Abstract
Background: Vibratory massage is now widely used to alleviate muscle fatigue. The effects of different vibration massage intensities on left and right upper trapezius (UT) fatigue have not been examined. Therefore, the present study first examined whether a vibration massage intervention had an effect on UT muscles and second compared the effects of 2 different levels (36 Hz and 46 Hz) of vibratory massage on the right and left oblique muscles under 3 different fatigue conditions. Methods: A total of 23 participants (12 female, 11 male; age: 26.5 ± 3.9 year, height: 170.5 ± 1.6 cm, mass: 57.5 ± 1.5 kg, BMI: 24.3 ± 1.6 kg/m2) were randomly divided into intervention and control groups. The 2 groups of subjects completed isometric contraction fatigue tasks of 30 s of fatigue, 60 s of fatigue and 90 s of fatigue in turn. The specific task of isotonic contraction was performed by subjects holding a 1 kg dumbbell in each hand and performing a straight arm weighted lateral supination exercise. After each exercise, the intervention group was randomized to apply a massage device with a vibration intensity of 36 Hz or 46 Hz on the left and right UT muscles for 5 min each. The control group did not receive any treatment. Both groups then repeated the same fatigue task as before. Then, the effects of different vibration massage interventions on UT muscles were derived by analyzing the changes in maximal voluntary contraction percentage (MVC%) of surface electromyography (sEMG) signals before and after the intervention, and the most effective vibration massage program for relieving left and right UT fatigue was summarized. Then, four classification algorithms were used to label and classify the collected sEMG data, and finally a UT muscle fatigue identification and vibration massage model was constructed. Results: After using the vibration massage level 1 (36 Hz) intervention, the MVC% of the right UT muscle showed significant reductions in the 30 s fatigue task, the 60 s fatigue task and the 90 s fatigue task (R1: p = 0.022, R2: p = 0.005, R3: p = 0.049). After using the vibration massage level 3 (46 Hz) intervention, the MVC% of the right UT muscle showed a significant decrease in both the 60 s fatigue task and the 90 s fatigue task (R2: p = 0.033, R3: p = 0.028). Significant decreases in MVC% for the left UT muscle were found only in the 90 s fatigue task (L3: p = 0.040). Then, by comparing the different performances of four commonly used classification algorithms, it was found that the bagging (accuracy = 0.860) algorithm had higher accuracy. Therefore, the bagging algorithm was used for the UT fatigue identification and vibration massage models. Conclusions: This was the first study to show the impacts of different levels of vibration massage on fatigue alleviation in the left and right UT muscles. Furthermore, the bilateral UT fatigue identification and vibration massage model developed in this study can help people to choose the most appropriate massage protocol for quick relief and relaxation of the UT muscles under three different fatigue tasks.
1. Introduction
Numerous studies have found that many workplaces require employees to repeatedly perform a task in order to improve efficiency. A high repetition of movements over a long period of time may result in an increased biomechanical load on specific muscle tissues, resulting in severe muscle fatigue [1,2]. Muscle fatigue is considered to have a significant role in the onset of work-related musculoskeletal diseases (WMSD) [3,4]. All musculoskeletal discomfort, tingling, muscular weakness, and numbness induced or aggravated by work and the environment in which it is conducted is referred to as WMSD. According to one report, 64% of people in Europe still perform repetitive manual work [5]. In India [6], long-time employees of intensive handicrafts operations also suffer from musculoskeletal disorders due to the repetition of simple tasks. This shows that WMSD is still a growing and significant social problem.
The surface electromyography signal (sEMG) is the combined effect of the superposition of the superficial muscle motor unit action potential (MUAP) in time and space and the electrical activity on the nerve trunk on the skin surface, which can respond to a certain extent to the level and function of muscle activity. Therefore, sEMG is commonly used to detect changes in muscle activity, and the extracted eigenvalues can be further analyzed to determine whether muscle fatigue has occurred. For example, Luger et al. [7] studied shoulder muscle fatigue during categorization work using sEMG. Motabar et al. [8] investigated the strength, endurance, and fatigue response of the shoulder girdle at various load levels using sEMG. Sarker et al. [9] used sEMG to study the effects of varied rest times on cervical muscular fatigue. Aside from the research listed above, there are other studies related to the use of sEMG data to evaluate muscle fatigue. Meanwhile, it can be seen that the upper limb shoulder and neck muscles are involved in activities such as assembly or manual handling, including repetitive movements [10], raised arm postures [11], restricted workstations, and prolonged persistent muscle contraction [12], all of which are risk factors for shoulder muscle fatigue. Keir et al. [13] specifically mentioned that repetitive upper-limb grip tasks may cause fatigue in the obliques, deltoids, and lower erector spinal muscles. Lee et al. [14] demonstrated that repetitive hand transfer work was more relevant to muscle fatigue in the trapezius and anterior deltoid muscles than in other upper limb muscles. Furthermore, some studies [15,16,17,18,19] have found that repetitive manipulative tasks in upper limbs muscles have a greater impact on the trapezius muscle, which is prone to muscle fatigue. As a result, it is critical to provide timely and effective interventions to alleviate trapezius fatigue during repetitive upper-limb work.
Researchers have advocated a number of physical therapies to prevent and relieve muscular tiredness, including stretching, cooling, and traditional massage. Among these physical interventions, Mika et al. [20] suggest that stretching can reduce muscle fatigue but can also have some negative effects, such as the nonuniform overstretching of some sarcomeres, leading to muscle injury. Some authors [21,22] have reported that cooling therapy has a positive effect on muscle recovery but may delay the healing effect due to the freezing effect. Traditional massage is a widely used intervention for the relief of muscle fatigue and muscle soreness. However, this method requires a professional massage therapist to spend a long time performing it.
