
Specific Immunoglobulin E and G to Common Food Antigens and Increased Serum Zonulin in IBS Patients: A Single-Center Bulgarian Study



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
- -
- Symptoms related to defecation (may be increased or unchanged);
- -
- Symptoms associated with a change in stool frequency;
- -
- Symptoms related to a change in stool form or appearance.
2.2. Methods
Statistical Analysis
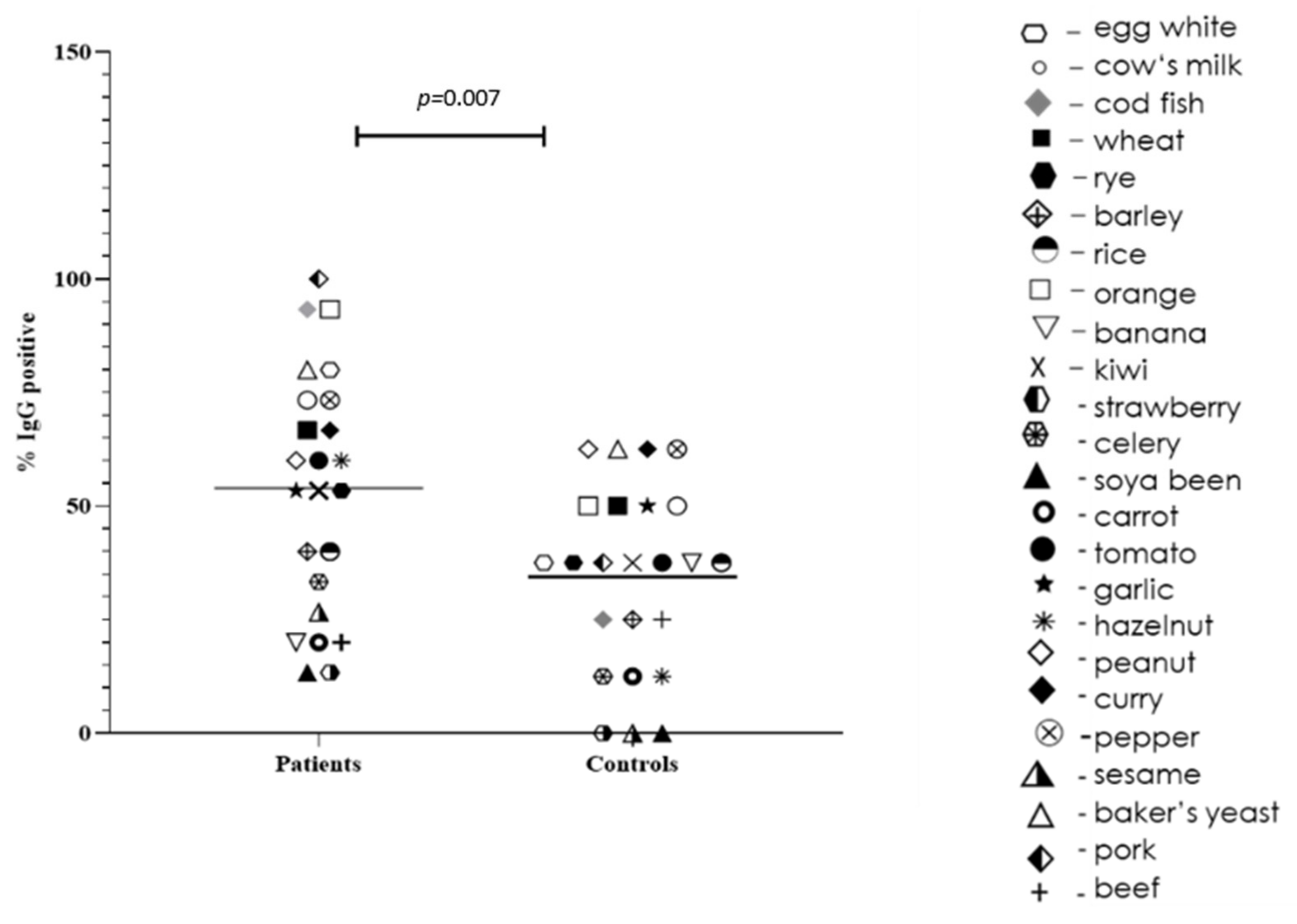
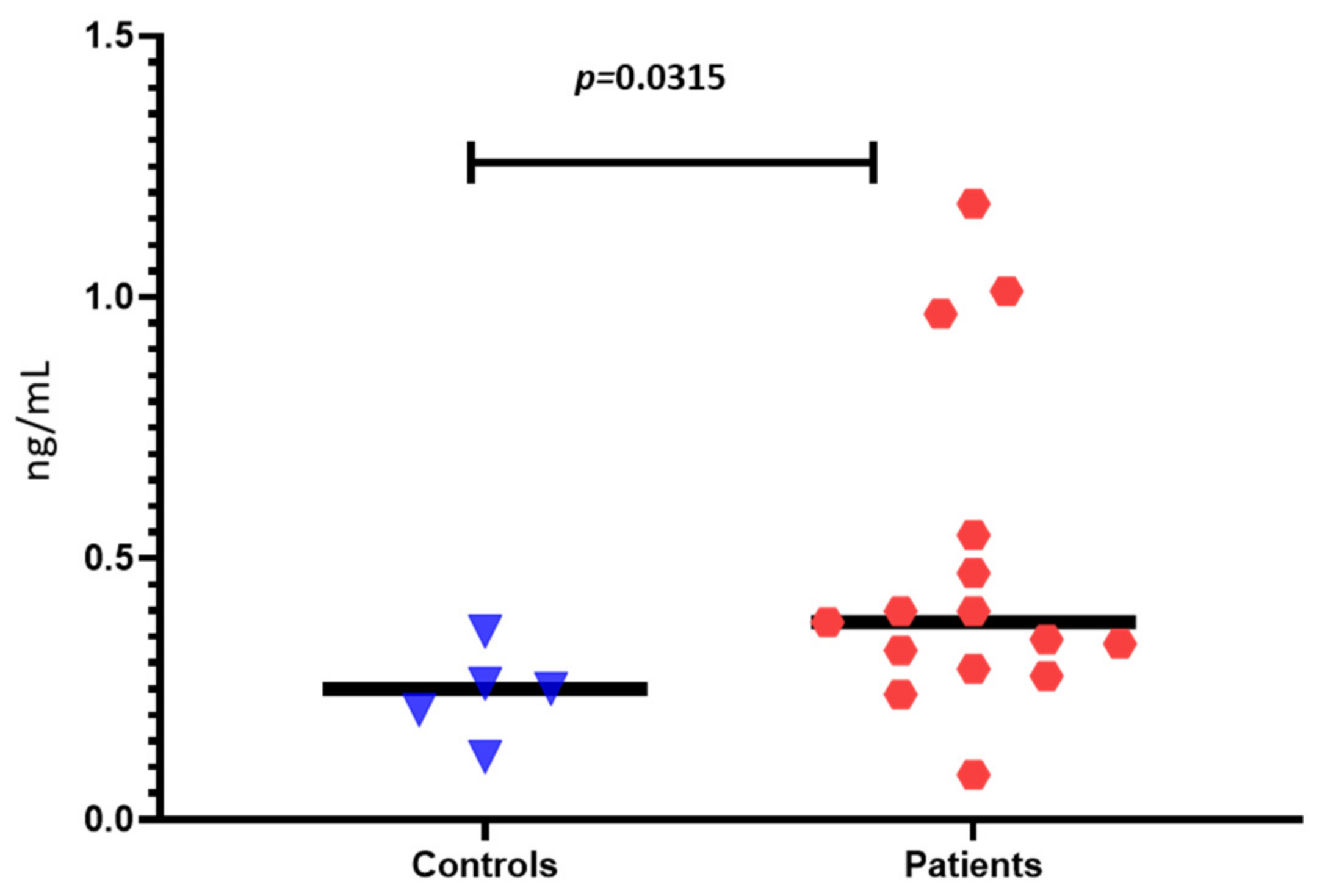
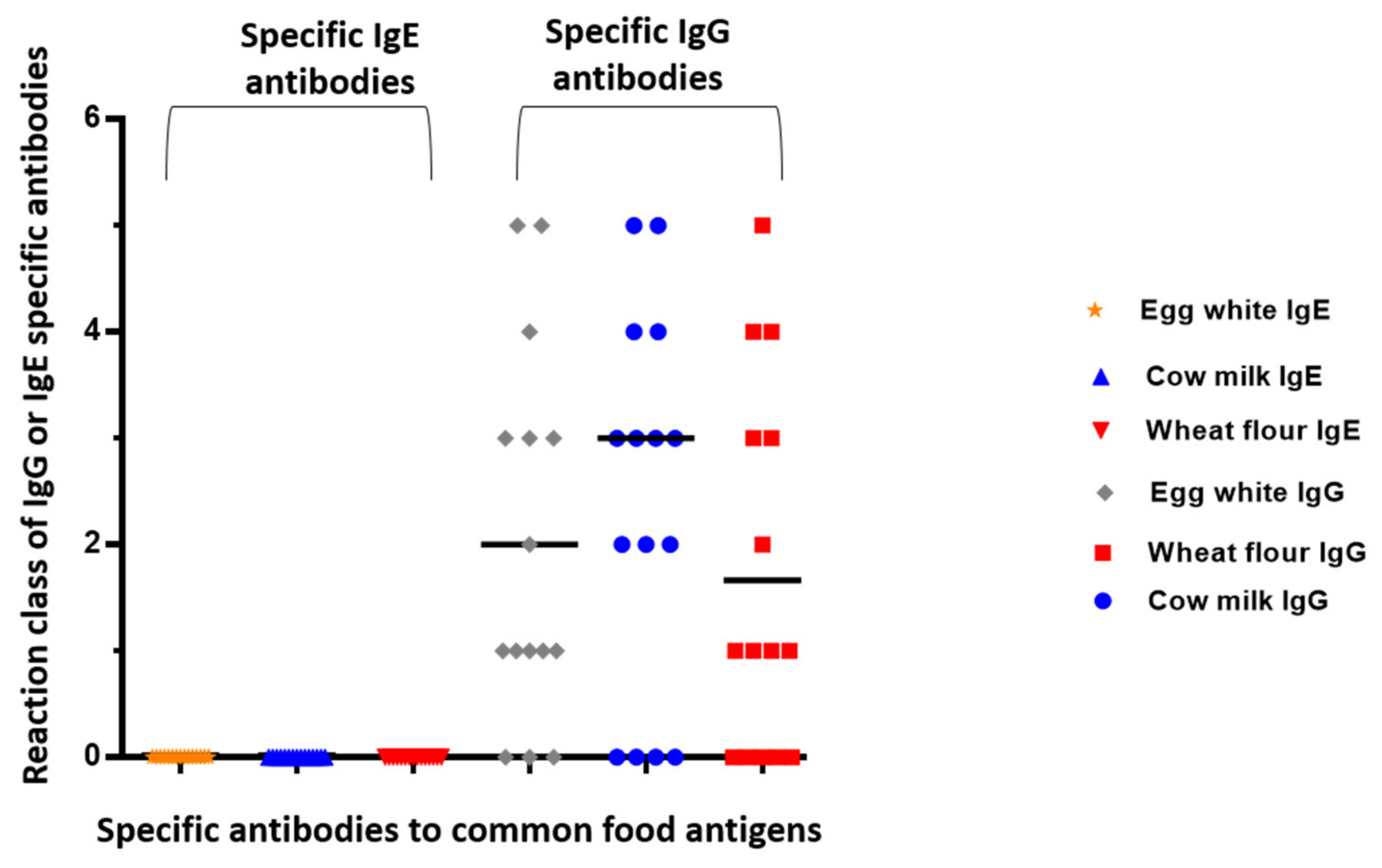
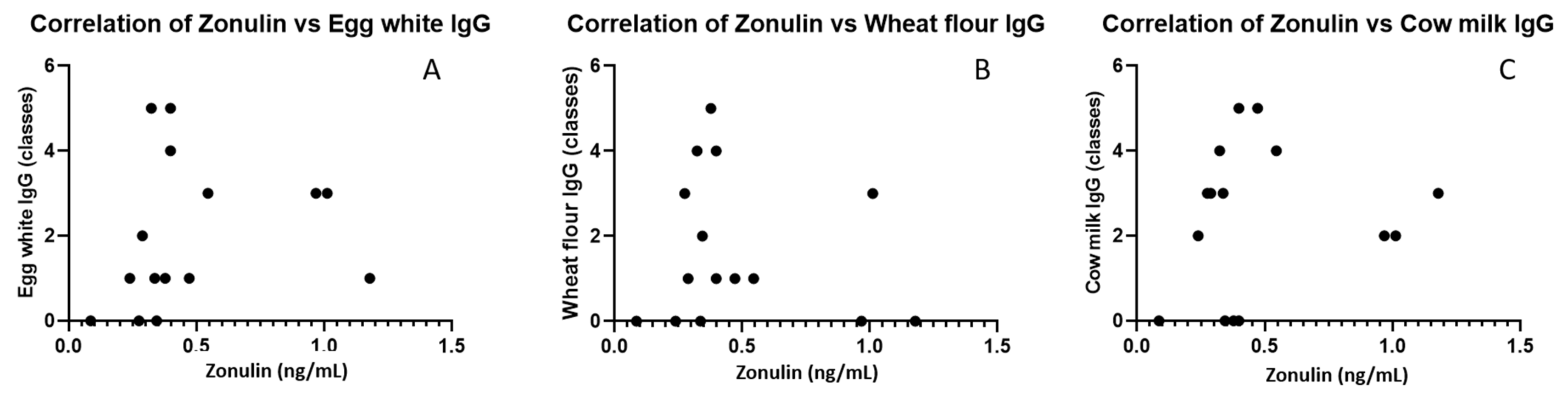
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Balmus, I.-M.; Ilie, O.-D.; Ciobica, A.; Cojocariu, R.-O.; Stanciu, C.; Trifan, A.; Cimpeanu, M.; Cimpeanu, C.; Gorgan, L. Irritable Bowel Syndrome between Molecular Approach and Clinical Expertise—Searching for Gap Fillers in the Oxidative Stress Way of Thinking. Medicina 2020, 56, 38. [Google Scholar] [CrossRef] [PubMed]
- Li, F.X.; Patten, S.B.; Hilsden, R.J.; Sutherland, L.R. Irritable bowel syndrome and health-related quality of life: A population-based study in Calgary, Alberta. Can. J. Gastroenterol. Hepatol. 2003, 17, 259–263. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lovell, R.M.; Ford, A.C. Global prevalence of and risk factors for irritable bowel syndrome: A meta-analysis. Clin. Gastroenterol. Hepatol. 2012, 10, 712–721.e4. [Google Scholar] [CrossRef]
- Foxx-Orenstein, A.E. New and emerging therapies for the treatment of irritable bowel syndrome: An update for gastroenterologists. Ther. Adv. Gastroenterol. 2016, 9, 354–375. [Google Scholar] [CrossRef] [PubMed]
- Adriani, A.; Ribaldone, D.G.; Astegiano, M.; Durazzo, M.; Saracco, G.M.; Pellicano, R. Irritable bowel syndrome: The clinical approach. Panminerva Med. 2018, 60, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Choung, R.S.; Talley, N.J. Food Allergy and Intolerance in IBS. Gastroenterol. Hepatol. 2006, 2, 756–760. [Google Scholar]
