
The Different Impact of PM2.5 on Atherogenesis in Overseas vs. Native Chinese in the CATHAY Study

 ,
,  and
and
Abstract
:1. Introduction
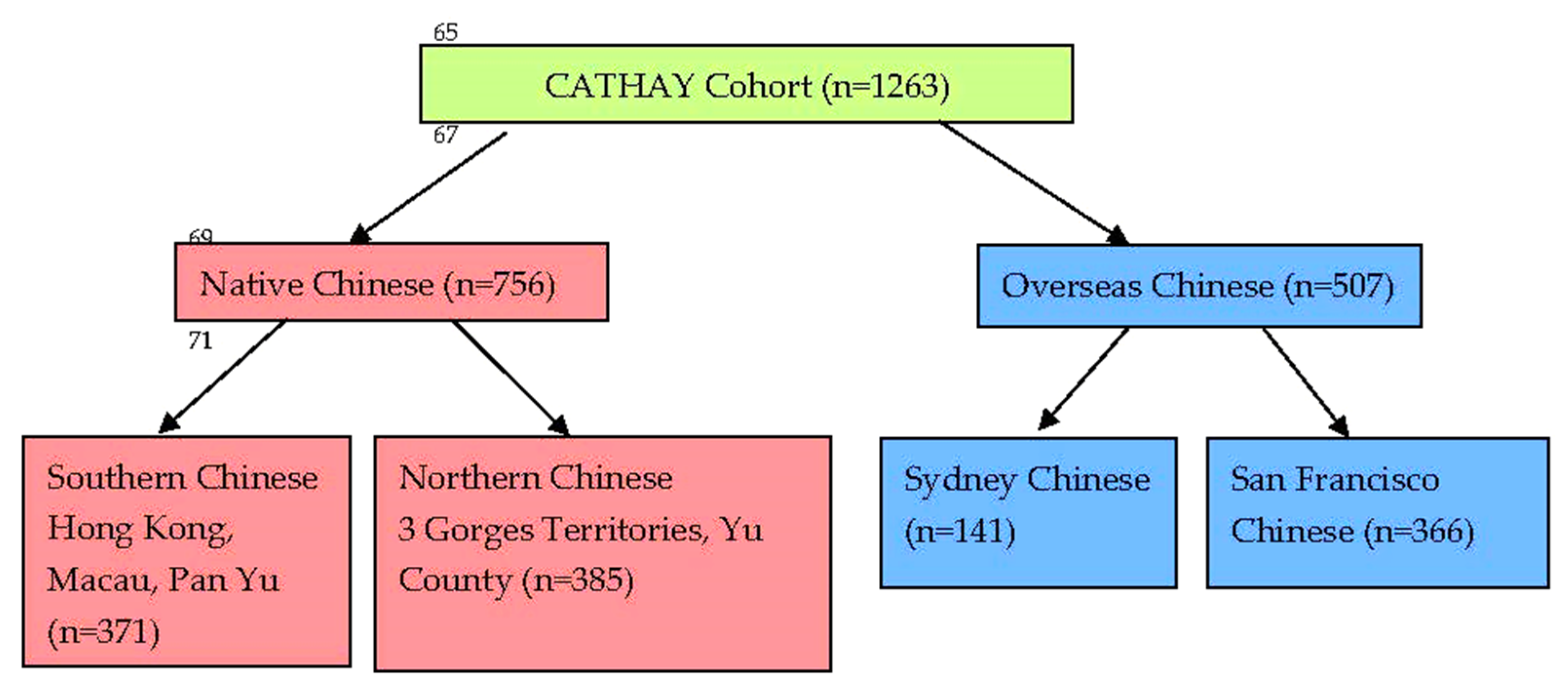
2. Subjects and Methods
2.1. Particulate Matter (PM2.5) Concentration Evaluation
2.2. Vascular Studies
3. Statistical Analyses
4. Results
4.1. Demographic and Clinical Characteristics
4.2. Vascular Parameters from Different Locations
4.3. Determinants of the Risk Factors for Brachial FMD and Carotid IMT
5. Discussion
6. Study Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Presentation
References
- Lloyd-Jones, D.; Adams, R.; Carnethon, M.; De Simone, G.; Ferguson, T.B.; Flegal, K.; Hong, Y. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics-2009 update: A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2009, 119, 480–486. [Google Scholar] [PubMed]
- Pepine, C.J. The effects of angiotensin-converting enzyme inhibition on endothelial dysfunction: Potential role in myocardial ischemia. Am J Cardiol. 1998, 82, 23S–27S. [Google Scholar] [CrossRef]
- Roth, G.A.; Johnson, C.; Abajobir, A.; Abd-Allah, F.; Abera, S.F.; Abyu, G.; Ahmed, M.; Aksut, B.; Alam, T.; Alam, K.; et al. Global regional and national burden of cardiovascular diseases for 10 causes, 1990–2015. J Am Coll Cardiol. 2017, 70, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Danaei, G.; Ding, E.; Mozaffarian, D.; Taylor, B.; Rehm, J.; Murray, C.J.L.; Ezzati, M. The preventable causes of death in the United States: Comparative risk assessment of dietary, lifestyle, and metabolic risk factors. PLoS Med. 2009, 6, e1000058. [Google Scholar] [CrossRef]
- Anand, S.S.; Yusuf, S.; Vuksan, V.; Devanesen, S.; Teo, K.K.; Montague, P.A.; Kelemen, L.; Yi, C.; Lonn, E.; Gerstein, H.; et al. Differences in risk factors, atherosclerosis, and cardiovascular disease between ethnic groups in Canada: The Study of Health Assessment and Risk in Ethnic Groups (SHARE). Lancet 2000, 356, 279–284. [Google Scholar] [CrossRef]
- Pope III, C.A.; Burnett, R.T.; Thurston, G.D.; Thun, M.J.; Calle, E.E.; Krewski, D.; Godleski, J.J. Cardiovascular mortality and long-term exposure to particular air pollution–Epidemiological evidence of general pathophysiological pathways of disease. Circulation 2004, 109, 71–77. [Google Scholar] [CrossRef] [Green Version]
- Rajagopalan, S.; Al-Kini, S.G.; Brook, R.D. Air pollution and cardiovascular disease. J. Am. Coll. Cardiol. 2018, 72, 2054–2070. [Google Scholar] [CrossRef]
