Abstract
There is a significant need for a computer-aided modeling, effective information analysis and ontology knowledge base models to support both special needs children and care providers. As this research work correlated to the symmetry scope, it proposes an innovative generic smart knowledge-based “School Care Coordination System” (SCCS), which is established on a novel holistic six-layered data management model. The development of the Smart-SCCS adopts a methodology of ontology engineering to transform the given theoretical unstructured special educational needs and disabilities (SEND) code of practice into a comprehensive knowledge representation and reasoning system. The intended purpose is to deliver a system that can coordinate and bring together education, health and social care services into a single application to meet the needs of children and young people (CYP) with SEND. Moreover, it enables coordination, integration and monitoring of education, health and social care activities between different actors (formal, informal and CYP in the education sector) involved in the school care process network to provide personalized care interventions based on a predefined care plan. The developed ontology knowledge-based model has been proven efficient and solved the enormous difficulties faced by schools and local authorities on a daily basis. It enabled the coordination of care and integration of information for CYP from different departments in health, social care and education. The developed model has received significant attention with great feedback from all the schools and the local authorities involved, showing its efficiency and robustness.
1. Introduction
The status of children and young people (CYP) with a special educational needs (SEN) has been transformed over the past 140 years [1]. Previously, most CYP with SEN were not valued members of their local school’s community; they were institutionalized and considered “ineducable”. Decades of social and legislative changes have resulted in the education of CYP with SEN becoming a vital topic within educational and political debate [2]. Since the beginning of September 2014, a new Special Educational Needs and Disabilities (SEND) Code of Practice (CoP) [3] was introduced in the United Kingdom (UK) for CYP. It provides statutory guidance on policies, procedures and duties relating to Part 3 of the Children and Families Act 2014 [4] which is related to CYP who have SEN and/or disabilities. All maintained educational settings, academies, local authorities (LAs), the National Health Service (NHS), Clinical Commissioning Group (CCG) and local health and social care partners, as well as other public bodies, must follow this new CoP.
Additionally, the education systems have been under a great deal of pressure in recent years to improve the quality of education, care, efficiency and achievement for CYP with SEND as well as reduce the cost of care. Therefore, this has led to the initiation of an integrated “Education, Health and Care Plan” (EHCP), which is a statutory document. It specifies the health, education and care support provided to CYP who have been identified to have SEND. The LA prepares it after an EHCP needs assessment with relevant partner agencies, parents and the CYP themselves [5]. The three main recommendations for SEND and the EHCP incorporated in the CoP [6] are:
- CYP and their carers or parents will have full involvement and better control in the decisions made regarding the type of provision and support they will require to meet the difficulties they face with health, education and/or social care services. The setup of additional support meeting these needs is recommended.
- The educational system needs to be person-centered for CYP, focusing on high aspirations, including life skills, employment, greater independence and support to remain in place up to the age of 25 where appropriate.
- The development of a multi-professional partnership between health, education and social care to deliver joined-up services. Professionals (formal care providers) are required to work together when guiding the joint planning and commissioning of services to ensure close cooperation.
These recommendations are regarded as the most significant in the last two decades. However, the Department for Education (DfE) has not produced a national generic “blueprint” for EHCP or supporting processes. It is up to individual pathfinder areas (local authorities of different boroughs) to design, pilot and implement their tools and procedures according to local rules, availability of provision and funding. Therefore, there is an apparent gap between the theoretical approach and the practical implementation of the new SEND CoP across different local authorities, school settings, CCG and other organizations involved in providing care to CYP.
The main objective of this research work is the proposal of the development of an innovative information infostructure to model and implement a smart generic “School Care Coordination System” (SCCS). It is based on a recommended design of an original holistic “six-layered data management model” Smart-SCCS that adopts a methodology of ontology engineering. This method transforms the given theoretical unstructured SEND code of practice and EHCP into a comprehensive knowledge representation and reasoning system, to support and bring together education, health and social care services into a single application. Additionally, it coordinates, integrates and monitors education, health and social care activities between different actors (formal, informal and SEND students) involved in the school care (SC) process network. It also provides personalized care interventions for CYP with SEND that already have a predefined EHCP. For example, if a CYP is scheduled to have intervention from a specific speech therapist who is unable to carry out the required intervention or is unavailable to participate, then there will be a procedure to allow the system to find a replacement with a similar profile and expertise level as the therapist that was unable to complete the designated intervention. In other words, it can generate rules and procedures to enable re-coordination of care providers to manage interventions when unexpected events deviate from the predefined EHCP.
This research intends to set the foundation for further research into this combined field, as there is a huge demand for a computer-aided modeling, effective information analysis and ontology knowledge-based models to support both the special needs children and the care providers. The aim is to create cultural change to help organize and operate the new shift in the education system to enable SEND CYP to meet their full potential in mainstream schools or any other educational settings.
2. Literature Review and State of the Art
The process and the surrounding legislation for the implementation of the new SEND CoP [7] are relatively new and are subject to local variation, depending on the existing philosophies, resources and practices. According to the latest findings published by the National Audit Office (NAO) in September 2019 [8], 1.3 million CYP in England have been identified as having SEND. This has increased the demand for support, and legal entitlements to support packages specific to needs were set out in the education, health and care plans (EHCPs) for approximately 20.6% of CYP. These are CYP whom LAs have assessed as having complex needs and require a higher amount of support. At the same time, nearly half (47.9%) of CYP were attending mainstream schools, with the remainder of CYP attending special schools.
Figure 1 [8] illustrates the number of LAs overspending according to their high-needs budgets from 2013 to 2018, and it is increasing each year, as can be seen from the graph. Funding of GBP 9.4 billion by the DfE was provided to support CYP with SEND in 2018–2019. Despite the high funding by the DfE, 81.3% of LAs have overspent their high-needs budget; this shows the magnitude of the fragmented implementation of the new SEND CoP due to schools being unable to meet their needs.
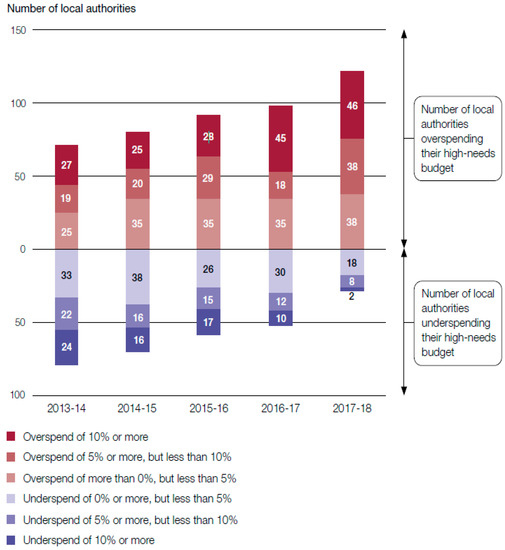
Figure 1.
Spending against high-needs budgets by local authorities (LAs).
2.1. Types of SEND Identified in CoP 2014
There are four primary areas of difficulties (disabilities) that have been classified in the latest SEND CoP 2014 for CYP with SEND, as summarized in the following sections.
2.1.1. Communication and Interaction
CYP with speech, language and communication needs (SLCN) are categorized into this area of need, for example, children with autistic spectrum disorder (ASD) or children with a stutter. It is difficult for children who are categorized in this area of need to express themselves appropriately to others through means of verbal communication. Meanwhile, ASD children find it challenging to perform typical behaviors [9] and instead demonstrate behaviors that are classified as unusual, such as displaying aggression and odd mannerisms or obsessively repeating actions [10].
2.1.2. Cognition and Learning
This area of need includes CYP with learning difficulties, where the individual finds it too challenging to understand either complex information or new information and therefore struggles to pick up new skills and cope on their own [11]. There is a variety of mild and profound learning difficulties ranging from Specific Learning Difficulties (SpLDs) to profound and multiple learning difficulties (PMLDs) [12]. Therefore, as an oversight, it is thought that children with cognition and learning skills require educational provision from schools so that they can work towards their best potential [13].
2.1.3. Sensory and/or Physical Needs
CYP who have physical or sensory impairments are categorized in this area of need, for example; cerebral palsy, vision loss, epilepsy or spina bifida. So that children are included and grouped under the SEND umbrella, they will require additional educational provision, and without the support of this provision they will find it difficult to access educational resources [7]. These CYP must prove that their disability has a direct impact on their learning for them to receive support; otherwise, they will not automatically receive additional education provision [7].
