Abstract
The forefoot plays an important role in providing body support and propulsion during walking. We investigated the effect of forefoot dysfunction on the gait pattern of a young adult with partial bilateral amputation of the toes. We measured our participant’s gait kinematics during barefoot and shod overground walking and analysed time-distance and joint range of motion (RoM) parameters against a group of healthy adults. Forefoot dysfunction gait is improved by footwear and walking experience; however, this improvement was still remarkably different (exceeded 95% CI) when compared to healthy gait at matching walking speed. Compared to healthy gait, walking barefoot had a slower speed and a 30% reduction in ankle and knee joint RoM, but a larger hip RoM. Shod gait resulted in a remarkable increase in ankle RoM and walking speed compared to barefoot gait. These results are consistent with the important role of the forefoot (tarsals and metatarsophalangeal joints) and suggest that footwear can facilitate gait function following toe amputation.
1. Introduction
The human foot is formed from numerous bones and ligaments, supports body weight and also serves as a lever to propel the body forward [1]. Two of the three major segments of the foot, the midfoot (arch structure) and forefoot (toes), have been identified as critical in gait because of the large range of motion displayed in the ankle and proximal interphalangeal joint. There are additional sources of deformation, such as the soft tissue on the plantar surface, as well as the longitudinal and transverse arches formed by numerous bones and ligaments [1,2]. Sensory information from numerous receptors in the foot is used to control movement and posture [2,3,4]. Furthermore, there is a specific timing of activation of intrinsic foot muscles during walking, different from that of extrinsic foot muscles [5]. Accordingly, changes in the foot’s structure may significantly impair its function during locomotion.
Previous studies examining forefoot dysfunction gait have focused on the assessment and treatment of conditions, such as hallus valgus [6,7], rheumatoid arthritis [8], claw toe [9], and diabetic neuropathy [10]. These studies show that patients with forefoot dysfunction tend to walk slower, with reduced step length, increased double-stance period, decreased ankle push-off power, and increased gait instability, when compared to healthy gait. Thus, deformity, pain and stiffness of the forefoot may cause significant disturbances of gait. An interesting case of forefoot dysfunction is amputation of the toes, which provides one way to further our understanding of the functional role of the toes during locomotion. Frostbite of the extremities is a common injury among alpinists participating in high altitude expeditions, particularly during inclement weather conditions. Frostbite is the most serious peripheral injury and can be classified as superficial or deep. In superficial frostbite, the skin loses sensibility and becomes white, and blister formation may follow. Deep frostbite involves necrosis of muscle and bone, in addition to the skin and subcutaneous tissue [11]. It mostly results in some form of amputation. The risk of frostbite is mostly related to the most peripheral parts of the body, especially toes and fingers. To our knowledge, there are no studies that have investigated the effect of frostbite leading to toe amputation on gait performance. Such investigations may contribute to our understanding of both the function of the forefoot [1,12] and inherent relationships between gait parameters and limb segment proportions [13].
Recent research has demonstrated that wearing athletic footwear (designed to increase sole thickness, providing cushioning against impacts) interferes with the functional ability of the human foot during walking. Walking barefoot compared to shod results in a reduced step and/or stride length [14,15,16,17,18], increased cadency [14,16,17], decreased double support time [14], decreased stance time [14,16,19], increased swing time [16], and decreased stride time [14,17]. Gait velocity differences between barefoot and footwear conditions revealed a decrease in velocity when barefoot [14,16]. Walking barefoot also led to a change in the ankle angle at initial contact, with a significant increase in plantarflexion corresponding to a flatter foot placement compared to athletic shoes, sandals, and flip-flops [15,19,20]. Footwear also appears to alter knee kinematics. An increase in knee flexion is observed at contact when walking barefoot [15,19], but a greater knee and ankle RoM exists throughout stance when wearing footwear [19]. Comparing the impact of shod versus barefoot walking after toe amputations may also provide important information for the development of prosthetic feet to facilitate locomotor functions.
