
Obesity, Lifestyle Behaviors, and Dietary Habits of Saudi Adolescents Living in Riyadh (ATLS-2 Project): Revisited after a Ten-Year Period


Abstract
:1. Introduction
2. Research Objectives
- Examine the prevalence of overweight, obesity, or abdominal obesity among Saudi adolescents in the current research project and compare such prevalence with the data collected ten years ago.
- Assess the prevalence of physical inactivity, sedentary behaviors, insufficient sleep duration, breakfast skipping, and healthy/unhealthy dietary habits among Saudi adolescents relative to the prevalence rates collected during the 2009/2010 study.
- Investigate the associations and the interactions of general obesity and abdominal obesity in Saudi adolescents with physical inactivity, sedentary behaviors, sleep duration, and dietary habits.
- Inspect the role of sociodemographic variables on obesity, lifestyle behaviors, and the dietary habits of Saudi adolescents.
- Assess the trends over the last ten-year period in being overweight/obese, physical activity, sedentary time, sleep duration, and the dietary habits of Saudi adolescents.
3. Methods and Procedures
3.1. Inclusion/Exclusion Criteria
3.2. Ethical Considerations
3.3. Sample Size and Sampling Technique
3.4. Measurements
3.4.1. Demographics and Socioeconomic Status (SES)
3.4.2. Anthropometric Measurements
3.4.3. Physical Activity
3.4.4. Sedentary Behaviors
3.4.5. Sleep Duration
3.4.6. Dietary Habits
3.4.7. Training Research Assistants
3.4.8. Research Timeline
3.5. Data and Statistical Analyses
4. Preliminary Results
4.1. Demographics and SES
4.2. Anthropometric Measurements
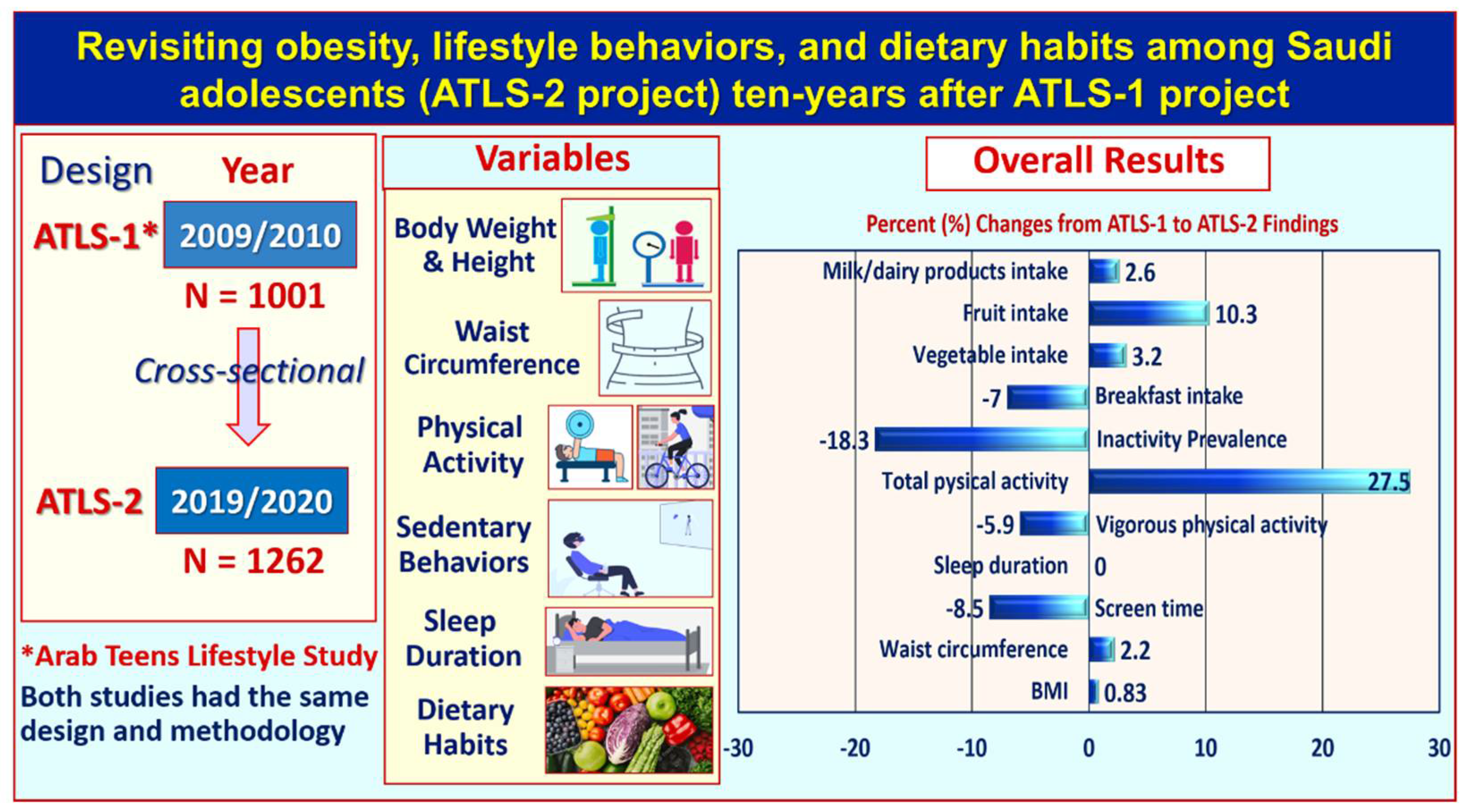
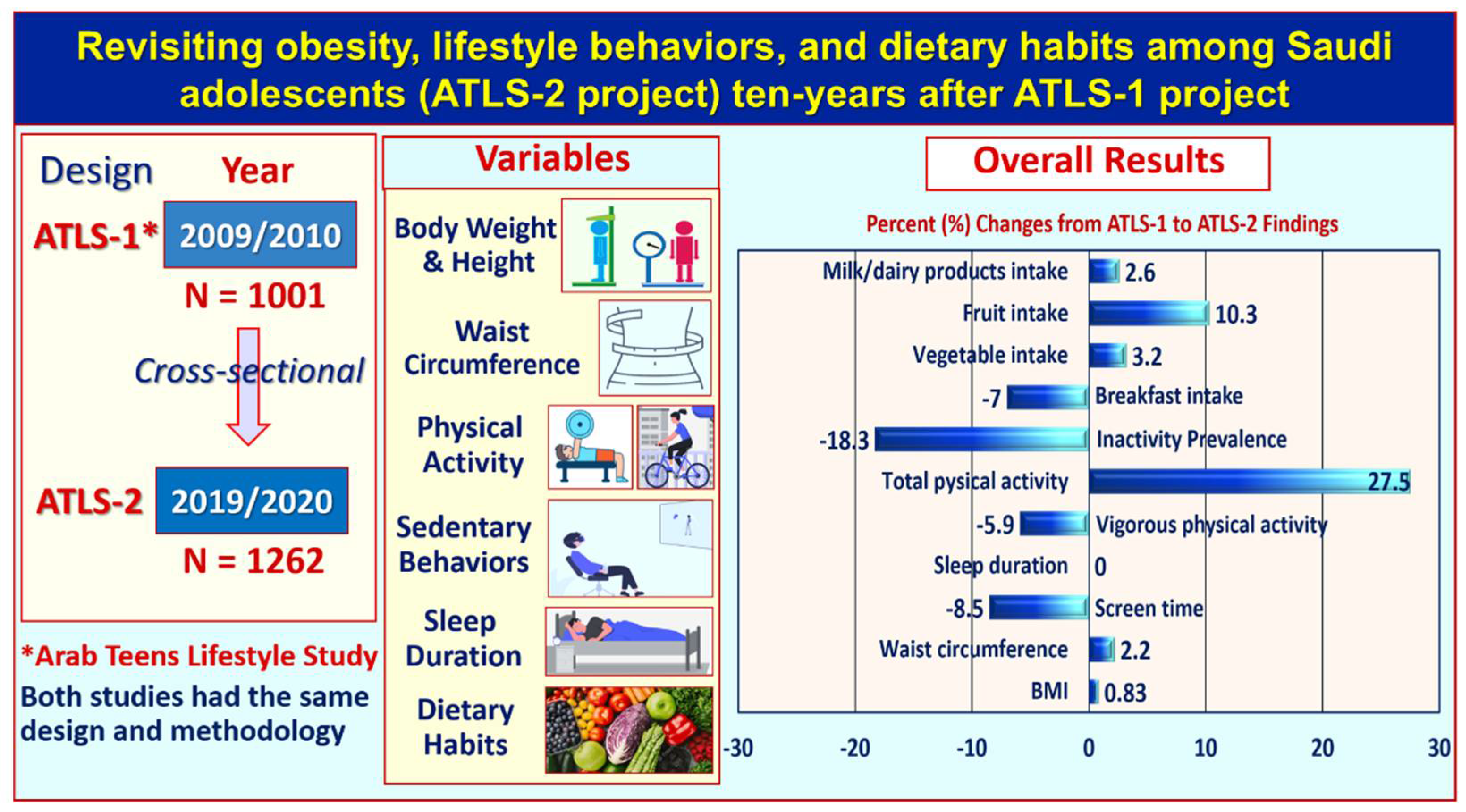
4.3. Proportional Changes between 2009/2010 and 2019/2020 Data
5. Discussion
- What is the prevalence of obesity and abdominal obesity among Saudi adolescents? Have these numbers decreased or increased compared to similar measurements collected ten years ago?
- What is the prevalence of physical inactivity and sedentary time among Saudi adolescents, and how has this changed in the past ten years?
- What is the prevalence of insufficient sleep duration among Saudi adolescents, and how has this decreased or increased compared to data collected in the year 2009/2010?