- Brook, R.D.; Rajagopalan, S.; Pope III, C.A.; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Kaufman, J.D. American Heart Association Council on Epidemiology and Prevention, Council on the Kidney in Cardiovascular Disease, and Council on Nutrition, Physical Activity and Metabolism. Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the American Heart Association. Circulation 2010, 121, 2331–2378. [Google Scholar]
- Jasarevic, T.; Thomas, G.; Osseiran, N. 7 Million Premature Deaths Annually Lined to Air Pollution; WHO Media Centre: Geneva, Switzerland, 2014. [Google Scholar]
- Woo, K.S.; Chook, P.; Raitakari, O.T.; McQuillan, B.; Feng, J.Z.; Celermajer, D.S. Westernization of Chinese adults and increased subclinical atherosclerosis. Arter. Thromb. Vasc. Biol. 1999, 19, 2487–2493. [Google Scholar] [CrossRef] [Green Version]
- Celermajer, D.S.; Chow, C.K.; Marijon, E.; Anstey, N.M.; Woo, K.S. Cardiovascular disease in the development world. Prevalence, patterns, and the potential of early disease detection. J. Am. Coll. Cardiol. 2012, 60, 1207–1216. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Siri, J.G.; Remais, J.V.; Cheng, Q.; Zhang, H.; Chan, K.K.Y.; Sun, Z.; Zhao, Y.; Cong, N.; Li, X.; et al. The Tsinghua-lancet commission on healthy cities in China: Unlocking the power of cities for a healthy China. Lancet 2018, 391, 2140–2184. [Google Scholar] [CrossRef] [Green Version]
- Woo, K.S.; McCrohon, J.A.; Chook, P.; Adams, M.R.; Robinson, J.T.C.; McCredie, R.J.; Lam, C.W.K.; Feng, J.Z.; Celermajer, D.S. Chinese Adults Are Less Susceptible Than Whites to Age-Related Endothelial Dysfunction. J. Am. Coll. Cardiol. 1997, 30, 113–118. [Google Scholar] [CrossRef] [Green Version]
- Thomas, G.N.; Chook, P.; Qiao, M.; Huang, X.S.; Leong, H.C.; Celermajer, D.S.; Woo, K.S. Deleterious impact of “high normal” glucose levels and other metabolic syndrome components on arterial endothelial function and intima-media thickness in apparently healthy Chinese subject: The CATHAY study. Arter. Thromb. Vasc. Biol. 2004, 24, 739–743. [Google Scholar] [CrossRef] [Green Version]
- Woo, K.S.; Lin, C.Q.; Yin, Y.H.; Guo, D.S.; Chook, P.; Kwok CYTimothy Celermajer, D.S. The Impact of Air Pollution (PM2.5) on Atherogenesis in Modernizing Southern versus Northern China. Atmosphere 2021, 12, 1552. [Google Scholar] [CrossRef]
