
An Intravascular Catheter Bending Recognition Method for Interventional Surgical Robots

Abstract
:1. Introduction
2. Principle and Simulation
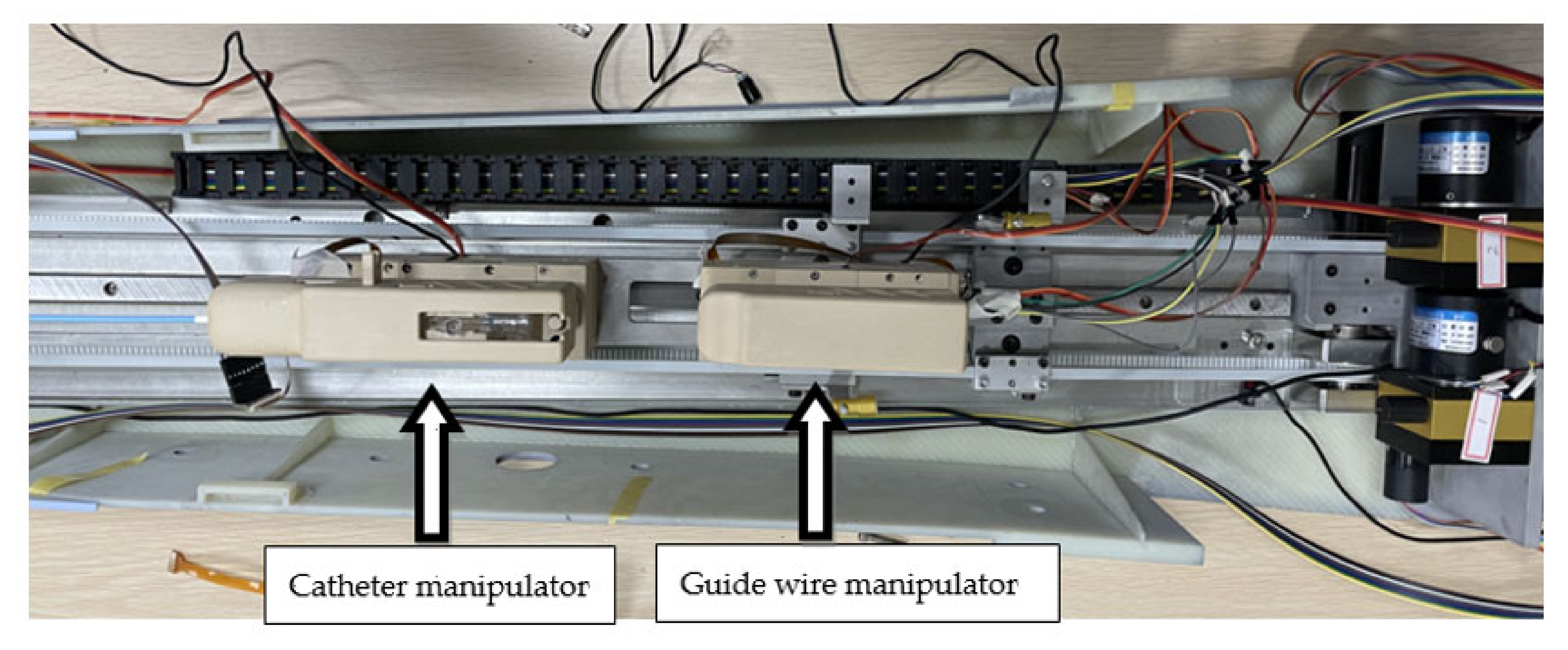
2.1. Overview of the Surgical Robot System
2.2. Catheter Motion Simulation
2.3. Pasting of Strain Gauges
2.4. The BP Neural Network
- (1)
- Determine the number of nodes in each layer, determine the initial value of the weighting coefficient and and select the learning rate .
- (2)
- Sample to obtain and ; calculate the error at this moment ().
- (3)
- Calculate the input and output of each layer of the neural network.
- (4)
- Adjust the weighting coefficients and through the gradient descent method to achieve parameter adjustment.
- (5)
- Let ; return to step (1).
