Abstract
Little information is available on the assessment of health impact concerning the Middle Eastern dust storms and PM10 concentration levels despite the aridity of the region and frequent dust storms occurring in this part of the world. A prospective study was conducted to determine the association between dust particles and morbidity and mortality rates for respiratory and cardiovascular diseases in Kuwait. Spearman and Pearson’s correlations were used to identify such associations. Results revealed a significant correlation between dust storms, suspended dust and rising dust (p < 0.01). Correlation between the occurrence of respiratory and cardiovascular diseases and dust storms showed that PM10 concentrations were significantly correlated with bronchial asthma at the 0.05 level (Pearson r = 0.292). Significant correlations at the 0.01 level were shown between bronchial asthma and both acute lower respiratory tract infection (r = 0.737) and acute upper respiratory tract infection (r = 0.839). Respiratory and cardiovascular mortality rates were both equal to 0.62 per 10,000 persons, each corresponding to 8.7% proportionate mortality rate. This study provides a good evidence of the consistent relationship between dust storm events, PM10 concentration levels, and respiratory diseases.
1. Introduction
Dust storms are natural phenomena, most of which originate in desert or semi-desert drylands, in which dust particles are transported away from the main source, sometimes over thousands of kilometers [1]. The northern region of the Arabian region is characterized by complex dust storm trajectories where they pass through the western desert of Syria and Iraq toward the Mesopotamian flood plain reaching the northeastern region of the peninsula into Kuwait at a dust fallout rate of 61.4 tons per km2 per year, where fallen dust compromises 37% of sand particles [2,3]. A particular feature of blown dust is its extreme particulate matter intensity that increases the ambient air dust concentrations for several days. Dust particles include both PM10 and PM2.5 particle sizes which have an aerodynamic diameter smaller than 10 and 2.5 μm, respectively. A large number of desert dust contains particles with concentrations exceeding the guidelines established by the World Health Organization (WHO) for human health protection (20 μg/m3 annual average; 50 μg/m3 a daily average) [4]. Atmospheric concentrations in individual dust events have recorded PM10 levels of 1000 μg/m3, with extreme values exceeding 10,000 μg/m3 during the notorious Red Dawn event in Australia in September 2009 [1]. Daily PM10 levels over 200 μg/m3 were suggested for small to medium scale dust events, while a higher cut-off point of 400 μg/m3 was used to define severe dust events [5,6]. Other studies have used much lower PM10 levels to identify dust storm days [7,8,9,10].
Because most air quality monitoring stations record data based on the PM10 measurements as opposed to other particulate matter size, the majority of epidemiological studies use PM10 level as exposure indicator. The World Health Organization air quality guidelines have provided a basis for characterizing human health effects of major air pollutants including PM10 [4]. The assessment of personal exposure to air pollution is a critical component of epidemiological studies in the evaluation of health effects from airborne particulate matter (PM). The recognized air pollution effects over public health include increased risk of hospital admissions and mortality by respiratory or cardiovascular diseases. An aggregate risk index is a useful tool to identify the additive effects of short-term exposure of the main air pollutants, including PM10 and PM2.5 [11]. Although fine particles below PM2.5 comprise the greatest health concern, since they are more likely to penetrate deep into the alveoli sacs of the lungs, the PM10 course particles represent the predominant part of dust in dust storms and cover most of the respiratory health issues, as large particles become trapped in the nasal passages, nose hair follicles and upper respiratory tract [12]; in contrast, fine particles decline due to high wind speed and long travel distances of dust storms [13,14].
Dust storm events have been strongly associated with mortality and morbidity rates with a broad range of health effects, but predominantly to the respiratory and cardiovascular systems. Several studies from various countries have examined the effects of dust storms and particulate matter on morbidity and mortality rates, and hospital admissions for various ill-health effects. During Saharan dust days, a daily increase of 10 μg/m3 of PM10 increased daily mortality by 8.4% in Barcelona (Spain) [15]. A 10 μg/m3 change in daily PM10 was associated with an approximately 1% increase in cardiovascular and respiratory mortality in the Coachella Valley, California [16]. Dust storms in Taiwan had a 7.66% increase in the risk for respiratory diseases [17], congestive heart failure [8] and daily pneumonia hospital admissions [9]. Asian dust storms had a 4.1% increase in the rate of deaths from cardiovascular and respiratory causes in Seoul, South Korea [18] and a significant increase in respiratory hospitalizations in China [19,20]. Dust blown from the Sahara to the Eastern Mediterranean resulted in an increase in all-cause hospital admissions including respiratory and cardiovascular diseases in Nicosia, Cyprus [7]. An Australian dust storm which lasted for only one day resulted in a 39% increase in hospital emergency admissions [21]. Increased asthma emergency admissions were associated with Saharan dust in the Caribbean island of Trinidad [22] and with Asian dust in Toyama, Japan [23].