2.1.4. Social, Emotional and Mental Health Difficulties
Social, emotional and behavioral needs were categorized as the final area of need before September 2014, but were removed in the revision [3]. Social, emotional and mental health difficulties have now replaced them, including CYP who have a variety of issues that are displayed in several different ways, for example: being withdrawn and/or exhibiting behaviors that are disruptive, seen as disturbing and found to be challenging [3]. The new SEND documentation discusses that the mentioned behaviors “reflect underlying mental health difficulties”, so rather than diagnosing the behaviors themselves, they should be investigated and supported [3]. For example, the Department for Education and the Department of Health have stated that mental health illnesses such as depression, anxiety, eating disorders, substance misuse, self-harming or other medically unexplained symptoms can potentially lead to negative behaviors. This is why it is of high importance to find the root cause to aid in supporting CYP to overcome these behaviors, instead of concentrating only on changing their behaviors.
The four classified difficulties (disabilities) identified for CYP with SEND demonstrates the diverse challenges schools are facing when providing support to these individuals. Therefore, having Smart-SCCS as a managing system will not only coordinate and integrate health and social care services with education settings to support these individuals, but it will also simplify complex needs and provide timely support to CYP when needed.
2.2. Current Issues with the New SEND CoP and EHCP
To the best of the authors’ knowledge, there are no intelligent frameworks or systems currently implemented in the education system using semantic web technologies, i.e., ontology engineering to coordinate, integrate and manage health, education and social care interventions (activities) in the school care setting for CYP with SEND. However, there are four particular care management systems implemented in the homecare domain for elderly people that use ontology-driven approaches, which can be summarized as follows:
The “Open Architecture for Accessible Services Integration and Standardization” (OASIS) [14] is a reference system and architecture which enables and facilitates interoperability, faultless connectivity and content sharing among different ontologies and services in the entire domain ontology applicable to applications meant for the elderly population [15]. Meanwhile, the European project “Knowledge-based Homecare eServices for an Ageing Europe” (K4Care) [16] aims to design, implement and validate an innovative ICT knowledge-based homecare model using mainly semantic web technologies.
The third one is “Mobilizing Advanced Technology for Care at Home” (MATCH) [17], which aims to develop an infrastructure system to support independent living at home by implementing improved methods to connect devices and appliances in the home using semantic web technology. Finally, the European project “Ambient Assisted Living Joint Program” (AALJP) [18] aims to create better living conditions for older adults using ICT-based solutions for the (self-)management of daily life activities of older adults at home and contains the essential scope of homecare’s broad theme.
Figure 2 demonstrates the magnitude of the current problems; some of the reoccurring issues in the existing education system for CYP with SEND are that each school has its own method of running their provisions to meet the needs of their CYP, as well as CYP attending schools outside their residential borough. The lack of communication between formal (paid professionals) and informal (family, friends, etc.) care providers has led to the care service delivery between the departments of health, education and social care becoming fragmented. This has made it too challenging to find assigned information as there is no precise detail of who is responsible for the allocated provision and how to implement a person-centered intervention approach. Therefore, it can be difficult to access the right support and provision.
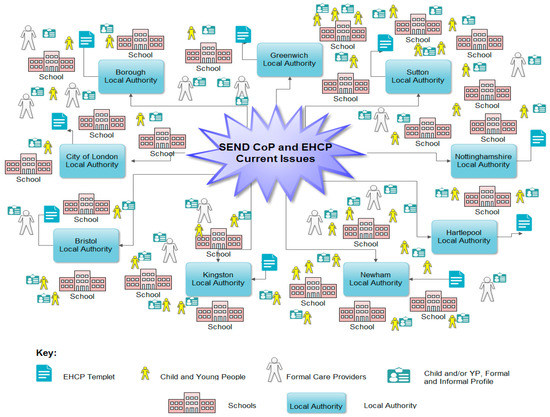
Figure 2.
Current issues with special educational needs and disabilities (SEND), code of practice (CoP) and education, health and care plans (EHCPs).
In many cases, the LAs implement SEND frameworks based on resources available rather than following the legal SEND framework. This has resulted in a “postcode lottery” of support services available to CYP with SEND, just five years after the DfE launched its reforms [19]. Substantial unexplained local variation across aspects of SEND provision has raised questions about whether CYP are receiving consistent support across the country. For example, the proportion of CYP aged between 5 and 15 with EHCPs ranged from 1.0% to 5.9% in different local areas [8].
The most recent inspections carried out by the Office for Standards in Education, Children’s Services and Skills (Ofsted) and the Care Quality Commission (CQC) have suggested that many local areas are not supporting CYP with SEND as effectively as they should be. They found significant areas of weakness in 47 (50.0%) of the 94 local regions inspected [8].
3. Smart-SCCS Holistic Model
The essential culture change associated with SEND support and the EHCP assessment process is to make sure an all-inclusive direction is followed to meet the needs of CYP in the current education system. This incorporates the assurance that suitable formal care providers from different departments, such as the education system, health and social care, participate when needed. Most importantly, this also takes into consideration the concerns of the broader family needs that are likely to occur because of the CYP’s special educational needs or disability. Hence, the proposed novel six-layered Smart-SCCS holistic model was invented as a proposed solution to the current SEND education system. This will act as a decision-making system for formal care providers and LAs to enable efficient monitoring, planning and reviewing of care intervention activities for children and YP with SEND. The six-layered Smart-SCCS framework is illustrated in Figure 3 [20]. Each layer is dependent on the next layer to form the complete Smart-SCCS infostructure; the following sections describe each layer in more detail.
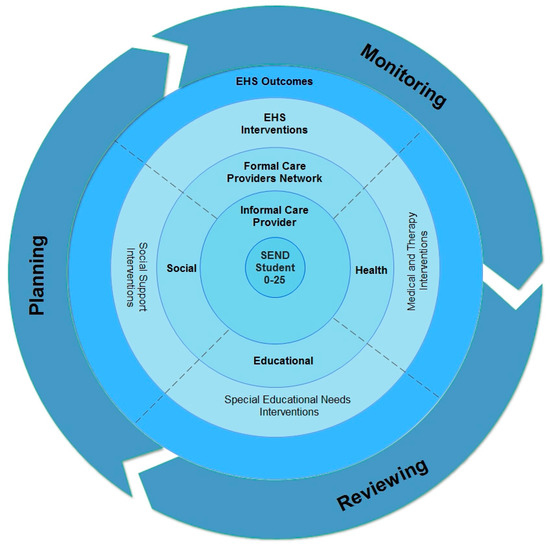
Figure 3.
Holistic six-Layered Smart School Care Coordination System (SCCS) model.
3.1. The First Layer: SEND Student 0–25
We refer to a typical SEND student as a CYP that has been diagnosed to have SEN, disabilities and/or comorbid disorders with complex medical, social and educational care needs, such as: physical disability, impaired self-dependency or learning difficulties. Previously, CYP with complex SEND profiles were eligible for a statement of SEN between the ages of two and 19 [21]. Under the new legislation, this age range has been extended to encompass CYP from birth to 25 years old. Therefore, this layer has been designed in line with the new SEND CoP (2014).
This layer consists of mainly personal information about the CYP’s medical history, symptoms and diagnosis, as well as educational needs and social conditions and limitations. This layer also contains information about the views, interests and aspirations of the CYP and their family/carers. The data and profile of the SEND CYP are gathered from his or her predefined EHCP issued by a local authority. It is essential to emphasize a person-centered approach (PCA) in this layer. A PCA is not a single technique but a collection of approaches that, jointly, seek to give disabled people control over their own lives and ensure that they are respected and valued. The term “person-centered” can be used to refer to a variety of approaches and definitions. It is an emerging concept, and as such, there is no single agreed definition of the concept. What is essential to one person may be unnecessary, or even undesirable, to another. It may also change over time as the individual’s needs change. The following subsections explain some of the currently available approaches.