- Elsenbruch, S. Abdominal pain in irritable bowel syndrome: A review of putative psychological, neural and neuro-immune mechanisms. Brain Behav. Immun. 2011, 25, 386–394. [Google Scholar] [CrossRef]
- Velikova, T.; Kukov, A.; Georgieva, V.; Peruhova, M.; Yurukova, N.; Mihova, A.; Mehandziyska-Marinova, T.; Mizgova, G.; Terzieva, V.; Zhelezova, G.; et al. Methods for detection of food intolerance. Recent Adv. Food Sci. 2018, 1, 106–119. [Google Scholar]
- Dainese, R.; Galliani, E.A.; De Lazzari, F.; Leo, V.D.; Naccarato, R. Discrepancies between reported food intolerance and sensitization test findings in irritable bowel syndrome patients. Am. J. Gastroenterol. 1999, 94, 1892–1897. [Google Scholar] [CrossRef] [PubMed]
- Gwynn, C.M.; Smith, J.M.; Leon, G.L.; Stanworth, D.R. Role of IgG4 subclass in childhood allergy. Lancet 1978, 1, 910–911. [Google Scholar] [CrossRef]
- Husby, S.; Oxelius, V.A.; Teisner, B.; Jensenius, J.C.; Svehag, S.-E. Humoral immunity to dietary antigens in healthy adults. Occurrence, isotype and IgG subclass distribution of serum antibodies to protein antigens. Int. Arch. Allergy Appl. Immunol. 1985, 77, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Barnes, R.M.; Harvey, M.M.; Blears, J.; Finn, R.; Johnson, P. IgG subclass of human serum antibodies reactive with dietary proteins. Int. Arch. Allergy Appl. Immunol. 1986, 81, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Hunter, J.O. Food elimination in IBS: The case for IgG testing remains doubtful. Gut 2005, 54, 1203. [Google Scholar] [PubMed]
