
Laboratory Characterization of In-Service Full-Mouth Rehabilitation with Monolithic Translucent Zirconia Restorations

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Topography Analysis
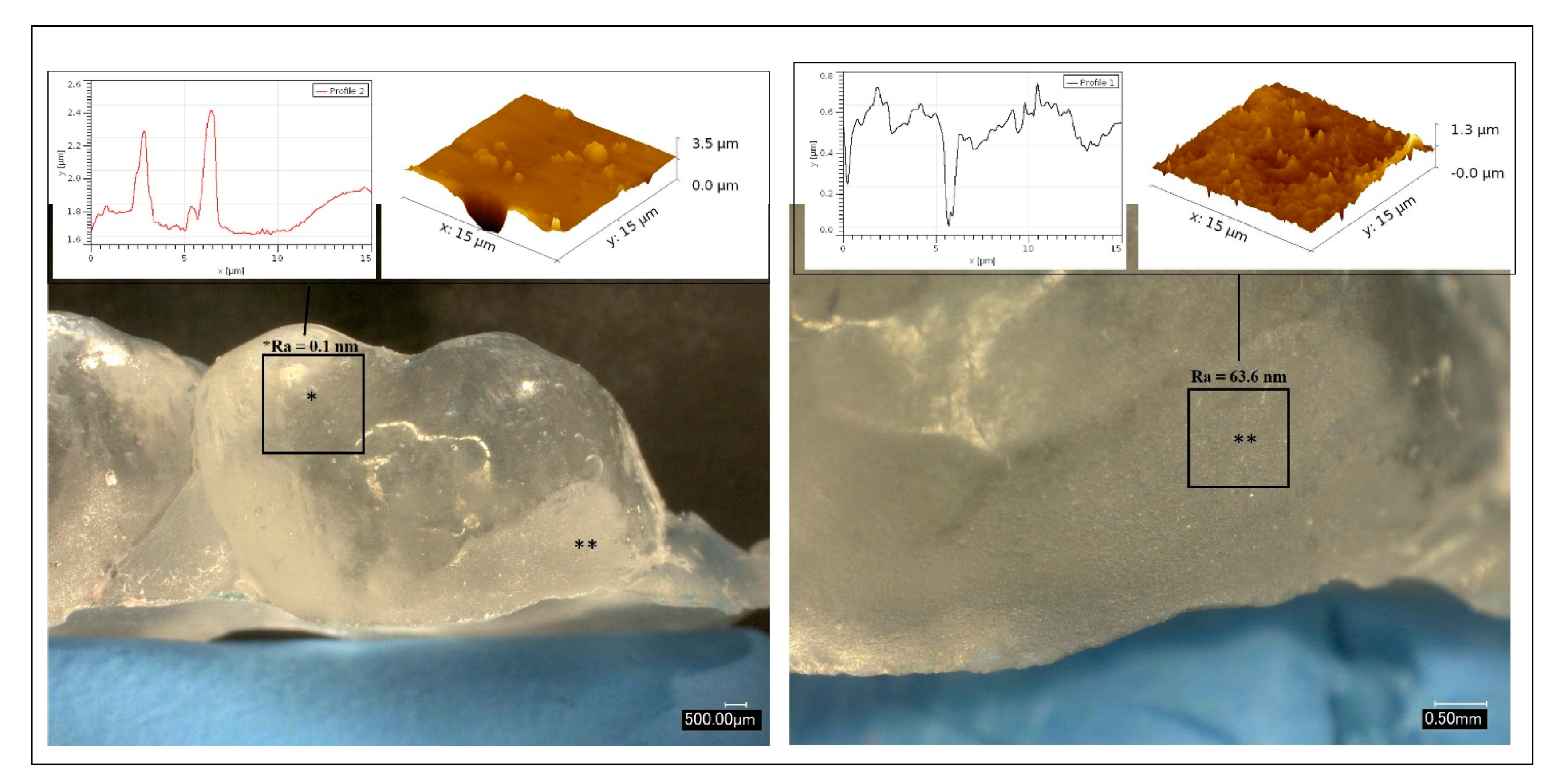
2.2. Surface Roughness Analysis
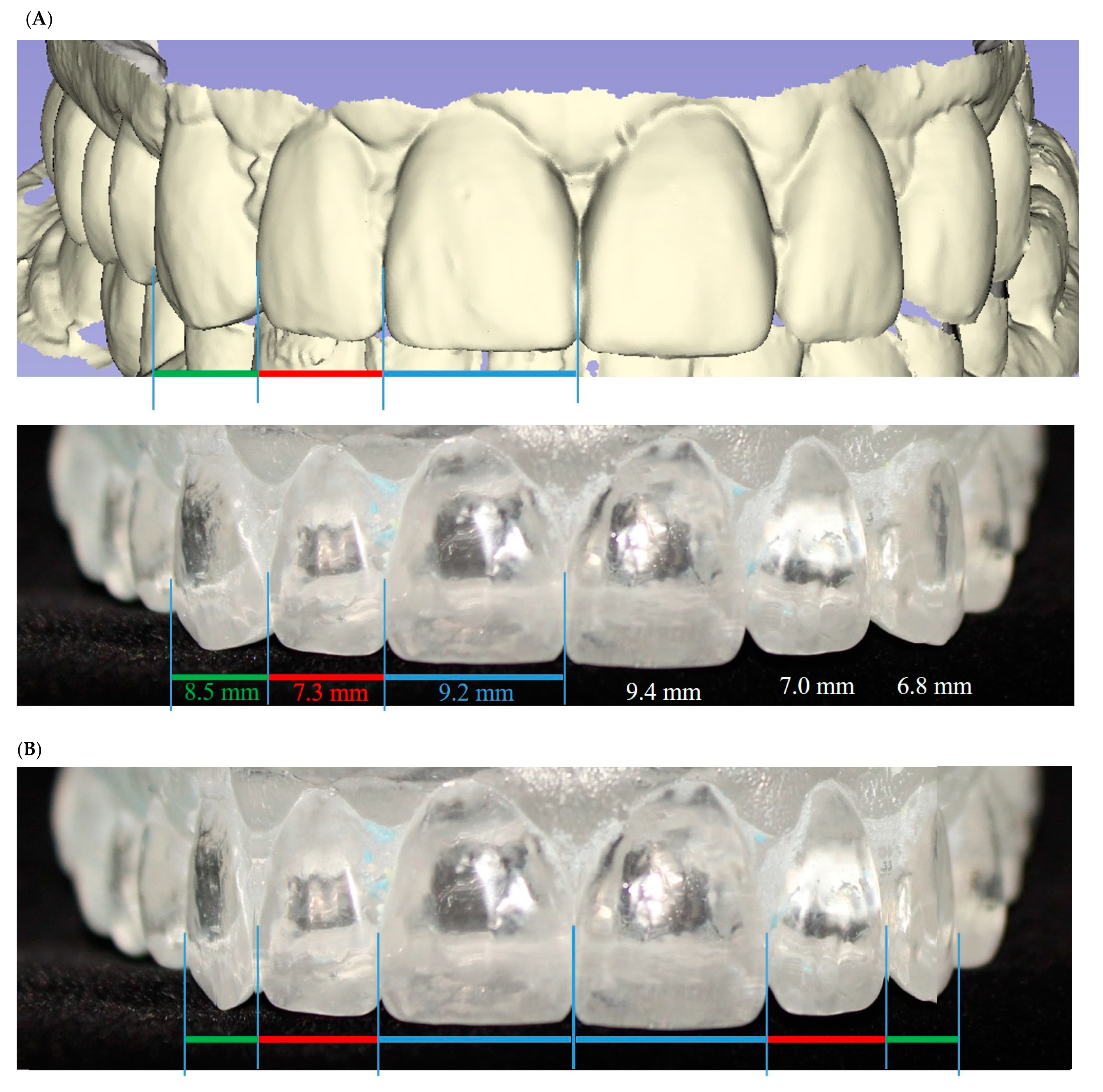
2.3. Symmetry Analysis
3. Results
3.1. Topography Analysis
3.2. Surface Roughness
3.3. Symmetry
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Salazar Marocho, S.M.; Studart, A.R.; Bottino, M.A.; Bona, A.D. Mechanical strength and subcritical crack growth under wet cyclic loading of glass-infiltrated dental ceramics. Dent. Mater. 2010, 26, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.R.; Benetti, P. Ceramic materials in dentistry: Historical evolution and current practice. Aust. Dent. J. 2011, 56, 84–96. [Google Scholar] [CrossRef] [PubMed]
- Fathy, S.M.; Al-Zordk, W.; EGrawish, M.; VSwain, M. Flexural strength and translucency characterization of aesthetic monolithic zirconia and relevance to clinical indications: A systematic review. Dent. Mater. 2021, 37, 711–730. [Google Scholar] [CrossRef]