Vibratory massage is now a more convenient and timely intervention than traditional massage methods [23]. It accelerates post-exercise muscle recovery by enhancing nutrient exchange and boosting the efficiency of perimuscular capillary and fluid cell feeding [24,25,26]. In addition, the heat generated in the muscle fibers as a consequence of the vibration massage enhances the healing response of muscles damaged during fatigue [27]. In recent years, many scholars have explored the effects of vibration massage on muscles. Chu et al. [28] observed that vibration massage had a direct effect on muscle fatigue in the erector spinae after strenuous exercise. Lurie et al. [29] tested the effects of vibration massage on the back muscles, which showed statistically significant differences in subjective scores before and after vibration massage. The findings of a study by Koumantakis et al. [30] indicate that muscle flexibility was positively influenced immediately after vibration massage or light hand massage. Based on the above studies, it can be seen that the studies on the effects of vibration massage on muscle fatigue are mainly focused on forearm muscles, lower limb muscles, and lower back muscles. There are fewer studies on the effects of vibration massage on other muscles [31]. The UT muscles are the muscle areas where fatigue often occurs in our daily work. Meanwhile, UT muscle fatigue is considered to be a serious risk factor for WMSD of the shoulder joint [32]. Studies have shown that the UT muscle of the neck is easily overworked during some upper extremity muscle activities, and if left untreated and unmitigated, it is likely to develop into a serious musculoskeletal disorder [17,18]. Many neck vibration massage products have now been produced for the relief of UT muscle fatigue. However, no studies have been conducted to determine whether vibration massage is truly physiologically effective in relieving fatigue in the UT muscles based on objective data. Moreover, the habitual use of the hands in some tasks is likely to lead to asymmetry in the activity or fatigue levels in the left and right UT muscles. Therefore, when using these vibration massage products, the use of incorrect vibration massage intensity for the UT muscles of the neck may further aggravate muscle fatigue and muscle damage.
The purpose of this study was to test whether different levels of vibration massage have significant effects on the left and right UT muscles by means of objective physiological signals surface electromyography, to find the best vibration massage relief solution through data analysis, and finally construct a bilateral UT fatigue identification and vibration massage model. For this article, we proposed 2 hypotheses:
Hypothesis 1:
Vibratory massage is effective in relieving UT muscle fatigue.
Hypothesis 2:
The effect of vibration massage at the same intensity on both sides of the UT muscle is asymmetrical.
2. Materials and Methods
2.1. Participants
We used the paired test method in the PASS sample size software (v15.0.5, NCSS, LLC., Atlanta, GA, USA) to first calculate the differences in RMS values before and after the intervention in the a priori sample, and then calculate the mean ± standard deviation of the RMS differences; then, we input these data into the software to calculate the required sample size for the experiment. The mean ± standard deviation of the difference in RMS values before and after the intervention was 36.07 ± 27.48 mv (the criteria were as follows: alpha level = 0.05, power = 0.90, f effect size = 0.25). Based on this procedure, the estimated number of subjects was thirteen. Therefore, to fulfil this condition, 23 healthy individuals (12 female, 11 male; age: 26.5 ± 3.9 year, height: 170.5 ± 1.6 cm, mass: 57.5 ± 1.5 kg, BMI: 24.3 ± 1.6 kg/m2) were recruited to participate in this experiment. They were randomized into two groups: thirteen participants in the intervention group and ten participants in the control group, receiving no treatment. Healthy individuals were defined as those who had a regular lifestyle, could move their shoulder and neck muscles normally, could participate in regular shoulder and neck exercises, and had no history of shoulder or neck pain. Subjects with a history of previous shoulder or neck pain, shoulder and neck muscle surgery, or any chronic musculoskeletal disorder related to the shoulder and neck (e.g., cervical spondylosis, cervical muscle strain, cervical myofascial inflammation, cervical fracture, or cervical disc herniation) were excluded from this trial. These volunteers were current postgraduate students, and they all had the right arm as their dominant hand. All the participants were told of the study’s objective, methodology, and potential hazards before submitting verbal and written informed consent. Additionally, to ensure that the experiment was carried out properly, the participants were instructed to avoid any rigorous exercise 48 h before the experiment, especially over-activity of the shoulder and neck muscles. All experimental procedures in this study were in accordance with the Declaration of Helsinki and were approved by the Ethics Review Committee for Scientific and Technological Research Involving Human Beings of Shanghai Jiao Tong University (approval number: I2022241I-R1).
2.2. Apparatus
A wireless sEMG sensor system was used to acquire experimental data for this investigation (Noraxon Inc., Scottsdale, AZ, USA). This system is a wireless multimodal device that provides high-fidelity data and a variety of measuring possibilities. These sensors sample at a rate of up to 4000 times per second, synchronize in real time, and have low baseline noise (one volt RMS) and minimal natural artifacts [33,34]. The Rongtai G10 vibrating massager was employed in our study (Shanghai Rongtai Health Technology Co., Ltd., Shanghai, China). The vibrating massage device has 3 different levels of vibration intensity: level 1 at 36 Hz, level 2 at 41 Hz, and level 3 at 46 Hz. However, because the massage impact of levels 2 and 3 was equivalent in the pre-test, level 1 or level 3 was chosen for muscle relaxation vibration massage in this experiment.
2.3. Experimental Design and Procedure
The experimental intervention group was set at 2 different vibration massage intensities, namely, level 1 at 36 Hz and level 3 at 46 Hz [35]. The control group did not receive any treatment. The experimental variable was the duration of the UT muscle isotonic contraction. For the setting of the fatigue task, we referred to a related report [36] that suggested that at least 30 s was required to obtain a subjective workload. Therefore, our specific task settings were as follows: UT muscle isotonic contraction for 30 s fatigue task, UT muscle isotonic contraction for 60 s fatigue task and UT muscle isotonic contraction for 90 s fatigue task [37].
Prior to the start of the experiment, 5 min was set aside for participants to fully practice the fatiguing tasks and movements of the experiment. Participants then performed a 2- to 3-min warm-up exercise to ensure that the shoulder and neck muscles were in a state of relaxation. After the warm-up, participants were asked to sit in a chair with their knees bent at 90 degrees, their upper body upright, and their arms hanging naturally [38]. A cotton ball soaked in 75% ethanol was used to clean the subject’s right and left UT surfaces and remove grease, and sEMG bipolar electrodes were fixed to the skin of the right and left UTs [39,40]. The electrode positions are shown in Figure 1. After fitting the electrodes, the participants were instructed to perform a UT muscle contraction test.
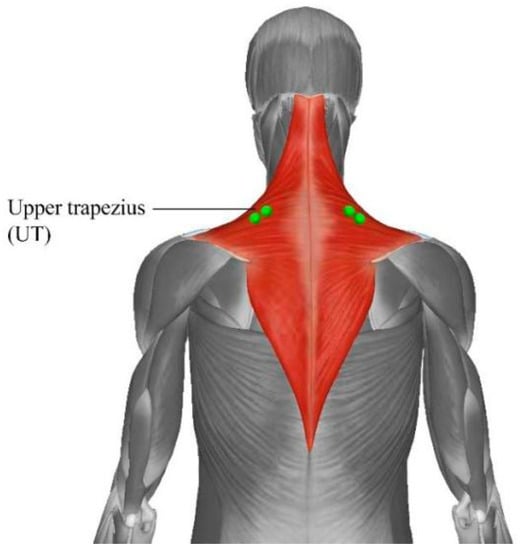
Figure 1.
