
The Hypothesis of the Interplay Between Air Particulate Matter PM2.5 and Acute Cellular Rejection Episodes Following Heart Transplantation

 ,
,  , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Method
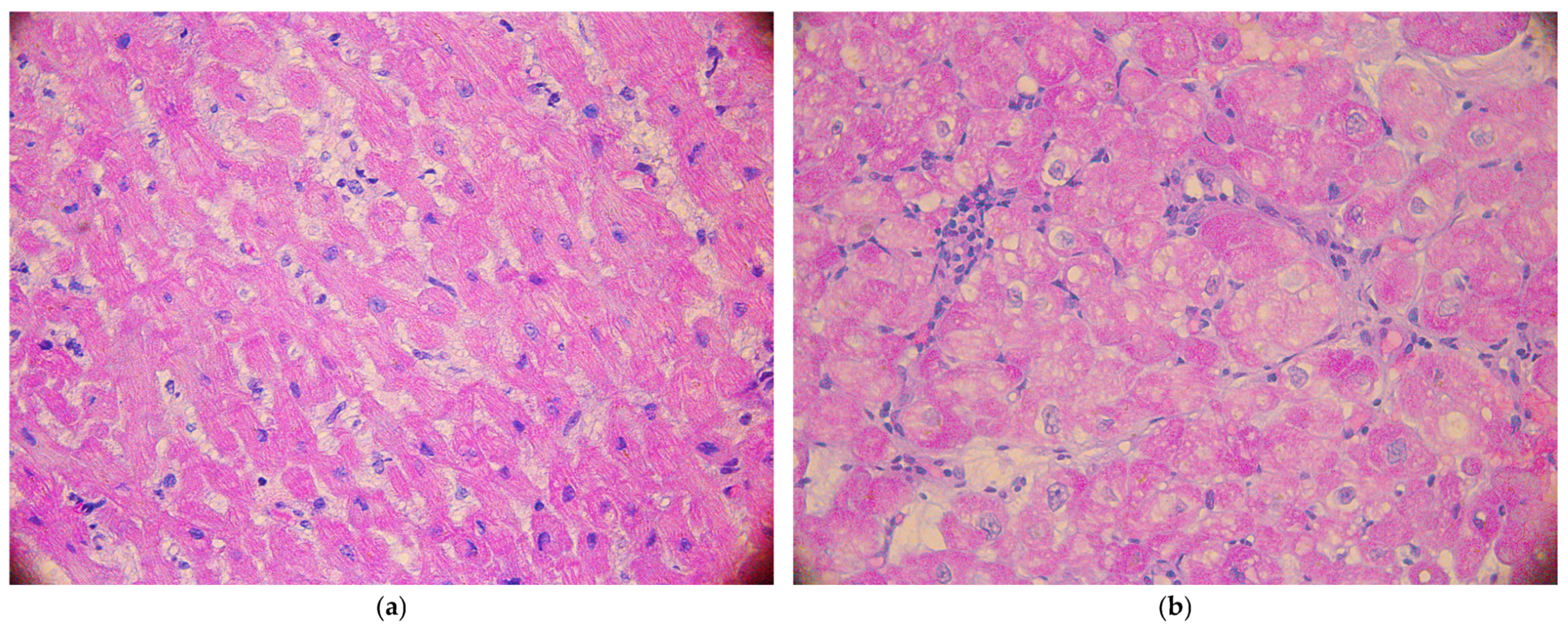
2.3. Endomyocardial Biopsies
2.4. Personalized Calculations of Air Pollution Exposure in Habitation Place
2.5. Statistical Analysis
2.6. Bioethics Committee
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Savarese, G.; Becher, P.M.; Lund, L.H.; Seferovic, P.; Rosano, G.M.C.; Coats, A.J.S. Global burden of heart failure: A comprehensive and updated review of epidemiology. Cardiovasc. Res. 2023, 118, 3272–3287. [Google Scholar] [CrossRef]
- Siopi, S.A.; Antonitsis, P.; Karapanagiotidis, G.T.; Tagarakis, G.; Voucharas, C.; Anastasiadis, K. Cardiac Failure and Cardiogenic Shock: Insights into Pathophysiology, Classification, and Hemodynamic Assessment. Cureus 2024, 16, e72106. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2023, 44, 3627–3639. [Google Scholar] [CrossRef] [PubMed]
- Crespo-Leiro, M.G.; Barge-Caballero, E. Advanced Heart Failure: Definition, Epidemiology, and Clinical Course. Heart Fail. Clin. 2021, 17, 533–545. [Google Scholar] [CrossRef] [PubMed]
- Kong, D.; Huang, S.; Miao, X.; Li, J.; Wu, Z.; Shi, Y.; Liu, H.; Jiang, Y.; Yu, X.; Xie, M.; et al. The dynamic cellular landscape of grafts with acute rejection after heart transplantation. J. Heart Lung Transplant. 2023, 42, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Kopecky, B.J.; Dun, H.; Amrute, J.M.; Lin, C.Y.; Bredemeyer, A.L.; Terada, Y.; Bayguinov, P.O.; Koenig, A.L.; Frye, C.C.; Fitzpatrick, J.A.J.; et al. Donor Macrophages Modulate Rejection After Heart Transplantation. Circulation 2022, 146, 623–638. [Google Scholar] [CrossRef]
- Kim, J.V.; Assadian, S.; Hollander, Z.; Burns, P.; Shannon, C.P.; Lam, K.; Toma, M.; Ignaszewski, A.; Davies, R.A.; Delgado, D.; et al. Regulatory T Cell Biomarkers Identify Patients at Risk of Developing Acute Cellular Rejection in the First Year Following Heart Transplantation. Transplantation 2023, 107, 1810–1819. [Google Scholar] [CrossRef]
- Duchesne, M.; Okoye, I.; Lacy, P. Epithelial cell alarmin cytokines: Frontline mediators of the asthma inflammatory response. Front. Immunol. 2022, 13, 975914. [Google Scholar] [CrossRef]