Little information is available on the assessment of health impact about dust storms and PM10 concentration levels in the Middle Eastern despite the facts that the region experiences frequent dust storms [24] and is considered a major source of global dust [1,3,25]. Many studies from Iran have demonstrated a positive association between dust particles and total mortality including cardiovascular and respiratory mortalities [26,27,28,29,30,31,32,33,34] and hospital admissions for cardiovascular and respiratory diseases [35,36]. Only three studies were conducted in Kuwait to determine the health impact of dust storms on morbidity and mortality rates. A study conducted by Thalib and Al-Taiar [24] concluded that dust storms had a significant impact on asthma and respiratory hospital admissions. Al-Rifaia et al. [37] and Al-Taiar and Thalib [5] showed that dust storms had little impact on short-term respiratory, cardiovascular or all-cause mortality.
The primary objective of this study was to assess the environmental burden of outdoor air, specifically dust storms and PM10 airborne concentration on the health impacts in Kuwait regarding morbidity and mortality rates.
2. Experiments
A prospective time-series study of daily PM10 concentrations and daily morbidity and mortality through hospital admissions were evaluated in a single district in Kuwait, Ali Sabah Al-Salem (ASA) during 2012. The effect of changes in daily levels of PM10 hospitalization for respiratory, non-respiratory, cardiovascular and all-cause diseases was investigated using parametric (Pearson) and non-parametric (Spearman) correlations. Daily attendance rates of air pollution-related group of diseases in ASA primary health care center were evaluated. Daily attendance rates were adjusted to correspond to hospital visits per week. Data collection also included daily PM10 concentration levels, PM10 respiratory-related morbidity rates and mortality rates. Daily PM10 concentrations were adjusted to represent weekly rates. The data of both PM10 and air pollution-related diseases allowed for the investigation of the pattern of association between air pollution and morbidity by correlating visits to public health centers for air pollution-related diseases and the daily measurements of PM10 pollutant level during 2012. Dust storms, rising dust, and suspended dust were collected from Kuwait international airport station for the last 53 years (1962–2015). PM10 pollutant levels were obtained from the Kuwait Environment Public Authority (KEPA) for the year 2012.
2.1. Study Area Description and Justification
Ali Sabah Al-Salem (ASA) is a suburban area of 7.65 km2, located south of Kuwait and it lies at the terminal of the urbanization areas. The estimated population during 2012 was 48,685 residents, of which 32,341 were Kuwaiti nationals. Although the area was recently built and inhabited, its occupants complained of air pollutants. Air pollution in this area may be due to its proximity (within 4 km) to industrial facilities which were established before the build-up of this community. ASA was considered as the research study index district on the basis that its population was demanding for studying the health impact of air pollution resulting from industries, and the fact that the district is located upwind from natural environmental events, such as sand and dust storms. ASA contains fixed meteorological stations that continuously monitor the level of air quality. Multiple air pollutants were studied during the whole project. The air pollutants were grouped into three categories: gaseous pollutants (SO2, NO2, H2S, O3, CO, CO2), organic pollutant compounds (CH4, NH3, NCH4), and PM10. PM10 and dust storm events were investigated to determine their potential impact on morbidity and mortality rates.
2.2. Health Classification
The International Statistical Classification System of Diseases and Related Health Problems from the World Health Organization ICD-10 was used for health classifications in the study [38]. ICD-10 was endorsed in May 1990 by the Forty-third World Health Assembly. It is cited in more than 20,000 scientific articles and used by more than 100 countries around the world. ICD is the foundation for the identification of health trends and statistics globally, and the international standard for reporting diseases and health conditions [38]. The list of a group of diseases related to air pollution was used to determine the selected diagnosis. Each group of diseases was classified under a heading following the ICD. A person may have one disease or more per year and coded as a case for each one. Thus, the number of cases and the attributed estimate rates may exceed the total population in some incidents. Respiratory diseases were identified by the ICD-10 codes J00-J99 and contain acute upper respiratory infection (J00-J06), influenza and pneumonia (J09-J18), other acute lower respiratory infection such as acute bronchitis (J20-J22), other diseases of upper respiratory tract such as chronic rhinitis (J30-J39), chronic lower respiratory diseases such as emphysema (J40-J47), bronchial asthma (J45-J46), and lung diseases due to external agents (J60-J70).
2.3. Quality Control
Certain quality control measures were incorporated throughout the study period. Health records of Kuwaiti citizens residing in ASA and meteorological records of the same district were investigated prospectively during the same period. Primary health care morbidity and mortality data were obtained from the information technology electronic database of the Ministry of Health of Kuwait. A case with multiple admissions for different morbidities was counted as multiple cases. Records of cases registered in Kuwait health information electronic file as suffering or dying from a pre-selected list of air pollution-related releases were selected. A special format was used to record daily average of continuous measurements for the ten air pollutants mentioned above. A record of any case present in the selected health establishment but residing in another area was excluded from data analysis. Digital raw data about particulate air pollution was obtained from the database of Kuwait Environment Public Authority (KEPA) fixed station located in the selected district. Only 11 days (<3%) had missing values from KEPA meteorological station (n = 354 days recorded out of 365 days/year).
2.4. Statistical Analysis
Descriptive statistics, parametric and non-parametric correlations were used in the study. Descriptive statistics were utilized to determine frequency distributions, measures of central tendencies (mean, medians) and measures of variability from data related to dust, PM10 and hospital visits for respiratory diseases. Pearson product-moment correlation, a parametric statistical test was used to determine the degree of association between PM10 concentration and morbidity health rates. Spearman’s rho rank correlation was utilized to investigate the monotonic association between dust storms, rising dust and suspended dust.
