
Treatment-Related Adverse Events with PD-1 or PD-L1 Inhibitors: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Outcomes
2.5. Risk of Bias Assessment
2.6. Data Synthesis and Analysis
3. Results
3.1. Results of the Search
3.2. Quality Assessment
3.3. Results of Treatment-Related Adverse Event
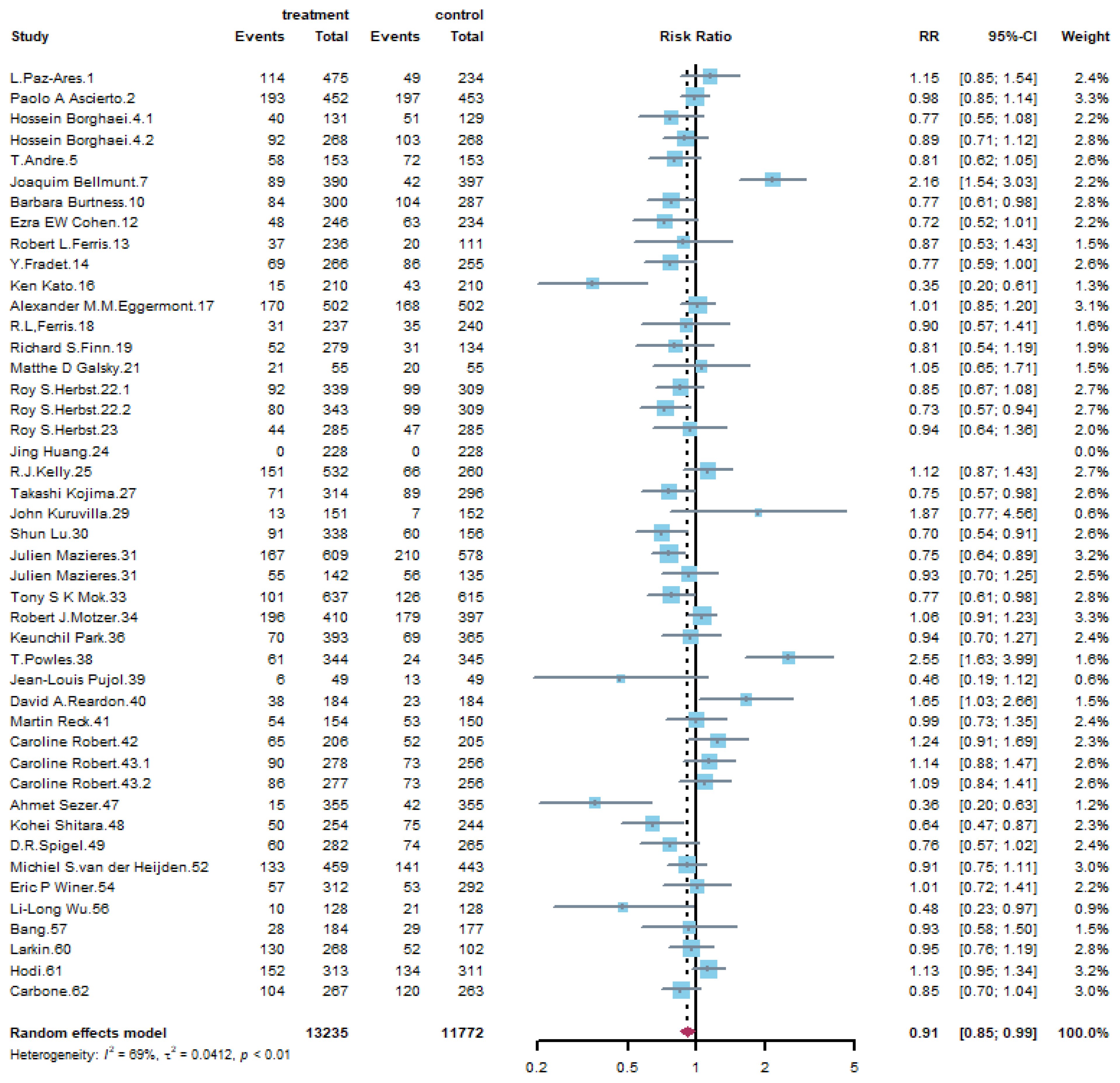
3.3.1. All Grade Adverse Events
3.3.2. Grade 3 or Higher Adverse Event
3.4. Results of Subgroup Analysis
3.4.1. Subgroup Analysis by Immune Checkpoint Inhibitors
3.4.2. Subgroup Analysis by Treatment Frequency
3.4.3. Subgroup Analysis by Control Group
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jiang, Y.; Chen, M.; Nie, H.; Yuan, Y. PD-1 and PD-L1 in cancer immunotherapy: Clinical implications and future considerations. Hum. Vaccin. Immunother. 2019, 15, 1111–1122. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.; Pelosof, L.; Lemery, S.; Gong, Y.; Goldberg, K.B.; Farrell, A.T.; Keegan, P.; Veeraraghavan, J.; Wei, G.; Blumenthal, G.M.; et al. Systematic Review of PD-1/PD-L1 Inhibitors in Oncology: From Personalized Medicine to Public Health. Oncologist 2021, 26, e1786–e1799. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Liu, D.; Li, L. PD-1/PD-L1 pathway: Current researches in cancer. Am. J. Cancer Res. 2020, 10, 727–742. [Google Scholar]
- Almutairi, A.R.; Alkhatib, N.; Martin, J.; Babiker, H.M.; Garland, L.L.; McBride, A.; Abraham, I. Comparative efficacy and safety of immunotherapies targeting the PD-1/PD-L1 pathway for previously treated advanced non-small cell lung cancer: A Bayesian network meta-analysis. Crit. Rev. Oncol. Hematol. 2019, 142, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Tartarone, A.; Roviello, G.; Lerose, R.; Roudi, R.; Aieta, M.; Zoppoli, P. Anti-PD-1 versus anti-PD-L1 therapy in patients with pretreated advanced non-small-cell lung cancer: A meta-analysis. Future Oncol. 2019, 15, 2423–2433. [Google Scholar] [CrossRef]
- Wan, N.; Ji, B.; Li, J.; Jiang, J.; Yang, C.; Zhang, T.; Huang, W. A pooled meta-analysis of PD-1/L1 inhibitors incorporation therapy for advanced non-small cell lung cancer. Onco Targets Ther. 2019, 12, 4955–4973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Facchinetti, F.; Di Maio, M.; Tiseo, M. Adding PD-1/PD-L1 Inhibitors to Chemotherapy for the First-Line Treatment of Extensive Stage Small Cell Lung Cancer (SCLC): A Meta-Analysis of Randomized Trials. Cancers (Basel) 2020, 12, 2645. [Google Scholar] [CrossRef]
- Wang, B.C.; Zhang, Z.J.; Fu, C.; Wang, C. Efficacy and safety of anti-PD-1/PD-L1 agents vs chemotherapy in patients with gastric or gastroesophageal junction cancer: A systematic review and meta-analysis. Medicine 2019, 98, e18054. [Google Scholar] [CrossRef]
- Buonerba, C.; Dolce, P.; Iaccarino, S.; Scafuri, L.; Verde, A.; Costabile, F.; Pagliuca, M.; Morra, R.; Riccio, V.; Ribera, D.; et al. Outcomes Associated with First-Line anti-PD-1/PD-L1 agents vs. Sunitinib in Patients with Sarcomatoid Renal Cell Carcinoma: A Systematic Review and Meta-Analysis. Cancers 2020, 12, 408. [Google Scholar] [CrossRef] [Green Version]
- da Silva, L.L.; Aguiar, P.N., Jr.; Park, R.; Edelman Saul, E.; Haaland, B.; de Lima Lopes, G. Comparative Efficacy and Safety of Programmed Death-1 Pathway Inhibitors in Advanced Gastroesophageal Cancers: A Systematic Review and Network Meta-Analysis of Phase III Clinical Trials. Cancers 2021, 13, 2614. [Google Scholar] [CrossRef]
- Ramos-Casals, M.; Brahmer, J.R.; Callahan, M.K.; Flores-Chávez, A.; Keegan, N.; Khamashta, M.A.; Lambotte, O.; Mariette, X.; Prat, A.; Suárez-Almazor, M.E. Immune-related adverse events of checkpoint inhibitors. Nat. Rev. Dis. Primers 2020, 6, 38. [Google Scholar] [CrossRef]
