Health Impact Assessment Associated with Exposure to PM10 and Dust Storms in Kuwait



Abstract
1. Introduction
2. Experiments
2.1. Study Area Description and Justification
2.2. Health Classification
2.3. Quality Control
2.4. Statistical Analysis
3. Results
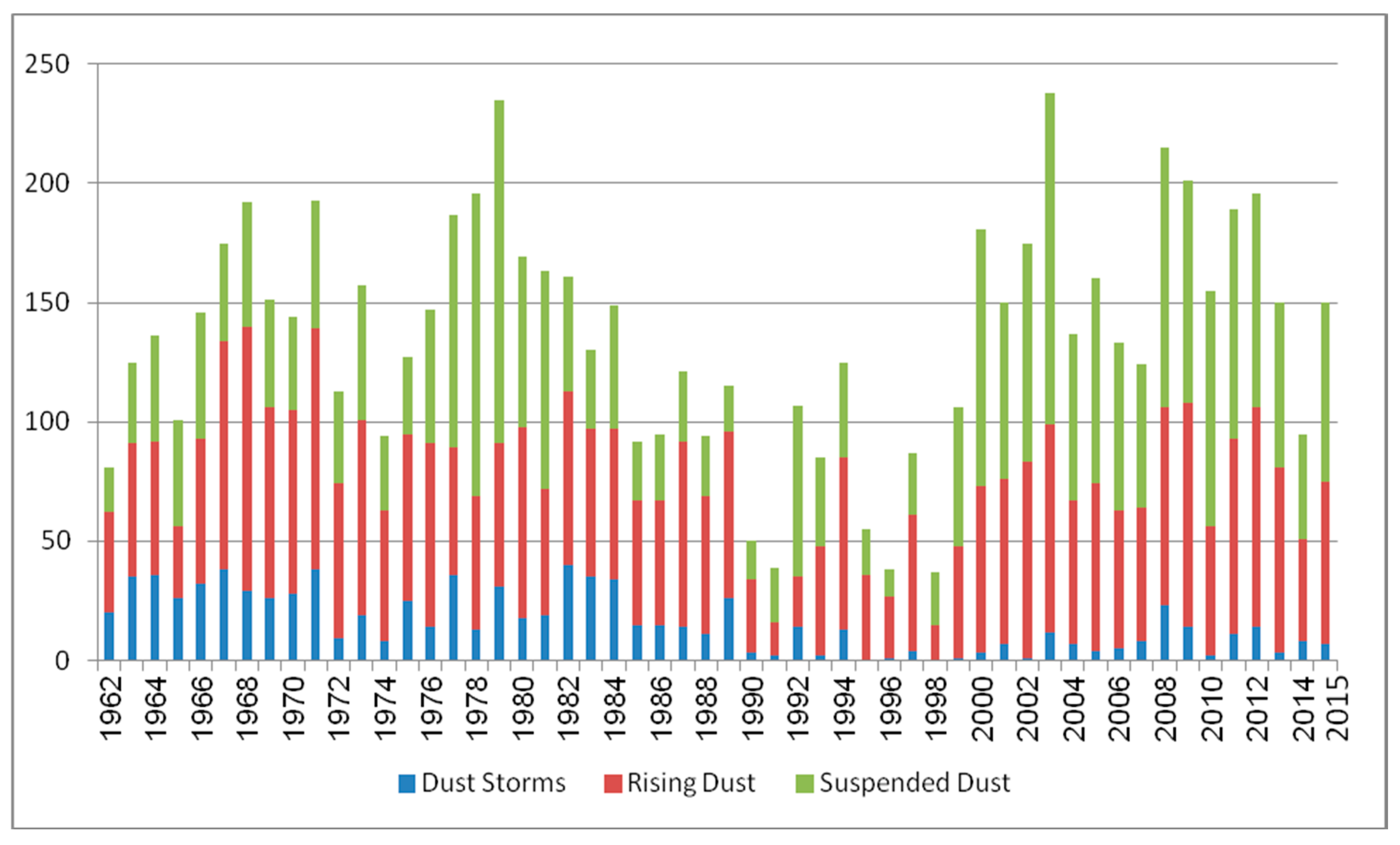
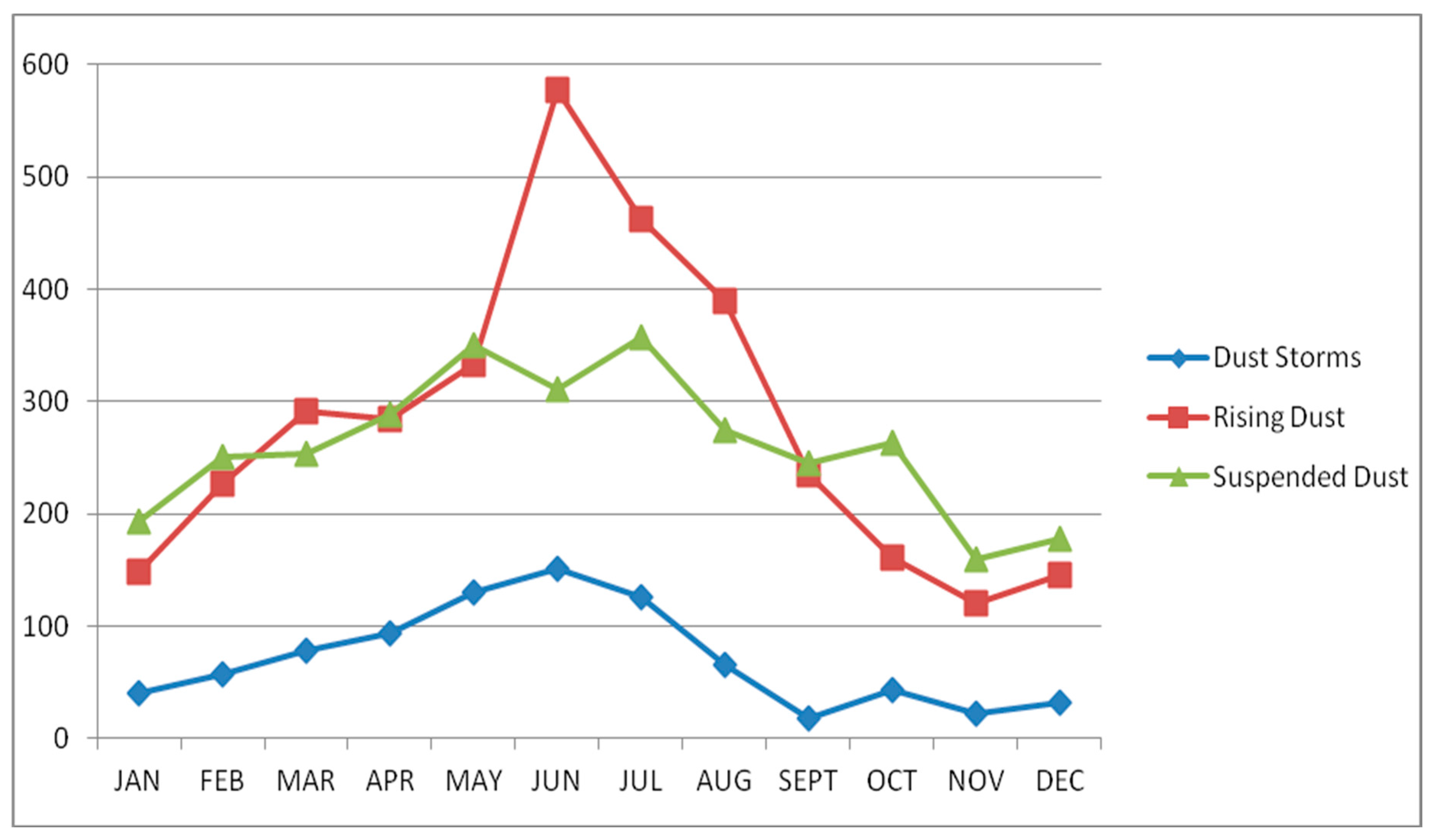
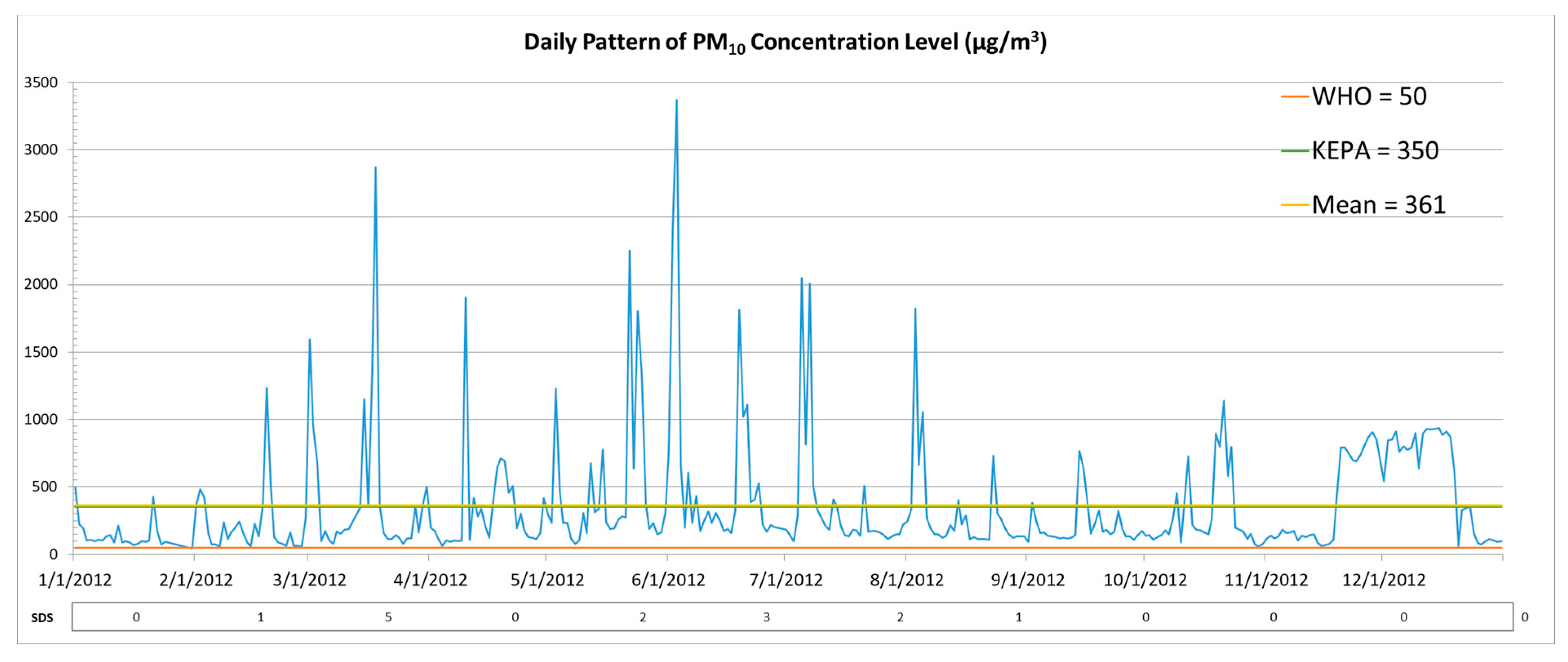
3.1. Sand and Dust Storms and PM10 Concentration Levels
3.2. Morbidity Indicators
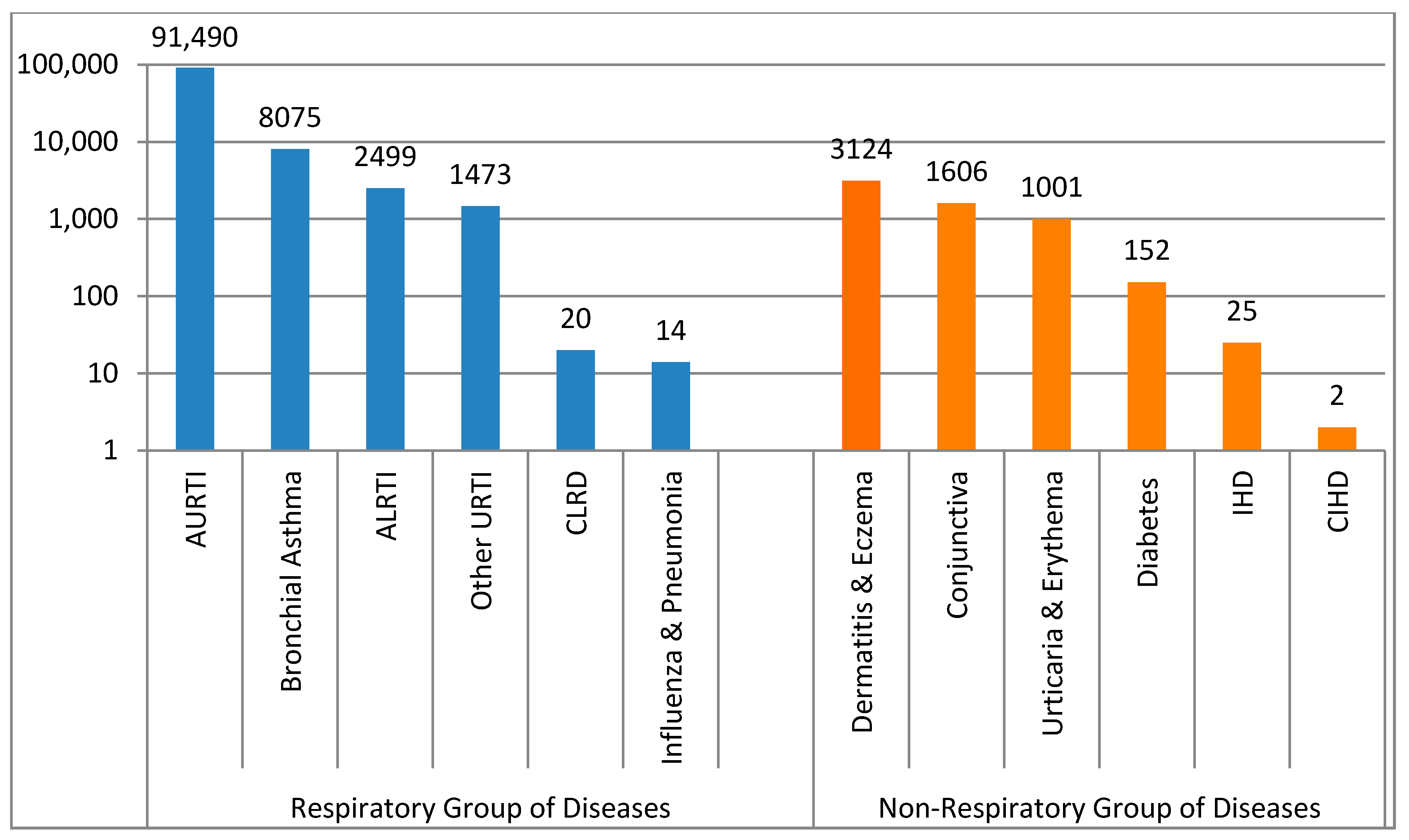
3.2.1. Adjusted Health Visits for Respiratory Diseases
3.2.2. Adjusted Health Visits for Non-Respiratory Diseases
3.2.3. Correlation between PM10 and Morbidity
3.3. Mortality Indicators
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References and Note
- Middleton, N.J. Desert dust hazards: A global review. Aeolian Res. 2017, 24, 56–63. [Google Scholar] [CrossRef]
- Al-Dousari, A.M.; Doronzo, D.; Ahmed, M. Types, indications and impact evaluation of sand and dust storms trajectories in the Arabian Gulf. Sustainability 2017, 9, 1526. [Google Scholar] [CrossRef]
- Al-Dousari, A.M.; Al-Awadhi, J.; Ahmed, M. Dust fallout characteristics within global dust storms major trajectories. Arab. J. Geosci. 2013, 6, 3877–3884. [Google Scholar] [CrossRef]
- WHO. WHO Air Quality Guidelines for Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide: Global Update 2005: Summary of Risk Assessment; WHO, World Health Organization: Geneva, Switzerland, 2006; p. 9, WHO/SDE/PHE/OEH/06.02. [Google Scholar]
