1. Introduction
Cataract is a disease that leads to visual impairment, and eventually to blindness, worldwide. With an aging population, the incidence and prevalence of cataract is increasing, as well as the number of treatments. Prokofyeva and co-workers reported that the prevalence of this disease in Europe increased from 5% of the population between 52 and 62 years-old and from 30% for 60–69 years old to 64% in population above 70 years-old (between 2000 and 2009) [
1]. More recent studies by Flaxman and co-workers and Bikbov and co-workers have not only confirmed this tendency, but forecasted further growth of cases [
2,
3]. Cataract surgery with intraocular lens (IOL) implantation has been quickly evolving over the years, with the development of new technology and techniques, such as phacoemulsification and new materials for IOL, making it a safer and more reliable procedure [
4,
5,
6]. Following cataract surgery, few complications can appear, one of the most serious being in-the-bag-IOL dislocation [
7]. This complication arises from a progressive zonular dehiscence associated with contraction of the capsular bag that leads to the dislocation of the IOL inside the bag. This results in a decrease of the patient’s visual acuity and usually its management requires complex surgical procedures [
8]. The risk factors for this condition include clinical conditions that cause zonular weakness such as pseudoexfoliation, connective tissue disorders, uveitis, retinitis pigmentosa, high myopia, and patients who underwent vitreoretinal surgery. Bag dislocation in these situations usually occurs a long time after cataract surgery, with a mean interval of 6.9–8.5 years [
9,
10,
11]. In silico studies shall help understand the mechanics of the IOL dislocation, and study the parameters that could influence this complication, due to its increasing incidence following the increase of procedures performed to remove cataracts [
12,
13,
14]. However, only a few computational studies on the crystalline lens are found in literature and to the authors’ knowledge there are none addressing the IOL dislocation. Previously published works had different purposes, such as understanding the mechanisms of the accommodation process in healthy or presbyopic eyes [
15,
16,
17], or computationally estimating mechanical properties of the human crystalline lens [
13,
18].
In fact, building reliable models of the eye is not straightforward because of its complex geometry, together with the lack of information on tissue properties. There are also limited clues on the biomechanics of eye degeneration [
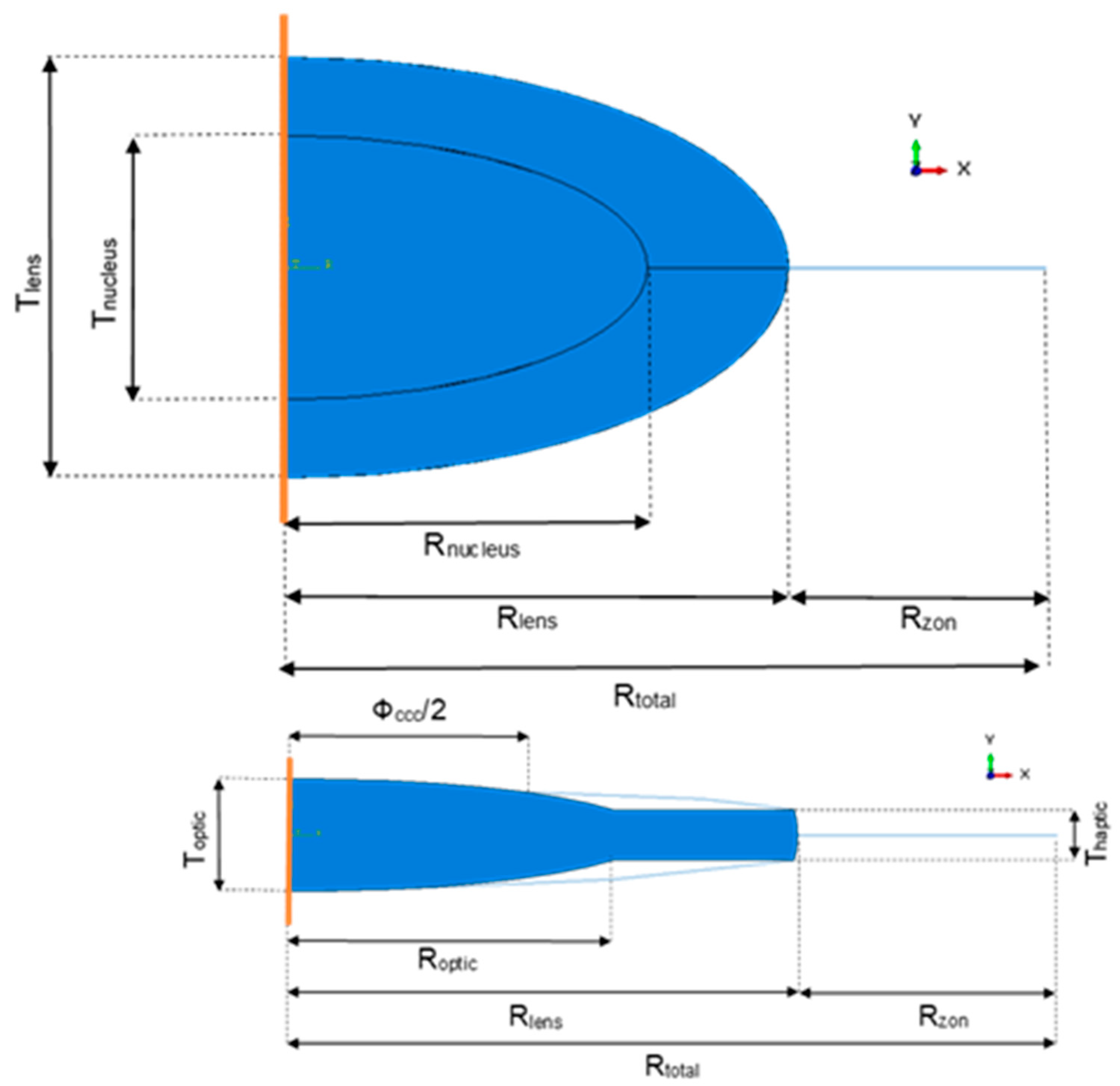
19]. The human eye lens complex is composed by four main components: the capsular bag (or capsule), the crystalline lens (composed by the cortex and the nucleus), the zonular fibers (or zonules), and the ciliary body. This complex is of extreme importance in the human visual system since it allows the eye to focus on objects, i.e., to accommodate. The crystalline lens is a transparent and flexible structure enclosed inside a thin membrane with a thickness of about 10 µm, even though Fisher and Pettet [
