Abstract
This study investigated the association between black carbon (BC) exposure and hospital admissions (HAs) and outpatient department/emergency room (OPD/ER) visits for cardiovascular diseases (CVD) among residents of Karachi, the largest city in Pakistan. We measured daily concentrations of BC in fine particulate matter (PM2.5) and collected records of HAs and OPD/ER visits for CVD from 2 major tertiary care hospitals serving Karachi for 6 weeks continuously during each quarter over 1 year (August 2008–August 2009). We subsequently analyzed daily counts of hospital and BC data over 0–3 lag days. Daily mean BC concentrations varied from 1 to 32 µg/m3. Results suggest that BC concentrations are associated with CVD HAs and OPD/ER visits. However, associations were generally only observed when modeled with BC from Tibet Center, the commercial-residential site, as compared to Korangi, the industrial-residential site. Overall, low statistical significance suggests that while BC may be a valuable indicator for CVD health risks from combustion-derived particles, further evaluation of the constituents of PM2.5 and their relative contributions to CVD health impacts is necessary.
1. Introduction
The unprecedented growth of urban areas worldwide is contributing to new and challenging threats to public health and the environment. Cities that are experiencing unregulated growth struggle to provide reliable and environmentally preferable transportation systems that their economies and inhabitants can rely upon. In turn, concurrent increases in population and vehicular traffic have given rise to dangerous levels of ambient air pollutants [1]. These issues are compounded by industrial activity, energy use, inadequate infrastructure and the absence of environmental regulation, and add to existing concerns about air quality and climate change [2]. Each year, one in every nine deaths worldwide are attributed to air pollution, with 4.3 million deaths linked to indoor air pollution and 3 million to outdoor air pollution. Consequently, air pollution has become the single largest environmental health risk factor worldwide [3,4].
Combustion of fossil fuels and biomass are significant sources of energy worldwide, and emit substantial quantities of ambient particulate pollution [1,2]. Fine particulate mass (airborne particulate matter with aerodynamic diameter <2.5 micrometers; (PM2.5)) has traditionally been employed in ecological study designs to estimate the health effects of ambient air pollution in a wide geographical area. However, a growing body of evidence has shifted attention toward evaluating the health effects of PM2.5 constituents individually or in combination with one another, which may pose a greater risk to health [5,6,7]. Black carbon (BC), often a significant constituent of PM2.5, is produced by the incomplete combustion of carbonaceous-fuels (e.g., fossil fuels and biomass) [8,9]. There are many important sources of BC pollution including, but not limited to, vehicles, heating and power generation, cooking stoves, forest fires, and burning of biomass and garbage. Sources of BC vary by region and sector, with Asia contributing approximately 40% of global BC emissions [10], and developing countries overall contributing more than 75% of global BC emissions [11]. In East Asia, transport and industrial use of coal are significant emitting sectors [10]. In addition to adversely impacting health, BC is the most strongly light-absorbing constituent of PM2.5 and has a warming effect on the climate that is substantially greater than that of carbon dioxide. BC deposited on ice and snow causes both atmospheric warming and an increase in melting rate. Additionally, BC influences cloud formation, regional circulation, and rainfall patterns [9].
Recent literature has demonstrated a relationship between BC from various sources and a variety of adverse cardiopulmonary health effects and premature mortality, as well as potentially adverse birth outcomes and neurodevelopmental effects in children [12,13,14]. Additionally, Janssen et al. [13,14] concluded that BC is associated with adverse cardiopulmonary health impacts that yield higher effect estimates per unit of mass concentration (µg/m3) compared with particulate mass, and that BC may represent a valuable proxy for assessing the health impacts of combustion-derived ambient air pollution. Most of the existing studies of BC and health have been carried out in Europe and North America. However, the burden of cardiovascular (CVD) mortality is higher in low- and middle-income countries [15], where only a limited number of studies have been conducted to examine the relationships between ambient air pollution and adverse CVD health outcomes [14,16]. An even smaller fraction of studies have examined associations between ambient air pollution and adverse CVD health outcomes in developing nations of southeast Asia [17], where approximately one quarter of the global ambient air pollution-related deaths occur [3].
Presently, there is a knowledge gap regarding the extent of these impacts in urban centers in southeast Asian countries. In our previous study, we measured PM2.5 at two sites in Karachi, and performed time-series analyses which showed evidence of positive associations between ambient PM2.5 and CVD in Karachi [18]. Elsewhere we also evaluated the distribution of PM2.5 constituents in Karachi and their temporal trends, as well as their association with CVD morbidity [19]. The present study is based on a previously published Master’s thesis [20], and is the first study to examine the short-term associations between ambient BC and CVD among individuals residing within a Pakistani megacity. This study is among the few to report on the growing concern over consequences for health of combustion-derived particulate pollution.