- Pathan, M.S.; Kheur, M.G.; Patankar, A.H.; Kheur, S.M. Assessment of antagonist enamel wear and clinical performance of full-contour monolithic zirconia crowns: One-year results of a prospective study. J. Prosthodont. 2019, 28, e411–e416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konstantinidis, I.; Trikka, D.; Gasparatos, S.; Mitsias, M.E. Clinical outcomes of monolithic zirconia crowns with CAD/CAM technology. A 1-Year Follow-Up Prospective Clinical Study of 65 Patients. Int. J. Environ. Res. Public Health 2018, 15, 2523. [Google Scholar] [CrossRef] [Green Version]
- Solá-Ruiz, M.F.; Baixauli-López, M.; Roig-Vanaclocha, A.; Amengual-Lorenzo, J.; Agustín-Panadero, R. Prospective study of monolithic zirconia crowns: Clinical behavior and survival rate at a 5-year follow-up. J. Prosthodont. Res. 2020. online ahead of print. [Google Scholar] [CrossRef]
- Denry, I. How and when does fabrication damage adversely affect the clinical performance of ceramic restorations? Dent. Mater. 2013, 29, 85–96. [Google Scholar] [CrossRef]
- Quinn, G.D. NIST Recommended Practice Guide: Fractography of Ceramics and Glasses; NIST: Gaithersburg, MD, USA, 2006.