3. Results
3.1. Sand and Dust Storms and PM10 Concentration Levels
Figure 1 shows the total number of dust storms (DS), rising dust (RD) and suspended dust (SD) collected from Kuwaiti meteorological stations for the last 53 years (1962–2015). A dust storm was defined as the result of surface winds exceeding 33 km/h raising large quantities of dust into the air and reducing visibility to less than 1000 m [39,40]. Rising dust was defined as elevated dust occurring when winds are moderately active at a speed of 15–40 km/h and visibility is 1000 m or more. Suspended dust occurs with calm wind speed of 6–26 km/h and horizontal visibility in the range of 1–5 km. A total of 859 SD occurred between 1962 and 2015 with an average of 15 SD per year. It is apparent that both RD and SD are significantly higher than DS throughout the period. The total number of RD is roughly equal to SD during the same period (3380 total RD vs. 3128 total SD) with an average of 62 vs. 58 dusts per year, respectively. A similar trend of DS, RD and SD occurs throughout the studied period except for a low episode between years 1990 and 1998, in large part, due to missing or incomplete data record during and after the Gulf War in 1990. Figure 2 presents monthly records of dust at the ASA area for the year 2012. It is apparent that all three dust types follow a similar pattern with a significantly higher number of dust storms, rising dust and suspended dust events during the summer season (June, July, September, August) and lower events during the remaining seasons. This phenomenon may be attributed to several factors including higher temperature and lower precipitation; daily average temperature recorded during the four summer months equaled to 38.3 °C with zero daily precipitation. Table 1 shows non-parametric Spearman’s rank correlation between all three dust types. A highly significant correlation is shown between dust storms, rising dust and suspended dust (p < 0.01).
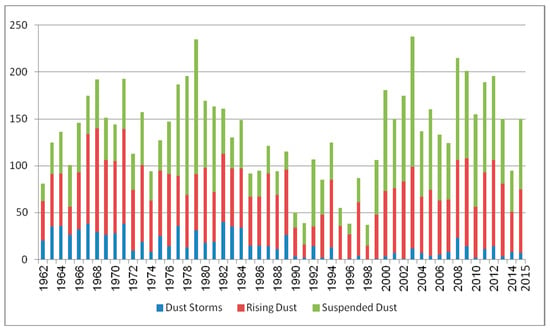
Figure 1.
Total number of dust storms (DS), rising dust (RD) and suspended dust (SD) in Kuwait, 1962–2015.
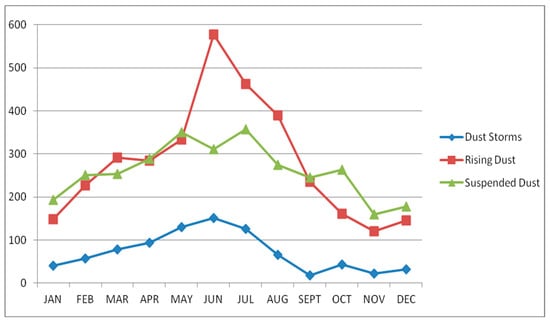
Figure 2.
Number of recorded dust storms (DS), rising dust (RD) and suspended dust (SD) by month (in ASA: Ali Sabah Al-Salem), 2012.

Table 1.
Spearman’s Rank correlation matrix between dust storms, rising dust and suspended dust in ASA, Kuwait.
Figure 3 shows that the mean daily air concentration of PM10 for the year 2012 was 361 μg/m3, which was 6.2 times higher than the 50 μg/m3 specified by the World Health Organization (WHO) air quality guidelines [4]. The highest monthly average concentration of PM10 was recorded in June (611 μg/m3) with a maximum concentration value of 3369 μg/m3, which was much higher than the Kuwait EPA maximum 24-h concentration level of 350 μg/m3 [41] (Table 2). A total of 104 days exceeded the maximum daily concentration level set by KEPA. The most probable explanation for the high PM10 concentrations in June is due to sand and dust storm (SDS) events during the summer seasons in Kuwait. As shown at the bottom of Figure 3, a total of 14 SDS events were recorded by Kuwaiti meteorological stations during 2012 of which 60% (8 SDS events) occurred during the four months of the summer season (May, June, July, and August). The month of January recorded the lowest monthly average concentration level of PM10 (141 μg/m3) with a minimum daily value of 45 μg/m3, a good justification for such low PM10 levels being related to lower SDS events in the winter season in Kuwait [24].

Figure 3.
Daily Pattern of PM10 concentration (in ASA) and number of sand and dust storms in Kuwait, 2012.
Table 2.
Descriptive statistics related to PM10 for ASA, Kuwait.