- Woo, K.S.; Chook, P.; Yu, C.W.; Sung, R.Y.; Qiao, M.; Leung, S.S.; Lam, C.W.; Metreweli, C.; Celermajer, D.S. Effects of diet and exercise on obesity-related vascular dysfunction in children. Circulation 2004, 109, 1981–1986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woo, K.S.; Chook, P.; Hu, Y.J.; Lao, X.Q.; Lin, C.Q.; Lee, P.W.A.; Kwok, C.Y.T.; Wei, A.N.; Guo, D.S.; Yin, Y.H.; et al. The Impact of Particulate Matter Air Pollution (PM2.5) on Atherosclerosis in Modernizing China: The report from CATHAY Study. Int. J. Epid. 2021, 50, 578–588. [Google Scholar] [CrossRef] [PubMed]
- Woo, K.S.; Kwok, T.C.Y.; Chook, P.; Hu, Y.J.; Yin, Y.H.; Lin, C.Q.; Lau, K.H.A.; Lee, P.W.A.; Celermajer, D.S. Independent Effects of Metabolic Syndrome and Air Pollution (PM2.5) on Atherosclerosis in Modernizing China. Austin. J. Public. Health Epidemiol. 2021, 8, 1097. [Google Scholar]
- Zimmet, P.; Alberti, K.; George, M.M.; Rios, M.S. A new International Diabetes Federation (IDF) worldwide definition of the metabolic syndrome: The rationale and the results. Rev. Esp. Cardiol. 2005, 58, 1371–1376. [Google Scholar] [CrossRef]
- Li, C.; Lau, A.K.H.; Mao, J.; Chu, D.A. Retrieval, validation, and application of the 1-km aerosol optical depth from MODIS measurements over Hong Kong. IEEE Trans. Geosci. Remote Sens. 2005, 43, 2650–2658. [Google Scholar]
- Lin, C.Q.; Li, Y.; Yuan, Z.B.; Lau, A.K.H.; Li, C.C.; Fung, J.C.H. Using satellite remote sensing data to estimate the high-resolution distribution of ground-level PM2.5. Remote Sens. Env. 2015, 156, 117–128. [Google Scholar] [CrossRef]
- Lin, C.Q.; Liu, G.; Lau, A.K.H.; Li, Y.; Li, C.C.; Fung, J.C.H.; Lao, X.Q. High-resolution satellite remote sensing of provincial PM2.5 trends in China from 2001 to 2015. Atmos. Env. 2018, 180, 110–116. [Google Scholar] [CrossRef]
- Celermajer, D.; Sorensen, K.; Gooch, V.; Spiegelhalter, D.; Miller, O.; Sullivan, I.; Lloyd, J.; Deanfield, J. Non-invasive detection of endothelial dysfunction in children and adults at risk of atherosclerosis. Lancet 1992, 340, 1111–1115. [Google Scholar] [CrossRef]
- Woo, K.S.; Chook, P.; Chan, L.L.; Cheung, A.S.; Fung, W.H.; Qiao, M.; Lolin, Y.I.; Thomas, G.N.; Sanderson, J.E.; Metreweli, C.; et al. Long-term improvement in homocysteine levels and arterial endothelial function after 1-year folic acid supplementation. Am. J. Med. 2002, 112, 535–539. [Google Scholar] [CrossRef]
- Woo, K.S.; Chook, P.; Yu, C.; Sung, R.Y.T.; Qiao, M.; Leung, S.S.F.; Lam, C.W.K.; Metreweli, C.; Celermajer, D.S. Overweight in children is associated with arterial endothelial dysfunction and intima-media thickening. Int. J. Obes. 2004, 28, 852–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salonen, J.T.; Salonen, R. Ultrasonographically assessed carotid morphology and the risk of coronary heart disease. Arter. Thromb. Vasc. Biol. 1991, 11, 1245–1249. [Google Scholar] [CrossRef] [Green Version]
