Teprotumumab for Thyroid Eye Disease: Mechanism, Clinical Efficacy, and Current Challenges

 , ,
, ,
Abstract
1. Introduction
2. Methods
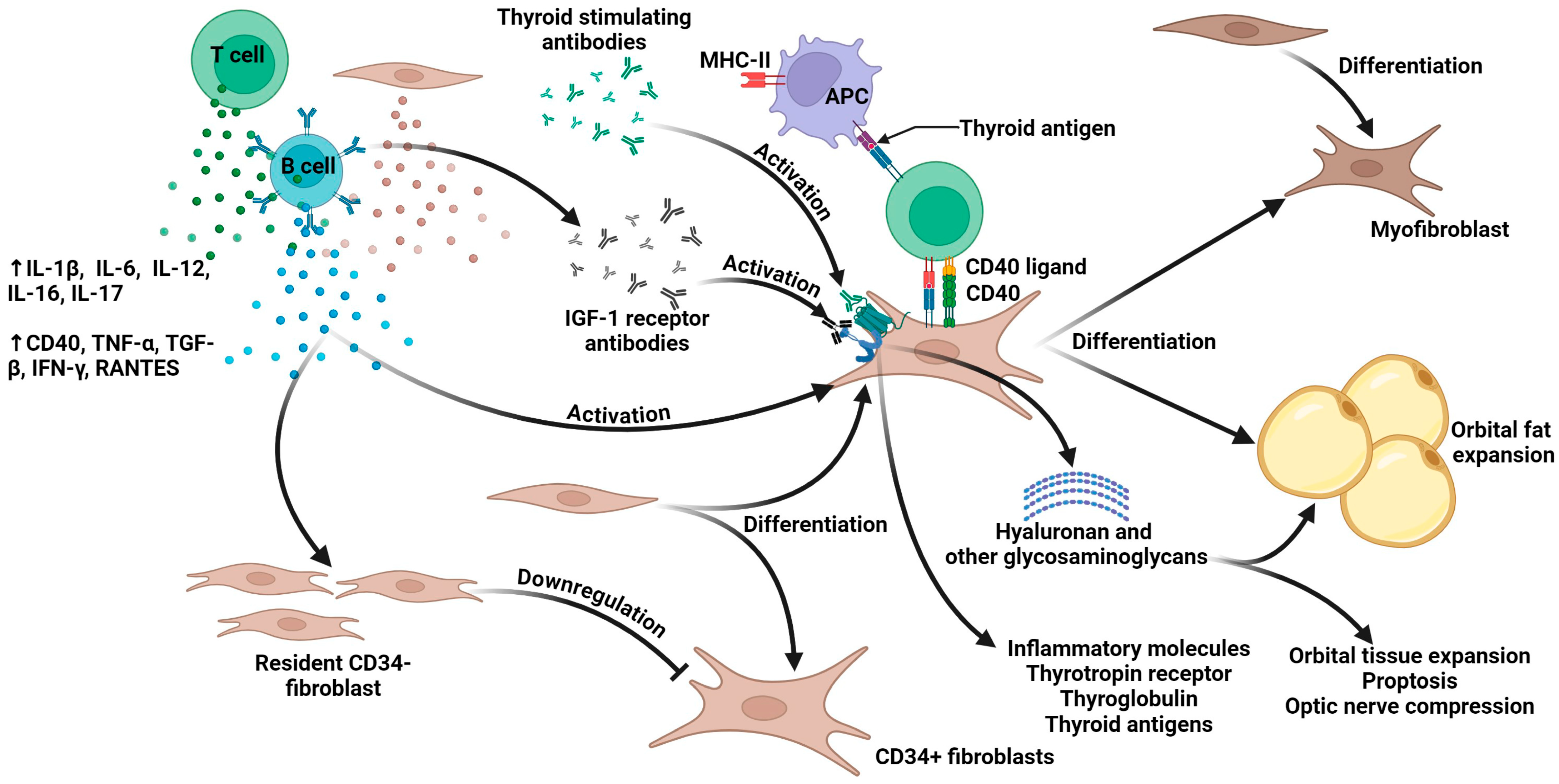
3. The Pathophysiology of Thyroid Eye Disease
4. The Traditional Clinical Management of TED
5. The Pharmacology of Teprotumumab
6. Clinical Translation of Teprotumumab: From Trials to Practice
6.1. Evidence from Pivotal Clinical Trials and FDA Approval
6.2. Real-World Evidence and Expanding Applications
7. Current Challenges in Teprotumumab Treatment
7.1. Safety Concerns and Adverse Events Profile
7.2. Economic Burden and Cost-Effectiveness Considerations
7.3. Treatment Durability and Insufficient Long-Term Data
8. Other Emerging IGF-1R Inhibitors for TED
9. Limitations
10. Conclusions and Future Directions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Rashad, R.; Pinto, R.; Li, E.; Sohrab, M.; Distefano, A.G. Thyroid Eye Disease. Life 2022, 12, 2084. [Google Scholar] [CrossRef]
- Ugradar, S.; Kang, J.; Kossler, A.L.; Zimmerman, E.; Braun, J.; Harrison, A.R.; Bose, S.; Cockerham, K.; Douglas, R.S. Teprotumumab for the treatment of chronic thyroid eye disease. Eye 2022, 36, 1553–1559. [Google Scholar] [CrossRef]
- Mallika, P.; Tan, A.; Aziz, S.; Alwi, S.S.; Chong, M.; Vanitha, R.; Intan, G. Thyroid associated ophthalmopathy—A review. Malays. Fam. Physician 2009, 4, 8–14. [Google Scholar]
- Nie, T.; Lamb, Y.N. Teprotumumab: A Review in Thyroid Eye Disease. Drugs 2022, 82, 1663–1670. [Google Scholar] [CrossRef] [PubMed]
- Scarabosio, A.; Surico, P.L.; Singh, R.B.; Tereshenko, V.; Musa, M.; D’Esposito, F.; Russo, A.; Longo, A.; Gagliano, C.; Agosti, E.; et al. Thyroid Eye Disease: Advancements in Orbital and Ocular Pathology Management. J. Pers. Med. 2024, 14, 776. [Google Scholar] [CrossRef]
- Markham, A. Teprotumumab: First Approval. Drugs 2020, 80, 509–512. [Google Scholar] [CrossRef] [PubMed]
- Douglas, R.S.; Kahaly, G.J.; Patel, A.; Sile, S.; Thompson, E.H.Z.; Perdok, R.; Fleming, J.C.; Fowler, B.T.; Marcocci, C.; Marinò, M.; et al. Teprotumumab for the Treatment of Active Thyroid Eye Disease. N. Engl. J. Med. 2020, 382, 341–352. [Google Scholar] [CrossRef] [PubMed]
- Smith Terry, J.; Kahaly George, J.; Ezra Daniel, G.; Fleming James, C.; Dailey Roger, A.; Tang Rosa, A.; Harris Gerald, J.; Antonelli, A.; Salvi, M.; Goldberg Robert, A.; et al. Teprotumumab for Thyroid-Associated Ophthalmopathy. N. Engl. J. Med. 2017, 376, 1748–1761. [Google Scholar] [CrossRef]
- Householder, N.A.; Ray, C. Teprotumumab’s Impact on Proptosis in Long-duration Thyroid Eye Disease: A Systematic Review and Meta-analysis. touchREVIEWS Endocrinol. 2024, 20, 100–109. [Google Scholar] [CrossRef]
- Abumohssin, A.G.; Alshareef, R.A.; Aljohani, S.; Alqutub, A.; Alqutub, A. Comparative efficacy and safety of rituximab, tocilizumab, and teprotumumab in Graves’ orbitopathy: A systematic review and meta-analysis. Eye 2025. [Google Scholar] [CrossRef]
- Huang, W.; Ou, X.; Lin, S.; Lin, W.; Chen, G.; Huang, H.; Wen, J. Efficacy and Safety of Teprotumumab in Thyroid Eye Disease: A Systematic Review and Meta-Analysis. Endocr. Pract. 2025, 31, 640–649. [Google Scholar] [CrossRef]
- Kamoi, K.; Uchimaru, K.; Tojo, A.; Watanabe, T.; Ohno-Matsui, K. HTLV-1 uveitis and Graves’ disease presenting with sudden onset of blurred vision. Lancet 2022, 399, 60. [Google Scholar] [CrossRef]