The measured muscle and the positions of the electrode sensor.
Since the intervention method of this experiment was vibration massage, if the electrodes had been worn to receive vibration massage, it would have made the electrode attachment area and surrounding area unable to receive massage stimulation, and the electrode position could have changed by then. Therefore, we marked the exact positions of the electrodes when they were worn for the first time. The electrodes were removed for the intervention during the vibratory massage and then worn again after the intervention was completed in the previously marked positions. Each time the electrodes were re-worn, the experimental assistant was required to check the signal waveform on the monitoring device according to the participant’s movements and to adjust the electrode position to ensure the correct electrode position.
At the beginning of the experiment, sEMG was measured for the 5 s resting period of the left and right UT muscles. Maximum voluntary contraction (MVC) tests were performed on the left and right UT muscles separately before the task. Each muscle was tested three times for MVC, with each test lasting three to four minutes. The highest MVC calculated was chosen as the MVC value. The location and testing of MVC were performed according to the recommendations of Johansen et al. [41]. A rest period of 20 min was provided after the completion of the MVC before all tasks and before the start of the fatigue task. During the experiment, the participants were asked to hold a 1 kg dumbbell in the left and the right hand for 30 s UT muscle isotonic contraction exercise. The isotonic contraction exercise task is described as follows: The subjects slowly lifted the dumbbells flat to the sides of the body until they were at shoulder height and then returned the dumbbells to the starting position [42,43]. The experimental movements are shown in Figure 2. The sEMG signal data were recorded for this period. For intervention group, after completing a 30 s UT muscle fatigue isotonic contraction task, the researchers performed a vibratory massage intervention on the left and right UT muscles using a level 1 36 Hz intensity vibrating massager, with the order of the left and right UT muscle interventions chosen randomly. The duration of the continuous vibratory massage intervention for each UT muscle was 5 min (10 min in total). Participants then performed another 30 s of UT muscle isometric contraction exercise and again recorded the sEMG signal data for that time period, saving the recorded data to a folder and changing the name of the file folder to “fatigue 30 s task”. The above experimental procedure is a complete set of experiments, with the set marked as the A1. For the A2, the duration of the isotonic contraction of the UT muscle was changed to 60 s. The rest of the experimental procedure was the same as for the A1. For the A3 of experiments, the duration of the isotonic contraction of the UT muscle was changed to 90 s, and the rest of the experimental procedure was the same as for the A1. The above three experimental interventions were all level 1 36 Hz intensity vibratory massages. The intervention was then changed to a level 3 46 Hz intensity vibration massage for B1, B2, and B3, with the other experimental procedures corresponding to the A1, A2, and A3 experiments in turn. Thus, the sequence of the six experiments was arranged as follows: the first experiment was A1, the second experiment was A2, the third experiment was A3, the fourth experiment was B1, the fifth experiment was B2 and the sixth experiment was B3. The participants were given a 10-min break during each set of experiments. The experiment ended after each participant had completed the six sets of experiments described above (A1, A2, A3, B1, B2, and B3). For the control group, the same experimental procedure was followed to complete the six sets of experiments described above (A1, A2, A3, B1, B2, and B3) but without receiving any intervention during the experiment.
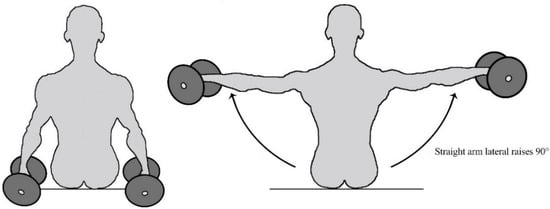
Figure 2.
Diagram of experimental movements.
Two assistants were involved throughout the experiment, one to record the entire experiment and the other to observe the participants, in order to ensure the reliability of the experiment.
2.4. Data Analysis and Processing
2.4.1. Selection of Features
In the literature, many characteristics of the sEMG signal have been found to be related to muscle activation [44]. Selecting appropriate features is critical for trapezius muscle fatigue classification. The root mean square (RMS) is a common sEMG signal feature of muscle fatigue, and its numerical magnitude is proportional to the signal amplitude, as shown in Equation (1) [45]. Continuous muscle contraction leads to muscle fatigue, and as muscle fatigue increases, the amplitude of the muscle sEMG signal gradually increases, as evidenced by an increase in the RMS on the sEMG. Therefore, the degree of muscle fatigue can be determined by a significant increase or decrease in RMS value on the sEMG [46]:
where xn is the value of the sEMG signal at a specific sampling point, and n is the number of samples.
2.4.2. Feature Extraction
All the raw sEMG signals were processed through a 20–500 Hz Butterworth bandpass filter to eliminate ambient noise. We selected 1000 ms sliding windows with 200 ms overlap to segment the sEMG signal. All sEMG signal data was processed and analyzed in MATLAB (MATLAB 7.8, The Math Works, Inc., Natick, MA, USA). The data is then transferred to an Excel spreadsheet for further normalization. We normalized the root mean square values to MVC values using the formula of Ramdera and Maras [47] MVC% = (RMS (fatigue task phase) − (RMS (rest phase)/(RMS (MVC of pre-fatigue task) − RMS (rest phase) × 100%.
2.4.3. Statistical Analysis
The statistical software SPSS (v26, Chicago, IL, USA) was used to analyze the collected data samples to verify the differences in muscle fatigue before and after UT muscle massage. The Shapiro–Wilk test was used to check the normality of the data. Analysis of covariance (ANCOVA) was used to compare differences in post-test values between groups after correction for differences in baseline values and to estimate adjusted post-test means for each outcome measure in each group. Because there were two dependent variables (three fatigue tasks) and (two vibration frequencies) within this experimental group, a 2-way ANOVA with repeated measures and a post hoc analysis with Bonferroni correction were used to perform parametric tests. The significance level for all analyses was set at p < 0.05.