- Barnes, R.M.; Lewis-Jones, M.S.; Allan, S.; Dixon, T.A.; Vickers, C.F.H. Development and isotype diversity of antibodies to inhalant and dietary antigens in childhood atopic eczema. Clin. Exp. Dermatol. 1993, 18, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, R.; Tsujimura, Y.; Obata, K.; Dixon, T.A.; Vickers, C.F.H. IgG-mediated systemic anaphylaxis to protein antigen can be induced even under conditions of limited amounts of antibody and antigen. Biochem. Biophys. Res. Commun. 2010, 402, 742–746. [Google Scholar] [CrossRef]
- Tsujimura, Y.; Obata, K.; Mukai, K.; Shindou, H.; Shindou, M.; Nishikado, H.; Kawano, Y.; Kawano, Y.; Shimizu, T.; Karasuyama, H. Basophils play a pivotal role in immunoglobulin-G-mediated but not immunoglobulin-E-mediated systemic anaphylaxis. Immunity 2008, 28, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Brandtzaeg, P. Food allergy: Separating the science from the mythology. Nat. Rev. Gastroenterol. Hepatol. 2010, 7, 380–400. [Google Scholar] [CrossRef] [PubMed]
- Vojdani, A. Detection of IgE, IgG, IgA and IgM antibodies against raw and processed food antigens. Nutr. Metab. 2009, 6, 22. [Google Scholar] [CrossRef]
- Bock, S.A. AAAAI Support of the EAACI Position Paper on IgG4; Position Statement. J. Allergy Clin. Immunol. 2010, 125, 1410. [Google Scholar] [CrossRef]
- Fasano, A. All disease begins in the (leaky) gut: Role of zonulin-mediated gut permeability in the pathogenesis of some chronic inflammatory diseases. F1000Research 2020, 9, 69. [Google Scholar] [CrossRef]
- Fasano, A. Zonulin, regulation of tight junctions, and autoimmune diseases. Ann. N. Y. Acad. Sci. 2012, 1258, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Stevens, B.R.; Goel, R.; Seungbum, K.; Richards, E.M.; Holbert, R.C.; Pepine, C.J.; Raizada, M.K. Increased human intestinal barrier permeability plasma biomarkers zonulin and FABP2 correlated with plasma LPS and altered gut microbiome in anxiety or depression. Gut 2018, 67, 1555–1557. [Google Scholar] [CrossRef] [PubMed]