- Al-Taiar, A.; Thalib, L. Short-term effect of dust storms on the risk of mortality due to respiratory, cardiovascular and all-causes in Kuwait. Int. J. Biometeorol. 2014, 58, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Draxler, R.; Gillette, D.; Kirkpatrick, J.; Heller, J. Estimating PM10 air concentrations from dust storms in Iraq, Kuwait and Saudi Arabia. Atmos. Environ. 2001, 35, 4315–4330. [Google Scholar] [CrossRef]
- Middleton, N.; Yiallouros, P.; Kleanthous, S.; Kolokotroni, O.; Schwartz, J.; Dockery, D.W.; Demokritou, P. Koutrakis, P. A 10-year time series analysis of respiratory and cardiovascular morbidity in Nicosia, Cyprus: The effect of short-term changes in air pollution and dust storms. Environ. Health 2008, 7, 39. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.Y.; Cheng, M.H.; Chen, C.C. Effects of Asian dust storm events on hospital admissions for congestive heart failure in Taipei, Taiwan. J. Toxicol. Environ. Health 2009, 72, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.F.; Ho, S.C.; Chiu, H.F.; Wu, T.N.; Chen, P.S.; Yang, C.Y. Consequences of exposure to Asian dust storm events on daily pneumonia hospital admissions in Taipei, Taiwan. J. Toxicol. Environ. Health 2008, 71, 1295–1299. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.L.; Levy, J.K.; Lin, Z. The effect of sandstorms and air pollution on cause-specific hospital admissions in Taipei, Taiwan. Occup. Environ. Med. 2008, 65, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Sicard, P.; Lesne, O.; Alexandre, N.; Mangin, A.; Collomp, R. Air quality trends and potential health effects: Development of an aggregate risk index. Atmos. Environ. 2011, 45, 1145–1153. [Google Scholar] [CrossRef]