- Bots, M.L.; Hoes, A.W.; Koudstaal, P.J.; Hofman, A.; Grobbee, D.E. Common carotid intima-media thickness and risk of stroke and myocardial infarction: The Rotterdam Study. Circulation 1997, 96, 1432–1437. [Google Scholar] [CrossRef] [Green Version]
- Touboul, P.J.; Hennerici, M.G.; Meairs, S.; Adams, H.; Amarenco, P.; Desvarieux, M.; Zannad, F. Advisory Board of the 3rd Watching the Risk Symposium 2004, 13th European Stroke Conference. Mannheim intima-media thickness consensus. Cereb. Dis. 2004, 18, 346–349. [Google Scholar] [CrossRef]
- Schulz, K.F.; Grimes, D.A. Sample size calculations in randomised trials: Mandatory and mystical. Lancet 2005, 365, 1348–1353. [Google Scholar] [CrossRef]
- Anderson, T.J.; Uehata, A.; Gerhard, M.D.; Meredith, I.T.; Knab, S.; Delagrange, D.; Lieberman, E.H.; Ganz, P.; Creager, M.A.; Yeung, A.C.; et al. Close relation of endothelial function in the human coronary and peripheral circulations. J. Am. Coll. Cardiol. 1995, 26, 1235–1241. [Google Scholar] [CrossRef] [Green Version]
- O’Leary, D.H.; Polak, J.F.; Kronmal, R.A.; Manolio, T.A.; Burke, G.L.; Wolfson, S.K., Jr. Carotid-artery intima and media thickness as a risk factor for myocardial infarction and stroke in older adults. N. Engl. J. Med. 1999, 340, 14–22. [Google Scholar] [CrossRef]
- Münzel, T.; Miller, M.R.; Sørensen, M.; Lelieveld, J.; Daiber, A.; Rajagopalan, S. Reduction of environmental pollutants for prevention of cardiovascular disease: It’s time to act. Eur Heart J. 2020, 41, 3989–3997. [Google Scholar] [CrossRef] [PubMed]
- Langrish, J.P.; Mills, N.L.; Chan, J.K.; Leseman, D.L.; Aitken, R.J.; Fokkens, P.H.; Cassee, F.R.; Li, J.; Donaldson, K.; Newby, D.E.; et al. Beneficial cardiovascular effects of reducing exposure to particulate air pollution with a simple facemask. Part. Fibre Toxicol. 2009, 6, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romieu, I.; Castro-Giner, F.; Dunzli, N.; Sunyer, J. Air pollution, oxidative stress and dietary supplementation: A review. Eur. Respir. J. 2008, 31, 179–196. [Google Scholar] [CrossRef] [PubMed]
- Allen, R.W.; Carlsten, C.; Karlen, B.; Leckie, S.; van Eeden, S.; Vedal, S.; Wong, I.; Brauer, M. An air filter intervention study of endothelial function among healthy adults in a woodsmoke-impacted community. Am. J. Respir. Crit. Care Med. 2011, 183, 1222–1230. [Google Scholar] [CrossRef] [Green Version]
