
When Autoantibodies Are Missing: The Challenge of Seronegative Rheumatoid Arthritis


Abstract
:1. Introduction
2. Epidemiology
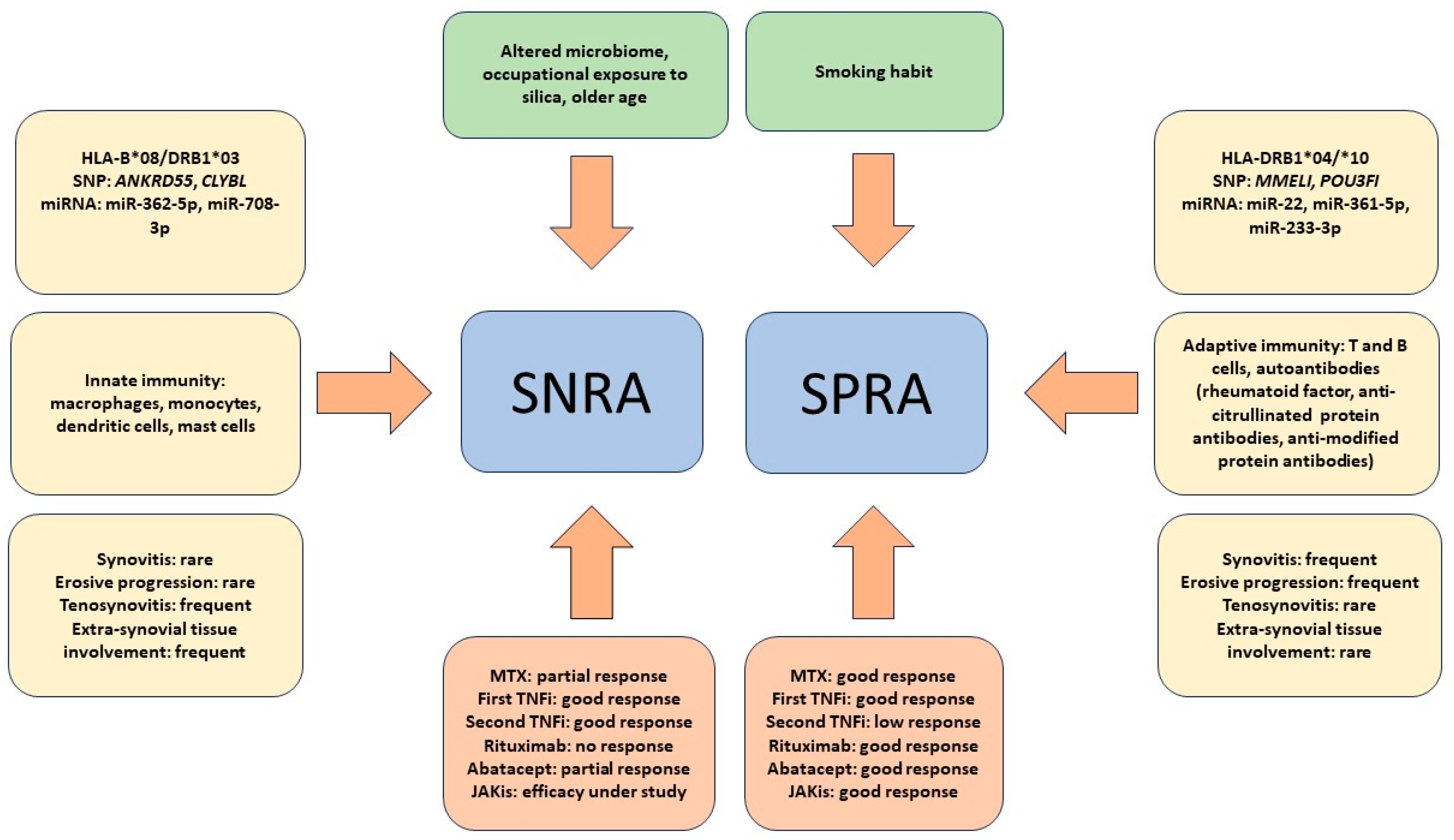
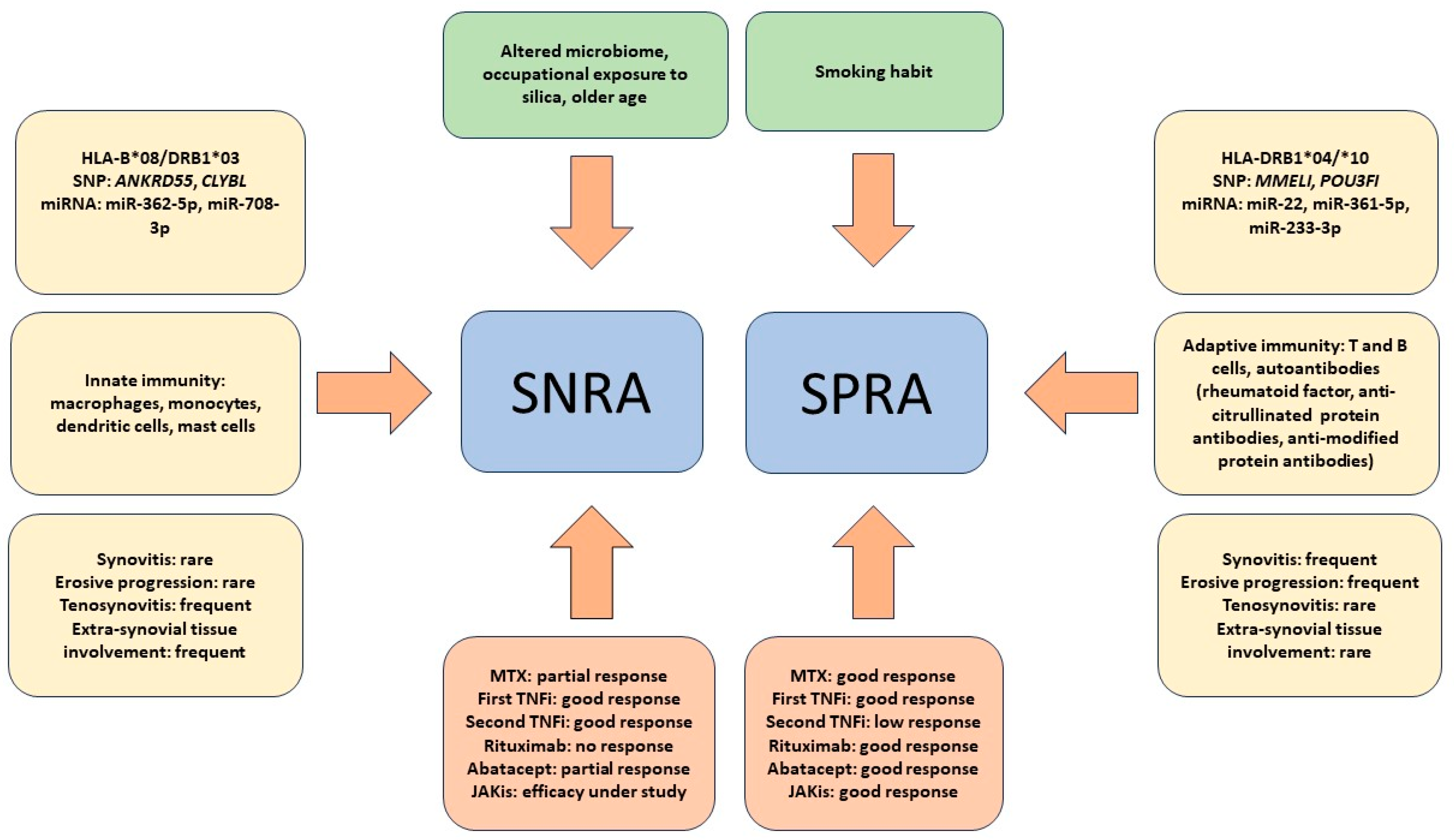
3. Pathogenesis
4. Diagnosis
5. Severity of the Disease
6. The Response to Therapy of SNRA Is Different from That of SPRA
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Smolen, J.S.; Aletaha, D.; McInnes, I.B. Rheumatoid arthritis. Lancet 2016, 388, 2023–2038. [Google Scholar] [CrossRef] [PubMed]
- Figus, F.A.; Piga, M.; Azzolin, I.; McConnell, R.; Iagnocco, A. Rheumatoid arthritis: Extra-articular manifestations and comorbidities. Autoimmun. Rev. 2021, 20, 102776. [Google Scholar] [CrossRef] [PubMed]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Kay, J.; Upchurch, K.S. ACR/EULAR 2010 rheumatoid arthritis classification criteria. Rheumatology (Oxford) 2012, 51 (Suppl. S6), vi5–vi9. [Google Scholar] [CrossRef]
- Pratt, A.G.; Isaacs, J.D. Seronegative rheumatoid arthritis: Pathogenetic and therapeutic aspects. Best Pract Res. Clin. Rheumatol. 2014, 28, 651–659. [Google Scholar] [CrossRef]
- Lenti, M.V.; Rossi, C.M.; Melazzini, F.; Gastaldi, M.; Bugatti, S.; Rotondi, M.; Bianchi, P.I.; Gentile, A.; Chiovato, L.; Montecucco, C.; et al. Seronegative autoimmune diseases: A challenging diagnosis. Autoimmun. Rev. 2022, 21, 103143. [Google Scholar] [CrossRef]
- Sokolova, M.V.; Schett, G.; Steffen, U. Autoantibodies in Rheumatoid Arthritis: Historical Background and Novel Findings. Clin. Rev. Allergy Immunol. 2022, 63, 138–151. [Google Scholar] [CrossRef]
- Kolarz, B.; Podgorska, D.; Podgorski, R. Insights of rheumatoid arthritis biomarkers. Biomarkers 2021, 26, 185–195. [Google Scholar] [CrossRef]
- Derksen, V.; Huizinga, T.W.J.; van der Woude, D. The role of autoantibodies in the pathophysiology of rheumatoid arthritis. Semin. Immunopathol. 2017, 39, 437–446. [Google Scholar] [CrossRef]
- Curtis, J.R.; Jain, A.; Askling, J.; Bridges, S.L., Jr.; Carmona, L.; Dixon, W.; Finckh, A.; Hyrich, K.; Greenberg, J.D.; Kremer, J.; et al. A comparison of patient characteristics and outcomes in selected European and U.S. rheumatoid arthritis registries. Semin. Arthritis Rheum. 2010, 40, 2–14 e11. [Google Scholar] [CrossRef]
- Courvoisier, D.S.; Chatzidionysiou, K.; Mongin, D.; Lauper, K.; Mariette, X.; Morel, J.; Gottenberg, J.E.; Bergstra, S.A.; Suarez, M.P.; Codreanu, C.; et al. The impact of seropositivity on the effectiveness of biologic anti-rheumatic agents: Results from a collaboration of 16 registries. Rheumatology 2021, 60, 820–828. [Google Scholar] [CrossRef] [PubMed]
- Myasoedova, E.; Davis, J.; Matteson, E.L.; Crowson, C.S. Is the epidemiology of rheumatoid arthritis changing? Results from a population-based incidence study, 1985-2014. Ann. Rheum. Dis. 2020, 79, 440–444. [Google Scholar] [CrossRef] [PubMed]
- Matthijssen, X.M.E.; Huizinga, T.W.J.; van der Helm-van Mil, A.H.M. Increasing incidence of autoantibody-negative RA is replicated and is partly explained by an aging population. Ann. Rheum. Dis. 2022, 81, e69. [Google Scholar] [CrossRef]
- Matthijssen, X.M.E.; Niemantsverdriet, E.; Huizinga, T.W.J.; van der Helm-van Mil, A.H.M. Enhanced treatment strategies and distinct disease outcomes among autoantibody-positive and -negative rheumatoid arthritis patients over 25 years: A longitudinal cohort study in the Netherlands. PLoS Med. 2020, 17, e1003296. [Google Scholar] [CrossRef] [PubMed]
- Takanashi, S.; Takeuchi, T.; Kaneko, Y. Effects of Aging on Rheumatoid Factor and Anticyclic Citrullinated Peptide Antibody Positivity in Patients With Rheumatoid Arthritis. J. Rheumatol. 2023, 50, 330–334. [Google Scholar] [CrossRef]
- Turkcapar, N.; Demir, O.; Atli, T.; Kopuk, M.; Turgay, M.; Kinikli, G.; Duman, M. Late onset rheumatoid arthritis: Clinical and laboratory comparisons with younger onset patients. Arch. Gerontol. Geriatr. 2006, 42, 225–231. [Google Scholar] [CrossRef]
- van Delft, M.A.M.; Huizinga, T.W.J. An overview of autoantibodies in rheumatoid arthritis. J. Autoimmun. 2020, 110, 102392. [Google Scholar] [CrossRef]
