
Associations between Incense-Burning Temples and Respiratory Mortality in Hong Kong



Abstract
1. Introduction
2. Materials and Methods
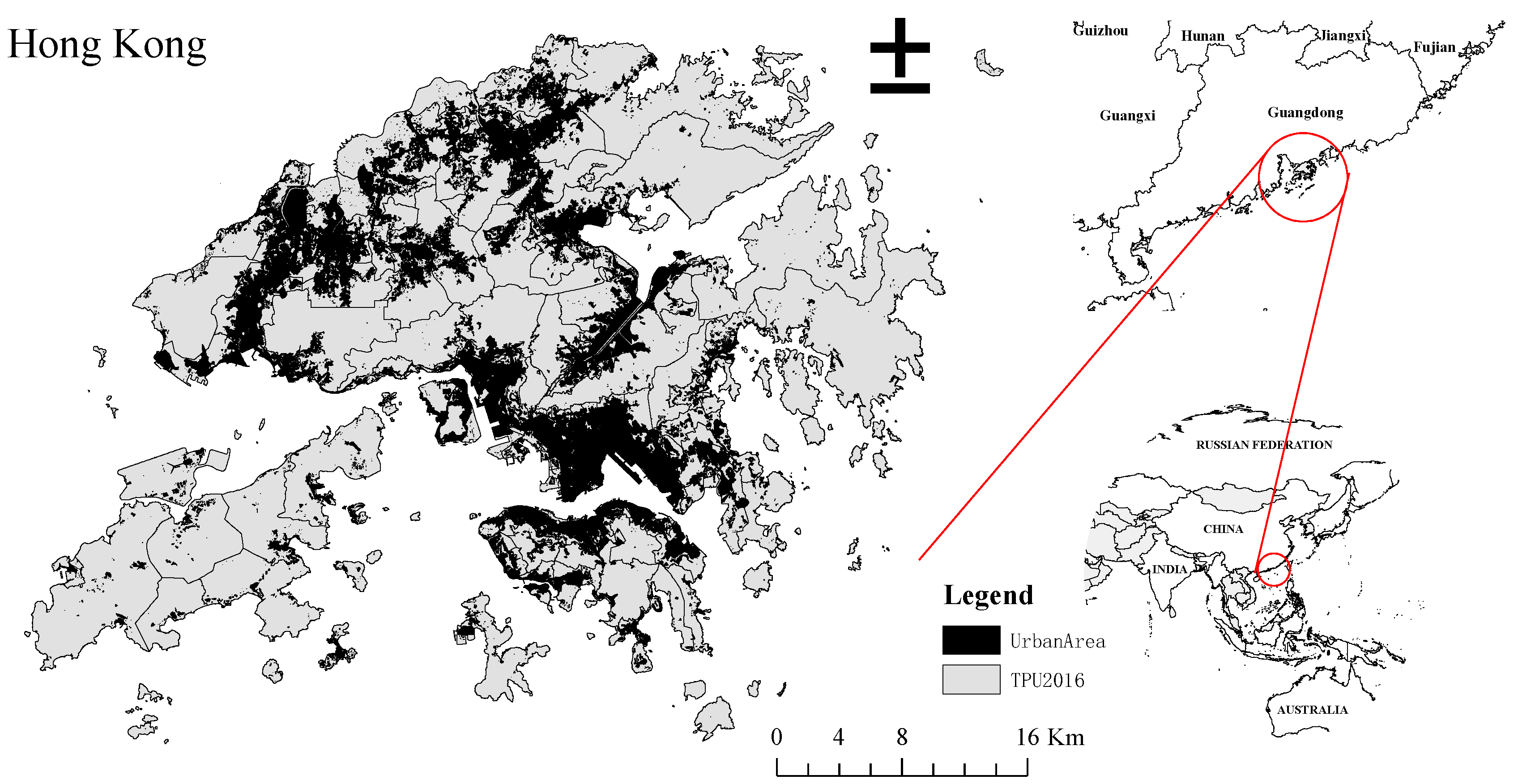
2.1. Study Area
2.2. Data
2.3. Methods of Analysis
2.3.1. Temple Classification
2.3.2. Statistical Analysis
3. Results
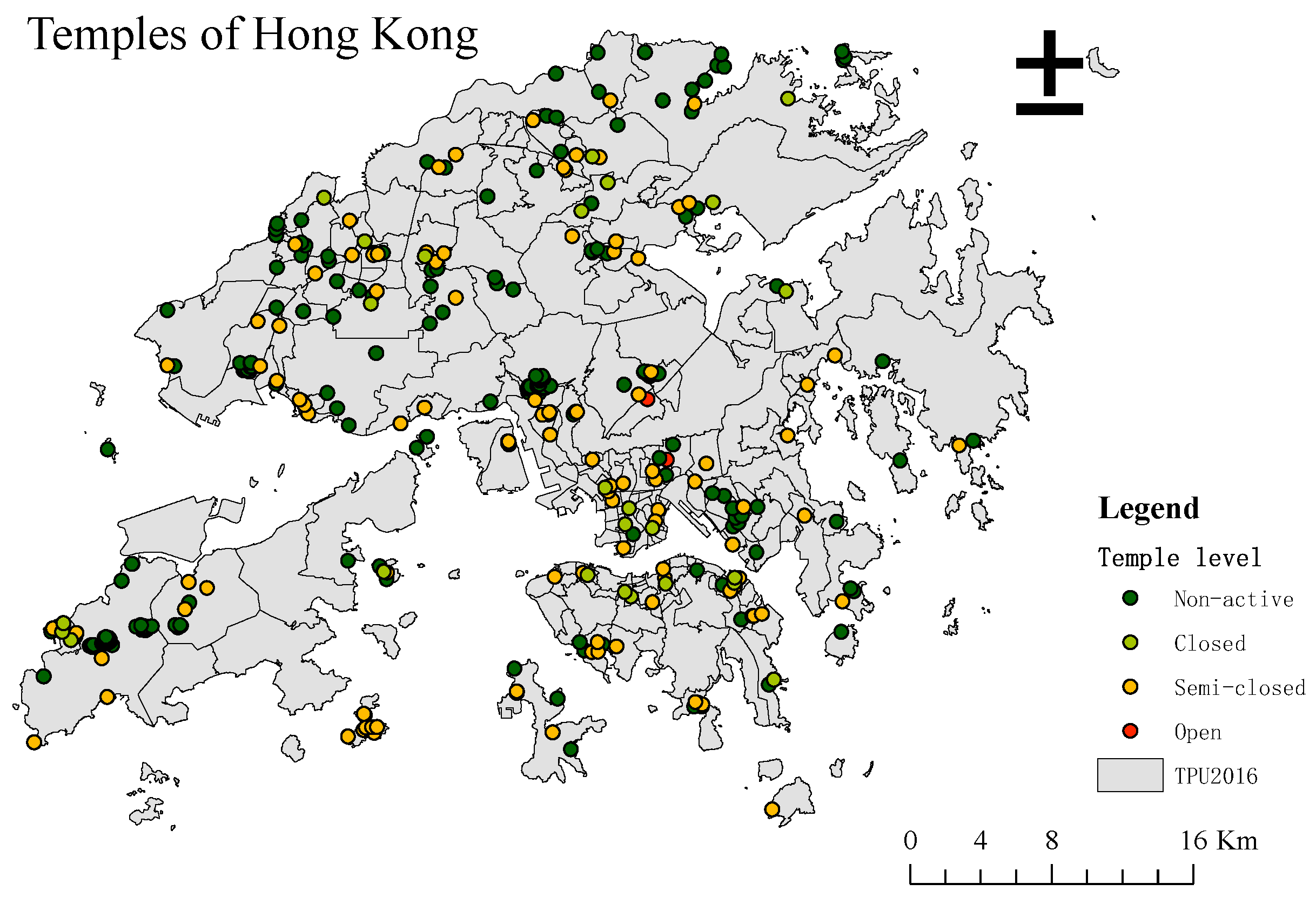
3.1. Temples’ Map
3.2. Principal Component Analysis
3.3. Linear Regression Model
3.4. Air-Quality Adjusted Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Mariani, S. Traditional Chinese Religion trusts in Hong Kong. Trusts Trustees 2015, 21, 538–545. [Google Scholar] [CrossRef]
- Liu, T.S. A Nameless but Active Religion: An Anthropologist’s View of Local Religion in Hong Kong and Macau. China Q. 2003, 373–394. [Google Scholar] [CrossRef]
- Jetter, J.J.; Guo, Z.; McBrian, J.A.; Flynn, M.R. Characterization of emissions from burning incense. Sci. Total Environ. 2002, 295, 51–67. [Google Scholar] [CrossRef]
- Lin, T.; Chang, F.; Hsieh, J.; Chao, H.; Chao, M. Characteristics of PAH and total suspended particulate in indoor and outdoor atmosphere of a Taiwanese temple. Hazard. Mater. 2002, 95, 1–12. [Google Scholar] [CrossRef]
- Wang, B.; Lee, S.C.; Ho, K.F.; Kang, Y.M. Characteristics of emissions of air pollutants from burning of incense in temples, Hong Kong. Sci. Total Environ. 2007, 377, 52–60. [Google Scholar] [CrossRef]
- Lee, S.C.; Wang, B. Characteristics of emissions of air pollutants from burning of incense in a large environmental chamber. Atmos. Environ. 2004, 38, 941–951. [Google Scholar] [CrossRef]
- Zhang, J.; Chen, W.; Li, J.; Yu, S.; Zhao, W. VOCs and Particulate Pollution due to Incense Burning in Temples, China. Procedia Eng. 2015, 121, 992–1000. [Google Scholar] [CrossRef]
- Ibald-mulli, A.; Wichmann, H.; Kreyling, W. Epidemiological Evidence on Health Effects of Ultrafine Particles. J. Aerosol Med. 2002, 15, 189–201. [Google Scholar] [CrossRef]
- Zhou, R.; An, Q.; Pan, X.W.; Yang, B.; Hu, J.; Wang, Y.H. Higher cytotoxicity and genotoxicity of burning incense than cigarette. Environ. Chem. Lett. 2015, 13, 465–471. [Google Scholar] [CrossRef]
- Sun, Q.; Wang, A.; Jin, X.; Natanzon, A.; Duquaine, D.; Brook, R.D.; Aguinaldo, J.G.S.; Fayad, Z.A.; Fuster, V.; Lippmann, M.; et al. Long-term air pollution exposure and acceleration of atherosclerosis and vascular inflammation in an animal model. J. Am. Med. Assoc. 2005, 294, 3003–3010. [Google Scholar] [CrossRef] [PubMed]