- Scherrer, S.S.; Quinn, J.B.; Quinn, G.D.; Wiskott, H.W. Fractographic ceramic failure analysis using the replica technique. Dent. Mater. 2007, 23, 1397–1404. [Google Scholar] [CrossRef] [Green Version]
- Mihlbachler, M.C.; Foy, M.; Beatty, B.L. Surface replication, fidelity and data loss in traditional dental microwear and dental microwear texture analysis. Sci. Rep. 2019, 9, 159. [Google Scholar] [CrossRef] [Green Version]
- Swileh, M.A.; Abuaffan, A.H.; Alhajj, M.N. Evaluation of the golden proportion and golden standard of maxillary anterior teeth in relation to smile attractiveness. Braz. Dent. Sci. 2019, 22, 178–189. [Google Scholar] [CrossRef] [Green Version]
- Al-Marzok, M.I.; Majeed, K.R.; Ibrahim, I.K. Evaluation of maxillary anterior teeth and their relation to the golden proportion in Malaysian population. BMC Oral Health 2013, 13, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chavan, A.D.; Suryawanshi, C.V. Correlation of fibonacci sequence and golden ratio with its applications in engineering and science. Int. J. Eng. Manag. Res. 2020, 10, 31–36. [Google Scholar] [CrossRef]
- Nečas, D.; Klapetek, P. Gwyddion: An open-source software for SPM data analysis. Cent. Eur. J. Phys. 2012, 10, 181–188. [Google Scholar] [CrossRef]
- Rekow, E.D.; Silva, N.R.; Coelho, P.G.; Zhang, Y.; Guess, P.; Thompson, V.P. Performance of dental ceramics: Challenges for improvements. J. Dent. Res. 2011, 90, 937–952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rashid, H. The effect of surface roughness on ceramics used in dentistry: A review of literature. Eur. J. Dent. 2014, 8, 571–579. [Google Scholar] [CrossRef]
- Lie, T.; Gusberti, F. Replica study of plaque formation on human tooth surfaces. Acta Odontol. Scand. 1979, 37, 65–72. [Google Scholar] [CrossRef]
- Ekfeldt, A.; Flöystrand, F.; Oilo, G. Replica techniques for in vivo studies of tooth surfaces and prosthetic materials. Scand. J. Dent. Res. 1985, 93, 560–565. [Google Scholar] [CrossRef]
- Pintado, M.R.; Conry, J.P.; Douglas, W.H. Fissure sealant wear at 30 months: New evaluation criteria. J. Dent. 1991, 19, 33–38. [Google Scholar] [CrossRef]
- Youngson, C.C.; Grey, N.J. An in vitro comparative analysis: Scanning electron microscopy of dentin/restoration interfaces. Dent. Mater. 1992, 8, 252–258. [Google Scholar] [CrossRef]
- Jodha, K.S.; Salazar Marocho, S.M.; Scherrer, S.S.; Griggs, J.A. Fractal analysis at varying locations of clinically failed zirconia dental implants. Dent. Mater. 2020, 36, 1052–1058. [Google Scholar] [CrossRef]
- Juma’ah, A.A.; Brunton, P.A.; Li, K.C.; Waddell, J.N. Simulated clinical adjustment and intra-oral polishing of two translucent, monolithic zirconia dental ceramics: An in vitro investigation of surface roughness. J. Dent. 2020, 101, 103447. [Google Scholar] [CrossRef]
- Øilo, M.; Quinn, G.D. Fracture origins in twenty-two dental alumina crowns. J. Mech. Behav. Biomed. 2016, 53, 93–103. [Google Scholar] [CrossRef]
- Coldea, A.; Fischer, J.; Swain, M.V.; Thiel, N. Damage tolerance of indirect restorative materials (including PICN) after simulated bur adjustments. Dent. Mater. 2015, 31, 684–694. [Google Scholar] [CrossRef]