3.1.1. Person-Centered Care
Person-centered care (PCC), is the most recent concept emerging in the health and social care literature [22,23]. In PC health and social care, formal care providers work collaboratively with individuals who use the services. Adopting PCC requires fundamental changes to how services are delivered and the relationship between all the parties involved, i.e., formal care providers and patients themselves. The term “person-centered care” is used to refer to many different principles and activities [24,25]. This is because if care is to be person-centered, then what it looks like will depend on the needs, circumstances and preferences of the individual receiving the care. What is important to one person in their health care may be unnecessary, or even undesirable, to another. It may also change over time as the individual’s needs change.
3.1.2. Person-Centered Planning
In the context of the education system, PCA is a relatively new emerging approach and has predominantly focused on person-centered planning (PCP) (Novak Amado and McBride, 1995; Rasheed and Miller, 2006; Murray and Sanderson, 2007). Helen Sanderson Associates [26] introduced the most influential work in the application of PCP in the UK in 2000, which has been widely referred to by the government. Sanderson talks about the PCP approach as being rooted in the principles of shared power and self-determination [27]. As far as possible, the individual that requires support is to be consulted throughout the planning process. The aim of the process itself is to emphasize placing individuals within the environment of their family/carers in their community and sharing equal power with the formal care providers who support them. The white paper “Valuing People” [28] was the official introduction of PCP as an approach to practice, in the UK, within adult learning disability services. This paper provided an authoritative guide to practice which focused on making children and adult services more responsive to individual needs and informing the educational field of its duties. Since then, legislation reinforced the application of PCP approaches within educational practices as best practice [29]. By 2015, the SEND CoP provided specific guidance on the implementation of PCP as a statutory practice [7] and made explicit reference to the use of the PCP approach, in particular during the period around the transition to adulthood, to facilitate of good outcomes, as well as allowing families/carers to engage and be involved in decision-making with the CYP. In other words, the overall idea of the PCP in SEND educational settings is to enable personalized outcomes to be tailored to support the needs of CYP and focus on identifying the different learning styles of a child or YP, by encouraging them to participate in educational institutions and to progress, achieve and enjoy their experience in the education system.
3.1.3. Person-Centered Review
Person-centered review (PCR) is part of the PCP approach which takes place annually. The PCR has become a statutory process for reviewing the outcomes, provisions, interventions and educational, health and social care needs for CYP with an EHCP. Advice and guidance for the use of PCP, in the “annual review” process, was first provided by the department of health (DoH) in 2010. This advice describes the “person-centered review” as distinct from previous approaches to planning. It outlines that the structure and techniques used in this approach ensure that the CYP is entirely at the center of the review and that it identifies actions that make a difference to their lives. Ever since, the subsequent Code of Practices has reinforced the obligation of educational practitioners in the use of person-centered thinking and planning. The introduction of the Children and Families Act 2014, Section 3 (part 19) highlighted the statutory duties placed on service providers. This made clear the principles under which local authorities were to carry out their processes. These rules reflected an interactionist perspective on “disability”.
3.2. The Second Layer: Informal Care Providers
Informal care providers (ICPs) are care providers who provide care services with an appropriate amount of support, not being tied by profession, such as family members, carers and/or voluntary care organizations. They form the second layer as they play a vital role in the management of the CYP and monitor the continuity of long-term care to enable the individuals that are cared for to reach their full potential and achieve independent living.
Formal care providers from health, education and social care, as well as LAs, are bound by a legal obligation to consider any information about the views of the CYP and their ICPs, who are to be seen as “equal partners” in the planning and commissioning of services [4]. This is a crucial message that is emphasized in the SEND CoP, in particular, aspects relating to EHCPs [7]. There are some examples of policies that highlight the positive impact of ICPs and their CYP when working in partnership with formal care providers [30]. However, the findings from the Lamb Inquiry in 2009 [31] initiate the idea that policy commitments made to children and family with regard to their participation are not enough. This means there needs to be more progress made to make sure these values are being put into practice with more evidence.
3.3. The Third Layer: Formal Care Providers Network
Formal care providers network (FCPN) refers to professionals that are involved in providing care services for CYP with additional needs who require extra support. This layer is divided by a dotted line into three sub-categories to indicate educational, health and social care providers and the intervention types they provide in the subsequent layer (education, health and social care (EHS) interventions). The care they provide will be based on the CYP with an EHCP. This involves the recognition of properties of care process activities, as well as identifying and determining the factors, such as the selection of care providers and whether they fulfil the eligibility requirements with regard to location, availability and, mainly, experience, that will enable re-coordination, if required, when a deviation of a predefined scheduled intervention occurs.
The SEND CoP and the CFA 2014 discuss cooperation between LAs and partners and the obligation to comply, when asked, to submit advice. However, there is no direct dialog regarding multi-professional collaboration and what it could look like in practice. Although there are challenges that come with multi-agency working, evidence supports the implementation of transdisciplinary teams like multi-agencies, as findings report they can lead to better outcomes for CYP, as well as facilitate positive feelings about professional identity [32].
3.4. The Fourth Layer: EHS Interventions
Education, health and social care (EHS) interventions are activities or a series of activities undertaken to respond to the needs of and provisions for CYP. The activities are carried out by different care providers across education, health, and social care. Each intervention is associated with the sort of actor that carries out that intervention. The care interventions provided are based on the predefined EHCP.
3.5. The Fifth Layer: EHS Outcomes
This layer specifies the outcomes as a result of the interventions applied to meet the needs of CYP with SEND. Once an individual’s needs are matched with a care provider, this will lead to the formation of person-centered care. At this level, a considerable volume of data and information is accessible and shared between all the actors involved in the care network. The organization of Smart-SCCS infostructure has great potential to impact the way that formal care providers deliver care to CYP with SEND.
3.6. The Sixth Layer: Planning, Reviewing and Monitoring
The sixth and final layer of the holistic Smart-SCCS model is where the monitoring, reviewing and planning of care service providers and care interventions take place. The purpose of each of the inner layers of the holistic Smart-SCCS model is to assist the CYP in varying degrees by personalizing care. Additionally, it includes coordinating the actors, provisions and interventions as has been established in the predefined EHCP, including improved communication between service providers and the CYP and their families/carers. This layer is intended for the issuing LA of an EHCP to perform the planning, monitoring and annual reviewing of the predefined EHCP to update outcomes and provisions to meet the evolving needs of CYP. This process usually takes place annually, using the person-centered review approach.
4. Care Coordination
In order to implement the Smart-SCCS and provide coordinated care interventions for CYP with SEND in the current education system, it is necessary to introduce the idea of care coordination and put the research into context. However, the term care coordination has proven to be very difficult to define by the various organizations and researchers that have addressed the topic. A technical review paper [33] identified over 40 definitions of the term “care coordination”, which pertains to a diverse set of patient populations, health care scenarios and organizational situations. This shows the magnitude of the difficulty in defining the term as it means different things to different communities as no agreed definition has fully evolved to date. Given the many various participants involved in care coordination, this lack of consensus comes as no surprise. The authors of the review paper combined many definitions of common elements to develop the working definition for use in identifying reviews of interventions in the area of care coordination, with this resulting in a purposely broad definition:
“Care coordination is the deliberate organization of patient care activities between two or more participants (including the patient) involved in a patient’s care to facilitate the appropriate delivery of health care services. Organizing care involves the marshalling of personnel and other resources needed to carry out all required patient care activities and is often managed by the exchange of information among participants responsible for different aspects of care”.
Presler [34] described care coordination as a process of planning, assessment, evaluation, implementation, support, monitoring and advocacy to make available timely access to services, enhance family well-being and promote continuity of care. The functions of care coordination were described as frustrating, complicated and time-consuming by the American Academy of Pediatrics policy statement, while also stressing that care coordination is key to effectively managing complex care issues [35]. Therefore, the two fundamental goals of care coordination, as stated below by Meyers [36], are:
- To appropriately transfer information from one participant in a patient’s care to another, such as medical history, patient preferences, test results and medication lists. This includes data being transferred to or from the patient.
- To clarify established accountability for the responsibility for each aspect of a patient’s overall care. This includes specifying who is primarily responsible for crucial care delivery activities, when that responsibility will be transferred to other care participants and the extent of that responsibility. The accountable entity (whether a health care organization, care team or health care professional) accepts responsibility for failures in the aspect(s) of care for which it is accountable. Other accountable entities may also be the patient or family.