- Sanches, T.R.; Parra, A.C.; Sun, P.; Graner, M.P.; Itto, L.Y.U.; Butter, L.M.; Claessen, N.; Roelofs, J.J.; Florquin, S.; Veras, M.M.; et al. Air pollution aggravates renal ischaemia-reperfusion-induced acute kidney injury. J. Pathol. 2024, 263, 496–507. [Google Scholar] [CrossRef]
- Jin, X.; Chen, Y.; Xu, B.; Tian, H. Exercise-Mediated Protection against Air Pollution-Induced Immune Damage: Mechanisms, Challenges, and Future Directions. Biology 2024, 13, 247. [Google Scholar] [CrossRef]
- Bellinato, F.; Adami, G.; Vaienti, S.; Benini, C.; Gatti, D.; Idolazzi, L.; Fassio, A.; Rossini, M.; Girolomoni, G.; Gisondi, P. Association Between Short-term Exposure to Environmental Air Pollution and Psoriasis Flare. JAMA Dermatol. 2022, 158, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Argacha, J.F. Effets de la pollution de l’air sur les évènements cardiovasculaires en unité de soins intensifs cardiologiques [Effects of air pollution on cardiovascular events in cardiac intensive care units]. Ann. Cardiol. Angeiol. 2023, 72, 101663. [Google Scholar] [CrossRef] [PubMed]
- Honda, A.; Okuda, T.; Nagao, M.; Miyasaka, N.; Tanaka, M.; Takano, H. PM2.5 collected using cyclonic separation causes stronger biological responses than that collected using a conventional filtration method. Environ. Res. 2021, 198, 110490. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; He, W.; Yue, H.; Zhao, P.; Li, J. Effective-components combination alleviates PM2.5-induced inflammation by evoking macrophage autophagy in COPD. J. Ethnopharmacol. 2024, 321, 117537. [Google Scholar] [CrossRef]
- Billingham, M.E.; Cary, N.R.; Hammond, M.E.; Kemnitz, J.; Marboe, C.; McCallister, H.A.; Snovar, D.C.; Winters, G.L.; Zerbe, A. A working formulation for the standardization of nomenclature in the diagnosis of heart and lung rejection: Heart Rejection Study Group. The International Society for Heart Transplantation. J. Heart Transplant. 1990, 9, 587–593. [Google Scholar]
- Urbanowicz, T.; Skotak, K.; Olasińska-Wiśniewska, A.; Filipiak, K.J.; Bratkowski, J.; Wyrwa, M.; Sikora, J.; Tyburski, P.; Krasińska, B.; Krasiński, Z.; et al. Long-Term Exposure to PM10 Air Pollution Exaggerates Progression of Coronary Artery Disease. Atmosphere 2024, 15, 216. [Google Scholar] [CrossRef]
- Available online: https://powietrze.gios.gov.pl/pjp/maps/modeling (accessed on 20 July 2018).