- Baumgartner, J.; Smith, K.R.; Chockalingam, A. Reducing CVD through improvements in household energy-Implications for policy-relevant research. Glob. Heart 2012, 7, 243–247. [Google Scholar] [CrossRef] [Green Version]
- Vieira, J.L.; Guimaraes, G.V.; Andre, P.A.; Cruz, F.D.; Saldiva, P.H.N.; Bocchi, E.A. Respiratory filter reduces the cardiovascular effects associated with diesel exhaust exposure. J. Am. Coll. Cardiol. Heart Fail. 2016, 4, 55–64. [Google Scholar] [CrossRef]
- Li, H.C.; Cai, J.; Chen, R.J.; Zhao, Z.H.; Ying, Z.K.; Wang, L.; Chen, J.; Hao, K.; Kinney, P.L.; Chen, H.; et al. Particulate matter exposure and stress hormone levels: A randomized, double-blind, crossover trial of air purification. Circulation 2017, 136, 618–627. [Google Scholar] [CrossRef]
- Woo, K.S.; Hu, Y.J.; Chook, P.; Wei, A.N.; Wu, M.J.; Li, L.; Woo, J.; Chan, T.Y.; Cheng, W.K.; Celermajer, D.S. The Impact of Lifestyle Changes on Cardiometabolic Health in Modernizing China: A Tale of Three Gorges in the Yangtze River. Metab. Syndr. Relat. Disord. 2020, 18, 65–71. [Google Scholar] [CrossRef]


{kind=link}
| Location | Year of Study | Number of Subjects | PM2.5 (µg/m3) |
|---|---|---|---|
| Sydney | 1997–1999 | 141 | 5.8 ± 0.1 |
| San Francisco (Bay Area) | 1999–2001 | 366 | 14.8 ± 2.8 |
| Southern China (Hong Kong, Macau, Pan Yu) | 1991–1997 | 371 | 41.5 ± 5.4 |
| Northern China (Three Gorges Territories, Yu County) | 2000–2007 | 385 | 73.2 ± 0.17 |
| Southern China | Northern China | Sydney | San Francisco | |
|---|---|---|---|---|
| Total Subjects | 371 | 385 | 141 | 366 |
| Male (%) | 53 | 55 | 55 | 46 §§ |
| Age (Years) | 45.6 ± 13.1 | 45.1 ± 10.1 | 44.9 ± 10.5 | 47.1 ± 11.9 |
| Smoking (%) | 11 | 39 * | 20 | 9 § |
| PM2.5 (μg/m3) | 41.5 ± 5.4 | 73.2 ± 0.7 * | 5.8± 0.1 | 14.8 ± 2.8 § |
| BMI | 23.2 ± 3.6 | 24.4 ± 3.4 | 23.0 ± 3.0 | 23.7 ± 4.0 |
| SBP (mmHg) | 117.5 ± 14.8 | 124.5 ± 15.0 * | 115.7 ± 15.5 | 120.4 ± 17.1 §§§ |
| DBP (mmHg) | 75.3 ± 9.3 | 82.0 ± 10.0 * | 76.7 ± 9.5 | 79.8 ± 10.5 §§§ |
| WHR | 0.84 ± 0.06 | 0.84 ± 0.07 | 0.84 ± 0.06 | 0.84 ± 0.07 |
| Glucose (mmol/L) | 5.55 ± 1.13 | 5.54 ± 0.94 | 5.01 ± 0.57 | 5.18 ± 0.85 |
| HDL-C (mmol/L) | 1.33 ± 0.36 | 1.11 ± 0.30 * | 1.42 ± 0.36 | 1.34 ± 0.38 |
| LDL-C (mmol/L) | 3.52 ± 0.95 | 2.34 ± 0.74 * | 3.21 ± 0.83 | 3.54 ± 0.87 § |
| TG (mmol/L) | 1.21 ± 0.79 | 1.60 ± 0.88 * | 1.45 ± 1.03 | 1.47 ± 1.05 |
| MS (%) | 16.3 | 29.9 * | 10.6 | 17.2 §§ |
| Folate (nmol/L) | 29.5 ± 15.2 | 13.2 ± 5.5 * | 21.0 ± 6.1 | 29.9 ± 13.6 § |
| MTHFR (TT%) | 3.8 | 28.5 * | 13.5 | 5.0 §§ |
| Homocysteine (μmol/L) | 9.6 ± 4.3 | 24.5 ± 20.3 * | 8.3 ± 2.3 | 7.2 ± 1.8 §§ |
