
A Nationwide Seroprevalence Study for Measles in Individuals of Fertile Age in Romania

 ,
,  , ,
, ,  , ,
, ,
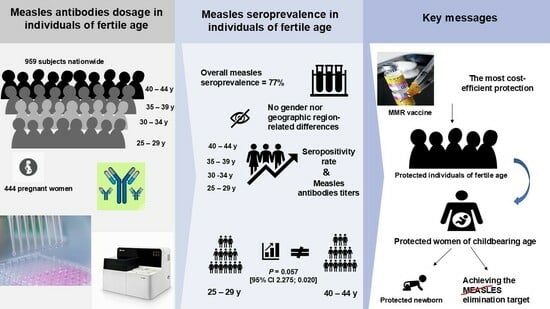
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guerra, F.M.; Bolotin, S.; Lim, G.; Heffernan, J.; Deeks, S.L.; Li, Y.; Crowcroft, N.S. The basic reproduction number (R0) of measles: A systematic review. Lancet Infect. Dis. 2017, 17, e420–e428. [Google Scholar] [CrossRef] [PubMed]
- Plans-Rubió, P. Are the Objectives Proposed by the WHO for Routine Measles Vaccination Coverage and Population Measles Immunity Sufficient to Achieve Measles Elimination from Europe? Vaccines 2020, 8, 218. [Google Scholar] [CrossRef] [PubMed]
- Immunization Agenda 2030: A Global Strategy to Leave No One Behind. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/strategies/ia2030 (accessed on 5 July 2024).
- WHO Regional Office for Europe. European Immunization Agenda 2030; World Health Organization: Geneva, Switzerland, 2021; ISBN 978-92-890-5605-2.
- Patricia, C.R.N.; Zulay, J.P.Y.; Carlos, R.L.J.; Alejandra, C.M.; Cristina, J.S.R.; Josefina, R.V. The Influence of Antivaccination Movements on the Re-emergence of Measles. J. Pure Appl. Microbiol. 2019, 13, 127–132. [Google Scholar]
- European Centre for Diseases Control, Measles on the Rise in the EU/EEA: Considerations for Public Health Response, 16 February 2024. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/measles-eu-threat-assessment-brief-february-2024.pdf (accessed on 27 June 2024).
- Muscat, M.; Ben Mamou, M.; Reynen-de Kat, C.; Jankovic, D.; Hagan, J.; Singh, S.; Datta, S.S. Progress and Challenges in Measles and Rubella Elimination in the WHO European Region. Vaccines 2024, 12, 696. [Google Scholar] [CrossRef]
- European Centre for Diseases Control. Weekly Communicable Disease Threats Report, Week 41, 5–11 October 2024. Available online: https://www.ecdc.europa.eu/en/publications-data/communicable-disease-threats-report-5-11-october-2024-week-41 (accessed on 15 October 2024).
- Hayman, D.T.S. Measles vaccination in an increasingly immunized and developed world. Hum. Vaccin. Immunother. 2019, 15, 28–33. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Manual for the Laboratory-Based Surveillance of Measles, Rubella, and Congenital Rubella Syndrome. Laboratory Testing for Determination of Population Immune Status. Available online: https://www.who.int/publications/m/item/chapter-9-manual-for-the-laboratory-based-surveillance-of-measles-rubella-and-congenital-rubella-syndrome (accessed on 20 December 2024).