We aimed to contribute to the understanding of the function of the human foot with a case report on gait performance in a young adult male with partial bilateral amputation of the toes following severe foot injury caused by frostbite. Our first goal was to investigate the gait kinematics, particularly flexion and extension range of motion (RoM)at the ankle, knee and hip. Since the use of footwear might affect gait characteristics [21], our second goal was to compare barefoot walking and walking in athletic shoes that partially restored normal proportions/integrity of the distal part of the foot and its elasticity.
2. Materials and Methods
2.1. Participant
The participant was a Caucasian 30-year-old male (height: 1.86 m; mass: ~82 kg). In November 2010, the participant’s right and left toes were amputated after severe frostbite. Data collection occurred 15 months (session 1), 6 years (session 2) and 8 years (session 3) after surgery. With respect to the right foot, surgery removed half of distal phalanx of great toe and half of the distal phalanx of 2nd and 3rd toes. With respect to the left foot, surgery removed the distal phalanx and 1/3 proximal phalanx of the great toe; distal and medial phalanx of the 2nd, 3rd, and 4th toes; and distal phalanx of the fifth toe (Figure 1). The subject reported a preference to wear shoes, even at home, since it is subjectively more stable and comfortable for him to walk in shoes rather than barefoot. The subject gave written informed consent. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved bythe Regional Bioethics Committee (registration no. 139/KBL/OIL/2011).
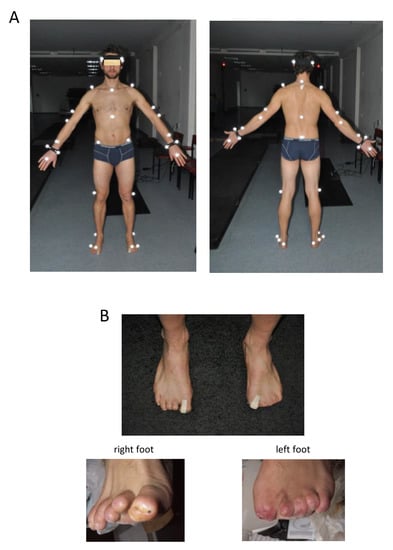
Figure 1.
Marker set for gait recordings (A) and left and right foot after amputation of the toes (B). Written informed consent was obtained from the individual for the publication of this image.
2.2. Data Recording and Analysis
The gait test involved over-ground walking along a 12-m walkway at a natural (self-selected) speed. The subject started walking 1.5 m before entering the motion capture volume in order to eliminate the initial steps. In session 1, walking trials were separated by footwear condition: barefoot and shod (participant’s athletic shoes). Eight trials were recorded in each footwear condition, where between two and four strides were obtained for each trial. In sessions 2 and 3, the experiment was conducted barefoot. The gait analysis was performed using a 5-camera video-based (120 Hz sampling rate) motion analysis system (Vicon 250; Oxford Metrics Ltd.; Oxford, UK). Thirty-five infrared reflective markers were attached to the body of the subject according to the Golem set-up: 4 were placed on the head, 4 on the trunk, 3 on the pelvis, 7 on each of the upper, and 5 on each of the lower limbs (Figure 1A). In the shod condition, 4 markers were placed on the shoe surface as close as possible to the original (barefoot) position. Since amputation of the toes was somewhat asymmetrical (the left foot was more severely affected, Figure 1), we recorded and analysed the kinematics of both the right and left legs.
The following parameters were calculated for each stride: walking speed, cadence, stride length and sagittal plane range of angular motion (RoM) at the ankle, knee and hip joints. The RoM was determined by the difference between the maximum and minimum joint angles that occurred during a full gait cycle. Due to asymmetrical amputation of the toes (Figure 1B), one could expect asymmetrical adjustments in the RoM across different joints of both legs. A simple measure for asymmetry index (ASI) [22] was used to assess the RoM differences between the left (L) and right (R) limbs:
An ASI = 0 represents perfect symmetry, while values greater than 10% have clinical relevance [23].