3.2. Morbidity Indicators
3.2.1. Adjusted Health Visits for Respiratory Diseases
Table 3 presents the annual adjusted health visits and average visits per 1000 person of air pollution-related respiratory and non-respiratory group of diseases in ASA health center during 2012. Annual adjusted health visits represent the total hospital admission, while the average visits represent hospital admission rate per 1000 person. Health visits may include more than one hospital admission by a single patient. Figure 4 shows the annual adjusted health visits per 1000 person of air pollution-related respiratory and non-respiratory group of diseases in ASA health center during 2012. For the respiratory group of diseases, the highest annual attendance rate was observed for acute upper respiratory tract infection (AURTI) (91,490 visits), which was followed by bronchial asthma (BA) (8075 visits), acute lower respiratory tract infection (ALRTI) (2499 visits), and other diseases of upper respiratory tract infection (other URTI) (1473 visits). However, lower attendance rates were observed for chronic lower respiratory diseases (CLRD) (20 visits), and influenza and pneumonia (IP) (14 visits). Table 4 presents the adjusted attendance rates (visits per week) to ASA health center during 2012. It shows that patients with AURTI diseases constitute the highest number with an average of 1711 visits per week, followed by bronchial asthma (148 visits per week) and ALRTI (47 visits per week).
Table 3.
Annual adjusted health visits and average visits per 1000 person of air pollution-related respiratory and non-respiratory group of diseases in ASA health center during 2012.
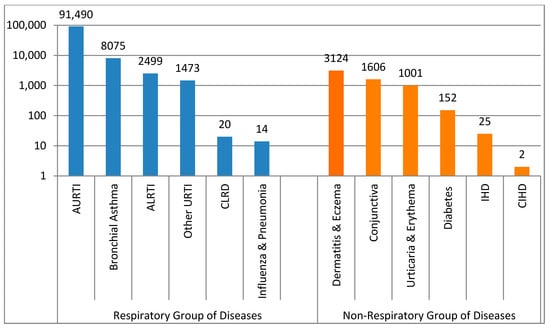
Figure 4.
Annual adjusted health visits of air pollution-related respiratory and non-respiratory diseases in Kuwait.
Table 4.
Average hospital visits for respiratory diseases (visits/week) in ASA, Kuwait.
3.2.2. Adjusted Health Visits for Non-Respiratory Diseases
The highest annual adjusted attendance visits per 1000 person for the non-respiratory group of diseases were recorded for dermatitis and eczema (DE) (3124 visits), which was followed by disorders of conjunctiva (1606 visits), urticaria and erythema (1001 visits), and diabetes mellitus (152 visits), However, ischemic heart diseases (IHD) and chronic ischemic heart diseases (CIHD) had the lowest annual attendance rates (25 and 2 visits, respectively) (Figure 4).
3.2.3. Correlation between PM10 and Morbidity
A correlation matrix is presented in Table 5 which provides the Pearson product-moment correlation between morbidity hospital visits due to respiratory diseases to ASA public health center and the PM10 concentration levels during 2012. The table shows that PM10 concentrations are significantly correlated at the 0.05 level with bronchial asthma (r = 0.292). Significant correlations at the 0.01 level were shown between bronchial asthma and both acute lower respiratory tract infection (r = 0.737) and acute upper respiratory tract infection (r = 0.839). Figure 5 shows, to some extent, a similar trend between PM10 concentrations and bronchial asthma hospital admissions during 2012 and provides more evidence of the positive relationship between PM10 concentrations and bronchial asthma attendance rates. Although high PM10 levels were recorded during June and July, which corresponded to the number of dust storms (3 in June, and 2 in July), asthma admissions were shown to be low, possibly because many people in Kuwait travel overseas during the summer vacation.
Table 5.
Pearson correlation matrix between PM10 concentration and respiratory diseases in ASA, Kuwait.

Figure 5.
PM10 concentrations and bronchial asthma admissions during 2012.
3.3. Mortality Indicators
Total death from all causes related to air pollution during 2012 in ASA was 23, corresponding to a death rate of 0.711 (23/32,341 total Kuwaiti residents in ASA). Table 6 demonstrates air pollution-related proportionate and cause-specific mortality rates in ASA during 2012. The burden of congenital anomalies and perinatal disease represent the primary causes of mortality with proportionate mortality rates of 26.1% (6/23 × 100) and 17.4% (5/23 × 100) respectively and cause-specific mortality rates of 1.86 (6/32,341 × 10,000) and 1.55 (5/32,341 × 10,000) per 10,000 persons, respectively. Congenital anomalies also known as birth defects are structural or functional metabolic disorders that occur during pregnancy and constitute a large mortality rate or long-term disability worldwide [42]. The most common severe congenital anomalies are heart defects, neural tube defects, and Down syndrome. Table 6 also shows that both respiratory and cardiovascular diseases have similar mortality rates, equal to 0.62 per 10,000 persons, each corresponding to 8.7% proportionate mortality rate.
Table 6.
Proportionate and cause-specific mortality rates in ASA during 2012, Kuwait.
4. Discussion
The health impact of dust storms and PM10 concentrations have been thoroughly studied in North America, Europe, and East Asia and to a lesser extent in Iran; however, only three studies have explored the association between dust particulates and health morbidity or mortality in Kuwait, of which two of the studies were done by the same authors [5,24]. Moreover, all regional Iranian studies [26,27,28,29,30,31,32,33,34,35,36] have used the AirQ 2.3.3 software to model the health impact of short-term exposure to PM10; this software was developed by the WHO to model European morbidity and mortality rates and may overestimate the relative risk and increase prediction error if used by non-European countries because of the obvious higher dust storm events and elevated levels of PM10 concentrations, especially in the Arabian region. This study used actual cases of morbidity and mortality and concluded that dust particulates were strongly correlated with acute lower/upper respiratory disorders and asthma. This study also revealed that dust storms, suspended dust, rising dust and PM10 followed a similar pattern throughout the studied period with high peaks during summer months, specifically in June, and lower during winter months; this finding confirms the robust link between dust storm events and ambient air PM10 levels and is in agreement with other studies in similar arid conditions [6,29,43,44]. Increased PM10 concentrations during the summer can be associated with the Middle Eastern dust storms from the arid lands of Iraq, Jordan, and Saudi Arabia which are the particular sources of dust events coming to Kuwait from the Northwest [2,29,45].