- Sbarra, A.N.; Cutts, F.T.; Fu, H.; Poudyal, I.; Rhoda, D.A.; Mosser, J.F.; Jit, M. Evaluating Scope and Bias of Population-Level Measles Serosurveys: A Systematized Review and Bias Assessment. Vaccines 2024, 12, 585. [Google Scholar] [CrossRef]
- Khetsuriani, N.; Chitadze, N.; Russell, S.; Ben Mamou, M. Measles and rubella seroprevalence among adults in Georgia in 2015: Helping guide the elimination efforts. Epidemiol. Infect. 2019, 147, e319. [Google Scholar] [CrossRef] [PubMed]
- Winter, A.K.; Martinez, M.E.; Cutts, F.T.; Moss, W.J.; Ferrari, M.J.; McKee, A.; Lessler, J.; Hayford, K.; Wallinga, J.; Metcalf, C.J.E. Benefits and Challenges in Using Seroprevalence Data to Inform Models for Measles and Rubella Elimination. J. Infect. Dis. 2018, 218, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Kafatos, G.; Andrews, N.; McConway, K.J.; Anastassopoulou, C.; Barbara, C.; De Ory, F.; Johansen, K.; Mossong, J.; Prosenc, K.; Vranckx, R.; et al. Estimating seroprevalence of vaccine-preventable infections: Is it worth standardizing the serological outcomes to adjust for different assays and laboratories? Epidemiol. Infect. 2015, 143, 2269–2278. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Andrews, N.; Tischer, A.; Siedler, A.; Pebody, R.G.; Barbara, C.; Cotter, S.; Duks, A.; Gacheva, N.; Bohumir, K.; Johansen, K.; et al. Towards elimination: Measles susceptibility in Australia and 17 European countries. Bull. World Health Organ. 2008, 86, 197–204. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- National Center for Disease Control. Evolution Analysis of Communicable Diseases Under Surveillance, Annual Reports. Available online: https://vajiramandravi.com/upsc-daily-current-affairs/prelims-pointers/national-centre-for-disease-control-ncdc/ (accessed on 12 November 2024).
- Donadel, M.; Stanescu, A.; Pistol, A.; Stewart, B.; Butu, C.; Jankovic, D.; Paunescu, B.; Zimmerman, L. Risk factors for measles deaths among children during a Nationwide measles outbreak—Romania, 2016–2018. BMC Infect. Dis. 2021, 21, 279. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- National Institute of Public Health. National Centre for Communicable Diseases Surveillance and Control, Monthly Reports. Romanian. Available online: https://insp.gov.ro/informari-lunare/ (accessed on 12 November 2024).
- Stanescu, A.; Ruta, S.M.; Cernescu, C.; Pistol, A. Suboptimal MMR Vaccination Coverages—A Constant Challenge for Measles Elimination in Romania. Vaccines 2024, 12, 107. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Eurostat. The Statistical Office of the European Union, Reference Metadata, Fertility. Available online: https://ec.europa.eu/eurostat/cache/metadata/en/demo_fer_esms.htm (accessed on 10 June 2024).