Appropriate care coordination depends mainly on the complex needs of an individual. The challenges involved in facilitating the delivery of proper care increases as the complexity increases. The following factors are known to increase the complexity of care for CYP with SEND:
- Social vulnerability and learning abilities, multiple chronic or acute physical health problems.
- Number of care providers involved in the care provision (formal and informal care providers).
- The environment settings required to meet CYP needs.
In the SEND education system context, we define care coordination as the interaction and integration of functions that help to ensure that CYP requirements and preferences for educational, health and social care services are adaptively met. This sequentially leads to the implementation and delivery of a person-centered approach for tailored school care interventions based on a predefined EHCP specific to the complex needs of a CYP with SEND. Additionally, this includes providing decision support to monitor and update the predefined EHCP when required based on the evolving needs of an individual, i.e., to identify further interventions and address coordination failures. Examples of coordination failure are highlighted in [37], a lack of information exchange among care providers being one of the key reasons, as well as inadequate patient knowledge and/or ability related to self-care.
From our ongoing reviews in this area, most care coordination systems do not address the social and educational care service dimensions of an integrated view of care coordination. Most systems are implemented widely in health care domains, such as hospitals, and are coordinated by nurses. However, our coordination of care network system architecture, as shown in Figure 4, is a commonly adopted platform approach to developing an integrated school care coordination support network for care service providers, wherein all the formal care providers from different sectors, as well as informal care providers, interact with each other. This involves sharing a standard set of information and knowledge about CYP SEND needs that will result in improved communication and increased quality of care coordination across health, social and educational settings for school care intervention. All the actors involved in the care coordination network, including CYP, have their profile available in the Smart-SCCS. The care provider profile holds information about their expertise, location and their availabilities (in a run-time engine, it is essential to coordinate these tasks efficiently to improve the global performance of care coordination between involved actors). The SEND CYP profile contains information about medical history, diagnosis, needs, provision, intervention required and personal information. The goal of implementing such a model of care is to coordinate health, social and educational support provisions using a holistic, person-centered approach.
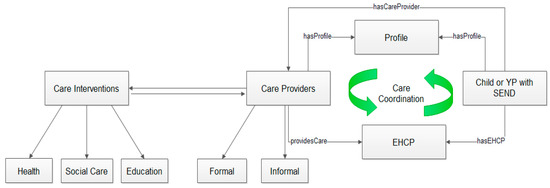
Figure 4.
An overview of Smart-SCCS coordination of care network architecture.
5. Ontologies
Ontology is described as the spine that allows semantic web technology (SWT) to provide the domains and machine-processable semantics. The process can be shared and it can assist in communication among people and other applications. Ontologies mainly aim to offer semantics, which create a web of meaning and work to assist the machines in processing and maintaining the information, as well as facilitate its sharing [38].
An ontology is a formal description of knowledge, a set of concepts within a domain and the relationships between them. It is described as a file or document that formally defines all the relationships between the terms used in the documents. For a description to be enabled, the user must formally specify components such as classes, individuals (instances of objects), relations and attributes, as well as axioms, rules and restrictions. As a result, ontologies can add new knowledge about the domain as well as introduce a sharable and reusable knowledge representation. The following section describes the benefits of using ontologies.
Benefits of Using Ontologies
The use of ontology in SWT has many advantages. One of the main benefits of ontologies is that, by having the essential relationships between concepts built into them, they enable automated reasoning about data. What is more, ontologies function like a “brain”; they work and reason with concepts and relationships in ways that are close to the way humans perceive interlinked concepts. Other benefits of using ontologies are summarized by Vishal Jain and Mayank Singh [39] as follows:
- One of the regular goals of developing ontologies is sharing a common understanding of the structure of information among people or software agents [40].
- The ontology allows reusability of domain knowledge in representing concepts and their relationships.
- Ontologies make it possible to change domain assumptions easily when the knowledge about a domain changes; this is an explicit function of the underlying implementation [41].
- Another common use of ontologies is separating the operational knowledge from the domain knowledge. This involves describing a task of configuring a product from its components according to a required specification and implementing a program that does this configuration independent of the components and products themselves [42].
- Analyzing the domain knowledge base on declared terms in a document is enabled when using ontologies.
- Every user has defined attributes and relationships between other users.
- Ontology is viewed as the backbone of software engineering. The concept of ontologies is used to translate semantic web data into machine-understandable language.
- Ontology development is a cooperative process, enabling more than one person to express their views on a given domain [43].
- Ontologies also provide the means to represent any data formats, including unstructured, semi-structured or structured data, enabling smoother data integration, more straightforward concept and text mining, and data-driven analytics [44].
6. Research Methodology and Implementation
6.1. Data Collection
In this research, information was collected about a varied number of professionals (referred to as formal care providers) and their roles and responsibilities to support CYP with SEND. These professionals come from different departments, such as: education systems, e.g., educational psychologists, special educational needs coordinators (SENCOs), specialist teachers; health departments, e.g., therapists (speech therapists, occupational therapists), specialist doctors and social workers from the department of social care. For example, the role of social work is to analyze and support a CYP’s needs within their family life, as well as assess the CYP’s eligibility and entitlement for a social care provision in the school setting and at home or assess facilities in the community, such as short breaks, respite, etc. This information was mainly gathered from online literature; such as the Department for Education and Department of Health SEND CoP [7]. Additionally, some SENCOs from mainstream and special schools were interviewed to find out about the different types of formal care providers that are involved with SEND CYP that have already been issued an EHCP and are receiving care in a school setting. This is mainly for CYP that have a primary diagnosis of autism spectrum disorder (ASD). ASD is the current dominating area of needs in schools and approximately 30% of CYP issued with an EHCP have some form of ASD diagnosis [8].
Twelve predefined EHCP case studies were selected for CYP with ASD and/or other comorbid diagnoses. The age range for the case study is CYP between the age of 6 and 14 years old (this is limited due to the ethical application). These individuals have diverse profiles ranging from mild to complex needs. They also attend different school settings, varying from maintained mainstream with or without special provision units, independent schools, special schools and academies. Theses case studies are the scenarios that have been used for testing and validating the Smart-SCCS framework. In the future, the framework can be used for varied CYP with different types of special needs as the model was designed and implemented as a generic model for SEND. The designed and implemented model demonstrates the applicability of the latest technologies and would allow for future technologies to be easily incorporated to enhance the model.
Information was collected about various care intervention services delivered by education, health and social care service providers, i.e., formal care providers. They provide different types of interventions and programs specifically devised for CYP with ASD. For example, applied behavior analysis (ABA) is an intervention program that can be classified as an educational intervention, and other medical, therapy and social care interventions have been identified and modeled in the Smart-SCCS framework. The information was mainly collected from online literature, such as a “Guide to evidence-based interventions” [45], the thesis by Elliott, titled “Effective interventions for children and adolescents with autism spectrum disorders and other special educational needs”. This thesis summarizes, in detail, effective interventions for children and adolescents with ASD [46]. However, the use of interventions was validated with mainstream, special schools and the “local offer” to ensure that the interventions are relevant and currently available to children and YP with ASD and other medical conditions and disabilities.
6.2. Smart-SCCS Implementation
In this section, we describe the technologies used to implement the proposed Smart-SCCS infostructure to enable coordination of care activities between the different actors involved in the school care network for CYP with SEND.
The ontology-building methodology adopted in this research is “Ontology development 101” [47]. It is a simple knowledge engineering methodology to develop ontologies and is based on a declarative knowledge representation system [47]. The authors developed this as an iterative approach based on their experience using ontology editing environments such as Protégé. It is one of the most cited methodologies for ontology development using Protégé. The method consists of eight general steps for designing and developing the proposed Smart-SCCS ontology, as illustrated in Figure 5 [47,48]. The steps are described as the following:
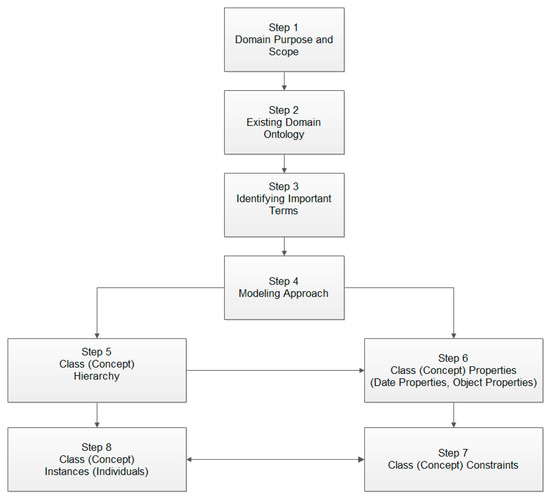
Figure 5.