20] showed it slightly changes with age and position, the capsular bag, and is connected to the ciliary body by the zonular fibers, at the zonular lamella. The zonules are known to be separated in three distinct groups, all around the circumference of the lens: the anterior, the equatorial, and the posterior group. They are considered as suspensory ligaments which not only hold the lens in position, but also reshape it during accommodation.
In addition, the mechanical loading depends on the state of accommodation (accommodated/unaccommodated), and a few theories about accommodation have arisen and were not always in concordance. The most popular one was the Helmholtz’s theory [
21] that stated that in the unaccommodated (or disaccommodated) state, the lens was held in a state of radial tension by all the zonules. When beginning the process of accommodation, the ciliary body contracted leading to a reduction of tension in the zonular fibers and to an increase of curvature of lens surfaces and optical power, until reaching the fully accommodated state. Opposed to Helmholtz’s, stood Schachar’s theory [
22] stating that when going from the unaccommodated to the accommodated state, the contraction of the ciliary body lead to an increase of tension in the zonular fibers, i.e., stating that the zonules had a direct effect on this process. From a mechanical point of view, Helmholtz claimed that the stress-free state of the lens complex was when it stood in an accommodated state, with no stresses on the zonular fibers, whereas Schachar stated that this stress-free state occurred in the unaccommodated state. Understanding the mechanisms of accommodation was very relevant to study complications regarding the crystalline lens and its associated structures. The main complication to be discussed in this work usually occurs in late adult life, when the crystalline lens loses transparency and becomes opaque—it is said to become a cataract. This results in the reduction of the transmission of light and in scattering light, leading to blurred vision, and in the extreme to blindness, when not treated in time. Recently, the most common solution available is the complete removal of the cataract, i.e., of the crystalline lens, followed by an implant of an IOL in the capsular bag to replace it, leaving the eye in a pseudophakic state [
12,
22,
23].
Assuming the mechanical environment plays an important role in the capsular failure and in the IOL performance, the main objective of this work was to propose a mechanical model of the IOL-capsular bag complex after cataract surgery. Knowing that late IOL-capsular bag dislocation was one of the most serious problems after this procedure, the goal was to study the stress in the capsular bag and in the zonular fibers through a suitable Finite Element (FE) model, to understand when did the zonules break and lead to the dislocation of the whole complex. The development of such a model would allow the assessment of the impact of different variables in the capsular and zonular stresses. In clinical practice, this could translate into changes in intraoperative maneuvers, like the type and size of capsulotomy opening created, or selection of a specific IOL material, design, or positioning in the capsular bag that would minimize the risk of a late in-the-bag-IOL dislocation. Meaningful parameters, as the diameter of the capsulotomy and the materials of the IOL were studied to assess their influence on this process and to seek the best configuration to avoid this complication with the IOL.