- Stober, T.; Bermejo, J.L.; Schwindling, F.S.; Schmitter, M. Clinical assessment of enamel wear caused by monolithic zirconia crowns. J. Oral Rehabil. 2016, 43, 621–629. [Google Scholar] [CrossRef]
- Esquivel-Upshaw, J.F.; Kim, M.J.; Hsu, S.M.; Abdulhameed, N.; Jenkins, R.; Neal, D.; Ren, F.; Clark, A.E. Randomized clinical study of wear of enamel antagonists against polished monolithic zirconia crowns. J. Dent. 2018, 68, 19–27. [Google Scholar] [CrossRef] [Green Version]
- Mundhe, K.; Jain, V.; Pruthi, G.; Shah, N. Clinical study to evaluate the wear of natural enamel antagonist to zirconia and metal ceramic crowns. J. Prosthet. Dent. 2015, 114, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Anami, L.C.; Pereira, C.A.; Guerra, E.; Assunção e Souza, R.O.; Jorge, A.O.; Bottino, M.A. Morphology and bacterial colonisation of tooth/ceramic restoration interface after different cement excess removal techniques. J. Dent. 2012, 40, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Pereira, S.; Anami, L.C.; Pereira, C.A.; Souza, R.; Kantorski, K.Z.; Bottino, M.A.; Jorge, A.; Valandro, L.F. Bacterial Colonization in the Marginal Region of Ceramic Restorations: Effects of Different Cement Removal Methods and Polishing. Oper. Dent. 2016, 41, 642–654. [Google Scholar] [CrossRef] [PubMed]
- Levin, E.I. Dental esthetics and the golden proportion. J. Prosthet. Dent. 1978, 40, 244–252. [Google Scholar] [CrossRef]
- Sterrett, J.D.; Oliver, T.; Robinson, F.; Fortson, W.; Knaak, B.; Russell, C.M. Width/length ratios of normal clinical crowns of the maxillary anterior dentition in man. J. Clin. Periodontol. 1999, 26, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Orozco-Varo, A.; Arroyo-Cruz, G.; Martínez-de-Fuentes, R.; Jiménez-Castellanos, E. Biometric analysis of the clinical crown and the width/length ratio in the maxillary anterior region. J. Prosthet. Dent. 2015, 113, 565–570.e2. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Álvarez, L.; Orozco-Varo, A.; Arroyo-Cruz, G.; Jiménez-Castellanos, E. Width/length ratio in maxillary anterior teeth. Comparative study of esthetic preferences among professionals and laypersons. J. Prosthodont. 2019, 28, 416–420. [Google Scholar] [CrossRef]
- Chieruzzi, M.; Rallini, M.; Pagano, S.; Eramo, S.; D’Errico, P.; Torre, L.; Kenny, J.K. Mechanical effect of static loading on endodontically treated teeth restored with fiber-reinforced posts. J. Biomed. Mater. Res. B Appl. Biomater. 2014, 102, 384–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Surface Damage | Surface Irregularities | |||||
|---|---|---|---|---|---|---|
| Location of Tooth | Tooth ID | # of Surfaces Affected | Percentage | Tooth ID | # of Surfaces Affected | Percentage |
| Anterior | 6 | L | 11.10% | 8 | F | 11.10% |
| 10 | L | 9 | F | |||
| 11 | I | 22 | L | |||
| 7 | I, L | 14.80% | None | None | 0% | |
| 9 | I, L | |||||
| 22 | F, I | |||||
| 23 | I, L | |||||
| Posterior | 2 3 4 5 12 13 14 18 19 20 30 31 | O O O O O O O O O O F F | 44.4% | 2 5 12 13 19 20 30 | F L L L L L L | 25.9% |