- Kamoi, K.; Watanabe, T.; Uchimaru, K.; Okayama, A.; Kato, S.; Kawamata, T.; Kurozumi-Karube, H.; Horiguchi, N.; Zong, Y.; Yamano, Y.; et al. Updates on HTLV-1 Uveitis. Viruses 2022, 14, 794. [Google Scholar] [CrossRef] [PubMed]
- Kamoi, K. Current challenges facing the clinical treatment for HTLV-1 ocular manifestations. Expert Rev. Ophthalmol. 2023, 18, 405–419. [Google Scholar] [CrossRef]
- Yang, M.; Kamoi, K.; Zong, Y.; Zhang, J.; Zou, Y.; Ohno-Matsui, K. Ripasudil as a Potential Therapeutic Agent in Treating Secondary Glaucoma in HTLV-1-Uveitis: An In Vitro Analysis. Int. J. Mol. Sci. 2024, 25, 3229. [Google Scholar] [CrossRef]
- Kamoi, K.; Okayama, A.; Izumo, S.; Hamaguchi, I.; Uchimaru, K.; Tojo, A.; Watanabe, T.; Ohno-Matsui, K. Tackling HTLV-1 infection in ophthalmology: A nationwide survey of ophthalmic care in an endemic country, Japan. Br. J. Ophthalmol. 2020, 104, 1647–1651. [Google Scholar] [CrossRef]
- Shan, S.J.C.; Douglas, R.S. The Pathophysiology of Thyroid Eye Disease. J. Neuro-Ophthalmol. 2014, 34, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Mishra, S.; Maurya, V.K.; Kumar, S.; Ankita; Kaur, A.; Saxena, S.K. Clinical management and therapeutic strategies for the thyroid-associated ophthalmopathy: Current and future perspectives. Curr. Eye Res. 2020, 45, 1325–1341. [Google Scholar] [CrossRef]
- Janssen, J.A.M.J.L.; Smith, T.J. Lessons Learned from Targeting IGF-I Receptor in Thyroid-Associated Ophthalmopathy. Cells 2021, 10, 383. [Google Scholar] [CrossRef]
- García-Mato, Á.; Cervantes, B.; Murillo-Cuesta, S.; Rodríguez-de la Rosa, L.; Varela-Nieto, I. Insulin-like Growth Factor 1 Signaling in Mammalian Hearing. Genes 2021, 12, 1553. [Google Scholar] [CrossRef]
- Yakar, S.; Adamo, M.L. Insulin-like growth factor 1 physiology: Lessons from mouse models. Endocrinol. Metab. Clin. N. Am. 2012, 41, 231–247. [Google Scholar] [CrossRef] [PubMed]
- Adams, T.E.; Epa, V.C.; Garrett, T.P.J.; Ward, C.W. Structure and function of the type 1 insulin-like growth factor receptor. Cell. Mol. Life Sci. CMLS 2000, 57, 1050–1093. [Google Scholar] [CrossRef]
- Bailes, J.; Soloviev, M. Insulin-Like Growth Factor-1 (IGF-1) and Its Monitoring in Medical Diagnostic and in Sports. Biomolecules 2021, 11, 217. [Google Scholar] [CrossRef] [PubMed]
- Khong, J.J.; McNab, A.A.; Ebeling, P.R.; Craig, J.E.; Selva, D. Pathogenesis of thyroid eye disease: Review and update on molecular mechanisms. Br. J. Ophthalmol. 2016, 100, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.S.; Kikkawa, D.O. Thyroid eye disease: From pathogenesis to targeted therapies. Taiwan J. Ophthalmol. 2022, 12, 3–11. [Google Scholar] [CrossRef]
- Shu, X.; Shao, Y.; Chen, Y.; Zeng, C.; Huang, X.; Wei, R. Immune checkpoints: New insights into the pathogenesis of thyroid eye disease. Front. Immunol. 2024, 15, 1392956. [Google Scholar] [CrossRef]
- Fang, S.; Lu, Y.; Huang, Y.; Zhou, H.; Fan, X. Mechanisms That Underly T Cell Immunity in Graves’ Orbitopathy. Front. Endocrinol. 2021, 12, 648732. [Google Scholar] [CrossRef]
- Wiersinga, W.M. Etiology and Pathogenesis of Graves’ Orbitopathy. In Surgery in and Around the Orbit: CrossRoads; Gooris, P.J.J., Mourits, M.P., Bergsma, J.E., Eds.; Springer International Publishing: Cham, Switzerland, 2023; pp. 279–285. [Google Scholar]
- Salvi, M.; Vannucchi, G.; Beck-Peccoz, P. Potential utility of rituximab for Graves’ orbitopathy. J. Clin. Endocrinol. Metab. 2013, 98, 4291–4299. [Google Scholar] [CrossRef]
