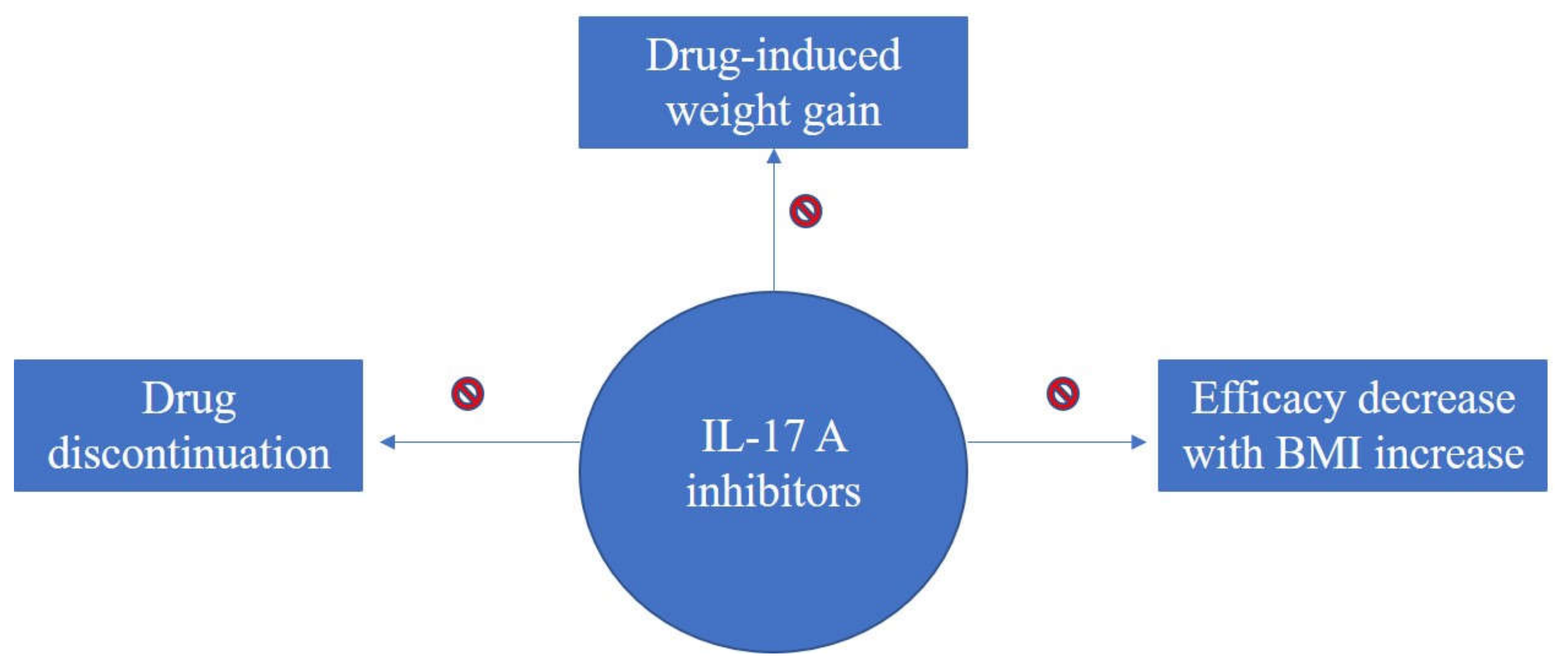
3.2. IL-17A Inhibitors and BMI
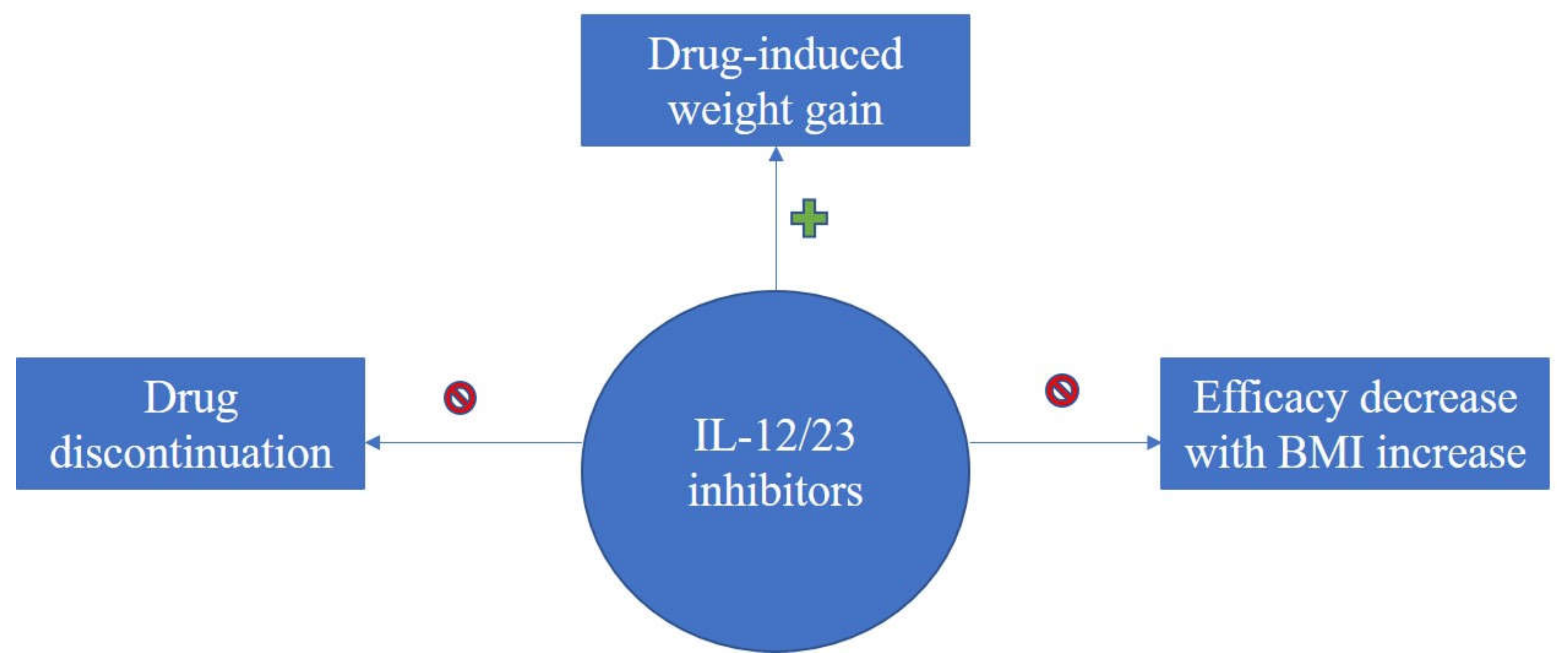
3.3. IL-12/23 Inhibitors and BMI
| IL-17A Inhibitors | Structure and Mechanism | Effect on BMI/Weight Gain | Influence of BMI on Drug Efficacy | Commentary |
|---|---|---|---|---|
| Secukinumab | recombinant fully human IgG1/kappa monoclonal antibody | Constant BMI levels; no weight gain [35,38] | Similar drug efficacy regardless of BMI values [35]; one study revealed that individuals <90kg had higher response rates [48] | Could be a better alternative for obese patients; Lack of sufficient data requires for extensive research to draw definitive conclusions |
| Ixekizumab | complete monoclonal antibody of the subclass IgG4 | No significant weight gain [36,38]; Lack of sufficient data | Similar drug efficacy regardless of BMI values [37] | Could be a better alternative for obese patients; Lack of sufficient data requires for extensive research to draw definitive conclusions |
| IL-12/23 Inhibitors | Structure and Mechanism | Effect on BMI/Weight Gain | Influence of BMI on Drug Efficacy | Commentary |
|---|---|---|---|---|
| Ustekinumab | fully human monoclonal antibody (mAb) that binds specifically to IL-12/IL-23p40 | No reported BMI changes following treatment [40] | Pharmacokinetic interactions affecting serum concentration and drug clearance [41] Reduced PASI response rates (efficacy) with mass increase [42,43,44,45] | Could be a better alternative for obese patients; Doubling the dose in individuals weighing more than 100 kg significantly increased efficacy [45,46,47] |
4. Discussion and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nestle, F.O.; Kaplan, D.H.; Barker, J. Psoriasis. New Engl. J. Med. 2009, 361, 496–509. [Google Scholar] [CrossRef] [PubMed]
- Parisi, R.; Symmons, D.P.; Griffiths, C.E.; Ashcroft, D.M. Global epidemiology of psoriasis: A systematic review of incidence and prevalence. J. Investig. Dermatol. 2013, 133, 377–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogawa, K.; Okada, Y. The current landscape of psoriasis genetics in 2020. J. Dermatol. Sci. 2020, 99, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Lowes, M.A.; Suárez-Fariñas, M.; Krueger, J.G. Immunology of psoriasis. Annu. Rev. Immunol. 2014, 32, 227–255. [Google Scholar] [CrossRef] [Green Version]
