

Investigation of Possible Factors Influencing the Neutralizing Anti-SARS-CoV-2 Antibody Titer after Six Months from the Second Vaccination Dose in a Sample of Italian Nursing Home Personnel

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Description of the Study
- -
- being an employee of the nursing home at work during the period January–August 2021;
- -
- being vaccinated with two doses of the Pfizer/BioNTech BNT162b2 anti-SARS-CoV-2 mRna vaccine between 12 January and 17 February of 2021 (i.e., the dates that we identified during the baseline investigation);
- -
- having participated to our first baseline investigation, with an available anti-SARS-CoV-2 IgG antibody titer determined via a serological test performed in our lab.
2.2. Statistical Analysis
3. Results
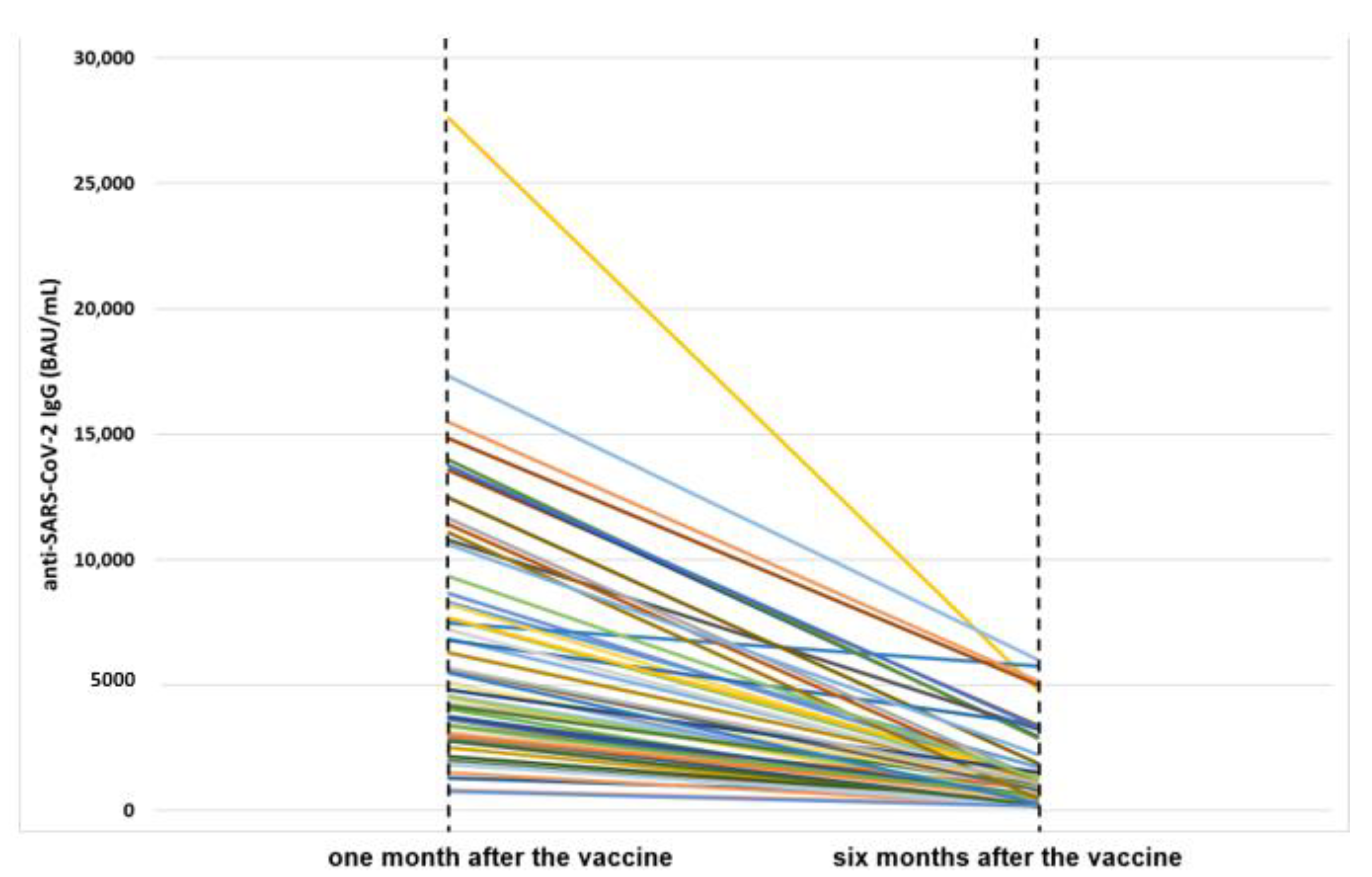
3.1. Characteristics of the Study Population and Anti-SARS-CoV-2 Antibody Titer in the Vaccinated Subjects after One Month and Six Months from the Second Vaccine Dose
3.2. Evaluation of the Decrease of Anti-SARS-CoV-2 Antibody Titer in the Vaccinated Subjects Six Months after the Second Dose and of the Possible Associated Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Achiron, A.; Mandel, M.; Dreyer-Alster, S.; Harari, G.; Gurevich, M. Humoral SARS-CoV-2 IgG decay within 6 months in COVID-19 healthy vaccinees: The need for a booster vaccine dose? Eur. J. Intern. Med. 2021, 94, 105–107. [Google Scholar] [CrossRef]
- Andrews, N.; Tessier, E.; Stowe, J.; Gower, C.; Kirsebom, F.; Simmons, R.; Gallagher, E.; Thelwall, S.; Groves, N.; Dabrera, G.; et al. Duration of Protection against Mild and Severe Disease by COVID-19 Vaccines. N. Engl. J. Med. 2022, 386, 340–350. [Google Scholar] [CrossRef]
- Israel, A.; Shenhar, Y.; Green, I.; Merzon, E.; Golan-Cohen, A.; Schäffer, A.A.; Ruppin, E.; Vinker, S.; Magen, E. Large-Scale Study of Antibody Titer Decay following BNT162b2 mRNA Vaccine or SARS-CoV-2 Infection. Vaccines 2021, 10, 64. [Google Scholar] [CrossRef]
- Poukka, E.; Baum, U.; Palmu, A.A.; Lehtonen, T.O.; Salo, H.; Nohynek, H.; Leino, T. Cohort study of COVID-19 vaccine effectiveness among healthcare workers in Finland, December 2020–October 2021. Vaccine 2022, 40, 701–705. [Google Scholar] [CrossRef]