- Sprigg, W.A.; Nickovic, S.; Galgiani, J.N.; Pejanovic, G.; Petkovic, S.; Vujadinovic, M.; Vukovic, A.; Dacic, M.; DiBiase, S.; Prasad, A.; et al. Regional dust storm modeling for health services: The case of valley fever. Aeolian Res. 2014, 14, 53–73. [Google Scholar] [CrossRef]
- Schwartz, J.; Norris, G.; Larson, T.; Sheppard, L.; Claiborne, C.; Koenig, J. Episodes of high coarse particle concentrations are not associated with increased mortality. Environ. Health Perspect. 1999, 107, 339–342. [Google Scholar] [CrossRef] [PubMed]
- Xie, S.; Yu, T.; Zhang, Y.; Zeng, L.; Qi, L.; Tang, X. Characteristics of PM10, SO2, NOx and O3 in ambient air during the dust storm period in Beijing. Sci. Total Environ. 2005, 345, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Perez, L.; Tobias, A.; Querol, X.; Kunzli, N.; Pey, J.; Alastuey, A.; Viana, M.; Valero, N.; Gonzalez-Cabre, M.; Sunyer, J. Coarse particles from Saharan dust and daily mortality. Epidemiology 2008, 19, 800–807. [Google Scholar] [CrossRef] [PubMed]
- Ostro, B.D.; Hurley, S.; Lipsett, M.J. Air pollution and daily mortality in the Coachella Valley, California: A study of PM10 dominated by coarse particles. Environ. Res. 1999, 81, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.S.; Sheen, P.C.; Chen, E.R.; Liu, Y.K.; Wu, T.N.; Yang, C.Y. Effect of Asian dust storm events on daily mortality in Taipei, Taiwan. Environ. Res. 2004, 95, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.J.; Cho, S.H.; Chun, Y.; Lagarde, F.; Pershagen, G. Effects of the Asian dust events on daily mortality in Seoul, Korea. Environ. Res. 2002, 90, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Tao, Y.; An, X.; Sun, Z.; Hou, Q.; Wang, Y. Association between dust weather and number of admissions for patients with respiratory diseases in spring in Lanzhou. Sci. Total Environ. 