- Brownstone, N.D.; Hong, J.; Mosca, M.; Hadeler, E.; Liao, W.; Bhutani, T.; Koo, J. Biologic treatments of psoriasis: An update for the Clinician. Biologics 2021, 15, 39–51. [Google Scholar] [CrossRef]
- Rønholt, K.; Iversen, L. Old and new biological therapies for psoriasis. Int J. Mol. Sci. 2017, 18, 2297. [Google Scholar] [CrossRef] [Green Version]
- Bahner, J.D.; Cao, L.Y.; Korman, N.J. Biologics in the management of psoriasis. Clin. Cosmet. Investig. Dermatol. 2009, 2, 111–128. [Google Scholar]
- Puig, L. Obesity and psoriasis: Body weight and body mass index influence the response to biological treatment. J. Eur. Acad. Dermatol. Venereol. 2011, 25, 1007–1011. [Google Scholar] [CrossRef]
- Tobin, A.M.; Kirby, B. TNF alpha inhibitors in the treatment of psoriasis and psoriatic arthritis. BioDrugs 2005, 19, 47–57. [Google Scholar] [CrossRef]
- Tan, E.; Baker, C.; Foley, P. Weight gain and tumour necrosis factor-alpha inhibitors in patients with psoriasis. Austral. J. Dermatol. 2013, 54, 259–263. [Google Scholar] [CrossRef]
- Højgaard, P.; Glintborg, B.; Kristensen, L.E.; Gudbjornsson, B.; Love, T.J.; Dreyer, L. The influence of obesity on response to tumour necrosis factor-α inhibitors in psoriatic arthritis: Results from the DANBIO and ICEBIO registries. Rheumatology 2016, 55, 2191–2199. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.; Facciorusso, A.; Singh, A.G.; Casteele, N.V.; Zarrinpar, A.; Prokop, L.J.; Grunvald, E.L.; Curtis, J.R.; Sandborn, W.J. Obesity and response to anti-tumor necrosis factor-α agents in patients with select immune-mediated inflammatory diseases: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0195123. [Google Scholar] [CrossRef] [Green Version]
- Patsalos, O.; Dalton, B.; Leppanen, J.; Ibrahim, M.; Himmerich, H. Impact of TNF-α Inhibitors on Body Weight and BMI: A Systematic Review and Meta-Analysis. Front. Pharmacol. 2020, 11, 481. [Google Scholar] [CrossRef] [Green Version]
- Florin, V.; Cottencin, A.C.; Delaporte, E.; Staumont-Sallé, D. Body weight increment in patients treated with infliximab for plaque psoriasis. J. Eur. Acad. Dermatol. Venereol. 2013, 27, e186–e190. [Google Scholar] [CrossRef]
- Mahé, E.; Reguiai, Z.; Barthelemy, H.; Quiles-Tsimaratos, N.; Chaby, G.; Girard, C.; Estève, E.; Maccari, F.; Descamps, V.; Schmutz, J.L.; et al. Evaluation of risk factors for body weight increment in psoriatic patients on infliximab: A multicentre, cross-sectional study. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 151–159. [Google Scholar] [CrossRef]