- Wang, Y.; Zhou, S.; Yang, F.; Qi, X.; Wang, X.; Guan, X.; Shen, C.; Duma, N.; Vera Aguilera, J.; Chintakuntlawar, A.; et al. Treatment-Related Adverse Events of PD-1 and PD-L1 Inhibitors in Clinical Trials: A Systematic Review and Meta-analysis. JAMA Oncol. 2019, 5, 1008–1019. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, R.; Imbimbo, M.; Malouf, R.; Paget-Bailly, S.; Calais, F.; Marchal, C.; Westeel, V. Single or combined immune checkpoint inhibitors compared to first-line platinum-based chemotherapy with or without bevacizumab for people with advanced non-small cell lung cancer. Cochrane Database Syst. Rev. 2021, 4, Cd013257. [Google Scholar] [CrossRef]
- Baxi, S.; Yang, A.; Gennarelli, R.L.; Khan, N.; Wang, Z.; Boyce, L.; Korenstein, D. Immune-related adverse events for anti-PD-1 and anti-PD-L1 drugs: Systematic review and meta-analysis. Br. Med J. 2018, 360, k793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duan, J.; Cui, L.; Zhao, X.; Bai, H.; Cai, S.; Wang, G.; Zhao, Z.; Zhao, J.; Chen, S.; Song, J.; et al. Use of Immunotherapy With Programmed Cell Death 1 vs Programmed Cell Death Ligand 1 Inhibitors in Patients With Cancer: A Systematic Review and Meta-analysis. JAMA Oncol. 2020, 6, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Naidoo, J.; Page, D.B.; Li, B.T.; Connell, L.C.; Schindler, K.; Lacouture, M.E.; Postow, M.A.; Wolchok, J.D. Toxicities of the anti-PD-1 and anti-PD-L1 immune checkpoint antibodies. Ann. Oncol. 2015, 26, 2375–2391. [Google Scholar] [CrossRef]
- Herbst, R.S.; Garon, E.B.; Kim, D.W.; Cho, B.C.; Perez-Gracia, J.L.; Han, J.Y.; Arvis, C.D.; Majem, M.; Forster, M.D.; Monnet, I.; et al. Long-Term Outcomes and Retreatment Among Patients With Previously Treated, Programmed Death-Ligand 1‒Positive, Advanced Non‒Small-Cell Lung Cancer in the KEYNOTE-010 Study. J. Clin. Oncol. 2020, 38, 1580–1590. [Google Scholar] [CrossRef]
- Robert, C.; Ribas, A.; Schachter, J.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.M.; Lotem, M.; et al. Pembrolizumab versus ipilimumab in advanced melanoma (KEYNOTE-006): Post-hoc 5-year results from an open-label, multicentre, randomised, controlled, phase 3 study. Lancet Oncol. 2019, 20, 1239–1251. [Google Scholar] [CrossRef]
- Carbone, D.P.; Reck, M.; Paz-Ares, L.; Creelan, B.; Horn, L.; Steins, M.; Felip, E.; van den Heuvel, M.M.; Ciuleanu, T.E.; Badin, F.; et al. First-Line Nivolumab in Stage IV or Recurrent Non-Small-Cell Lung Cancer. N Engl. J. Med. 2017, 376, 2415–2426. [Google Scholar] [CrossRef]
- Bang, Y.J.; Ruiz, E.Y.; Van Cutsem, E.; Lee, K.W.; Wyrwicz, L.; Schenker, M.; Alsina, M.; Ryu, M.H.; Chung, H.C.; Evesque, L.; et al. Phase III, randomised trial of avelumab versus physician’s choice of chemotherapy as third-line treatment of patients with advanced gastric or gastro-oesophageal junction cancer: Primary analysis of JAVELIN Gastric 300. Ann. Oncol. 2018, 29, 2052–2060. [Google Scholar] [CrossRef]
- Larkin, J.; Minor, D.; D’Angelo, S.; Neyns, B.; Smylie, M.; Jr, W.H.M.; Gutzmer, R.; Linette, G.; Chmielowski, B.; Lao, C.D.; et al. Overall Survival in Patients With Advanced Melanoma Who Received Nivolumab Versus Investigator’s Choice Chemotherapy in CheckMate 037 A Randomized, Controlled, Open-Label Phase III Trial. J. Clin. Oncol. 2018, 36, 383. [Google Scholar] [CrossRef]
- Hodi, F.S.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Nivolumab plus ipilimumab or nivolumab alone versus ipilimumab alone in advanced melanoma (CheckMate 067): 4-year outcomes of a multicentre, randomised, phase 3 trial. Lancet Oncol. 2018, 19, 1480–1492. [Google Scholar] [CrossRef]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulières, D.; Tahara, M.; de Castro, G.; Psyrri, A.; Basté, N.; Neupane, P.; Bratland, Å.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef]
- Cohen, E.E.W.; Soulières, D.; Le Tourneau, C.; Dinis, J.; Licitra, L.; Ahn, M.J.; Soria, A.; Machiels, J.P.; Mach, N.; Mehra, R.; et al. Pembrolizumab versus methotrexate, docetaxel, or cetuximab for recurrent or metastatic head-and-neck squamous cell carcinoma (KEYNOTE-040): A randomised, open-label, phase 3 study. Lancet 2019, 393, 156–167. [Google Scholar] [CrossRef]