- Tagaris, E.; Sotiropoulou, R.E.P.; Gounaris, N.; Andronopoulos, S.; Vlachogiannis, D. Effect of the Standard Nomenclature for Air Pollution (SNAP) categories on air quality over Europe. Atmosphere 2015, 6, 1119–1128. [Google Scholar] [CrossRef]
- Chrysakis, N.; Magouliotis, D.E.; Spiliopoulos, K.; Athanasiou, T.; Briasoulis, A.; Triposkiadis, F.; Skoularigis, J.; Xanthopoulos, A. Heart Transplantation. J. Clin. Med. 2024, 13, 558–576. [Google Scholar] [CrossRef]
- Agbor-Enoh, S.; Shah, P.; Tunc, I.; Hsu, S.; Russell, S.; Feller, E.; Shah, K.; Rodrigo, M.E.; Najjar, S.S.; Kong, H.; et al. Cell-Free DNA to Detect Heart Allograft Acute Rejection. Circulation 2021, 143, 1184–1197. [Google Scholar] [CrossRef]
- Pérez-Carrillo, L.; Giménez-Escamilla, I.; Sánchez-Lázaro, I.; Triviño, J.C.; Feijóo-Bandín, S.; Lago, F.; González-Juanatey, J.R.; Martínez-Dolz, L.; Portolés, M.; Tarazón, E.; et al. Alpha-cardiac Actin Serum Expression Levels Detect Acute Cellular Rejection in Heart Transplant Patients. Transplantation 2023, 107, 466–474. [Google Scholar] [CrossRef]
- Sutaria, N.; Sylvia, L.; DeNofrio, D. Immunosuppression and Heart Transplantation. Handb. Exp. Pharmacol. 2022, 272, 117–137. [Google Scholar] [PubMed]
- Paintner, P.; Lehner, A.; Riley, R.; Fischer, M.; Kozlik-Feldmann, R.; Rosenthal, L.; Orban, M.; Jakob, A.; Haas, N.; Ulrich, S. Comparison of the Prolonged- and Immediate-Release Tacrolimus Capsule Formulation: The Patient’s View and Medication Satisfaction of Patients After Pediatric Heart Transplantation. Transplant. Proc. 2023, 55, 1656–1663. [Google Scholar] [CrossRef] [PubMed]
- Panackel, C.; Mathew, J.F.; Fawas, N.M.; Jacob, M. Immunosuppressive Drugs in Liver Transplant: An Insight. J. Clin. Exp. Hepatol. 2022, 12, 1557–1571. [Google Scholar] [CrossRef] [PubMed]
- Urbanowicz, T.; Straburzyńska-Migaj, E.; Casadei, V.; Bociański, M.; Jemielity, M. Different Routes of Proton Pumps Inhibitors Co-Administration have Significant Impact on Mycophenolate Acid (MPA) Serum Levels in Heart Transplant Recipients. Ann. Transplant. 2020, 25, e920225. [Google Scholar] [CrossRef]
- Barshes, N.R.; Goodpastor, S.E.; Goss, J.A. Pharmacologic immunosuppression. Front. Biosci. 2004, 9, 411–420. [Google Scholar] [CrossRef]