- Prignano, F.; Ricceri, F.; Pescitelli, L.; Buggiani, G.; Troiano, M.; Zanieri, F.; Rossari, S.; Lotti, T. Comparison of body weight and clinical-parameter changes following the treatment of plaque psoriasis with biological therapies. Curr. Med. Res. Op. 2009, 25, 2311–2316. [Google Scholar] [CrossRef]
- Gisondi, P.; Cotena, C.; Tessari, G.; Girolomoni, G. Anti-tumour necrosis factor-alpha therapy increases body weight in patients with chronic plaque psoriasis: A retrospective cohort study. J. Eur. Acad. Dermatol. Venereol. 2008, 22, 341–344. [Google Scholar]
- Onsun, N.; Akaslan, T.Ç.; Sallahoglu, K.; Gülcan, A.S.; Bulut, H.; Yabacı, A. Effects of TNF inhibitors and an IL12/23 inhibitor on changes in body weight and adipokine levels in psoriasis patients: A 48-week comparative study. J. Derm. Treat. 2021, 1–16. [Google Scholar] [CrossRef]
- Saraceno, R.; Schipani, C.; Mazzotta, A.; Esposito, M.; Di Renzo, L.; De Lorenzo, A.; Chimenti, S. Effect of anti-tumor necrosis factor-alpha therapies on body mass index in patients with psoriasis. Pharm. Res. 2008, 57, 290–295. [Google Scholar] [CrossRef]
- Takamura, S.; Takahashi, A.; Inoue, Y.; Teraki, Y. Effects of tumor necrosis factor-α, interleukin-23 and interleukin-17A inhibitors on bodyweight and body mass index in patients with psoriasis. J. Dermatol. 2018, 45, 1130–1134. [Google Scholar] [CrossRef]
- Naldi, L.; Addis, A.; Chimenti, S.; Giannetti, A.; Picardo, M.; Tomino, C.; Maccarone, M.; Chatenoud, L.; Bertuccio, P.; Caggese, E.; et al. Impact of body mass index and obesity on clinical response to systemic treatment for psoriasis: Evidence from the Psocare Project. Dermatology 2008, 217, 365–373. [Google Scholar] [CrossRef]
- Chiricozzi, A.; Zangrilli, A.; Bavetta, M.; Bianchi, L.; Chimenti, S.; Saraceno, R. Real-life 9-year experience with adalimumab in psoriasis and psoriatic arthritis: Results of a single-centre, retrospective study. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 304–311. [Google Scholar] [CrossRef]
- Esposito, M.; Mazzotta, A.; Saraceno, R.; Schipani, C.; Chimenti, S. Influence and variation of the body mass index in patients treated with etanercept for plaque-type psoriasis. Int J. Immunopat. Pharm. 2009, 22, 219–225. [Google Scholar] [CrossRef]