2012, 423, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.J. The impact of air pollution on human health in Suwon city. Asian J. Atmos. Environ. 2013, 7, 227–233. [Google Scholar] [CrossRef]
- Barnett, A.G.; Fraser, J.F.; Munck, L. The effects of the 2009 dust storm on emergency admissions to a hospital in Brisbane, Australia. Int. J. Biometeorol. 2012, 56, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Gyan, K.; Henry, W.; Lacaille, S.; Laloo, A.; Lamsee-Ebanks, C.; McKay, S.; Antonie, R.M.; Monteil, M.A. African dust clouds are associated with increased pediatric asthma accident and emergency admissions on the Caribbean island of Trinidad. Int. J. Biometeorol. 2005, 49, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Kanatani, K.T.; Ito, I.; Al-Delaimy, W.K.; Adachi, Y.; Mathews, W.C.; Ramsdell, J.W. Desert dust exposure is associated with increased risk of asthma hospitalization in children. Am. J. Respir. Crit. Care Med. 2010, 182, 1475–1481. [Google Scholar] [CrossRef] [PubMed]
- Thalib, L.; Al-Taiar, A. Dust storms and the risk of asthma admissions to hospitals in Kuwait. Sci. Total Environ. 2012, 433, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Washington, R.; Todd, M.; Middleton, N.J.; Goudie, A.S. Dust-storm source areas determined by the total ozone monitoring spectrometer and surface observations. Ann. Assoc. Am. Geogr. 2003, 93, 297–313. [Google Scholar]