2. Materials and Methods
2.1. Study Site
Situated along the Arabian Sea, Karachi is the largest city (area = 3527 km2) in Pakistan. Karachi’s estimated population of 20 million inhabit 5 five densely populated sub-districts, which are comprised of 18 towns. Karachi is considered a premier hub for economic activity, including industrial, manufacturing, and trade activities. Karachi’s climate is subtropical, with distinct fall (October–December), winter (January–March), spring (April–June), and summer (July–September) seasons. Annual average rainfall is approximately 170 mm, and annual mean temperature is 30 °C. Monsoon seasons bring strong west and southwesterly airflows of marine air, whereas during winter months the wind direction is predominately east and north-east.
2.2.Outcome Definition and Measurement
During the period of August 2008 to August 2009, we recorded daily visits of all CVD patients visiting an outpatient department (OPD), emergency room (ER), and/or admitted to the hospital (HA) from two major hospitals in Karachi: Aga Khan University (AKU) and National Institute of Cardiovascular Diseases (NICVD). These are the two major hospitals in the city to which patients with serious CVD would come. AKU is a private hospital likely to receive higher income patients, whereas NICVD is a specialized major tertiary care public hospital which provides CVD care to patients of all socioeconomic strata. According to NICVD, their outpatient department provides care to approximately 500,000 patients per year and their emergency department which is accessible 24 h a day, 7 days a week, receives and provides care to an average of 600 patients per day [21]. We collected patient information on age, gender, town of residence, date of visitation, and diagnosis code(s). Principal diagnosis (provisional or final) was recorded from the registers and later were coded according to ICD classification by our trained physicians at NICVD. At AKU, data was extracted from an established hospital information management system and then coded according to ICD classification. Most outpatients had a provisional diagnosis while most admitted patients had a final diagnosis, as recorded by physicians. The study was approved by Ethical Review Committees of hospital and the Institutional Review Boards of the New York State Department of Health, University at Albany and Aga Khan University (IRB#09-063, IRB# 07-252, and 833-CHS/ERC-07).
2.3. Air Sample Collection and Data Acquisition
We collected air samples at two sites in Karachi, Pakistan. The Korangi site is a residential area mixed with various types of heavy and light industries, including oil refineries, textile, chemical, and tanneries. Whereas, Saddar town (Tibet Center) is a commercial-residential site which does not have such industries. Daily (24 h) ambient air samples for PM2.5 were collected at both sites continuously for 6 weeks during each quarter of the year between 2008 and 2009. The sampler was comprised of a pre-weighted polytetrafluoroethylene (PTFE) filter and a pump operated at 16.7 L/min. The filters were weighted with a microbalance (ATI CAHN, Model C-44) in a clean room. PM2.5 concentrations were calculated by using the weight difference and the recorded air volume. We used a non-destructive dual-wavelength optical transmissometer (Model OT-21, 2007) to analyze black carbon at wavelengths of 370 and 880 nm. We applied correction factors (k) for the effect of loading on filters [22], (k = 0.0002 for 880-nm channel and k = 0.0037 for 370-nm channel, respectively), which were based on aethalometer measurements conducted in Karachi during a 2-month period in 2006 [23]. More information on PM2.5 collection and BC determination for this study are available elsewhere [18,20]. Daily mean temperature, humidity and weather conditions of Karachi was obtained from the Weather Underground (www.wunderground.com). We maintained a strict quality assurance and control plan throughout the study [18].
2.4. Statistical Analysis
We conducted time-series analyses (in SAS 9.2-SAS Institute Inc., Cary, NC, USA), to determine Relative Risks (RR) of association between exposure to daily mean BC and OPD/ER visit or HA for CVD. Analyses were stratified by the sampling sites, and were conducted to assess the influence of age groups, gender, and season. Three age groups were selected for comparison (0–40, 41–60, and >60 years). We also performed a separate analysis to evaluate the effect of the patient’s location of residency on association between BC and CVD outcomes. For this analysis, each patient was assigned the BC level measured at the site nearest to their town of residence (e.g., when town code = 08, 09, 12, 17, exposure level equals BC measured at Korangi site). Samples with a reported measurement error (i.e., power failure or pump malfunction) were excluded. Missing mean daily BC data were identified and we estimated a measure for the statistical analyses by calculating an average of the measurements of the day before and after the missing value. Data were over dispersed, therefore we applied a negative binomial generalized linear regression and assessed for goodness of fit of the model using Pearson residuals and deviance. We calculated mean, standard deviation, minimum, maximum, and percentiles for BC. We adjusted for temporal trends (day of week, holidays, season, cubic splines of study day with knots at the first sampling of each month), and meteorological variables (cubic splines of average temperature and relative humidity). Estimates were analyzed for lag time of 0-, 1-, 2-, and 3-days between BC exposure and OPD/ER visits or HA for CVD.
3. Results and Discussion
3.1. Overview
Table 1 presents summary statistics of daily cardiovascular admissions and OPD/ER visits, concentrations of BC, and meteorological variables during the study period. During the study period 24,124 patients visited an OPD or ER (68.6%) and 11,023 (31.4%) were admitted to a hospital due to CVDs. Overall, there were more male hospitalizations than female, and female ER visits were higher than for males. More information on types of CVD observed is detailed in Khwaja et al. [18]. Mean BC concentrations monitored at Korangi (4.75 µg/m3) were higher compared to Tibet Center (2.53 µg/m3). The minimum mean temperature was 17.2°C and maximum was 35.6 °C, with an annual mean of 27.8 °C. The relative humidity had greater seasonal variation: annual mean relative humidity was 62.99% with a minimum of 24.0% and maximum of 90.0%.