| 21 | LO | 3.70% | 3 | F, O | 11.10% | |
| 28 | O, L | |||||
| 29 | O, L | |||||
| Location | Tooth ID | # of Damaged Surfaces | Damaged Total Surface Area (mm2) | Remaining Undamaged Surface Area (mm2) |
|---|---|---|---|---|
| Anterior | 6 | L | 37.8 | 45.7 |
| 7 | LI | 21.5 | 45.1 | |
| 9 | LI | 28.4 | 13.6 | |
| 10 | L | 18.0 | 43.2 | |
| 11 | I | 1.2 | 2.8 | |
| 22 | FI | 19.9 | 67.3 | |
| 23 | IL | 8.1 | 40.6 | |
| Posterior | 2 | O | 1.6 | 74.9 |
| 3 | O | 20.8 | 60.5 | |
| 4 | O | 14.1 | 27.9 | |
| 5 | O | 6.2 | 32.4 | |
| 12 | O | 17.8 | 34.3 | |
| 13 | O | 6.2 | 50.7 | |
| 14 | O | 22.0 | 58.6 | |
| 18 | O | 30.5 | 3.5 | |
| 19 | O | 2.9 | 75.2 | |
| 20 | O | 4.0 | 36.0 | |
| 21 | LO | 5.9 | 59.4 | |
| 30 | F | 5.9 | 67.4 | |
| 31 | F | 1.1 | 67.1 |
| Teeth # | Incisal Third Width (mm) | Middle Third Width (mm) | Gingival Third Width (mm) | Visible Width (mm) | Height (mm) | Width-to-Height Ratio | Form |
|---|---|---|---|---|---|---|---|
| 6 | 9.7 | 10.1 | 10.1 | 8.5 | 10.6 | 11:10 (80%) | Tapered |
| 7 | 7.2 | 7.3 | 7.1 | 7.3 | 11.1 | 11:7 (66%) | Tapered |
| 8 | 8.7 | 9.2 | 7.9 | 9.2 | 11.8 | 4:3 (78%) | Tapered |
| 9 | 9.3 | 9.4 | 7.6 | 9.4 | 11.6 | 4:3 (81%) | Tapered |
| 10 | 7.0 | 7.3 | 5.8 | 7.0 | 11.1 | 11:7 (63%) | Tapered |
| 11 | 11.4 | 11.3 | 9.7 | 6.8 | 11.6 | 12:7 (59%) | Tapered |
| 22 | 7.7 | 10.1 | 10.1 | --- | 10.9 | 11:8 (93%) | Square tapered |
| 23 | 5.5 | 5.6 | 5.0 | --- | 10.2 | 2:1 (54%) | Square tapered |
| 24 | 5.0 | 5.2 | 4.2 | --- | 9.9 | 2:1 (52%) | Square tapered |
| 25 | 5.2 | 5.1 | 3.7 | --- | 9.8 | 2:1 (52%) | Square tapered |
| 26 | 5.4 | 5.8 | 5.0 | --- | 10.1 | 2:1 (57%) | Square tapered |
| 27 | 7.7 | 10.1 | 10.5 | --- | 11.07 | 11:9 (91%) | Square tapered |
| Tooth # | Total Width (mm) | Visible Width (mm) |
|---|---|---|
| 2 | 11.1 | 0.7 |
| 3 | 12.6 | 1.6 |
| 4 | 8.4 | 1.6 |
| 5 | 9.2 | 2.7 |
| 12 | 10.3 | 2.1 |
| 13 | 9.7 | 0.3 |
| 14 | 12.9 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salazar Marocho, S.M.; VanLandingham, M.B.; Mourad, F.; Pappa, A.; Koka, S. Laboratory Characterization of In-Service Full-Mouth Rehabilitation with Monolithic Translucent Zirconia Restorations. Symmetry 2021, 13, 1755. https://doi.org/10.3390/sym13091755
Salazar Marocho SM, VanLandingham MB, Mourad F, Pappa A, Koka S. Laboratory Characterization of In-Service Full-Mouth Rehabilitation with Monolithic Translucent Zirconia Restorations. Symmetry. 2021; 13(9):1755. https://doi.org/10.3390/sym13091755
Chicago/Turabian StyleSalazar Marocho, Susana M., Mary Beth VanLandingham, Firas Mourad, Andres Pappa, and Sreenivas Koka. 2021. "Laboratory Characterization of In-Service Full-Mouth Rehabilitation with Monolithic Translucent Zirconia Restorations" Symmetry 13, no. 9: 1755. https://doi.org/10.3390/sym13091755
APA StyleSalazar Marocho, S. M., VanLandingham, M. B., Mourad, F., Pappa, A., & Koka, S. (2021). Laboratory Characterization of In-Service Full-Mouth Rehabilitation with Monolithic Translucent Zirconia Restorations. Symmetry, 13(9), 1755. https://doi.org/10.3390/sym13091755