2.4.4. Classification Models
Machine learning algorithms have been frequently employed in research on muscle fatigue, with classification being one of the most common methods of information mining. Classification is a supervised learning technique that aims to predict target groups in data where different categories are predefined at different times [48]. In the literature, researchers can now apply a range of categorization techniques. However, some of the current cutting-edge algorithms have many technical and operational limitations, so this study chose the four most common classifiers, including K-nearest neighbors (k-NN), support vector machine (SVM), decision tree (DT), and bagging for muscle fatigue recognition and classification training. A 10-fold cross-validation was used to evaluate the classification performance. The following are the indicators utilized in this study to evaluate the model’s performance:
Accuracy is the most commonly used classification performance metric, as shown in Equation (2). It can be used to evaluate a model’s accuracy by dividing the number of correct identifications by the model’s total number of samples. In general, the higher the precision of a model, the better the model:
where TP—true positive, TN—true negative, FP—false positive, and FN—false negative.
Precision indicates the proportion of samples identified by the model as positive classes that are positive, as shown in Equation (3):
Recall is also known as the ratio of the number of samples correctly identified by the sensitive indicator model as positive classes to the total number of positive samples, as shown in Equation (4).
The last metric considered was the F1-score, which is defined as the summed average of the correct and recall rates, as shown in Equation (5).
3. Results
3.1. Analysis of UT Muscle Fatigue and Vibration Massage Intensity Results
Table 1 shows the comparison of the mean post-test measurements of sEMG activity (MVC%) between the intervention and control groups after correction for differences in baseline values (ANCOVA). We compared all outcome test values between the two groups according to the corrected baseline value differences and found significant changes in all experimental conditions in both intervention and control groups for the right UT muscle (p = 0.043, p = 0.015, p = 0.060, p = 0.010, p = 0.043, p = 0.030). In contrast, the left UT muscle showed significant differences between the intervention and control groups in the fatigue 90 s task only in the condition of the vibration massage level 3 intervention (p = 0.007).

Table 1.
Comparison of mean post-test measurements of sEMG activity (MVC%) between Intervention and control groups after correction for differences in baseline values (ANCOVA).
Table 2 shows the mean and SD of the sEMG activities (MVC%) values of the left and right UT muscles before and after the experiment for the vibration massage level 1 (36 Hz) intervention group and the control group. The results showed a significant decrease in MVC% of the right UT muscle before and after the intervention using vibration massage level 1 for the fatigue 30 s, 60 s, and 90 s tasks (R1: p = 0.022, R2: p = 0.005, R3: p = 0.049). However, the MVC% of the left UT muscle did not show significant differences in the fatigue 30 s, 60 s, and 90 s tasks. (L1: p = 0.076, L2: p = 1.000, L3: p = 0.345). In the control group, no significant changes were observed in the MVC% of both left and right lateral UT muscles (p = 1.000).
Table 2.
Mean values ± SD of the sEMG activities (MVC%) of the right (R) and left (L) UT muscles before and after the vibratory massage level 1 (36 Hz) intervention.
Table 3 shows the mean and SD of the sEMG activities (MVC%) values of the left and right UT muscles before and after the experiment for the vibration massage level 3 (46 Hz) intervention group and the control group. The results showed that in the vibration massage level 3 intervention group, no significant differences were present in the MVC% of both left and right lateral UT muscles during the fatigue 30 s task. (R1: p = 0.116, L1: p = 0.301). In the fatigue 60 s task, there was a significant decrease in MVC% for the right side UT muscle (R2: p = 0.033), but no significant change in MVC% was observed for the left UT muscle (L2: p = 0.274). In the fatigue 90 s task, a significant decrease in MVC% was observed in both the right and left lateral UT muscles (R3: p = 0.028, L3: p = 0.040). In the control group, no significant changes in MVC% were observed in both right and left lateral UT muscles (p = 1.000).
Table 3.
Mean values ± SD of the sEMG activities (MVC%) of the right (R) and left (L) UT muscles before and after the vibratory massage level 3 (46 Hz) intervention.
3.2. Massage Scheme Recognition Model
The muscle fatigue identification and massage model was constructed in three parts. The MVC% values of the sEMG signals extracted above were labeled according to the period of UT muscle fatigue, with data from 30 s of fatigue labeled as category 1, data from 60 s of fatigue called category 2, and data from 90 s of fatigue labeled as category 3.
In the second part, the labeled data were then input into four different machine learning algorithms for classification training. Table 4 shows the parameters and performance of the four machine learning algorithms implemented. The performance of the DT was significantly lower than that of the other algorithms on the 10-fold cross-validation method. The SVM had a precision and recall of 0.774 and 0.784, respectively, and the KNN had a precision and recall of 0.740 and 0.762. Both machine learning algorithms performed relatively similarly in terms of their parameters. However, the results of the bagging algorithm had a higher precision of 0.860, a recall of 0.814, and an f-value of 0.797 compared with the other algorithms. A higher recall percentage allowed the correct level of muscle fatigue to be identified. Finally, the results showed that the bagging algorithm performed the best in all performance parameters for these four algorithms in identifying the degree of UT muscle fatigue, and therefore, the bagging machine learning classifier was chosen as the model to build for this study.
Table 4.
Comparison of classification performance for UT muscle fatigue detection.
In the third part, effective massage protocols for different fatigue tasks were derived from the above statistical analysis as follows: Plan 1, using a vibration massage level 1 intervention was more effective in fatigue relief for the right UT muscle during the 30 s fatigue task (R1: p = 0.022); Plan 2, in the 60 s fatigue task, using a vibration massage level 1 intervention was more effective in relieving fatigue in the right UT muscle (R2: p = 0.005); and plan 3, in the 90 s fatigue task, a vibration massage level 3 intervention was more effective in relieving fatigue in both left and right UT muscles (R3: p = 0.028, L3: p = 0.040). The above-mentioned labels for the different categories of fatigue data were matched to the three plans, category 1 as plan 1, category 2 as plan 2, and category 3 as plan 3. If the model outputs a label of category 1, this means that using plan1 to massage right UT muscle is most effective in that fatigue situation. The output label is category 2, which means that using plan 2 to massage the right UT muscles is most effective for muscle relaxation, and the output label is category 3, which means that using plan 3 to massage the UT muscles on both sides is most effective.