- Murdock, J.; Nguyen, J.; Hurtgen, B.J.; Andorfer, C.; Walsh, J.; Lin, A.; Tubbs, C.; Erickson, K.; Cockerham, K. The role of IL-6 in thyroid eye disease: An update on emerging treatments. Front. Ophthalmol. 2025, 5, 1544436. [Google Scholar] [CrossRef]
- Smith, T.J. Understanding Pathogenesis Intersects With Effective Treatment for Thyroid Eye Disease. J. Clin. Endocrinol. Metab. 2022, 107 (Suppl. 1), S13–S26. [Google Scholar] [CrossRef]
- Bartalena, L.; Kahaly, G.J.; Baldeschi, L.; Dayan, C.M.; Eckstein, A.; Marcocci, C.; Marinò, M.; Vaidya, B.; Wiersinga, W.M.; EUGOGO. The 2021 European Group on Graves’ orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves’ orbitopathy. Eur. J. Endocrinol. 2021, 185, G43–G67. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Liu, L. Advances of IGF-1R inhibitors in Graves’ ophthalmopathy. Int. Ophthalmol. 2024, 44, 435. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Mester, T.; Raychaudhuri, N.; Kauh, C.Y.; Gupta, S.; Smith, T.J.; Douglas, R.S. Teprotumumab, an IGF-1R Blocking Monoclonal Antibody Inhibits TSH and IGF-1 Action in Fibrocytes. J. Clin. Endocrinol. Metab. 2014, 99, E1635–E1640. [Google Scholar] [CrossRef] [PubMed]
- Fernando, R.; Caldera, O.; Smith, T.J. Therapeutic IGF-I receptor inhibition alters fibrocyte immune phenotype in thyroid-associated ophthalmopathy. Proc. Natl. Acad. Sci. USA 2021, 118, e2114244118. [Google Scholar] [CrossRef]
- Krieger, C.C.; Sui, X.; Kahaly, G.J.; Neumann, S.; Gershengorn, M.C. Inhibition of TSH/IGF-1 Receptor Crosstalk by Teprotumumab as a Treatment Modality of Thyroid Eye Disease. J. Clin. Endocrinol. Metab. 2022, 107, e1653–e1660. [Google Scholar] [CrossRef]
- Burch, H.B.; Perros, P.; Bednarczuk, T.; Cooper, D.S.; Dolman, P.J.; Leung, A.M.; Mombaerts, I.; Salvi, M.; Stan, M.N. Management of thyroid eye disease: A Consensus Statement by the American Thyroid Association and the European Thyroid Association. Eur. Thyroid J. 2022, 11, e220189. [Google Scholar] [CrossRef]
- Xin, Y.; Xu, F.; Gao, Y.; Bhatt, N.; Chamberlain, J.; Sile, S.; Hammel, S.; Holt, R.J.; Ramanathan, S. Pharmacokinetics and Exposure-Response Relationship of Teprotumumab, an Insulin-Like Growth Factor-1 Receptor-Blocking Antibody, in Thyroid Eye Disease. Clin. Pharmacokinet. 2021, 60, 1029–1040. [Google Scholar] [CrossRef]
- Douglas, R.S.; Kossler, A.L.; Abrams, J.; Briceño, C.A.; Gay, D.; Harrison, A.; Lee, M.; Nguyen, J.; Joseph, S.S.; Schlachter, D.; et al. Expert Consensus on the Use of Teprotumumab for the Management of Thyroid Eye Disease Using a Modified-Delphi Approach. J. Neuroophthalmol. 2022, 42, 334–339. [Google Scholar] [CrossRef]
- Kahaly, G.J.; Douglas, R.S.; Holt, R.J.; Sile, S.; Smith, T.J. Teprotumumab for patients with active thyroid eye disease: A pooled data analysis, subgroup analyses, and off-treatment follow-up results from two randomised, double-masked, placebo-controlled, multicentre trials. Lancet Diabetes Endocrinol. 2021, 9, 360–372. [Google Scholar] [CrossRef]
- Douglas, R.S.; Kahaly, G.J.; Ugradar, S.; Elflein, H.; Ponto, K.A.; Fowler, B.T.; Dailey, R.; Harris, G.J.; Schiffman, J.; Tang, R.; et al. Teprotumumab Efficacy, Safety, and Durability in Longer-Duration Thyroid Eye Disease and Re-treatment: OPTIC-X Study. Ophthalmology 2022, 129, 438–449. [Google Scholar] [CrossRef]