“Ontology development 101” process.
The first step of developing an ontology begins with identifying the domain, then extending the domain to define its scope and purpose. The purpose of the ontology is to guide the design process by providing domain conceptualization [47]. This is achieved by answering the following questions [49]:
- Which domain does the ontology cover?
- What is the purpose of the ontology?
- What are the questions that can be answered via the information provided in the ontology?
The second step involves checking similarly developed ontologies, as the manipulation of existing ontologies is easier than generating a new ontology from scratch to suit one’s needs and requirements. One of the advantages of using ontology is being able to reuse already existing ontologies, for example, to have a shared understanding of the structure of information among people or software agents.
- To allow domain knowledge to be reused
- To make domain assumptions explicit
- To separate domain knowledge from the operational knowledge
- To analyze domain knowledge
The third step is brainstorming, identifying and counting the most important ontological concepts and phrases in the given domain. Creating a taxonomy of Smart-SCCS components is a way of classifying a set of concepts, utilizing a hierarchical structure.
The fourth step includes finding an approach suitable to modeling the ontology: top-down, middle-out or bottom-up. The top-down method starts by identifying the domain’s most general concepts, then more specialized ones. In contrast, the bottom-up approach commences by defining the most detailed classes, then groups them into more general concepts. The middle-out approach starts by identifying the essential terms in each area before moving on to more specific and abstract ones.
The fifth and sixth step are closely interlinked. The arrow between them is unidirectional, as once the class hierarchy is completed, it then pushes forward the possibility to identify its concepts’ properties. At the fifth stage, the classes (concepts) and their hierarchy are identified. Meanwhile, the sixth stage is where their properties are identified. The class hierarchy can again be determined by using the top-down, middle-out or bottom-up approaches. All terms listed at stage three, have an independent existence should be extracted into the various classes (concepts) of the ontology. Determining its hierarchical organization involves asking if each of the instances in a class could also be an instance of a more general class. If so, then the former class becomes a subclass of the latter and drifts further away from the ontology’s root concept. After defining all the classes, the internal structures (properties) of the concepts need to be described. Yet again, these properties should be readily available from the list generated at the third stage.
At the seventh step, properties have facets attached, which means describing the allowed values, the value type (data property), their number (cardinality) and other features which are deemed to be vital. Consequently, constraints are placed on the types of data allowed. The constraint relationship is employed to represent a restriction on operations which may be executed, which in turn helps to limit the number of links between instances (individuals) of the entities or relationships which are permitted [50].
The last step provides examples of each of the classes by involving the means to create individuals in the classes.
6.3. Smart-SCCS Unified Modeling Language (UML) for User Case Diagram
In order to visualize the functionality of the framework from a users’ perspective, a use case diagram was used. A use case diagram specifies a set of interactions between actors and use cases to achieve a particular goal [51]. Actors represent a person, organization or external system that plays a role in one or more interactions within a system, and in this research, actors represent users. A use case is presented as an oval and describes a sequence of actions that provide something of quantifiable value to an actor, i.e., functionality of a system. Lines represent associations. Finally, a system boundary defines the scope of the system, representing a collection of functionalities.
Figure 6 represents a high-level abstract interpretation of the core functionality of the Smart-SCCS framework. As can be seen, there are seven participants; formal care providers (healthcare providers, social care providers, educational providers, local authorities), CYP (SEND student), informal care providers (families/carers) and system engineer.
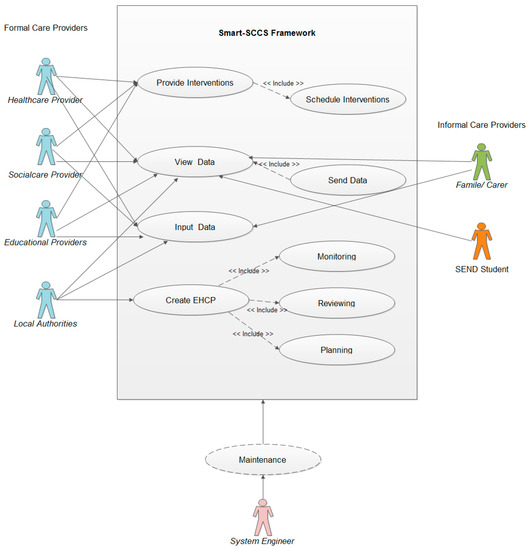
Figure 6.
High-level Smart-SCCS user case diagram.
The formal care providers are the primary users of the framework. The local authority actors are responsible for creating an EHCP, and their role includes the ongoing monitoring, reviewing and planning of the issued plans. Meanwhile, health care, social care and educational providers are responsible for providing the personalized and coordinated care interventions required based on the predefined EHCP for a SEND student. All the formal care providers have system privileges to view, enter and edit data related to a SEND student.
Informal care providers and the SEND student are secondary users. Although they will not interact directly with the system, they will interact with the applications created and be able to view the data. However, informal care providers will also have system privileges to manipulate the data.
System engineers are the tertiary users of the system and have the responsibility to maintain, update and further develop various components and services of the framework.
6.4. Protégé Ontology Editor and Knowledge Management System
The Smart-SCCS ontology was developed using the Protégé-OWL editor and knowledge management framework for building intelligent systems, version 5.5. Protégé [52] is a flexible, open-source platform, developed by Stanford University. According to the book Model-Driven Engineering and Ontology Development, Protégé is the leading ontological engineering tool [53]. It has a strong community of thousands of users including academic, government and corporate users. Protégé is developed in Java and supports the ontology language OWL [54]. The use of OWL is significant because it allows for the distribution of ontological knowledge [55]. This ontology editor provides a graphical user interface to define ontologies. This provides easy integration of a set of tools to build and edit the ontology of constructed domain models and knowledge-based applications, i.e., it supports the creation, visualization and manipulation of ontologies in various representation formats [56,57]. Protégé was the chosen ontology editor for developing the Smart-SCCS as it was found to provide a flexible base for quick ontology development. Most importantly, it also offers a user-friendly interface and a well-supported document and error-checking mechanism [54].
It is clear that ontology development is mostly an ad hoc approach. A user has several viable alternatives and is required to find which one would work best for the management of the intended task and which option is easily and effectively expressed and maintained. The basis that ontology was founded on is logic; however, it is also a model of reality, and the concepts in the ontology must reflect this reality.
6.5. Pellet Reasoner
Pellet was employed to check the consistency of the developed Smart-SCCS ontology and to infer additional facts from the knowledge and relationships within the ontology model developed in the given environment. It provides cutting-edge reasoning facilities for OWL [58,59]. The key benefits of using Pellet [60] can be summarized as follows:
First, the consistency checking guarantees that the ontology contains no contradictory facts. Second, the classification computes the subclass relations amongst every given class to generate the complete class hierarchy, which in turn can be employed to answer specific queries, such as identifying only or all of the direct subclasses of a class. Third, the realization finds the particular classes to which an individual relates, i.e., it computes the direct types for each individual. The realization can be executed hierarchically. Based on the classification hierarchy, it becomes possible to identify all the types for certain individuals.
6.6. Class Hierarchy
The whole picture of the ontology domain is described in classes and class hierarchy within the Protégé-OWL editor environment. Classes offer an abstraction mechanism that groups together resources with similar characteristics. The same values of aspects are defined as it specifies the concept of the domain as a collection of abstract objects. The OWL language is used for ontology modeling. Every OWL class is associated with a set of individuals. The principal task of reasoners is to arrange individuals into classes based on the properties that they exhibit and the intentional definitions of the classes [61]. Classes can be related to one another through subsumption relations, i.e., a particular class may be defined as being a subclass of another class, or equivalence class relations, i.e., being extensionally equivalent. The idea behind subclasses and subsumption is closely linked to the view of a class as a set of individuals, in that the individuals belonging to a subclass by definition are a subset of the individuals belonging to the superclass. In many languages, there exists a defined top class (in Protégé this is called OWL: Thing) of which all other classes are subclasses and, thus, of which all individuals are members.