Two interesting studies by Thalib and Al-Taiar [5,24] used the generalized additive model (GAM) to analyze hospital admission and mortality data about dust storms after adjusting for covariates. This statistical model estimates the relative risk on admission and mortality counts, which typically follow a Poisson distribution, after adjusting for potential cofounders like temperature, relative humidity, weekday or weekend, and seasons as adjustment variables using various smoothing parameters. In this study, we presented correlation variables (r) derived from bivariate plots. Estimated effects from the time-series (GAM) model were not shown; however, proportionate and cause-specific mortality rates were derived using simple mathematical calculations. Statistical modeling processes of ecological time series studies are complex, and GAM models using R software (version 2.14.2) were shown to produce problematic standard errors [5]; others researchers recommend the use of S-plus software [46] which was not available during the current research study.
This study concluded that dust particulates were strongly correlated with acute lower/upper respiratory disorders and asthma. Thalib and Al-Taiar [24] showed that Kuwaiti children with asthma are particularly vulnerable to dust storm events. Other studies showed that respiratory admissions to hospitals were attributable to PM10 concentrations above 20 μg/m3 [47]. An estimated effect of 3% decline in daily forced expiratory volume (FEV1) change was observed for every 10 μg/m3 increase in ambient PM10 level [48]. Other studies showed a strong association between dust events and asthma admissions in Japan [23], Trinidad [22], Taiwan [49], South Korea [50,51] and southern Europe [52].
This study identified that cause-specific respiratory and cardiovascular mortality rates for all pollutants including PM10 ranked third after congenital anomalies and perinatal diseases. Studies of 29 European cities [53] showed an increase in daily mortality with an increase in PM10 concentrations. The impact of particulate matter on daily mortality has been shown by similar studies [54,55]; other studies demonstrated that short-term impacts of PM10 on mortality were exceeded even at concentrations complying with the European air ambient monitoring regulation [56].
Some limitations of this study are the unknown composition of the chemical and biological dust particles; future research should provide analysis of total dust and PM10 compositions and study the link between the individual components and the health impact. Another limitation of this study is that it did not consider intra-individual susceptibility to health disorders, particularly the impact of dust storms on asthma patients; further epidemiological studies are needed.
5. Conclusions
The impact of dust storms on human health has drawn great interest of research from various regions, especially in the western and east Asian countries; very little research was conducted to study the association of Arabian Peninsula dust storms or PM10 levels and associated health impact. The evidence on airborne particulates and its impact on morbidity and mortality are consistent in showing adverse health effects in both developed and developing countries. Dust storm events and PM10 concentration levels may vary across different regions in Kuwait, but only to a limited degree because of the very small geographic area (17,000 km2) and similar climatic conditions across the country. It is assumed that dust concentration variation may not be very significantly different across multiple cities and individuals are most likely to be exposed to the same level of exposure. All the population is affected, but susceptibility to the pollution may vary with health or age. Findings of this study suggest that there are strong associations between dust storms and PM10 and morbidity rates of asthma and acute upper and lower tract infections. The risk for various outcomes has been shown to increase with exposure, and there is little evidence to suggest a threshold below which no adverse health effects would be anticipated [3]. However, it may be worthwhile to further investigate the health impact of dust storm events across Kuwait, and such further evaluation can improve our understanding of the health impact of dust storms and PM10 pollutants.
Acknowledgments
The research study was initially triggered by the Kuwait Ministry of Health to assess the health impact of Ali Sabah Al-Salem area in Kuwait; the study started in the year 2000 and was completed in the year 2005. A recent project (2017) has been carried out at the Kuwait Institute for Scientific Research (KISR) and was funded by the Kuwait Environment Public Authority (KEPA) (KISR no. EC109K), through a task entitled “risk assessment study for dust storms”.
Author Contributions
Ali Al-Hemoud developed the research methodology, analyzed the data using SPSS and finished writing the manuscript; Ali Al-Dousari provided significant details on dust fallout characteristics and sandstorm trajectories and revised the manuscript; Ahmed Al-Shatti defined the health characteristics of morbidity and mortality and defined the research theme; Ahmed Al-Khayat carried out the statistical analysis using SPSS; Weam Behbehani analyzed the data and performed all figures, graphs, and tables; Mariam Malak collected the meteorological data and presented the time-series analysis of PM10 pollutants.
Conflicts of Interest
The authors declare no conflict of interest.