- Abbasi, J. Fourth COVID-19 Vaccine Dose Increases Low Antibodies. JAMA 2022, 327, 517. [Google Scholar] [CrossRef] [PubMed]
- Kamar, N.; Abravanel, F.; Marion, O.; Esposito, L.; Hebral, A.L.; Médrano, C.; Guitard, J.; Lavayssière, L.; Cointault, O.; Nogier, M.B.; et al. Anti-SARS-CoV-2 spike protein and neutralizing antibodies at 1 and 3 months after three doses of SARS-CoV-2 vaccine in a large cohort of solid organ transplant patients. Am. J. Transplant. 2022, 22, 1467–1474. [Google Scholar] [CrossRef] [PubMed]
- Kundu, R.; Narean, J.S.; Wang, L.; Fenn, J.; Pillay, T.; Fernandez, N.D.; Conibear, E.; Koycheva, A.; Davies, M.; Tolosa-Wright, M.; et al. Cross-reactive memory T cells associate with protection against SARS-CoV-2 infection in COVID-19 contacts. Nat. Commun. 2022, 13, 80. [Google Scholar] [CrossRef] [PubMed]
- Barrière, J.; Carles, M.; Audigier-Valette, C.; Re, D.; Adjtoutah, Z.; Seitz-Polski, B.; Gounant, V.; Detscamps, D.; Zalcman, G. Third dose of anti-SARS-CoV-2 vaccine for patients with cancer: Should humoral responses be monitored? A position article. Eur. J. Cancer 2022, 162, 182–193. [Google Scholar] [CrossRef]
- Toda, M.; Yoshifuji, A.; Kikuchi, K.; Komatsu, M.; Fujii, K.; Kato, A.; Kikuchi, T.; Nakazawa, A.; Ryuzaki, M. Factors associated with SARS-CoV-2 antibody titers and prognosis of breakthrough infection in hemodialysis patients. Clin. Exp. Nephrol. 2022, 26, 571–580. [Google Scholar] [CrossRef]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based COVID-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef]
- Fraley, E.; LeMaster, C.; Khanal, S.; Banerjee, D.; Pastinen, T.; Grundberg, E.; Selvarangan, R.; Bradley, T. Prior infection and age impacts antibody persistence after SARS-CoV-2 mRNA vaccine. Clin. Infect. Dis. 2021, 75, ciab850. [Google Scholar] [CrossRef]
- U.S. Centers for Disease Control and Prevention (CDC). People with Certain Medical Conditions. 2022. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html (accessed on 5 July 2022).