3. Results
For each model, the von Mises stress in the zonules (SZ), in the capsular bag (SCB) and in the IOL (SIOL), were assessed, as well as the radial displacement in the X-direction (δr) and the resulting force at the tip of the zonules (RFZ). All of the models built had the purpose of letting us compare different models for pseudophakic eyes, with different diameters of capsulorhexis, different materials for the different one-piece IOL, and with different traction forces towards the center of the capsulorhexis, that simulated part of the process of fibrosis.
3.1. Post-Surgery
A comparison between the eye before (model M1) and after surgery with a small capsulorhexis, a hydrophilic acrylic IOL, and no traction force (model M 2.1) was possible and is shown in
Figure 5. The average values of stresses, radial displacement, and resulting force are shown in
Table 4 for both models. The values of stresses in the zonular fibers are almost the double from M1 to M 2.1, going from an average value of 4.7 × 10
−2 to 8.9 × 10
−2 MPa, and from the crystalline to the IOL it substantially increased 30 times from an average value of 1.9 × 10
−4 to 5.8 × 10
−3 MPa, whereas in the capsular bag the values decreased, going from average values of 8.0 × 10
−2 to 1.9 × 10
−3 MPa. The radial displacement in M 2.1, equal to 7.3 × 10
−3 mm was almost fifty-times smaller than in M1, 3.5 × 10
−1 mm. Another value that increased from M1 to M 2.1 was the resulting force at the tip of the zonular fibers, with computed values of 7.1 × 10
−2 and 12.8 × 10
−2 N for the model before and after surgery, respectively. All of these outcomes were expected with the increase of stiffness of the three IOL materials in comparison with the natural cortex and nucleus of the crystalline. With a maximum of 1.5 × 10
−1 MPa, the higher stress in M1 was located on the capsular bag, whereas in model M 2.1 this was located on the zonular fibers with a value of 9.7 × 10
−2 MPa.
3.2. Influence of IOL Stiffness
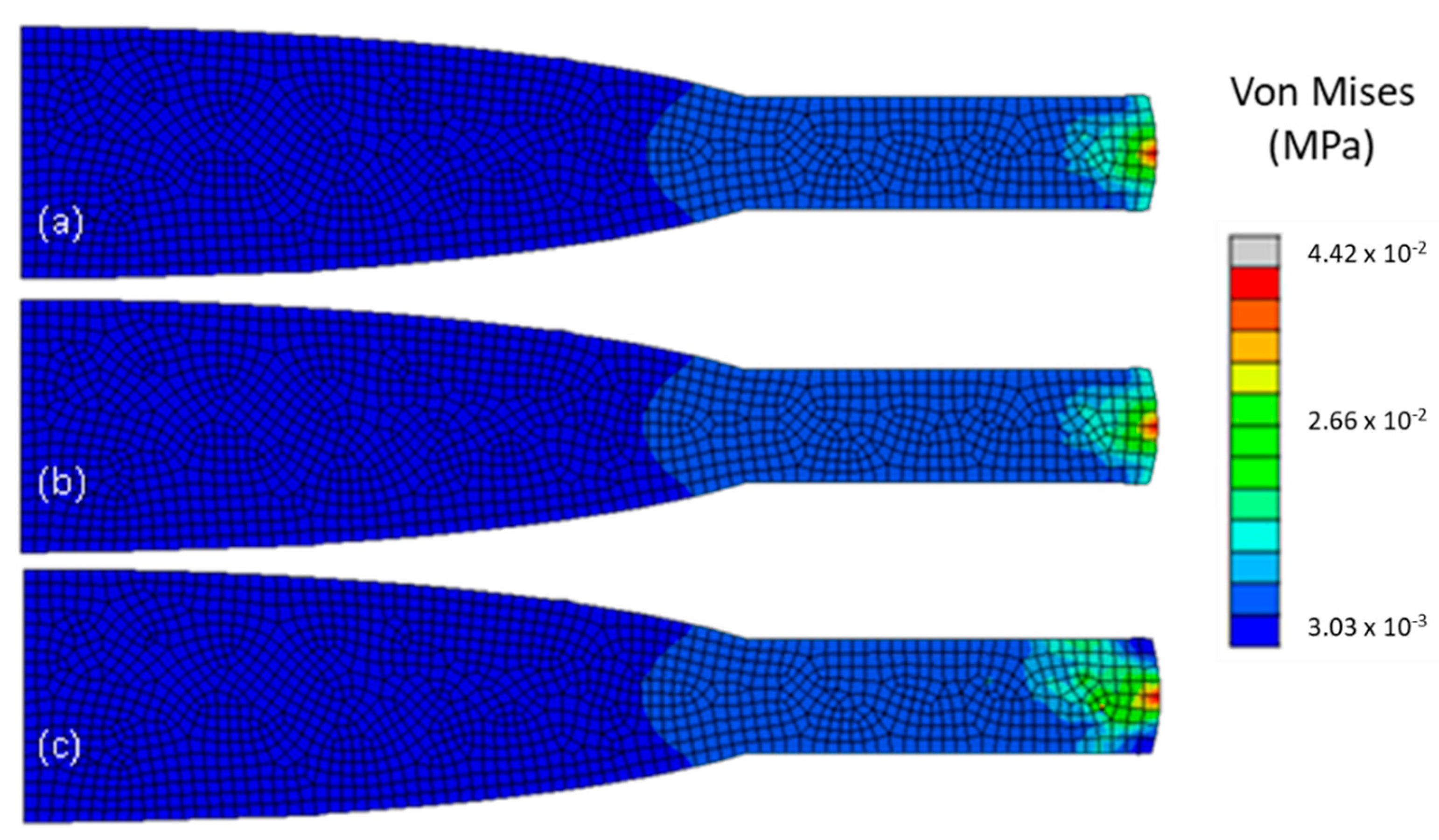
To study the influence of the stiffness of the IOL in the pseudophakic eye, a comparison between models M 2.1., M 2.2., and M 2.3. was performed. These three models had the same ΦCCC and TF, equal to zero, but differed in their IOL material and consequently, in their stiffness. The results drawn in this section can be drawn for every other three sets of models, that only differ in IOL stiffness.