References and Note
- Middleton, N.J. Desert dust hazards: A global review. Aeolian Res. 2017, 24, 56–63. [Google Scholar] [CrossRef]
- Al-Dousari, A.M.; Doronzo, D.; Ahmed, M. Types, indications and impact evaluation of sand and dust storms trajectories in the Arabian Gulf. Sustainability 2017, 9, 1526. [Google Scholar] [CrossRef]
- Al-Dousari, A.M.; Al-Awadhi, J.; Ahmed, M. Dust fallout characteristics within global dust storms major trajectories. Arab. J. Geosci. 2013, 6, 3877–3884. [Google Scholar] [CrossRef]
- WHO. WHO Air Quality Guidelines for Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide: Global Update 2005: Summary of Risk Assessment; WHO, World Health Organization: Geneva, Switzerland, 2006; p. 9, WHO/SDE/PHE/OEH/06.02. [Google Scholar]
- Al-Taiar, A.; Thalib, L. Short-term effect of dust storms on the risk of mortality due to respiratory, cardiovascular and all-causes in Kuwait. Int. J. Biometeorol. 2014, 58, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Draxler, R.; Gillette, D.; Kirkpatrick, J.; Heller, J. Estimating PM10 air concentrations from dust storms in Iraq, Kuwait and Saudi Arabia. Atmos. Environ. 2001, 35, 4315–4330. [Google Scholar] [CrossRef]
- Middleton, N.; Yiallouros, P.; Kleanthous, S.; Kolokotroni, O.; Schwartz, J.; Dockery, D.W.; Demokritou, P. Koutrakis, P. A 10-year time series analysis of respiratory and cardiovascular morbidity in Nicosia, Cyprus: The effect of short-term changes in air pollution and dust storms. Environ. Health 2008, 7, 39. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.Y.; Cheng, M.H.; Chen, C.C. Effects of Asian dust storm events on hospital admissions for congestive heart failure in Taipei, Taiwan. J. Toxicol. Environ. Health 2009, 72, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.F.; Ho, S.C.; Chiu, H.F.; Wu, T.N.; Chen, P.S.; Yang, C.Y. Consequences of exposure to Asian dust storm events on daily pneumonia hospital admissions in Taipei, Taiwan. J. Toxicol. Environ. Health 2008, 71, 1295–1299. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.L.; Levy, J.K.; Lin, Z. The effect of sandstorms and air pollution on cause-specific hospital admissions in Taipei, Taiwan. Occup. Environ. Med. 2008, 65, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Sicard, P.; Lesne, O.; Alexandre, N.; Mangin, A.; Collomp, R. Air quality trends and potential health effects: Development of an aggregate risk index. Atmos. Environ. 2011, 45, 1145–1153. [Google Scholar] [CrossRef]
- Sprigg, W.A.; Nickovic, S.; Galgiani, J.N.; Pejanovic, G.; Petkovic, S.; Vujadinovic, M.; Vukovic, A.; Dacic, M.; DiBiase, S.; Prasad, A.; et al. Regional dust storm modeling for health services: The case of valley fever. Aeolian Res. 2014, 14, 53–73. [Google Scholar] [CrossRef]
- Schwartz, J.; Norris, G.; Larson, T.; Sheppard, L.; Claiborne, C.; Koenig, J. Episodes of high coarse particle concentrations are not associated with increased mortality. Environ. Health Perspect. 1999, 107, 339–342. [Google Scholar] [CrossRef] [PubMed]
- Xie, S.; Yu, T.; Zhang, Y.; Zeng, L.; Qi, L.; Tang, X. Characteristics of PM10, SO2, NOx and O3 in ambient air during the dust storm period in Beijing. Sci. Total Environ. 2005, 345, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Perez, L.; Tobias, A.; Querol, X.; Kunzli, N.; Pey, J.; Alastuey, A.; Viana, M.; Valero, N.; Gonzalez-Cabre, M.; Sunyer, J. Coarse particles from Saharan dust and daily mortality. Epidemiology 2008, 19, 800–807. [Google Scholar] [CrossRef] [PubMed]
- Ostro, B.D.; Hurley, S.; Lipsett, M.J. Air pollution and daily mortality in the Coachella Valley, California: A study of PM10 dominated by coarse particles. Environ. Res. 1999, 81, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.S.; Sheen, P.C.; Chen, E.R.; Liu, Y.K.; Wu, T.N.; Yang, C.Y. Effect of Asian dust storm events on daily mortality in Taipei, Taiwan. Environ. Res. 2004, 95, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.J.; Cho, S.H.; Chun, Y.; Lagarde, F.; Pershagen, G. Effects of the Asian dust events on daily mortality in Seoul, Korea. Environ. Res. 2002, 90, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Tao, Y.; An, X.; Sun, Z.; Hou, Q.; Wang, Y. Association between dust weather and number of admissions for patients with respiratory diseases in spring in Lanzhou. Sci. Total Environ. 2012, 423, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.J. The impact of air pollution on human health in Suwon city. Asian J. Atmos. Environ. 2013, 7, 227–233. [Google Scholar] [CrossRef]
