
Epidemiological Characterization of Clinical Fungal Isolates from Pauls Stradinš Clinical University Hospital, Latvia: A 4-Year Surveillance Report

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Location and Design
2.2. Sample Collection and Determination of Antifungal Resistance Rates
2.3. Data Collection and Analysis
3. Results
3.1. Candida spp. Were the Most Frequently Isolated Nosocomial Fungal Species
3.2. Characterization of Candida spp. Isolates
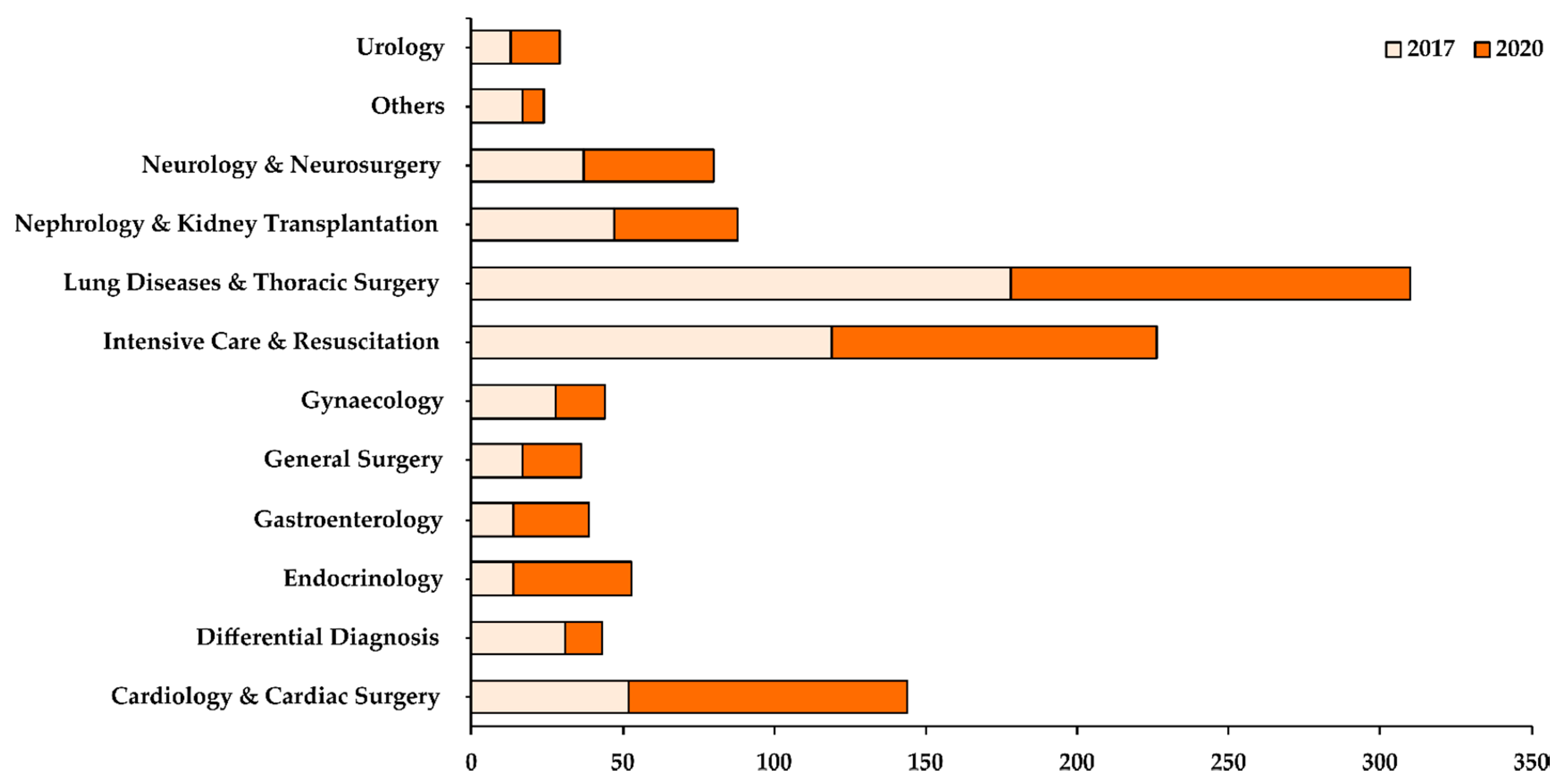
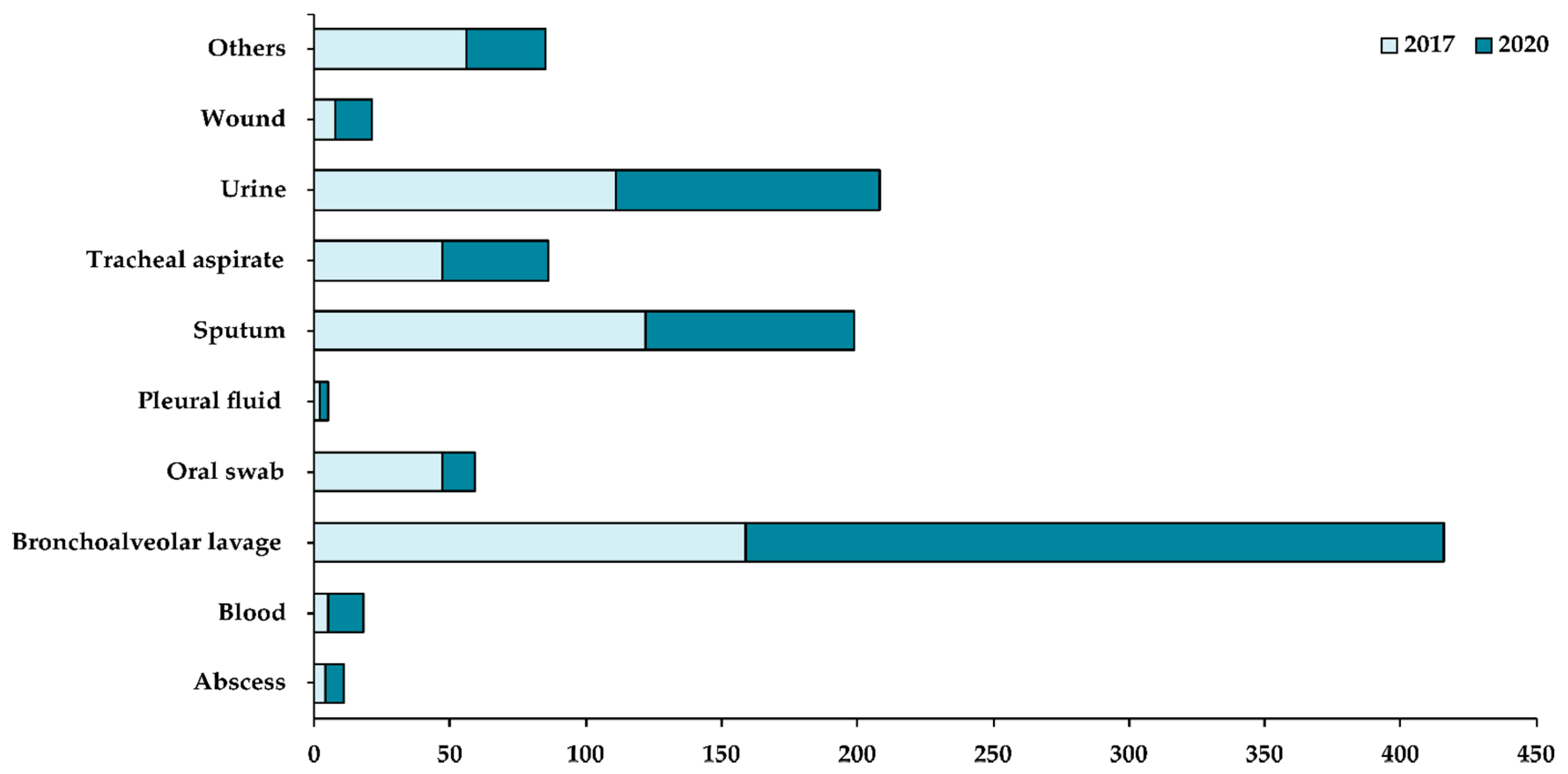
3.3. Distribution of Candida Isolates Based on Department and Patient Specimen Collected
3.4. Distribution of Candida Isolates Based on Cases of Candidemia
4. Discussion
4.1. Candida spp. as Nosocomial Fungal Agents
4.2. Aspergillus spp. as Nosocomial Fungal Agents
4.3. Geotrichum spp. as Nosocomial Fungal Agents
4.4. Other Nosocomial Fungal Agents
4.5. Antifungal Treatment Principles
4.6. Antifungal Resistance Mechanisms
4.7. Antifungal Stewardship, Infection Control, and Future Strategies
- (i)
- The development of institutional treatment guidelines for prophylaxis and empiric therapy, including the identification of high-risk patients, the estimation of a proper dosage, the timely identification of the agent, etc.;
- (ii)
- The development of targeted education programs for appropriate diagnosis and treatment for clinicians, specialists, nurses, etc.;
- (iii)
- An antifungal prescription review for drug–drug interactions, including the identification of over-prescribed agents and the rationalization of prescription strategies;
- (iv)
- The development, encouragement, and adoption of an intravenous-to-oral antifungal drug transition program;
- (v)
- Local surveillance and reporting of invasive fungal diseases to prescribers, management, and other relevant health monitoring bodies at the national and EU/EEA level to contribute towards a comprehensive national database.