Since the PMMA lens was at least 500-timed stiffer than both acrylic lenses, the expected outcome would be that it would support more stress in it with a consequent decrease of stress in the capsular bag. This phenomenon is visible in
Figure 6, where model M 2.3 had a different stress distribution, with the stress more distributed through the IOL haptic, than M 2.1 and M 2.2, with a maximum value of 4.4 × 10
−2 MPa, at the intersection between the capsular bag, the IOL and the insertion of the zonule. Whereas the general decrease of stress in the capsular bag was very slight between the hydrophilic and the hydrophobic acrylic lens, with average values ranging from 1.9 × 10
−3 to 1.4 × 10
−3 MPa respectively, an accentuated change was clearly seen in model M 2.3., with an average value of 8.9 × 10
−6 MPa, being 150-times lower than in M 2.1 or M 2.2. With the increase of stiffness in the IOL, more resistance to the equatorial pull in the zonules in the materials would be encountered, leading to a steep decrease of radial displacement in the IOL, with the one in model M 2.3, 1.2 × 10
−5 mm, being 6000-times higher than in the other two models, 7.3 × 10
−3 mm for the hydrophilic and 5.0 × 10
−3 mm for the hydrophobic acrylic lens. In
Table 5, the values with the biggest noticeable changes are depicted.
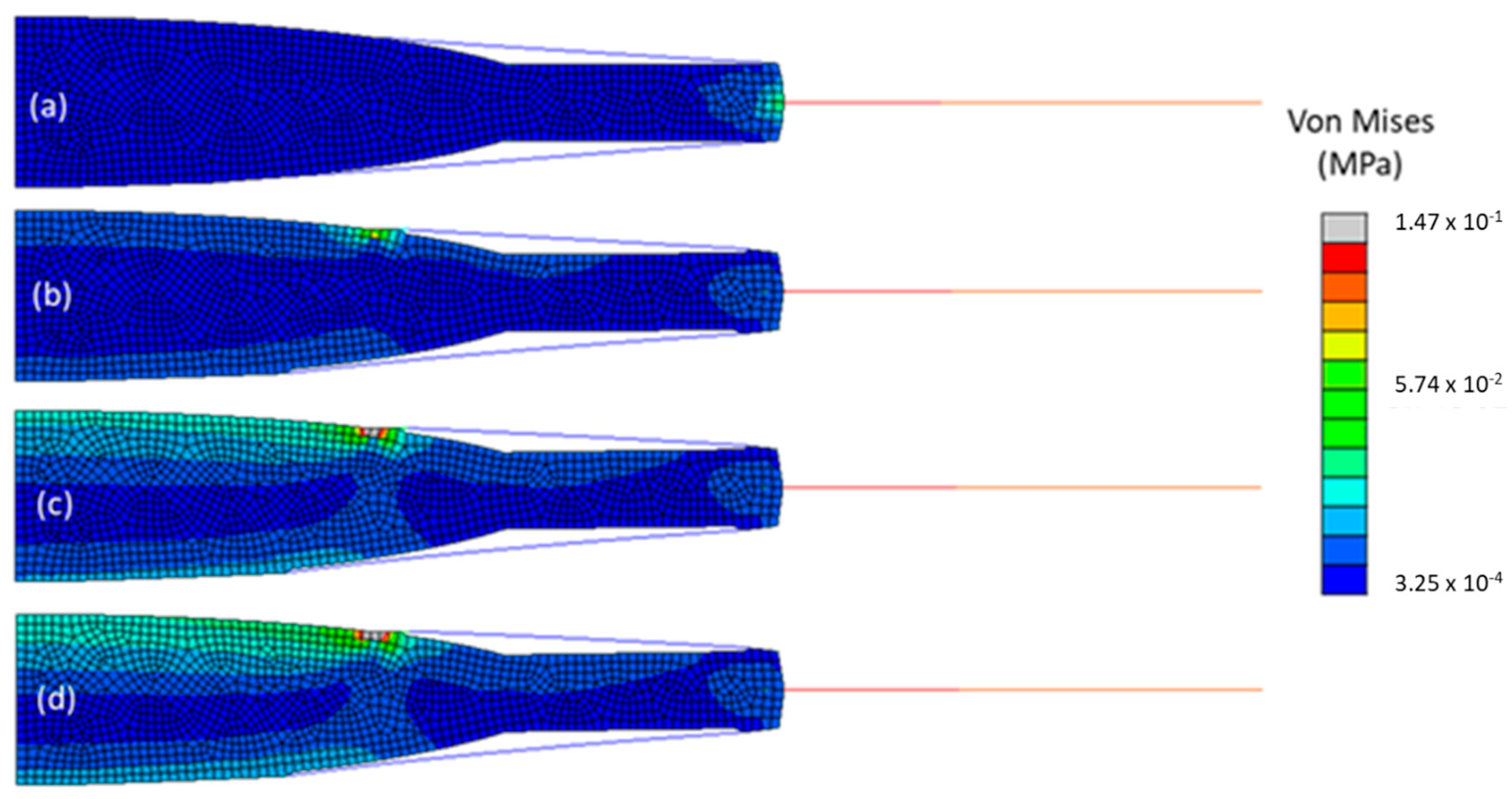
3.3. Influence of Traction Force
To study the influence of the traction force on the capsulorhexis on the pseudophakic eyes, models M 2.1., M 4.1., M 6.1., and M 8.1. were compared, as shown in
Figure 7. They all had a one-piece IOL made of hydrophilic acrylic and the same Φ
CCC but differed in the traction force that was applied. It increased from 0 to 0.15 N, from model M 2.1 to model M 8.1. The outcomes for this parametric study are depicted in
Table 5.
With the increase of the traction force, no change in stress in the zonules nor in the resulting force at their tip was noticeable, with an average value of 8.9 × 10−2 MPa for the stress and 12.9 × 10−2 N for the resulting force in all models. Overall, the average value of stress in the capsular bag increased 3.5 times from the model with no traction force to the one with a traction force of 0.15 N. The stress in the IOL and radial displacement had the greatest change, with the average stress of 1.4 × 10−2 MPa in the IOL of M 8.1, being almost 2.5-times the average stress, which was equal to 5.8 × 10−3 MPa in M 2.1. The radial displacement, 7.3 × 10−3 mm in M 2.1, was almost three-times higher than the one in M 8.1, 2.8 × 10−3 mm.