- What is the prevalence of breakfast skipping among Saudi adolescents, and how has this decreased or increased compared to the prevalence in the year 2009/2010?
- What is the prevalence of vegetable, fruit, and milk/dairy-product intake among Saudi adolescents, and has this decreased or increased since the first study?
- What is the prevalence of unhealthy dietary habits, such as consumption of fast food, French fries, or sugar-sweetened drinks among Saudi adolescents, and has the prevalence of this consumption decreased or increased since the year 2009/2010?
- What is the correlation between the physical inactivity and sedentary time findings obtained by the ATLS questionnaires and the data obtained by accelerometers?
- What are the major lifestyle behaviors or dietary habits that may be influencing obesity, abdominal obesity, or breakfast skipping among Saudi adolescents?
- Are there any gender differences relative to obesity, lifestyle behaviors, or eating habits among Saudi adolescents?
- What are the associations between overweight and obesity status and breakfast intake and other behaviors among Saudi adolescents?
- What are the relationships between demographics and SES with lifestyle behaviors or eating habits among Saudi adolescents?
- Finally, is there a clustering of health-related behaviors among Saudi adolescents? A clustering of unhealthy lifestyle habits such as unhealthy dietary practice, inactivity, and sedentary behaviors may be a major public-health concern.
Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Global Action Plan for the Prevention and Control of NCDs 2013–2020. Available online: http://www.who.int/nmh/publications/ncd-action-plan/en/ (accessed on 28 July 2021).
- World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; For the Lancet Physical Activity Series Working Group. Effect of physical inactivity on the world’s major non-communicable diseases. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Katzmarzyk, P.T.; Church, T.S.; Craig, C.L.; Bouchard, C. Sitting time and mortality from all causes, cardiovascular disease, and cancer. Med. Sci. Sports Exerc. 2009, 41, 998–1005. [Google Scholar] [CrossRef]
- World Health Organization. World Health Organization Guidelines on Physical Activity and Sedentary Behavior; World Health Organization: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/bitstream/handle/10665/336656/9789240015128-eng.pdf?sequence=1&isAllowed=y (accessed on 11 March 2021).
- Ley, S.H.; Ardisson Korat, A.V.; Sun, Q.; Tobias, D.K.; Zhang, C.; Qi, L.; Willett, W.C.; Manson, J.E.; Hu, F.B. Contribution of the Nurses’ Health Studies to Uncovering Risk Factors for Type 2 Diabetes: Diet, Lifestyle, Biomarkers, and Genetics. Am. J. Public Health 2016, 106, 1624–1630. [Google Scholar] [CrossRef]
- Grøntved, A.; Pan, A.; Mekary, R.A.; Stampfer, M.; Willett, C.; Manson, J.E.; Hu, F.B. Muscle-strengthening and conditioning activities and risk of type 2 diabetes: A prospective study in two cohorts of US women. PLoS Med. 2014, 11, e1001587. [Google Scholar] [CrossRef]
- Kallio, P.; Pahkala, K.; Heinonen, O.J.; Tammelin, T.; Hirvensalo, M.; Telama, R.; Juonala, M.; Magnussen, C.G.; Rovio, S.; Helajärvi, H.; et al. Physical inactivity from youth to adulthood and risk of impaired glucose metabolism. Med. Sci. Sports Exerc. 2018, 15. [Google Scholar] [CrossRef]
- Al-Hazzaa, H. The public health burden of physical inactivity in Saudi Arabia. J. Community Fam. Med. 2004, 11, 45–51. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3410089/ (accessed on 15 July 2021).