- Miri, M.; Aval, H.E.; Ehrampoush, M.H.; Mohammadi, A.; Toolabi, A.; Nikonahad, A.; Derakhshan, Z.; Abdollahnejad, A. Human health impact assessment of exposure to particulate matter: An AirQ software modeling. Envirorn. Sci. Pollut. R. 2017, 24, 16513–16519. [Google Scholar] [CrossRef] [PubMed]
- Miri, M.; Derakhshan, Z.; Allahabadi, A.; Ahmadi, E.; Conti, G.O.; Ferrante, M.; Aval, H.E. Mortality and morbidity due to exposure to outdoor air pollution in Mashhad metropolis, Iran: The AirQ model approach. Environ. Res. 2016, 151, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Goudarzi, G.; Daryanoosh, S.M.; Godini, H.; Hopke, P.K.; Sicard, P.; De Marco, A.; Rad, H.D.; Habizadeh, A.; Jahedi, F.; Mohammadi, M.J.; et al. Health risk assessment of exposure to the Middle-Eastern dust storms in the Iranian megacity of Kermanshah. Public Health 2017, 148, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Nourmoradi, H.; Khaniabadi, Y.O.; Goudarzi, G.; Daryanoosh, S.M.; Khoshgoftar, M.; Omidi, F.; Armin, A. Air quality and health risks associated with exposure to particulate matter: A cross-sectional study in Khorramabad, Iran. Health Scope 2016, 5. [Google Scholar] [CrossRef]
- Mohammadi, A.; Azhdarpoor, A.; Shahsavani, A.; Tabatabaee, H. Health impacts of exposure to PM10 on inhabitants of Shiraz, Iran. Health Scope 2015, 4. [Google Scholar] [CrossRef]
- Zallaghi, E.; Goudarzi, G.; Geravandi, S.; Mohammadi, M.J. Epidemiological Indexes Attributed to Particulates With Less Than 10 Micrometers in the Air of Ahvaz City During 2010 to 2013. Health Scope 2014, 3. [Google Scholar] [CrossRef]
- Daryanoosh, M.; Goudarzi, G.; Rashidi, R.; Keishams, F.; Hopke, P.K.; Mohammadi, M.J.; Nourmoradi, H.; Sicard, P.; Takdastan, A.; Vosoughi, M.; et al. Risk of morbidity attributed to ambient PM10 in western cities of Iran. Toxin Rev. 2017. [Google Scholar] [CrossRef]