- Barnett, A.G.; Fraser, J.F.; Munck, L. The effects of the 2009 dust storm on emergency admissions to a hospital in Brisbane, Australia. Int. J. Biometeorol. 2012, 56, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Gyan, K.; Henry, W.; Lacaille, S.; Laloo, A.; Lamsee-Ebanks, C.; McKay, S.; Antonie, R.M.; Monteil, M.A. African dust clouds are associated with increased pediatric asthma accident and emergency admissions on the Caribbean island of Trinidad. Int. J. Biometeorol. 2005, 49, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Kanatani, K.T.; Ito, I.; Al-Delaimy, W.K.; Adachi, Y.; Mathews, W.C.; Ramsdell, J.W. Desert dust exposure is associated with increased risk of asthma hospitalization in children. Am. J. Respir. Crit. Care Med. 2010, 182, 1475–1481. [Google Scholar] [CrossRef] [PubMed]
- Thalib, L.; Al-Taiar, A. Dust storms and the risk of asthma admissions to hospitals in Kuwait. Sci. Total Environ. 2012, 433, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Washington, R.; Todd, M.; Middleton, N.J.; Goudie, A.S. Dust-storm source areas determined by the total ozone monitoring spectrometer and surface observations. Ann. Assoc. Am. Geogr. 2003, 93, 297–313. [Google Scholar]
- Miri, M.; Aval, H.E.; Ehrampoush, M.H.; Mohammadi, A.; Toolabi, A.; Nikonahad, A.; Derakhshan, Z.; Abdollahnejad, A. Human health impact assessment of exposure to particulate matter: An AirQ software modeling. Envirorn. Sci. Pollut. R. 2017, 24, 16513–16519. [Google Scholar] [CrossRef] [PubMed]
- Miri, M.; Derakhshan, Z.; Allahabadi, A.; Ahmadi, E.; Conti, G.O.; Ferrante, M.; Aval, H.E. Mortality and morbidity due to exposure to outdoor air pollution in Mashhad metropolis, Iran: The AirQ model approach. Environ. Res. 2016, 151, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Goudarzi, G.; Daryanoosh, S.M.; Godini, H.; Hopke, P.K.; Sicard, P.; De Marco, A.; Rad, H.D.; Habizadeh, A.; Jahedi, F.; Mohammadi, M.J.; et al. Health risk assessment of exposure to the Middle-Eastern dust storms in the Iranian megacity of Kermanshah. Public Health 2017, 148, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Nourmoradi, H.; Khaniabadi, Y.O.; Goudarzi, G.; Daryanoosh, S.M.; Khoshgoftar, M.; Omidi, F.; Armin, A. Air quality and health risks associated with exposure to particulate matter: A cross-sectional study in Khorramabad, Iran. Health Scope 2016, 5. [Google Scholar] [CrossRef]
- Mohammadi, A.; Azhdarpoor, A.; Shahsavani, A.; Tabatabaee, H. Health impacts of exposure to PM10 on inhabitants of Shiraz, Iran. Health Scope 2015, 4. [Google Scholar] [CrossRef]
- Zallaghi, E.; Goudarzi, G.; Geravandi, S.; Mohammadi, M.J. Epidemiological Indexes Attributed to Particulates With Less Than 10 Micrometers in the Air of Ahvaz City During 2010 to 2013. Health Scope 2014, 3. [Google Scholar] [CrossRef]
- Daryanoosh, M.; Goudarzi, G.; Rashidi, R.; Keishams, F.; Hopke, P.K.; Mohammadi, M.J.; Nourmoradi, H.; Sicard, P.; Takdastan, A.; Vosoughi, M.; et al. Risk of morbidity attributed to ambient PM10 in western cities of Iran. Toxin Rev. 2017. [Google Scholar] [CrossRef]
- Khaniabadi, Y.O.; Daryanoosh, S.Y.; Amrane, A.; Polosa, R.; Hopke, P.K.; Goudarzi, G.; Mohammadi, M.J.; Sicard, P.; Armin, H. Impacts of Middle Eastern dust storms on human health. Atmos. Pollut. Res. 2017, 8, 606–613. [Google Scholar] [CrossRef]
- Geravandi, S.; Sicard, P.; Khaniabadi, Y.O.; De Marco, A.; Ghomeishi, A.; Goudarzi, G.; Mahboubi, M.; Yari, A.R.; Dobaradaran, S.; Hassani, G.; et al. A comparative study of hospital admissions for respiratory diseases during normal and dusty days in Iran. Environ. Sci. Pollut. Res. 2017, 4, 18152–18159. [Google Scholar] [CrossRef] [PubMed]
- Gharehchahi, E.; Mahvi, A.; Amini, H.; Nabizadeh, R.; Akhlaghi, A.; Shamsipour, M.; Yunesian, M. Health impact assessment of air pollution in Shiraz, Iran: A two-part study. Iran. J. Environ. Health 2013, 11. [Google Scholar] [CrossRef] [PubMed]
- Naddafi, K.; Hassanvand, M.S.; Yunesian, M.; Momeniha, F.; Nabizadeh, R.; Faridi, S.; Gholampour, A. Health impact assessment of air pollution in megacity of Tehran, Iran. Iran. J. Environ. Health 2012, 9. [Google Scholar] [CrossRef] [PubMed]
- Al-Rifaia, N.; Elmi, A.; Khan, A.R. Exploring possible seasonal trends in mortality rate in relation to age, gender and environmental conditions in Kuwait: A preliminary analysis. J. Eng. Res.-Kuwait 2011, 8, 19–27. [Google Scholar] [CrossRef]
- International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) Version for 2010. Chapter X. Available online: http://apps.who.int/classifications/icd10/browse/2010/en (accessed on 29 November 2016).