- Al-Hazzaa, H.M.; Abahussain, N.; Al-Sobayel, H.; Qahwaji, D.; Musaiger, A.O. Physical activity, sedentary behaviors and dietary habits among Saudi adolescents relative to age, gender and region. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Hazzaa, H.M. Physical inactivity in Saudi Arabia revisited: A systematic review of inactivity prevalence and perceived barriers to active living. Int. J. Health Sci. 2018, 12, 50–64. [Google Scholar]
- Moradi-Lakeh, M.; El Bcheraoui, C.; Tuffaha, M.; Daoud, F.; Al Saeedi, M.; Basulaiman, M.; Memish, Z.A.; Al Mazroa, M.A.; Al Rabeeah, A.A.; Mokdad, A. The health of Saudi youths: Current challenges and future opportunities. BMC Fam. Pract. 2016, 17, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahim, H.F.; Sibai, A.; Khader, Y.; Hwalla, N.; Fadhil, I.; Alsiyabi, H.; Mataria, A.; Mendis, S.; Mokdad, P.A.H.; Husseini, A. Non-communicable diseases in the Arab world. Lancet 2014, 383, 356–367. [Google Scholar] [CrossRef]
- Almahmeed, W.; Arnaout, M.S.; Chettaoui, R.; Ibrahim, M.; Kurdi, M.I.; Taher, M.A.; Mancia, G. Coronary artery disease in Africa and the Middle East. Ther. Clin. Risk Manag. 2012, 8, 65–72. [Google Scholar] [CrossRef] [Green Version]
- Musaiger, A.O.; Al-Hazzaa, H.M. Prevalence and risk factors associated with nutrition related non-communicable diseases in the Eastern Mediterranean Region. Int. J. Gen. Med. 2012, 5, 199–217. [Google Scholar] [CrossRef] [Green Version]
- Al-Rubeaan, K.; Al-Manaa, H.A.; Khoja, T.A.; Ahmad, N.A.; Al-Sharqawi, A.H.; Siddiqui, K.; Alnaqeb, D.; Aburisheh, K.H.; Youssef, A.M.; Al-Batel, M.; et al. Epidemiology of abnormal glucose metabolism in a country facing its epidemic: SAUDI-DM study. J. Diabetes 2015, 7, 622–632. [Google Scholar] [CrossRef]
- Hamilton, M.T.; Hamilton, D.G.; Zderic, T.W. Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular disease. Diabetes 2007, 56, 2655–2667. [Google Scholar] [CrossRef] [Green Version]
- Katzmarzyk, P.T.; Powell, K.E.; Jakicic, J.M.; Troiano, R.P.; Piercy, K.; Tennant, B.; The 2018 Physical Activity Guidelines Advisory Committee. Sedentary Behavior and Health: Update from the 2018 Physical Activity Guidelines Advisory Committee. Med. Sci. Sports Exerc. 2019, 51, 1227–1241. [Google Scholar] [CrossRef] [PubMed]
- Mann, K.D.; Howe, L.D.; Basterfield, L.; Parkinson, K.N.; Pearce, M.S.; Reilly, J.K.; Adamson, A.J.; Reilly, J.J.; Janssen, X. Longitudinal study of the associations between change in sedentary behavior and change in adiposity during childhood and adolescence: Gateshead Millennium Study. Int. J. Obes. 2017, 41, 1042–1047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaabane, S.; Chaabna, K.; Abraham, A.; Mamtani, R.; Cheema, S. Physical activity and sedentary behaviour in the Middle East and North Africa: An overview of systematic reviews and meta-analysis. Sci. Rep. 2020, 10, 9363. [Google Scholar] [CrossRef] [PubMed]
- Lobstein, T.; Baur, L.; Uauy, R.; IASO International Obesity Task Force. Obesity in children and young people: A crisis in public health. Obes. Rev. 2004, 5 (Suppl. 1), 4–104. [Google Scholar] [CrossRef]
- Al-Hazzaa, H.M. Prevalence and trends in obesity among school boys in Central Saudi Arabia between 1988 and 2005. Saudi Med. J. 2007, 28, 1569–1574. [Google Scholar]
- Al-Hazzaa, H.M.; Abahussain, N.; Al-Sobayel, H.; Qahwaji, D.; Musaiger, A.O. Prevalence of overweight, obesity and abdominal obesity among urban Saudi adolescents: Gender and regional variations. J. Health Popul. Nutr. 2014, 32, 634–645. [Google Scholar]
- Barlow, S.E. Expert Committee: Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity. Summary report. Pediatrics 2007, 120 (Suppl. 4), S164–S192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Hazzaa, H.M.; Abahussain, N.; Al-Sobayel, H.; Qahwaji, D.; Musaiger, A.O. Lifestyle factors associated with overweight and obesity among Saudi adolescents. BMC Public Health 2012, 12, 354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Hazzaa, H.M.; Al-Sobayel, H.; Abahussain, N.; Qahwaji, D.; Al-Haifi, A.; Desoki, T.; Kerkadi, A. Daily breakfast consumption is favorably associated with obesity measures and health behaviors among adolescents living in eight major cities in the GCC countries. Obes. Rev. 2014, 15 (Suppl. 2), 139. [Google Scholar]
- Al-Hazzaa, H.M.; Al-Resheedi, A.A.; Alsulaimani, R.; Jabri, L. Anthropometric, familial- and lifestyle-related characteristics of school children skipping breakfast in Jeddah, Saudi Arabia. Nutrients 2020, 12, 3668. [Google Scholar] [CrossRef] [PubMed]
- Al-Hazzaa, H.M.; Musaiger, A.O.; Abahussain, N.; Al-Sobayel, H.; Qahwaji, D. Prevalence of short sleep duration and its association with obesity among Saudi adolescents. Ann. Thorac. Med. 2012, 7, 133–139. [Google Scholar] [CrossRef]
- Duncan, S.; Duncan, E.K.; Fernandes, R.A.; Buonani, C.; Bastos, K.; Segatto, A.F.M.; Codogno, J.S.; Gomes, I.C.; Freitas, I.F., Jr. Modifiable risk factors for overweight and obesity in children and adolescents from Sao Paulo, Brazil. BMC Public Health 2011, 11, 585. [Google Scholar] [CrossRef] [Green Version]
- Croezen, S.; Visscher, T.L.; Ter Bogt, N.C.; Veling, M.L.; Haveman-Nies, A. Skipping breakfast, alcohol consumption and physical inactivity as risk factors for overweight and obesity in adolescents: Results of the E-MOVO project. Eur. J. Clin. Nutr. 2009, 63, 405–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradlee, M.L.; Singer, M.R.; Qureshi, M.M.; Moore, L.L. Food group intake and central obesity among children and adolescents in the Third National Health and Nutrition Examination Survey (NHANES III). Public Health Nutr. 2010, 13, 797–805. [Google Scholar] [CrossRef] [Green Version]
- Brown, C.M.; Dulloo, A.G.; Montani, J.P. Sugary drinks in the pathogenesis of obesity and cardiovascular diseases. Int. J. Obes. 2008, 32 (Suppl. 6), S28–S34. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Global Strategy on Diet, Physical Activity and Health; WHA57.17; WHO: Geneva, Switzerland, 2004. [Google Scholar]
- World Health Organization (WHO). Saudi Arabia Country Cooperation Strategy 2011–2016. Available online: http://apps.who.int/iris/bitstream/10665/113227/1/CCS_Saudia_2013_EN_14914.pdf?ua=1 (accessed on 27 July 2021).