- Khaniabadi, Y.O.; Daryanoosh, S.Y.; Amrane, A.; Polosa, R.; Hopke, P.K.; Goudarzi, G.; Mohammadi, M.J.; Sicard, P.; Armin, H. Impacts of Middle Eastern dust storms on human health. Atmos. Pollut. Res. 2017, 8, 606–613. [Google Scholar] [CrossRef]
- Geravandi, S.; Sicard, P.; Khaniabadi, Y.O.; De Marco, A.; Ghomeishi, A.; Goudarzi, G.; Mahboubi, M.; Yari, A.R.; Dobaradaran, S.; Hassani, G.; et al. A comparative study of hospital admissions for respiratory diseases during normal and dusty days in Iran. Environ. Sci. Pollut. Res. 2017, 4, 18152–18159. [Google Scholar] [CrossRef] [PubMed]
- Gharehchahi, E.; Mahvi, A.; Amini, H.; Nabizadeh, R.; Akhlaghi, A.; Shamsipour, M.; Yunesian, M. Health impact assessment of air pollution in Shiraz, Iran: A two-part study. Iran. J. Environ. Health 2013, 11. [Google Scholar] [CrossRef] [PubMed]
- Naddafi, K.; Hassanvand, M.S.; Yunesian, M.; Momeniha, F.; Nabizadeh, R.; Faridi, S.; Gholampour, A. Health impact assessment of air pollution in megacity of Tehran, Iran. Iran. J. Environ. Health 2012, 9. [Google Scholar] [CrossRef] [PubMed]
- Al-Rifaia, N.; Elmi, A.; Khan, A.R. Exploring possible seasonal trends in mortality rate in relation to age, gender and environmental conditions in Kuwait: A preliminary analysis. J. Eng. Res.-Kuwait 2011, 8, 19–27. [Google Scholar] [CrossRef]
- International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) Version for 2010. Chapter X. Available online: http://apps.who.int/classifications/icd10/browse/2010/en (accessed on 29 November 2016).