4. Discussion
The purpose of this study is to investigate whether different levels of vibration massage have significant effects on the left and right UT muscles by measuring objective physiological signals surface electromyography. The analysis was used to find the best vibration massage program for the UT muscles and then to construct a bilateral UT fatigue identification and vibration massage model. To achieve this aim, we first performed a statistical analysis of the between-group differences between the intervention and control groups, and we observed a significant change in the between-group differences between the intervention and control groups. This suggests that the vibration massage intervention had a significant effect on UT muscle fatigue. Similar to what we found, Alam et al. [49] found a significant effect of vibration on grip endurance time in the forearm: Vibration treatment at 35 Hz in the forearm enhanced grip strength and grip endurance time at 50% MVC, indicating that vibration therapy at 35 Hz in the forearm had a favorable effect on neuromuscular performance. Some studies have found that low-frequency vibration massage (1–50 Hz) increases local temperature and leads to the relaxation of myofascial tissue, which can have a muscle-calming effect [50,51,52]. Chwała et al. [27] found a significant difference before and after vibration massage during isometric contractions. In particular, the results of this study imply that the selection of appropriate low-frequency vibrations is an effective way to accelerate the recovery of fatigued motor muscle groups and restore lost motor function.
Then, we further analyzed the specific effects of the level 1 vibration massage intervention and the level 3 vibration massage intervention on the UT muscles. We found that significant decreases in MVC% values of the right UT muscle occurred before and after the level 1 vibration massage intervention in the 30 s fatigue, 60 s fatigue, and 90 s fatigue tasks, but no significant changes in MVC% values of the left UT muscle occurred. Significant decreases in MVC% values of the right UT muscle occurred before and after the 3-level vibration massage intervention in both the 60 s fatigue and 90 s fatigue tasks. Significant changes in MVC% values occurred in the left UT muscle only in the 90 s fatigue task. This result suggests that the fatigue mechanisms and relief effects produced by bilateral UT muscles under the same conditions are not symmetrical, and that the researchers’ observations of the effects of assessing UT muscle fatigue differ between the two sides, possibly due to various factors [53,54,55].
The asymmetry in the fatigue and relief effects of the right and left UT may be due to differences in fatigue characteristics between the dominant and non-dominant sides. This problem was also observed by Farina [56], who believed that the fatigue characteristics of the superior UT muscles were asymmetrical between the dominant and non-dominant sides. The author collected electromyograms of static constant force contractions of the arm under different loads and found statistically significant differences between the dominant and non-dominant sides by comparing the rate of change of electromyogram spectra. By measuring the stiffness of the upper oblique muscle electronically during cervical flexion, Jun Zhang et al. [57] discovered a substantial variation in the elastic modulus of the superior oblique muscle between the dominant and non-dominant sides. The thick-ness of the lower trapezius muscle was likewise shown to be higher on the dominant side (0.43 0.02 mm) by Uthaikhup et al. [58]. The increase in non-dominant UT muscle activity was attributed by Januario et al. [59] to an overflow of afferents from ipsilateral muscles to contralateral motor neurons. Moreover, as mentioned by Diederichsen [60], the preference for the dominant hand may be related to the unique movement pattern of the individual. Seong-Gil Kim et al. [61] measured the activity of the muscles near the scapula by the lateral scapular sliding test (LSST) and analyzed the correlation between left–right asymmetry and the activity of the muscles around the scapula. Their study showed that the asymmetry of the right and left scapulae gradually increased with upper limb abduction during external rotation activity, which led to an increase in the difference in activity of the right and left UT muscles. It has also been observed [62] that differences in interlimb gap frequency can result in differences between the dominant and non-dominant sides. This study suggests that muscle rest and gap frequency on the dominant side versus the non-dominant side result in different movement and recovery patterns, with the dominant side allowing for fewer intervals between rest periods thereby obtaining maximum muscle rest, while the non-dominant side requires longer intervals between rest periods, to obtain muscle rest. All of these reasons could be responsible for the asymmetry found in this study and the asymmetry in the effective massage strength of the UT muscles on both sides. Thus, the experimental results of the present study are consistent with the previously found anatomical and physiological asymmetries at all levels of the nervous system. More experimental validation is needed in future studies regarding the specific causes of adaptation site differences and asymmetries that lead to activation of nerve fibers in the right and left UT muscles to continue in-depth investigation and research.
After the comparison and analysis of the data, four different machine learning algorithms were tested using the RMS of the collected sEMG data, in which we added the first half of the UT muscle fatigue data to the training set and used the second half as the data validation set with the test set. The analysis revealed that the bagging classification method achieved a classification accuracy of 0.860, which outperformed other classification algorithms. In common with our findings, some studies have also evaluated and validated the applicability of integrated classifiers [63,64]. Sharon et al. [48] concluded that bagging classification methods are more accurate and efficient than single algorithms, and also can effectively improve the performance of the underlying classifier, while integration techniques have been successfully applied in reality. Thus, the authors combined a bagging machine lea rning classification algorithm to construct a bilateral UT fatigue recognition and vibration massage model. The model can suggest effective vibration solutions for different levels of fatigue in bilateral UT muscles, helping people to relax their muscles during a busy day and actively prevent the onset of musculoskeletal disorders.
The present research has a number of limitations. Firstly, only the UT muscles were identified as target muscles for this study; the study did not cover other muscle groups that are linked to neck tiredness. Additionally, our subjects were all current postgraduate students, and there were no restrictions on gender, age, or activity level. Our present study derived a fatigue recognition and vibration massage model, but this may be specific to a single age group, or gender group. In future studies, we will test more subjects of different genders and ages while combining algorithms to construct a real-time prediction model for muscle fatigue in the UT, which can appropriately avoid the effects of muscle asymmetry due to the dominant side.
5. Conclusions
In this study, we focused on testing two new hypotheses and constructing a bilateral UT fatigue identification and vibration massage model. First, we determined that the vibration massage intervention did have a significant effect on UT muscles by analyzing the MVC% difference values between the intervention and control groups. We also explored the effect of a level 1 vibration massage intervention (36 Hz) versus a level 3 vibration massage intervention (46 Hz) on bilateral UT muscles by analyzing the changes in MVC% values for the left and right side UTs under three different fatigue conditions, respectively. The results of this analysis showed an asymmetric effect of the same vibration level on the relief of bilateral UT muscles. This validates the second hypothesis we proposed. Then, we summarized to derive the best relief scheme for bilateral UT muscles corresponding to different vibration massage levels. The sEMG signal data collected in the experiments was used to train four machine learning algorithms, and the performance metrics of the four methods were compared. Finally, the bagging classification method was selected to build a bilateral UT fatigue recognition and vibration massage model, which can select the corresponding vibration massage frequency according to the different fatigue levels of the UT muscles, reducing the risk of muscle damage caused by improper manual selection of vibration frequencies. In future studies, the number and diversity of subjects should be expanded to include subjects of different occupations, ages, and genders to obtain more representative data. This data should be used to optimize the fatigue recognition and vibration massage models for a wider range of people.