- Diniz, S.B.; Cohen, L.M.; Roelofs, K.A.; Rootman, D.B. Early Experience With the Clinical Use of Teprotumumab in a Heterogenous Thyroid Eye Disease Population. Ophthalmic Plast. Reconstr. Surg. 2021, 37, 583–591. [Google Scholar] [CrossRef] [PubMed]
- Sears, C.M.; Wang, Y.; Bailey, L.A.; Turbin, R.; Subramanian, P.S.; Douglas, R.; Cockerham, K.; Kossler, A.L. Early efficacy of teprotumumab for the treatment of dysthyroid optic neuropathy: A multicenter study. Am. J. Ophthalmol. Case Rep. 2021, 23, 101111. [Google Scholar] [CrossRef] [PubMed]
- Ugradar, S.; Braun, J.; Wang, Y.; Zimmerman, E.; Douglas, R.S. Facial and Eyelid Changes in Thyroid Eye Disease Are Reversed by Teprotumumab. Plast. Reconstr. Surg. Glob. Open 2021, 9, e3809. [Google Scholar] [CrossRef]
- Wang, Y.; Mester, T.; Ugradar, S.; Douglas, R. Teprotumumab for the Treatment of Thyroid Eye Disease: Clinical Experience from Expanded Access Program (EAP). Investig. Ophthalmol. Vis. Sci. 2021, 62, 3339. [Google Scholar]
- Douglas, R.S.; Wang, Y.; Bruch, J.; Anzeljc, A.; Sile, S.; Vescio, T.; Phelps, P.; Ramesh, S.; Wulc, A.; Meador, A.; et al. Teprotumumab use in a real-world setting: Expanded access program findings. Investig. Ophthalmol. Vis. Sci. 2021, 62, 3345. [Google Scholar]
- Ugradar, S.; Douglas, R. RF35 | PSAT268 Reversal of Graves’ Disease Associated Facial Volume Expansion and Eyelid Changes Following Teprotumumab Therapy. J. Endocr. Soc. 2022, 6 (Suppl. 1), A861–A862. [Google Scholar] [CrossRef]
- Adetunji, M.O.; Nguyen, B.J.; McGeehan, B.; Tamhankar, M.A.; Briceño, C.A. Effect of teprotumumab on intraocular pressure in thyroid-associated ophthalmopathy. Taiwan J. Ophthalmol. 2022, 12, 325–329. [Google Scholar] [CrossRef]
- Kotwal, A. Real-World Use of Teprotumumab and Tocilizumab in Moderate-to-Severe Steroid-Resistant Thyroid Eye Disease. Clin. Thyroidol. 2023, 35, 364–367. [Google Scholar] [CrossRef]
- Ho, T.C.; Maamari, R.N.; Kossler, A.L.; Sears, C.M.; Freitag, S.K.; Reshef, E.R.; Shinder, R.; Rootman, D.B.; Diniz, S.B.; Kahana, A.; et al. Outcomes of Patients With Thyroid Eye Disease Partially Treated With Teprotumumab. Ophthalmic Plast. Reconstr. Surg. 2023, 39, 150–155. [Google Scholar] [CrossRef]
- Douglas, R.S.; Couch, S.; Wester, S.T.; Fowler, B.T.; Liu, C.Y.; Subramanian, P.S.; Tang, R.; Nguyen, Q.T.; Maamari, R.N.; Ugradar, S.; et al. Efficacy and Safety of Teprotumumab in Patients With Thyroid Eye Disease of Long Duration and Low Disease Activity. J. Clin. Endocrinol. Metab. 2023, 109, 25–35. [Google Scholar] [CrossRef]
- Shah, S.A.; Amarikwa, L.; Sears, C.M.; Clauss, K.D.; Rajjoub, R.D.; Kang, J.Y.; Tamhankar, M.A.; Briceño, C.A.; Harrison, A.R.; Dosiou, C.; et al. Teprotumumab-Related Adverse Events in Thyroid Eye Disease: A Multicenter Study. Ophthalmology 2024, 131, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Men, C.J.; Amarikwa, L.; Pham, B.; Sears, C.; Clauss, K.; Lee, B.W.; Lee, W.W.; Pasol, J.; Ugradar, S.; Shinder, R.; et al. Teprotumumab for the Treatment of Recalcitrant Thyroid Eye Disease. Ophthalmic Plast. Reconstr. Surg. 2024, 40, 276–285. [Google Scholar] [CrossRef] [PubMed]
- Hiromatsu, Y.; Ishikawa, E.; Kozaki, A.; Takahashi, Y.; Tanabe, M.; Hayashi, K.; Imagawa, Y.; Kaneda, K.; Mimura, M.; Dai, X.; et al. A randomised, double-masked, placebo-controlled trial evaluating the efficacy and safety of teprotumumab for active thyroid eye disease in Japanese patients. Lancet Reg. Health West. Pac. 2025, 55, 101464. [Google Scholar] [CrossRef]