- Velleca, A.; Shullo, M.A.; Dhital, K.; Azeka, E.; Colvin, M.; DePasquale, E.; Farrero, M.; García-Guereta, L.; Jamero, G.; Khush, K.; et al. The International Society for Heart and Lung Transplantation (ISHLT) guidelines for the care of heart transplant recipients. J. Heart Lung Transplant. 2023, 42, e1–e141. [Google Scholar]
- Brunet, M.; van Gelder, T.; Åsberg, A.; Haufroid, V.; Hesselink, D.A.; Langman, L.; Lemaitre, F.; Marquet, P.; Seger, C.; Shipkova, M.; et al. Therapeutic Drug Monitoring of Tacrolimus-Personalized Therapy: Second Consensus Report. Ther. Drug Monit. 2019, 41, 261–307. [Google Scholar] [CrossRef]
- Zhang, B.; Weuve, J.; Langa, K.M.; D’Souza, J.; Szpiro, A.; Faul, J.; Mendes de Leon, C.; Gao, J.; Kaufman, J.D.; Sheppard, L.; et al. Comparison of Particulate Air Pollution from Different Emission Sources and Incident Dementia in the US. JAMA Intern. Med. 2023, 183, 1080–1089. [Google Scholar] [CrossRef]
- Thangavel, P.; Park, D.; Lee, Y.C. Recent Insights into Particulate Matter (PM2.5)-Mediated Toxicity in Humans: An Overview. Int. J. Environ. Res. Public Health 2022, 19, 7511–7533. [Google Scholar] [CrossRef]
- Hou, T.; Zhu, L.; Wang, Y.; Peng, L. Oxidative stress is the pivot for PM2.5-induced lung injury. Food Chem. Toxicol. 2024, 184, 114362. [Google Scholar] [CrossRef]
- Henning, R.J. Particulate Matter Air Pollution is a Significant Risk Factor for Cardiovascular Disease. Curr. Probl. Cardiol. 2024, 49, 102094. [Google Scholar] [CrossRef] [PubMed]
- Urbanowicz, T.; Skotak, K.; Olasińska-Wiśniewska, A.; Szczepański, K.; Tykarski, A.; Jemielity, M. Five-year mortality disparities across urban and rural areas in patients treated with coronary artery bypass grafting. Pol. Arch. Intern. Med. 2024, 134, 16847–16852. [Google Scholar] [CrossRef] [PubMed]
- Urbanowicz, T.; Skotak, K.; Olasińska-Wiśniewska, A.; Filipiak, K.J.; Płachta-Krasińska, A.; Piecek, J.; Krasińska, B.; Krasiński, Z.; Tykarski, A.; Jemielity, M. The Possible Role of PM2.5 Chronic Exposure on 5-Year Survival in Patients with Left Ventricular Dysfunction Following Coronary Artery Bypass Grafting. Toxics 2024, 12, 697–707. [Google Scholar] [CrossRef] [PubMed]
- Yuan, G.; Liu, Y.; Wang, Z.; Wang, X.; Han, Z.; Yan, X.; Meng, A. PM2.5 activated NLRP3 inflammasome and IL-1β release in MH-S cells by facilitating autophagy via activating Wnt5a. Int. J. Immunopathol. Pharmacol. 2022, 36, 3946320221137464. [Google Scholar] [CrossRef]