Author Contributions
Conceptualization, J.H., L.W. and M.F.; methodology, J.H., L.W. and M.F.; software, L.W. and M.F.; validation, L.W. and M.F.; formal analysis, J.H., L.W. and M.F.; investigation, L.W. and M.F.; resources, J.H. and L.W.; data curation, M.F.; writing—original draft preparation, L.W. and M.F; writing—review and editing, L.W.; visualization, M.F.; supervision, M.F.; project administration, J.H. and L.W.; funding acquisition, J.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research funded by the National Natural Science Foundation of China (No. 52035007, 51975360), Major Project of National Social Science Foundation of China (No. 17ZDA020), Ministry of Education “Human Factors and Ergonomics” University Industry Collaborative Education Project (No.202002SJ, 202209LH16) and Cross Fund for medical and Engineering of Shanghai Jiao Tong University (No.YG2021QN118).
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Review Committee for Scientific and Technological Research Involving Humans of Shanghai Jiao Tong University (protocol code I2022241I-R1 and approval date 15 July 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Santos, J.; Baptista, J.S.; Monteiro, P.R.R.; Miguel, A.S.; Santos, R.; Vaz, M.A. The influence of task design on upper limb muscles fatigue during low-load repetitive work: A systematic review. Int. J. Ind. Ergon. 2016, 52, 78–91. [Google Scholar] [CrossRef]
- Mathiassen, S.E. Diversity and variation in biomechanical exposure: What is it, and why would we like to know? Appl. Ergon. 2006, 37, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Nussbaum, M.A.; Clark, L.L.; Lanza, M.A.; Rice, K.M. Fatigue and Endurance Limits During Intermittent Overhead Work. AIHAJ Am. Ind. Hyg. Assoc. 2001, 62, 446–456. [Google Scholar] [CrossRef]
- Lomond, K.V.; Côté, J.N. Shoulder functional assessments in persons with chronic neck/shoulder pain and healthy subjects: Reliability and effects of movement repetition. Work 2011, 38, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Telaprolu, N.; Anne, S.D. Physical and psychological work demands as potential risk factors for musculoskeletal disorders among workers in weaving operations. Indian J. Occup. Environ. Med. 2014, 18, 129–134. [Google Scholar] [CrossRef]
- Gangopadhyay, S.; Ghosh, T.; DAS, T.; Ghoshal, G.; DAS, B.B. Prevalence of Upper Limb Musculo Skeletal Disorders among Brass Metal Workers in West Bengal, India. Ind. Health 2007, 45, 365–370. [Google Scholar] [CrossRef]
- Luger, T.; Bosch, T.; Hoozemans, M.; De Looze, M.; Veeger, D. Task variation during simulated, repetitive, low-intensity work—Influence on manifestation of shoulder muscle fatigue, perceived discomfort and upper-body postures. Ergonomics 2015, 58, 1851–1867. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Mork, P.J.; Westgaard, R.H. Long-term electromyographic activity in upper trapezius and low back muscles of women with moderate physical activity. J. Appl. Physiol. 2005, 99, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Sarker, P.; Norasi, H.; Koenig, J.; Hallbeck, M.S.; Mirka, G. Effects of break scheduling strategies on subjective and objective measures of neck and shoulder muscle fatigue in asymptomatic adults performing a standing task requiring static neck flexion. Appl. Ergon. 2020, 92, 103311. [Google Scholar] [CrossRef] [PubMed]
- Van Rijn, R.M.; Huisstede, B.M.; Koes, B.; Burdorf, A. Associations between work-related factors and specific disorders of the shoulder—A systematic review of the literature. Scand. J. Work. Environ. Health 2010, 36, 189–201. [Google Scholar] [CrossRef]
- Kim, J.Y.; Park, J.S.; Kim, D.J.; Im, S. Evaluation of fatigue patterns in individual shoulder muscles under various external conditions. Appl. Ergon. 2020, 91, 103280. [Google Scholar] [CrossRef] [PubMed]
- Côté, J.N. Adaptations to Neck/Shoulder Fatigue and Injuries. In Progress in Motor Control. Vol 826. Advances in Experimental Medicine and Biology; Levin, M.F., Ed.; Springer: New York, NY, USA, 2014; pp. 205–228. [Google Scholar] [CrossRef]
- Keir, P.J.; Sanei, K.; Holmes, M.W. Task rotation effects on upper extremity and back muscle activity. Appl. Ergon. 2011, 42, 814–819. [Google Scholar] [CrossRef]
- Lee, C.-L.; Lu, S.-Y.; Sung, P.-C.; Liao, H.-Y. Working height and parts bin position effects on upper limb muscular strain for repetitive hand transfer. Int. J. Ind. Ergon. 2015, 50, 178–185. [Google Scholar] [CrossRef]
- Nimbarte, A.D. Risk of neck musculoskeletal disorders among males and females in lifting exertions. Int. J. Ind. Ergon. 2014, 44, 253–259. [Google Scholar] [CrossRef]
- Lee, S.; Choi, Y.-H.; Kim, J. Effects of the cervical flexion angle during smartphone use on muscle fatigue and pain in the cervical erector spinae and upper trapezius in normal adults in their 20s. J. Phys. Ther. Sci. 2017, 29, 921–923. [Google Scholar] [CrossRef]
- Richter, H.O.; Zetterberg, C.; Forsman, M. Trapezius muscle activity increases during near work activity regardless of accommodation/vergence demand level. Eur. J. Appl. Physiol. 2015, 115, 1501–1512. [Google Scholar] [CrossRef] [PubMed]
- Fei-Ruo, Z.; Li-Hua, H.; Shan-Shan, W.; Jing-Yun, L.; Kang-Pin, Y.; Sheng, W. Quantify work load and muscle functional activation patterns in neck-shoulder muscles of female sewing machine operators using surface electromyogram. Chin. Med. J. 2011, 124, 3731–3737. [Google Scholar]