The data from the literature served as the patient’s control to illustrate differences in gait kinematics between our participant and a group of healthy young adults. During shod walking at a natural speed, our subject was compared to the data published by Perry [24]. During barefoot walking, we used the previous recordings of gait kinematics in a sample of healthy adults (n = 20) walking barefoot at different speeds [25,26] and chose only those strides that corresponded to the range of speeds 1 to 1.4 m/s for the comparison with the patient’s data. Note that the height and mass of our subject falls within the 95% confidence interval of those in the control group.
2.3. Statistical Analysis
Descriptive statistics included means ± SD. Student’s t-tests were used to show how footwear condition affects kinematics and to compare the RoM between the right and left leg joints. Significance was set at p < 0.05. To assess how the kinematics deviate from normal population, a one-tailed t-test was used to evaluate whether the mean joint RoM at the ankle, knee and hip exceeds the 95% confidence interval of a speed-matched sample (n = 20) of healthy (barefoot)gait.
3. Results
General gait parameters (session 1) are illustrated in Figure 2A and Table 1. The walking speed and stride length (session 1) were significantly smaller during barefoot versus shod walking (p < 0.001 for both parameters, Student’s t-test). Overall, the patient’s self-selected speed tended to be slower in both footwear conditions with respect to that of normal population (Figure 2A).
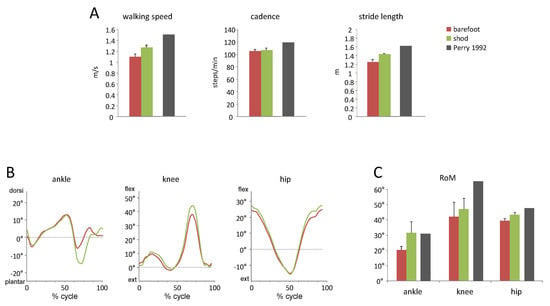
Figure 2.
Gait parameters at a natural speed in two footwear conditions: barefoot and shod (session 1). (A)—walking speed, cadence and stride length (mean + SD). (B)—ensemble-averaged angular waveforms of the ankle, knee, and hip joint oscillations of the right leg. The data are plotted versus the normalised gait cycle. (C)—range of motion (RoM) in the ankle, knee and hip joints. For comparison in panel (A) and (C), we plotted the published data of Perry (1992, [24]), who described healthy population during shod walkingat natural speed (grey bars).

Table 1.
Natural barefoot walking speed, cadence and stride length (mean ± SD) in sessions 1, 2, and 3 and the corresponding normative values of Perry [24].
The patient showed significantly smaller amplitudes of motion in all lower limb joints during walking barefoot in comparison with shod walking (all p < 0.001, Figure 2C). In particular, barefoot walking was associated with reduced plantarflexion in the ankle joint during push-off and reduced flexion in the knee and hip joints during swing (Figure 2B). Thus, wearing shoes resulted in faster self-selected walking speeds and larger amplitudes of angular motion.
The RoM in both footwear conditions was smaller compared to healthy gait (Figure 2A). However, since the kinematic parameters can be compromised by the effect of walking speed [27], we performed comparisons at matching speeds. Figure 3A illustrates the RoM of all strides analysed in the patient (n = 54 strides) and healthy subjects (n = 167 strides) as a function of walking speed.
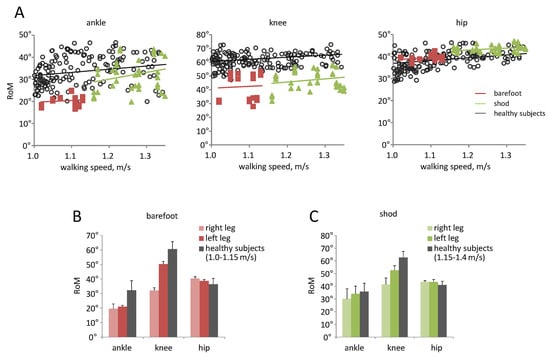
Figure 3.
Range of motion in the ankle, knee and hip joints in the patient (session 1) and in healthy subjects. For comparison, we also plotted the data for healthy subjects walking barefoot previously published in [25,26]. (A)—RoM as a function of walking speed. Each point represents the value for the individual stride. The data for the left and right leg in the patient were pooled together. Linear regression lines are also illustrated. (B)—RoM (mean + SD) in the patient during barefoot walking and in healthy subjects at matched walking speeds 1.0–1.15 m/s. The data for the left and right leg were shown separately. (C)—RoM in the lower limb joints in the patient during shod footwear condition and in healthy subjects at matched walking speeds 1.15–1.40 m/s.