3.4. Influence of Capsulorhexis Diameter
In this subsection, models M 4.1 and M 5.1 are compared. They had the same material properties and a traction force applied at the opening of the capsulorhexis of 0.07 N but differed in the diameter of the capsulorhexis. Models M 2.1 and M 4.1 had a small capsulorhexis with a 4-mm diameter and models M 3.1 and M 5.1 had a large one, with a 4.5-mm diameter. There was no noticeably great variation in the average values of stress in all components.
4. Discussion
Comparing the human crystalline complex with a pseudophakic eye, a decrease of stress in the capsular bag and of radial displacement of the new complex was observed, with a consequent increase of resulting force and stress in the zonules, as well as an increase in stress in the IOL. These outcomes could be compared with the influence of the stiffness of the IOL material through the pseudophakic models, since the biggest difference in the eye after surgery, is the difference in stiffness of the human crystalline compared with the stiffness of all the synthetic IOL materials. The IOLs were at least a thousand-times stiffer than any component of the crystalline, making them support more stress than the crystalline and consequently relieve the stress in the capsular bag. With all of the models undergoing the same displacement of 0.5 mm at the tip of the zonules, the stiff IOL lead to the zonules having to stretch more to pull the lens and the capsular bag, and consequently putting the zonular fibers in a higher state of stress, with its maximum at the intersection node of the three parts of the model. On one hand, the IOLs gave more support to minimize stress in the capsule and eventually decrease its risk of rupture, but on the other hand it put the zonules into a state of more stress with a higher possibility for them to break and lead to an IOL-capsular bag dislocation. Ideally, to avoid this post-operative complication, a lens with a stiffness closer to the one of the human crystalline would be the best solution to try and maintain the state of stress of the capsular bag and the zonules closer to their original state.