- Geng, T.T.; Jafar, T.H.; Yuan, J.M.; Koh, W.P. Long-term incense use and the risk of end-stage renal disease among Chinese in Singapore: The Singapore Chinese health study. BMC Nephrol. 2019, 20, 9. [Google Scholar] [CrossRef]
- Dominici, F.; Peng, R.D.; Bell, M.L.; Pham, L.; McDermott, A.; Zeger, S.L.; Samet, J.M. Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. J. Am. Med. Assoc. 2006, 295, 1127–1134. [Google Scholar] [CrossRef]
- Janssen, N.A.H.; Fischer, P.; Marra, M.; Ameling, C.; Cassee, F.R. Short-term effects of PM2.5, PM10 and PM2.5–10 on daily mortality in the Netherlands. Sci. Total Environ. 2013, 463–464, 20–26. [Google Scholar] [CrossRef]
- Sun, S.; Tian, L.; Cao, W.; Lai, P.; Wong, P.; Lee, R.S.-Y.; Mason, T.G.; Krämer, A.; Wong, C.-M. Urban climate modified short-term association of air pollution with pneumonia mortality in Hong Kong. Sci. Total. Environ. 2019, 646, 618–624. [Google Scholar] [CrossRef]
- Navasumrit, P.; Arayasiri, M.; Hiang, O.M.T.; Leechawengwongs, M.; Promvijit, J.; Choonvisase, S.; Chantchaemsai, S.; Nakngam, N.; Mahidol, C.; Ruchirawat, M. Potential health effects of exposure to carcinogenic compounds in incense smoke in temple workers. Chem. Biol. Interact. 2008, 173, 19–31. [Google Scholar] [CrossRef]
- Goel, A.; Wathore, R.; Chakraborty, T.; Agrawal, M. Characteristics of exposure to particles due to incense burning inside temples in Kanpur, India. Aerosol Air Qual. Res. 2017, 17, 608–615. [Google Scholar] [CrossRef]
- Yang, Y.; Tang, R.; Qiu, H.; Lai, P.C.; Wong, P.; Thach, T.Q.; Allen, R.; Brauer, M.; Tian, L.; Barratt, B. Long term exposure to air pollution and mortality in an elderly cohort in Hong Kong. Environ. Int. 2018, 117, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Bootdee, S.; Chantara, S.; Prapamontol, T. Determination of PM2.5 and polycyclic aromatic hydrocarbons from incense burning emission at shrine for health risk assessment. Atmos. Pollut. Res. 2016, 7, 680–689. [Google Scholar] [CrossRef]
- Brook, R.D.; Rajagopalan, S.; Pope, C.A.; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.; Mittleman, M.A.; et al. Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the american heart association. Circulation 2010, 121, 2331–2378. [Google Scholar] [CrossRef]