- Ferris, R.L.; Licitra, L.; Fayette, J.; Even, C.; Blumenschein, G.; Harrington, K.J.; Guigay, J.; Vokes, E.E.; Saba, N.F.; Haddad, R.; et al. Nivolumab in Patients with Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck: Efficacy and Safety in CheckMate 141 by Prior Cetuximab Use. Clin. Cancer Res. 2019, 25, 5221–5230. [Google Scholar] [CrossRef] [Green Version]
- Fradet, Y.; Bellmunt, J.; Vaughn, D.J.; Lee, J.L.; Fong, L.; Vogelzang, N.J.; Climent, M.A.; Petrylak, D.P.; Choueiri, T.K.; Necchi, A.; et al. Randomized phase III KEYNOTE-045 trial of pembrolizumab versus paclitaxel, docetaxel, or vinflunine in recurrent advanced urothelial cancer: Results of >2 years of follow-up. Ann. Oncol. 2019, 30, 970–976. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Cho, B.C.; Takahashi, M.; Okada, M.; Lin, C.Y.; Chin, K.; Kadowaki, S.; Ahn, M.J.; Hamamoto, Y.; Doki, Y.; et al. Nivolumab versus chemotherapy in patients with advanced oesophageal squamous cell carcinoma refractory or intolerant to previous chemotherapy (ATTRACTION-3): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 1506–1517. [Google Scholar] [CrossRef]
- Finn, R.S.; Ryoo, B.Y.; Merle, P.; Kudo, M.; Bouattour, M.; Lim, H.Y.; Breder, V.; Edeline, J.; Chao, Y.; Ogasawara, S.; et al. Pembrolizumab As Second-Line Therapy in Patients With Advanced Hepatocellular Carcinoma in KEYNOTE-240: A Randomized, Double-Blind, Phase III Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2020, 38, 193–202. [Google Scholar] [CrossRef]
- Mok, T.S.K.; Wu, Y.L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- Pujol, J.L.; Greillier, L.; Audigier-Valette, C.; Moro-Sibilot, D.; Uwer, L.; Hureaux, J.; Guisier, F.; Carmier, D.; Madelaine, J.; Otto, J.; et al. A Randomized Non-Comparative Phase II Study of Anti-Programmed Cell Death-Ligand 1 Atezolizumab or Chemotherapy as Second-Line Therapy in Patients With Small Cell Lung Cancer: Results From the IFCT-1603 Trial. J. Thorac. Oncol. 2019, 14, 903–913. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csoszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Updated analysis of KEYNOTE-024: Pembrolizumab versus platinum-based chemotherapy for advanced non–small-cell lung cancer with PD-L1 tumor proportion score of 50% or greater. J. Clin. Oncol. 2019, 37, 537–546. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Spira, A.; Raben, D.; Planchard, D.; Cho, B.C.; Özgüroğlu, M.; Daniel, D.; Villegas, A.; Vicente, D.; Hui, R.; et al. Outcomes with durvalumab by tumour PD-L1 expression in unresectable, stage III non-small-cell lung cancer in the PACIFIC trial. Ann. Oncol. 2020, 31, 798–806. [Google Scholar] [CrossRef] [PubMed]
- Ascierto, P.A.; Del Vecchio, M.; Mandalá, M.; Gogas, H.; Arance, A.M.; Dalle, S.; Cowey, C.L.; Schenker, M.; Grob, J.J.; Chiarion-Sileni, V.; et al. Adjuvant nivolumab versus ipilimumab in resected stage IIIB-C and stage IV melanoma (CheckMate 238): 4-year results from a multicentre, double-blind, randomised, controlled, phase 3 trial. Lancet Oncol. 2020, 21, 1465–1477. [Google Scholar] [CrossRef]
- Borghaei, H.; Gettinger, S.; Vokes, E.E.; Chow, L.Q.M.; Burgio, M.A.; de Castro Carpeno, J.; Pluzanski, A.; Arrietac, O.; Frontera, O.A.; Chiari, R.; et al. Five-year outcomes from the randomized, phase iii trials checkmate 017 and 057: Nivolumab versus docetaxel in previously treated non-small-cell lung cancer. J. Clin. Oncol. 2021, 39, 723–733. [Google Scholar] [CrossRef] [PubMed]
- André, T.; Shiu, K.K.; Kim, T.W.; Jensen, B.V.; Jensen, L.H.; Punt, C.; Smith, D.; Garcia-Carbonero, R.; Benavides, M.; Gibbs, P.; et al. Pembrolizumab in Microsatellite-Instability-High Advanced Colorectal Cancer. N. Engl. J. Med. 2020, 383, 2207–2218. [Google Scholar] [CrossRef]
- Eggermont, A.M.M.; Kicinski, M.; Blank, C.U.; Mandala, M.; Long, G.V.; Atkinson, V.; Dalle, S.; Haydon, A.; Khattak, A.; Carlino, M.S.; et al. Association Between Immune-Related Adverse Events and Recurrence-Free Survival Among Patients With Stage III Melanoma Randomized to Receive Pembrolizumab or Placebo: A Secondary Analysis of a Randomized Clinical Trial. JAMA Oncol. 2020, 6, 519–527. [Google Scholar] [CrossRef] [Green Version]