- Saudi Arabia Ministry of Health; MOH Initiatives 2030. Available online: https://www.moh.gov.sa/en/Ministry/nehs/Pages/vision2030.aspx (accessed on 27 July 2021).
- Saudi Vision 2030, National Transformation Program 2020. Available online: http://vision2030.gov.sa/en (accessed on 28 July 2021).
- Al-Hazzaa, H.M.; Musaiger, A.O.; ATLS Research Group. Arab Teens Lifestyle Study (ATLS): Objectives, design, methodology and implications. Diabetes Metab. Syndr. Obes. 2011, 4, 417–426. [Google Scholar] [CrossRef] [Green Version]
- Al-Hazzaa, H.M.; Al-Sobayel, H.I.; Abahussain, N.A.; Qahwaji, D.M.; Alahmadi, M.A.; Musaiger, A.O. Association of dietary habits with levels of physical activity and screen time among adolescents living in Saudi Arabia. J. Hum. Nutr. Diet. 2014, 27 (Suppl. 2), 204–213. [Google Scholar] [CrossRef]
- Al-Hazzaa, H.M. Lifestyle Behaviors and Obesity: Brief Observations from the Arab Teens Lifestyle Study (ATLS) Findings. Obes. Open Access 2018, 4. Available online: https://sciforschenonline.org/journals/obesity/article-data/OOA-4-136/OOA-4-136.pdf (accessed on 20 July 2021).
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef]
- McCarthy, H.D.; Ashwell, M. A study of central fatness using waist-to-height ratios in UK children and adolescents over two decades supports the simple message—‘keep your waist circumference to less than half your height’. Int. J. Obes. 2006, 30, 988–992. [Google Scholar] [CrossRef] [Green Version]
- Taylor, R.W.; Jones, I.E.; Williams, S.M.; Goulding, A. Evaluation of waist circumference, waist-to-hip ratio, and the conicity index as screening tools for high trunk fat mass, as measured by dual-energy X-ray absorptiometry, in children aged 3–19 y. Am. J. Clin. Nutr. 2000, 72, 490–495. [Google Scholar] [CrossRef] [Green Version]
- Al-Hazzaa, H.M.; Al-Sobayel, H.I.; Musaiger, A.O. Convergent validity of the Arab Teens Lifestyle Study (ATLS) physical activity questionnaire. Int. J. Environ. Res. Public Health 2011, 8, 3810–3820. [Google Scholar] [CrossRef] [Green Version]
- Al-Hazzaa, H.M.; Al-Ahmadi, M.A. Self-reported questionnaire for the assessment of physical activity in youth 15–25 years: Development, reliability and construct validity. Arab. J. Food Nutr. 2003, 4, 279–291. [Google Scholar]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, G.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A Second Update of Codes and MET Values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butte, N.F.; Watson, K.B.; Ridley, K.; Zakeri, I.F.; Mcmurray, R.G.; Pfeiffer, K.A.; Crouter, S.E.; Herrmann, S.D.; Bassett, D.R.; Long, A.; et al. A Youth Compendium of Physical Activities: Activity Codes and Metabolic Intensities. Med. Sci. Sports Exerc. 2018, 50, 246–256. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics: Committee on Public Education. American Academy of Pediatrics: Children, adolescents, and television. Pediatrics 2001, 107, 423–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirshkowitz, M.; Whiton, K.; Albert, S.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Katz, E.S.; Kheirandish-Gozal, L.; et al. National Sleep Foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health 2015, 1, 40–50. Available online: http://www.sleephealthjournal.org/article/S2352-7218%2815%2900015-7/fulltext (accessed on 20 July 2021). [CrossRef]
- General Authority for Statistics (GAS). Saudi Youth in numbers: A report for International Youth Day 2020. Available online: https://www.stats.gov.sa/sites/default/files/saudi_youth_in_numbers_report_2020en_0.pdf (accessed on 28 July 2021).