- Ugradar, S.; Parunakian, E.; Malkhasyan, E.; Raika, P.; Tolentino, J.; Kossler, A.L.; Cockerham, K.; Amarikwa, L.; Weinberg, D.A.; Douglas, R.S. Teprotumumab for thyroid eye disease in patients with hypothyroid/euthyroid state: A multicenter case series. Graefe’s Arch. Clin. Exp. Ophthalmol. 2025, 263, 225–230. [Google Scholar] [CrossRef]
- Ugradar, S.; Parunakian, E.; Malkhasyan, E.; Chiou, C.A.; Walsh, H.L.; Tolentino, J.; Wester, S.T.; Freitag, S.K.; Douglas, R.S. The Rate of Re-treatment in Patients Treated with Teprotumumab: A Multicenter Study of 119 Patients with 1 Year of Follow-up. Ophthalmology 2025, 132, 92–97. [Google Scholar] [CrossRef]
- Lustig-Barzelay, Y.; Yagoda, D.; Zunz, E.; Hamed-Azzam, S.; Avisar, I.; Kehat-Ophir, S.; Gur, Z.; Cukierman-Yaffe, T.; Agmon-Levin, N.; Landau-Prat, D.; et al. Time to improvement following teprotumumab treatment of thyroid eye disease: Real world experience. Graefe’s Arch. Clin. Exp. Ophthalmol. 2025. [Google Scholar] [CrossRef]
- Zong, Y.; Miyagaki, M.; Yang, M.; Zhang, J.; Zou, Y.; Ohno-Matsui, K.; Kamoi, K. Ophthalmic Use of Targeted Biologics in the Management of Intraocular Diseases: Current and Emerging Therapies. Antibodies 2024, 13, 86. [Google Scholar] [CrossRef] [PubMed]
- Zong, Y.; Kamoi, K.; Miyagaki, M.; Zhang, J.; Yang, M.; Zou, Y.; Ohno-Matsui, K. Applications of Biological Therapy for Latent Infections: Benefits and Risks. Int. J. Mol. Sci. 2024, 25, 9184. [Google Scholar] [CrossRef]
- Kulbay, M.; Tanya, S.M.; Tuli, N.; Dahoud, J.; Dahoud, A.; Alsaleh, F.; Arthurs, B.; El-Hadad, C. A Comprehensive Review of Thyroid Eye Disease Pathogenesis: From Immune Dysregulations to Novel Diagnostic and Therapeutic Approaches. Int. J. Mol. Sci. 2024, 25, 11628. [Google Scholar] [CrossRef]
- Ugradar, S.; Shi, L.; Wang, Y.; Mester, T.; Yang, H.; Douglas, R.S. Teprotumumab for non-inflammatory thyroid eye disease (TED): Evidence for increased IGF-1R expression. Eye 2021, 35, 2607–2612. [Google Scholar] [CrossRef]
- Blandford, A.D.; Zhang, D.; Chundury, R.V.; Perry, J.D. Dysthyroid optic neuropathy: Update on pathogenesis, diagnosis, and management. Expert Rev. Ophthalmol. 2017, 12, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Douglas, R.S.; Dailey, R.; Subramanian, P.S.; Barbesino, G.; Ugradar, S.; Batten, R.; Qadeer, R.A.; Cameron, C. Proptosis and Diplopia Response With Teprotumumab and Placebo vs the Recommended Treatment Regimen With Intravenous Methylprednisolone in Moderate to Severe Thyroid Eye Disease: A Meta-analysis and Matching-Adjusted Indirect Comparison. JAMA Ophthalmol. 2022, 140, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Kahaly, G.J.; Xi, A.; Barretto, N.; Patel, H.; Qashqai, A.; Shokoohi, M.; Spin, P.; Holt, R.J. Teprotumumab Improves Quality of Life in Thyroid Eye Disease: Meta-analysis and Matching-adjusted Indirect Comparison. J. Endocr. Soc. 2025, 9, bvaf063. [Google Scholar] [CrossRef]
- Stan, M.N.; Krieger, C.C. The Adverse Effects Profile of Teprotumumab. J. Clin. Endocrinol. Metab. 2023, 108, e654–e662. [Google Scholar] [CrossRef] [PubMed]
- TEPEZZA-Prescribing-Information.pdf. Available online: https://fda.report/DailyMed/3e6c54a1-cefd-4a5b-a855-ab9f268b6cce (accessed on 24 May 2025).