4.8. Limitations of the Present Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pai, V.; Ganavalli, A.; Kikkeri, N.N. Antifungal Resistance in Dermatology. Indian J. Dermatol. 2018, 63, 361–368. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kapil, A. (Ed.) Ananthanarayan & Paniker’s Textbook of Microbiology, 9th ed.; University Press Private Limited: Hyderabad, India, 2013; pp. 589–615. [Google Scholar]
- Berman, J.; Krysan, D.J. Drug resistance and tolerance in fungi. Nat. Rev. Microbiol. 2020, 18, 319–331, Erratum in 2020, 18, 539. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kanafani, Z.A.; Perfect, J.R. Antimicrobial resistance: Resistance to antifungal agents: Mechanisms and clinical impact. Clin. Infect. Dis. 2008, 46, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Rossi, N.M.; Peres, N.T.; Rossi, A. Antifungal resistance mechanisms in dermatophytes. Mycopathologia 2008, 166, 369–383. [Google Scholar] [CrossRef] [PubMed]
- White, T.C.; Marr, K.A.; Bowden, R.A. Clinical, cellular, and molecular factors that contribute to antifungal drug resistance. Clin. Microbiol. Rev. 1998, 11, 382–402. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Perlin, D.S.; Shor, E.; Zhao, Y. Update on Antifungal Drug Resistance. Curr. Clin. Microbiol. Rep. 2015, 2, 84–95. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vandeputte, P.; Ferrari, S.; Coste, A.T. Antifungal resistance and new strategies to control fungal infections. Int. J. Microbiol. 2012, 2012, 713687. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Costa-Orlandi, C.B.; Sardi, J.C.; Santos, C.T.; Fusco-Almeida, A.M.; Mendes-Giannini, M.J. In vitro characterization of Trichophyton rubrum and, T. mentagrophytes biofilms. Biofouling 2014, 30, 719–727. [Google Scholar] [CrossRef] [PubMed]
- van der Linden, J.W.; Camps, S.M.; Kampinga, G.A.; Arends, J.P.; Debets-Ossenkopp, Y.J.; Haas, P.J.; Rijnders, B.J.; Kuijper, E.J.; van Tiel, F.H.; Varga, J.; et al. Aspergillosis due to voriconazole highly resistant Aspergillus fumigatus and recovery of genetically related resistant isolates from domiciles. Clin. Infect. Dis. 2013, 57, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Sikora, A.; Zahra, F. Nosocomial Infections. [Updated 2021 July 7]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK559312 (accessed on 30 July 2021).