| Risk Factors | Native Chinese | Overseas Chinese | p-Value | Post-Bonferroni Adjustment |
|---|---|---|---|---|
| Total Subjects | 756 | 507 | ||
| Male (%) | 54 | 49 | 0.078 | (>0.9) |
| Age (Years) | 45.3 ± 11.7 | 46.5 ± 11.6 | 0.087 | (>0.9) |
| Smoking (%) | 29 | 12 | <0.0001 | (<0.0015) |
| PM2.5 (μg/m3) | 57.7 ± 6.3 | 12.3 ± 4.4 | <0.0001 | (<0.0015) |
| BMI | 23.8 ± 3.6 | 23.5 ± 3.8 | −0.149 | (>0.9) |
| SBP (mmHg) | 121.2 ± 15.3 | 119.1 ± 16.8 | 0.025 | −0.375 |
| DBP (mmHg) | 78.7 ± 10.2 | 79.0 ± 10.3 | 0.681 | (>0.9) |
| WHR | 0.84 ± 0.07 | 0.84 ± 0.07 | 0.84 | (>0.9) |
| Glucose (mmol/L) | 5.6 ± 1.0 | 5.1 ± 0.8 | <0.0001 | (<0.0015) |
| HDL-C (mmol/L) | 1.22 ± 0.35 | 1.37 ± 0.37 | <0.0001 | (<0.0015) |
| LDL-C (mmol/L) | 2.92 ± 1.04 | 3.44 ± 0.87 | <0.0001 | (<0.0015) |
| TG (mmol/L) | 1.41 ± 0.86 | 1.47 ± 1.04 | 0.271 | (>0.9) |
| MS (%) | 23.1 | 15.4 | <0.0001 | (<0.0015) |
| Folate (mmol/L) | 21.2 ± 13.9 | 28.6 ± 13.2 | <0.0001 | (<0.0015) |
| MTHFR (TT%) | 17.1 | 13.5 | <0.0001 | (<0.0015) |
| Homocysteine (μmol/L) | 17.2 ± 16.5 | 7.6 ± 2.1 | <0.0001 | (<0.0015) |
| Native Chinese (n = 756) | Overseas Chinese (n = 507) | |||||
|---|---|---|---|---|---|---|
| Parameters | Southern China | Northern China | p-Value | San Francisco | Sydney | p-Value |
| GTN (%) | 18.2 ± 4.1 | 18.5 ± 3.2 | >0.9 § | 18.0 ± 2.9 | 20.1 ± 4.2 | <0.0004 § |
| (95% CI) | (17.8–18.7) | (18.0 –18.9) | (17.6–18.3) | (19.0–21.6) | ||
| Hyperemia (%) | 649 ± 273 | 782 ± 201 | <0.0004 § | 716 ± 264 | 696 ± 243 | >0.9 |
| (95% CI) | (619–680) | (753–812) | (682–750) | (63–762) | ||
| FMD (%) | 8.5 ± 2.6 | 7.2 ± 1.9 | <0.0001 | 8.1 ± 2.2 | 8.8 ± 2.6 | 0.044 |
| (95% CI) | (8.2–8.8) | (6.9–7.4) | (7.9–8.4) | (8.1–9.5) | ||
| Carotid IMT (mm) | 0.58 ± 0.13 | 0.64 ± 0.12 | <0.0001 | 0.68 ± 0.15 | 0.59 ± 0.15 | <0.0001 |
| (95% CI) | (0.56–0.59) | (0.62–0.65) | (0.66–0.69) | (0.57–0.62) | ||
| Parameters | Native Chinese (n = 756) | Overseas Chinese (n = 507) | p-Value |
|---|---|---|---|
| GTN (%) | 18.3 ± 3.8 | 18.4 ± 3.3 | >0.9 § |
| (95% CI) | (18.0–18.6) | (18.0–18.8) | |
| Hyperemia (%) | 698 ± 257 | 712 ± 260 | >0.9 § |
| (95% CI) | (675–721) | (682–743) | |
| FMD (%) | 8.0 ± 2.5 | 8.3 ± 2.3 | 0.136 |
| (95% CI) | (7.8–8.2) | (8.0–8.5) | |
| Carotid IMT (mm) | 0.61 ± 0.12 | 0.65 ± 0.16 | <0.0001 |
| (95% CI) | (0.60–0.62) | (0.64–0.67) |
| Factors | Native Chinese * | Overseas Chinese ** | ||
|---|---|---|---|---|
| Beta-Value | p-Value | Beta-Value | p-Value | |
| Gender | −0.139 | 0.022 | −0.089 | 0.187 |