There were some asymmetries in gait kinematics (e.g., in the knee RoM, Figure 3B,C), likely as a result of asymmetrical amputation of the toes (Figure 1B). The ASI values are indicated in Table 2. Interestingly, a more severe toe amputation in the left foot was accompanied by a significant reduction in the knee RoM of the contralateral (right) leg (p < 0.001, Figure 3B). The hip RoM ASI was below 5%, and therefore considered as ‘not clinically relevant’. Nevertheless, despite some asymmetries, the patient showed significantly smaller oscillations of the ankle and knee joints of both legs than healthy subjects walking barefoot at matching speeds (p < 0.05 for both angles, one-tailed t-test), while the amplitude of the hip joint angle slightly increased (Figure 3B). Walking in shoes increased the ankle RoM, while it reduced RoM and asymmetry at the knee (Figure 3C, Table 2).
Table 2.
Asymmetry indices (ASI) in the ankle, knee, and hip joints (mean ± SD).
In sessions 2 and 3, the participant showed an improved gait (Table 1 and Table 2). For instance, the self-selected walking speed, cadence, and stride length during barefoot walking were similar to those of the normal population [24], and the ASI values decreased significantly with respect to those in the first session (Table 2).
The range of motion in the knee joint (58.7° ± 2.1°) during the second session came to be similar, while the RoM in the hip (47.4° ± 3.3°) and ankle (25.3° ± 1.9°) joints remained increased and reduced, respectively, with respect to those of normal population (Figure 3A,B) when comparing at matched speeds. In the third session, gait parameters and ASI values were similar to those in session 2 (Table 1 and Table 2).
4. Discussion
The results of this study show that partial amputation of the toes contributes to the deviation from a healthy kinematic gait pattern. The role of the foot–ankle complex can be described during three sub-phases of stance: the weight acceptance (heel rocker), the upright posture support (ankle rocker), and the forward progression (forefoot rocker). Our participant’s condition mainly affects the second and third sub-phases, because the forward progression of foot pressure is restricted to the length of the foot. As a result, ankle joint torque and forward propulsion are compromised. To overcome these biomechanical restrictions, the locomotor control system may undertake compensation behaviour. This study reveals compensations for lower-limb joint range of motion in a forefoot partial amputation.
One limitation of our study is the small number of recruited patients. Nevertheless, such rare cases may provide interesting information about locomotor body scheme and inherent relationships between gait parameters and limb segment proportions [13]. This case study was also chosen because we were interested in the long-term process of gait performance adaptation following amputation of the toes (performing the follow up study 6–8 years after surgery). To our knowledge, there are no empirical data available for such a case.
The function of the forefoot in humans is specifically adopted for bipedal walking. Human bipedality was made possible by the redesign of an ancestral foot, with five long toes for the limbs of trees [28]. Their main role is to enlarge the weightbearing area so that, when the heel is raised, full body weight is not taken on the metatarsal heads alone [12]. The great toe is the final element (except for the Morton form of the foot, i.e., when the 1st metatarsal is shorter than the 2nd metatarsal [1]) in a chain of events to transfer body weight and provide propulsion during gait. By differential contraction of the flexors of the toes, it is possible to adjust the distribution of pressure between parts of the foot and any deformities and forefoot disfunction leading to the reduction in the function of the toes. Nevertheless, the link between ankle joint RoM and the function of the midfoot and forefoot is not obvious.