Table 1.
Summary statistics of daily cardiovascular admissions and OPD/ER visits, concentration of BC, and meteorological variables in Karachi, Pakistan during the study.
3.2. Daily Mean Black Carbon Concentrations
The samples obtained at the two sites were dramatically different in color, ranging from predominately dark black a Tibet Center to light grey or brown at Korangi. Visual differences in sample color observed in other studies are believed to represent local variation in PM sources. For example, combustion of biomass and lignite may emit organic aerosols that appear brown or yellowish in color, which is due in part to their light absorbing properties [8,24]. Lu et al. [19] addresses the significant local variation in PM constituents observed at both sites.
At Tibet Center, higher daily mean BC concentrations (Figure 1) were observed during the winter (3.39 µg/m3) and summer (3.26 µg/m3). Increased wintertime emissions from heating sources and combustion of biomass in addition to low boundary layer heights may have contributed to high concentrations of BC at Tibet Center. These observations are consistent with several other studies examining BC concentrations in Karachi [23,25]. In contrast, these studies also observed better dispersion of pollutants because of increased boundary layer heights and enriched wet deposition during summer monsoon rainfall [26,27,28].
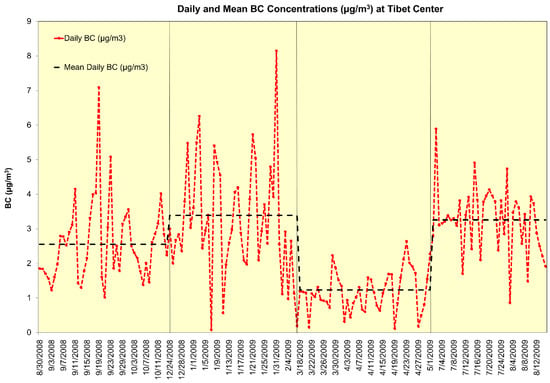
Figure 1.
Daily and mean BC concentrations (µg/m3) at Tibet Center during the study period.
At the Korangi site, concentrations of BC were higher than at the Tibet Center. We also observed a seasonal variation in daily mean BC concentrations. However, unlike those at Tibet Center, BC concentrations at Korangi (Figure 2) were highest in the summer (8.87 µg/m3) and spring (5.65 µg/m3), and lowest in the winter (2.96 µg/m3) and fall (2.69 µg/m3). The maximum BC concentration measured was 31.7 µg/m3 at Korangi site in summer. Karachi experienced several city-wide power outages during the study period, which predominantly occurred during the summer months. Sharp increases in BC concentrations at Korangi during summer may be attributed to the use of industrial power generators to support the many industries and plants during the outages.
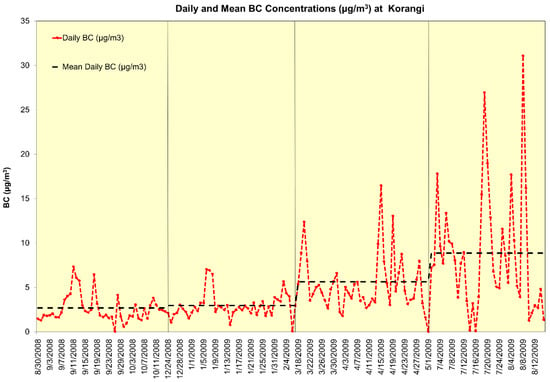
Figure 2.
Daily and mean BC concentrations (µg/m3) at Korangi during the study period.
Other studies have examined the significance of anthropogenic emissions on BC concentrations in Karachi. Dutkiewicz et al. [23] measured daily mean BC concentrations in Karachi that ranged from 1 to 15 µg/m3, with occasional short-term levels up to 40 µg/m3 that primarily occurred during morning and evening rush-hour periods. A strong impact from morning vehicular traffic was observed; however, this effect was strongly modified by meteorological conditions. Throughout the study period, BC emissions were highest during business hours and when traffic flow was at its greatest intensity. Bibi et al. [25] similarly observed high BC morning peaks, which they attributed to anthropogenic activities such as traffic and industrial activities.
3.3. Cardiovascular Health Effects of Ambient Black Carbon Pollution
This is the first study to evaluate short term associations between BC and CVD in Pakistan. The limited availability of such information and the need for improved understanding of these associations was underscored in a recent systematic review [17] of existing studies conducted in South Asian developing countries. Out of nine studies meeting the inclusion criteria for the review, only one study was conducted in Pakistan. In this cross-sectional study, Sughis et al. [29] examined associations between outdoor and indoor air pollution and blood pressure among school children in Lahore, Pakistan, finding evidence of significantly higher blood pressure among children living in highly polluted areas of the city [29].