- Feng, Y.; Jones, M.R.; Ahn, J.B.; Garonzik-Wang, J.M.; Segev, D.L.; McAdams-DeMarco, M. Ambient air pollution and posttransplant outcomes among kidney transplant recipients. Am. J. Transplant. 2021, 21, 3333–3345. [Google Scholar] [CrossRef]
- Amubieya, O.; Weigt, S.; Shino, M.Y.; Jackson, N.J.; Belperio, J.; Ong, M.K.; Norris, K. Ambient Air Pollution Exposure and Outcomes in Patients Receiving Lung Transplant. JAMA Netw. Open 2024, 7, e2437148. [Google Scholar] [CrossRef]
- Chang, S.H.; Merzkani, M.; Murad, H.; Wang, M.; Bowe, B.; Lentine, K.L.; Al-Aly, Z.; Alhamad, T. Association of Ambient Fine Particulate Matter Air Pollution with Kidney Transplant Outcomes. JAMA Netw. Open 2021, 4, e2128190. [Google Scholar] [CrossRef]
- Choi, D.; North, M.; Ahmed, M.; Belousova, N.; Vasileva, A.; Matelski, J.; Singer, L.G.; Wu, J.K.Y.; Jeong, C.H.; Evans, G.; et al. Pollution exposure in the first 3 months post transplant is associated with lower baseline FEV1 and higher CLAD risk. J. Heart Lung Transplant. 2024, 43, 1987–1997. [Google Scholar] [CrossRef]
- Al-Kindi, S.G.; Sarode, A.; Zullo, M.; Brook, J.; Burnett, R.; Oliveira, G.H.; Huang, W.; Brook, R.; Rajagopalan, S. Ambient Air Pollution and Mortality After Cardiac Transplantation. J. Am. Coll. Cardiol. 2019, 74, 3026–3035. [Google Scholar] [CrossRef]
- Gemelli, M.; Doulamis, I.P.; Tzani, A.; Rempakos, A.; Kampaktsis, P.; Alvarez, P.; Guariento, A.; Xanthopoulos, A.; Giamouzis, G.; Spiliopoulos, K.; et al. Rejection Requiring Treatment within the First Year following Heart Transplantation: The UNOS Insight. J. Pers. Med. 2023, 14, 52–64. [Google Scholar] [CrossRef]
- Shi, Y.Y.; Hesselink, D.A.; van Gelder, T. Pharmacokinetics and pharmacodynamics of immunosuppressive drugs in elderly kidney transplant recipients. Transplant. Rev. 2015, 29, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Urbanowicz, T.; Skotak, K.; Olasińska-Wiśniewska, A.; Filipiak, K.J.; Bratkowski, J.; Krasińska, B.; Krasiński, Z.; Tykarski, A.; Jemielity, M. The Interplay between Dyslipidemia and Neighboring Developments in Coronary Artery Disease Progression: A Personalized Approach. J. Pers. Med. 2024, 14, 237–251. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Whole Group n = 30 | Rejection Group n = 8 | Control Group n = 22 | p Rejection vs. Control Group |