- Ferris, R.L.; Haddad, R.; Even, C.; Tahara, M.; Dvorkin, M.; Ciuleanu, T.E.; Clement, P.M.; Mesia, R.; Kutukova, S.; Zholudeva, L.; et al. Durvalumab with or without tremelimumab in patients with recurrent or metastatic head and neck squamous cell carcinoma: EAGLE, a randomized, open-label phase III study. Ann. Oncol. 2020, 31, 942–950. [Google Scholar] [CrossRef]
- Galsky, M.D.; Mortazavi, A.; Milowsky, M.I.; George, S.; Gupta, S.; Fleming, M.T.; Dang, L.H.; Geynisman, D.M.; Walling, R.; Alter, R.S.; et al. Randomized Double-Blind Phase II Study of Maintenance Pembrolizumab Versus Placebo after First-Line Chemotherapy in Patients with Metastatic Urothelial Cancer. J. Clin. Oncol. 2020, 38, 1797–1806. [Google Scholar] [CrossRef]
- Herbst, R.S.; Giaccone, G.; de Marinis, F.; Reinmuth, N.; Vergnenegre, A.; Barrios, C.H.; Morise, M.; Felip, E.; Andric, Z.; Geater, S.; et al. Atezolizumab for first-line treatment of PD-L1–selected patients with NSCLC. N. Engl. J. Med. 2020, 383, 1328–1339. [Google Scholar] [CrossRef]
- Huang, J.; Xu, J.; Chen, Y.; Zhuang, W.; Zhang, Y.; Chen, Z.; Chen, J.; Zhang, H.; Niu, Z.; Fan, Q.; et al. Camrelizumab versus investigator’s choice of chemotherapy as second-line therapy for advanced or metastatic oesophageal squamous cell carcinoma (ESCORT): A multicentre, randomised, open-label, phase 3 study. Lancet Oncol. 2020, 21, 832–842. [Google Scholar] [CrossRef]
- Kojima, T.; Shah, M.A.; Muro, K.; Francois, E.; Adenis, A.; Hsu, C.H.; Doi, T.; Moriwaki, T.; Kim, S.B.; Lee, S.H.; et al. Randomized Phase III KEYNOTE-181 Study of Pembrolizumab Versus Chemotherapy in Advanced Esophageal Cancer. J. Clin. Oncol. 2020, 38, 4138–4148. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.; Wang, J.; Cheng, Y.; Mok, T.; Chang, J.; Zhang, L.; Feng, J.; Tu, H.Y.; Wu, L.; Zhang, Y.; et al. Nivolumab versus docetaxel in a predominantly Chinese patient population with previously treated advanced non-small cell lung cancer: 2-year follow-up from a randomized, open-label, phase 3 study (CheckMate 078). Lung Cancer 2021, 152, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Mazieres, J.; Rittmeyer, A.; Gadgeel, S.; Hida, T.; Gandara, D.R.; Cortinovis, D.L.; Barlesi, F.; Yu, W.; Matheny, C.; Ballinger, M.; et al. Atezolizumab Versus Docetaxel in Pretreated Patients With NSCLC: Final Results From the Randomized Phase 2 POPLAR and Phase 3 OAK Clinical Trials. J. Thorac. Oncol. 2021, 16, 140–150. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Escudier, B.; George, S.; Hammers, H.J.; Srinivas, S.; Tykodi, S.S.; Sosman, J.A.; Plimack, E.R.; Procopio, G.; McDermott, D.F.; et al. Nivolumab versus everolimus in patients with advanced renal cell carcinoma: Updated results with long-term follow-up of the randomized, open-label, phase 3 CheckMate 025 trial. Cancer 2020, 126, 4156–4167. [Google Scholar] [CrossRef]
- Powles, T.; Park, S.H.; Voog, E.; Caserta, C.; Valderrama, B.P.; Gurney, H.; Kalofonos, H.; Radulović, S.; Demey, W.; Ullén, A.; et al. Avelumab maintenance therapy for advanced or metastatic urothelial carcinoma. N. Engl. J. Med. 2020, 383, 1218–1230. [Google Scholar] [CrossRef]
- Reardon, D.A.; Brandes, A.A.; Omuro, A.; Mulholland, P.; Lim, M.; Wick, A.; Baehring, J.; Ahluwalia, M.S.; Roth, P.; Bähr, O.; et al. Effect of Nivolumab vs Bevacizumab in Patients with Recurrent Glioblastoma: The CheckMate 143 Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1003–1010. [Google Scholar] [CrossRef]
- Robert, C.; Long, G.V.; Brady, B.; Dutriaux, C.; Di Giacomo, A.M.; Mortier, L.; Rutkowski, P.; Hassel, J.C.; McNeil, C.M.; Kalinka, E.A.; et al. Five-year outcomes with nivolumab in patients with wild-type BRAF advanced melanoma. J. Clin. Oncol. 2020, 38, 3937–3946. [Google Scholar] [CrossRef]