- Sweeting, H.; Anderson, A.; West, P. Socio-demographic correlates of dietary habits in mid to late adolescence. Eur. J. Clin. Nutr. 1994, 48, 736–748. [Google Scholar]
- World Health Organization. Every Woman, Every Child, Every Adolescent: Achievements and Prospects: The Final Report of the Independent Expert Review Group on Information and Accountability for Women’s and Children’s Health; World Health Organization: Geneva, Switzerland, 2015; Available online: https://apps.who.int/iris/handle/10665/183585 (accessed on 28 July 2021).
- Tremblay, M.S.; Colley, R.C.; Saunders, T.J.; Healy, G.N.; Owen, N. Physiological and health implications of a sedentary lifestyle. Appl. Physiol. Nutr. Metab. 2010, 35, 725–740. [Google Scholar] [CrossRef]
- Al-Hazzaa, H.M.; Alahmadi, M.A.; Al-Sobayel, H.; Abahussain, N.; Qahwaji, D.; Musaiger, A.O. Patterns and determinants of physical activity among Saudi youth. J. Phys. Act. Health 2014, 11, 1202–1211. [Google Scholar] [CrossRef]
- Alsobayel, H.; Al-Hazzaa, H.M.; Abahussain, N.; Qahwaji, D.; Musaiger, A.O. Gender differences in leisure-time versus non-leisure-time physical activity among Saudi adolescents. Ann. Agric. Environ. Med. 2015, 22, 334–348. [Google Scholar] [CrossRef] [Green Version]
- Carson, V.; Rinaldi, R.L.; Torrance, B.; Maximova, K.; Ball, G.D.; Majumdar, S.R.; Plotnikoff, R.C.; Veugelers, P.; Boulé, N.G.; Wozny, P.; et al. Vigorous physical activity and longitudinal associations with cardiometabolic risk factors in youth. Int. J. Obes. 2014, 38, 16–21. [Google Scholar] [CrossRef]
- Henderson, M.; Benedetti, A.; Gray-Donald, K. Dietary composition and its associations with insulin sensitivity and insulin secretion in youth. Br. J. Nutr. 2014, 111, 527–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, X.; Basterfield, L.; Parkinson, K.N.; Pearce, M.S.; Reilly, J.K.; Adamson, A.J.; Reilly, J.J. Non-linear longitudinal associations between moderate-to-vigorous physical activity and adiposity across the adiposity distribution during childhood and adolescence: Gateshead Millennium Study. Int. J. Obes. 2019, 43, 744–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janz, K.F.; Letuchy, E.M.; Burns, T.L.; Gilmore, J.M.E.; Torner, J.C.; Levym, S.M. Objectively measured physical activity trajectories predict adolescent bone strength: Iowa Bone Development Study. Br. J. Sports Med. 2014, 48, 1032–1036. [Google Scholar] [CrossRef] [PubMed]
- Janz, K.F.; Dawson, J.D.; Mahoney, L.T. Tracking physical fitness and physical activity from childhood to adolescence: The Muscatine study. Med. Sci. Sports Exerc. 2000, 32, 1250–1257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raitakari, O.T.; Taimela, S.; Porkka, K.V.; Telama, R.; Välimäki, I.; Akerblom, H.K.; Viikari, J.S. Associations between physical activity and risk factors for coronary heart disease: The Cardiovascular Risk in Young Finns Study. Med. Sci. Sports Exerc. 1997, 29, 1055–1061. [Google Scholar] [CrossRef] [PubMed]
- Hills, A.P.; Andersen, L.B.; Byrne, N.M. Physical activity and obesity in children. Br. J. Sports Med. 2011, 45, 866–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booth, V.M.; Rowlands, A.V.; Dollman, J. Physical activity temporal trends among children and adolescents. J. Sci. Med. Sport 2015, 18, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.C.E.; Anedda, B.; Burchartz, A.; Oriwol, D.; Kolb, S.; Wäsche, H.; Niessner, C.; Woll, A. The physical activity of children and adolescents in Germany 2003–2017: The MoMo-study. PLoS ONE 2020, 15, e0236117. [Google Scholar] [CrossRef] [PubMed]
- Booth, V.; Rowlands, A.; Dollman, J. Physical activity trends in separate contexts among South Australian older children (10–12 Y) and early adolescents (13–15 Y) from 1985 to 2013. Pediatr. Exerc. Sci. 2019, 31, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Amiri, P.; Naseri, P.; Vahedi-Notash, G.; Jalali-Farahani, S.; Mehrabi, Y.; Hamzavi-Zarghani, N.; Azizi, F.; Hadaegh, F.; Khalili, D. Trends of low physical activity among Iranian adolescents across urban and rural areas during 2006–2011. Sci. Rep. 2020, 10, 21318. [Google Scholar] [CrossRef] [PubMed]