- Regueiro, C.; Rodriguez-Rodriguez, L.; Lopez-Mejias, R.; Nuno, L.; Triguero-Martinez, A.; Perez-Pampin, E.; Corrales, A.; Villalba, A.; Lopez-Golan, Y.; Abasolo, L.; et al. A predominant involvement of the triple seropositive patients and others with rheumatoid factor in the association of smoking with rheumatoid arthritis. Sci. Rep. 2020, 10, 3355. [Google Scholar] [CrossRef]
- Bergot, A.S.; Giri, R.; Thomas, R. The microbiome and rheumatoid arthritis. Best Pract. Res. Clin. Rheumatol. 2019, 33, 101497. [Google Scholar] [CrossRef]
- Morotti, A.; Sollaku, I.; Franceschini, F.; Cavazzana, I.; Fredi, M.; Sala, E.; De Palma, G. Systematic Review and Meta-analysis on the Association of Occupational Exposure to Free Crystalline Silica and Rheumatoid Arthritis. Clin. Allergy Immunol. 2022, 62, 333–345. [Google Scholar] [CrossRef]
- De Stefano, L.; D’Onofrio, B.; Manzo, A.; Montecucco, C.; Bugatti, S. The Genetic, Environmental, and Immunopathological Complexity of Autoantibody-Negative Rheumatoid Arthritis. Int. J. Mol. Sci. 2021, 22, 12386. [Google Scholar] [CrossRef] [PubMed]
- Padyukov, L. Genetics of rheumatoid arthritis. Semin. Immunopathol. 2022, 44, 47–62. [Google Scholar] [CrossRef]
- Saevarsdottir, S.; Stefansdottir, L.; Sulem, P.; Thorleifsson, G.; Ferkingstad, E.; Rutsdottir, G.; Glintborg, B.; Westerlind, H.; Grondal, G.; Loft, I.C.; et al. Multiomics analysis of rheumatoid arthritis yields sequence variants that have large effects on risk of the seropositive subset. Ann. Rheum. Dis. 2022, 81, 1085–1095. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.; Li, X.; Lin, A.; Larsson, S.C. Interleukins and rheumatoid arthritis: Bi-directional Mendelian randomization investigation. Semin. Arthritis Rheum. 2022, 53, 151958. [Google Scholar] [CrossRef] [PubMed]
- Eyre, S.; Bowes, J.; Diogo, D.; Lee, A.; Barton, A.; Martin, P.; Zhernakova, A.; Stahl, E.; Viatte, S.; McAllister, K.; et al. High-density genetic mapping identifies new susceptibility loci for rheumatoid arthritis. Nat. Genet. 2012, 44, 1336–1340. [Google Scholar] [CrossRef] [PubMed]
- Bossini-Castillo, L.; de Kovel, C.; Kallberg, H.; van’t Slot, R.; Italiaander, A.; Coenen, M.; Tak, P.P.; Posthumus, M.D.; Wijmenga, C.; Huizinga, T.; et al. A genome-wide association study of rheumatoid arthritis without antibodies against citrullinated peptides. Ann. Rheum. Dis. 2015, 74, e15. [Google Scholar] [CrossRef]
- He, X.H.; Xiao, Y.T.; Chen, W.Y.; Wang, M.J.; Wu, X.D.; Mei, L.Y.; Gao, K.X.; Huang, Q.C.; Huang, R.Y.; Chen, X.M. In silico analysis of serum miRNA profiles in seronegative and seropositive rheumatoid arthritis patients by small RNA sequencing. PeerJ 2023, 11, e15690. [Google Scholar] [CrossRef]
- Alivernini, S.; Tolusso, B.; Petricca, L.; Bui, L.; Di Mario, C.; Gigante, M.R.; Di Sante, G.; Benvenuto, R.; Fedele, A.L.; Federico, F.; et al. Synovial Predictors of Differentiation to Definite Arthritis in Patients With Seronegative Undifferentiated Peripheral Inflammatory Arthritis: microRNA Signature, Histological, and Ultrasound Features. Front. Med. 2018, 5, 186. [Google Scholar] [CrossRef]
- Ding, B.; Padyukov, L.; Lundstrom, E.; Seielstad, M.; Plenge, R.M.; Oksenberg, J.R.; Gregersen, P.K.; Alfredsson, L.; Klareskog, L. Different patterns of associations with anti-citrullinated protein antibody-positive and anti-citrullinated protein antibody-negative rheumatoid arthritis in the extended major histocompatibility complex region. Arthritis Rheum. 2009, 60, 30–38. [Google Scholar] [CrossRef]
- Chang, C.; Xu, L.; Zhang, R.; Jin, Y.; Jiang, P.; Wei, K.; Xu, L.; Shi, Y.; Zhao, J.; Xiong, M.; et al. MicroRNA-Mediated Epigenetic Regulation of Rheumatoid Arthritis Susceptibility and Pathogenesis. Front. Immunol. 2022, 13, 838884. [Google Scholar] [CrossRef]
- Alivernini, S.; Bruno, D.; Tolusso, B.; Bui, L.; Petricca, L.; Gigante, M.R.; Birra, D.; Fedele, A.L.; Peluso, G.; Federico, F.; et al. Differential synovial tissue biomarkers among psoriatic arthritis and rheumatoid factor/anti-citrulline antibody-negative rheumatoid arthritis. Arthritis Res. Ther. 2019, 21, 116. [Google Scholar] [CrossRef]