- Shitara, K.; Van Cutsem, E.; Bang, Y.J.; Fuchs, C.; Wyrwicz, L.; Lee, K.W.; Kudaba, I.; Garrido, M.; Chung, H.C.; Lee, J.; et al. Efficacy and Safety of Pembrolizumab or Pembrolizumab plus Chemotherapy vs Chemotherapy Alone for Patients with First-line, Advanced Gastric Cancer: The KEYNOTE-062 Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1571–1580. [Google Scholar] [CrossRef]
- Wu, Y.L.; Zhang, L.; Fan, Y.; Zhou, J.; Zhang, L.; Zhou, Q.; Li, W.; Hu, C.; Chen, G.; Zhang, X.; et al. Randomized clinical trial of pembrolizumab vs chemotherapy for previously untreated Chinese patients with PD-L1-positive locally advanced or metastatic non–small-cell lung cancer: KEYNOTE-042 China Study. Int. J. Cancer 2020. [Google Scholar] [CrossRef]
- Bellmunt, J.; Hussain, M.; Gschwend, J.E.; Albers, P.; Oudard, S.; Castellano, D.; Daneshmand, S.; Nishiyama, H.; Majchrowicz, M.; Degaonkar, V.; et al. Adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma (IMvigor010): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2021, 22, 525–537. [Google Scholar] [CrossRef]
- Kelly, R.J.; Ajani, J.A.; Kuzdzal, J.; Zander, T.; van Cutsem, E.; Piessen, G.; Mendez, G.; Feliciano, J.; Motoyama, S.; Lièvre, A.; et al. Adjuvant nivolumab in resected esophageal or gastroesophageal junction cancer. N. Engl. J. Med. 2021, 384, 1191–1203. [Google Scholar] [CrossRef]
- Kuruvilla, J.; Ramchandren, R.; Santoro, A.; Paszkiewicz-Kozik, E.; Gasiorowski, R.; Johnson, N.A.; Fogliatto, L.M.; Goncalves, I.; de Oliveira, J.S.R.; Buccheri, V.; et al. Pembrolizumab versus brentuximab vedotin in relapsed or refractory classical Hodgkin lymphoma (KEYNOTE-204): An interim analysis of a multicentre, randomised, open-label, phase 3 study. Lancet Oncol. 2021, 22, 512–524. [Google Scholar] [CrossRef]
- Park, K.; Özgüroğlu, M.; Vansteenkiste, J.; Spigel, D.; Yang, J.C.H.; Ishii, H.; Garassino, M.; de Marinis, F.; Szczesna, A.; Polychronis, A.; et al. Avelumab Versus Docetaxel in Patients With Platinum-Treated Advanced NSCLC: 2-Year Follow-Up From the JAVELIN Lung 200 Phase 3 Trial. J. Thorac. Oncol. 2021. [Google Scholar] [CrossRef]
- Sezer, A.; Kilickap, S.; Gümüş, M.; Bondarenko, I.; Özgüroğlu, M.; Gogishvili, M.; Turk, H.M.; Cicin, I.; Bentsion, D.; Gladkov, O.; et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: A multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet 2021, 397, 592–604. [Google Scholar] [CrossRef]
- Spigel, D.R.; Vicente, D.; Ciuleanu, T.E.; Gettinger, S.; Peters, S.; Horn, L.; Audigier-Valette, C.; Pardo Aranda, N.; Juan-Vidal, O.; Cheng, Y.; et al. Second-line nivolumab in relapsed small-cell lung cancer: CheckMate 331☆. Ann. Oncol. 2021, 32, 631–641. [Google Scholar] [CrossRef]
- van der Heijden, M.S.; Loriot, Y.; Durán, I.; Ravaud, A.; Retz, M.; Vogelzang, N.J.; Nelson, B.; Wang, J.; Shen, X.; Powles, T. Atezolizumab Versus Chemotherapy in Patients with Platinum-treated Locally Advanced or Metastatic Urothelial Carcinoma: A Long-term Overall Survival and Safety Update from the Phase 3 IMvigor211 Clinical Trial. Eur. Urol. 2021, 8, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Winer, E.P.; Lipatov, O.; Im, S.A.; Goncalves, A.; Muñoz-Couselo, E.; Lee, K.S.; Schmid, P.; Tamura, K.; Testa, L.; Witzel, I.; et al. Pembrolizumab versus investigator-choice chemotherapy for metastatic triple-negative breast cancer (KEYNOTE-119): A randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 499–511. [Google Scholar] [CrossRef]
- Nishijima, T.F.; Shachar, S.S.; Nyrop, K.A.; Muss, H.B. Safety and Tolerability of PD-1/PD-L1 Inhibitors Compared with Chemotherapy in Patients with Advanced Cancer: A Meta-Analysis. Oncologist 2017, 22, 470–479. [Google Scholar] [CrossRef] [Green Version]
