Muscular Strength Imbalances Are not Associated with Skin Temperature Asymmetries in Soccer Players

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
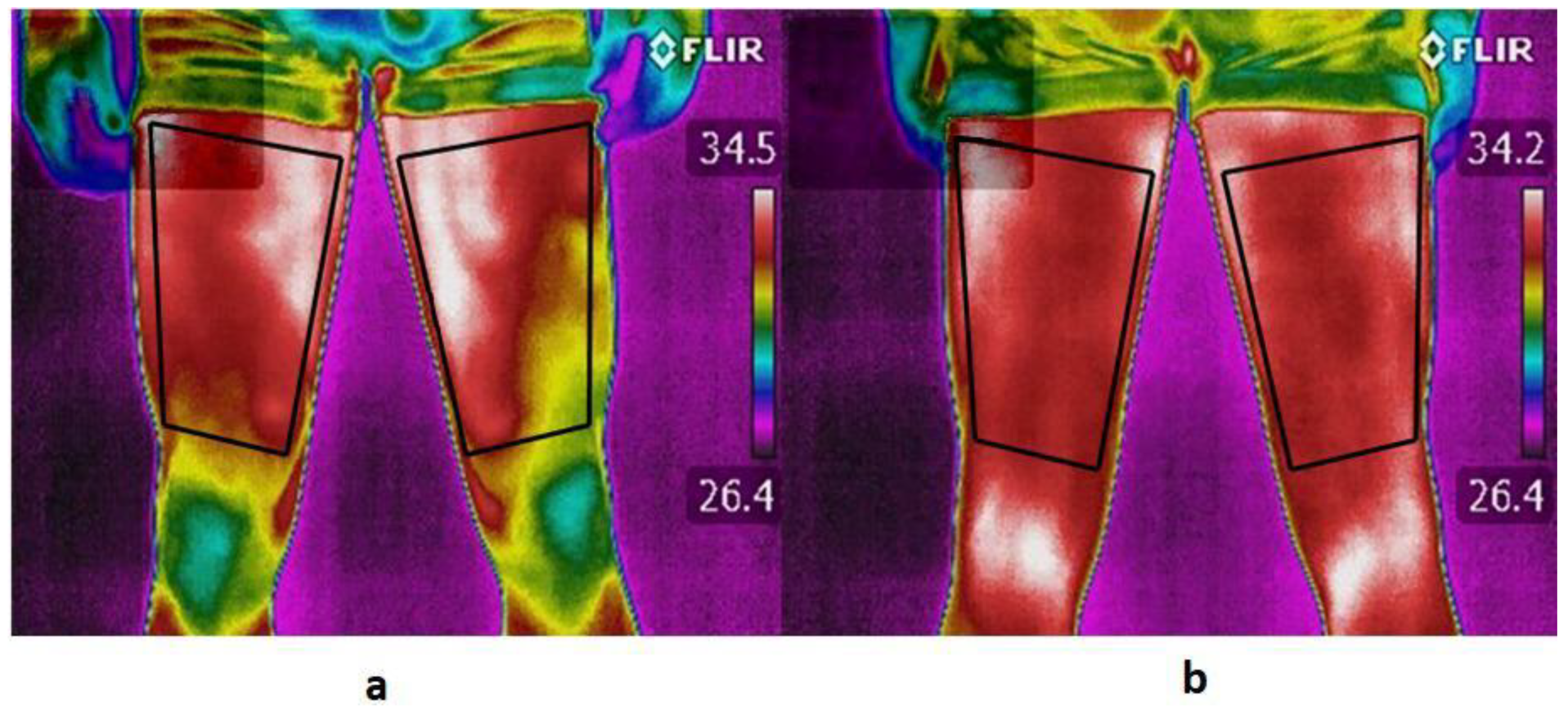
2.2. Thermography Data Collection and Analysis
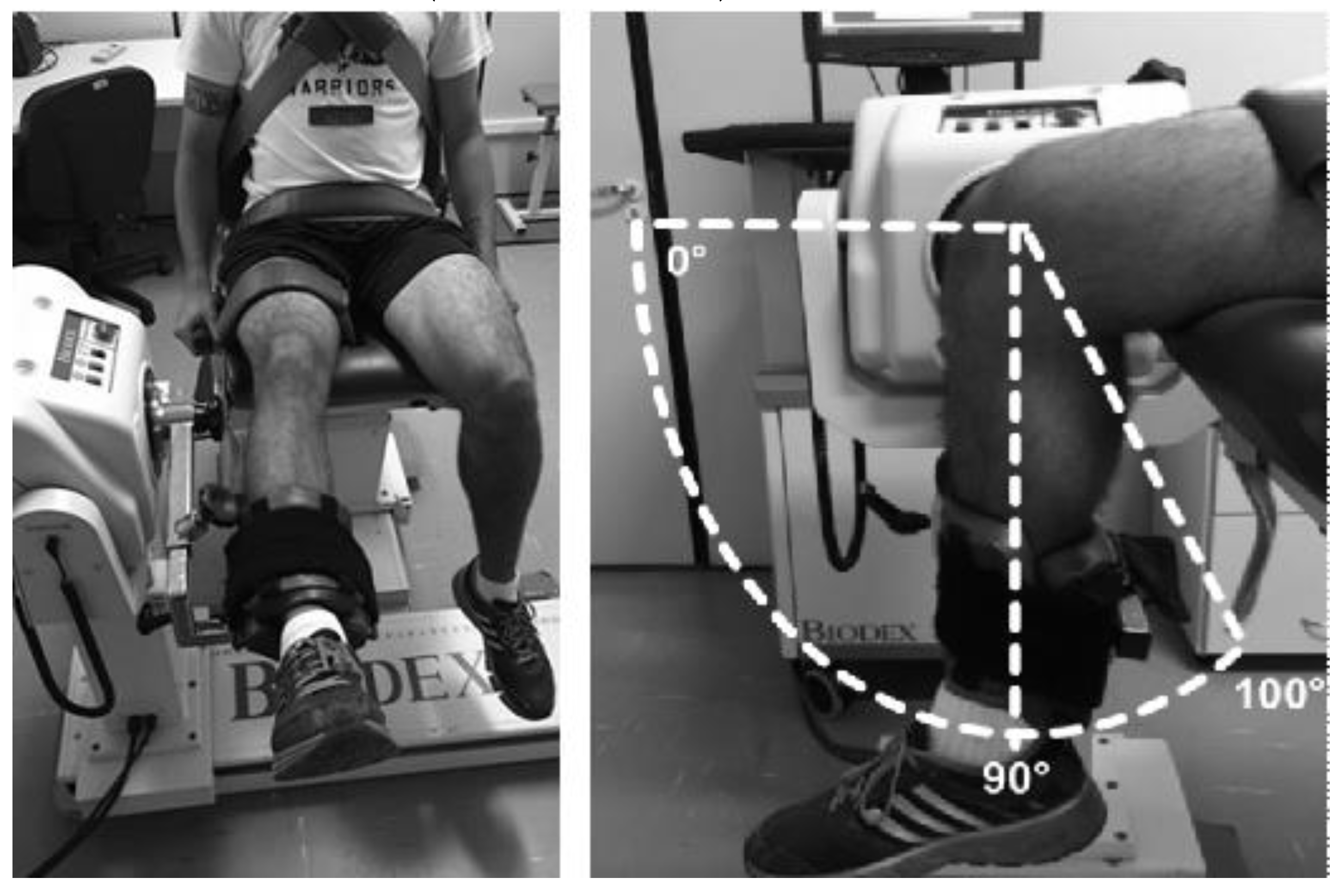
2.3. Isokinetic Data Collection and Analysis
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ekstrand, J.; Hägglund, M.; Waldén, M. Epidemiology of muscle injuries in professional football (soccer). Am. J. Sports Med. 2011, 39, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- Pfirrmann, D.; Herbst, M.; Ingelfinger, P.; Simon, P.; Tug, S. Analysis of injury incidences in male professional adult and elite youth soccer players: A systematic review. J. Athl. Train. 2016, 51, 410–424. [Google Scholar] [CrossRef] [PubMed]
- Fousekis, K.; Tsepis, E.; Vagenas, G. Lower limb strength in professional soccer players: Profile, asymmetry, and training age. J. Sports Sci. Med. 2010, 9, 364–373. [Google Scholar] [PubMed]
- Boccia, G.; Brustio, P.R.; Buttacchio, G.; Calabrese, M.; Bruzzone, M.; Casale, R.; Rainoldi, A. Interlimb asymmetries identified using the rate of torque development in ballistic contraction targeting submaximal torques. Front. Physiol. 2018, 9, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Croisier, J.-L.; Ganteaume, S.; Binet, J.; Genty, M.; Ferret, J.-M. Strength imbalances and prevention of hamstring injury in professional soccer players: A prospective study. Am. J. Sports Med. 2008, 36, 1469–1475. [Google Scholar] [CrossRef] [PubMed]
- Lehance, C.; Binet, J.; Bury, T.; Croisier, J.L. Muscular strength, functional performances and injury risk in professional and junior elite soccer players. Scand. J. Med. Sci. Sports 2009, 19, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro-Alvares, J.B.; Dornelles, M.P.; Fritsch, C.G.; de Lima-e-Silva, F.X.; Medeiros, T.M.; Severo-Silveira, L.; Marques, V.B.; Baroni, B.M. Prevalence of hamstring strain injury risk factors in professional and under-20 male football (soccer) players. J. Sport Rehabil. 2019, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Petersen, J.; Thorborg, K.; Nielsen, M.B.; Budtz-Jørgensen, E.; Hölmich, P. Preventive effect of eccentric training on acute hamstring injuries in men’s soccer. Am. J. Sports Med. 2011, 39, 2296–2303. [Google Scholar] [CrossRef]