- Suleyman, G.; Alangaden, G.J. Nosocomial Fungal Infections: Epidemiology, Infection Control, and Prevention. Infect. Dis. Clin. N. Am. 2016, 30, 1023–1052. [Google Scholar] [CrossRef] [PubMed]
- Vazquez, J.A.; Miceli, M.H.; Alangaden, G. Invasive fungal infections in transplant recipients. Ther. Adv. Infect. Dis. 2013, 1, 85–105. [Google Scholar] [CrossRef]
- Sievert, D.M.; Ricks, P.; Edwards, J.R.; Schneider, A.; Patel, J.; Srinivasan, A.; Kallen, A.; Limbago, B.; Fridkin, S.; National Healthcare Safety Network (NHSN) Team and Participating NHSN Facilities. Antimicrobial-resistant pathogens associated with healthcare-associated infections: Summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2009–2010. Infect. Control Hosp. Epidemiol. 2013, 34, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Perlroth, J.; Choi, B.; Spellberg, B. Nosocomial fungal infections: Epidemiology, diagnosis, and treatment. Med. Mycol. 2007, 45, 321–346. [Google Scholar] [CrossRef] [PubMed]
- Wilson, L.S.; Reyes, C.M.; Stolpman, M.; Speckman, J.; Allen, K.; Beney, J. The direct cost and incidence of systemic fungal infections. Value Health 2002, 5, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, W.R. Epidemiology of nosocomial fungal infections, with emphasis on Candida species. Clin. Infect. Dis. 1995, 20, 1526–1530. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, W.R.; Martone, W.J. Predominant pathogens in hospital infections. J. Antimicrob. Chemother. 1992, 29 (Suppl. A), 19–24. [Google Scholar] [CrossRef] [PubMed]
- Krysan, D.J. The unmet clinical need of novel antifungal drugs. Virulence 2017, 8, 135–137. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Carolus, H.; Pierson, S.; Lagrou, K.; Van Dijck, P. Amphotericin B and Other Polyenes-Discovery, Clinical Use, Mode of Action and Drug Resistance. J. Fungi 2020, 6, 321. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hazen, E.L.; Brown, R. Fungicidin, an antibiotic produced by a soil actinomycete. Proc. Soc. Exp. Biol. Med. 1951, 76, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Zotchev, S.B. Polyene macrolide antibiotics and their applications in human therapy. Curr. Med. Chem. 2003, 10, 211–223. [Google Scholar] [CrossRef] [PubMed]
- Mesa-Arango, A.C.; Scorzoni, L.; Zaragoza, O. It only takes one to do many jobs: Amphotericin B as antifungal and immunomodulatory drug. Front. Microbiol. 2012, 3, 286. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kinsky, S.C. Antibiotic interaction with model membranes. Annu. Rev. Pharmacol. 1970, 10, 119–142. [Google Scholar] [CrossRef] [PubMed]
- Palacios, D.S.; Dailey, I.; Siebert, D.M.; Wilcock, B.C.; Burke, M.D. Synthesis-enabled functional group deletions reveal key underpinnings of amphotericin B ion channel and antifungal activities. Proc. Natl. Acad. Sci. USA 2011, 108, 6733–6738. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gray, K.C.; Palacios, D.S.; Dailey, I.; Endo, M.M.; Uno, B.E.; Wilcock, B.C.; Burke, M.D. Amphotericin primarily kills yeast by simply binding ergosterol. Proc. Natl. Acad. Sci. USA 2012, 109, 2234–2239. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sangalli-Leite, F.; Scorzoni, L.; Mesa-Arango, A.C.; Casas, C.; Herrero, E.; Gianinni, M.J.; Rodríguez-Tudela, J.L.; Cuenca-Estrella, M.; Zaragoza, O. Amphotericin B mediates killing in Cryptococcus neoformans through the induction of a strong oxidative burst. Microbes Infect. 2011, 13, 457–467. [Google Scholar] [CrossRef] [PubMed]
- Dutcher, J.D. The discovery and development of amphotericin, B. Dis. Chest 1968, 54 (Suppl. S1), 296–298. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekar, P. Management of invasive fungal infections: A role for polyenes. J. Antimicrob. Chemother. 2011, 66, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, A.G.; Marquês, J.T.; Carreira, A.C.; Castro, I.R.; Viana, A.S.; Mingeot-Leclercq, M.P.; de Almeida, R.F.M.; Silva, L.C. The molecular mechanism of Nystatin action is dependent on the membrane biophysical properties and lipid composition. Phys. Chem. Chem. Phys. 2017, 19, 30078–30088. [Google Scholar] [CrossRef] [PubMed]
- Allen, D.; Wilson, D.; Drew, R.; Perfect, J. Azole antifungals: 35 years of invasive fungal infection management. Expert Rev. Anti-Infect. Ther. 2015, 13, 787–798. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, D.J.; Hitchcock, C.A.; Sibley, C.M. Current and emerging azole antifungal agents. Clin. Microbiol. Rev. 1999, 12, 40–79. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cappelletty, D.; Eiselstein-McKitrick, K. The echinocandins. Pharmacotherapy 2007, 27, 369–388. [Google Scholar] [CrossRef] [PubMed]
- Mroczyńska, M.; Brillowska-Dąbrowska, A. Review on Current Status of Echinocandins Use. Antibiotics 2020, 9, 227. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Odds, F.C.; Brown, A.J.; Gow, N.A. Antifungal agents: Mechanisms of action. Trends Microbiol. 2003, 11, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Pegu, R.; Borah, R.; Pratihar, S. Synthetic Compounds for Antifungal Chemotherapy. In Recent Trends in Antifungal Agents and Antifungal Therapy; Basak, A., Chakraborty, R., Mandal, S.M., Eds.; Springer: New Delhi, India, 2016; pp. 191–215. [Google Scholar]
- Jain, N.; Jansone, I.; Obidenova, T.; Simanis, R.; Meisters, J.; Straupmane, D.; Reinis, A. Antimicrobial Resistance in Nosocomial Isolates of Gram-Negative Bacteria: Public Health Implications in the Latvian Context. Antibiotics 2021, 10, 791. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- European Centre for Disease Prevention and Control EU Case Definitions. 2021. Available online: https://www.ecdc.europa.eu/en/surveillance-and-disease-data/eu-case-definitions (accessed on 21 April 2021).