|---|---|---|---|---|
| Recipients | ||||
| Demographic: | ||||
| Age (years) (median (Q1–Q3) | 49 (38–60) | 60 (55–62) | 46 (38–57) | 0.046 |
| Sex (male (%)/female (%)) | 25 (83)/5 (17) | 5 (62)/3 (38) | 20 (91)/2 (9) | 0.075 |
| BMI (kg/m2) (median (Q1–Q3) | 25.3 (23.5–28.7) | 25.1 (24.3–26.5) | 26.1 (22.6–29.7) | 0.639 |
| Primary diagnosis: | ||||
| DCM (n (%)) | 17 (57) | 2 (25) | 15 (68) | 0.041 |
| ICM (n (%)) | 6 (20) | 4 (50) | 2 (9) | 0.016 |
| Other (n (%)) | 7 (23) | 2 (25) | 5 (23) | 1.000 |
| Co-morbidities: | ||||
| Arterial hypertension (n (%)) | 10 (33) | 3 (38) | 7 (32) | 0.796 |
| Dyslipidemia (n (%)) | 9 (30) | 3 (38) | 6 (27) | 0.616 |
| Kidney dysfunction (n (%)) | 6 (20) | 1 (13) | 5 (23) | 0.565 |
| Diabetes mellitus (n (%)) | 5 (17) | 2 (50) | 3 (14) | 0.490 |
| COPD (n (%)) | 3 (10) | 0 (0) | 3 (14) | 0.545 |
| Smoking (n (%)) | 6 (20) | 0 (0) | 6 (27) | 0.155 |
| Donors | ||||
| Demographic: | ||||
| Age (years) (median (Q1–Q3) | 31 (26–41) | 30 (25–38) | 32 (27–43) | 0.756 |
| Sex (male (%)/female (%)) | 27 (90)/3 (10) | 7 (87)/1 (13) | 20 (91)/2 (9) | 1.000 |
| BMI (kg/m2) (median (Q1–Q3) | 23 (20–25) | 23 (21–24) | 23 (19–25) | 0.812 |
| Parameters | Whole Group n = 30 | Rejection Group n = 8 | Control Group n = 22 | p Rejection vs. Control Group |
|---|---|---|---|---|
| 1st EMB | ||||
| Time after HTX (days) (median (Q1–Q3) | 21 (17–28) | 20 (19–28) | 22 (17–28) | 0.925 |
| Immunosupression: | ||||
| TACR daily dose (mg) (median (Q1–Q3) | 6.0 (4.0–7.8) | 6.0 (3.0–6.3) | 6.0 (4.0–8.0) | 0.523 |
| TACR serum concetration (ng/mL) (median (Q1–Q3) | 13.9 (11.5–17.9) | 17.6 (11.6–22.1) | 13.6 (11.5–17.0) | 0.341 |
| MMF daily dose (g) (median (Q1–Q3) | 2.5 (1.6–3.0) | 2.0 (1.5–2.6) | 2.5 (2.0–3.0) | 0.239 |
| MMF level (ug/mL) (median (Q1–Q3) | 2.9 (1.8–4.8) | 4.90 (2.48–5.23) | 2.75 (1.88–3.68) | 0.273 |
| Steroid daily dose | 45 (30–65) | 55 (30–60) | 45 (21.3–62.5) | 0.918 |
| Echocardiography | ||||
| LVEDD (mm) (median (Q1–Q3) | 45 (43–48) | 43 (41–47) | 45 (44–48) | 0.945 |
| LVEF (%) (median (Q1–Q3) | 65 (65–68) | 65 (65–68) | 66 (65–68) | 1.000 |
| EMB results: | ||||
| no-ACR (n (%)) | 27 (90) | 5 (63) | 22 (100) | 0.014 |
| ACR (n (%)) | 3 (10) | 3 (37) | 0 (0) | |