- Ekstrand, J.; Hagglund, M.; Walden, M. Injury incidence and injury patterns in professional football: The UEFA injury study. Br. J. Sports Med. 2011, 45, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Anne-Marie van Beijsterveldt, A.M.C.; Stubbe, J.H.; Schmikli, S.L.; Van De Port, I.G.L.; Backx, F.J.G. Differences in injury risk and characteristics between Dutch amateur and professional soccer players. J. Sci. Med. Sport 2015, 18, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Denadai, B.S.; de Oliveira, F.B.D.; de Abreu Camarda, S.R.; Ribeiro, L.; Greco, C.C. Hamstrings-to-quadriceps strength and size ratios of male professional soccer players with muscle imbalance. Clin. Physiol. Funct. Imaging 2016, 36, 159–164. [Google Scholar] [CrossRef]
- Grygorowicz, M.; Kubacki, J.; Pilis, W.; Gieremek, K.; Rzapka, R. Selected isokinetic tests in knee injury prevention. Biol. Sport 2010, 27, 47–51. [Google Scholar] [CrossRef]
- Carpes, F.P.; Mello-Carpes, P.B.; Priego Quesada, J.I.; Pérez-Soriano, P.; Salvador Palmer, R.; Ortiz de Anda, R.M.C. Insights on the use of thermography in human physiology practical classes. Adv. Physiol. Educ. 2018, 42, 521–525. [Google Scholar] [CrossRef]
- Moreira, D.G.; Costello, J.T.; Brito, C.J.; Adamczyk, J.G.; Ammer, K.; Bach, A.J.E.; Costa, C.M.A.; Eglin, C.; Fernandes, A.A.; Fernández-Cuevas, I.; et al. Thermographic imaging in sports and exercise medicine: A Delphi study and consensus statement on the measurement of human skin temperature. J. Therm. Biol. 2017, 69, 155–162. [Google Scholar] [CrossRef]
- Lahiri, B.B.; Bagavathiappan, S.; Jayakumar, T.; Philip, J. Medical applications of infrared thermography: A review. Infrared Phys. Technol. 2012, 55, 221–235. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, A.A.; Dos Santos Amorim, P.R.; Brito, C.J.; De Moura, A.G.; Moreira, D.G.; Costa, C.M.A.; Sillero-Quintana, M.; Marins, J.C.B. Measuring skin temperature before, during and after exercise: A comparison of thermocouples and infrared thermography. Physiol. Meas. 2014, 35, 189–203. [Google Scholar] [CrossRef] [PubMed]
- Hildebrandt, C.; Raschner, C.; Ammer, K. An overview of recent application of medical infrared thermography in sports medicine in Austria. Sensors 2010, 10, 4700–4715. [Google Scholar] [CrossRef]
- Colim, A.; Arezes, P.; Flores, P.; Vardasca, R.; Braga, A.C. Thermographic differences due to dynamic work tasks on individuals with different obesity levels: A preliminary study. Comput. Methods Biomech. Biomed. Eng. Imaging Vis. 2020, 8, 323–333. [Google Scholar] [CrossRef]