- The European Committee on Antimicrobial Susceptibility Testing Antifungal Agents Breakpoint Tables for Interpretation of MICs. Version 9.0; valid from Feb 2018. 2021. Available online: http://www.eucast.org (accessed on 5 July 2021).
- European Antimicrobial Resistance Surveillance Network (EARS-Net). 2017–2019. Available online: https://www.ecdc.europa.eu/en/antimicrobial-resistance/surveillance-and-disease-data/report (accessed on 5 July 2021).
- Benedict, K.; Jackson, B.R.; Chiller, T.; Beer, K.D. Estimation of Direct Healthcare Costs of Fungal Diseases in the United States. Clin. Infect. Dis. 2019, 68, 1791–1797. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Benedict, K.; Molinari, N.A.; Jackson, B.R. Public Awareness of Invasive Fungal Diseases—United States, 2019. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 1343–1346. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Think Fungus: Fungal Disease Awareness Week. Available online: https://www.cdc.gov/fungal/awareness-week.html (accessed on 30 July 2021).
- de Oliveira Santos, G.C.; Vasconcelos, C.C.; Lopes, A.J.O.; de Sousa Cartágenes, M.D.S.; Filho, A.K.D.B.; do Nascimento, F.R.F.; Ramos, R.M.; Pires, E.R.R.B.; de Andrade, M.S.; Rocha, F.M.G.; et al. Candida Infections and Therapeutic Strategies: Mechanisms of Action for Traditional and Alternative Agents. Front. Microbiol. 2018, 9, 1351. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sardi, J.C.O.; Scorzoni, L.; Bernardi, T.; Fusco-Almeida, A.M.; Mendes Giannini, M.J.S. Candida species: Current epidemiology, pathogenicity, biofilm formation, natural antifungal products and new therapeutic options. J. Med. Microbiol. 2013, 62 Pt 1, 10–24. [Google Scholar] [CrossRef] [PubMed]
- Paramythiotou, E.; Frantzeskaki, F.; Flevari, A.; Armaganidis, A.; Dimopoulos, G. Invasive fungal infections in the ICU: How to approach, how to treat. Molecules 2014, 19, 1085–1119. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pappas, P.G.; Lionakis, M.S.; Arendrup, M.C.; Ostrosky-Zeichner, L.; Kullberg, B.J. Invasive candidiasis. Nat. Rev. Dis. Primers 2018, 4, 18026. [Google Scholar] [CrossRef] [PubMed]
- Spampinato, C.; Leonardi, D. Candida infections, causes, targets, and resistance mechanisms: Traditional and alternative antifungal agents. Biomed Res. Int. 2013, 2013, 204237. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wächtler, B.; Citiulo, F.; Jablonowski, N.; Förster, S.; Dalle, F.; Schaller, M.; Wilson, D.; Hube, B. Candida albicans-epithelial interactions: Dissecting the roles of active penetration, induced endocytosis and host factors on the infection process. PLoS ONE 2012, 7, e36952. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Maccallum, D.M. Hosting infection: Experimental models to assay Candida virulence. Int. J. Microbiol. 2012, 2012, 363764. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Miceli, M.H.; Díaz, J.A.; Lee, S.A. Emerging opportunistic yeast infections. Lancet Infect. Dis. 2011, 11, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Diekema, D.J. Epidemiology of invasive candidiasis: A persistent public health problem. Clin. Microbiol. Rev. 2007, 20, 133–163. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- López-Martínez, R. Candidosis, a new challenge. Clin. Dermatol. 2010, 28, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Jahagirdar, V.L.; Davane, M.S.; Aradye, S.C.; Nagoba, B.S. Candida species as potential nosocomial pathogens—A review. Electron. J. Gen. Med. 2018, 15, em05. [Google Scholar] [CrossRef]
- Ha, J.F.; Italiano, C.M.; Heath, C.H.; Shih, S.; Rea, S.; Wood, F.M. Candidemia and invasive candidiasis: A review of the literature for the burns surgeon. Burns 2011, 37, 181–195. [Google Scholar] [CrossRef] [PubMed]
- Rangel-Frausto, M.S.; Houston, A.K.; Bale, M.J.; Fu, C.; Wenzel, R.P. An experimental model for study of Candida survival and transmission in human volunteers. Eur. J. Clin. Microbiol. Infect. Dis. 1994, 13, 590–595. [Google Scholar] [CrossRef] [PubMed]
- Silva, S.; Negri, M.; Henriques, M.; Oliveira, R.; Williams, D.W.; Azeredo, J. Candida glabrata, Candida parapsilosis and Candida tropicalis: Biology, epidemiology, pathogenicity and antifungal resistance. FEMS Microbiol. Rev. 2012, 36, 288–305. [Google Scholar] [CrossRef] [PubMed]
- Deorukhkar, S.C.; Saini, S.; Mathew, S. Virulence Factors Contributing to Pathogenicity of Candida tropicalis and Its Antifungal Susceptibility Profile. Int. J. Microbiol. 2014, 2014, 456878. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Deorukhkar, S.; Saini, S. Evaluation of phospholipase activity in biofilm forming Candida species isolated from intensive care unit patients. Br. Microbiol. Res. J. 2013, 3, 440–447. [Google Scholar] [CrossRef]
- Garey, K.W.; Rege, M.; Pai, M.P.; Mingo, D.E.; Suda, K.J.; Turpin, R.S.; Bearden, D.T. Time to initiation of fluconazole therapy impacts mortality in patients with candidemia: A multi-institutional study. Clin. Infect. Dis. 2006, 43, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Righi, E.; Ansaldi, F.; Merelli, M.; Trucchi, C.; De Pascale, G.; Diaz-Martin, A.; Luzzati, R.; Rosin, C.; Lagunes, L.; et al. A multicenter study of septic shock due to candidemia: Outcomes and predictors of mortality. Intensive Care Med. 2014, 40, 839–845, Erratum in 2014, 40, 1186. [Google Scholar] [CrossRef] [PubMed]
- Clancy, C.J.; Nguyen, M.H. Finding the “missing 50%” of invasive candidiasis: How nonculture diagnostics will improve understanding of disease spectrum and transform patient care. Clin. Infect. Dis. 2013, 56, 1284–1292. [Google Scholar] [CrossRef] [PubMed]
- Nicolle, M.C.; Benet, T.; Vanhems, P. Aspergillosis: Nosocomial or community-acquired? Med. Mycol. 2011, 49 (Suppl. S1), S24–S29. [Google Scholar] [CrossRef] [PubMed]
- Patterson, T.F.; Mandell, G.L.; Benett, J.E.; Dolin, R. Aspergillus Species, Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 6th ed.; Elsevier Churchill Livingstone: Philadelphia, PA, USA, 2005; pp. 2958–2973. [Google Scholar]
- Pfaller, M.A.; Diekema, D.J. Epidemiology of invasive mycoses in North America. Crit. Rev. Microbiol. 2010, 36, 1–53. [Google Scholar] [CrossRef] [PubMed]
- Warris, A.; Voss, A.; Verweij, P.E. Hospital sources of Aspergillus: New routes of transmission? Rev. Iberoam. Micol. 2001, 18, 156–162. [Google Scholar] [PubMed]
- Verweij, P.E.; Kerremans, J.J.; Voss, A.; Meis, J.F. Fungal contamination of tobacco and marijuana. JAMA 2000, 284, 2875. [Google Scholar] [CrossRef] [PubMed]
- Rhame, F.S. Prevention of nosocomial aspergillosis. J. Hosp. Infect. 1991, 18 (Suppl. A), 466–472. [Google Scholar] [CrossRef] [PubMed]
- National Guidelines for the Prevention of Nosocomial Invasive Aspergillosis during Construction/Renovation Activities/Developed by a Sub-Committee of the Scientific Advisory Committee of the National Disease Surveillance Centre. National Disease Surveillance Centre (NDSC) [Lenus—The Irish Health Repository]. Available online: http://hdl.handle.net/10147/43715 (accessed on 31 July 2021).