- Paterson, B.M.; Lammers, K.M.; Arrieta, M.C.; Fasano, A.; Meddings, J.B. The safety, tolerance, pharmacokinetic and pharmacodynamic effects of single doses of AT-1001 in coeliac disease subjects: A proof of concept study. Aliment. Pharmacol. Ther. 2007, 26, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Sturgeon, C.; Lan, J.; Fasano, A. Zonulin transgenic mice show altered gut permeability and increased morbidity/mortality in the DSS colitis model. Ann. N. Y. Acad. Sci. 2017, 1397, 130–142. [Google Scholar] [CrossRef] [PubMed]
- Velikova, T.V.; Altankova, I.; Peruhova, M.; Mihova, A.; Kukov, A.; Georgieva, V.; Yurukova, N.; Mizgova, G.; Mehandzhiyska-Marinova, T.; Terzieva, V.; et al. Prevalence of Specific IgG to Food Antigens in Bulgarian IBS Patients: A Preliminary Study. Mathews J. Nutr. Diet. 2018, 3, 017. [Google Scholar]
- Velikova, T.V.; Altankova, I.; Mihova, A.; Terzieva, V.; Georgieva, V.; Kukov, A.; Yurukova, N.; Mehandzhiyska-Marinova, T.; Mizgova, G.; Zhelezova, G.; et al. IgG-mediated immune reactivity in patients with Irritable Bowel Syndrome: A pilot study. In Yearbook of Bulgarian Association for Clinical Immunology; Central Medical Library, Medical University: Sofia, Bulgaria, 2018; Volume 12, pp. 31–71. [Google Scholar]
- Schur, P.H.; Rosen, F.; Norman, M.E. Immunoglobulin subclasses in normal children. Pediatr. Res. 1979, 13, 181–183. [Google Scholar] [CrossRef] [PubMed]
- Bentley, S.J.; Pearson, D.J.; Rix, K.J. Food hypersensitivity in irritable bowel syndrome. Lancet 1983, 2, 295–297. [Google Scholar] [CrossRef]
- Zar, S.; Mincher, L.; Benson, M.J.; Kumar, D. Food-specific IgG4 antibodyguided exclusion diet improves symptoms and rectal compliance in irritable bowel syndrome. Scand. J. Gastroenterol. 2005, 40, 800–807. [Google Scholar] [CrossRef]