Table 2 presents estimates of the relative risk (RR) and 95% confidence intervals for a 1 µg/m3 increase in BC from Tibet Center and Korangi for all patients by gender and age group for HAs and OPD/ER visits on lag days 0, 1, 2, and 3. We observed positive associations between BC collected at Tibet Center and HAs and OPD/ER visits, although most did not reach statistical significance. In general, RR estimates were greater among OPD/ER visits in all age groups than for Has. We observed the highest RR for all OPD/ER visits associated with single day lag (RR = 1.026; 95% CI, 0.992, 1.060). We observed little association between BC from Korangi and CVD outcomes except for a few positive RRs for hospitalizations of patients ages 0–40 and greater than 60 years (lags 1 and 3) and OPD/ER visits of male patients in the 0–40 and 41–60 age groups (lag 1). However, we observed a statistically significant protective effect for visits to an OPD/ER associated with lag 2 BC concentrations in Korangi.
Table 2.
Relative risk estimates (95% Confidence Intervals) by lag day (0 to 3) for all daily hospital admissions and cardiovascular outpatient department/emergency room visits by gender and age group associated with a 1 µg/m3 increase of BC in Karachi during the study period.
We observed a slightly increased risk of CVD visits due to BC exposure from Tibet Center among all age groups, but these risks failed to reach statistical significance. RRs were higher for OPD/ERs patients, with the greatest risk among patients 41–60 years of age and lag 1 BC (RR = 1.042; 95% CI, 0.986, 1.102). This age group comprises a substantial proportion of the working class in Pakistan [30]. Among patients 0–40 years of age, elevated risk of hospitalization and OPD/ER visits were associated with lag 1 and lag 0 BC concentrations from Tibet Center, respectively. Similarly, for lag 0 and lag 1 BC concentrations from Tibet Center we observed slightly increased risks of hospitalization and OPD/ER visits among patients greater than 60 years of age, respectively. Female patients were at greater risk of visiting an OPD/ER and female hospitalizations and OPD/ER visits were more strongly associated with lag 1 BC from Tibet Center. Among males, we observed the strongest association between lag 0 BC at Tibet and HAs and OPD/ER visits. We observed the greatest elevation in risk of OPD/ER visits among females associated with lag 1 BC at Tibet Center (RR = 1.037; 95% CI, 0.984, 1.092), while the highest risk for males occurred at lag 0 BC, (RR = 1.017; 95% CI, 0.998, 1.059).
Overall, effect estimates were greater for BC concentrations measured at Tibet Center compared with those for BC from Korangi and those for PM2.5 from both sites [18]. While none were statistically significant, they may indicate a slightly increased risk of CVD associated with BC or suggest that BC is a potentially important indicator of risk for combustion-derived ambient air pollution. Risk was greater for OPD/ER visits than HAs, with the greatest magnitude observed for single day lag BC. Patients above 40 years of age were at greatest risk. BC concentration increased the risk of HAs for patients 60 years and older at both sites; however, risk of OPD/ER visits were greater patients among 40 and 60 years old. Females had a greater risk than males of visiting an OPD/ER. Female HAs and OPD/ER visits were more strongly associated with lag 1 BC from Tibet Center, compared with males who had the strongest association with lag 0 BC at Tibet. We saw the greatest elevation in risk of OPD/ER visits among females associated with lag 1 BC at Tibet Center. These observations may be explained by the influence of gender norms and gender-specific risk factors for CVD in Karachi. Females comprise a fraction (30%) of the workforce in Pakistan, and generally spend the majority of the day at home performing household duties on behalf of their extended family. Gender norms often prevent women from seeking healthcare unless life-threatening [31,32]. Jafar et al. (2008) found 20% of a population of adults 40 years of age or older in Karachi may have underlying coronary artery disease (CAD), and observed higher risk among women than men as a result of a greater prevalence of risk factors (e.g., diabetes, hypertension, obesity) [33]. Although residential biomass fuel use is less common in Karachi than in rural areas of Pakistan, urban households still depend on biomass fuels. Combustion of these fuels along with other sources contribute to significant quantities of indoor air pollution, which women and children are disproportionately exposed to [34]. While these may help to explain the observed elevation of risk OPD/ER visits among females in our study, data remains limited regarding female’s exposures, the influence of gender norms, and other risk factors for CVD. With respect to men in Karachi, Khan et al. (2007) documented a tendency among subjects (78% male) at NICVD experiencing Acute Myocardial Infarction to delay seeking medical attention. Delayed presentation was often a result of unwillingness to admit to experiencing a health issue and lack of subject’s knowledge of signs and symptoms [35]. Furthermore, a dearth ambulatory transport and its high cost has also been shown to affect presentation in Karachi and elsewhere in Pakistan [35,36] These observed behaviors and limited awareness which affect presentation may potentially suggest that our results are underestimating risk particularly among males.