- Modenese, A.; Casolari, L.; Rossi, G.; Della Vecchia, E.; Glieca, F.; D’Elia, C.; Garavini, D.; Righi, E.; Mariani, S.; Venturelli, L.; et al. Factors Associated with SARS-CoV-2 Infection Risk among Healthcare Workers of an Italian University Hospital. Healthcare 2021, 9, 1495. [Google Scholar] [CrossRef] [PubMed]
- Justiz Vaillant, A.A.; Qurie, A. Immunodeficiency. In StatPearls. Treasure Island (FL); StatPearls Publishing: Tampa, FL, USA, 2022. [Google Scholar]
- Loef, B.; van Baarle, D.; van der Beek, A.J.; Sanders, E.A.M.; Bruijning-Verhagen, P.; Proper, K.I. Shift Work and Respiratory Infections in Health-Care Workers. Am. J. Epidemiol. 2019, 188, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Rizza, S.; Coppeta, L.; Grelli, S.; Ferrazza, G.; Chiocchi, M.; Vanni, G.; Bonomo, O.C.; Bellia, A.; Andreoni, M.; Magrini, A.; et al. High body mass index and night shift work are associated with COVID-19 in health care workers. J. Endocrinol. Investig. 2021, 44, 1097–1101. [Google Scholar] [CrossRef]
- Maidstone, R.; Anderson, S.G.; Ray, D.W.; Rutter, M.K.; Durrington, H.J.; Blaikley, J.F. Shift work is associated with positive COVID-19 status in hospitalised patients. Thorax 2021, 76, 601–606. [Google Scholar] [CrossRef]
- Wang, X.; Jiang, X.; Huang, Q.; Wang, H.; Gurarie, D.; Ndeffo-Mbah, M.; Fan, F.; Fu, P.; Horn, M.A.; Mondal, A.; et al. Risk factors of SARS-CoV-2 infection in healthcare workers: A retrospective study of a nosocomial outbreak. Sleep Med. X 2020, 2, 100028. [Google Scholar] [CrossRef]
- Munter, G.; Levi-Vineberg, T.; Sylvetsky, N. Vitamin D deficiency among physicians: A comparison between hospitalists and community-based physicians. Osteoporos. Int. 2015, 26, 1673–1676. [Google Scholar] [CrossRef]
- Meltzer, D.O.; Best, T.J.; Zhang, H.; Vokes, T.; Arora, V.M.; Solway, J. Association of Vitamin D Levels, Race/Ethnicity, and Clinical Characteristics With COVID-19 Test Results. JAMA Netw. Open. 2021, 4, e214117. [Google Scholar] [CrossRef]
- Benskin, L.L. A Basic Review of the Preliminary Evidence That COVID-19 Risk and Severity Is Increased in Vitamin D Deficiency. Front. Public Health 2020, 8, 513. [Google Scholar] [CrossRef]
- Zhou, R.; Wang, P.; Wong, Y.C.; Xu, H.; Lau, S.Y.; Liu, L.; Mok, B.W.-Y.; Peng, Q.; Liu, N.; Woo, K.-F.; et al. Nasal prevention of SARS-CoV-2 infection by intranasal influenza-based boost vaccination in mouse models. eBioMedicine 2022, 75, 103762. [Google Scholar] [CrossRef]
- Greco, M.; Cucci, F.; Portulano, P.; Lazzari, R.A.; Caldararo, C.; Sicuro, F.; Catanese, C.; Lobreglio, G. Effects of Influenza Vaccination on the Response to BNT162b2 Messenger RNA COVID-19 Vaccine in Healthcare Workers. J. Clin. Med. Res. 2021, 13, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Modenese, A.; Paduano, S.; Bargellini, A.; Bellucci, R.; Marchetti, S.; Bruno, F.; Grazioli, P.; Vivoli, R.; Gobba, F. Neutralizing Anti-SARS-CoV-2 Antibody Titer and Reported Adverse Effects, in a Sample of Italian Nursing Home Personnel after Two Doses of the BNT162b2 Vaccine Administered Four Weeks Apart. Vaccines 2021, 9, 652. [Google Scholar] [CrossRef] [PubMed]
- Euroimun. Anti-SARS-CoV-2 QuantiVac ELISA (IgG). 2021. Available online: https://www.coronavirus-diagnostics.com/documents/Indications/Infections/Coronavirus/EI_2606_D_UK_E.pdf (accessed on 5 July 2022).
- First WHO International Standard Anti-SARS-CoV-2 Immunoglobulin (Human). Product Number 20/136. 2020. Available online: https://www.nibsc.org/documents/ifu/20-136.pdf (accessed on 5 July 2022).