- Zeng, Q.; Dong, S.Y.; Wu, L.X.; Li, H.; Sun, Z.-J.; Li, J.-B.; Jiang, H.-X.; Chen, Z.-H.; Wang, Q.-B.; Chen, W.-W. Variable food-specific IgG antibody levels in healthy and symptomatic Chinese adults. PLoS ONE 2013, 8, e53612. [Google Scholar] [CrossRef]
- Ligaarden, S.C.; Lydersen, S.; Farup, P.G. IgG and IgG4 antibodies in subjects with irritable bowel syndrome: A case control study in the general population. BMC Gastroenterol. 2012, 12, 166. [Google Scholar] [CrossRef] [PubMed]
- Kvehaugen, A.S.; Tveiten, D.; Farup, P.G. Is perceived intolerance to milk and wheat associated with the corresponding IgG and IgA food antibodies? A cross sectional study in subjects with morbid obesity and gastrointestinal symptoms. BMC Gastroenterol. 2018, 18, 22. [Google Scholar] [CrossRef] [PubMed]
- Wilders-Truschnig, M.; Mangge, H.; Lieners, C.; Gruber, H.-J.; Mayer, C.; März, W. IgG antibodies against food antigens are correlated with inflammation and intima media thickness in obese juveniles. Exp. Clin. Endocrinol. Diabetes 2008, 116, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Aydinlar, E.I.; Dikmen, P.Y.; Tiftikci, A.; Saruc, M.; Aksu, M.; Gunsoy, H.G.; Tozun, N. IgG-based elimination diet in migraine plus irritable bowel syndrome. Headache 2013, 53, 514–525. [Google Scholar] [CrossRef] [PubMed]
- Drisko, J.; Bischoff, B.; Hall, M.; McCallum, R. Treating irritable bowel syndrome with a food elimination diet followed by food challenge and probiotics. J. Am. Coll. Nutr. 2006, 25, 514–522. [Google Scholar] [CrossRef]
- Atkinson, W.; Sheldon, T.A.; Shaath, N.; Whorwell, P.J. Food elimination based on IgG antibodies in irritable bowel syndrome: A randomised controlled trial. Gut 2004, 53, 1459–1464. [Google Scholar] [CrossRef]