- Steven, K.; Thompson, S. Wiley Series in Probability and Statistics, 3rd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2012; ISBN 978-0-470-40231-3. [Google Scholar]
- National Institute of Statistics. Romanian. Available online: http://statistici.insse.ro/tempoins/ (accessed on 10 June 2024).
- Wiedermann, U.; Garner-Spitzer, E.; Wagner, A. Primary vaccine failure to routine vaccines: Why and what to do? Hum. Vaccin. Immunother. 2016, 12, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Pambudi, N.A.; Sarifudin, A.; Gandidi, I.M.; Romadhon, R. Vaccine cold chain management and cold storage technology to address the challenges of vaccination programs. Energy Rep. 2022, 8, 955–972. [Google Scholar] [CrossRef]
- Griffin, D.E. The Immune Response in Measles: Virus Control, Clearance and Protective Immunity. Viruses 2016, 8, 282. [Google Scholar] [CrossRef]
- Nic Lochlainn, L.M.; de Gier, B.; van der Maas, N.; Strebel, P.M.; Goodman, T.; van Binnendijk, R.S.; de Melker, H.E.; Hahné, S.J.M. Immunogenicity, effectiveness, and safety of measles vaccination in infants younger than 9 months: A systematic review and meta-analysis. Lancet Infect. Dis. 2019, 19, 1235–1245. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gonçalves, G.; Frade, J.; Nunes, C.; Mesquita, J.R.; Nascimento, M.S. Persistence of measles antibodies, following changes in the recommended age for the second dose of MMR-vaccine in Portugal. Vaccine 2015, 33, 5057–5063. [Google Scholar] [CrossRef]
- Kang, H.J.; Han, Y.W.; Kim, S.J.; Kim, Y.J.; Kim, A.R.; Kim, J.A.; Jung, H.D.; Eom, H.E.; Park, O.; Kim, S.S. An increasing, potentially measles-susceptible population over time after vaccination in Korea. Vaccine 2017, 35, 4126–4132. [Google Scholar] [CrossRef] [PubMed]
- Ghafoori, F.; Mokhtari-Azad, T.; Foroushani, A.R.; Farahmand, M.; Shadab, A.; Salimi, V. Assessing seropositivity of MMR antibodies in individuals aged 2–22: Evaluating routine vaccination effectiveness after the 2003 mass campaign-a study from Iran’s National Measles Laboratory. BMC Infect. Dis. 2024, 24, 696. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Williamson, K.M.; Faddy, H.; Nicholson, S.; Stambos, V.; Hoad, V.; Butler, M.; Housen, T.; Merritt, T.; Durrheim, D.N. A Cross-Sectional Study of Measles-Specific Antibody Levels in Australian Blood Donors—Implications for Measles Post-Elimination Countries. Vaccines 2024, 12, 818. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Quach, H.Q.; Ovsyannikova, I.G.; Grill, D.E.; Warner, N.D.; Poland, G.A.; Kennedy, R.B. Seroprevalence of Measles Antibodies in a Highly MMR-Vaccinated Population. Vaccines 2022, 10, 1859. [Google Scholar] [CrossRef]