- Chivu-Economescu, M.; Bleotu, C.; Grancea, C.; Chiriac, D.; Botezatu, A.; Iancu, I.V.; Pitica, I.; Necula, L.G.; Neagu, A.; Matei, L.; et al. Kinetics and persistence of cellular and humoral immune responses to SARS-CoV-2 vaccine in healthcare workers with or without prior COVID-19. J. Cell Mol. Med. 2022, 26, 1293–1305. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Kim, Y.R.; Heo, S.T.; Oh, H.; Kim, M.; Lee, H.R.; Yoo, J.R. Healthcare Workers in South Korea Maintain a SARS-CoV-2 Antibody Response Six Months After Receiving a Second Dose of the BNT162b2 mRNA Vaccine. Front. Immunol. 2022, 13, 827306. [Google Scholar] [CrossRef] [PubMed]
- Helle, F.; Moyet, J.; Demey, B.; François, C.; Duverlie, G.; Castelain, S.; Bloch, F.; Brochot, E. Humoral anti-SARS-CoV-2 immune response after two doses of Comirnaty vaccine in nursing home residents by previous infection status. Vaccine 2022, 40, 531–535. [Google Scholar] [CrossRef]
- Ministero della Salute. Piano Vaccini Anti COVID-19. 2022. Available online: https://www.salute.gov.it/portale/nuovocoronavirus/dettaglioContenutiNuovoCoronavirus.jsp?lingua=italiano&id=5452&area=nuovoCoronavirus&menu=vuoto (accessed on 5 July 2022).
- Modenese, A.; Gobba, F. Increased Risk of COVID-19-Related Deaths among General Practitioners in Italy. Healthcare 2020, 8, 155. [Google Scholar] [CrossRef]
- Di Resta, C.; Ferrari, D.; Viganò, M.; Moro, M.; Sabetta, E.; Minerva, M.; Ambrosio, A.; Locatelli, M.; Tomaiuolo, R. The Gender Impact Assessment among Healthcare Workers in the SARS-CoV-2 Vaccination-An Analysis of Serological Response and Side Effects. Vaccines 2021, 9, 522. [Google Scholar] [CrossRef]


{kind=link}
| N (%) * | Anti-SARS-CoV-2 IgG (BAU/mL) One Month after Vaccination–MD (Range: Min–Max) | Anti-SARS-CoV-2 IgG (BAU/mL) Six Months after Vaccination—MD (Range: Min–Max) | p-Value | ∆ Anti-SARS-CoV-2 IgG (One vs. Six Months after Vaccination) BAU/mL MD (Q1; Q3) | % (Anti-SARS-CoV-2 IgG) Decline Six Months after Vaccination MD (Q1; Q3) | p-Value | ||
|---|---|---|---|---|---|---|---|---|
| Overall | 63 (100) | 4821 (764–27,600) | 876 (156–6034) | <0.001 | 3802 (2465; 7367) | 82.9 (78.5; 88.6) | ||
| Sex | Males | 13 (20.6) | 3398 (764–17,300) | 355 (161–6034) | <0.001 | 2870 (1790; 7367) | 84.5 (78.9; 91.0) | 0.445 |
| Females | 50 (79.4) | 5285 (830–27,600) | 895 (156–5748) | <0.001 | 4074 (2472; 7010) | 82.1 (78.5; 87.1) | ||
| Age class a | ≤30 | 6 (9.5) | 8288 (3695–13,749) | 756 (239–3347) | <0.001 | 7783 (4472; 10,402) | 91.3 (81.2; 94.9) | 0.041 |
| 31–40 | 11 (17.5) | 3074 (1824–11,390) | 355 (169–1398) | <0.001 | 2452 (1789; 3426) | 83.4 (81.8; 91.0) | ||
| 41–50 | 12 (19.1) | 4820 (2508–12,465) | 882 (245–2242) | <0.001 | 4074 (2623; 5473) | 83.6 (80.5; 86.7) | ||
| 51–60 | 21 (33.3) | 4821 (830–15,474) | 1035 (156–5748) | <0.001 | 3280 (2627; 6556) | 84.2 (74.9; 85.9) | ||
| >60 | 13 (20.6) | 6783 (764–27,600) | 1293 (161–6034) | <0.001 | 5034 (3085; 9811) | 78.5 (69.9; 82.5) | ||
| BMI | <25 | 32 (51.6) | 4700 (830–13,749) | 668 (169–3347) | <0.001 | 3844 (2438; 5817) | 83.6 (79.5; 89.9) | 0.208 |
| 25–29.9 | 25 (40.3) | 6783 (764–17,300) | 1169 (161–6034) | <0.001 | 3372 (2472; 7540) | 80.2 (73.5; 85.1) | ||