- Argyriou, A.; Wadsworth, M.H., 2nd; Lendvai, A.; Christensen, S.M.; Hensvold, A.H.; Gerstner, C.; van Vollenhoven, A.; Kravarik, K.; Winkler, A.; Malmstrom, V.; et al. Single cell sequencing identifies clonally expanded synovial CD4(+) T(PH) cells expressing GPR56 in rheumatoid arthritis. Nat. Commun. 2022, 13, 4046. [Google Scholar] [CrossRef] [PubMed]
- Angelopoulou, F.; Bogdanos, D.; Dimitroulas, T.; Sakkas, L.; Daoussis, D. Immune checkpoint inhibitor-induced musculoskeletal manifestations. Rheumatol. Int. 2021, 41, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Bridgewood, C.; Wittmann, M.; Macleod, T.; Watad, A.; Newton, D.; Bhan, K.; Amital, H.; Damiani, G.; Giryes, S.; Bragazzi, N.L.; et al. T Helper 2 IL-4/IL-13 Dual Blockade with Dupilumab Is Linked to Some Emergent T Helper 17—Type Diseases, Including Seronegative Arthritis and Enthesitis/Enthesopathy, but Not to Humoral Autoimmune Diseases. J. Investig. Dermatol. 2022, 142, 2660–2667. [Google Scholar] [CrossRef] [PubMed]
- Yarwood, A.; Huizinga, T.W.; Worthington, J. The genetics of rheumatoid arthritis: Risk and protection in different stages of the evolution of RA. Rheumatology 2016, 55, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Bardin, T.; Legrand, L.; Naveau, B.; Marcelli-Barge, A.; Debeyre, N.; Lathrop, G.M.; Poirier, J.C.; Schmid, M.; Ryckewaert, A.; Dryll, A. HLA antigens and seronegative rheumatoid arthritis. Ann. Rheum. Dis. 1985, 44, 50–53. [Google Scholar] [CrossRef] [PubMed]
- Kaarela, K.; Kautiainen, H. Continuous progression of radiological destruction in seropositive rheumatoid arthritis. J. Rheumatol. 1997, 24, 1285–1287. [Google Scholar]
- Choi, S.; Lee, K.H. Clinical management of seronegative and seropositive rheumatoid arthritis: A comparative study. PLoS ONE 2018, 13, e0195550. [Google Scholar] [CrossRef]
- Martin-Sanchez, F.; Diamond, C.; Zeitler, M.; Gomez, A.I.; Baroja-Mazo, A.; Bagnall, J.; Spiller, D.; White, M.; Daniels, M.J.; Mortellaro, A.; et al. Inflammasome-dependent IL-1beta release depends upon membrane permeabilisation. Cell Death Differ. 2016, 23, 1219–1231. [Google Scholar] [CrossRef]
- Bird, P.; Littlejohn, G.; Butcher, B.; Smith, T.; O’Sullivan, C.; Witcombe, D.; Griffiths, H. Real-world evaluation of effectiveness, persistence, and usage patterns of monotherapy and combination therapy tofacitinib in treatment of rheumatoid arthritis in Australia. Clin. Rheumatol. 2022, 41, 53–62. [Google Scholar] [CrossRef]
- Sugawara, M.; Fujieda, Y.; Noguchi, A.; Tanimura, S.; Shimizu, Y.; Nakagawa, I.; Yoshimura, M.; Abe, N.; Kono, M.; Kato, M.; et al. Prediction of the intolerance or non-responder to Janus kinase inhibitors in patients with rheumatoid arthritis: A preliminary retrospective study with integrative cluster analysis. Clin. Exp. Rheumatol. 2022, 40, 1674–1680. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.Y.; Lee, E.; Kim, J.W.; Suh, C.H.; Kim, H.A. Efficacy and drug retention of tofacitinib in rheumatoid arthritis: From the nationwide Korean College of Rheumatology Biologics registry. Clin. Exp. Rheumatol. 2023, 41, 1034–1041. [Google Scholar] [CrossRef] [PubMed]
- Dalbeth, N.; Gosling, A.L.; Gaffo, A.; Abhishek, A. Gout. Lancet 2021, 397, 1843–1855. [Google Scholar] [CrossRef] [PubMed]
- Mauro, D.; Thomas, R.; Guggino, G.; Lories, R.; Brown, M.A.; Ciccia, F. Ankylosing spondylitis: An autoimmune or autoinflammatory disease? Nat. Rev. Rheumatol. 2021, 17, 387–404. [Google Scholar] [CrossRef] [PubMed]
- Nordberg, L.B.; Lillegraven, S.; Lie, E.; Aga, A.B.; Olsen, I.C.; Hammer, H.B.; Uhlig, T.; Jonsson, M.K.; van der Heijde, D.; Kvien, T.K.; et al. Patients with seronegative RA have more inflammatory activity compared with patients with seropositive RA in an inception cohort of DMARD-naive patients classified according to the 2010 ACR/EULAR criteria. Ann. Rheum. Dis. 2017, 76, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Boeters, D.M.; Gaujoux-Viala, C.; Constantin, A.; van der Helm-van Mil, A.H.M. The 2010 ACR/EULAR criteria are not sufficiently accurate in the early identification of autoantibody-negative rheumatoid arthritis: Results from the Leiden-EAC and ESPOIR cohorts. Semin. Arthritis Rheum. 2017, 47, 170–174. [Google Scholar] [CrossRef]