- McTainish, G.H.; Pitbaldo, J.R. Dust storms and related phenomena measured from meteorological records in Australia. Earth Surf. Process. 1987, 12, 415–424. [Google Scholar] [CrossRef]
- World Meteorological Organization (WMO). Climate Change and Land Degradation WMO-No 989; WMO: Geneva, Switzerland, 2005; ISBN 92-63-10989-3. [Google Scholar]
- KEPA, Kuwait EPA Regulations concerning the safety of workers in all establishments and the requirements and criteria for adequate ventilation in enclosed and semi-enclosed public places. Articles 19 and 20 of Kuwait Environmental Protection Act No. 42, Kuwait Al-Youm No. 1341, 2014.
- Congenital Anomalies, Fact Sheet, World Health Organization. Updated 2016. Available online: http://www.who.int/mediacentre/factsheets/ fs370/en (accessed on 1 September 2016).
- Mirhosseini, S.H.; Birjandi, M.; Zare, M.R.; Fatehizadeh, A. Analysis of Particulate matter (PM10 and PM2.5) concentration in Khorramabad city. Int. J. Environ. Health Eng. 2013, 2. [Google Scholar] [CrossRef]
- Shahsavani, A.; Naddafi, K.; Jafarzade, H.N.; Mesdaghinia, A.; Yunesian, M.; Nabizadeh, R.; Arahami, M.; Sowlat, M.H.; Yarahmadi, M.; Saki, H. The evaluation of PM10, PM2.5, and PM1 concentrations during the Middle Eastern Dust (MED) events in Ahvaz, Iran, from April through September 2010. J. Arid Environ. 2012, 77, 72e83. [Google Scholar] [CrossRef]
- Al-Hemoud, A.; Al-Sudairawi, M.; Neelamanai, S.; Naseeb, A.; Behbehani, W. Socioeconomic effect of dust storms in Kuwait. Arab. J. Geosci. 2017, 10. [Google Scholar] [CrossRef]
- Dominici, F.; McDermott, A.; Hastie, T.J. Improved semiparametric time series models of air pollution and mortality. J. Am. Stat. Assoc. 2004, 99, 938–948. [Google Scholar] [CrossRef]
- Tominz, R.; Mazzoleni, B.; Daris, F. Estimate of potential health benefits of the reduction of air pollution with PM10 in Trieste, Italy. Epidemiol. Prev. 2005, 29, 149–155. [Google Scholar] [PubMed]
- Brauer, M.; Ebelt, S.T.; Fisher, T.V.; Brumm, J.; Petkau, A.J.; Vedal, S. Exposure of chronic obstructive pulmonary disease patients to particles: Respiratory and cardiovascular health effects. J. Expo. Anal. Environ. Epidemiol. 2001, 11, 490–500. [Google Scholar] [CrossRef] [PubMed]
- Tam, W.; Wong, T.; Wong, A.; Hui, D. Effect of dust storm events on daily emergency admissions for respiratory diseases. Respirology 2012, 17, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.C.; Pan, X.C.; Kim, S.Y.; Park, K.; Park, E.J.; Jin, X.; Yi, S.M.; Kim, Y.H.; Park, C.H.; Song, S.; et al. Asian dust storm and pulmonary function of school children in Seoul. Sci. Total Environ. 2010, 408, 754–759. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Lee, K.K. Effects of Asian dust events on daily asthma in Seoul, Korea. Meteorol. Appl. 2014, 21, 202–209. [Google Scholar] [CrossRef]
- Stafoggia, M.; Zauli-Sajan, S.; Pey, J.; Samoli, J.; Alessandrini, E.; Basagaña, X.; Cernigliaro, A.; Chiusolo, M.; Demaria, M.; Díaz, J.; et al. Desert Dust Outbreaks in Southern Europe: Contribution to Daily PM10 Concentrations and Short-Term Associations with Mortality and Hospital Admissions. Environ. Health Perspect. 2016, 124, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Katsouyanni, K.; Touloumi, G.; Samoli, E.; Gryparis, A.; Le Tertre, A.; Monopolis, Y.; Rossi, G.; Zmirou, D.; Ballester, F.; Boumghar, A.; et al. Confounding and effect modification in the short-term effects of ambient particles on total mortality: Results from 29 European cities within the APHEA2 project. Epidemiology 2001, 12, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Tobias, A.; Perez, L.; Diaz, J.; Linares, C.; Pey, J.; Alastruey, A.; Querol, X. Short-term effects of particulate matter on total mortality during Saharan dust outbreaks: A case-crossover analysis in Madrid (Spain). Sci. Total Environ. 