Most of the parameters tested seemed to have influenced the overall behavior of the model. In summary, with the increase of the traction force and of the stiffness of the materials, i.e., their Young’s modulus, the stress in the IOL would increase, whereas the stress in the capsular bag and the radial displacement would decrease. With the increase of the diameter of the capsulorhexis, and the traction force equal to zero, the overall stress in the models would not change. The radial displacement would decrease and the resulting force increase, but its low magnitude is not significant. Finally, with the increase of the diameter of the capsulorhexis, all the parameters studied seemed to vary slightly and would have a contrary behavior than the ones described earlier, i.e., the stress in the zonules and in the IOL decreased, as well as the resulting force at the tip of the zonules, whereas the stress in the capsular bag and the radial displacement increased.
It was also important to notice that across all models of pseudophakic eyes, the part that would undergo the least change were the zonules, where no parameter seemed to influence greatly their maximum and average values of stress nor the resulting forces computed at their tips. The maximum variation between the average values of stress was 1% and between the resulting force was 0.8%.
Comparing only pseudophakic eyes, knowing that the stiffer PMMA IOL was at least 500-times stiffer than the acrylic lenses, a slight increase of 5% in average stress of the IOL can be considered negligible. The biggest changes observed while increasing the stiffness of the IOL was a big decrease in average capsular stress and in radial displacement. This outcome is comparable with the case studied before, i.e., the substitution of the crystalline with any IOL, where an increase in IOL stiffness would give more support to the capsular bag and minimize its average stress. In the zonules, no change in maximum and average values of stress was observed, nor change in the resulting force at their tip.
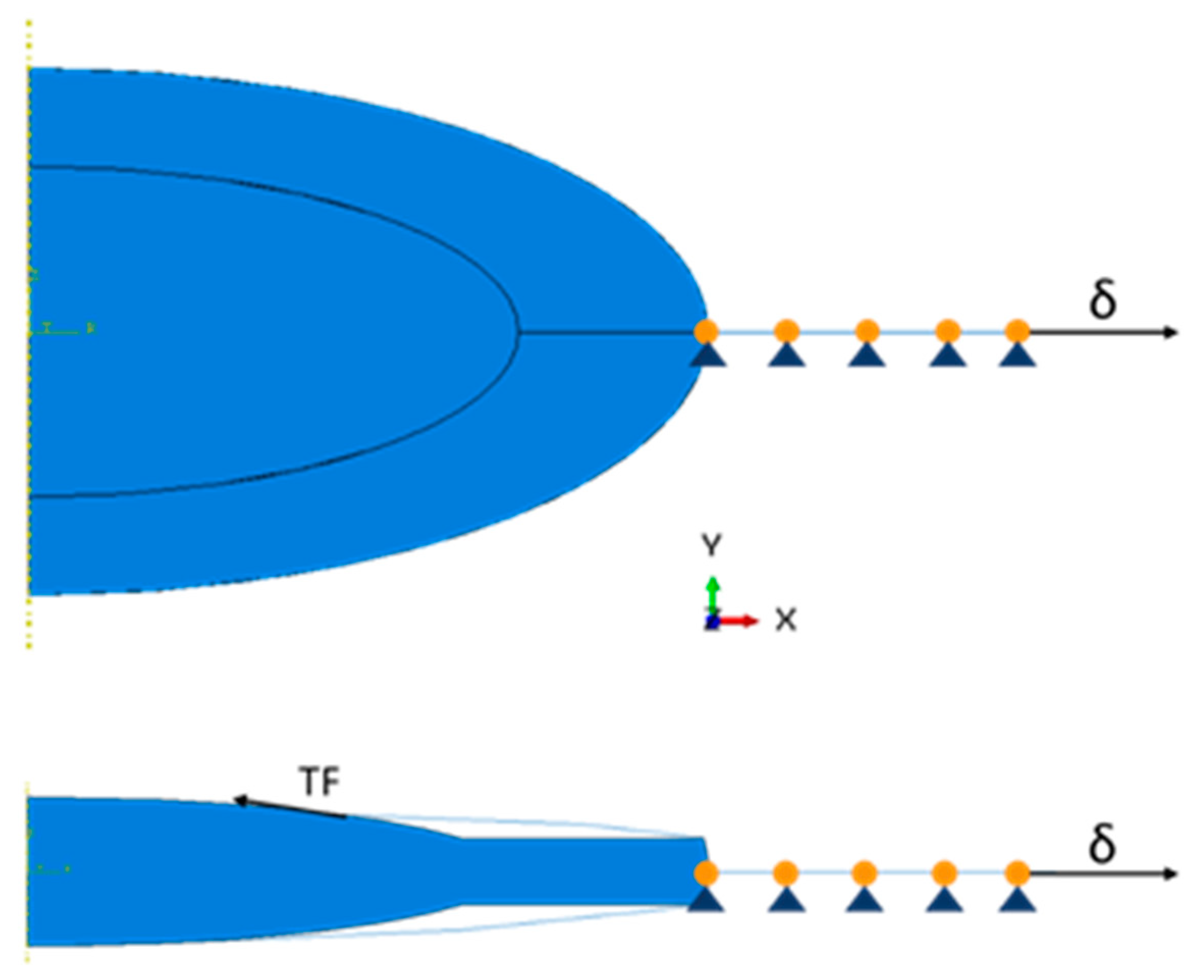
The increase of the traction force at the opening of the capsulorhexis showed a big influence in the distribution of stress in all of the models, increasing the stress in the IOL (principally in its optic) and decreasing the radial displacement, substantially. Even without knowing the in vivo values of the traction force at the edge of the capsulorhexis, it was relevant to study it to understand if the models built in this work were sensible to its variation. It was expected to observe an increase in average stress in the capsular bag and in the IOL, since these two parts were subjected to an increasing load in the opposite direction from that of the ciliary body relaxation. Furthermore, the natural fibrosis growing on the edge of the capsulotomy is understood to produce a centripetal force towards the center of its opening. This force is greater than the force exerted by the zonules, i.e., it could lead to the rupture of the zonular fibers and cause late IOL-capsular bag dislocation [
14,
33]. However, in this work, it was shown that an increase of this centripetal force, i.e., the traction force that was applied, did not influence the average stress in the zonules, even when it was higher than the resulting force in the zonules.