- Sarawanangkoor, N.; Wanlapakorn, N.; Srimuan, D.; Thatsanathorn, T.; Thongmee, T.; Poovorawan, Y. Persistence of Antibodies against Measles, Mumps, and Rubella after the Two-Dose MMR Vaccination: A 7-Year Follow-Up Study. Vaccines 2024, 12, 744. [Google Scholar] [CrossRef] [PubMed]
- Franconeri, L.; Antona, D.; Cauchemez, S.; Lévy-Bruhl, D.; Paireau, J. Two-dose measles vaccine effectiveness remains high over time: A French observational study, 2017–2019. Vaccine 2023, 41, 5797–5804. [Google Scholar] [CrossRef] [PubMed]
- Plotkin, S.A.; Orenstein, W.A.; Offit, P.; Edwards, K.M. Plotkin’s Vaccines, 7th ed.; Elsevier: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Antona, D.; Morel, P.; Jacquot, C.; Fonteneau, L.; Dina, J.; Vauloup-Fellous, C.; Gimeno, L.; Degeorges, A.; Gallian, P.; Lévy-Bruhl, D. Measles and rubella seroprevalence in a population of young adult blood donors, France 2013. Epidemiol. Infect. 2019, 147, e109. [Google Scholar] [CrossRef] [PubMed]
- Robert, A.; Suffel, A.M.; Kucharski, A.J. Long-term waning of vaccine-induced immunity to measles in England: A mathematical modelling study. Lancet Public Health 2024, 9, e766–e775. [Google Scholar] [CrossRef] [PubMed]
- Bitzegeio, J.; Majowicz, S.; Matysiak-Klose, D.; Sagebiel, D.; Werber, D. Estimating age-specific vaccine effectiveness using data from a large measles outbreak in Berlin, Germany, 2014/15: Evidence for waning immunity. Eurosurveillance 2019, 24, 1800529. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dayan, G.H.; Panero, M.S.; Urquiza, A.; Molina, M.; Prieto, S.; Del Carmen Perego, M.; Scagliotti, G.; Galimberti, D.; Carroli, G.; Wolff, C.; et al. Rubella and measles seroprevalence among women of childbearing age, Argentina, 2002. Epidemiol. Infect. 2005, 133, 861–869. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef]
- Coppeta, L.; Ferrari, C.; Somma, G.; Giovinazzo, V.; Buonomo, E.; Aurilio, M.T.; Treglia, M.; Magrini, A. Serological Evaluation for Measles among Italian and Foreign Medical Students in a University Hospital in Rome. Vaccines 2023, 11, 1256. [Google Scholar] [CrossRef]
- Nasika, A.; Bogogiannidou, Z.; Mouchtouri, V.A.; Dadouli, K.; Kyritsi, M.A.; Vontas, A.; Voulgaridi, I.; Tsinaris, Z.; Kola, K.; Matziri, A.; et al. Measles Immunity Status of Greek Population after the Outbreak in 2017–2018: Results from a Seroprevalence National Survey. Vaccines 2023, 11, 1220. [Google Scholar] [CrossRef]