- Partridge-Hinckley, K.; Liddell, G.M.; Almyroudis, N.G.; Segal, B.H. Infection control measures to prevent invasive mould diseases in hematopoietic stem cell transplant recipients. Mycopathologia 2009, 168, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Segal, B.H. Aspergillosis. N. Engl. J. Med. 2009, 360, 1870–1884. [Google Scholar] [CrossRef] [PubMed]
- Einsele, H.; Quabeck, K.; Müller, K.D.; Hebart, H.; Rothenhöfer, I.; Löffler, J.; Schaefer, U.W. Prediction of invasive pulmonary aspergillosis from colonisation of lower respiratory tract before marrow transplantation. Lancet 1998, 352, 1443. [Google Scholar] [CrossRef] [PubMed]
- VandenBergh, M.F.; Verweij, P.E.; Voss, A. Epidemiology of nosocomial fungal infections: Invasive aspergillosis and the environment. Diagn. Microbiol. Infect. Dis. 1999, 34, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Anaissie, E.J.; Costa, S.F. Nosocomial aspergillosis is waterborne. Clin. Infect. Dis. 2001, 33, 1546–1548. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.J. Primary cutaneous aspergillosis--an emerging infection among immunocompromised patients. Clin. Infect. Dis. 1998, 27, 453–457. [Google Scholar] [CrossRef] [PubMed]
- Martino, P.; Venditti, M.; Micozzi, A.; Morace, G.; Polonelli, L.; Mantovani, M.P.; Petti, M.C.; Burgio, V.L.; Santini, C.; Serra, P.; et al. Blastoschizomyces capitatus: An emerging cause of invasive fungal disease in leukemia patients. Rev. Infect. Dis. 1990, 12, 570–582. [Google Scholar] [CrossRef] [PubMed]
- Fouassier, M.; Joly, D.; Cambon, M.; Peigue-Lafeuille, H.; Condat, P. Infection à Geotrichum capitatum chez un patient neutropénique. A propos d’un cas et revue de la littérature [Geotrichum capitatum infection in a neutropenic patient. Apropos of a case and review of the literature]. Rev. Med. Interne 1998, 19, 431–433. (In French) [Google Scholar] [CrossRef] [PubMed]
- Mazzocato, S.; Marchionni, E.; Fothergill, A.W.; Sutton, D.A.; Staffolani, S.; Gesuita, R.; Skrami, E.; Fiorentini, A.; Manso, E.; Barchiesi, F. Epidemiology and outcome of systemic infections due to saprochaete capitata: Case report and review of the literature. Infection 2015, 43, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Pamidimukkala, U.; Kancharla, A.; Sudhaharan, S.; Gundeti, S.; Mandarapu, S.; Nagalla, V.K.; Raju, S.B.; Karanam, S.D. Isolation of the Rare Opportunistic Yeast Saprochaete capitata from Clinical Samples-Experience from a Tertiary Care Hospital in Southern India and a Brief Review of the Literature. J. Clin. Diagn. Res. 2017, 11, DC36–DC42. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Girmenia, C.; Pagano, L.; Martino, B.; D’Antonio, D.; Fanci, R.; Specchia, G.; Melillo, L.; Buelli, M.; Pizzarelli, G.; Venditti, M.; et al. Invasive infections caused by Trichosporon species and Geotrichum capitatum in patients with hematological malignancies: A retrospective multicenter study from Italy and review of the literature. J. Clin. Microbiol. 2005, 43, 1818–1828. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gurgui, M.; Sanchez, F.; March, F.; Lopez-Contreras, J.; Martino, R.; Cotura, A.; Galvez, M.L.; Roig, C.; Coll, P. Nosocomial outbreak of Blastoschizomyces capitatus associated with contaminated milk in a haematological unit. J. Hosp. Infect. 2011, 78, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Radic, M.; Goic Barisic, I.; Kuscevic, D.; Novak, A.; Tonkic, M.; Rubic, Z. Geotrichum capitatum respiratory tract infection in a patient with polytrauma. Infez. Med. 2015, 23, 270–274. [Google Scholar] [PubMed]
- Hajar, Z.; Medawar, W.; Rizk, N. Saprochaete capitata (Geotrichum capitatum), an emerging fungal infection in kidney transplant recipients. J. Mycol. Med. 2018, 28, 387–389. (In French) [Google Scholar] [CrossRef] [PubMed]
- Ulu-Kilic, A.; Atalay, M.A.; Metan, G.; Cevahir, F.; Koç, N.; Eser, B.; Çetin, M.; Kaynar, L.; Alp, E. Saprochaete capitata as an emerging fungus among patients with haematological malignencies. Mycoses 2015, 58, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Bonini, A.; Capatti, C.; Parmeggiani, M.; Gugliotta, L.; Micozzi, A.; Gentile, G.; Capria, S.; Girmenia, C. Galactomannan detection in Geotrichum capitatum invasive infections: Report of 2 new cases and review of diagnostic options. Diagn. Microbiol. Infect. Dis. 2008, 62, 450–452. [Google Scholar] [CrossRef] [PubMed]
- Vallabhaneni, S.; Haselow, D.; Lloyd, S.; Lockhart, S.; Moulton-Meissner, H.; Lester, L.; Wheeler, G.; Gladden, L.; Garner, K.; Derado, G.; et al. Cluster of Cryptococcus neoformans Infections in Intensive Care Unit, Arkansas, USA, 2013. Emerg. Infect. Dis. 2015, 21, 1719–1724. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ellis, D.H.; Pfeiffer, T.J. Ecology, life cycle, and infectious propagule of Cryptococcus neoformans. Lancet 1990, 336, 923–925. [Google Scholar] [CrossRef] [PubMed]