- De Velasco, G.; Je, Y.; Bosse, D.; Awad, M.M.; Ott, P.A.; Moreira, R.B.; Schutz, F.; Bellmunt, J.; Sonpavde, G.P.; Hodi, F.S.; et al. Comprehensive Meta-analysis of Key Immune-Related Adverse Events from CTLA-4 and PD-1/PD-L1 Inhibitors in Cancer Patients. Cancer Immunol. Res. 2017, 5, 312–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.; Liang, H.; Wang, W.; Zhao, S.; Cai, X.; Zhao, Y.; Li, C.; Cheng, B.; Xiong, S.; Li, J.; et al. Immune-related adverse events of a PD-L1 inhibitor plus chemotherapy versus a PD-L1 inhibitor alone in first-line treatment for advanced non-small cell lung cancer: A meta-analysis of randomized control trials. Cancer 2021, 127, 777–786. [Google Scholar] [CrossRef]
- Kleiner, D.E.; Berman, D. Pathologic changes in ipilimumab-related hepatitis in patients with metastatic melanoma. Dig. Dis. Sci. 2012, 57, 2233–2240. [Google Scholar] [CrossRef] [Green Version]
- Sonpavde, G.P.; Grivas, P.; Lin, Y.; Hennessy, D.; Hunt, J.D. Immune-related adverse events with PD-1 versus PD-L1 inhibitors: A meta-analysis of 8730 patients from clinical trials. Future Oncol. 2021, 17, 2545–2558. [Google Scholar] [CrossRef]
- Rizvi, N.A.; Mazieres, J.; Planchard, D.; Stinchcombe, T.E.; Dy, G.K.; Antonia, S.J.; Horn, L.; Lena, H.; Minenza, E.; Mennecier, B.; et al. Activity and safety of nivolumab, an anti-PD-1 immune checkpoint inhibitor, for patients with advanced, refractory squamous non-small-cell lung cancer (CheckMate 063): A phase 2, single-arm trial. Lancet Oncol. 2015, 16, 257–265. [Google Scholar] [CrossRef] [Green Version]
- Zimmer, L.; Goldinger, S.M.; Hofmann, L.; Loquai, C.; Ugurel, S.; Thomas, I.; Schmidgen, M.I.; Gutzmer, R.; Utikal, J.S.; Goppner, D.; et al. Neurological, respiratory, musculoskeletal, cardiac and ocular side-effects of anti-PD-1 therapy. Eur. J. Cancer 2016, 60, 210–225. [Google Scholar] [CrossRef] [PubMed]
- Varga, A.; Piha-Paul, S.; Ott, P.A.; Mehnert, J.M.; Berton-Rigaud, D.; Morosky, A.; Yang, P.; Ruman, J.; Matei, D. Pembrolizumab in patients with programmed death ligand 1-positive advanced ovarian cancer: Analysis of KEYNOTE-028. Gynecol. Oncol. 2019, 152, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Chiu, N.; Chiu, L.; Chow, R.; Lam, H.; Verma, S.; Pasetka, M.; Chow, E.; DeAngelis, C. Taxane-induced arthralgia and myalgia: A literature review. J. Oncol. Pharm. Pract. 2017, 23, 56–67. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Author | Year | Disease | Clinical Trial | Phase | Drug | Dose | Frequency | N | Data Source (1 = clinical trials website, 2=Article) | Median Follow-Up |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Carbone et al. [19] | 2017 | nonsmall cell lung cancer | CheckMate-026 | III | nivolumab3 | 3 mg/kg | q2w | 267 | 1 | 13.5 |
| 2 | Bang et al. [20] | 2018 | gastric or gastro-esophageal junction cancer | JAVELIN gastric 300 | III | avelumabmab | 10 mg/kg | q2w | 184 | 1 | 10.6 |
| 3 | Larkin et al. [21] | 2018 | melanoma | CheckMate-037 | III | nivolumab | 3 mg/kg | q2w | 268 | 1 | 24 |
| 4 | Hodi et al. [22] | 2018 | melanoma | CheckMate-067 | III | nivolumab | 3 mg/kg | q2w | 313 | 1 | 46.9 |
| 5 | Barbara Burtness et al. [23] | 2019 | head and neck squamous cell carcinoma | KeyNote-048 | III | pembrolizumab | 200 mg | q3w | 300 | 1 | 11.5 |
| 6 | Ezra EW. Cohen et al. [24] | 2019 | head and neck squamous cell carcinoma | KeyNote-040 | III | pembrolizumab | 200 mg | q3w | 246 | 1 | 7.5 |
| 7 | Robert L. Ferris et al. [25] | 2019 | head and neck squamous cell carcinoma | CheckMate-141 | III | nivolumab | 3 mg/kg | q2w | 236 | 2 | 24 |
| 8 | Y. Fradet et al. [26] | 2019 | urothelial carcinoma | KeyNote-045 | III | pembrolizumab | 200 mg | q3w | 266 | 1 | 27.7 |
| 9 | Ken Kato et al. [27] | 2019 | esophageal squamous cell carcinoma | ATTRACTION-3 | III | nivolumab | 240 mg | q2w | 210 | 2 | 8 |
| 10 | Richard S. Finn et al. [28] | 2019 | hepatocellular | KeyNote-240 | III | pembrolizumab | 200 mg | q3w | 279 | 1 | 13.8 |
| 11 | Tony S K Mok et al. [29] | 2019 | nonsmall cell lung cancer | KeyNote-042 | III | pembrolizumab | 200 mg | q3w | 637 | 1 | 12.8 |
| 12 | Jean-Louis Pujol et al. [30] | 2019 | small cell lung cancer | IFCT-1603 | II | atezolizumab | 1200 mg | q3w | 49 | 2 | 13.7 |