| 2nd EMB | ||||
| Time after HTX (days) (median (Q1–Q3) | 35 (31–42) | 32 (29–36) | 36 (30–44) | 0.118 |
| Immunosupression: | ||||
| TACR daily dose (mg) (median (Q1–Q3) | 6.0 (5.0–7.8) | 5.8 (5.0–7.0) | 6.0 (4.3–7.8) | 0.687 |
| TACR serum concetration (ng/mL) (median (Q1–Q3) | 15.3 (11.4–18.4) | 17.7 (16.2–20.6) | 13.9 (11.0–18.3)) | 0.079 |
| MMF daily dose (g) (median (Q1–Q3) | 2.0 (1.5–2.5) | 1.8 (1.5–2.1) | 2.0 (1.5–2.9) | 0.466 |
| MMF level (ug/mL) (median (Q1–Q3) | 2.7 (1.8–3.9) | 1.8 (1.4–2.8) | 2.8 (1.9–4.3) | 0.184 |
| Steroid daily dose | 35 (15–50) | 45 (28–55) | 35 (16–44) | |
| Echocardiography | ||||
| LVEDD (mm) (median (Q1–Q3) | 43 (41–46) | 42 (42–44) | 43 (40–47) | 0.439 |
| LVEF (%) (median (Q1–Q3) | 68 (65–68) | 65 (62–67) | 68 (65–68) | 0.092 |
| EMB results: | ||||
| no-ACR (n (%)) | 29 (90) | 7 (88) | 22 (100) | 0.267 |
| ACR (n (%)) | 1 (10) | 1 (12) | 0 (0) | |
| 3rd EMB | ||||
| Time after HTX (days) (median (Q1–Q3) | 69 (57–77) | 68 (54–76) | 70 (58–78) | 0.205 |
| Immunosupression: | ||||
| TACR daily dose (mg) (median (Q1–Q3) | 5.0 (4.0–7.0) | 3.5 (2.8–5.8) | 5.0 (4.3–7.0) | 0.228 |
| TACR serum concetration (ng/mL) (median (Q1–Q3) | 13.2 (10.9–16.0) | 15.7 (13.2–16.7) | 12.7 (10.9–15.2) | 0.270 |
| MMF daily dose (g) (median (Q1–Q3) | 1.5 (1.5–2.0) | 2.0 (1.5–2.0) | 1.5 (1.5–2.1) | 0.889 |
| MMF level (ug/mL) (median (Q1–Q3) | 2.8 (1.7–3.8) | 2.4 (0.8–3.5) | 2.4 (1.7–4.2) | 0.366 |
| Steroid daily dose | 25 (15–40) | 40 (30–40) | 23 (11–30) | 0.076 |
| Echocardiography | ||||
| LVEDD (mm) (median (Q1–Q3) | 45 (42–49) | 43 (39–47) | 46 (43–50) | 0.519 |
| LVEF (%) (median (Q1–Q3) | 65 (65–68) | 65 (63–67) | 68 (65–70) | 0.321 |
| EMB results: | ||||
| no-ACR (n (%)) | 28 (93) | 6 (75) | 22 (100) | 0.064 |
| ACR (n (%)) | 2 (7) | 2 (25) | 0 (0) | |
| 4th EMB | ||||
| Time after HTX (days) (median (Q1–Q3) | 92 (82–97) | 79 (67–96) | 92 (90–99) | 0.259 |
| Immunosupression: | ||||
| TACR daily dose (mg) (median (Q1–Q3) | 3.8 (3.2–5.2) | 3.3 (3.0–5.5) | 4.0 (3.3–5.0) | 0.867 |
| TACR serum concetration (ng/mL) (median (Q1–Q3) | 12.8 (11.0–15.2) | 12.9 (11.2–14.7) | 12.7 (10.4–16.2) | 0.729 |
| MMF daily dose (g) (median (Q1–Q3) | 1.8 (1.5–1.9) | 2.0 (1.5–2.0) | 1.5 (1.5–2.1) | 0.077 |
| MMF level (ug/mL) (median (Q1–Q3) | 4.6 (3.2–6.1) | 4.0 (2.9–5.5) | 5.0 (4.0–7.0) | 0.213 |