- Saha, D.C.; Goldman, D.L.; Shao, X.; Casadevall, A.; Husain, S.; Limaye, A.P.; Lyon, M.; Somani, J.; Pursell, K.; Pruett, T.L.; et al. Serologic evidence for reactivation of cryptococcosis in solid-organ transplant recipients. Clin. Vaccine Immunol. 2007, 14, 1550–1554. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wnamalil, S.S.; Nagdeo, N.N.; Thombare, V.R.; Mathurkar, H. Curvularia A Most Common Missed Occulomycosis in Ocular Trauma. J. Med. Sci. Clin. Res. (JMSCR) 2014, 6, 1344–1348. Available online: https://jmscr.igmpublication.org/v2-i6/12%20jmscr.pdf (accessed on 10 August 2021).
- Ismail, Y.; Johnson, R.H.; Wells, M.V.; Pusavat, J.; Douglas, K.; Arsura, E.L. Invasive sinusitis with intracranial extension caused by Curvularia lunata. Arch. Intern. Med. 1993, 153, 1604–1606. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, M.; Noyola, D.E.; Rossmann, S.N.; Edwards, M.S. Cutaneous phaeohyphomycosis caused by Curvularia lunata and a review of Curvularia infections in pediatrics. Pediatr. Infect. Dis. J. 1999, 18, 727–731. [Google Scholar] [CrossRef] [PubMed]
- Safdar, A. Curvularia--favorable response to oral itraconazole therapy in two patients with locally invasive phaeohyphomycosis. Clin. Microbiol. Infect. 2003, 9, 1219–1223. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi, M.G.; Phillips, P.; Schwartz, J.G.; Winn, R.E.; Holt, G.R.; Shagets, F.W.; Elrod, J.; Nishioka, G.; Aufdemorte, T.B. Human Curvularia infections. Report of five cases and review of the literature. Diagn. Microbiol. Infect. Dis. 1987, 6, 27–39. [Google Scholar] [CrossRef] [PubMed]
- Nucci, M.; Anaissie, E. Fusarium infections in immunocompromised patients. Clin. Microbiol. Rev. 2007, 20, 695–704. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- van Diepeningen, A.D.; Brankovics, B.; Iltes, J.; van der Lee, T.A.; Waalwijk, C. Diagnosis of Fusarium Infections: Approaches to Identification by the Clinical Mycology Laboratory. Curr. Fungal Infect. Rep. 2015, 9, 135–143. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nucci, M.; Anaissie, E. Cutaneous infection by Fusarium species in healthy and immunocompromised hosts: Implications for diagnosis and management. Clin. Infect. Dis. 2002, 35, 909–920. [Google Scholar] [CrossRef] [PubMed]
- Nelson, P.E.; Dignani, M.C.; Anaissie, E.J. Taxonomy, biology, and clinical aspects of Fusarium species. Clin. Microbiol. Rev. 1994, 7, 479–504. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Anaissie, E.J.; Kuchar, R.T.; Rex, J.H.; Francesconi, A.; Kasai, M.; Müller, F.M.; Lozano-Chiu, M.; Summerbell, R.C.; Dignani, M.C.; Chanock, S.J.; et al. Fusariosis associated with pathogenic fusarium species colonization of a hospital water system: A new paradigm for the epidemiology of opportunistic mold infections. Clin. Infect. Dis. 2001, 33, 1871–1878. [Google Scholar] [CrossRef] [PubMed]
- Paula, C.R.; Krebs, V.L.; Auler, M.E.; Ruiz, L.S.; Matsumoto, F.E.; Silva, E.H.; Diniz, E.M.; Vaz, F.A. Nosocomial infection in newborns by Pichia anomala in a Brazilian intensive care unit. Med. Mycol. 2006, 44, 479–484. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Murphy, N.; Buchanan, C.R.; Damjanovic, V.; Whitaker, R.; Hart, C.A.; Cooke, R.W. Infection and colonisation of neonates by Hansenula anomala. Lancet 1986, 1, 291–293. [Google Scholar] [CrossRef] [PubMed]
- Bakir, M.; Cerikcioğlu, N.; Tirtir, A.; Berrak, S.; Ozek, E.; Canpolat, C. Pichia anomala fungaemia in immunocompromised children. Mycoses 2004, 47, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Lunardi, L.W.; Aquino, V.R.; Zimerman, R.A.; Goldani, L.Z. Epidemiology and outcome of Rhodotorula fungemia in a tertiary care hospital. Clin. Infect. Dis. 2006, 43, e60–e63. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wirth, F.; Goldani, L.Z. Epidemiology of Rhodotorula: An emerging pathogen. Interdiscip. Perspect. Infect. Dis. 2012, 2012, 465717. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- De Almeida, G.M.; Costa, S.F.; Melhem, M.; Motta, A.L.; Szeszs, M.W.; Miyashita, F.; Pierrotti, L.C.; Rossi, F.; Burattini, M.N. Rhodotorula spp. isolated from blood cultures: Clinical and microbiological aspects. Med. Mycol. 2008, 46, 547–556. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Pérez-Torrado, R.; Querol, A. Opportunistic Strains of Saccharomyces cerevisiae: A Potential Risk Sold in Food Products. Front. Microbiol. 2016, 6, 1522. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Enache-Angoulvant, A.; Hennequin, C. Invasive Saccharomyces infection: A comprehensive review. Clin. Infect. Dis. 2005, 41, 1559–1568. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, P.; Bouza, E.; Cuenca-Estrella, M.; Eiros, J.M.; Pérez, M.J.; Sánchez-Somolinos, M.; Rincón, C.; Hortal, J.; Peláez, T. Saccharomyces cerevisiae fungemia: An emerging infectious disease. Clin. Infect. Dis. 2005, 40, 1625–1634. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Torrado, R.; Llopis, S.; Jespersen, L.; Fernández-Espinar, T.; Querol, A. Clinical Saccharomyces cerevisiae isolates cannot cross the epithelial barrier in vitro. Int. J. Food Microbiol. 2012, 157, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.J.; Groll, A.; Hiemenz, J.; Fleming, R.; Roilides, E.; Anaissie, E. Infections due to emerging and uncommon medically important fungal pathogens. Clin. Microbiol. Infect. 2004, 10 (Suppl. S1), 48–66. [Google Scholar] [CrossRef] [PubMed]
- Ashley, E.S.D.; Lewis, R.; Lewis, J.S.; Martin, C.; Andes, D. Pharmacology of systemic antifungal agents. Clin. Infect. Dis. 2006, 43, S28–S39. [Google Scholar] [CrossRef]
- Seyedmousavi, S.; Rafati, H.; Ilkit, M.; Tolooe, A.; Hedayati, M.T.; Verweij, P. Systemic Antifungal Agents: Current Status and Projected Future Developments. Methods Mol. Biol. 2017, 1508, 107–139. [Google Scholar] [CrossRef] [PubMed]
- Dismukes, W.E. Introduction to antifungal drugs. Clin. Infect. Dis. 2000, 30, 653–657. [Google Scholar] [CrossRef] [PubMed]
- Sienkiewicz, B.M.; Łapiński, Ł.; Wiela-Hojeńska, A. Comparison of clinical pharmacology of voriconazole and posaconazole. Contemp. Oncol. 2016, 20, 365–373. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Prasad, R.; Shah, A.H.; Rawal, M.K. Antifungals: Mechanism of action and drug resistance. In Yeast Membrane Transporter Advances in Experimental Medicine and Biology; Ramos, J., Sychrová, H., Kschischo, M., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 327–349. [Google Scholar]
- Nett, J.E.; Andes, D.R. Antifungal Agents: Spectrum of Activity, Pharmacology, and Clinical Indications. Infect. Dis. Clin. N. Am. 2016, 30, 51–83. [Google Scholar] [CrossRef] [PubMed]
- Onyewu, C.; Eads, E.; Schell, W.A.; Perfect, J.R.; Ullmann, Y.; Kaufman, G.; Horwitz, B.A.; Berdicevsky, I.; Heitman, J. Targeting the calcineurin pathway enhances ergosterol biosynthesis inhibitors against Trichophyton mentagrophytes in vitro and in a human skin infection model. Antimicrob. Agents Chemother. 2007, 51, 3743–3746. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gamal, A.; Chu, S.; McCormick, T.S.; Borroto-Esoda, K.; Angulo, D.; Ghannoum, M.A. Ibrexafungerp, a Novel Oral Triterpenoid Antifungal in Development: Overview of Antifungal Activity Against Candida glabrata. Front. Cell Infect. Microbiol. 2021, 11, 642358. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ghannoum, M.; Arendrup, M.C.; Chaturvedi, V.P.; Lockhart, S.R.; McCormick, T.S.; Chaturvedi, S.; Berkow, E.L.; Juneja, D.; Tarai, B.; Azie, N.; et al. Ibrexafungerp: A Novel Oral Triterpenoid Antifungal in Development for the Treatment of Candida auris Infections. Antibiotics 2020, 9, 539. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- da Silva Ferreira, M.E.; Capellaro, J.L.; dos Reis Marques, E.; Malavazi, I.; Perlin, D.; Park, S.; Anderson, J.B.; Colombo, A.L.; Arthington-Skaggs, B.A.; Goldman, M.H.; et al. In vitro evolution of itraconazole resistance in Aspergillus fumigatus involves multiple mechanisms of resistance. Antimicrob. Agents Chemother. 2004, 48, 4405–4413. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Coste, A.T.; Karababa, M.; Ischer, F.; Bille, J.; Sanglard, D. TAC1, transcriptional activator of CDR genes, is a new transcription factor involved in the regulation of Candida albicans ABC transporters CDR1 and CDR2. Eukaryot Cell. 2004, 3, 1639–1652. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sanglard, D. Resistance of human fungal pathogens to antifungal drugs. Curr. Opin. Microbiol. 2002, 5, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Marie, C.; White, T.C. Genetic Basis of Antifungal Drug Resistance. Curr. Fungal Infect. Rep. 2009, 3, 163–169. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Noël, T. The cellular and molecular defense mechanisms of the Candida yeasts against azole antifungal drugs. J. Mycol. Med. 2012, 22, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, Y.; Geber, A.; Miyazaki, H.; Falconer, D.; Parkinson, T.; Hitchcock, C.; Grimberg, B.; Nyswaner, K.; Bennett, J.E. Cloning, sequencing, expression and allelic sequence diversity of ERG3 (C-5 sterol desaturase gene) in Candida albicans. Gene 1999, 236, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Kelly, S.L.; Lamb, D.C.; Kelly, D.E.; Manning, N.J.; Loeffler, J.; Hebart, H.; Schumacher, U.; Einsele, H. Resistance to fluconazole and cross-resistance to amphotericin B in Candida albicans from AIDS patients caused by defective sterol delta5,6-desaturation. FEBS Lett. 1997, 400, 80–82. [Google Scholar] [CrossRef] [PubMed]