- Chen, R.Y.; Ho, K.F.; Hong, G.B.; Chuang, K.J. Houseplant, indoor air pollution, and cardiovascular effects among elderly subjects in Taipei, Taiwan. Sci. Total Environ. 2020, 705, 135770. [Google Scholar] [CrossRef] [PubMed]
- Franklin, P.J. Indoor air quality and respiratory health of children. Paediatr. Respir. Rev. 2007, 8, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Lau, O.W.; Luk, S.F. Leaves of Bauhinia blakeana as indicators of atmospheric pollution in Hong Kong. Atmos. Environ. 2001, 35, 3113–3120. [Google Scholar] [CrossRef]
- Shen, H.; Tsai, C.M.; Yuan, C.S.; Jen, Y.H.; Ie, I.R. How incense and joss paper burning during the worship activities influences ambient mercury concentrations in indoor and outdoor environments of an Asian temple? Chemosphere 2017, 167, 530–540. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Brager, G.S.; Augenbroe, G.; Song, X. Impact of outdoor air quality on the natural ventilation usage of commercial buildings in the US. Appl. Energy 2019, 235, 673–684. [Google Scholar] [CrossRef]
- Environmental Protection Department, Air Quality in Hong Kong 2019. 2019. Available online: https://www.aqhi.gov.hk/api_history/english/report/files/AQR2019e_final.pdf (accessed on 2 February 2021).
- Jo, B.W.; Khan, R.M.A. An internet of things system for underground mine air quality pollutant prediction based on azure machine learning. Sensors 2018, 18, 930. [Google Scholar] [CrossRef]
- Smith, L.I. A tutorial on Principal Components Analysis (Computer Science Technical Report No. OUCS-2002-12). 2002. Available online: http://hdl.handle.net/10523/7534 (accessed on 25 February 2021).
- Kaiser, H.F. The Application of Electronic Computers to Factor Analysis. Educ. Psychol. Meas. 1960, 20, 141–151. [Google Scholar] [CrossRef]
- Helsel, D.R.; Hirsch, R.M.; Ryberg, K.R.; Archfield, S.A.; Gilroy, E.J. Statistical methods in water resources. U.S. Geol. Surv. Tech. Methods 2020, 2020, 1–484. [Google Scholar] [CrossRef]
- Višić, B.; Kranjc, E.; Pirker, L.; Bačnik, U.; Tavčar, G.; Škapin, S.; Remškar, M. Incense powder and particle emission characteristics during and after burning incense in an unventilated room setting. Air Qual. Atmos. Health 2018, 11, 649–663. [Google Scholar] [CrossRef]
- Wong, P.P.Y.; Lai, P.C.; Allen, R.; Cheng, W.; Lee, M.; Tsui, A.; Tang, R.; Thach, T.Q.; Tian, L.; Brauer, M.; et al. Vertical monitoring of traffic-related air pollution (TRAP) in urban street canyons of Hong Kong. Sci. Total Environ. 2019, 670, 696–703. [Google Scholar] [CrossRef]