- Fernández-Cuevas, I.; Lastras, J.A.; Galindo, V.E.; Carmona, P.G. Infrared thermography for the detection of injury in sports medicine. In Application of Infrared Thermography in Sports Science; Priego Quesada, J.I., Ed.; Biological and Medical Physics, Biomedical Engineering; Springer International Publishing: Cham, Switzerland, 2017; pp. 81–109. ISBN 978-3-319-47409-0. [Google Scholar]
- Vardasca, R.; Ring, E.; Plassmann, P. Thermal symmetry of the upper and lower extremities in healthy subjects. Thermol. Int. 2012, 22, 53–60. [Google Scholar]
- Sanchis-Sánchez, E.; Vergara-Hernández, C.; Cibrián, R.M.; Salvador, R.; Sanchis, E.; Codoñer-Franch, P. Infrared thermal imaging in the diagnosis of musculoskeletal injuries: A systematic review and meta-analysis. Am. J. Roentgenol. 2014, 203, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Côrte, A.C.; Pedrinelli, A.; Marttos, A.; Souza, I.F.G.; Grava, J.; José Hernandez, A. Infrared thermography study as a complementary method of screening and prevention of muscle injuries: Pilot study. BMJ Open Sport Exerc. Med. 2019, 5, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Carmona, P.; Fernández-Cuevas, I.; Sillero-Quintana, M.; Arnaiz-Lastras, J.; Navandar, A. Infrared thermography protocol on reducing the incidence of soccer injuries. J. Sport Rehabil. 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Gatt, A.; Formosa, C.; Cassar, K.; Camilleri, K.P.; De Raffaele, C.; Mizzi, A.; Azzopardi, C.; Mizzi, S.; Falzon, O.; Cristina, S.; et al. Thermographic patterns of the upper and lower limbs: Baseline data. Int. J. Vasc. Med. 2015, 2015, 1–9. [Google Scholar] [CrossRef]
- van Melick, N.; Meddeler, B.M.; Hoogeboom, T.J.; Nijhuis-van der Sanden, M.W.G.; van Cingel, R.E.H. How to determine leg dominance: The agreement between self-reported and observed performance in healthy adults. PLoS ONE 2017, 12. [Google Scholar] [CrossRef]
- Priego Quesada, J.I.; Lucas-Cuevas, A.G.; Salvador Palmer, R.; Pérez-Soriano, P.; Cibrián Ortiz de Anda, R.M. Definition of the thermographic regions of interest in cycling by using a factor analysis. Infrared Phys. Technol. 2016, 75, 180–186. [Google Scholar] [CrossRef]
- Marins, J.C.B.; Moreira, D.G.; Cano, S.P.; Quintana, M.S.; Soares, D.D.; de Andrade Fernandes, A.; da Silva, F.S.; Costa, C.M.A.; dos Santos Amorim, P.R. Time required to stabilize thermographic images at rest. Infrared Phys. Technol. 2014, 65, 30–35. [Google Scholar] [CrossRef]