- Amarikwa, L.; Mohamed, A.; Kim, S.H.; Kossler, A.L.; Dosiou, C. Teprotumumab-Related Hyperglycemia. J. Clin. Endocrinol. Metab. 2023, 108, 858–864. [Google Scholar] [CrossRef]
- Hoang, T.D.; Nguyen, N.T.; Chou, E.; Shakir, M.K. Rapidly progressive cognitive decline associated with teprotumumab in thyroid eye disease. BMJ Case Rep. 2021, 14, e242153. [Google Scholar] [CrossRef]
- Yee, M.D.; McCarthy, J.; Quinn, B.; Surani, A. Teprotumumab-Induced Encephalopathy: A Rare Side Effect of a Novel Therapeutic. WMJ 2023, 122, 134–137. [Google Scholar]
- Martel, A.; Rocher, F.; Gerard, A. Teprotumumab for the Treatment of Thyroid Eye Disease: Why Should We Keep Our Eyes “Wide Open”?—A Clinical and Pharmacovigilance Point of View. J. Pers. Med. 2024, 14, 1027. [Google Scholar] [CrossRef]
- Shah, S.A.; Lu, T.; Yu, M.; Hiniker, S.; Dosiou, C.; Kossler, A.L. Comparison of treatment cost and quality-of-life impact of thyroid eye disease therapies. Investig. Ophthalmol. Vis. Sci. 2022, 63, 4002-A0344. [Google Scholar]
- Rosenblatt, T.R.; Chiou, C.A.; Yoon, M.K.; Wolkow, N.; Lee, N.G.; Freitag, S.K. Proptosis Regression After Teprotumumab Treatment for Thyroid Eye Disease. Ophthalmic Plast. Reconstr. Surg. 2024, 40, 187–191. [Google Scholar] [CrossRef]
- Amgen Study of Teprotumumab in Participants with Thyroid Eye Disease (TED) (NCT05002998). Available online: https://clinicaltrials.gov/study/NCT05002998 (accessed on 24 May 2025).
- Viridian Announces Positive Data from Ongoing Phase 1/2 Trial Evaluating VRDN-001 in Patients Diagnosed with Chronic TED. Available online: https://www.ophthalmologytimes.com/view/viridian-announces-positive-data-from-ongoing-phase-1-2-trial-evaluating-vrdn-001-in-patients-diagnosed-with-chronic-ted (accessed on 22 June 2025).
- Jiayun Men, C.; Kossler, A.L. Advances in the Medical Treatment of Thyroid Eye Disease: Current and Emerging Therapies. touchREVIEWS Ophthalmol. 2024, 18, 33–40. [Google Scholar] [CrossRef]
- Salvi, M.; Foster, K.; Dickinson, B.; Matthew, A.; Vijayaraghavan, J.; Michalsky, C.; Bedian, V. VRDN-003, a full antagonist antibody to IGF-1R for thyroid eye disease (TED): Phase 1 results show potential for subcutaneous administration. Presented at the 46th Annual Meeting of the European Thyroid Association (ETA) 2024, Athens, Greece, 7–10 September 2024; Volume 101, p. OP-13-01, Endocrine Abstracts. [Google Scholar] [CrossRef]
- Luffy, M.; Ganz, A.-L.; Wagner, S.; Wolf, J.; Ropertz, J.; Zeidan, R.; Kent, J.D.; Douglas, R.S.; Kahaly, G.J. Linsitinib inhibits proliferation and induces apoptosis of both IGF-1R and TSH-R expressing cells. Front. Immunol. 2024, 15, 1488220. [Google Scholar] [CrossRef] [PubMed]
- Ugradar, S.; Kostick, D.; Spadaro, J.; Grover, A.; Imm, S.; Chesler, S.; Mpofu, S.; Khong, J. Preliminary Safety and Efficacy of Subcutaneous Lonigutamab (anti-IGF-1R) From a Phase 1/2 Proof of Concept Study in Patients With Thyroid Eye Disease. J. Endocr. Soc. 2024, 8, A1067–A1068. [Google Scholar] [CrossRef]

{kind=link}
| Treatment Phase | Disease Stage | Therapeutic Approach | Intervention | Clinical Indications | Key Considerations |
|---|---|---|---|---|---|
| Initial Management | All Stages | Foundational Measures |
| All newly diagnosed TED cases |
|
| Ocular Support |
| Universal TED presentation | Heightened vigilance for keratopathy | ||
| Behavioral Modification |
| All TED patients | Tobacco use exacerbates disease progression | ||
| Specialist Consultation | Referral to TED multidisciplinary center | Moderate to severe or progressive disease | Facilitates timely, tailored management | ||
| Mild TED | Active Phase | Pharmacotherapy |
| Mild active TED, particularly in endemic selenium-deficient areas |
|
| Surveillance |
| Stable, minimally symptomatic presentations | Escalate therapy if progression occurs | ||
| Inactive Phase | Reconstructive Intervention |
| Persistent retraction or cosmetic impairment | Requires ≥ 6 months of thyroid stability | |
| Moderate-to-Severe TED | Active Phase | Intravenous Corticosteroids |
| Active inflammatory moderate to severe TED |
|
| Biologic Agents |
|