- Farooq, A.; Martin, A.; Janssen, X.; Wilson, M.G.; Gibson, A.M.; Hughes, A.; Reilly, J.J. Longitudinal changes in moderate-to-vigorous-intensity physical activity in children and adolescents: A systematic review and meta-analysis. Obes. Rev. 2020, 21, e12953. [Google Scholar] [CrossRef] [Green Version]
- Janssen, X.; Mann, K.D.; Basterfield, L.; Parkinson, K.N.; Pearce, M.S.; Reilly, J.K.; Adamson, A.J.; Reilly, J.J. Development of sedentary behavior across childhood and adolescence: Longitudinal analysis of the Gateshead Millennium Study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 88. [Google Scholar] [CrossRef] [Green Version]
- Yang, L.; Cao, C.; Kantor, E.D.; Nguyen, L.H.; Zheng, X.; Park, Y.; Giovannucci, E.L.; Matthews, C.E.; Colditz, G.A.; Cao, Y.; et al. Trends in Sedentary Behavior among the US Population, 2001–2016. JAMA 2019, 321, 1587–1597. [Google Scholar] [CrossRef]
- Bucksch, J.; Sigmundova, D.; Hamrik, Z.; Troped, P.J.; Melkevik, O.; Ahluwalia, N.; Borraccino, A.; Tynjälä, J.; Kalman, M.; Inchley, J. International trends in adolescent screen-time behaviors from 2002 to 2010. J. Adolesc. Health 2016, 58, 417–425. [Google Scholar] [CrossRef]
- Dalene, K.E.; Anderssen, S.A.; Andersen, L.B.; Steene-Johannessen, J.; Ekelund, U.; Hansen, B.H.; Kolle, E. Secular and longitudinal physical activity changes in population-based samples of children and adolescents. Scand. J. Med. Sci. Sports 2018, 28, 161–171. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Height and body-mass index trajectories of school-aged children and adolescents from 1985 to 2019 in 200 countries and territories: A pooled analysis of 2181 population-based studies with 65 million participants. Lancet 2020, 396, 1511–1524. [Google Scholar] [CrossRef]
- Aars, N.A.; Beldo, S.; Jacobsen, B.K.; Horsch, A.; Morseth, B.; Emaus, N.; Furberg, A.-S.; Grimsgaard, S. Association between objectively measured physical activity and longitudinal changes in body composition in adolescents: The Tromso study fit futures cohort. BMJ Open 2020, 10, e036991. [Google Scholar] [CrossRef] [PubMed]
- Cooper, A.R.; Goodman, A.; Page, A.S.; Sherar, L.B.; Esliger, D.W.; van Sluijs, E.M.; Andersen, L.B.; Anderssen, S.; Cardon, G.; Davey, R.; et al. Objectively measured physical activity and sedentary time in youth: The International children’s accelerometry database (ICAD). Int. J. Behav. Nutr. Phys. Act. 2015, 12, 113. [Google Scholar] [CrossRef] [Green Version]
- Alexy, U.; Wicher, M.; Kersting, M. Breakfast trends in children and adolescents: Frequency and quality. Public Health Nutr. 2010, 13, 1795–1802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasmussen, M.; Krølner, R.; Svastisalee, C.M.; Due, P.; Holstein, B.E. Secular trends in fruit intake among Danish schoolchildren, 1988 to 2006: Changing habits or methodological artefacts? Int. J. Behav. Nutr. Phys. Act. 2008, 5, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kant, A.K.; Graubard, B.I. 20-Year trends in dietary and meal behaviors were similar in U.S. children and adolescents of different race/ethnicity. J. Nutr. 2011, 141, 1880–1888. [Google Scholar] [CrossRef] [PubMed]
- Fleary, S.A.; Joseph, P.; Zhang, E.; Freund, K. Disparities in Adolescents’ Obesogenic Behaviors, 2005–2017. Am. J. Health Behav. 2021, 45, 677–694. [Google Scholar] [CrossRef]
- Jongenelis, M.I.; Scully, M.; Morley, B.; Pratt, I.S. Vegetable and fruit intake in Australian adolescents: Trends over time and perceptions of consumption. Appetite 2018, 129, 49–54. [Google Scholar] [CrossRef]
- Miller, G.; Merlo, C.; Demissie, Z.; Sliwa, S.; Park, S. Trends in beverage consumption among high school students—United States, 2007–2015. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 112–116. [Google Scholar] [CrossRef] [Green Version]