We separately evaluated the effect of the patient’s location of residency (i.e., town code) on associations between levels of BC and CVD outcomes. A total of 31,749 patients were successfully matched to BC levels according to their town codes, with 9572 patients assigned BC measurements from Korangi and 22,177 patients assigned BC measures from Tibet Center. Those with missing town code values were excluded. Table 3 presents estimates of the relative risk (RR) and 95% confidence intervals for a 1 µg/m3 increase in BC from Tibet Center and Korangi for all patients for HAs and OPD/ER visits on lag days 0, 1, 2, and 3, and adjusted by town of residence closest to the BC monitoring site. Among patients residing near the Korangi site, we observed positive associations between BC and HAs up to 3 lag days, with the greatest elevation of risk on lag day 1 (RR = 1.0197; 95% CI, 0.9755, 1.0659). We observed no association between Korangi BC and OPD/ER visits. Among patients residing near Tibet Center, we observed positive associations with both HAs and OPD/ER visits up to 2 and 3 lag days, respectively. We observed a significant positive association between second day lag BC from Tibet Center and HAs (RR = 1.0226; 95% CI, 1.0008, 1.0448). We similarly observed positive associations between increasing levels of BC and CVD outcomes in both analyses. However, after adjusting for town of residence, we observed stronger associations between BC from Korangi and CVD outcomes. This may suggest that neighborhood and community BC exposures are more important than city-wide exposures. BC is understood to significantly vary locally as a result of mobile sources [9]. In a developing megacity such as Karachi, there are countless BC emission sources which may contribute to a spatially heterogeneous BC exposure risk. Greater spatial resolution of BC concentrations and more information on social and behavioral factors are needed to understand the likelihood and frequency of BC exposure. Furthermore, information is also needed on the relative contributions to BC exposure of residential, neighborhood, community or city-wide emissions. Overall, there appeared to be greater elevation of risk among patients residing near Tibet Center, likely a result of significant motor-vehicle traffic.
Table 3.
Adjusted relative risk estimates (95% CI) by lag day (0 to 3) for all daily hospital admissions and cardiovascular outpatient department/emergency room visits associated with a 1 µg/m3 increase of BC in Karachi during the study period. All patients were assigned exposure based on the monitoring site closest to their town code.
Other studies examining short-term associations between ambient BC concentrations and CVD health impacts have observed similar associations. Janssen et al. [13,14] evaluated the epidemiological and toxicological literature and concluded that BC is associated with adverse cardiopulmonary health impacts that yield higher effect estimates per unit of mass concentration (µg/m3) compared with particulate mass. Magalhaes et al. [37] performed a review of the epidemiological evidence regarding impacts of exposure to BC on blood pressure, finding that existing evidence supports a positive association among adults. In addition, Grahame et al. [12] conducted a review of the literature regarding health effects of BC and concluded that there is a causal relationship between BC and various CVD mortality and morbidity endpoints. Finally, a literature review performed by Li et al. [38], of existing epidemiological studies of the health effects of both PM2.5 mass and BC, demonstrated that BC may be more harmful than PM2.5 mass as well as its constituents. However, the ability to differentiate the health effects of various constituents of PM2.5 remains a limitation.
Li et al. [38] simulated annual average BC concentrations for the year 2010 from anthropogenic sources across the continental United States. The maximum simulated BC value in the continental United States was 3.0 µg/m3 and the mean was 0.3 µg/m3. These concentrations are much lower than our observed BC concentrations in Karachi. Li et al. [38] used a risk estimate for all-cause mortality associated with PM2.5 from Krewski et al. [39], and estimated that 13,910 (95% CI: 9419–18,391) deaths in the United States resulted from anthropogenic BC emissions in 2010 [39]. Furthermore, they performed a sensitivity analysis of the national BC related mortality using a BC-specific risk estimate from Janssen et al. [13], which yielded an estimated 133,807 (95% CI: 92,259–174,523) BC-related deaths in the United States. Karachi has among the highest levels of ambient air pollution worldwide, which is conservatively estimated to contribute to an excess of approximately 15,000 deaths each year. Of these excess deaths, it is estimated that approximately 5200 are due to cardiovascular mortality [40,41]. Dutkiewicz et al. [23] estimated daily emissions in Karachi varied from 14,000 to 22,000 kg of BC per day, totaling 6.7 kilometric tons per year and 17.5 kilometric tons per year for the greater metropolitan area. Considering the greater concentrations of BC observed in Karachi, compared with those in cities in the developed world, research should continue to evaluate the disproportionate adverse health effects of BC in developing countries.