- Priego Quesada, J.I.; Kunzler, M.R.; Carpes, F.P. Methodological aspects of infrared thermography in human assessment. In Application of Infrared Thermography in Sports Science; Springer International Publishing: Cham, Switzerland, 2017; pp. 49–79. ISBN 978-3-319-47410-6. [Google Scholar]
- Steketee, J. Spectral emissivity of skin and pericardium. Phys. Med. Biol. 1973, 18, 307. [Google Scholar] [CrossRef] [PubMed]
- Chavet, P.; Lafortune, M.; Gray, J.R. Asymmetry of lower extremity responses to external impact loading. Hum. Mov. Sci. 1997, 16, 391–406. [Google Scholar] [CrossRef]
- Ruas, C.V.; Minozzo, F.; Pinto, M.D.; Brown, L.E.; Pinto, R.S. Lower-extremity strength ratios of professional soccer players according to field position. J. Strength Cond. Res. 2015, 29, 1220–1226. [Google Scholar] [CrossRef]
- Nunes, R.F.H.; Dellagrana, R.A.; Nakamura, F.Y.; Buzzachera, C.F.; Almeida, F.A.M.; Flores, L.J.F.; Guglielmo, L.G.A.; da Silva, S.G. Isokinetic assessment of muscular strength and balance in brazilian elite futsal players. Int. J. Sports Phys. Ther. 2018, 13, 94–103. [Google Scholar] [CrossRef]
- Ekstrand, J.; Healy, J.C.; Waldén, M.; Lee, J.C.; English, B.; Hägglund, M. Hamstring muscle injuries in professional football: The correlation of MRI findings with return to play. Br. J. Sports Med. 2012, 46, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Aicale, R.; Tarantino, D.; Maffulli, N. Overuse injuries in sport: A comprehensive overview. J. Orthop. Surg. 2018, 13, 309. [Google Scholar] [CrossRef] [PubMed]
- Garrett, W.E. Muscle strain injuries: Clinical and basic aspects. Med. Sci. Sports Exerc. 1990, 22, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.Y.; Mok, K.-M.; Chan, H.C.K.; Yung, P.S.H.; Chan, K.-M. Eccentric hamstring strength deficit and poor hamstring-to-quadriceps ratio are risk factors for hamstring strain injury in football: A prospective study of 146 professional players. J. Sci. Med. Sport 2018, 21, 789–793. [Google Scholar] [CrossRef]
- Shadle, I.B.; Cacolice, P.A. Eccentric exercises reduce hamstring strains in elite adult male soccer players: A critically appraised topic. J. Sport Rehabil. 2016, 26, 573–577. [Google Scholar] [CrossRef]
- Van Der Horst, N.; Smits, D.W.; Petersen, J.; Goedhart, E.A.; Backx, F.J.G. The preventive effect of the nordic hamstring exercise on hamstring injuries in amateur soccer players: A randomized controlled trial. Am. J. Sports Med. 2015, 43, 1316–1323. [Google Scholar] [CrossRef]