A small and large capsulorhexis, with 72.73% and 82.83% of the diameter of the IOL optic were compared and seemed to have a slight impact on the stresses of the model. With a smaller capsulorhexis it seemed possible to relieve some of the stress in the capsular bag and eventually avoid its rupture, with a consequent IOL dislocation. This outcome seemed to be contrary to the one given by Gimbel and co-workers that stated that a smaller capsulorhexis lead to a higher probability of incidence of IOL-capsular bag dislocation, because it developed more fibrosis than a large capsulorhexis [
34]. In this work, it was assumed that both large and small capsulorhexis had suffered the same level of natural fibrosis and that the resulting traction force on its edge was the same in both cases. For that same traction force, the smaller capsulorhexis seemed more favorable in giving support to the capsular bag.
The stress in the zonules doubled after surgery whereas in the capsular bag the same outcomes decreased significantly in most of the models. This is related to the increased stiffness in any IOL compared with the crystalline. The fact that the IOLs have a stiffness at least a thousand-times higher than the human crystalline lead to the IOLs supporting the capsular bag, shielding it from the native stress distribution. No parameter studied here lowered the general state of stress in the zonules post-surgery. The simplified geometry of the natural human crystalline lens model could have an impact on the distribution of stress in the capsular bag, but the outcomes of the pseudophakic eye models were not significantly altered. This is most likely associated with the shape alteration of the capsule after surgery, shrinking itself to the IOL.
Since this work presented an axisymmetric model, the IOLs were simplified to represent perfectly axisymmetric lenses, which is not the real configuration of the lens. The geometry of the IOLs could be improved in future works, as in 3D models with different types of asymmetric IOLs (one-piece, three-piece, or plate IOLs). Moreover, additional parameters could be studied to understand their influence in the overall stress along the different sections of the models, i.e., to study the influence of the gravity, the positioning of the IOL, the type of capsulotomy performed, and different densities of zonules (to mimic zonular dehiscence). In this study, the solid and fluid problems were completely decoupled, and the influence of the surrounding aqueous humor was not considered. Considering that the stresses measured in the crystalline lens and in the IOL are larger than those generated in the aqueous humor, a complementary computational fluid dynamics (CFD) study could also be performed to study the influence of the aqueous humor over the solid part of the model (CFD-FE coupled simulation) [
35]. In vivo values of the tensile strength of the zonules and the capsular bag would also have a great impact on the models, since it would be possible to replicate more realistic behaviors in these materials and to know when they would tear and lead to an IOL dislocation. This lack of in vivo information about the materials’ properties is a major limitation for works in this field, so the necessary parameters were sourced from in silico studies of the complete crystalline complex.