3. Experiments and Results
3.1. Experiment Procedure
3.2. Training and Results
3.3. Optimization of Neural Network
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lloyd-Jones, D.; Adams, R.J.; Brown, T.M.; Carnethon, M.; Dai, S.; De Simone, G.; Ferguson, T.B.; Ford, E.; Furie, K.; Gillespie, C. Heart Disease and Stroke Statistics—2010 Update: A Report from the American Heart Association. Circulation 2010, 121, 948–954. [Google Scholar] [PubMed]
- Guo, J.; Shao, L.; Guo, S.; Yu, Y.; Gao, Q. A multidimensional information monitoring method for a novel robotic vascular interventional system. In Proceedings of the IEEE International Conference on Information and Automation, Lijiang, China, 1 October 2015; pp. 609–613. [Google Scholar]
- Kim, K.P.; Miller, D.L.; De Gonzalez, A.B.; Balter, S.; Kleinerman, R.A.; Ostroumova, E.; Simon, S.L.; Linet, M.S. Occupational radiation doses to operators performing fluoroscopically-guided procedures. Health Phys. 2012, 103, 80–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daneshmand, M.; Bilici, O.; Bolotnikova, A.; Anbarjafari, G. Medical robots with potential applications in participatory and opportunistic remote sensing: A review. Robot Auton. Syst. 2017, 95, 160–180. [Google Scholar] [CrossRef]
- Faddis, M.N.; Blume, W.; Finney, J.; Hall, A.; Rauch, J.; Sell, J.; Bae, K.T.; Talcott, M.; Lindsay, B. Novel, magnetically guided catheter for endocardial mapping and radiofrequency catheter ablation. Circulation 2002, 106, 2980–2985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrozza, J.P. Robotic-Assisted Percutaneous Coronary Intervention—Filling an Unmet Need. J. Cardiovasc. Transl. Res. 2012, 5, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Khan, E.M.; Frumkin, W.; Ng, G.A.; Neelagaru, S.; Abi-Samra, F.M.; Lee, J.; Giudici, M.; Gohn, D.; Winkle, R.A.; Sussman, J.; et al. First experience with a novel robotic remote catheter system: Amigo™ mapping trial. J. Interv. Card. Electrophysiol. 2013, 37, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Guo, S.; Tamiya, T.; Hirata, H.; Ishihara, H. A Virtual Reality-based Method of Decreasing Transmission Time of Visual Feedback for A Tele-operative Robotic Catheter Operating System. Int. J. Med. Robot. Comput. Assist. Surg. 2016, 12, 32–45. [Google Scholar] [CrossRef] [PubMed]
- Yogesh, T.; Jeffrey, S.; David, W.; Maria, D. Design and Performance Evaluation of a Remote Catheter Navigation System. IEEE Trans. Biomed. Eng. 2009, 56, 1901–1908. [Google Scholar]
- Ma, X.; Guo, S.; Xiao, N.; Yoshida, S.; Tamiya, T. Evaluating Performance of a Novel Developed Robotic Catheter Manipulating System. J. Micro Bio Robot. 2013, 8, 133–143. [Google Scholar] [CrossRef]
- Jian, G.; Xiaoliang, J.; Shuxiang, G. Study of the Operational Safety of a Vascular Interventional Surgical Robotic System. Micromachines 2018, 9, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bao, X.; Guo, S.; Xiao, N.; Li, Y.; Shi, L. Compensatory Force Measurement and Multimodal Force Feedback for Remote-controlled Vascular Interventional Robot. Biomed. Microdevices 2018, 20, 74.1–74.11. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Guo, S.; Bao, X.; Xiao, N.; Shi, L.; Li, Y.; Jiang, Y. A Vascular Interventional Surgical Robot Based on Surgeon’s Operating Skills. Med. Biol. Eng. Comput. 2019, 57, 1999–2010. [Google Scholar] [CrossRef] [PubMed]