- Bouzas Marins, J.C.; de Andrade Fernandes, A.; Gomes Moreira, D.; Souza Silva, F.; Costa, C.M.A.; Pimenta, E.M.; Sillero-Quintana, M. Thermographic profile of soccer players’ lower limbs. Rev. Andal. Med. Deporte 2014, 7, 1–6. [Google Scholar] [CrossRef]
- Arfaoui, A.; Bertucci, W.; Letellier, T.; Polidori, G. Thermoregulation during incremental exercise in masters cycling. J. Sci. Cycl. 2014, 3, 33–41. [Google Scholar]
- Trecroci, A.; Formenti, D.; Ludwig, N.; Gargano, M.; Bosio, A.; Rampinini, E.; Alberti, G. Bilateral asymmetry of skin temperature is not related to bilateral asymmetry of crank torque during an incremental cycling exercise to exhaustion. PeerJ 2018, 6, e4438. [Google Scholar] [CrossRef]
- Chudecka, M.; Lubkowska, A. Thermal maps of young women and men. Infrared Phys. Technol. 2015, 69, 81–87. [Google Scholar] [CrossRef]
- Herborn, K.A.; Graves, J.L.; Jerem, P.; Evans, N.P.; Nager, R.; McCafferty, D.J.; McKeegan, D.E.F. Skin temperature reveals the intensity of acute stress. Physiol. Behav. 2015, 152, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Priego-Quesada, J.I.; Pérez-Guarner, A.; Gandia-Soriano, A.; Oficial-Casado, F.; Galindo, C.; Anda, R.M.C.O.D.; Piñeiro-Ramos, J.D.; Sánchez-Illana, Á.; Kuligowski, J.; Barbosa, M.A.G.; et al. Effect of a marathon on skin temperature response after a cold-stress test and its relationship with perceptive, performance, and oxidative-stress biomarkers. Int. J. Sports Physiol. Perform. 2020, 1, 1–9. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Isokinetic Variables | PL (N.m) | NPL (N.m) | AI (%) | p |
|---|---|---|---|---|
| Quadriceps | ||||
| 60°/s Conc. | 206 ± 36 | 196 ± 36 | 3.99 ± 13.7 | 0.15 |
| 240°/s Conc. | 127 ± 21 | 128 ± 26 | −1.04 ± 18.0 | 0.93 |
| Hamstrings | ||||
| 30°/s Ecc. | 172 ± 31 | 160 ± 31 | 6.62 ± 14.3 | 0.03 * |
| 60°/s Con. | 115 ± 23 | 114 ± 28 | 0.81 ± 26.1 | 0.85 |
| 120°/s Ecc. | 173 ± 33 | 162 ± 27 | 4.66 ± 15.5 | 0.04 * |
| 240°/s Con. | 84 ± 15 | 78 ± 14 | 6.77 ± 11.7 | 0.02 * |
| H/Q Ratio | ||||
| Conc/Conc 60°/s | 0.56 ± 0.09 | 0.59 ± 0.16 | - | 0.22 |
| Conc/Conc 240°/s | 0.66 ± 0.08 | 0.62 ± 0.09 | - | 0.006 * |
| Ecc30°/s/Conc240°/s | 1.37 ± 0.24 | 1.27 ± 0.24 | - | 0.03 * |
| Variables | Imbalance Risk | PL (°C) | NPL (°C) | F 1 | p |
|---|---|---|---|---|---|
| Quadriceps | High | 32.51 ± 0.81 | 32.49 ± 0.76 | 0.002 | 0.964 |
| Low | 32.38 ± 0.82 | 32.37 ± 0.79 | |||
| Hamstrings | High | 32.32 ± 0.77 | 32.35 ± 0.75 | 0.002 | 0.962 |
| Low | 32.29 ± 0.68 | 32.30 ± 0.69 | |||