Figure 7 shows a screenshot of part of the Smart-SCCS class hierarchy and its subclasses implemented using the built-in create class hierarchy tab using the Protégé-OWL editor.
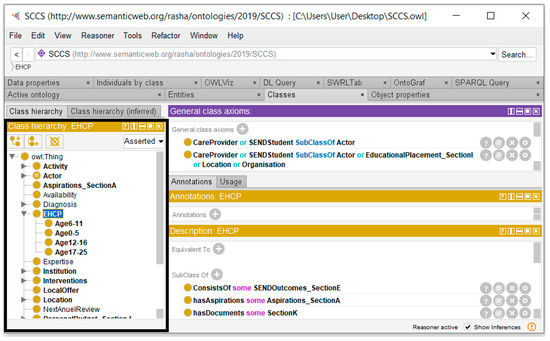
Figure 7.
Smart-SCCS class hierarchy and its subclasses.
6.7. Actor Concept Ontology
The actor class is all the humans that are interacting with the Smart-SCCS framework, i.e., formal and informal care providers, as well as the CYP with SEND (referred to in the ontological model as the SEND student). This class holds essential personal information to describe the actors, such as their name, gender, age, address, etc., as well as their relationships to other classes. For example, the formal actors have relationship links to other classes, such as location, expertise and institution classes to enable care coordination.
As can be seen from Figure 8, the upper level of the actor class hierarchy consists of two sub-branches, SEND student and care providers, which in turn is further classified into formal and informal care providers. The formal care provider is also classified into four other classes: social care providers, health care providers, educational care providers and other care providers (local authority actors and other relevant actors that interact with the Smart-SCCS). The informal care provider class is also classified into other classes to represent family members, etc. Each branch is disjoined and has its own hierarchy.
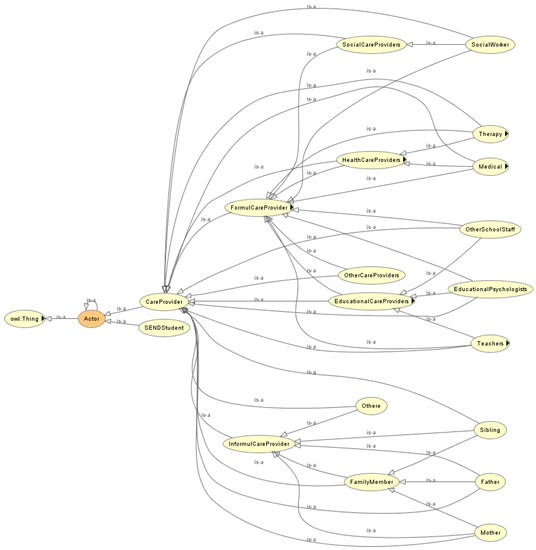
Figure 8.
Actor concept ontology.
7. Experiments and Results
This section discusses the case scenarios used to validate the Smart-SCCS.
7.1. Case Scenarios
Twelve predefined EHCP case studies were collected from informal care providers for CYP with various SEND diagnoses. The age range for the case studies is between the age of 6 and 14 years old. These individuals have diverse profiles ranging from mild to complex learning, health and social care needs. They attend different school settings varying from maintained mainstream with or without special provision units, independent schools, special schools and academies. They also require different care interventions delivered by several care providers from education, health and social care departments.
Figure 9 gives a snapshot of the twelve case studies, implemented as individuals as instances of subclass SEND student using the protégé-OWL editor. Each case scenario was created for an individual CYP, and is labeled as Student1001, representing case study one, Student1002, representing case study two, and so on. They represent the twelve case studies collected. These case studies form part of the scenarios were been employed to test the validity of the proposed Smart-SCCS model. The model was designed and implemented as a generic model for CYP with any type of special educational needs and disability. The model demonstrates the applicability of the latest technologies and could allow for future technologies to be easily incorporated, to enhance it further in the future to accommodate the changing needs of the current education system.
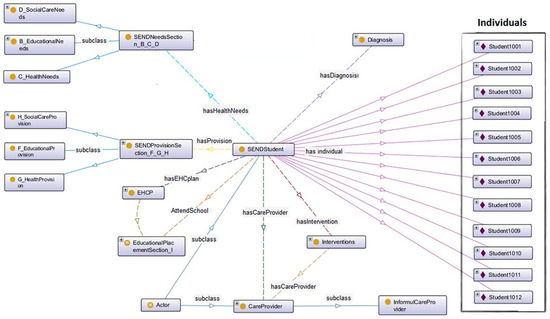
Figure 9.
Twelve case studies implemented in Protégé-OWL editor.
7.2. SEND Student Case Scenario Results
The following is a case scenario implemented using ontologies to model care coordination for a 14-year-old male student that was diagnosed with high functioning autism. He requires daily educational and therapeutic interventions. Educational care providers, such as a specialist teacher, will provide a tailored numeracy study program to support him. Additionally, a speech and language therapist from the Department of Health will be providing a specifically tailored literacy program with visual support and assistive tools once a week. The case scenario for a SEND student with autism is illustrated in Figure 10.
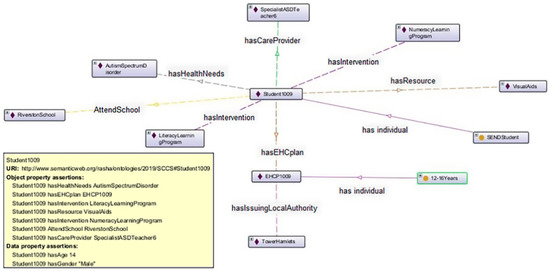
Figure 10.
Case scenario for a SEND student with autism.
There is a need for a well-integrated and coordinated system to hold relevant information for an intervention to be carried out successfully. This includes the type of interventions and availability of formal care providers that will provide the intervention and their expertise level, as well as the full CYP profile, i.e., the identified needs and provision type required to meet these needs and provide the right support. The Smart-SCCS acts as a knowledge base of all the required information in one place and has been demonstrated as a solution in real time. For example, if a speech therapist has been allocated a specific time slot to provide an intervention to a CYP at school and, for whatever reason, she/he is unavailable to attend or carry out the allocated intervention, then we will be able to search within the Smart-SCCS knowledge base for an available speech therapist that matches the characteristics (profile), i.e., expertise level, of the therapist that was unable to carry out the intervention.
It is not the intention of this research to implement a fully operational platform, but rather a generic model high-level framework which represents the main architectural components and services of such a system.
8. Conclusions and Further Research
This research work proposed the development of an innovative computerized information infostructure to model and implement a smart generic “School Care Coordination System” (SCCS). It is based on a novel design of an original holistic “six-layered data management model” Smart-SCCS. The framework adopts a methodology of ontology engineering to transform the given theoretical unstructured SEND code of practice into a comprehensive knowledge representation and reasoning system, to support and bring together education, health and social care services into a single application. Additionally, it coordinates, integrates and monitors education, health and social care activities between different actors (formal, informal and CYP) involved in the school care process network to provide personalized care interventions for CYP with SEND. In conclusion, the proposed Smart-SCCS in this research offers a practical and promising solution to support and manage the current education system for CYP with SEND.
This research intends to set the foundation for further research into this combined field and to create cultural change to help to organize and operate the new shift in the education system to enable SEND CYP to meet their full potential in mainstream schools or any other educational settings.
The developed model was introduced to a range of schools, families of CYP, social care and health care providers along with local authorities and has received considerable attention from all involved with great feedback, showing the efficiency and robustness of the developed model.
Author Contributions
Conceptualization, R.H. and M.S.S.; methodology, R.H.; software, R.H. and M.S.S.; validation, R.H., A.H.A.-B. and A.S.A.; formal analysis, R.H.; investigation, R.H.; resources, M.S.S., A.H.A.-B., A.S.A., M.O.A. and M.A.A.; data curation, R.H.; writing—original draft preparation, R.H.; writing—review and editing, M.S.S., A.H.A.-B., A.S.A., M.O.A. and M.A.A.; visualization, R.H. and A.H.A.-B.; supervision, M.S.S.; project administration, M.S.S., A.H.A.-B., A.S.A., M.O.A. and M.A.A.; funding acquisition, M.S.S., A.H.A.-B. and A.S.A. All authors have read and agreed to the published version of the manuscript.