- Renzo, L.D.; Saraceno, R.; Schipani, C.; Rizzo, M.; Bianchi, A.; Noce, A.; Esposito, M.; Tiberti, S.; Chimenti, S.; De Lorenzo, A. Prospective assessment of body weight and body composition changes in patients with psoriasis receiving anti-TNF-α treatment. Dermatol. Ther. 2011, 24, 446–451. [Google Scholar] [CrossRef] [Green Version]
- Ross, C.; Marshman, G.; Grillo, M.; Stanford, T. Biological therapies for psoriasis: Adherence and outcome analysis from a clinical perspective. Australas. J. Derm. 2016, 57, 137–140. [Google Scholar] [CrossRef]
- Di Lernia, V.; Tasin, L.; Pellicano, R.; Zumiani, G.; Albertini, G. Impact of body mass index on retention rates of anti-TNF-alfa drugs in daily practice for psoriasis. J. Dermatol. Treat. 2012, 23, 404–409. [Google Scholar] [CrossRef] [Green Version]
- Duarte, A.A. Moderate to severe psoriasis treated with infliximab—53 patients: Patients profile, efficacy and adverse effects. Ann. Bras. Dermatol. 2011, 86, 257–263. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, T.U.; Koo, J. Etanercept in the treatment of plaque psoriasis. Clin. Cosmet. Investig. Dermatol. 2009, 19, 77–84. [Google Scholar]
- Reich, K.; Gottlieb, A.B.; Kimball, A.; Li, S. Consistency of infliximab response across subgroups of patients with psoriasis: Integrated results from randomized controlled clinical trials. J. Am. Acad. Dermatol. 2006, 54, 215. [Google Scholar] [CrossRef]
- Von Stebut, E.; Boehncke, W.H.; Ghoreschi, K.; Gori, T.; Kaya, Z.; Thaci, D.; Schäffler, A. IL-17A in psoriasis and beyond: Cardiovascular and metabolic implications. Front. Immunol. 2020, 10, 3096. [Google Scholar] [CrossRef] [Green Version]
- Langley, R.G.; Elewski, B.E.; Lebwohl, M.; Reich, K.; Griffiths, C.E.; Papp, K.A.; Puig, L.; Nakagawa, H.; Spelman, L.; Sigurgeirsson, B.; et al. Secukinumab in plaque psoriasis—Results of two phase 3 trials. New Engl. J. Med. 2014, 371, 326–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, K.B.; Colombel, J.F.; Hardin, D.S. Phase 3 trials of ixekizumab in moderate-to-severe plaque psoriasis. New Engl. J. Med. 2016, 375, 2102. [Google Scholar] [CrossRef] [PubMed]