| ∆Temp (H-Q) | High | −0.19 ± 0.51 | −0.13 ± 0.49 | 0.022 | 0.882 |
| Low | −0.10 ± 0.46 | −0.07 ± 0.43 |
| Variables | Rate of Players (%) |
|---|---|
| Bilateral Difference | |
| Conc 60°/s | 14/59 (23.7) |
| Conc 240°/s | 6/59 (10.2) |
| Ecc 30°/s | 18/59 (30.5) |
| Ecc 120°/s | 13/59 (22.0) |
| ∆ Temp. (Quadriceps PL–Quadriceps NPL) | 2/59 (3.9) |
| ∆ Temp. (Hamstring PL–Hamstring NPL) | 0/59 (0.0) |
| Preferred Limb | |
| Conc 60°/s/Conc 60°/s | 5/59 (8.5) |
| Conc 240°/s/Conc 240°/s | 0/59 (0.0) |
| Mixed Ecc 30°/s/Conc2 40°/s | 1/59 (1.7) |
| ∆Temp. (Hamstrings–Quadriceps) | 17/59 (28.8) |
| Non-preferred Limb | |
| Conc 60°/s/Conc 60°/s | 6/59 (10.2) |
| Conc 240°/s/Conc 240°/s | 2/59 (3.4) |
| Mixed Ecc3 0°/s/Conc 240°/s | 4/59 (6.8) |
| ∆ Temp. (Hamstrings–Quadriceps) | 26/59 (44.1) |
| Injury Criteria | |
| Deficiency at least 2 parameters | 22/59 (37.3) |
| Total difference of temperature | 31/59 (52.5) |
| Frequency Analysis | Overall |
|---|---|
| Strength imbalance (%) | 37.3 |
| Skin temperature imbalance (%) | 52.5 |
| Difference (%) | 15.2 |
| Sensitivity (%) | 22.0 |
| Specificity (%) | 32.2 |
| Negative-false (%) | 15.3 |
| Positive-false (%) | 30.5 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendonça Teixeira, R.; Dellagrana, R.A.; Priego-Quesada, J.I.; Machado, J.C.B.P.; Fernandes da Silva, J.; Pacheco dos Reis, T.M.; Rossato, M. Muscular Strength Imbalances Are not Associated with Skin Temperature Asymmetries in Soccer Players. Life 2020, 10, 102. https://doi.org/10.3390/life10070102
Mendonça Teixeira R, Dellagrana RA, Priego-Quesada JI, Machado JCBP, Fernandes da Silva J, Pacheco dos Reis TM, Rossato M. Muscular Strength Imbalances Are not Associated with Skin Temperature Asymmetries in Soccer Players. Life. 2020; 10(7):102. https://doi.org/10.3390/life10070102
Chicago/Turabian StyleMendonça Teixeira, Rodrigo, Rodolfo A. Dellagrana, Jose I. Priego-Quesada, João Claudio B.P. Machado, Juliano Fernandes da Silva, Tallyne Mayara Pacheco dos Reis, and Mateus Rossato. 2020. "Muscular Strength Imbalances Are not Associated with Skin Temperature Asymmetries in Soccer Players" Life 10, no. 7: 102. https://doi.org/10.3390/life10070102
APA StyleMendonça Teixeira, R., Dellagrana, R. A., Priego-Quesada, J. I., Machado, J. C. B. P., Fernandes da Silva, J., Pacheco dos Reis, T. M., & Rossato, M. (2020). Muscular Strength Imbalances Are not Associated with Skin Temperature Asymmetries in Soccer Players. Life, 10(7), 102. https://doi.org/10.3390/life10070102