- Singh, P.; Silvester, J.; Chen, X.; Xu, H.; Sawhney, V.; Rangan, V.; Iturrino, J.; Nee, J.; Duerksen, D.R.; Lembo, A. Serum zonulin is elevated in, I.B.S.; correlates with stool frequency in, I.B.S.-D. United Eur. Gastroenterol. J. 2019, 7, 709–715. [Google Scholar] [CrossRef]
- Caviglia, G.P.; Rosso, C.; Ribaldone, D.G.; Dughera, F.; Fagoonee, S.; Astegiano, M.; Pellicano, R. Physiopathology of intestinal barrier and the role of zonulin. Minerva Biotecnol. 2019, 31, 83–92. [Google Scholar] [CrossRef]
- Barbaro, M.R.; Cremon, C.; Caio, G.; de Giorgio, R.; Volta, U.; Stanghellini, V.; Barbara, G. 247 Zonulin serum levels are increased in non-celiac gluten sensitivity and irritable bowel syndrome with diarrhea. Gastroenterology 2015, 148, S56. [Google Scholar] [CrossRef]
- Prospero, L.; Riezzo, G.; Linsalata, M.; Orlando, A.; D’Attoma, B.; Russo, F. Psychological and Gastrointestinal Symptoms of Patients with Irritable Bowel Syndrome Undergoing a Low-FODMAP Diet: The Role of the Intestinal Barrier. Nutrients 2021, 13, 2469. [Google Scholar] [CrossRef]
- Tripathi, A.; Lammers, K.M.; Goldblum, S.; Shea-Donohue, T.; Netzel-Arnett, S.; Buzza, M.S.; Antalis, T.M.; Vogel, S.N.; Zhao, A.; Yang, S.; et al. Identification of human zonulin, a physiological modulator of tight junctions, as prehaptoglobin-2. Proc. Natl. Acad. Sci. USA 2009, 106, 16799–16804. [Google Scholar] [CrossRef]
- Koch, W.; Latz, W.; Eichinger, M.; Gschwendner, C.; Teige, B.; Schomig, A.; Kastrati, A. Haptoglobin gene subtyping by restriction enzyme analysis. Clin. Chem. 2003, 49, 1937–1940. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Meira de-Faria, F.; Bednarska, O.; Ström, M.; Söderholm, J.D.; Walter, S.A.; Keita, Å.V. Colonic paracellular permeability and circulating zonulin-related proteins. Scand. J. Gastroenterol. 2021, 56, 424–431. [Google Scholar] [CrossRef] [PubMed]