- Marchi, S.; Remarque, E.J.; Viviani, S.; Rizzo, C.; Monteverde Spencer, G.T.; Coluccio, R.; Montomoli, E.; Trombetta, C.M. Measles immunity over two decades in two large Italian Regions: How far is the elimination goal? Vaccine 2021, 39, 5928–5933. [Google Scholar] [CrossRef] [PubMed]
- Grassi, T.; Bagordo, F.; Rota, M.C.; Dettori, M.; Baldovin, T.; Napolitano, F.; Panico, A.; Massaro, E.; Marchi, S.; Furfaro, G.; et al. Seroprevalence of measles antibodies in the Italian general population in 2019–2020. Vaccine 2024, 42, 126012. [Google Scholar] [CrossRef] [PubMed]
- Bugdaycı Yalcın, B.N.; Sasmaz, C.T. Measles Seroprevalence and Related Factors in Women Aged 15–49 Years Old, in Mersin, Turkey. Iran. J. Public Health 2023, 52, 593–602. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dimech, W.; Mulders, M.N. A 16-year review of seroprevalence studies on measles and rubella. Vaccine 2016, 34, 4110–4118. [Google Scholar] [CrossRef] [PubMed]
- Khalil, A.; Samara, A.; Campbell, C.; Ladhani, S.N. Pregnant women and measles: We need to be vigilant during outbreaks. eClinicalMedicine 2024, 72, 102594. [Google Scholar] [CrossRef] [PubMed]
- Latner, D.R.; Sowers, S.B.; Anthony, K.; Colley, H.; Badeau, C.; Coates, J.; Wong, P.; Fakile, Y.; Interiano, C.; Pannell, K.B.; et al. Qualitative Variation among Commercial Immunoassays for Detection of Measles-Specific IgG. J. Clin. Microbiol. 2020, 58, e265–e320. [Google Scholar] [CrossRef]
- Gieles, N.C.; Mutsaerts, E.A.M.L.; Kwatra, G.; Bont, L.; Cutland, C.L.; Jones, S.; Moultrie, A.; Madhi, S.A.; Nunes, M.C. Measles seroprevalence in pregnant women in Soweto, South Africa: A nested cohort study. Clin. Microbiol. Infect. 2020, 26, 515.e1–515.e4. [Google Scholar] [CrossRef] [PubMed]
- Janaszek, W.; Slusarczyk, J. Immunity against measles in populations of women and infants in Poland. Vaccine 2003, 21, 2948–2953. [Google Scholar] [CrossRef]
- Ben-Chetrit, E.; Oster, Y.; Jarjou’i, A.; Megged, O.; Lachish, T.; Cohen, M.J.; Stein-Zamir, C.; Ivgi, H.; Rivkin, M.; Milgrom, Y.; et al. Measles-related hospitalizations and associated complications in Jerusalem, 2018–2019. Clin. Microbiol. Infect. 2020, 26, 637–642. [Google Scholar] [CrossRef]
- Principi, N.; Esposito, S. Early vaccination: A provisional measure to prevent measles in infants. Lancet Infect. Dis. 2019, 19, 1157–1158. [Google Scholar] [CrossRef]
- Mathew, J.L.; Wagner, A.L.; Ratho, R.K.; Patel, P.N.; Suri, V.; Bharti, B.; Carlson, B.F.; Dutta, S.; Singh, M.P.; Boulton, M.L. Maternally transmitted anti-measles antibodies, and susceptibility to disease among infants in Chandigarh, India: A prospective birth cohort study. PLoS ONE 2023, 18, 0287110. [Google Scholar] [CrossRef] [PubMed]