Funding
This project was funded by the deanship of scientific research (DSR), King Abdulaziz University, under grant No. (KEP 19-611-38).
Acknowledgments
The authors would like to thank the professionals who took part in this research from Newham Local Authority Special Educational Needs and Disability (SEND) department, Newham SENDIASS (Special Educational Needs Disability Information Advice Support Services), the headteachers and their staff members from Woodcroft Special School, Ronald Openshaw Nursery Education Centre (RONEC), as well as parent support groups: East London Special Educational Needs and Disability Network (East London, SEND-Net), Let Us Communicate (LUC) and Newham Parent Forum (NPF). The authors, also, acknowledge with thanks DSR technical and financial support.
Conflicts of Interest
The authors have no conflict of interest.
References
- Hewitt, H. The Changing Face of SEN: 140 Years of Provision. SEN Mag. 2011. Available online: https://senmagazine.co.uk/articles/articles/senarticles/the-changing-face-of-sen-140-years-of-provision (accessed on 20 June 2020).
- Cochrane, H. Exploring Perceptions and Experiences of the Education, Health and Care Process. Ph.D. Thesis, School of Education, University of Birmingham, Birmingham, UK, July 2016. Available online: https://etheses.bham.ac.uk//id/eprint/7020/1/Cochrane16ApEd%26ChildPsyD_vol_1_Redacted.pdf (accessed on 4 February 2020).
- Poulter, D.; Timpson, E. 0 to 25 SEND Code of Practice: A Guide for Health Professionals, Advice for Clinical Commissioning Groups, Health Professionals and Local Authorities. Departmet of Education; Department of Health. 2016. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/502913/Health_Professional_Guide_to_the_Send_Code_of_Practice.pdf (accessed on 10 April 2020).
- Children and Families Act 2014. Chapter 6. Children and Young People in England with Special Educational Needs or Disabilities. 2014. Available online: https://www.legislation.gov.uk/ukpga/2014/6/pdfs/ukpga_20140006_en.pdf (accessed on 4 May 2020).
- Adams, L.; Tindle, A.; Basran, S.; Dobie, S.; Thomson, D. Education, Health and Care Plans: A Qualitative Investigation into Service User Experiences of the Planning Process. Department of Education. Social Science in Coverment. 2018. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/695100/Education_Health_and_Care_plans_-_a_qualitative_investigation.pdf (accessed on 4 February 2020).
- Poulter, D.; Timpson, E. Special Educationak Needs and Disability Code of Practice: 0 to 25 Years. Statutory Guidance for Organisations Which Work with and Support Children and Young People Who Have Special Educational Needs or Disabilities. Department of Education; Department of Health. January 2015; p. 35. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/398815/SEND_Code_of_Practice_January_2015.pdf (accessed on 1 February 2020).
- Poulter, D.; Timpson, E. Special Educational Needs and Disability: Managing the September 2014 Changes to the System. Department of Education; Department of Health. 2016. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/567622/Special_educational_needs_and_disability_managing_the_September_2014_changes_to_the_system.pdf (accessed on 10 July 2020).
- National Audit Office. Support for Pupils with Special Educational Needs and Disabilities in England; Department for Education: London, UK, September 2019.
- Milne, S. Children and Young People’s Mental Health Local Transformation Plans—A Summary of Key Themes. NHS Englan Publication. 2016. Available online: https://www.england.nhs.uk/mentalhealth/wp-content/uploads/sites/29/2016/08/cyp-mh-ltp.pdf (accessed on 12 July 2020).
- Tidy, C. Autism Spectrum Disorders. Autism Information at Patient. 2016. Available online: https://patient.info/childrens-health/autistic-spectrum-disorders-leaflet (accessed on 15 July 2020).
- NHS. Learning Disabilities. 2019. Available online: https://www.nhs.uk/conditions/learning-disabilities/ (accessed on 10 May 2020).
- The Good Schools Guide. Moderate Learning Difficulties. 2015. Available online: https://www.goodschoolsguide.co.uk/special-educational-needs/learning/moderate-learning-difficulties (accessed on 15 February 2020).
- Matthews, P.; Lewis, P. How Do School Leaders Successfully Lead Learning? 2009. Available online: https://dera.ioe.ac.uk/254/1/download%3Fid%3D23637%26filename%3Dhow-do-school-leaders-successfully-lead-learning.pdf (accessed on 18 July 2020).
- OASIS. Welcome to OASISwebsite. 2008. Available online: http://www.oasis-project.eu/ (accessed on 12 February 2020).
- Panou, M.; Bekiaris, E.; Cabrera-Umpierrez, M.F.; Jiménez Mixco, V.; Arredondo, M.T. Use cases functionality of the OASIS HCI. In Lecture Notes in Computer Science (Including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); Springer: Berlin/Heidelberg, Germany, 2009; Volume 5614, Part 1, pp. 269–277. [Google Scholar]
- K4CARE. K4Care—Knowledge-Based Home-Care eServices for an Ageing Europe. 2010. Available online: https://ec.europa.eu/digital-single-market/en/news/k4care-knowledge-based-home-care-eservices-ageing-europe (accessed on 15 February 2020).
- MATCH. MATCH—Mobilising Advanced Technologies for Care at Home. 2012. Available online: http://www.cs.stir.ac.uk/~kjt/research/match/main/main.html#skipnav (accessed on 12 February 2020).
- AALJP. AAL Home—AAL Programme. 2013. Available online: http://www.aal-europe.eu/ (accessed on 1 February 2020).
- Snowdon, K. SEND Review Launched to Tackle ‘Postcode Lottery’ of Support. Schools Week. 2019. Available online: https://schoolsweek.co.uk/send-review-launched-to-tackle-postcode-lottery-of-support/ (accessed on 12 May 2020).
- Hafidh, R.; Sharif, M.S.; Alsallal, M. Smart Holistic Model for Children and Youth with Special Educational Needs and Disabilities. In Proceedings of the 2019 International Conference on Computing, Electronics & Communications Engineering, London, UK, 22–23 August 2019; pp. 130–135. [Google Scholar] [CrossRef]
- Morris, E.M.P. Special Educational Needs Code of Practice. Education and Skills. DfES. 2001. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/273877/special_educational_needs_code_of_practice.pdf (accessed on 12 July 2020).
- The Health Foundation. Person-Centred Care Made Simple What Everyone Should Know about Person-Centred Care; Health Foundation: London, UK, 2016. [Google Scholar]
- Novak, A.; McBride, M. Increasing Person-Centered Thinking: Improving the Quality of Person-Centered Planning: A Manual for Person-Centered Planning Facilitators; University of Minnesota, Institute on Community Integration: Minneapolis, MN, USA, 2001; Available online: https://rtc.umn.edu/docs/pcpmanual1.pdf (accessed on 1 July 2020).
- Rasheed, S.A.; Miller, S. Person-Centered Planning: Practices, Promises, and Provisos. J. Vocat. Spec. Needs Educ. 2006, 28, 47–59. [Google Scholar]
- Murray, P.; Sanderson, H. Developing Person Centred Approaches in Schools. Helen Sanderson Associates and ibk Initiatives. HSA Press. 2007. Available online: https://www.sthelens.gov.uk/media/8869/developing-person-centered-approaches-in-schools.pdf (accessed on 1 May 2020).
- Anderson, H. HSA, Person-centred, Personalisation, Training, Consultancy. 2020. Available online: http://helensandersonassociates.co.uk/ (accessed on 10 February 2020).
- Sanderson, H. Person Centered Planning: Key Features and Approaches; Joseph Rowntree Foundation: York, UK, 2000. [Google Scholar]
- Blair, T. Valuing People: A New Strategy for Learning Disability for the 21st Century. A White Paper. Department of Health. 2001. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/250877/5086.pdf (accessed on 10 July 2020).
- Department for Children, Schools and Families: Resource Accounts 2008–2009. The Stationery Office. 2009. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/340543/DCSF-Accounts_2008-09.pdf (accessed on 1 July 2020).