We observed elevated but mostly not statistically significant effects of BC on CVD in Karachi, with a stronger relationship between BC collected at a commercial/residential site (Tibet Center) with substantial vehicular traffic compared to an industrial/residential site (Korangi). Existing evidence supports that aerosols derived from combustion, and in particular traffic-related air pollution, may be more harmful to human health compared to other particulate air pollutants [42]. Several studies have identified vehicular traffic as one of the principal sources of atmospheric pollution in Karachi. Dutkiewicz et al. [23] observed a BC concentration pattern in Karachi that was indicative of strong vehicular emissions, with the highest emissions during business hours when traffic flow is highest. It is estimated that the number of registered vehicles on the road in Karachi may exceed 2.21 million [43]. Tibet Center is located in the center of Karachi, and experiences significant motor vehicle traffic. Approximately 300,000 vehicles pass through Tibet Center each day [44]. In a separate study, we evaluated the relative contributions of different sources to PM2.5 mass, and concluded that particles from the vehicular exhaust and industrial combustion were likely to be major contributors to the health burdens due to CVD in Karachi [19]. Our findings suggest that vehicular traffic contributes significantly to BC concentrations at Tibet Center and in turn greatly impacts CVD in Karachi. The complex
3.4. Strengths and Limitations
This study is the first to evaluate the CVD health effects associated with ambient BC concentrations in Pakistan. Our study has many strengths as well as some limitations. We collected health data from the largest public hospital for CVD in Pakistan in addition to another general hospital. We implemented a rigorous study design and methodology, including ascertainment of quality hospital data. The results were also consistent with other studies conducted in developed countries. Nonetheless a few limitations must be considered while interpreting the results. First, air pollutant concentrations were measured at fixed sites and served as a proxy for the personal exposure. As is the case in many ecological study designs, the validity of the exposure assumption is impacted by several mediating factors that were not measured in this study: Indoor and outdoor emission sources, indoor exposures, variation of time spent indoors and outdoors, life style and smoking habits of the individual patient and other household members (second hand smoke). We did not test a multipollutant model, and therefore we were unable to characterize the relative contribution of other constituents of PM2.5 to CVD risk. Additionally, while we did evaluate single day lags from 0–3 days we did not evaluate cumulative lags. Moreover, miscoding and diagnosis of CVD events may have potentially occurred randomly and consequently reduced the observed magnitude of risk. To overcome this limitation and diminish misclassification of CVD outcomes, we used only primary diagnosis. We collected information from the two hospitals only, therefore those patients who did not seek treatment or died at home were not captured by our study. Those who came to hospitals may be considered more severe cases and therefore the measured effect estimates may be an underestimate of the actual risk. This study did not evaluate the prospective development of disease nor did we collect information on patient’s medical histories, rather we focused on the accentuation of existing CVD. Although likely negligible, we could not differentiate between multiple hospitalizations for one patient from single hospitalizations for several patients, and whether a patient visiting an OPD/ER became admitted to a hospital.
4. Conclusions
Our findings compliment those of previous studies, and further demonstrate the potential importance of vehicular traffic, industrial activity, acute power shortages, and open burning of garbage to the significant concentrations of ambient BC in Karachi. Compared with our previous evaluation of the short-term effects of PM2.5, the elevated effect estimates per 1 µg/m3 for BC that we observed in this study were substantially greater [18]. Effect estimates were also generally much higher for BC collected at Tibet Center than at Korangi. We observed an elevation of risk for females, compared with males, potentially indicating their enhanced sensitivity and/or greater exposure to BC. The greatest number of patients were between the ages of 41–60 and were also at greatest risk of an OPD/ER visit per 1 µg/m3 for BC. This age group comprises a substantial proportion of the working class in Pakistan. However, individuals >60 were at greater risk of hospitalization per 1 µg/m3 for BC. Overall, low statistical significance suggests that while BC may be a valuable indicator for CVD health risks from combustion-derived particles, further evaluation of the constituents of PM2.5 and their relative contributions to CVD health impacts is necessary. Nevertheless, our results suggest that combustion-derived particulate matter, likely from vehicular traffic, at the commercial-residential Tibet Center site potentially pose threats to CVD health in Karachi.
Author Contributions
(1) D.M. carried out all aspects of data management and analysis, interpretation of results, and prepared drafts of the manuscript. (2) H.A.K. assisted in designing the study, facilitating data acquisition, and preparation, refinement, and presentation of the results in the manuscript. (3) Z.F. coordinated the acquisition of patient data and provided expertise on the interpretation of results regarding hospital data. (4) A.S. and a team of trained graduate students from the University of Karachi, collected air pollution samples. (5,6) S.L. and Y.L. assisted in epidemiological analysis of the data. (7) Finally, D.C. assisted in the design of the study design, facilitation of data acquisition, interpretation of study results, and presentation of findings.
Funding
This work was supported by the Pakistan-US Science and Technology Cooperative Program (administered by National Academy of Sciences US and Higher Education Commission, Pakistan) under the grant # PGA-7251-07-010 to David O. Carpenter and Zafar Fatmi.