| Limited longitudinal data on efficacy | ||
| Radiotherapy |
| Progressive ocular motility impairment or steroid contraindications |
| ||
| Inactive Phase | Surgical Correction |
| Quiescent disease (≥6 months) with residual functional/aesthetic deficits |
| |
| Sight-Threatening TED | Active Phase | Urgent Medical Therapy |
| Dysthyroid optic neuropathy or acute visual decline | Surgical decompression if inadequate response within 2 weeks |
| Emergency Surgery |
| Vision deterioration despite medical therapy | Requires subspecialty orbital surgical expertise | ||
| Corneal Salvage |
| Impending corneal perforation or ulceration | Surgical delay risks irreversible visual loss |
| Study Design | Sample Size | Patient Characteristics | Treatment Dosage | Primary Outcomes | Secondary Outcomes | Notes | Study |
|---|---|---|---|---|---|---|---|
| Cross-sectional cohort | 21 | Heterogeneous TED including three DON cases | 8 doses | 71.4% achieved ≥2 mm proptosis reduction | CAS −2.2, motility +16.9° | DON cases improved | Diniz et al., 2021 [42] |
| Multicenter case series | 10 | DON patients in whom conventional therapy failed | 8 infusions | VA improvement = 0.87 logMAR | Proptosis −4.7 mm, CAS −5.25 | Rapid DON improvement | Sears et al., 2021 [43] |
| Prospective longitudinal | 23 | Patients with TED accompanied by facial/eyelid changes | 8 infusions | Reduction in facial soft tissue volume | Improvement in eyelid position | Orbital soft tissue expansion was also reduced | Ugradar et al., 2021 [44] |
| Retrospective EAP study | 13 | Active moderate–severe TED | 8 infusions (77%) | Proptosis −4.6 mm | CAS −4.0, light sensitivity −9.1 | Expanded access program | Wang et al., 2021 [45] |
| EAP study | 22 | Active moderate–severe TED | 8 infusions (86%) | QOL improvement | Not specified | All patients reported AEs; mainly muscle spasms (n = 11), fatigue (n = 10) | Douglas et al., 2021 [46] |
| Prospective longitudinal | 43 | Active TED with facial changes | 8 infusions | Facial volume reduction (mean decrease = 8.4 mL) | Proptosis improvement | Pan-facial assessment | Ugradar & Douglas, 2022 [47] |
| Retrospective review | 31 | Chronic TED (>2 years) | Mean: 7 infusions | Proptosis −3.5 mm | 67% diplopia improvement | Teprotumumab treatment had therapeutic efficacy in patients with chronic TED | Ugradar et al., 2022 [2] |
| Retrospective review | 17 | TED with IOP concerns | Mean: 12 weeks | Mean IOP was decreased at last record of follow-up by 4.9 mm Hg | Not specified | Teprotumumab treatment reduced IOP | Adetunji et al., 2022 [48] |
| Retrospective study | 37 | Steroid-naive and steroid-resistant TED | Up to 8 infusions | 81% proptosis response in steroid-resistant group | 45% diplopia resolution, 86% disease inactivation | Comparison with tocilizumab | Kotwal et al., 2023 [49] |
| Observational cross-sectional | 74 | Active (n = 62) and minimal-activity (n = 12) TED; treatment interrupted | Average of 4.2 infusions | Proptosis: −2.9 mm (active), −2.8 mm (minimal) | CAS −3.4 | COVID-19 interrupted this study | Ho et al., 2023 [50] |
| RCT | 62 | Chronic/low-activity TED (2–10 years) | 8 infusions | Proptosis: −2.41 mm vs. −0.92 mm(placebo) | Not specified | First chronic placebo-controlled trial with TED | Douglas et al., 2023 [51] |
| Multicenter retrospective | 131 | All stages/activity levels of TED | ≥4 infusions | 76% achieved proptosis −3.0 mm | 3.2-point average CAS reduction, GDS improved by at least 1 point for 50% | Comprehensive AE study | Shah et al., 2024 [52] |
| Multicenter retrospective | 66 | Recalcitrant TED for which conventional therapy failed | ≥4 infusions | 85.9% proptosis response | CAS 93.8%, diplopia 69.1% | Poor response post-decompression | Men et al., 2024 [53] |
| RCT | 54 | Active moderate–severe TED in Japanese cohort | 8 infusions | 89% vs. 11% (placebo) proptosis responses | 78% vs. 4% (placebo) overall responses | First Japanese RCT | Hironmatsu et al., 2025 [54] |
| Multicenter case series | 26 | Hypothyroid/euthyroid TED | 8 infusions | Proptosis −2.7 mm | CAS and diplopia improvements | Non-hyperthyroid TED | Ugradar et al., 2025 [55] |