| 13 | Martin Reck et al. [31] | 2019 | nonsmall cell lung cancer | KeyNote-024 | III | pembrolizumab | 200 mg | q3w | 154 | 1 | 25.2 |
| 14 | Caroline Robert et al. [18] | 2019 | melanoma | KeyNote-006 | III | pembrolizumab | 10 mg/kg | q2w | 278 | 1 | 57.7 |
| 15 | Caroline Robert et al. [18] | 2019 | melanoma | KeyNote-006 | III | pembrolizumab | 10 mg/kg | q3w | 277 | 1 | 57.7 |
| 16 | L. Paz-Ares et al. [32] | 2020 | nonsmall cell lung cancer | PACIFIC | III | durvalumab | 10 mg/kg | q2w | 475 | 1 | 33.3 |
| 17 | Paolo A Ascierto et al. [33] | 2020 | melanoma | CheckMate-238 | III | nivolumab | 3 mg/kg | q2w | 452 | 1 | 51.1 |
| 18 | Hossein Borghaei et al. [34] | 2020 | nonsmall cell lung cancer | CheckMate-017 | III | nivolumab | 3 mg/kg | q3w | 131 | 1 | 69.4 |
| 19 | Hossein Borghaei et al. [34] | 2020 | nonsmall cell lung cancer | CheckMate-057 | III | nivolumab | 3 mg/kg | q3w | 268 | 1 | 69.5 |
| 20 | Thierry. Andre et al. [35] | 2020 | colorectal cancer | KeyNote-177 | III | pembrolizumab | 200 mg | q3w | 153 | 2 | 32.4 |
| 21 | Alexander M.M. Eggermont et al. [36] | 2020 | melanoma | KeyNote-054 | III | pembrolizumab | 200 mg | q3w | 502 | 1 | 15 |
| 22 | R.L. Ferris et al. [37] | 2020 | head and neck squamous cell carcinoma | EAGLE | III | durvalumab | 10 mg/kg | q2w | 237 | 1 | 7.6 |
| 23 | Matthe D Galsky et al. [38] | 2020 | urothelial carcinoma | HCRN GU14-182 | II | pembrolizumab | 200 mg | q3w | 55 | 2 | 12.9 |
| 24 | Roy S. Herbst et al. [17] | 2020 | nonsmall cell lung cancer | KeyNote-010 | III | pembrolizumab | 2 mg/kg | q3w | 339 | 1 | 31 |
| 25 | Roy S. Herbst et al. [17] | 2020 | nonsmall cell lung cancer | KeyNote-010 | III | pembrolizumab | 10 mg/kg | q3w | 343 | 1 | 31 |
| 26 | Roy S. Herbst et al. [39] | 2020 | nonsmall cell lung cancer | IMpower110 | III | atezolizumab | 1200 mg | q3w | 285 | 1 | 42.6 |
| 27 | Jing Huang et al. [40] | 2020 | esophageal squamous cell carcinoma | ESCORT | III | camrelizumab | 200 mg | q2w | 228 | 2 | 8.3 |
| 28 | Takashi Kojima et al. [41] | 2020 | esophageal cancer | KeyNote-181 | III | pembrolizumab | 200 mg | q3w | 314 | 1 | 7.1 |
| 29 | Shun Lu et al. [42] | 2020 | nonsmall cell lung cancer | CheckMate-078 | III | nivolumab | 3 mg/kg | q2w | 338 | 1 | 25.9 |
| 30 | Julien Mazieres et al. [43] | 2020 | nonsmall cell lung cancer | OAK | III | atezolizumab | 1200 mg | q3w | 609 | 1 | 47.7 |
| 31 | Julien Mazieres et al. [43] | 2020 | nonsmall cell lung cancer | POPLAR | II | atezolizumab | 1200 mg | q3w | 142 | 1 | 48.6 |
| 32 | Robert J.Motzer et al. [44] | 2020 | renal cell carcinoma | CheckMate-025 | III | nivolumab | 3 mg/kg | q2w | 410 | 1 | 72 |
| 33 | T.Powles et al. [45] | 2020 | urothelial carcinoma | JAVELIN Bladder 100 | III | avelumab | 10 mg/kg | q2w | 344 | 1 | 19 |
| 34 | David A.Reardon et al. [46] | 2020 | glioblastoma | CheckMate-143 | III | nivolumab | 3 mg/kg | q2w | 184 | 2 | 9.4 |
| 35 | Caroline Robert et al. [47] | 2020 | melanoma | CheckMate-066 | III | nivolumab | 3 mg/kg | q2w | 206 | 1 | 32 |
| 36 | Kohei Shitara et al. [48] | 2020 | gastric cancer | KeyNote-062 | III | pembrolizumab | 200 mg | q3w | 254 | 1 | 29.4 |
| 37 | Li-Long Wu et al. [49] | 2020 | nonsmall cell lung cancer | KeyNote-042 China Study | III | pembrolizumab | 200 mg | q3w | 128 | 1 | 12.8 |
| 38 | Joaquim Bellmunt et al. [50] | 2021 | urothelial carcinoma | IMvigor010 | III | atezolizumab | 1200 mg | q3w | 390 | 1 | 21.9 |
| 39 | R.J.Kelly et al. [51] | 2021 | esophageal or gastroesophageal junction cancer | CheckMate-577 | III | nivolumab | 240 mg | q2w | 532 | 1 | 24.4 |
| 40 | John Kuruvilla et al. [52] | 2021 | Hodgkin’s lymphoma | KeyNote-204 | III | pembrolizumab | 200 mg | q3w | 151 | 2 | 25.7 |
| 41 | Keunchil Park et al. [53] | 2021 | nonsmall cell lung cancer | JAVELIN Lung 200 | III | avelumab | 10 mg/kg | q2w | 393 | 1 | 35.4 |
| 42 | Ahmet Sezer et al. [54] | 2021 | nonsmall cell lung cancer | EMPOWER Lung 1 | III | cemiplimab | 350 mg | q3w | 355 | 2 | 10.8 |