- Thach, T.-Q.; Tsang, H.; Lai, P.; Lee, R.S.-Y.; Wong, P.P.-Y. Long-term effects of traffic exposures on mortality in a Chinese cohort. J. Transp. Health 2019, 14, 100609. [Google Scholar] [CrossRef]
- Wang, H.C.; Tseng, C.H. Health damages from indoor air pollution quantified using a novel office building diagnosis methodology. Environ. Eng. Manag. J. 2018, 17, 2061–2069. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Aghamohammadi, N.; Sulaiman, N.M.N.; Lin, H.; Zhao, J. Commuting on Public Transport: Health Risks and Responses. In Air Pollution-Monitoring, Quantification and Removal of Gases and Particles; IntechOpen: London, UK, 2018. [Google Scholar]
- Ekpenyong, C.E.; Ettebong, E.O.; Akpan, E.E.; Samson, T.K.; Daniel, N.E. Urban city transportation mode and respiratory health effect of air pollution: A cross-sectional study among transit and non-transit workers in Nigeria. BMJ Open 2012, 2. [Google Scholar] [CrossRef]
- Wu, J.; Xie, W.; Li, W.; Li, J. Effects of urban landscape pattern on PM2.5 Pollution—A Beijing Case Study. PLoS ONE 2015, 10, e0142449. [Google Scholar] [CrossRef] [PubMed]
- Caraka, R.E.; Noh, M.; Chen, R.C.; Lee, Y.; Gio, P.U.; Pardamean, B. Connecting climate and communicable disease to penta helix using hierarchical likelihood structural equation modelling. Symmetry 2021, 13, 657. [Google Scholar] [CrossRef]
- Yu, S. Water spray geoengineering to clean air pollution for mitigating haze in China’s cities. Environ. Chem. Lett. 2014, 12, 109–116. [Google Scholar] [CrossRef]
- Yang, T.T.; Lin, T.S.; Chang, M. Characteristics of emissions of volatile organic compounds from smoldering incense. Bull. Environ. Contam. Toxicol. 2007, 78, 308–313. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data | Period | Sources |
|---|---|---|
| TPU | 2001, 2006, 2011, 2016 | Planning Department (PlanD) |
| Temple | - | Digitize using Google Earth |
| Basic environmental data | - | Lands Department (iB5000 Digital Topographic Map) |
| Respiratory Mortality data (ICD-10) | 2001–2016 | Census and Statistics Department (C&SD) |
| Population | 2001, 2006, 2011, 2016 | |
| Air quality (NO2, FSP/PM2.5) | 2001, 2006, 2011, 2016 | Environmental Protection Department (EPD) |
| KMO and Bartlett’s Test | 2001 | 2006 | 2011 | 2016 | |