Acknowledgments
The authors would like to thank Wadsworth Center, New York State Department of Health, University at Albany, Higher Education Commission, Pakistan, Aga Khan University Hospital, and NICVD, University of Karachi and the physicians who provided and collected the health data used in this study. We owe a debt of gratitude to Kelly Robbins, Vincent Dutkiewicz, Amber Sinclair, Aneeta Khoso, Sumayya Saied, Naseem Parvez Ali, Jahan Zeb and Kamran Khan who assisted in all aspects of this work. We also extend our thanks to Kim McClive-Reed for editing the manuscript.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Molina, M.J.; Molina, L.T. Megacities and atmospheric pollution. J. Air Waste Manag. Assoc. 2004, 54, 644–680. [Google Scholar] [CrossRef] [PubMed]
- Baklanov, A.; Molina, L.T.; Gauss, M. Mesgacities, air quality and climate. Atmos. Environ. 2016, 126, 235–249. [Google Scholar] [CrossRef]
- WHO. Ambient Air Pollution: A Global Assessment of Exposure and Burden of Disease; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- WHO. Preventing Disease through Healthy Environments: A Global Assessment of the Burden of Disease from Environmental Risks; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Lippmann, M. Toxicological and epidemiological studies of cardiovascular effects of ambient air fine particulate matter (PM2.5) and its chemical components: Coherence and public health implications. Crit. Rev. Toxicol. 2014, 44, 299–347. [Google Scholar] [CrossRef] [PubMed]
- Rohr, A.C.; Wyzga, R.E. Attributing health effects to individual particulate matter constituents. Atmos. Environ. 2012, 62, 130–152. [Google Scholar] [CrossRef]
- Stanek, L.W.; Sacks, J.D.; Dutton, S.J.; Dubois, J.J.B. Attributing health effects to apportioned components and sources of particulate matter: An evaluation of collective results. Atmos. Environ. 2011, 45, 5655–5663. [Google Scholar] [CrossRef]
- Andreae, M.O.; Gelencsér, A. Black carbon or brown carbon? The nature of light-absorbing carbonaceous aerosols. Atmos. Chem. Phys. 2006, 6, 3131–3148. [Google Scholar] [CrossRef]
- Bond, T.C.; Doherty, S.J.; Fahey, D.W. Bounding the role of black carbon in the climate system: A scientific assessment. J. Geophys. Res. Atmos. 2013, 118, 5380–5552. [Google Scholar] [CrossRef]
- Lamarque, J.F.; Bond, T.C.; Eyring, V. Historical (1850–2000) gridded anthropogenic and biomass burning emissions of reactive gases and aerosols: Methodology and application. Atmos. Chem. Phys. 2010, 10, 7017–7039. [Google Scholar] [CrossRef]
- Schmidt, C.W. Black Carbon: The Dark Horse of Climate Change Drivers. Environ. Health. Perspect. 2011, 119, A172–A175. [Google Scholar] [CrossRef] [PubMed]
- Grahame, T.J.; Klemm, R.; Schlesinger, R.B. Public health and components of particulate matter: The changing assessment of black carbon. J. Air Waste Manag. Assoc. 2014, 64, 620–660. [Google Scholar] [CrossRef] [PubMed]
- Janssen, N.H.; Hoek, G.; Simic, L.M. Black Carbon as an Additional Indicator of the Adverse Health Effects of Airborne Particles Compared with PM(10) and PM(2.5). Environ. Health Perspect. 2011, 119, 1691–1699. [Google Scholar] [CrossRef] [PubMed]
- Janssen, N.H.; Janssen, N.; Gerlofs, N.M. Health Effects of Black Carbon; World Health Organization: Copenhagen, Denmak, 2012. [Google Scholar]
- Alwan, A. Global Status Report on Noncommunicable Diseases 2010; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Chen, R.; Chu, C.; Tan, J. Ambient air pollution and hospital admission in Shanghai, China. J. Hazard. Mater. 2010, 181, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.S.; Phalkey, R.; Malik, A.A. A systematic review of air pollution as a risk factor for cardiovascular disease in South Asia: Limited evidence from India and Pakistan. Int. J. Hyg. Environ. Health 2014, 217, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Khwaja, H.; Fatmi, Z.; Malashock, D. Effect of air pollution on daily morbidity in Karachi, Pakistan. J. Local Glob. Health Sci. 2012, 217, 1–13. [Google Scholar] [CrossRef]
- Lu, Y.; Lin, S.; Fatmi, Z. Assessing the association between fine particulate matter (PM2.5) constituents and cardiovascular diseases in a mega-city of Pakistan. Environ. Health Perspect. 2018. [Google Scholar]
- Malashock, D. Short-Term Associations between PM2.5, Black Carbon, Delta-C, and Cardiovascular Diseases in a Large Developing Megacity. Master’s Thesis, State University of New York, New York, NY, USA, 2012. [Google Scholar]
- NICVD. Our Services: Out-Patients and Emergency. Available online: http://nicvd.org/ (accessed on 5 October 2018).