| 43 | D.R.Spigel et al. [55] | 2021 | small cell lung cancer | CheckMate-131 | III | nivolumab | 240 mg | q2w | 282 | 1 | 7 |
| 44 | Michiel S.van der Heijden et al. [56] | 2021 | urothelial carcinoma | IMvigor211 | III | atezolizumab | 1200 mg | q3w | 459 | 1 | 17.8 |
| 45 | Eric P Winer et al. [57] | 2021 | triple negative breast cancer | KeyNote-119 | III | pembrolizumab | 200 mg | q3w | 312 | 1 | 31.4 |
| Adverse Events | No. of Trials | RR | 95% CI | Test of Heterogeneity | |
|---|---|---|---|---|---|
| p | I2% | ||||
| General disorders | |||||
| Fatigue | 43 | 0.91 | 0.85–0.99 | <0.01 | 69 |
| Fever | 39 | 1.12 | 0.97–1.29 | <0. 01 | 72 |
| headache | 37 | 1.17 | 1.04–1.32 | <0. 01 | 45 |
| Peripheral neuropathy | 32 | 0.23 | 0.16–0.33 | <0.01 | 60 |
| Skin disorders | |||||
| Pruritus | 40 | 2.34 | 1.85–2.96 | <0.01 | 87 |
| Rash | 42 | 1.53 | 1.25–1.87 | <0.01 | 84 |
| Respiratory disorders | |||||
| Cough | 39 | 1.33 | 1.21–1.48 | <0.01 | 61 |
| Dyspnea | 39 | 1.23 | 1.12–1.35 | <0.01 | 42 |
| Chest pain | 35 | 1.26 | 1.07–1.47 | <0.01 | 61 |
| pneumonia | 40 | 0.96 | 0.79–1.18 | <0.01 | 48 |
| Gastrointestinal disorders | |||||
| Loss of appetite | 39 | 0.90 | 0.78–1.04 | <0.01 | 82 |
| nausea | 45 | 0.67 | 0.57–0.79 | <0.01 | 90 |
| vomiting | 41 | 0.79 | 0.68–0.92 | <0.01 | 78 |
| diarrhea | 45 | 0.86 | 0.74–0.99 | <0.01 | 87 |
| constipation | 41 | 0.91 | 0.81–1.01 | <0.01 | 70 |
| Abdominal pain | 32 | 0.95 | 0.86–1.05 | 0.30 | 10 |
| Liver disorders | |||||
| ALT elevation | 34 | 1.58 | 1.26–1.99 | <0.01 | 70 |
| AST elevation | 28 | 1.56 | 1.22–2.00 | <0. 01 | 71 |
| Hepatitis | 26 | 3.54 | 1.96–6.38 | 1.00 | 0 |
| Endocrine disorders | |||||
| hypothyroid | 37 | 5.29 | 4.00–6.99 | <0.01 | 59 |
| Musculoskeletal disorders | |||||
| myalgia | 29 | 1.00 | 0.75–1.32 | <0.01 | 81 |
| arthralgia | 39 | 1.27 | 1.10–1.47 | <0.01 | 66 |
| Blood disorders | |||||
| anemia | 43 | 0.58 | 0.49–0.68 | <0.01 | 87 |
| Neutrophil decrease | 32 | 0.08 | 0.07–0.10 | 0.39 | 5 |
| Disease | No. of Trials | RR | 95% CI | Test of Heterogeneity | ||
|---|---|---|---|---|---|---|
| Q | p | I2% | ||||
| General disorders | ||||||
| fatigue | 37 | 0.78 | 0.54–1.13 | 27.04 | 0.86 | 0 |
| fever | 40 | 1.19 | 0.91–1.56 | 36.34 | 0.59 | 0 |
| Respiratory disorders | ||||||
| dyspnea | 35 | 1.55 | 1.13–2.12 | 28.60 | 0.73 | 0 |
| pneumonia | 39 | 0.94 | 0.81–1.09 | 41.13 | 0.34 | 8 |
| Gastrointestinal disorders | ||||||
| nausea | 34 | 0.60 | 0.39–0.91 | 23.53 | 0.89 | 0 |
| vomiting | 37 | 0.56 | 0.38–0.83 | 30.88 | 0.71 | 0 |
| diarrhea | 42 | 0.57 | 0.44–0.74 | 62.04 | 0.02 | 34 |
| constipation | 30 | 0.66 | 0.41–1.07 | 25.61 | 0.65 | 0 |
| abdominal pain | 36 | 0.75 | 0.53–1.05 | 18.74 | 0.99 | 0 |
| Liver disorders | ||||||
| ALT elevation | 25 | 1.63 | 0.96–2.77 | 15.28 | 0.91 | 0 |
| hepatitis | 26 | 3.45 | 1.91–6.23 | 4.31 | 1.00 | 0 |
| Kidney disorders | ||||||
| kidney injury | 31 | 1.14 | 0.79–1.62 | 24.94 | 0.73 | 0 |
| Blood disorders | ||||||
| anemia | 40 | 0.50 | 0.35–0.71 | 67.26 | 0.003 | 42 |
| neutrophil decrease | 22 | 0.09 | 0.06–0.16 | 12.56 | 0.92 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; La, B.; Liang, B.; Gu, Y. Treatment-Related Adverse Events with PD-1 or PD-L1 Inhibitors: A Systematic Review and Meta-Analysis. Life 2021, 11, 1277. https://doi.org/10.3390/life11111277
Zhang Y, La B, Liang B, Gu Y. Treatment-Related Adverse Events with PD-1 or PD-L1 Inhibitors: A Systematic Review and Meta-Analysis. Life. 2021; 11(11):1277. https://doi.org/10.3390/life11111277
Chicago/Turabian StyleZhang, Yixi, Bin La, Baosheng Liang, and Yangchun Gu. 2021. "Treatment-Related Adverse Events with PD-1 or PD-L1 Inhibitors: A Systematic Review and Meta-Analysis" Life 11, no. 11: 1277. https://doi.org/10.3390/life11111277
APA StyleZhang, Y., La, B., Liang, B., & Gu, Y. (2021). Treatment-Related Adverse Events with PD-1 or PD-L1 Inhibitors: A Systematic Review and Meta-Analysis. Life, 11(11), 1277. https://doi.org/10.3390/life11111277