| Age (Years) | −0.217 | < 0.0001 | −0.189 | 0.003 |
| Smoking Status | −0.105 | 0.091 | −0.105 | 0.072 |
| BMI | 0.013 | 0.814 | −0.009 | 0.882 |
| MS | −0.038 | 0.650 | −0.121 | 0.049 |
| LDL-C (mmol/L) | −0.108 | 0.108 | 0.008 | 0.896 |
| Homocysteine (μmol/L) | −0.028 | 0.678 | −0.054 | 0.486 |
| MTHFR (TT%) | −0.023 | 0.699 | 0.039 | 0.499 |
| PM2.5 (μg/m3) | −0.058 | 0.630 | 0.186 | 0.230 |
| Location | −0.281 | 0.011 | −0.268 | 0.060 |
| Factors | Native Chinese * | Overseas Chinese ** | ||
|---|---|---|---|---|
| Beta-Value | p-Value | Beta-Value | p-Value | |
| Gender | 0.123 | 0.040 | 0.133 | 0.004 |
| Age (Years) | 0.412 | <0.0001 | 0.380 | <0.0001 |
| Smoking Status | 0.084 | 0.049 | −0.037 | 0.376 |
| BMI | 0.097 | 0.015 | 0.051 | 0.226 |
| MS | 0.107 | 0.011 | 0.070 | 0.099 |
| LDL-C (mmol/L) | 0.114 | 0.009 | 0.113 | 0.006 |
| Homocysteine (μmol/L) | 0.125 | 0.004 | 0.047 | 0.350 |
| MTHFR (TT%) | −0.024 | 0.552 | 0.008 | 0.832 |
| PM2.5 (μg/m3) | 0.389 | <0.0001 | 0.050 | 0.659 |
| Location | −0.241 | <0.0001 | 0.159 | 0.137 |
| Factors | Brachial FMD * | Carotid IMT ** | ||
|---|---|---|---|---|
| Beta-Value | p-Value | Beta-Value | p-Value | |
| Gender | −0.163 | <0.0001 | 0.180 | <0.0001 |
| Age (Years) | −0.264 | <0.0001 | 0.461 | <0.0001 |
| Smoking Status | −0.099 | 0.013 | −0.026 | 0.37 |
| PM2.5 (μg/m3) | −0.368 | <0.0001 | 0.359 | <0.0001 |
| Location | −0.210 | <0.0001 | 0.419 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Woo, K.-S.; Chan, S.-W.; Kwok, T.C.Y.; Yin, Y.-H.; Chook, P.; Lin, C.-Q.; Celermajer, D.S. The Different Impact of PM2.5 on Atherogenesis in Overseas vs. Native Chinese in the CATHAY Study. Atmosphere 2022, 13, 1236. https://doi.org/10.3390/atmos13081236
Woo K-S, Chan S-W, Kwok TCY, Yin Y-H, Chook P, Lin C-Q, Celermajer DS. The Different Impact of PM2.5 on Atherogenesis in Overseas vs. Native Chinese in the CATHAY Study. Atmosphere. 2022; 13(8):1236. https://doi.org/10.3390/atmos13081236
Chicago/Turabian StyleWoo, Kam-Sang, Shu-Wing Chan, Timothy C. Y. Kwok, Yue-Hui Yin, Ping Chook, Chang-Qing Lin, and David S. Celermajer. 2022. "The Different Impact of PM2.5 on Atherogenesis in Overseas vs. Native Chinese in the CATHAY Study" Atmosphere 13, no. 8: 1236. https://doi.org/10.3390/atmos13081236
APA StyleWoo, K.-S., Chan, S.-W., Kwok, T. C. Y., Yin, Y.-H., Chook, P., Lin, C.-Q., & Celermajer, D. S. (2022). The Different Impact of PM2.5 on Atherogenesis in Overseas vs. Native Chinese in the CATHAY Study. Atmosphere, 13(8), 1236. https://doi.org/10.3390/atmos13081236