- Thaçi, D.; Blauvelt, A.; Reich, K.; Tsai, T.-F.; Vanaclocha, F.; Kingo, K.; Ziv, M.; Pinter, A.; Hugot, S.; You, R.; et al. Secukinumab is superior to ustekinumab in clearing skin of subjects with moderate to severe plaque psoriasis: CLEAR, a randomized controlled trial. J. Am. Acad. Dermatol. 2015, 73, 400–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blauvelt, A.; Reich, K.; Tsai, T.F.; Tyring, S.; Vanaclocha, F.; Kingo, K.; Ziv, M.; Pinter, A.; Vender, R.; Hugot, S.; et al. Secukinumab is superior to ustekinumab in clearing skin of subjects with moderate-to-severe plaque psoriasis up to 1 year: Results from the CLEAR study. J. Am. Acad. Dermatol. 2017, 76, 60–69. [Google Scholar] [PubMed]
- Pirro, F.; Caldarola, G.; Chiricozzi, A.; Burlando, M.; Mariani, M.; Parodi, A.; Peris, K.; De Simone, C. Impact of Body Mass Index on the Efficacy of Biological Therapies in Patients with Psoriasis: A Real-World Study. Clin Drug Investig. 2021, 41, 917–925. [Google Scholar] [CrossRef] [PubMed]
- Egeberg, A.; Wu, J.J.; Korman, N.; Solomon, J.A.; Goldblum, O.; Zhao, F.; Mallbris, L. Ixekizumab treatment shows a neutral impact on cardiovascular parameters in patients with moderate-to-severe plaque psoriasis: Results from UNCOVER-1, UNCOVER-2, and UNCOVER-3. J. Am. Acad. Dermatol. 2018, 79, 104–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reich, K.; Puig, L.; Mallbris, L.; Zhang, L.; Osuntokun, O.; Leonardi, C. The effect of bodyweight on the efficacy and safety of ixekizumab: Results from an integrated database of three randomised, controlled Phase 3 studies of patients with moderate-to-severe plaque psoriasis. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 1196–1207. [Google Scholar] [CrossRef] [PubMed]
- Piros, É.A.; Szabó, Á.; Rencz, F.; Brodszky, V.; Wikonkál, N.; Miheller, P.; Horváth, M.; Holló, P. Anti-interleukin-17 therapy of severe psoriatic patients results in an improvement of serum lipid and inflammatory parameters’ levels, but has no effect on body composition parameters. Life 2021, 11, 535. [Google Scholar] [CrossRef]
- Yeilding, N.; Szapary, P.; Brodmerkel, C.; Benson, J.; Plotnick, M.; Zhou, H.; Goyal, K.; Schenkel, B.; Giles-Komar, J.; Mascelli, M.A.; et al. Development of the IL-12/23 antagonist ustekinumab in psoriasis: Past, present, and future perspectives. Ann. N. Y. Acad. Sci. 2011, 1222, 30–39. [Google Scholar] [CrossRef]
- Gisondi, P.; Conti, A.; Galdo, G.; Piaserico, S.; De Simone, C.; Girolomoni, G. Ustekinumab does not increase body mass index in patients with chronic plaque psoriasis: A prospective cohort study. British J. Derm. 2013, 168, 1124–1127. [Google Scholar] [CrossRef]