|---|---|---|---|---|---|
| Kaiser-Meyer-Olkin Measure of Sampling Adequacy | 0.772 | 0.785 | 0.776 | 0.786 | |
| Bartlett’s Test of Sphericity | Approx. Chi-Square | 1182 | 1485 | 1514 | 1469 |
| df | 15 | 15 | 15 | 15 | |
| p value | <0.05 | <0.05 | <0.05 | <0.05 | |
| PCs | 2001 | 2006 | 2011 | 2016 | |
|---|---|---|---|---|---|
| 1 | Eigenvalue | 3.365 | 3.608 | 3.595 | 3.638 |
| % of Variance | 56.089 | 60.133 | 59.912 | 60.630 | |
| Cumulative % | 56.089 | 60.133 | 59.912 | 60.630 | |
| 2 | Eigenvalue | 1.070 | 1.041 | 1.056 | 1.012 |
| % of Variance | 17.831 | 17.342 | 17.608 | 16.863 | |
| Cumulative % | 73.920 | 77.475 | 77.520 | 77.493 |
| PCs | Variables | 2001 | 2006 | 2011 | 2016 |
|---|---|---|---|---|---|
| 1 | Temple index | 0.712 | |||
| Population density | 0.617 | 0.622 | 0.830 | ||
| Building density | 0.789 | 0.849 | 0.860 | 0.900 | |
| Greenery density | −0.692 | −0.724 | −0.720 | −0.757 | |
| Road density | 0.636 | 0.730 | 0.741 | 0.899 | |
| Water density | −0.867 | −0.838 | −0.832 | −0.314 | |
| 2 | Temple index | 0.829 | 0.874 | 0.872 | 0.510 |
| Population density | 0.740 | 0.608 | 0.607 | ||
| Building density | 0.503 | 0.419 | 0.398 | −0.303 | |
| Greenery density | −0.389 | ||||
| Road density | 0.654 | 0.574 | 0.564 | ||
| Water density | 0.848 |
| Model Summary | R | R Square | Adjusted R Square | F | p-Value |
|---|---|---|---|---|---|
| 2001 | 0.390 | 0.152 | 0.138 | 10.747 | <0.01 |
| 2006 | 0.602 | 0.363 | 0.352 | 34.079 | <0.01 |
| 2011 | 0.592 | 0.35 | 0.34 | 32.271 | <0.01 |
| 2016 | 0.341 | 0.117 | 0.102 | 7.895 | <0.01 |
| Model | Variables | Unstandardized | Standardized | t | Sig. | 95% Confidence Interval for B | Correlations | Collinearity Statistics | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | Std. Error | Beta | Lower Bound | Upper Bound | Partial | Part | Tolerance | VIF | ||||
| 2001 | (Constant) | 0.154 | 0.011 | 14.460 | 0.000 | 0.133 | 0.175 | |||||
| Population Density | −0.124 | 0.089 | −0.092 | −1.397 | 0.163 | −0.299 | 0.051 | −0.073 | −0.068 | 0.546 | 1.830 | |
| Temple index | −0.011 | 0.005 | −0.136 | −2.435 | 0.015 ** | −0.020 | −0.002 | −0.127 | −0.118 | 0.752 | 1.331 | |
| Building Density | 0.001 | 0.000 | 0.540 | 4.637 | 0.000 ** | 0.001 | 0.001 | 0.237 | 0.225 | 0.174 | 5.750 | |
| Greenery Density | 0.001 | 0.000 | 0.374 | 5.393 | 0.000 ** | 0.000 | 0.001 | 0.273 | 0.262 | 0.489 | 2.047 | |