- Trouw, L.A.; Mahler, M. Closing the serological gap: Promising novel biomarkers for the early diagnosis of rheumatoid arthritis. Autoimmun. Rev. 2012, 12, 318–322. [Google Scholar] [CrossRef]
- Kwon, E.J.; Ju, J.H. Impact of Posttranslational Modification in Pathogenesis of Rheumatoid Arthritis: Focusing on Citrullination, Carbamylation, and Acetylation. Int. J. Mol. Sci. 2021, 22, 10576. [Google Scholar] [CrossRef]
- Arnett, F.C.; Edworthy, S.M.; Bloch, D.A.; McShane, D.J.; Fries, J.F.; Cooper, N.S.; Healey, L.A.; Kaplan, S.R.; Liang, M.H.; Luthra, H.S.; et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988, 31, 315–324. [Google Scholar] [CrossRef]
- Burgers, L.E.; Raza, K.; van der Helm-van Mil, A.H. Window of opportunity in rheumatoid arthritis—Definitions and supporting evidence: From old to new perspectives. RMD Open 2019, 5, e000870. [Google Scholar] [CrossRef]
- Coffey, C.M.; Crowson, C.S.; Myasoedova, E.; Matteson, E.L.; Davis, J.M., 3rd. Evidence of Diagnostic and Treatment Delay in Seronegative Rheumatoid Arthritis: Missing the Window of Opportunity. Mayo Clin. Proc. 2019, 94, 2241–2248. [Google Scholar] [CrossRef] [PubMed]
- Muilu, P.; Rantalaiho, V.; Kautiainen, H.; Virta, L.J.; Eriksson, J.G.; Puolakka, K. Increasing incidence and shifting profile of idiopathic inflammatory rheumatic diseases in adults during this millennium. Clin. Rheumatol. 2019, 38, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Neogi, T.; Aletaha, D.; Silman, A.J.; Naden, R.L.; Felson, D.T.; Aggarwal, R.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; et al. The 2010 American College of Rheumatology/European League Against Rheumatism classification criteria for rheumatoid arthritis: Phase 2 methodological report. Arthritis Rheum. 2010, 62, 2582–2591. [Google Scholar] [CrossRef] [PubMed]
- Burns, T.M.; Calin, A. The hand radiograph as a diagnostic discriminant between seropositive and seronegative ‘rheumatoid arthritis’: A controlled study. Ann. Rheum. Dis. 1983, 42, 605–612. [Google Scholar] [CrossRef] [PubMed]
- el-Khoury, G.Y.; Larson, R.K.; Kathol, M.H.; Berbaum, K.S.; Furst, D.E. Seronegative and seropositive rheumatoid arthritis: Radiographic differences. Radiology 1988, 168, 517–520. [Google Scholar] [CrossRef]
- Panayi, G.S.; Celinska, E.; Emery, P.; Griffin, J.; Welsh, K.I.; Grahame, R.; Gibson, T. Seronegative and seropositive rheumatoid arthritis: Similar diseases. Br. J. Rheumatol. 1987, 26, 172–180. [Google Scholar] [CrossRef]
- Carbonell-Bobadilla, N.; Soto-Fajardo, C.; Amezcua-Guerra, L.M.; Batres-Marroquin, A.B.; Vargas, T.; Hernandez-Diazcouder, A.; Jimenez-Rojas, V.; Medina-Garcia, A.C.; Pineda, C.; Silveira, L.H. Patients with seronegative rheumatoid arthritis have a different phenotype than seropositive patients: A clinical and ultrasound study. Front. Med. 2022, 9, 978351. [Google Scholar] [CrossRef]
- Gadeholt, O.; Hausotter, K.; Eberle, H.; Klink, T.; Pfeil, A. Differing X-ray patterns in seronegative and seropositive rheumatoid arthritis. Clin. Rheumatol. 2019, 38, 2403–2410. [Google Scholar] [CrossRef]
- Lin, D.; Zhao, M.; Zhang, Y.; Xie, Y.; Cao, J.; Pan, Y. Seronegative rheumatic arthritis has milder inflammation and bone erosion in an ultrasound study of disease-modifying anti-rheumatic drugs (DMARDs)-naive Chinese cohort. Ann. Transl. Med. 2022, 10, 661. [Google Scholar] [CrossRef]
- Naredo, E.; Bonilla, G.; Gamero, F.; Uson, J.; Carmona, L.; Laffon, A. Assessment of inflammatory activity in rheumatoid arthritis: A comparative study of clinical evaluation with grey scale and power Doppler ultrasonography. Ann. Rheum. Dis. 2005, 64, 375–381. [Google Scholar] [CrossRef]
- Brown, A.K.; Conaghan, P.G.; Karim, Z.; Quinn, M.A.; Ikeda, K.; Peterfy, C.G.; Hensor, E.; Wakefield, R.J.; O’Connor, P.J.; Emery, P. An explanation for the apparent dissociation between clinical remission and continued structural deterioration in rheumatoid arthritis. Arthritis Rheum. 2008, 58, 2958–2967. [Google Scholar] [CrossRef] [PubMed]