| Multicenter retrospective | 119 | Complete treatment with 1-year follow-up | 8 infusions | 24% re-treatment rate | Not specified | Age was the only significant driver of re-treatment | Ugradar et al., 2025 [56]. |
| Retrospective cohort study | 32 | Failed intravenous glucocorticoid treatment; four with prior decompression surgery | 8 infusions | Proptosis: R −2.4 mm, L −2.0 mm | Improvement in diplopia | One case of teprotumumab-induced encephalopathy was reported and successfully treated using plasma exchange; decompression surgery history did not affect efficacy | Lustig-Barzelay et al., 2025 [57] |
| Author (Year) | Patients Treated with Teprotumumab | Total AE Rate | Common AEs (>10%) | Serious AEs | Special Notes |
|---|---|---|---|---|---|
| Ho et al., 2023 [50] | 74 | Initial: 66% Final: 29% | - Muscle spasms (27%) - Alopecia (18%) - Hyperglycemia (14%) - Hearing changes (11%) - Fatigue (9%) - GI discomfort (8%) | Three new diabetes cases; one severe hyperglycemia case (>700 mg/dL) | - AEs decreased over time - No new DON cases during interruption - One patient discontinued treatment due to hyperglycemia—three patients required oral diabetes medication |
| Diniz et al., 2021 [42] | 21 | 85.7% | - Fatigue (43%) - Muscle spasms (33%) - Dysgeusia (26%) - Nausea (19%) - Weight loss (14%) - Hearing issues (14%) - Hyperglycemia (14%) | Three cases requiring diabetes medication | - Most AEs were of a grade 1–2 severity - One discontinuation due to multiple AEs - Two/three hyperglycemia cases in non-diabetic patients - Age may be risk factor for hearing issues |
| Lustig-Barzelay et al., 2025 [57] | 32 | Not specified | - Myalgia (n = 12%) - Hyperglycemia (n = 9%) - Diarrhea (n = 9%) - Hearing issues (n = 12%) | One case of encephalopathy | - Encephalopathy successfully treated with plasmapheresis - Real-world Israeli cohort experience |
| Douglas et al., 2021 [46] | 22 | 100% | - Muscle spasms (50%) - Fatigue (45%) - Hypoacusis (23%)–headache (23%) - Nausea (23%) - Extremity pain (18%)–alopecia (18%) - Hypertension (18%) | One case of appendicitis (deemed unrelated) | - Multiple other AEs reported in smaller numbers (n = 3): dry skin, diarrhea, tinnitus, myalgia, increased lacrimation, hypogeusia |
| Kotwal et al., 2023 [49] | 37 | 76% | - Hearing changes (46%) - Hyperglycemia (23%) | Not specified | - Compared with the tocilizumab group which reported no AEs |
| Shah et al., 2024 [52] | 131 | 82% | - Musculoskeletal (58.0%) - GI (38%) - Skin (38%) - Ear/hearing (31%) - Nervous system (21%) - Metabolic (15%)–reproductive (12%) | 8.4% (11/131) severe AEs | - Mean AE onset: 7.9 weeks - Mean duration: 17.6 weeks - 46% had persistent AEs at last follow- up - 12.2% discontinued therapy (hearing loss n = 4, IBD n = 2, hyperglycemia n = 1, muscle spasms n = 1, multiple AEs n = 8) |
| Hironmatsu et al., 2025 [54] | 27 | Not specified | - Hyperglycemia (22%) - Hearing impairment (15%) | Not specified | - The Japanese population - Placebo-controlled comparison available |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zong, Y.; Qiu, S.; Yang, M.; Zhang, J.; Zou, Y.; Jing, Y.; Ohno-Matsui, K.; Kamoi, K. Teprotumumab for Thyroid Eye Disease: Mechanism, Clinical Efficacy, and Current Challenges. Antibodies 2025, 14, 55. https://doi.org/10.3390/antib14030055
Zong Y, Qiu S, Yang M, Zhang J, Zou Y, Jing Y, Ohno-Matsui K, Kamoi K. Teprotumumab for Thyroid Eye Disease: Mechanism, Clinical Efficacy, and Current Challenges. Antibodies. 2025; 14(3):55. https://doi.org/10.3390/antib14030055
Chicago/Turabian StyleZong, Yuan, Shuang Qiu, Mingming Yang, Jing Zhang, Yaru Zou, Yuxin Jing, Kyoko Ohno-Matsui, and Koju Kamoi. 2025. "Teprotumumab for Thyroid Eye Disease: Mechanism, Clinical Efficacy, and Current Challenges" Antibodies 14, no. 3: 55. https://doi.org/10.3390/antib14030055
APA StyleZong, Y., Qiu, S., Yang, M., Zhang, J., Zou, Y., Jing, Y., Ohno-Matsui, K., & Kamoi, K. (2025). Teprotumumab for Thyroid Eye Disease: Mechanism, Clinical Efficacy, and Current Challenges. Antibodies, 14(3), 55. https://doi.org/10.3390/antib14030055