Forefoot dysfunction caused by partial amputation of the tarsals resulted in significant reduction in walking speed, stride length and ankle joint RoM (Figure 2 and Figure 3). The results are in accordance with previous studies [7] showing that forefoot dysfunction induces changes to the proximal joints. In particular, reduction in the ankle RoM was accompanied by a decrease in knee RoM and greater hip RoM when compared to healthy gait at matched walking speeds (Figure 3). Asymmetrical toe amputation also resulted in clinically relevant ASI values for knee joint RoM (Table 2). Finally, walking experience and training may account for a partial gait adaptation in the follow-up study. Our subject, a member of a mountain rescue team, came back to regular training (running, climbing, skiing) 2 years following amputation, which represented a great treatment for improving his locomotion capacities. For instance, the index of asymmetry has been considerably diminished during the second session (Table 2) even though the RoM of the ankle joint remained smaller than that of healthy subjects during walking barefoot.
As angular movements are not independent of each other, the observed locomotor adjustments and compensation (Figure 2 and Figure 3) can be related to dynamic coupling between limb segments [29] and inherent relationships between gait parameters and limb segment proportions [13]. The perception and control of movement may also rely on a priori knowledge about intrinsic dynamics of limb segment motion and inherent relationships between gait parameters and limb segment proportions [13]. For instance, a relative increment in the shank segment length with respect to the foot segment (due to surgery or using stilts [30,31]) produces similar locomotor adjustments in the relative amplitude of limb joint angles, namely: decrements in the ankle and knee RoM and increments in the hip RoM. Minimum and safe foot clearance during swing represents a precise endpoint control task for the minimisation of trip-related falls [27,32,33] and also relies on a priori knowledge about inherent limb segment proportions. Thus, even small changes in the relative length of limb segments might affect the endpoint (foot) trajectory control.
Since the toes are responsible for enlarging the weightbearing area during walking, it can be assumed that the differences noted between walking after amputation and healthy gait may also be associated with a greater risk of losing stability. A more precautious gait is manifested by slower speed, shorter steps, and reduction in the ankle joint amplitude. Finally, the results show the rationale for the use of footwear to provide more comfortable gait [22]. Walking in shoes resulted in faster speeds and increased RoM (Figure 2 and Figure 3). Recent research has demonstrated that walking in footwear is associated with an increase in stride length [14], and greater dorsiflexion at foot-ground contact [15,20].
Overall, the development of assistive technologies, such as prosthetic feet, may benefit from a better understanding of the role of the toes for both stability and reduction in fatigue-related challenges experienced by amputees [34].
Author Contributions
Conceptualisation, W.F.-K., A.K., and Y.I.; methodology, W.F.-K., Y.I.; software, G.C., A.H.D.; validation, S.T. and G.C.; formal analysis, Y.I.; investigation, W.F.-K., A.K., and G.C.; data curation, W.F.-K., G.C.; writing—original draft preparation, W.F.-K., S.T., and Y.I.; writing—review and editing, S.T., A.H.D., and Y.I.; visualisation, Y.I.; supervision, Y.I.; project administration, W.F.-K. and G.C.; funding acquisition, W.F.-K. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the Polish Ministry of Science and Higher Education (Project No 66 /MN/IBN/2014) and Italian Ministry of Health (IRCCS Fondazione Santa Lucia RicercaCorrente). The APC is supported under the programme established by the Ministry of Science and Higher Education, named “Regional Initiative of Excellence”, spanning the period 2019–2022 (Project No 022/RID/2018/19, amount of financing: PLN 11 919 908 PLN).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Regional Bioethics Committee (registration no. 139/KBL/OIL/2011).
Informed Consent Statement
Written informed consent has been obtained from the subject to publish this paper.
Data Availability Statement
Data may be made available by contacting the corresponding author.