- Espinel-Ingroff, A. Mechanisms of resistance to antifungal agents: Yeasts and filamentous fungi. Rev. Iberoam. Micol. 2008, 25, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.D.; Lewis, R.E.; Dodds Ashley, E.S.; Ostrosky-Zeichner, L.; Zaoutis, T.; Thompson, G.R.; Andes, D.R.; Walsh, T.J.; Pappas, P.G.; Cornely, O.A.; et al. Core Recommendations for Antifungal Stewardship: A Statement of the Mycoses Study Group Education and Research Consortium. J. Infect. Dis. 2020, 222 (Suppl. S3), S175–S198. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Seebacher, C.; Bouchara, J.P.; Mignon, B. Updates on the epidemiology of dermatophyte infections. Mycopathologia 2008, 166, 335–352. [Google Scholar] [CrossRef] [PubMed]
- Posteraro, B.; Romano, L.; Sanguinetti, M.; Masucci, L.; Morace, G.; Fadda, G. Commercial systems for fluconazole susceptibility testing of yeasts: Comparison with the broth microdilution method. Diagn. Microbiol. Infect. Dis. 2000, 38, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Barry, A.L.; Pfaller, M.A.; Brown, S.D.; Espinel-Ingroff, A.; Ghannoum, M.A.; Knapp, C.; Rennie, R.P.; Rex, J.H.; Rinaldi, M.G. Quality control limits for broth microdilution susceptibility tests of ten antifungal agents. J. Clin. Microbiol. 2000, 38, 3457–3459. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]



{kind=link}
{kind=link}
| Genus | Prevalence (%) | Overall Prevalence (%) | |||
|---|---|---|---|---|---|
| 2017 | 2018 | 2019 | 2020 | ||
| Aspergillus spp. | 00.00 | 03.19 | 03.34 | 03.83 | 02.59 |
| Candida spp. | 99.82 | 96.62 | 94.43 | 91.08 | 95.44 |
| Cryptococcus spp. | 00.00 | 00.00 | 00.16 | 00.18 | 00.09 |
| Curvularia spp. | 00.00 | 00.00 | 00.16 | 00.00 | 00.05 |
| Fusarium spp. | 00.18 | 00.00 | 00.00 | 00.00 | 00.05 |
| Geotrichum spp. | 00.00 | 00.19 | 00.95 | 04.00 | 01.28 |
| Pichia spp. | 00.00 | 00.00 | 00.16 | 00.00 | 00.05 |
| Rhodotorula spp. | 00.00 | 00.00 | 00.16 | 00.00 | 00.05 |
| Saccharomyces spp. | 00.00 | 00.00 | 00.48 | 00.91 | 00.35 |
| Trichoderma spp. | 00.00 | 00.00 | 00.16 | 00.00 | 00.05 |
| Total (%) | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 |
| Species | Prevalence amongst Candida isolates (%) | Overall Prevalence (%) | |||
|---|---|---|---|---|---|
| 2017 | 2018 | 2019 | 2020 | ||
| C. albicans | 74.20 | 69.92 | 65.82 | 63.14 | 68.37 |
| C. dubliniensis | 00.00 | 01.36 | 03.03 | 02.00 | 01.61 |
| C. glabrata | 08.48 | 06.99 | 08.42 | 10.00 | 08.46 |
| C. inconspicua | 00.00 | 00.00 | 00.34 | 01.60 | 00.46 |
| C. kefyr | 00.71 | 01.94 | 02.36 | 06.21 | 02.71 |
| C. krusei | 03.36 | 03.88 | 05.05 | 04.01 | 04.09 |
| C. lusitaniae | 00.18 | 00.19 | 01.01 | 00.80 | 00.55 |
| C. parapsilosis | 01.24 | 02.52 | 03.03 | 03.01 | 02.44 |
| C. tropicalis | 08.30 | 09.71 | 08.42 | 06.02 | 08.14 |
| Others | 03.53 | 03.49 | 02.52 | 03.21 | 03.17 |
| Total (%) | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 |
| Species | 2017 | 2018 | 2019 | 2020 | Overall |
|---|---|---|---|---|---|
| C. albicans | 3 | 4 | 2 | 9 | 18 |
| C. glabrata | 1 | 3 | 3 | 0 | 7 |
| C. parapsilosis | 0 | 1 | 0 | 0 | 1 |
| C. tropicalis | 0 | 1 | 2 | 1 | 4 |
| C. krusei | 0 | 0 | 1 | 0 | 1 |
| C. inconspicua | 0 | 0 | 0 | 2 | 2 |
| C. lusitaniae | 0 | 0 | 1 | 0 | 1 |
| Total cases | 4 | 9 | 9 | 12 | 34 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jain, N.; Jansone, I.; Obidenova, T.; Sīmanis, R.; Meisters, J.; Straupmane, D.; Reinis, A. Epidemiological Characterization of Clinical Fungal Isolates from Pauls Stradinš Clinical University Hospital, Latvia: A 4-Year Surveillance Report. Life 2021, 11, 1002. https://doi.org/10.3390/life11101002
Jain N, Jansone I, Obidenova T, Sīmanis R, Meisters J, Straupmane D, Reinis A. Epidemiological Characterization of Clinical Fungal Isolates from Pauls Stradinš Clinical University Hospital, Latvia: A 4-Year Surveillance Report. Life. 2021; 11(10):1002. https://doi.org/10.3390/life11101002
Chicago/Turabian StyleJain, Nityanand, Inese Jansone, Tatjana Obidenova, Raimonds Sīmanis, Jānis Meisters, Dagnija Straupmane, and Aigars Reinis. 2021. "Epidemiological Characterization of Clinical Fungal Isolates from Pauls Stradinš Clinical University Hospital, Latvia: A 4-Year Surveillance Report" Life 11, no. 10: 1002. https://doi.org/10.3390/life11101002
APA StyleJain, N., Jansone, I., Obidenova, T., Sīmanis, R., Meisters, J., Straupmane, D., & Reinis, A. (2021). Epidemiological Characterization of Clinical Fungal Isolates from Pauls Stradinš Clinical University Hospital, Latvia: A 4-Year Surveillance Report. Life, 11(10), 1002. https://doi.org/10.3390/life11101002