- Colebatch, A.N.; Edwards, C.J.; Ostergaard, M.; van der Heijde, D.; Balint, P.V.; D’Agostino, M.A.; Forslind, K.; Grassi, W.; Haavardsholm, E.A.; Haugeberg, G.; et al. EULAR recommendations for the use of imaging of the joints in the clinical management of rheumatoid arthritis. Ann. Rheum. Dis. 2013, 72, 804–814. [Google Scholar] [CrossRef] [PubMed]
- van de Stadt, L.A.; Bos, W.H.; Meursinge Reynders, M.; Wieringa, H.; Turkstra, F.; van der Laken, C.J.; van Schaardenburg, D. The value of ultrasonography in predicting arthritis in auto-antibody positive arthralgia patients: A prospective cohort study. Arthritis Res. Ther. 2010, 12, R98. [Google Scholar] [CrossRef] [PubMed]
- Minowa, K.; Ogasawara, M.; Murayama, G.; Gorai, M.; Yamada, Y.; Nemoto, T.; Matsuki, Y.; Sugisaki, N.; Ando, S.; Kon, T.; et al. Predictive grade of ultrasound synovitis for diagnosing rheumatoid arthritis in clinical practice and the possible difference between patients with and without seropositivity. Mod. Rheumatol. 2016, 26, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Freeston, J.E.; Wakefield, R.J.; Conaghan, P.G.; Hensor, E.M.; Stewart, S.P.; Emery, P. A diagnostic algorithm for persistence of very early inflammatory arthritis: The utility of power Doppler ultrasound when added to conventional assessment tools. Ann. Rheum. Dis. 2010, 69, 417–419. [Google Scholar] [CrossRef]
- Lage-Hansen, P.R.; Lindegaard, H.; Chrysidis, S.; Terslev, L. The role of ultrasound in diagnosing rheumatoid arthritis, what do we know? An updated review. Rheumatol. Int. 2017, 37, 179–187. [Google Scholar] [CrossRef]
- Wang, J.; Wu, Z.; Wang, M.; Qi, Q.; Song, Q.; Sun, B.; Li, C.; Dong, Y. Evaluation of tenosynovitis in patients with seronegative rheumatoid arthritis using microvascular flow imaging. Med. Eng. Phys. 2022, 110, 103839. [Google Scholar] [CrossRef]
- den Hollander, N.K.; Verstappen, M.; Sidhu, N.; van Mulligen, E.; Reijnierse, M.; van der Helm-van Mil, A.H.M. Hand and foot MRI in contemporary undifferentiated arthritis: In which patients is MRI valuable to detect rheumatoid arthritis early? A large prospective study. Rheumatology 2022, 61, 3963–3973. [Google Scholar] [CrossRef]
- Sahbudin, I.; Singh, R.; De Pablo, P.; Rankin, E.; Rhodes, B.; Justice, E.; Derrett-Smith, E.; Amft, N.; Narayan, N.; McGrath, C.; et al. The value of ultrasound-defined tenosynovitis and synovitis in the prediction of persistent arthritis. Rheumatology 2023, 62, 1057–1068. [Google Scholar] [CrossRef]
- Mandl, P.; Navarro-Compan, V.; Terslev, L.; Aegerter, P.; van der Heijde, D.; D’Agostino, M.A.; Baraliakos, X.; Pedersen, S.J.; Jurik, A.G.; Naredo, E.; et al. EULAR recommendations for the use of imaging in the diagnosis and management of spondyloarthritis in clinical practice. Ann. Rheum. Dis. 2015, 74, 1327–1339. [Google Scholar] [CrossRef]
- Gadeholt, O. Rheumatoid arthritis is not a single disease. Clin. Exp. Rheumatol. 2017, 35 (Suppl. S104), 20–21. [Google Scholar] [PubMed]
- Mease, P.J.; Bhutani, M.K.; Hass, S.; Yi, E.; Hur, P.; Kim, N. Comparison of Clinical Manifestations in Rheumatoid Arthritis vs. Spondyloarthritis: A Systematic Literature Review. Rheumatol. Ther. 2022, 9, 331–378. [Google Scholar] [CrossRef] [PubMed]
- Felbo, S.K.; Terslev, L.; Ostergaard, M. Imaging in peripheral and axial psoriatic arthritis: Contributions to diagnosis, follow-up, prognosis and knowledge of pathogenesis. Clin. Exp. Rheumatol. 2018, 36 (Suppl. S114), 24–34. [Google Scholar]
- Taniguchi, Y.; Kumon, Y.; Takata, T.; Sano, S.; Ohnishi, T.; Nogami, M.; Ogawa, Y.; Terada, Y. Imaging assessment of enthesitis in spondyloarthritis. Ann. Nucl. Med. 2013, 27, 105–111. [Google Scholar] [CrossRef]
- Fournie, B.; Margarit-Coll, N.; Champetier de Ribes, T.L.; Zabraniecki, L.; Jouan, A.; Vincent, V.; Chiavassa, H.; Sans, N.; Railhac, J.J. Extrasynovial ultrasound abnormalities in the psoriatic finger. Prospective comparative power-doppler study versus rheumatoid arthritis. Joint. Bone Spine 2006, 73, 527–531. [Google Scholar] [CrossRef]
- Sieper, J.; Poddubnyy, D. Axial spondyloarthritis. Lancet 2017, 390, 73–84. [Google Scholar] [CrossRef]