Acknowledgments
We are grateful to our subject who volunteered to participate in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Morton, D.J. The Human Foot: Its Evolution, Physiology and Functional Disorders; Columbia University Press: New York, NY, USA, 1935. [Google Scholar]
- Wright, W.G.; Ivanenko, Y.P.; Gurfinkel, V.S. Foot anatomy specialization for postural sensation and control. J. Neurophysiol. 2012, 107, 1513–1521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kavounoudias, A.; Roll, R.; Roll, J.P. The plantar sole is a ‘dynamometric map’ for human balance control. Neuroreport 1998, 9, 3247–3252. [Google Scholar] [CrossRef] [Green Version]
- Fallon, J.B.; Bent, L.R.; McNulty, P.A.; Macefield, V.G. Evidence for strong synaptic coupling between single tactile afferents from the sole of the foot and motoneurons supplying leg muscles. J. Neurophysiol. 2005, 94, 3795–3804. [Google Scholar] [CrossRef] [Green Version]
- Zelik, K.E.; La Scaleia, V.; Ivanenko, Y.P.; Lacquaniti, F. Coordination of intrinsic and extrinsic foot muscles during walking. Eur. J. Appl. Physiol. 2015, 115, 691–701. [Google Scholar] [CrossRef]
- Nix, S.E.; Vicenzino, B.T.; Collins, N.J.; Smith, M.D. Gait parameters associated with hallux valgus: A systematic review. J. Foot Ankle Res. 2013, 6, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shih, K.-S.; Chien, H.-L.; Lu, T.-W.; Chang, C.-F.; Kuo, C.-C. Gait changes in individuals with bilateral hallux valgus reduce first metatarsophalangeal loading but increase knee abductor moments. Gait Posture 2014, 40, 38–42. [Google Scholar] [CrossRef]
- Laroche, D.; Ornetti, P.; Thomas, E.; Ballay, Y.; Maillefert, J.F.; Pozzo, T. Kinematic adaptation of locomotor pattern in rheumatoid arthritis patients with forefoot impairment. Exp. Brain Res. 2007, 176, 85–97. [Google Scholar] [CrossRef]
- Bus, S.A.; Maas, M.; Michels, R.P.J.; Levi, M. Role of intrinsic muscle atrophy in the etiology of claw toe deformity in diabetic neuropathy may not be as straightforward as widely believed. Diabetes Care 2009, 32, 1063–1067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sacco, I.C.N.; Hamamoto, A.N.; Tonicelli, L.M.; Watari, R.; Ortega, N.R.; Sartor, C. Abnormalities of plantar pressure distribution in early, intermediate, and late stages of diabetic neuropathy. Gait Posture 2014, 40, 570–574. [Google Scholar] [CrossRef]
- Ward, M.P.; Garnham, J.R.; Simpson, B.R.; Morley, G.H.; Winter, J.S. Frostbite: General observations and report of cases treated by hyperbaric oxygen. Proc. R. Soc. Med. 1968, 61, 787–789. [Google Scholar] [PubMed]
- Hughes, J.; Clark, P.; Klenerman, L. The importance of the toes in walking. J. Bone Joint Surg. Br. 1990, 72, 245–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ivanenko, Y.P.; Dominici, N.; Daprati, E.; Nico, D.; Cappellini, G.; Lacquaniti, F. Locomotor body scheme. Hum. Mov. Sci. 2011, 30, 341–351. [Google Scholar] [CrossRef] [PubMed]
- Lythgo, N.; Wilson, C.; Galea, M. Basic gait and symmetry measures for primary school-aged children and young adults whilst walking barefoot and with shoes. Gait Posture 2009, 30, 502–506. [Google Scholar] [CrossRef]
- Oeffinger, D.; Brauch, B.; Cranfill, S.; Hisle, C.; Wynn, C.; Hicks, R.; Augsburger, S. Comparison of gait with and without shoes in children. Gait Posture 1999, 9, 95–100. [Google Scholar] [CrossRef]
- Moreno-Hernández, A.; Rodríguez-Reyes, G.; Quiñones-Urióstegui, I.; Núñez-Carrera, L.; Pérez-SanPablo, A.I. Temporal and spatial gait parameters analysis in non-pathological Mexican children. Gait Posture 2010, 32, 78–81. [Google Scholar] [CrossRef]