- Zhu, Y.; Hu, C.; Lu, M.; Liao, S.; Marini, J.C.; Yohrling, J.; Yeilding, N.; Davis, H.M.; Zhou, H. Population pharmacokinetic modeling of ustekinumab, a human monoclonal antibody targeting IL-12 ⁄ 23p40, in patients with moderate to severe plaque psoriasis. J. Clin. Pharmacol. 2009, 49, 162–175. [Google Scholar] [CrossRef]
- Lebwohl, M.; Yeilding, N.; Szapary, P.; Wang, Y.; Li, S.; Zhu, Y.; Reich, K.; Langley, R.G.; Papp, K.A. Impact of weight on the efficacy and safety of ustekinumab in patients with moderate to severe psoriasis: Rationale for dosing recommendations. J. Am. Acad. Dermatol. 2010, 63, 571–579. [Google Scholar] [CrossRef]
- Papp, K.; Kimball, A.; Wasfi, Y.; Chan, D.; Bissonnette, R.; Sofen, H.; Yeilding, N.; Li, S.; Szapary, P.; Gordon, K.B.; et al. Long-term efficacy and safety of ustekinumab in patients with moderate to severe psoriasis through 5 years of follow-up: Results from the PHOENIX 1 long-term extension. J. Dermatol. 2012, 39, 63–64. [Google Scholar]
- Papp, K.; Langley, R.; Lebwohl, M.; Krueger, G.G.; Szapary, P.; Yeilding, N.; Guzzo, C.; Hsu, M.-C.; Wang, Y.; Li, S.; et al. Efficacy and safety of ustekinumab, a human interleukin-12/23 monoclonal antibody, in patients with psoriasis: 52-week results from a randomised, double-blind, placebo-controlled trial (PHOENIX 2). Lancet 2008, 371, 1675–1684. [Google Scholar] [CrossRef]
- Young, M.S.; Horn, E.J.; Cather, J.C. The ACCEPT study: Ustekinumab versus etanercept in moderate-to-severe psoriasis patients. Expert Rev. Clin. Immunol. 2011, 7, 9–13. [Google Scholar] [CrossRef]
- Zweegers, J.; van den Reek, J.; van de Kerkhof, P.; Otero, M.E.; Kuijpers, A.L.A.; Koetsier, M.I.A.; Arnold, W.P.; Berends, M.A.M.; Weppner-Parren, L.; Ossenkoppele, P.M.; et al. Body mass index predicts discontinuation due to ineffectiveness and female sex predicts discontinuation due to side effects in patients with psoriasis treated with adalimumab, etanercept or ustekinumab in daily practice: A prospective, comparative, long-term drug-survival study from the BioCAPTURE registry. Br. J. Dermatol. 2016, 175, 340–347. [Google Scholar]
- Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/stelara-epar-product-information_en.pdf (accessed on 1 September 2021).