- Paalanen, K.; Rannio, K.; Rannio, T.; Asikainen, J.; Hannonen, P.; Sokka, T. Does early seronegative arthritis develop into rheumatoid arthritis? A 10-year observational study. Clin. Exp. Rheumatol. 2019, 37, 37–43. [Google Scholar]
- Paalanen, K.; Puolakka, K.; Nikiphorou, E.; Hannonen, P.; Sokka, T. Is seronegative rheumatoid arthritis true rheumatoid arthritis? A nationwide cohort study. Rheumatology 2021, 60, 2391–2395. [Google Scholar] [CrossRef]
- Jantti, J.K.; Kaarela, K.; Lehtinen, K.E. Seronegative oligoarthritis: A 23-year follow-up study. Clin. Rheumatol. 2002, 21, 353–356. [Google Scholar] [CrossRef]
- Tidblad, L.; Westerlind, H.; Delcoigne, B.; Askling, J.; Saevarsdottir, S. Comorbidities at diagnosis of rheumatoid arthritis: A population-based case-control study. Rheumatology 2021, 60, 3760–3769. [Google Scholar] [CrossRef]
- van Boheemen, L.; van Beers-Tas, M.H.; Kroese, J.M.; van de Stadt, L.A.; van Schaardenburg, D.; Nurmohamed, M.T. Cardiovascular risk in persons at risk of developing rheumatoid arthritis. PLoS ONE 2020, 15, e0237072. [Google Scholar] [CrossRef]
- Doss, J.; Mo, H.; Carroll, R.J.; Crofford, L.J.; Denny, J.C. Phenome-Wide Association Study of Rheumatoid Arthritis Subgroups Identifies Association Between Seronegative Disease and Fibromyalgia. Arthritis Rheumatol. 2017, 69, 291–300. [Google Scholar] [CrossRef]
- Wolfe, F.; Walitt, B. No Association of Fibromyalgia and Seronegative Rheumatoid Arthritis-The Need for Uniform Application of Fibromyalgia Criteria in Research Studies: Comment on the Article by Doss et al. Arthritis Rheumatol. 2017, 69, 679–680. [Google Scholar] [CrossRef] [PubMed]
- van der Helm-van Mil, A.H.; Verpoort, K.N.; Breedveld, F.C.; Toes, R.E.; Huizinga, T.W. Antibodies to citrullinated proteins and differences in clinical progression of rheumatoid arthritis. Arthritis Res. Ther. 2005, 7, R949–R958. [Google Scholar] [CrossRef] [PubMed]
- Asikainen, J.; Nikiphorou, E.; Kaarela, K.; Lindqvist, E.; Hakkinen, A.; Kautiainen, H.; Hannonen, P.; Rannio, T.; Sokka, T. Is long-term radiographic joint damage different between men and women? Prospective longitudinal data analysis of four early RA cohorts with greater than 15 years follow-up. Clin. Exp. Rheumatol. 2016, 34, 641–645. [Google Scholar] [PubMed]
- Goekoop-Ruiterman, Y.P.; de Vries-Bouwstra, J.K.; Allaart, C.F.; van Zeben, D.; Kerstens, P.J.; Hazes, J.M.; Zwinderman, A.H.; Ronday, H.K.; Han, K.H.; Westedt, M.L.; et al. Clinical and radiographic outcomes of four different treatment strategies in patients with early rheumatoid arthritis (the BeSt study): A randomized, controlled trial. Arthritis Rheum. 2005, 52, 3381–3390. [Google Scholar] [CrossRef] [PubMed]
- Klareskog, L.; Alfredsson, L.; Rantapaa-Dahlqvist, S.; Berglin, E.; Stolt, P.; Padyukov, L. What precedes development of rheumatoid arthritis? Ann. Rheum. Dis. 2004, 63 (Suppl. S2), ii28–ii31. [Google Scholar] [CrossRef]
- Huizinga, T.W.; Amos, C.I.; van der Helm-van Mil, A.H.; Chen, W.; van Gaalen, F.A.; Jawaheer, D.; Schreuder, G.M.; Wener, M.; Breedveld, F.C.; Ahmad, N.; et al. Refining the complex rheumatoid arthritis phenotype based on specificity of the HLA-DRB1 shared epitope for antibodies to citrullinated proteins. Arthritis Rheum. 2005, 52, 3433–3438. [Google Scholar] [CrossRef]
- Lundstrom, E.; Kallberg, H.; Alfredsson, L.; Klareskog, L.; Padyukov, L. Gene-environment interaction between the DRB1 shared epitope and smoking in the risk of anti-citrullinated protein antibody-positive rheumatoid arthritis: All alleles are important. Arthritis Rheum. 2009, 60, 1597–1603. [Google Scholar] [CrossRef]
- Bugatti, S.; Manzo, A.; Montecucco, C.; Caporali, R. The Clinical Value of Autoantibodies in Rheumatoid Arthritis. Front. Med. 2018, 5, 339. [Google Scholar] [CrossRef]
- Willemze, A.; Trouw, L.A.; Toes, R.E.; Huizinga, T.W. The influence of ACPA status and characteristics on the course of RA. Nat. Rev. Rheumatol. 2012, 8, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Barra, L.; Pope, J.E.; Orav, J.E.; Boire, G.; Haraoui, B.; Hitchon, C.; Keystone, E.C.; Thorne, J.C.; Tin, D.; Bykerk, V.P.; et al. Prognosis of seronegative patients in a large prospective cohort of patients with early inflammatory arthritis. J. Rheumatol. 2014, 41, 2361–2369. [Google Scholar] [CrossRef] [PubMed]