| ≥30 | 5 (8.1) | 4557 (2783–14,834) | 588 (156–5024) | <0.003 | 3969 (2870; 6285) | 84.5 (81.8; 87.1) | ||
| Smoking habit | Non-smokers | 48 (76.2) | 4568 (764–27,600) | 669 (156–6034) | <0.001 | 3752 (2462; 8197) | 82.7 (78.7; 88.4) | 0.796 |
| Smokers | 15 (23.8) | 6783 (1824–13,551) | 1205 (175–5748) | <0.001 | 3986 (2472; 6556) | 83.0 (74.9; 88.6) | ||
| Job type | HCW | 28 (44.4) | 6226 (1504–27,600) | 1163 (169–6034) | <0.001 | 4355 (3018; 8926) | 82.3 (74.2; 86.0) | 0.407 |
| Other employees | 35 (55.6) | 4150 (764–15,474) | 588 (156–5174) | <0.001 | 3456 (2452; 6285) | 83.0 (79.1; 89.1) | ||
| Nightshifts at work | No | 49 (80.3) | 4254 (764–17,300) | 588 (156–6033) | <0.001 | 3456 (2465; 7367) | 84.5 (79.1; 89.1) | 0.085 |
| Yes | 12 (19.7) | 5959 (2508–27,600) | 1221 (245–5748) | <0.001 | 4074 (2448; 6493) | 80.5 (75.7; 83.3) | ||
| Anti-influenza vaccine | No | 39 (61.9) | 5062 (830–27,600) | 1035 (175–5748) | <0.001 | 3702 (2404; 8354) | 81.2 (75.1; 85.0) | 0.017 |
| Yes | 24 (38.1) | 4527 (764–17,300) | 558 (156–6034) | <0.001 | 3886 (2811; 5879) | 86.6 (79.4; 92.0) | ||
| COVID-19 diagnosis | No | 34 (54.0) | 3721 (764–27,600) | 512 (156–5174) | <0.001 | 3310 (2452; 6556) | 85.2 (79.3; 91.5) | 0.016 |
| Yes | 29 (46.0) | 6783 (1310–17,300) | 1205 (178–6034) | <0.001 | 5034 (2870; 9811) | 81.2 (73.5; 85.0) | ||
| Pathologies number | 0 | 32 (50.8) | 4364 (830–15,474) | 759 (175–5174) | <0.001 | 3752 (2438; 6720) | 82.6 (79.0; 87.3) | 0.420 |
| 1 | 22 (34.9) | 5695 (764–27,600) | 540 (161–6034) | <0.001 | 3679 (2535; 8041) | 85.2 (78.9; 88.7) | ||
| ≥2 | 9 (14.3) | 4821 (2783–14,834) | 1169 (156–5024) | <0.001 | 3969 (3085; 6285) | 79.0 (72.5; 85.0) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Modenese, A.; Paduano, S.; Bellucci, R.; Marchetti, S.; Bruno, F.; Grazioli, P.; Vivoli, R.; Gobba, F.; Bargellini, A. Investigation of Possible Factors Influencing the Neutralizing Anti-SARS-CoV-2 Antibody Titer after Six Months from the Second Vaccination Dose in a Sample of Italian Nursing Home Personnel. Antibodies 2022, 11, 59. https://doi.org/10.3390/antib11030059
Modenese A, Paduano S, Bellucci R, Marchetti S, Bruno F, Grazioli P, Vivoli R, Gobba F, Bargellini A. Investigation of Possible Factors Influencing the Neutralizing Anti-SARS-CoV-2 Antibody Titer after Six Months from the Second Vaccination Dose in a Sample of Italian Nursing Home Personnel. Antibodies. 2022; 11(3):59. https://doi.org/10.3390/antib11030059
Chicago/Turabian StyleModenese, Alberto, Stefania Paduano, Rossana Bellucci, Simona Marchetti, Fulvio Bruno, Pietro Grazioli, Roberto Vivoli, Fabriziomaria Gobba, and Annalisa Bargellini. 2022. "Investigation of Possible Factors Influencing the Neutralizing Anti-SARS-CoV-2 Antibody Titer after Six Months from the Second Vaccination Dose in a Sample of Italian Nursing Home Personnel" Antibodies 11, no. 3: 59. https://doi.org/10.3390/antib11030059
APA StyleModenese, A., Paduano, S., Bellucci, R., Marchetti, S., Bruno, F., Grazioli, P., Vivoli, R., Gobba, F., & Bargellini, A. (2022). Investigation of Possible Factors Influencing the Neutralizing Anti-SARS-CoV-2 Antibody Titer after Six Months from the Second Vaccination Dose in a Sample of Italian Nursing Home Personnel. Antibodies, 11(3), 59. https://doi.org/10.3390/antib11030059