- Shuxiang, G.; Wang, Y.; Nan, X.; Youxiang, L.; Yuhua, J. Study on Real-time Force Feedback for A Master-salve Interventional Surgical Robotic System. Biomed. Microdevices 2018, 20, 37. [Google Scholar] [CrossRef]
- Payne, C.J.; Rafii-Tari, H.; Yang, G.Z. A Force Feedback System for Endovascular Catheterization. In Proceedings of the IEEE/RSJ International Conference on Intelligent Robots & Systems, Vilamoura, Portugal, 7 October 2012; pp. 1298–1304. [Google Scholar]
- Zhou, J.; Mei, Z.; Miao, J.; Mao, J.; Wang, L.; Wu, D.; Sun, D.; Zhao, Y. A Remote-Controlled Robotic System with Safety Protection Strategy Based on Force-Sensing and Bending Feedback for Transcatheter Arterial Chemoembolization. Micromachines 2020, 11, 805. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Wang, H.; Chang, J.; Niu, J.; Wang, F.; Yan, Y.; Tian, H.; Fang, J.; Lu, H. A Novel Vascular Intervention Surgical Robot Based on Force Feedback and Flexible Clamping. Appl. Sci. 2021, 11, 611. [Google Scholar] [CrossRef]
- Zhang, L.; Gu, S.; Guo, S.; Tamiya, T. A Magnetorheological Fluids-Based Robot-Assisted Catheter/Guidewire Surgery System for Endovascular Catheterization. Micromachines 2021, 12, 640. [Google Scholar] [CrossRef] [PubMed]
- Pang, C.; Lee, G.Y.; Kim, T.I.; Kim, S.M.; Kim, H.N.; Ahn, S.H.; Suh, K.Y. A Flexible and Highly Sensitive Strain-gauge Sensor using Reversible Interlocking of Nanofibers. Nat. Mater. 2012, 11, 795–801. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, B.H.M. A BP-neural Network Predictor Model for Plastic Injection Molding Process. J. Mater. Processing Technol. 2000, 103, 411–416. [Google Scholar] [CrossRef]
- Zhizhong, Z.; Haiping, X.; Yaqiong, R.; Xuesong, G. Application and Comparison of BP Neural Network Algorithm in MATLAB. In Proceedings of the International Conference on Measuring Technology & Mechatronics Automation, Changsha, China, 13–14 March 2010; pp. 590–593. [Google Scholar]
- Shifei, D.; Su, C.; Yu, J. An Optimizing BP Neural Network Algorithm Based on Genetic Algorithm. Artif. Intell. Rev. 2011, 36, 153–162. [Google Scholar]























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Product Model | ZNLBS-IIX |
|---|---|
| Detection range | 0–5 N |
| Accuracy | 0.1% F.S |
| Resolution | 0.1% F.S |
| Zero output | ±1% F.S |
| Sensitivity | 1.5 mV/V |
| Parameters | Value |
|---|---|
| Length | 80 cm |
| External diameter | 2.7 mm |
| Internal diameter | 2.2 mm |
| Elastic modulus | 6,000,000 N/m2 |
| Middle Poisson’s ratio | 0.47 |
| Mass density | 1290 kg/m3 |
| Tensile strength | 13,000,000 N/m2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wei, W.; Yang, D.; Li, L.; Xia, Y. An Intravascular Catheter Bending Recognition Method for Interventional Surgical Robots. Machines 2022, 10, 42. https://doi.org/10.3390/machines10010042
Wei W, Yang D, Li L, Xia Y. An Intravascular Catheter Bending Recognition Method for Interventional Surgical Robots. Machines. 2022; 10(1):42. https://doi.org/10.3390/machines10010042
Chicago/Turabian StyleWei, Wei, Dong Yang, Li Li, and Yuxuan Xia. 2022. "An Intravascular Catheter Bending Recognition Method for Interventional Surgical Robots" Machines 10, no. 1: 42. https://doi.org/10.3390/machines10010042
APA StyleWei, W., Yang, D., Li, L., & Xia, Y. (2022). An Intravascular Catheter Bending Recognition Method for Interventional Surgical Robots. Machines, 10(1), 42. https://doi.org/10.3390/machines10010042