2011, 412–413, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Janssen, N.; Fischer, P.; Marra, M.; Ameling, C.; Cassee, F. Short-term effects of PM2.5, PM10 and PM2.5–10 on daily mortality in the Netherlands. Sci. Total Environ. 2013, 463, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Corso, M.; Blanchard, M.; Host, S.; Pascal, L.; Larrieu, S. Short-term impacts of particulate matter (PM10, PM10–2.5, PM2.5) on mortality in nine French cities. Atmos. Environ. 2014, 95, 175–184. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dust Type | Dust Storm | Rising Dust | Suspended Dust |
|---|---|---|---|
| Dust Storm | 1 | ||
| Rising Dust | 0.746 ** | 1 | |
| Suspended Dust | 0.722 ** | 0.709 ** | 1 |
| PM Type | N | Min | Max | Mean | SD | DES | KEPA 24-h Mean | WHO 24-h Guideline | WHO Guideline for Annual Mean |
|---|---|---|---|---|---|---|---|---|---|
| PM10 | 354 | 45.18 | 3369.33 | 361.69 | 431.20 | 104 | 350 | 50 | 20 |
| Respiratory Group of Diseases | Adjusted Health Visits | Average Visits * | Non-Respiratory Group of Diseases | Adjusted Health Visits | Average Visits * |
|---|---|---|---|---|---|
| AURTI | 91,490 | 2772 | Dermatitis & Eczema | 3124 | 93 |
| Bronchial Asthma | 8075 | 246 | Conjunctiva | 1606 | 48 |
| ALRTI | 2499 | 76 | Urticaria & Erythema | 1001 | 30 |
| Other URTI | 1473 | 44 | Diabetes | 152 | 5 |
| CLRD | 20 | 0.6 | IHD | 25 | 0.8 |
| Influenza & Pneumonia | 14 | 0.5 | CIHD | 2 | 0.1 |
| Respiratory Disease | Mean | SD |
|---|---|---|
| AURTI | 1711 | 813.14 |
| Bronchial Asthma | 148 | 62.28 |
| ALRTI | 47 | 26.43 |
| Correlation Matrix | PM10 | Bronchial Asthma | AURTI | ALRTI |
|---|---|---|---|---|
| PM10 | 1 | |||
| Bronchial Asthma | 0.292 * | 1 | ||
| AURTI | 0.232 | 0.839 ** | 1 | |
| ALRTI | 0.255 | 0.737 ** | 0.827 ** | 1 |
| Cause of Mortality | Number of Deaths | Proportionate Mortality Rate % * | Cause-Specific Mortality Rate ** |
|---|---|---|---|
| Congenital Anomalies | 6 | 26.1 | 1.86 |
| Perinatal Disease | 5 | 17.4 | 1.55 |
| Respiratory Diseases | 2 | 8.7 | 0.62 |
| Cardiovascular Diseases | 2 | 8.7 | 0.62 |
| Non-Respiratory Diseases | 1 | 4.3 | 0.31 |
| Diabetes Mellitus | 1 | 4.3 | 0.31 |
| Other Causes | 7 | 30.5 | 2.16 |
| Total | 23 | 100% |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Hemoud, A.; Al-Dousari, A.; Al-Shatti, A.; Al-Khayat, A.; Behbehani, W.; Malak, M. Health Impact Assessment Associated with Exposure to PM10 and Dust Storms in Kuwait. Atmosphere 2018, 9, 6. https://doi.org/10.3390/atmos9010006
Al-Hemoud A, Al-Dousari A, Al-Shatti A, Al-Khayat A, Behbehani W, Malak M. Health Impact Assessment Associated with Exposure to PM10 and Dust Storms in Kuwait. Atmosphere. 2018; 9(1):6. https://doi.org/10.3390/atmos9010006
Chicago/Turabian StyleAl-Hemoud, Ali, Ali Al-Dousari, Ahmad Al-Shatti, Ahmed Al-Khayat, Weam Behbehani, and Mariam Malak. 2018. "Health Impact Assessment Associated with Exposure to PM10 and Dust Storms in Kuwait" Atmosphere 9, no. 1: 6. https://doi.org/10.3390/atmos9010006
APA StyleAl-Hemoud, A., Al-Dousari, A., Al-Shatti, A., Al-Khayat, A., Behbehani, W., & Malak, M. (2018). Health Impact Assessment Associated with Exposure to PM10 and Dust Storms in Kuwait. Atmosphere, 9(1), 6. https://doi.org/10.3390/atmos9010006