| Steroid daily dose | 15.7 (14–20) | 17.5 (15–20) | 15 (13–20) | 0.639 |
| Echocardiography | ||||
| LVEDD (mm) (median (Q1–Q3) | 45 (42–49) | 43 (39–47) | 45 (42–50) | 0.174 |
| LVEF (%) (median (Q1–Q3) | 65 (63–68) | 65 (62–67) | 65 (63–68) | 0.899 |
| EMB results: | ||||
| no-ACR (n (%)) | 28 (93) | 6 (75) | 22 (100) | 0.064 |
| ACR (n (%)) | 2 (7) | 2 (25) | 0 (0) | |
| Air Pollutants | OR | 95% CI | p |
|---|---|---|---|
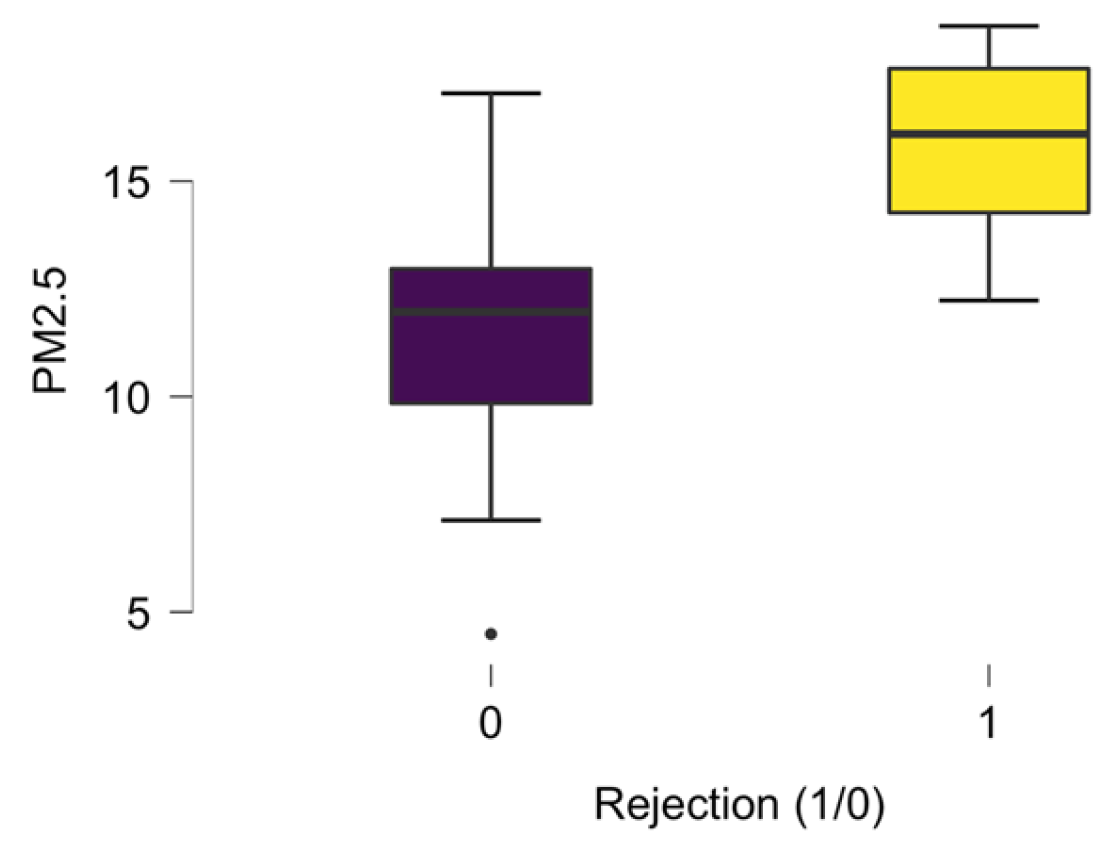
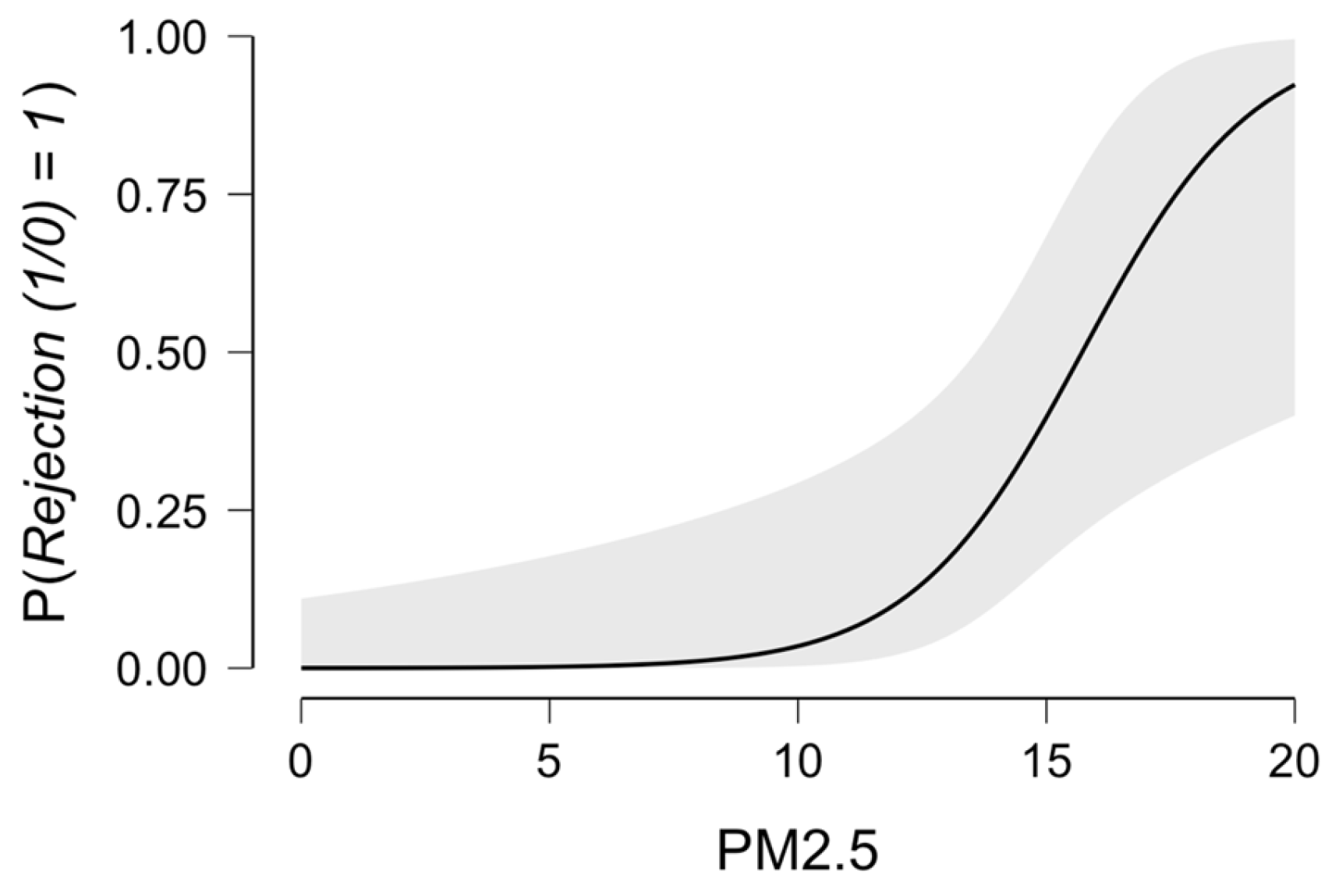
| PM2.5 | 1.79 | 1.11–2.89 | 0.018 |
| PM10 | 1.94 | 0.87–3.21 | 0.174 |
| NO2 | 6.93 | 0.65–12.56 | 0.167 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urbanowicz, T.; Skotak, K.; Konecka-Mrówka, D.; Wachowiak-Baszyńska, H.; Skowronek, R.; Sikora, J.; Bratkowski, J.; Kaczmarek, J.; Misiorny, M.; Straburzyńska-Migaj, E.; et al. The Hypothesis of the Interplay Between Air Particulate Matter PM2.5 and Acute Cellular Rejection Episodes Following Heart Transplantation. Atmosphere 2025, 16, 234. https://doi.org/10.3390/atmos16020234
Urbanowicz T, Skotak K, Konecka-Mrówka D, Wachowiak-Baszyńska H, Skowronek R, Sikora J, Bratkowski J, Kaczmarek J, Misiorny M, Straburzyńska-Migaj E, et al. The Hypothesis of the Interplay Between Air Particulate Matter PM2.5 and Acute Cellular Rejection Episodes Following Heart Transplantation. Atmosphere. 2025; 16(2):234. https://doi.org/10.3390/atmos16020234
Chicago/Turabian StyleUrbanowicz, Tomasz, Krzysztof Skotak, Dominika Konecka-Mrówka, Hanna Wachowiak-Baszyńska, Rafał Skowronek, Jędrzej Sikora, Jakub Bratkowski, Jan Kaczmarek, Maksymilian Misiorny, Ewa Straburzyńska-Migaj, and et al. 2025. "The Hypothesis of the Interplay Between Air Particulate Matter PM2.5 and Acute Cellular Rejection Episodes Following Heart Transplantation" Atmosphere 16, no. 2: 234. https://doi.org/10.3390/atmos16020234
APA StyleUrbanowicz, T., Skotak, K., Konecka-Mrówka, D., Wachowiak-Baszyńska, H., Skowronek, R., Sikora, J., Bratkowski, J., Kaczmarek, J., Misiorny, M., Straburzyńska-Migaj, E., Nożyński, J., & Jemielity, M. (2025). The Hypothesis of the Interplay Between Air Particulate Matter PM2.5 and Acute Cellular Rejection Episodes Following Heart Transplantation. Atmosphere, 16(2), 234. https://doi.org/10.3390/atmos16020234