- Padilha, U.C.; Vieira, A.; Vieira, D.C.L.; De Lima, F.D.; Junior, V.A.R.; Tufano, J.J.; Bottaro, M. Could inter-set stretching increase acute neuromuscular and metabolic responses during resistance exercise? Eur. J. Transl. Myol. 2019, 29, 8579. [Google Scholar] [CrossRef] [PubMed]
- Mika, A.; Mika, P.; Fernhall, B.; Unnithan, V.B. Comparison of Recovery Strategies on Muscle Performance After Fatiguing Exercise. Am. J. Phys. Med. Rehabil. 2007, 86, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Hohenauer, E.; Taeymans, J.; Baeyens, J.-P.; Clarys, P.; Clijsen, R. The Effect of Post-Exercise Cryotherapy on Recovery Characteristics: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0139028. [Google Scholar] [CrossRef] [PubMed]
- Eguchi, Y.; Jinde, M.; Murooka, K.; Konno, Y.; Ohta, M.; Yamato, H. Stretching versus transitory icing: Which is the more effective treatment for attenuating muscle fatigue after repeated manual labor? Eur. J. Appl. Physiol. 2014, 114, 2617–2623. [Google Scholar] [CrossRef] [PubMed]
- Lau, W.Y.; Nosaka, K. Effect of Vibration Treatment on Symptoms Associated with Eccentric Exercise-Induced Muscle Damage. Am. J. Phys. Med. Rehabil. 2011, 90, 648–657. [Google Scholar] [CrossRef] [PubMed]
- Oliveri, D.J.; Lynn, K.; Hong, C.-Z. Increased Skin Temperature after Vibratory Stimulation. Am. J. Phys. Med. Rehabil. 1989, 68, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Hausswirth, C.; Le Meur, Y. Physiological and nutritional aspects of post-exercise recovery: Specific recommendations for female athletes. Sports Med. 2011, 41, 861–882. [Google Scholar] [CrossRef] [PubMed]
- Iii, E.B.L.; Sackiriyas, K.S.B.; Bains, G.S.; Calandra, G.; Lobo, C.; Nakhro, D.; Malthankar, G.; Paul, S. A comparison of whole body vibration and moist heat on lower extremity skin temperature and skin blood flow in healthy older individuals. Med. Sci. Monit. 2012, 18, CR415–CR424. [Google Scholar] [CrossRef][Green Version]
- Chwała, W.; Pogwizd, P.; Rydzik, Ł.; Ambroży, T. Effect of Vibration Massage and Passive Rest on Recovery of Muscle Strength after Short-Term Exercise. Int. J. Environ. Res. Public Health 2021, 18, 11680. [Google Scholar] [CrossRef] [PubMed]
- Chu, Y.; Zhao, Y.; Hu, S.; Wang, Q.; Semeah, L.M.; Jia, H.; Lv, T.; Li, X.; Wang, R. Immediate Effect of Local Vibration Therapy for Sport-induced Fatigue Based on Traditional Chinese Medicine’s Holistic Theory. J. Multidiscip. Health 2020, 13, 1993–2001. [Google Scholar] [CrossRef]
- Lurie, R.C.; Cimino, S.R.; Gregory, D.E.; Brown, S. The effect of short duration low back vibration on pain developed during prolonged standing. Appl. Ergon. 2018, 67, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Koumantakis, G.A.; Roussou, E.; Angoules, G.A.; Angoules, N.A.; Alexandropoulos, T.; Mavrokosta, G.; Nikolaou, P.; Karathanassi, F.; Papadopoulou, M. The immediate effect of IASTM vs. Vibration vs. Light Hand Massage on knee angle repositioning accuracy and hamstrings flexibility: A pilot study. J. Bodyw. Mov. Ther. 2020, 24, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Pournot, H.; Tindel, J.; Testa, R.; Mathevon, L.; Lapole, T. The Acute Effect of Local Vibration as a Recovery Modality from Exercise-Induced Increased Muscle Stiffness. J. Sports Sci. Med. 2016, 15, 142–147. [Google Scholar] [PubMed]
- Mahdavi, N.; Motamedzade, M.; Jamshidi, A.A.; Darvishi, E.; Moghimbeygi, A.; Heidarimoghadam, R. Upper trapezius fatigue in carpet weaving: The impact of a repetitive task cycle. Int. J. Occup. Saf. Ergon. 2016, 24, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-Y.; Yu, I.-Y.; Oh, J.-S.; Kang, M.-H. Effects of Intended Scapular Posterior Tilt Motion on Trapezius Muscle Electromyography Activity. Int. J. Environ. Res. Public Health 2021, 18, 9147. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.; Song, D.; Park, D.; Kim, H.; Shin, G. Reflexive Response of Neck Muscle to Sudden Perturbation after Prolonged Smartphone Use. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2021, 65, 1250–1253. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed]
- Kirst, M.A. Effects of Tool Weight on Fatigue and Performance during Short Cycle Overhead Work Operations. Ph.D. Thesis, Virginia Tech, Blacksburg, VA, USA, 1999. [Google Scholar]
- Kleine, B.-U.; Schumann, N.-P.; Stegeman, D.F.; Scholle, H.-C. Surface EMG mapping of the human trapezius muscle: The topography of monopolar and bipolar surface EMG amplitude and spectrum parameters at varied forces and in fatigue. Clin. Neurophysiol. 2000, 111, 686–693. [Google Scholar] [CrossRef]
- Farina, D.; Madeleine, P.; Graven-Nielsen, T.; Merletti, R.; Arendt-Nielsen, L. Standardising surface electromyogram recordings for assessment of activity and fatigue in the human upper trapezius muscle. Eur. J. Appl. Physiol. 2002, 86, 469–478. [Google Scholar] [CrossRef]
- Jensen, C.; Westgaard, R.H. Functional subdivision of the upper trapezius muscle during low-level activation. Eur. J. Appl. Physiol. 1997, 76, 335–339. [Google Scholar] [CrossRef]
- Jensen, C.; Vasseljen, O.; Westgaard, R.H. The influence of electrode position on bipolar surface electromyogram recordings of the upper trapezius muscle. Eur. J. Appl. Physiol. 1993, 67, 266–273. [Google Scholar] [CrossRef]
- Johansen, T.I.; Samani, A.; Antle, D.M.; Côté, J.N.; Madeleine, P. Gender effects on the coordination of subdivisions of the trapezius muscle during a repetitive box-folding task. Eur. J. Appl. Physiol. 2012, 113, 175–182. [Google Scholar] [CrossRef]