- Moghadas, S.M.; Alexander, M.E.; Sahai, B.M. Waning herd immunity: A challenge for eradication of measles. J. Math. 2008, 38, 5. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Group | Females | Males | Seroprevalence of IgG Positives (%) | Females IgG Positives | Males IgG Positives | p |
|---|---|---|---|---|---|---|
| 25–29 years (N = 193) | 90 | 103 | 128 (66.3%) | 55 (61.1%) | 73 (70.9%) | 0.153 |
| 30–34 years (N = 241) | 112 | 129 | 176 (73%) | 88 (78.6%) | 88 (68.2%) | 0.708 |
| 35–40 years (N = 243) | 112 | 131 | 199 (81.9%) | 90 (80.4%) | 109 (83.2%) | 0.565 |
| 40–44 years (N = 282) | 132 | 150 | 235 (83.3%) | 112 (84.8%) | 123 (82%) | 0.521 |
| Total (N = 959) | 446 (46.5%) | 513 (54.5%) | 738 (77%) | 345 (77.4%) | 393 (76.6%) | 0.796 |
| Age Group | Total | ||||
|---|---|---|---|---|---|
| 25–29 y | 30–34 y | 35–39 y | 40–44 y | ||
| Nr of seropositives | 128a | 176a,b | 199b,c | 235c | 738 |
| Seroprevalence | 66.30% | 73.00% | 81.90% | 83.30% | 77.00% |
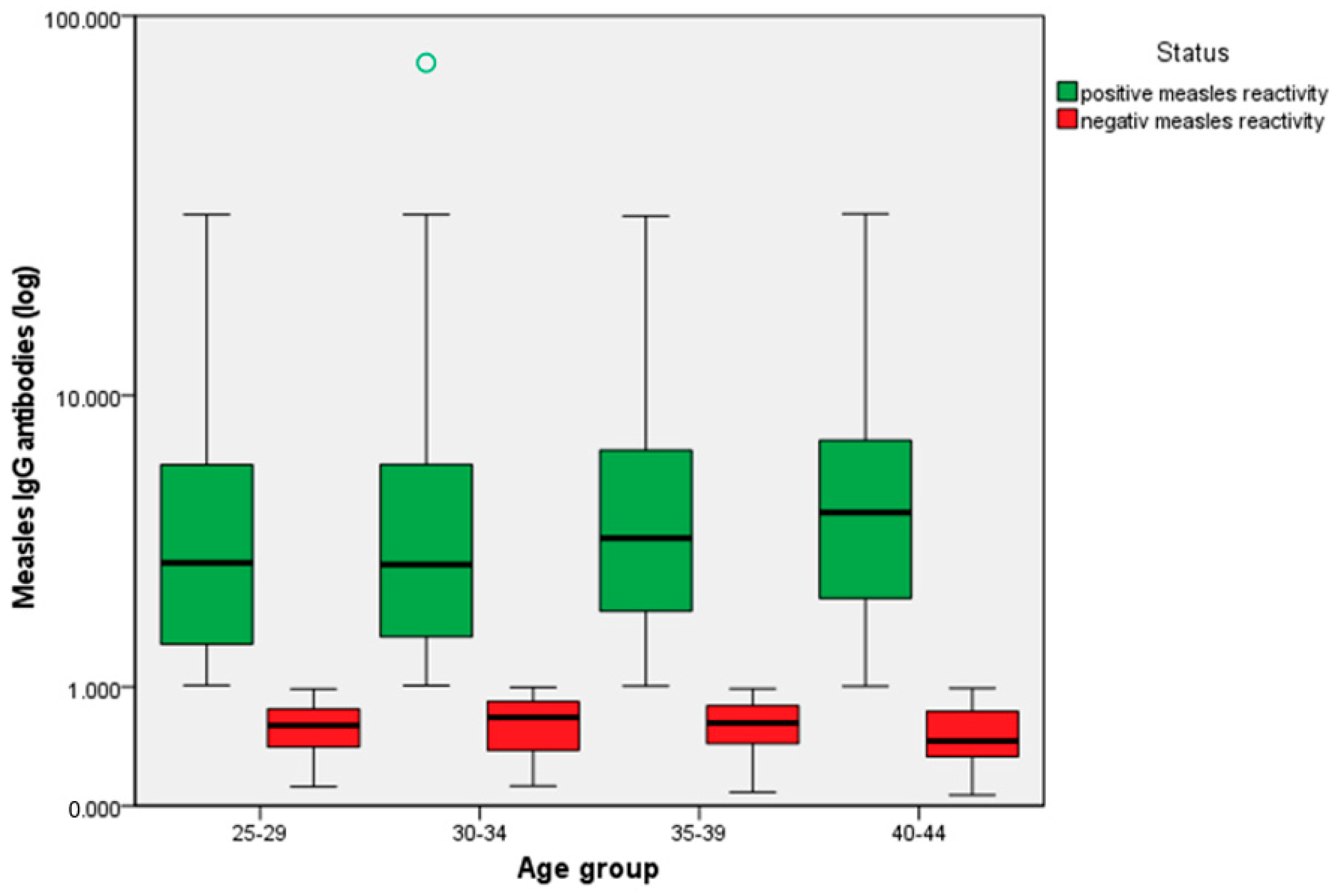
| Age Group Compared | Age Group to Be Compared with | Mean Measles Reactivity Differences Between Age Groups | p |
|---|---|---|---|
| 25–29 y | 30–34 y | −0.656 | 0.870 (−2.293; 0.979) |
| 35–39 y | −0.505 | 0.772 (−1.591; 0.580) | |
| 40–44 y | −1.127 | 0.057 (−2.275; 0.020) | |
| 30–34 y | 35–39 y | 0.151 | 1 (−1.386; 1.689) |
| 40–44 y | −0.470 | 0.966 (−2.052; 1.112) | |
| 35–39 y | 40–44 y | −0.621 | 0.471 (−1.621; 0.377) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stanescu, A.; Ruta, S.M.; Leustean, M.; Iosif, I.; Sultana, C.; Panaitescu, A.M.; Furtunescu, F.L.; Cernescu, C.; Pistol, A. A Nationwide Seroprevalence Study for Measles in Individuals of Fertile Age in Romania. Antibodies 2025, 14, 32. https://doi.org/10.3390/antib14020032
Stanescu A, Ruta SM, Leustean M, Iosif I, Sultana C, Panaitescu AM, Furtunescu FL, Cernescu C, Pistol A. A Nationwide Seroprevalence Study for Measles in Individuals of Fertile Age in Romania. Antibodies. 2025; 14(2):32. https://doi.org/10.3390/antib14020032
Chicago/Turabian StyleStanescu, Aurora, Simona Maria Ruta, Mihaela Leustean, Ionel Iosif, Camelia Sultana, Anca Maria Panaitescu, Florentina Ligia Furtunescu, Costin Cernescu, and Adriana Pistol. 2025. "A Nationwide Seroprevalence Study for Measles in Individuals of Fertile Age in Romania" Antibodies 14, no. 2: 32. https://doi.org/10.3390/antib14020032
APA StyleStanescu, A., Ruta, S. M., Leustean, M., Iosif, I., Sultana, C., Panaitescu, A. M., Furtunescu, F. L., Cernescu, C., & Pistol, A. (2025). A Nationwide Seroprevalence Study for Measles in Individuals of Fertile Age in Romania. Antibodies, 14(2), 32. https://doi.org/10.3390/antib14020032