- Smolen, J.S.; Landewe, R.B.M.; Bijlsma, J.W.J.; Burmester, G.R.; Dougados, M.; Kerschbaumer, A.; McInnes, I.B.; Sepriano, A.; van Vollenhoven, R.F.; de Wit, M.; et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann. Rheum. Dis. 2020, 79, 685–699. [Google Scholar] [CrossRef] [PubMed]
- Wevers-de Boer, K.; Visser, K.; Heimans, L.; Ronday, H.K.; Molenaar, E.; Groenendael, J.H.; Peeters, A.J.; Westedt, M.L.; Collee, G.; de Sonnaville, P.B.; et al. Remission induction therapy with methotrexate and prednisone in patients with early rheumatoid and undifferentiated arthritis (the IMPROVED study). Ann. Rheum. Dis. 2012, 71, 1472–1477. [Google Scholar] [CrossRef]
- Nordberg, L.B.; Lillegraven, S.; Aga, A.B.; Sexton, J.; Olsen, I.C.; Lie, E.; Berner Hammer, H.; Uhlig, T.; van der Heijde, D.; Kvien, T.K.; et al. Comparing the disease course of patients with seronegative and seropositive rheumatoid arthritis fulfilling the 2010 ACR/EULAR classification criteria in a treat-to-target setting: 2-year data from the ARCTIC trial. RMD Open 2018, 4, e000752. [Google Scholar] [CrossRef]
- Greenwood, M.; Shipa, M.; Yeoh, S.A.; Roussou, E.; Mukerjee, D.; Ehrenstein, M.R. Methotrexate reduces withdrawal rates of TNF inhibitors due to ineffectiveness in rheumatoid arthritis but only in patients who are seropositive. Ann. Rheum. Dis. 2020, 79, 1516–1517. [Google Scholar] [CrossRef]
- Hernandez-Breijo, B.; Brenis, C.M.; Plasencia-Rodriguez, C.; Martinez-Feito, A.; Novella-Navarro, M.; Pascual-Salcedo, D.; Balsa, A. Methotrexate Reduces the Probability of Discontinuation of TNF Inhibitors in Seropositive Patients With Rheumatoid Arthritis. A Real-World Data Analysis. Front. Med. 2021, 8, 692557. [Google Scholar] [CrossRef]
- Fernandez, C.A. Pharmacological strategies for mitigating anti-TNF biologic immunogenicity in rheumatoid arthritis patients. Curr. Opin. Pharmacol. 2023, 68, 102320. [Google Scholar] [CrossRef]
- Isaacs, J.D.; Cohen, S.B.; Emery, P.; Tak, P.P.; Wang, J.; Lei, G.; Williams, S.; Lal, P.; Read, S.J. Effect of baseline rheumatoid factor and anticitrullinated peptide antibody serotype on rituximab clinical response: A meta-analysis. Ann. Rheum. Dis. 2013, 72, 329–336. [Google Scholar] [CrossRef]
- Sokolove, J.; Schiff, M.; Fleischmann, R.; Weinblatt, M.E.; Connolly, S.E.; Johnsen, A.; Zhu, J.; Maldonado, M.A.; Patel, S.; Robinson, W.H. Impact of baseline anti-cyclic citrullinated peptide-2 antibody concentration on efficacy outcomes following treatment with subcutaneous abatacept or adalimumab: 2-year results from the AMPLE trial. Ann. Rheum. Dis. 2016, 75, 709–714. [Google Scholar] [CrossRef]
- Norris-Grey, C.; Cambridge, G.; Moore, S.; Reddy, V.; Leandro, M. Long-term persistence of rituximab in patients with rheumatoid arthritis: An evaluation of the UCL cohort from 1998 to 2020. Rheumatology 2022, 61, 591–596. [Google Scholar] [CrossRef] [PubMed]
- Alten, R.; Mariette, X.; Flipo, R.M.; Caporali, R.; Buch, M.H.; Patel, Y.; Marsal, S.; Sanmarti, R.; Nurmohamed, M.T.; Griffiths, H.; et al. Retention of subcutaneous abatacept for the treatment of rheumatoid arthritis: Real-world results from the ASCORE study: An international 2-year observational study. Clin. Rheumatol. 2022, 41, 2361–2373. [Google Scholar] [CrossRef] [PubMed]
- van Dongen, H.; van Aken, J.; Lard, L.R.; Visser, K.; Ronday, H.K.; Hulsmans, H.M.; Speyer, I.; Westedt, M.L.; Peeters, A.J.; Allaart, C.F.; et al. Efficacy of methotrexate treatment in patients with probable rheumatoid arthritis: A double-blind, randomized, placebo-controlled trial. Arthritis Rheum. 2007, 56, 1424–1432. [Google Scholar] [CrossRef] [PubMed]
- Shipa, M.R.A.; Di Cicco, M.; Balogh, E.; Nitu, N.A.; Mainuddin, M.D.; Bhadauria, N.; Mukerjee, D.; Roussou, E. Drug-survival profiling of second-line biologic therapy in rheumatoid arthritis: Choice of another tumour necrosis factor inhibitor or a biologic of different mode of action? Mod. Rheumatol. 2023, 33, 700–707. [Google Scholar] [CrossRef]