- Lee, J.E.; Wang, J.; Florian, J.; Wang, Y.-M.; Kettl, D.; Marcus, K.; Woitach, A. Effect of body weight on risk-benefit and dosing regimen recommendation of secukinumab for the treatment of moderate to severe plaque psoriasis. Clin. Pharmacol. Ther. 2019, 106, 78–80. [Google Scholar] [CrossRef]
- Di Minno, M.N.; Peluso, R.; Iervolino, S.; Russolillo, A.; Lupoli, R.; Scarpa, R.; CaRRDs Study Group. Weight loss and achievement of minimal disease activity in patients with psoriatic arthritis starting treatment with tumour necrosis factor α blockers. Ann. Rheum. Dis. 2014, 73, 1157–1162. [Google Scholar] [CrossRef] [Green Version]
- Pona, A.; Haidari, W.; Kolli, S.S.; Feldman, S.R. Diet and psoriasis. Dermatol. Online J. 2019, 25, 1. [Google Scholar] [CrossRef]
- Murray, M.; Bergstresser, P.; Adams-Huet, B.; Cohen, J.B. Relationship of psoriasis severity to obesity using same-gender siblings as controls for obesity. Clin. Exp. Dermatol. 2009, 34, 140–144. [Google Scholar] [CrossRef]
- Gisondi, P.; Del Giglio, M.; Di Francesco, V.; Zamboni, M.; Girolomoni, G. Weight loss improves the response of obese patients with moderate-tosevere chronic plaque psoriasis to low-dose cyclosporine therapy: A randomized, controlled, investigator-blinded clinical trial. Am. J. Clin. Nutr. 2008, 88, 1242–1247. [Google Scholar]
- Edson-Heredia, E.; Sterling, K.; Alatorre, C.; Carter, G.C.; Paczkowski, R.; Zarotsky, V.; Maeda-Chubachi, T. Heterogeneity of response to biologic treatment: Perspective for psoriasis. J. Investig. Dermatol. 2014, 134, 18–23. [Google Scholar] [CrossRef] [Green Version]
- Al-Mutairi, N.; Nour, T. The effect of weight reduction on treatment outcomes in obese patients with psoriasis on biologic therapy: A randomized controlled prospective trial. Exp. Opin. Biol. Ther. 2014, 14, 749–756. [Google Scholar] [CrossRef]
- Bach, E.; Nielsen, R.R.; Vendelbo, M.H.; Møller, A.B.; Jessen, N.; Buhl, M.; Hafstrom, T.K.; Holm, L.; Pedersen, S.B.; Pilegaard, H.; et al. Direct effects of TNF-α on local fuel metabolism and cytokine levels in the placebo-controlled, bilaterally infused human leg: Increased insulin sensitivity, increased net protein breakdown, and increased IL-6 release. Diabetes 2013, 62, 4023–4029. [Google Scholar] [CrossRef] [Green Version]
- Patel, H.J.; Patel, B.M. TNF-α and cancer cachexia: Molecular insights and clinical implications. Life Sci. 2017, 170, 56–63. [Google Scholar] [CrossRef]
- Tzanavari, T.; Giannogonas, P.; Karalis, K.P. TNF-alpha and obesity. Curr. Dir. Autoimmun. 2010, 11, 145–156. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anghel, F.; Nitusca, D.; Cristodor, P. Body Mass Index Influence for the Personalization of the Monoclonal Antibodies Therapy for Psoriasis. Life 2021, 11, 1316. https://doi.org/10.3390/life11121316
Anghel F, Nitusca D, Cristodor P. Body Mass Index Influence for the Personalization of the Monoclonal Antibodies Therapy for Psoriasis. Life. 2021; 11(12):1316. https://doi.org/10.3390/life11121316
Chicago/Turabian StyleAnghel, Flavia, Diana Nitusca, and Patricia Cristodor. 2021. "Body Mass Index Influence for the Personalization of the Monoclonal Antibodies Therapy for Psoriasis" Life 11, no. 12: 1316. https://doi.org/10.3390/life11121316
APA StyleAnghel, F., Nitusca, D., & Cristodor, P. (2021). Body Mass Index Influence for the Personalization of the Monoclonal Antibodies Therapy for Psoriasis. Life, 11(12), 1316. https://doi.org/10.3390/life11121316