- Scheffler, L.; Crane, A.; Heyne, H.; Tönjes, A.; Schleinitz, D.; Ihling, C.H.; Stumvoll, M.; Freire, R.; Fiorentino, M.; Fasano, A.; et al. Widely used commercial ELISA does not detect precursor of haptoglobin2, but recognizes properdin as a potential second member of the zonulin family. Front. Endocrinol. 2018, 9, 22. [Google Scholar] [CrossRef] [PubMed]
- Ajamian, M.; Steer, D.; Rosella, G.; Gibson, P.R. Serum zonulin as a marker of intestinal mucosal barrier function: May not be what it seems. PLoS ONE 2019, 14, e0210728. [Google Scholar] [CrossRef]
- Talley, N.J.; Holtmann, G.J.; Jones, M.; Koloski, N.A.; Walker, M.M.; Burns, G.; Potter, M.D.E.; Shah, A.; Keely, S. Zonulin in serum as a biomarker fails to identify the IBS, functional dyspepsia and non-coeliac wheat sensitivity. Gut 2020, 69, 1719–1722. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peruhova, M.; Mihova, A.; Altankova, I.; Velikova, T. Specific Immunoglobulin E and G to Common Food Antigens and Increased Serum Zonulin in IBS Patients: A Single-Center Bulgarian Study. Antibodies 2022, 11, 23. https://doi.org/10.3390/antib11020023
Peruhova M, Mihova A, Altankova I, Velikova T. Specific Immunoglobulin E and G to Common Food Antigens and Increased Serum Zonulin in IBS Patients: A Single-Center Bulgarian Study. Antibodies. 2022; 11(2):23. https://doi.org/10.3390/antib11020023
Chicago/Turabian StylePeruhova, Milena, Antoaneta Mihova, Iskra Altankova, and Tsvetelina Velikova. 2022. "Specific Immunoglobulin E and G to Common Food Antigens and Increased Serum Zonulin in IBS Patients: A Single-Center Bulgarian Study" Antibodies 11, no. 2: 23. https://doi.org/10.3390/antib11020023
APA StylePeruhova, M., Mihova, A., Altankova, I., & Velikova, T. (2022). Specific Immunoglobulin E and G to Common Food Antigens and Increased Serum Zonulin in IBS Patients: A Single-Center Bulgarian Study. Antibodies, 11(2), 23. https://doi.org/10.3390/antib11020023