- Wang, Y.; Hopke, P.K.; Rattigan, O.V.; Xia, X.; Chalupa, D.C.; Utell, M.J. Characterization of Residential Wood Combustion Particles Using the Two-Wavelength Aethalometer. Environ. Sci. Technol. 2011, 45, 7387–7393. [Google Scholar] [CrossRef] [PubMed]
- Dutkiewicz, V.; Alvi, S.; Ghauri, B.M.; Choudhary, M.; Husain, L. Black carbon aerosols in urban air in South Asia. Atmos. Environ. 2009, 43, 1737–1744. [Google Scholar] [CrossRef]
- Kirchstetter, T.W.; Novakov, T.; Hobbs, P.V. Evidence that the spectral dependence of light absorption by aerosols is affected by organic carbon. J. Geophys. Res. 2004, 109, D21208. [Google Scholar] [CrossRef]
- Bibi, S.; Alam, K.; Chishtie, F.; Bibi, H.; Rahman, S. Temporal variation of Black Carbon concentration using Aethalometer observations and its relationships with meteorological variables in Karachi, Pakistan. J. Atmos. Sol. Terr. Phys. 2017, 157–158, 67–77. [Google Scholar] [CrossRef]
- Li, K.; Liao, H.; Mao, Y.; Ridley, D.A. Source sector and region contributions to concentration and direct radiative forcing of black carbon in China. Atmos. Environ. 2016, 124, 351–366. [Google Scholar] [CrossRef]
- Lu, Z.; Zhang, Q.; Streets, D.G. Sulfur dioxide and primary carbonaceous aerosol emissions in China and India; 1996–2010. Atmos. Chem. Phys. 2011, 11, 9840–9864. [Google Scholar] [CrossRef]
- Zhang, L.; Liao, H.; Li, J. Impacts of Asian summer monsoon on seasonal and interannual variations of aerosols over eastern China. J. Geophys. Res. 2010, 115. [Google Scholar] [CrossRef]
- Sughis, M.; Nawrot, T.S.; Ihsan, H.S.; Amjad, A.; Nemery, B. Blood pressure and particulate air pollution in schoolchildren of Lahore, Pakistan. BMC Public Health 2012, 12, 378–386. [Google Scholar] [CrossRef] [PubMed]
- PBS. Labour Force Participation Rates and Un-Employment Rates by Age, Sex and Area, 2012–2013. 2013; Statistical Reports and Publications of the Pakistan Bureau of Statistics. Available online: http://www.pbs.gov.pk/sites/default/files/Labour%20Force/publications/lfs_Annual_2012_13/t14-pak.pdf (accessed on 15 August 2018).
- Ali, T.S.; Krantz, G.; Gul, R.; Asad, N.; Johansson, E.; Mogren, I. Gender roles and their influence on life prospects for women in urban Karachi, Pakistan: A qualitative study. Glob. Health Action 2011, 4, 7448. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, N.S.; Khan, K.; Shaikh, B.T. Gender: Shaping personality, lives and health of women in Pakistan. BMC Womens Health 2014, 14, 53. [Google Scholar] [CrossRef] [PubMed]
- Jafar, T.H.; Qadri, Z.; Chaturvedi, N. Coronary artery disease epidemic in Pakistan: More electrocardiographic evidence of ischaemia in women than in men. Heart 2008, 94, 408. [Google Scholar] [CrossRef] [PubMed]
- WHO. Indoor Air P Indoor Air Pollution and Child Health in Pollution and Child Health in Pakistan; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Khan, M.S.; Jafary, F.H.; Faruqui, A.M. High prevalence of lack of knowledge of symptoms of acute myocardial infarction in Pakistan and its contribution to delayed presentation to the hospital. BMC Public Health 2007, 7, 284. [Google Scholar] [CrossRef] [PubMed]
- Zia, N.; Shahzad, H.; Baqir, S.M. Ambulance use in Pakistan: An analysis of surveillance data from emergency departments in Pakistan. BMC Emerg. Med. 2015, 15, S9. [Google Scholar] [CrossRef] [PubMed]
- Magalhaes, S.; Baumgartner, J.; Weichenthal, S. Impacts of exposure to black carbon, elemental carbon, and ultrafine particles from indoor and outdoor sources on blood pressure in adults: A review of epidemiological evidence. Environ. Res. 2018, 161, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Henze, D.K.; Jack, D.; Henderson, B.H.; Kinney, P.L. Assessing public health burden associated with exposure to ambient black carbon in the United States. Sci. Total Environ. 2016, 539, 515–525. [Google Scholar] [CrossRef] [PubMed]
- Krewski, D.; Jerrett, M.; Burnett, R.T. Extended follow-up and spatial analysis of the American Cancer Society study linking particulate air pollution and mortality. Res. Rep. Health Eff. Inst. 2009, 140, 115–136. [Google Scholar]
- Gurjar, B.R.; Butler, T.M.; Lawrence, M.G.; Lelieveld, J. Evaluation of emissions and air quality in megacities. Atmos. Environ. 2008, 42, 1593–1606. [Google Scholar] [CrossRef]
- Gurjar, B.R.; Jain, A.; Sharma, A. Human health risks in megacities due to air pollution. Atmos. Environ. 2010, 44, 4606–4613. [Google Scholar] [CrossRef]
- Ira, T.; Kenneth, D.; Mark, F.; Michael, J.; Frank, K. Traffic-related air pollution: A critical review of the literature on emissions, exposure, and health effects. Res. Rep. Health Eff. Inst. 2010, 17, 386. [Google Scholar]
- Kazmi, J.H.; Zubair, S. Estimation of Vehicle Damage Cost Involved in Road Traffic Accidents in Karachi; Pakistan: A Geospatial Perspective. Procedia Eng. 2014, 77, 70–78. [Google Scholar] [CrossRef]
- Sabzwari, S.R.; Fatmi, Z. Comparison of exhaled carbon monoxide levels among commuters and roadside vendors in an urban and a suburban population in Pakistan. Environ. Monit. Assess. 2011, 180, 399–408. [Google Scholar] [CrossRef] [PubMed]


© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).