- Wolf, S.; Simon, J.; Patikas, D.; Schuster, W.; Armbrust, P.; Doederlein, L. Foot motion in children shoes—A comparison of barefoot walking with shod walking in conventional and flexible shoes. Gait Posture 2008, 27, 51–59. [Google Scholar] [CrossRef]
- Keenan, G.S.; Franz, J.R.; Dicharry, J.; Della Croce, U.; Kerrigan, D.C. Lower limb joint kinetics in walking: The role of industry recommended footwear. Gait Posture 2011, 33, 350–355. [Google Scholar] [CrossRef]
- Zhang, X.; Paquette, M.R.; Zhang, S. A comparison of gait biomechanics of flipflops, sandals, barefoot and shoes. J. Foot Ankle Res. 2013, 6, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morio, C.; Lake, M.J.; Gueguen, N.; Rao, G.; Baly, L. The influence of footwear on foot motion during walking and running. J. Biomech. 2009, 42, 2081–2088. [Google Scholar] [CrossRef] [PubMed]
- Fong Yan, A.; Sinclair, P.J.; Hiller, C.; Wegener, C.; Smith, R.M. Impact attenuation during weight bearing activities in barefoot vs. shod conditions: A systematic review. Gait Posture 2013, 38, 175–186. [Google Scholar] [CrossRef]
- Aruin, A.S.; Kanekar, N. Effect of a textured insole on balance and gait symmetry. Exp. Brain Res. 2013, 231, 201–208. [Google Scholar] [CrossRef]
- Patterson, K.K.; Gage, W.H.; Brooks, D.; Black, S.E.; McIlroy, W.E. Evaluation of gait symmetry after stroke: A comparison of current methods and recommendations for standardization. Gait Posture 2010, 31, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Perry, J. Gait Analysis: Normal and Pathological Function; SLACK Incorporated: Thorofare, NJ, USA, 1992; ISBN 978-1-55642-192-1. [Google Scholar]
- Cappellini, G.; Ivanenko, Y.P.; Dominici, N.; Poppele, R.E.; Lacquaniti, F. Motor patterns during walking on a slippery walkway. J. Neurophysiol. 2010, 103, 746–760. [Google Scholar] [CrossRef] [Green Version]
- Martino, G.; Ivanenko, Y.P.; Serrao, M.; Ranavolo, A.; d’Avella, A.; Draicchio, F.; Conte, C.; Casali, C.; Lacquaniti, F. Locomotor patterns in cerebellar ataxia. J. Neurophysiol. 2014, 112, 2810–2821. [Google Scholar] [CrossRef]
- Ivanenko, Y.P.; Grasso, R.; Macellari, V.; Lacquaniti, F. Control of Foot Trajectory in Human Locomotion: Role of Ground Contact Forces in Simulated Reduced Gravity. J. Neurophysiol. 2002, 87, 3070–3089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elftman, H. Dynamic structure of the human foot. Artif. Limbs 1969, 13, 49–58. [Google Scholar]
- Zajac, F.E.; Neptune, R.R.; Kautz, S.A. Biomechanics and muscle coordination of human walking: Part II: Lessons from dynamical simulations and clinical implications. Gait Posture 2003, 17, 1–17. [Google Scholar] [CrossRef]
- Dominici, N.; Daprati, E.; Nico, D.; Cappellini, G.; Ivanenko, Y.P.; Lacquaniti, F. Changes in the limb kinematics and walking-distance estimation after shank elongation: Evidence for a locomotor body schema? J. Neurophysiol. 2009, 101, 1419–1429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, J.C.; Noble, J.W.; Prentice, S.D. Locomotor strategies in response to altered lower limb segmental mechanical properties. Hum. Mov. Sci. 2011, 30, 1199–1209. [Google Scholar] [CrossRef] [PubMed]
- Begg, R.; Best, R.; Dell’Oro, L.; Taylor, S. Minimum foot clearance during walking: Strategies for the minimisation of trip-related falls. Gait Posture 2007, 25, 191–198. [Google Scholar] [CrossRef]
- Winter, D.A. Foot trajectory in human gait: A precise and multifactorial motor control task. Phys. Ther. 1992, 72, 45–53; discussion 54–56. [Google Scholar] [CrossRef] [PubMed]
- Grabowski, A.M.; Rifkin, J.; Kram, R.K. Promoter TM Prosthetic Foot Reduces the Metabolic Cost of Walking for Unilateral Transtibial Amputees. JPO J. Prosthet. Orthot. 2010, 22, 113–120. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).