- Bird, P.; Hall, S.; Nash, P.; Connell, C.A.; Kwok, K.; Witcombe, D.; Thirunavukkarasu, K. Treatment outcomes in patients with seropositive versus seronegative rheumatoid arthritis in Phase III randomised clinical trials of tofacitinib. RMD Open 2019, 5, e000742. [Google Scholar] [CrossRef]
- Paroli, M.; Becciolini, A.; Bravi, E.; Andracco, R.; Nucera, V.; Parisi, S.; Ometto, F.; Lumetti, F.; Farina, A.; Del Medico, P.; et al. Long-Term Retention Rate of Tofacitinib in Rheumatoid Arthritis: An Italian Multicenter Retrospective Cohort Study. Medicina 2023, 59, 1480. [Google Scholar] [CrossRef]
- Braaten, T.J.; Brahmer, J.R.; Forde, P.M.; Le, D.; Lipson, E.J.; Naidoo, J.; Schollenberger, M.; Zheng, L.; Bingham, C.O.; Shah, A.A.; et al. Immune checkpoint inhibitor-induced inflammatory arthritis persists after immunotherapy cessation. Ann. Rheum. Dis. 2020, 79, 332–338. [Google Scholar] [CrossRef]
- Michot, J.M.; Bigenwald, C.; Champiat, S.; Collins, M.; Carbonnel, F.; Postel-Vinay, S.; Berdelou, A.; Varga, A.; Bahleda, R.; Hollebecque, A.; et al. Immune-related adverse events with immune checkpoint blockade: A comprehensive review. Eur. J. Cancer 2016, 54, 139–148. [Google Scholar] [CrossRef]
- Chang, M.H.; Nigrovic, P.A. Antibody-dependent and -independent mechanisms of inflammatory arthritis. JCI Insight 2019, 4, 6483516. [Google Scholar] [CrossRef]
- Gianchecchi, E.; Delfino, D.V.; Fierabracci, A. Recent insights into the role of the PD-1/PD-L1 pathway in immunological tolerance and autoimmunity. Autoimmun. Rev. 2013, 12, 1091–1100. [Google Scholar] [CrossRef]
- Tuttle, J.; Drescher, E.; Simon-Campos, J.A.; Emery, P.; Greenwald, M.; Kivitz, A.; Rha, H.; Yachi, P.; Kiley, C.; Nirula, A. A Phase 2 Trial of Peresolimab for Adults with Rheumatoid Arthritis. N. Engl. J. Med. 2023, 388, 1853–1862. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Feature | SNRA | SPRA | References |
|---|---|---|---|
| HLA-B*08/DRB1*03 | High | Low | [21] |
| HLA-DRB1*04/*10 | No | High | [29] |
| SNP ANKRD55 | High | No | [25] |
| SNP CLYBL | High | No | [26] |
| has-miR-362-5p | High | Low | [27] |
| has-miR-708-3p | High | Low | [28] |
| has-miR-24 | High | High | [30] |
| has-miR-125a | High | High | [30] |
| has-miR-22 | Low | High | [30] |
| has-miR-361-5p | Low | High | [30] |
| has-miR-233-3p | Low | High | [30] |
| Cell Type | SNRA | SPRA | References |
|---|---|---|---|
| Synovial lining CD68+ cells | Rare | Frequent | [28] |
| Synovial CD4+ T cells | Rare | Frequent | [28] |
| Synovial vessel CD31+ cells | Rare | Frequent | [28] |
| Synovial monocytes | Frequent | Rare | [21] |
| Synovial macrophages | Frequent | Rare | [21] |
| Plasma cells | Frequent | Rare | [32] |
| PD-1+ T cells | Rare | Frequent | [33] |
| Feature | SNRA | SPRA | References |
|---|---|---|---|
| mTSS | Low | High | [71] |
| MCP II damage | Low | High | [60] |
| MCP III damage | Low | High | [60] |
| MCP V damage | Low | High | [60] |
| Synovitis | Rare | Frequent | [66] |
| Tenosynovitis | Frequent | Rare | [67] |
| Extra-synovial involvement | Frequent | Rare | [70] |
| Drug | SNRA | SPRA | References |
|---|---|---|---|
| MTX | Limited | Good | [96] |
| TNFi | Good | Good | [104] |
| Second TNFi | Good | Limited | [104] |
| Anti-CD20 biologic | No | Good | [101] |
| Anti-CD80/CD86 biologic | Limited | Good | [102] |
| JAKis | Uncertain | Good | [105] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paroli, M.; Sirinian, M.I. When Autoantibodies Are Missing: The Challenge of Seronegative Rheumatoid Arthritis. Antibodies 2023, 12, 69. https://doi.org/10.3390/antib12040069
Paroli M, Sirinian MI. When Autoantibodies Are Missing: The Challenge of Seronegative Rheumatoid Arthritis. Antibodies. 2023; 12(4):69. https://doi.org/10.3390/antib12040069
Chicago/Turabian StyleParoli, Marino, and Maria Isabella Sirinian. 2023. "When Autoantibodies Are Missing: The Challenge of Seronegative Rheumatoid Arthritis" Antibodies 12, no. 4: 69. https://doi.org/10.3390/antib12040069
APA StyleParoli, M., & Sirinian, M. I. (2023). When Autoantibodies Are Missing: The Challenge of Seronegative Rheumatoid Arthritis. Antibodies, 12(4), 69. https://doi.org/10.3390/antib12040069