- McTainish, G.H.; Pitbaldo, J.R. Dust storms and related phenomena measured from meteorological records in Australia. Earth Surf. Process. 1987, 12, 415–424. [Google Scholar] [CrossRef]
- World Meteorological Organization (WMO). Climate Change and Land Degradation WMO-No 989; WMO: Geneva, Switzerland, 2005; ISBN 92-63-10989-3. [Google Scholar]
- KEPA, Kuwait EPA Regulations concerning the safety of workers in all establishments and the requirements and criteria for adequate ventilation in enclosed and semi-enclosed public places. Articles 19 and 20 of Kuwait Environmental Protection Act No. 42, Kuwait Al-Youm No. 1341, 2014.
- Congenital Anomalies, Fact Sheet, World Health Organization. Updated 2016. Available online: http://www.who.int/mediacentre/factsheets/ fs370/en (accessed on 1 September 2016).
- Mirhosseini, S.H.; Birjandi, M.; Zare, M.R.; Fatehizadeh, A. Analysis of Particulate matter (PM10 and PM2.5) concentration in Khorramabad city. Int. J. Environ. Health Eng. 2013, 2. [Google Scholar] [CrossRef]
- Shahsavani, A.; Naddafi, K.; Jafarzade, H.N.; Mesdaghinia, A.; Yunesian, M.; Nabizadeh, R.; Arahami, M.; Sowlat, M.H.; Yarahmadi, M.; Saki, H. The evaluation of PM10, PM2.5, and PM1 concentrations during the Middle Eastern Dust (MED) events in Ahvaz, Iran, from April through September 2010. J. Arid Environ. 2012, 77, 72e83. [Google Scholar] [CrossRef]
- Al-Hemoud, A.; Al-Sudairawi, M.; Neelamanai, S.; Naseeb, A.; Behbehani, W. Socioeconomic effect of dust storms in Kuwait. Arab. J. Geosci. 2017, 10. [Google Scholar] [CrossRef]
- Dominici, F.; McDermott, A.; Hastie, T.J. Improved semiparametric time series models of air pollution and mortality. J. Am. Stat. Assoc. 2004, 99, 938–948. [Google Scholar] [CrossRef]
- Tominz, R.; Mazzoleni, B.; Daris, F. Estimate of potential health benefits of the reduction of air pollution with PM10 in Trieste, Italy. Epidemiol. Prev. 2005, 29, 149–155. [Google Scholar] [PubMed]
- Brauer, M.; Ebelt, S.T.; Fisher, T.V.; Brumm, J.; Petkau, A.J.; Vedal, S. Exposure of chronic obstructive pulmonary disease patients to particles: Respiratory and cardiovascular health effects. J. Expo. Anal. Environ. Epidemiol. 2001, 11, 490–500. [Google Scholar] [CrossRef] [PubMed]
- Tam, W.; Wong, T.; Wong, A.; Hui, D. Effect of dust storm events on daily emergency admissions for respiratory diseases. Respirology 2012, 17, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.C.; Pan, X.C.; Kim, S.Y.; Park, K.; Park, E.J.; Jin, X.; Yi, S.M.; Kim, Y.H.; Park, C.H.; Song, S.; et al. Asian dust storm and pulmonary function of school children in Seoul. Sci. Total Environ. 2010, 408, 754–759. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Lee, K.K. Effects of Asian dust events on daily asthma in Seoul, Korea. Meteorol. Appl. 2014, 21, 202–209. [Google Scholar] [CrossRef]
- Stafoggia, M.; Zauli-Sajan, S.; Pey, J.; Samoli, J.; Alessandrini, E.; Basagaña, X.; Cernigliaro, A.; Chiusolo, M.; Demaria, M.; Díaz, J.; et al. Desert Dust Outbreaks in Southern Europe: Contribution to Daily PM10 Concentrations and Short-Term Associations with Mortality and Hospital Admissions. Environ. Health Perspect. 2016, 124, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Katsouyanni, K.; Touloumi, G.; Samoli, E.; Gryparis, A.; Le Tertre, A.; Monopolis, Y.; Rossi, G.; Zmirou, D.; Ballester, F.; Boumghar, A.; et al. Confounding and effect modification in the short-term effects of ambient particles on total mortality: Results from 29 European cities within the APHEA2 project. Epidemiology 2001, 12, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Tobias, A.; Perez, L.; Diaz, J.; Linares, C.; Pey, J.; Alastruey, A.; Querol, X. Short-term effects of particulate matter on total mortality during Saharan dust outbreaks: A case-crossover analysis in Madrid (Spain). Sci. Total Environ. 2011, 412–413, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Janssen, N.; Fischer, P.; Marra, M.; Ameling, C.; Cassee, F. Short-term effects of PM2.5, PM10 and PM2.5–10 on daily mortality in the Netherlands. Sci. Total Environ. 2013, 463, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Corso, M.; Blanchard, M.; Host, S.; Pascal, L.; Larrieu, S. Short-term impacts of particulate matter (PM10, PM10–2.5, PM2.5) on mortality in nine French cities. Atmos. Environ. 2014, 95, 175–184. [Google Scholar]
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).