- Öberg, T. Muscle fatigue and calibration of EMG measurements. J. Electromyogr. Kinesiol. 1995, 5, 239–243. [Google Scholar] [CrossRef]
- Borstad, J.D.; Szucs, K.; Navalgund, A. Scapula kinematic alterations following a modified push-up plus task. Hum. Mov. Sci. 2009, 28, 738–751. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, R.H.; Reaz, M.B.I.; Ali, M.A.B.M.; Bakar, A.A.A.; Chellappan, K.; Chang, T.G. Surface Electromyography Signal Processing and Classification Techniques. Sensors 2013, 13, 12431–12466. [Google Scholar] [CrossRef] [PubMed]
- Tkach, D.; Huang, H.; Kuiken, T.A. RSetseuardchy of stability of time-domain features for electromyographic pattern recognition. J. Neuroeng. Rehabil. 2010, 7, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Moussavi, Z.K.; Cooper, J.E.; Shwedyk, E. Fatigue pattern of trapezius muscle in relation to its functional role. In Proceedings of the 18th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Amsterdam, The Netherlands, 31 October–3 November 1996; Volume 4, pp. 1451–1453. [Google Scholar] [CrossRef]
- Lavender, S.A.; Marras, W.S. An electromyographic analysis of an ergonomic intervention with the jackleg drill. Appl. Ergon. 1990, 21, 90–100. [Google Scholar] [CrossRef]
- Sharon, H.; Elamvazuthi, I.; Lu, C.-K.; Parasuraman, S.; Natarajan, E. Development of Rheumatoid Arthritis Classification from Electronic Image Sensor Using Ensemble Method. Sensors 2019, 20, 167. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.M.; Khan, A.A.; Farooq, M. Effects of vibratory massage therapy on grip strength, endurance time and forearm muscle performance. Work 2021, 68, 619–632. [Google Scholar] [CrossRef]
- Rittweger, J.; Mutschelknauss, M.; Felsenberg, D. Acute changes in neuromuscular excitability after exhaustive whole body vibration exercise as compared to exhaustion by squatting exercise. Clin. Physiol. Funct. Imaging 2003, 23, 81–86. [Google Scholar] [CrossRef]
- Torvinen, S.; Kannus, P.; Sievänen, H.; Jarvinen, T.A.H.; Pasanen, M.; Kontulainen, S.; Järvinen, T.L.N.; Järvinen, M.; Oja, P.; Vuori, I. Effect of a vibration exposure on muscular performance and body balance. Randomized cross-over study: Effects of vibration on perfor-mance and balance. Clin. Physiol. Funct. Imaging 2002, 22, 145–152. [Google Scholar] [CrossRef]
- Diego, M.A.; Field, T.; Sanders, C.; Hernandez-Reif, M. Massage therapy of moderate and light pressure and vibrator effects on EEG and heart rate. Int. J. Neurosci. 2004, 114, 31–44. [Google Scholar] [CrossRef]
- Barnes, M.J.; Perry, B.G.; Mündel, T.; Cochrane, D.J. The effects of vibration therapy on muscle force loss following eccentrically induced muscle damage. Eur. J. Appl. Physiol. 2011, 112, 1189–1194. [Google Scholar] [CrossRef]
- Fuller, J.T.; Thomson, R.L.; Howe, P.R.; Buckley, J.D. Vibration Therapy Is No More Effective Than the Standard Practice of Massage and Stretching for Promoting Recovery from Muscle Damage After Eccentric Exercise. Clin. J. Sport Med. 2015, 25, 332–337. [Google Scholar] [CrossRef]
- Merletti, R.; Sabbahi, M.A.; De Luca, C.J. Median frequency of the myoelectric signal. Eur. J. Appl. Physiol. Occup. Physiol. 1984, 52, 258–265. [Google Scholar] [CrossRef]
- Farina, D.; Kallenberg, L.A.C.; Merletti, R.; Hermens, H.J. Effect of side dominance on myoelectric manifestations of muscle fatigue in the human upper trapezius muscle. Eur. J. Appl. Physiol. 2003, 90, 480–488. [Google Scholar] [CrossRef]
- Zhang, J.; Yu, J.; Liu, C.; Tang, C.; Zhang, Z. Modulation in Elastic Properties of Upper Trapezius with Varying Neck Angle. Appl. Bionics Biomech. 2019, 2019, 6048562. [Google Scholar] [CrossRef]
- Uthaikhup, S.; Bsc, N.W.; Kummaung, P. Effects of gender and hand dominance on size of the lower trapezius muscle: Lower Trapezius Size. Muscle Nerve 2015, 52, 576–579. [Google Scholar] [CrossRef]
- Januario, L.B.; França, D.B.; Moreira, R.D.F.C.; Oliveira, A.B. Comparison of muscle activity from upper trapezius and wrist extensors between dominant and non-dominant upper limbs during computer-based tasks. Work 2018, 61, 295–301. [Google Scholar] [CrossRef]
- Diederichsen, L.P.; Nørregaard, J.; Dyhre-Poulsen, P.; Winther, A.; Tufekovic, G.; Bandholm, T.; Rasmussen, L.R.; Krogsgaard, M. The effect of handedness on electromyographic activity of human shoulder muscles during movement. J. Electromyogr. Kinesiol. 2007, 17, 410–419. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-G. Correlation between Scapular Asymmetry and Differences in Left and Right Side Activity of Muscles Adjacent to the Scapula. Osong Public Health Res. Perspect. 2017, 8, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Marker, R.J.; Balter, J.E.; Nofsinger, M.L.; Anton, D.; Fethke, N.B.; Maluf, K.S. Upper trapezius muscle activity in healthy office workers: Reliability and sensitivity of occupational exposure measures to differences in sex and hand dominance. Ergonomics 2016, 59, 1205–1214. [Google Scholar] [CrossRef] [PubMed]
- Shiezadeh, Z.; Sajedi, H.; Aflakie, E. Diagnosis of rheumatoid arthritis using an ensemble learning approach. Comput. Sci. Inf. Technol. 2015, 5, 139–148. [Google Scholar] [CrossRef]
- Das, R.; Sengur, A. Evaluation of ensemble methods for diagnosing of valvular heart disease. Expert Syst. Appl. 2010, 37, 5110–5115. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).