- HM Government. Working Together to Safeguard Children 2018. A Guide to Inter-Agency Working to Safeguard and Promote the Welfare of Children; National Archives: Kew, London, 2018. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/779401/Working_Together_to_Safeguard-Children.pdf (accessed on 14 June 2020).
- Lamb, B. Report to the Secretary of State on the Lamb Inquiry Review of SEN and Disability Information; Department for Children, Schools and Families: London, UK, 2009.
- Gaskell, S.; Leadbetter, J. Educational psychologists and multi-agency working: Exploring professional identity. Educ. Psychol. Pract. 2009, 25, 97–111. [Google Scholar] [CrossRef]
- Shojania, K.G.; McDonald, K.M.; Wachter, R.M.; Owens, D.K. Closing the Quality Gap: A Critical Analysis of Quality Improvement Strategies; Care Cordination; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2007; Volume 7. Available online: https://www.ncbi.nlm.nih.gov/books/NBK44015/ (accessed on 1 July 2020).
- Mcallister, J.; Presler, E.; Cooley, W. Practice-Based Care Coordination: A Medical Home. Pediatrics. June 2007, pp. 1–27. Available online: https://www.researchgate.net/publication/6073035_Practice_Based_Care_Coordination_A_Medical_Home_Essential (accessed on 1 April 2020).
- Smucker, J.M.R. Managed care and children with special health care needs. J. Pediatr. Health Care 2001, 15, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Meyers, D.T.L.; Peikes, D.; Genevro, J.; Peterson, G.; Fries, E. The Roles of Patient-Centered Medical Homes and Accountable Care Organizations in Coordinating Patient Care the Roles of Patient-Centered Medical Homes and Accountable Care Organizations in Coordinating Patient Care. Agency for Healthcare Research and Quality U.S. Department of Health and Human Services. 2010. Available online: https://pcmh.ahrq.gov/sites/default/files/attachments/Roles%20of%20PCMHs%20And%20ACOs%20in%20Coordinating%20Patient%20Care.pdf. (accessed on 20 June 2020).
- Kripalani, S.; Henderson, L.E.; Jacobson, T.A.; Vaccarino, V. Medication Use Among Inner-City Patients After Hospital Discharge: Patient-Reported Barriers and Solutions. Mayo Clin. Proc. 2008, 83, 529–535. [Google Scholar] [CrossRef]
- Buraga, S.; Ciobanu, G. A RDF-based model for expressing spatio-temporal relations between Web sites. In Proceedings of the Third International Conference on Web Information Systems Engineering, Singapore, 14 December 2002; pp. 355–361. Available online: https://ieeexplore.ieee.org/abstract/document/1181671 (accessed on 20 June 2020).
- Jain, V.; Singh, M. Ontology Development and Query Retrieval using Protégé Tool. Int. J. Intell. Syst. Appl. 2013, 5, 67–75. [Google Scholar] [CrossRef]
- Chandrasekaran, B.; Josephson, J.R.; Benjamins, V.R. What aro ontologies, and why do we need them? IEEE Intell. Syst. Their Appl. 1999, 14, 20–26. [Google Scholar] [CrossRef]
- Berners-lee, T.; Shadbolt, N.; Hall, W. The Semantic Web Revisited. IEEE Intell. Syst. 2006. Available online: https://eprints.soton.ac.uk/262614/1/Semantic_Web_Revisted.pdf (accessed on 17 April 2020).
- Tankelevičienė, L. Ontology and Ontology Engineering: Analysis of Concepts, Classifications and Potential Use in E-Learning Context. Technical Report. Institute of Mathematics and Informatic. Vilnius LT. Lithuania 2008. Available online: https://pdfs.semanticscholar.org/53ff/8c0773dcd6df03370b2cb9a8b0007c17928d.pdf (accessed on 27 March 2020).
- Sugumaran, V.; Storey, V.C. The role of domain ontologies in database design: An ontology management and conceptual modeling environment. ACM Trans. Database Syst. 2006, 31, 1064–1094. [Google Scholar] [CrossRef]
- Ontotext. What Are Ontologies and What Are the Benefits of Using Ontologies.Knowledge Hu. 2019. Available online: https://www.ontotext.com/knowledgehub/fundamentals/what-are-ontologies (accessed on 12 April 2020).
- Bodenhorn, K. Autism Spectrum Disorders: Guide to Evidence-based Interventions. Missouri Autism Guidel. Initiat. 2012. Available online: https://autismguidelines.dmh.mo.gov/documents/Interventions.pdf (accessed on 4 May 2020).
- Elliott, N.A. Effective Interventions for Children and Adolescents with Autism Spectrum Disorders and Other Special Educational Needs. Ph.D. Thesis, School of Psychology. College of Life and Environmental Sciences. University of Birmingham, Birmingham, UK, 2015. Available online: https://etheses.bham.ac.uk//id/eprint/6844/1/Elliott16PhD.pdf. (accessed on 23 May 2020).
- Noy, N.F.; McGuinness, D. Ontology Development 101: A Guide to Creating Your First Ontology; Stanford University: Stanford, CA, USA, 2001. [Google Scholar]
- Al-Khawaldeh, M.; Chen, X.; Moore, P.; Al-Naimi, I. Nowledge-based auto-configuration system using ubiquitous robotics for services delivery in smart home. Int. J. Embed. Syst. 2019, 11, 182–199. [Google Scholar] [CrossRef]
- Bechhofer, I.H.S.; Goble, C. Requirements of Ontology Languages. 2003. Available online: http//ontoweb.aifb.unikarlsruhe.de/About/Deliverables (accessed on 12 July 2020).
- Boyce, S.; Pahl, C. Developing Domain Ontologies for Course Content. Educ. Technol. Soc. 2007, 10, 275–288. Available online: https://core.ac.uk/download/pdf/11310019.pdf (accessed on 4 May 2020).
- Britton, C.; Doake, J. A Student Guide to Object-Oriented Development; Elsevier: Amsterdam, The Netherlands, 2005. [Google Scholar]
- Protégé 5.5. 2020. Available online: https://protege.stanford.edu/ (accessed on 21 February 2020).
- Gašević, D.; Djurić, D.; Devedžić, V. Model Driven Architecture and Ontology Development; Springer: Berlin/Heidelberg, Germany, 2006. [Google Scholar]
- Noy, F. Protégé-2000: An open-source ontology-development and knowledge-acquisition environment. AMIA Annu. Symp. Proc. 2003, 953. Available online: https://pubmed.ncbi.nlm.nih.gov/14728458/ (accessed on 3 July 2020).
- Knublauch, H.; Fergerson, R.W.; Noy, N.F.; Musen, M.A. The Protégé OWL Plugin: An Open Development Environment for Semantic Web Applications; Springer: Berlin/Heidelberg, Germany, 2004; pp. 229–243. [Google Scholar]
- Gennari, J.H. The evolution of Protégé: An environment for knowledge-based systems development. Comput. Stud. 2003, 58, 89–123. [Google Scholar] [CrossRef]
- Rodríguez-Valenzuela, S.; Holgado-Terriza, J.A.; Petkov, P.; Helfert, M. Modeling Context-Awareness in a Pervasive Computing Middleware Using Ontologies and Data Quality Profiles; Springer: Berlin/Heidelberg, Germany, 2013; pp. 271–282. [Google Scholar]
- Singh, S.; Karwayun, R. A Comparative Study of Inference Engines. In Proceedings of the Seventh International Conference on Information Technology: New Generations, Las Vegas, NV, USA, 12–14 April 2010; pp. 53–57. [Google Scholar]
- W3C. OWL 2 Web Ontology Language Document Overview (Second Edition). W3C Recommendation. 2012. Available online: https://www.w3.org/TR/owl2-overview/ (accessed on 6 July 2020).
- Křemen, P.; Kouba, K. Ontology-driven information system design. IEEE Trans. Syst. Man Cybern. Part C Appl. Rev. 2012, 42, 334–344. [Google Scholar] [CrossRef]
- Steffen, R.S.; Studer, R. Handbook on Ontologies, 2nd ed.: International Handbooks on Information Systems; Springer: Berlin/Heidelberg, Germany, 2009; Available online: https://www.springer.com/gb/book/9783540709992#otherversion=9783540926733 (accessed on 4 July 2020).










© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).