- Allafi, A.; Al-Haifi, A.R.; Al-Fayez, M.A.; Al-Athari, B.I.; Al-Ajmi, F.A.; Al-Hazzaa, H.M.; Musaiger, A.O.; Ahmed, F. Physical activity, sedentary behaviors and dietary habits among Kuwaiti adolescents: Gender differences. Public Health Nutr. 2014, 17, 2045–2052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ullrich, A.; Baumann, S.; Voigt, L.; John, U.; Ulbricht, S. Measurement Reactivity of Accelerometer-Based Sedentary Behavior and Physical Activity in 2 Assessment Periods. J. Phys. Act. Health 2021, 18, 185–191. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| SN | School Name | Gender | Type of School | Number of Participants |
|---|---|---|---|---|
| 1 | First High School | Females | Public | 85 |
| 2 | High School 39 | Females | Public | 73 |
| 3 | High School 58 | Females | Public | 97 |
| 4 | High School 68 | Females | Public | 73 |
| 5 | High School 139 | Females | Public | 96 |
| 6 | Tarbiah Namozhejiah High School | Females | Private | 63 |
| 7 | Sorooq Almarifah High School | Females | Private | 54 |
| 8 | Near Private High School | Females | Private | 60 |
| 9 | Imam Shawkani High School | Males | Public | 105 |
| 10 | Prince Sultan Complex High School | Males | Public | 89 |
| 11 | Muhammed bin Wasie High School | Males | Public | 115 |
| 12 | Abeer High School | Males | Private | 66 |
| 13 | Fursan High School | Males | Private | 74 |
| 14 | Maahad Asameh High School | Males | Public | 113 |
| 15 | Shoura High School | Males | Public | 99 |
| Total selected students = 1262 (Females = 601; Males = 661) | ||||
| Variable | All | Males | Females | p-Value * |
|---|---|---|---|---|
| Number of participants | 1262 | 661 (52.4%) | 601 (47.6%) | - |
| Age (year) | 16.4 ± 0.95 | 16.4 ± 0.94 | 16.3 ± 0.96 | 0.050 |
| School type (%) | 0.001 | |||
| Public | 74.8 | 78.8 | 70.5 | |
| Private | 25.2 | 21.2 | 29.5 |
| Variable | All n = 1261 | Male n = 660 | Female n = 601 | p-Value * |
|---|---|---|---|---|
| Body weight (kg) | 65.6 ± 20.9 | 73.2 ± 23.1 | 57.3 ± 14.3 | <0.001 |
| Body height (cm) | 163.6 ± 8.9 | 169.7 ± 6.8 | 157.0 ± 5.5 | <0.001 |
| Body mass index (kg/m2) | 24.3 ± 6.6 | 25.3 ± 7.4 | 23.2 ± 5.4 | <0.001 |
| Overweight + obesity ** | 40.5 | 47.3 | 32.8 | <0.001 |
| Variable | Change | Percent Change (%) | p-Value * |
|---|---|---|---|
| Age (year) | Increased | 2.5 | <0.001 |
| Body weight (kg) | Increased | 3.1 | 0.107 |
| Body mass index (kg/m2) | Increased | 0.83 | 0.582 |
| Waist circumference (cm) | Increased | 2.2 | 0.027 |
| Screen time (hours/day) | Decreased | 8.5 | <0.001 |
| Sleep duration (hours/night) | No change | 0.0 | 0.558 |
| All moderate-intensity physical activity (METs-min/week) | Increased | 111.9 | <0.001 |
| All vigorous-intensity physical activity (METs-min/week) | Decrease | 5.9 | <0.001 |
| Total physical activity (METs-min/week) | Increased | 27.5 | <0.001 |
| Inactivity prevalence (<1680 METs-min/week) | Decreased | 18.3 | <0.001 |
| Breakfast intake (day/week) | Decreased | 7.0 | 0.015 |
| Vegetable intake (day/week) | Increased | 3.2 | 0.247 |
| Fruit intake (day/week) | Increased | 10.3 | 0.002 |
| Milk/dairy-product intake (day/week) | Increased | 2.6 | 0.187 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Hazzaa, H.M.; Albawardi, N.M. Obesity, Lifestyle Behaviors, and Dietary Habits of Saudi Adolescents Living in Riyadh (ATLS-2 Project): Revisited after a Ten-Year Period. Life 2021, 11, 1078. https://doi.org/10.3390/life11101078
Al-Hazzaa HM, Albawardi NM. Obesity, Lifestyle Behaviors, and Dietary Habits of Saudi Adolescents Living in Riyadh (ATLS-2 Project): Revisited after a Ten-Year Period. Life. 2021; 11(10):1078. https://doi.org/10.3390/life11101078
Chicago/Turabian StyleAl-Hazzaa, Hazzaa M., and Nada M. Albawardi. 2021. "Obesity, Lifestyle Behaviors, and Dietary Habits of Saudi Adolescents Living in Riyadh (ATLS-2 Project): Revisited after a Ten-Year Period" Life 11, no. 10: 1078. https://doi.org/10.3390/life11101078
APA StyleAl-Hazzaa, H. M., & Albawardi, N. M. (2021). Obesity, Lifestyle Behaviors, and Dietary Habits of Saudi Adolescents Living in Riyadh (ATLS-2 Project): Revisited after a Ten-Year Period. Life, 11(10), 1078. https://doi.org/10.3390/life11101078