5. Conclusions
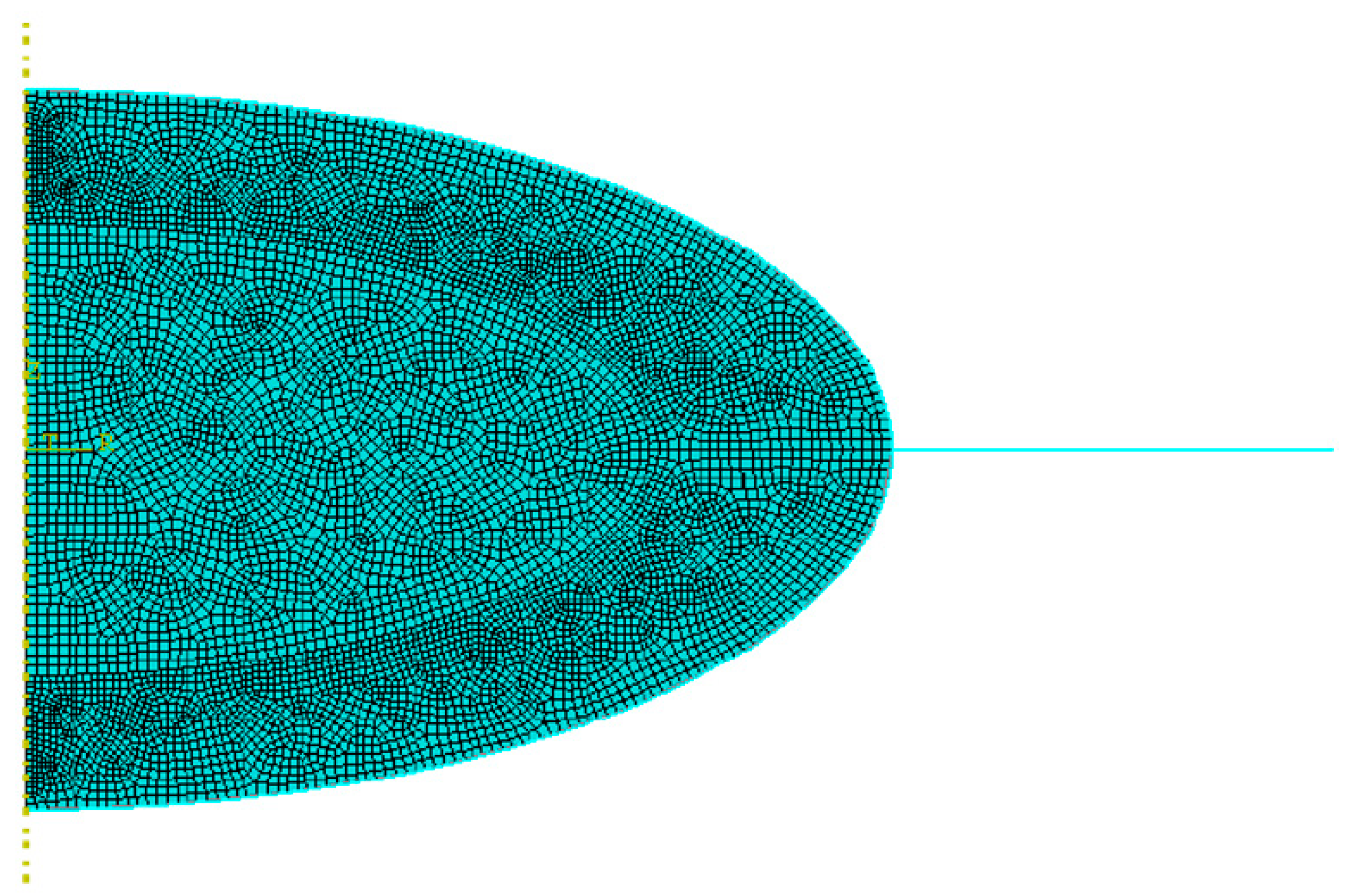
In this work, a human crystalline lens and its associated structures were discretized to an axisymmetric FE model, before and post-IOL implantation. As so, the models included the capsular bag and the zonular fibers, and pseudophakic eyes with a one-piece IOL. A radial displacement was applied at the tip of the zonular fibers to mimic the movement of the ciliary body during the process of disaccommodation.
The major finding from this work is that the variation of parameters in the pseudophakic models showed no significant impact on the zonules. It was important to verify the impact of the increase of the Young’s moduli of the IOLs, different diameters of capsulorhexis and increased traction force on the zonules, since their rupture is the main precursor of IOL-capsular bag dislocation. Since no significant alterations were observed, it is possible to speculate that a more realistic geometry of an IOL could have a greater influence on the outcomes of the simulations.
To the authors’ best knowledge, this is the first FE study addressing the eye under cataract surgery. Notwithstanding the model limitations, the outcomes presented here can be an important complement for the existing studies on the crystalline complex, both on clinical practice and biomechanics research.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}