| Road Density | −0.002 | 0.001 | −0.245 | −2.240 | 0.026 * | −0.003 | 0.000 | −0.117 | −0.109 | 0.197 | 5.068 | |
| Water Density | −0.008 | 0.004 | −0.113 | −1.920 | 0.056 | −0.016 | 0.000 | −0.101 | −0.093 | 0.683 | 1.463 | |
| 2006 | (Constant) | 0.131 | 0.018 | 7.350 | 0.000 ** | 0.096 | 0.166 | |||||
| Population Density | −0.797 | 0.306 | −0.213 | −2.609 | 0.009 ** | −1.398 | −0.196 | −0.136 | −0.110 | 0.267 | 3.740 | |
| Temple index | 0.023 | 0.007 | 0.151 | 3.120 | 0.002 ** | 0.009 | 0.038 | 0.162 | 0.131 | 0.758 | 1.319 | |
| Building Density | 0.001 | 0.000 | 0.347 | 3.222 | 0.001 ** | 0.168 | 0.136 | 0.153 | 6.519 | |||
| Greenery Density | −0.001 | 0.000 | −0.457 | −7.282 | 0.000 ** | −0.359 | −0.307 | 0.450 | 2.223 | |||
| Road Density | −0.001 | 0.002 | −0.094 | −0.849 | 0.397 | −0.045 | −0.036 | 0.145 | 6.918 | |||
| Water Density | 0.013 | 0.007 | 0.099 | 1.907 | 0.057 | 0.100 | 0.080 | 0.658 | 1.521 | |||
| 2011 | (Constant) | 0.160 | 0.018 | 8.989 | 0.000 | 0.125 | 0.195 | |||||
| Population Density | −0.454 | 0.306 | −0.128 | −1.486 | 0.138 | −1.056 | 0.147 | −0.078 | −0.063 | 0.242 | 4.125 | |
| Temple index | 0.008 | 0.007 | 0.054 | 1.109 | 0.268 | −0.006 | 0.022 | 0.058 | 0.047 | 0.754 | 1.327 | |
| Building Density | 0.001 | 0.000 | 0.279 | 2.580 | 0.010 ** | 0.000 | 0.001 | 0.135 | 0.110 | 0.154 | 6.479 | |
| Greenery Density | −0.001 | 0.000 | −0.383 | −6.022 | 0.000 ** | −0.001 | −0.001 | −0.303 | −0.256 | 0.448 | 2.234 | |
| Road Density | 0.000 | 0.002 | 0.032 | 0.276 | 0.783 | −0.003 | 0.004 | 0.015 | 0.012 | 0.135 | 7.411 | |
| Water Density | −0.001 | 0.007 | −0.009 | −0.170 | 0.865 | −0.014 | 0.012 | −0.009 | −0.007 | 0.654 | 1.528 | |
| 2016 | (Constant) | 0.197 | 0.030 | 6.662 | 0.000 | 0.139 | 0.255 | |||||
| Population Density | 0.537 | 0.409 | 0.118 | 1.313 | 0.190 | −0.267 | 1.342 | 0.069 | 0.065 | 0.306 | 3.266 | |
| Temple index | 0.007 | 0.013 | 0.034 | 0.578 | 0.563 | −0.018 | 0.033 | 0.031 | 0.029 | 0.702 | 1.425 | |
| Building Density | 0.000 | 0.001 | 0.039 | 0.293 | 0.770 | −0.001 | 0.001 | 0.015 | 0.015 | 0.141 | 7.078 | |
| Greenery Density | −0.001 | 0.000 | −0.275 | −3.732 | 0.000 ** | −0.002 | −0.001 | −0.193 | −0.185 | 0.454 | 2.204 | |
| Road Density | −0.001 | 0.002 | −0.046 | −0.370 | 0.711 | −0.006 | 0.004 | −0.020 | −0.018 | 0.157 | 6.389 | |
| Water Density | 0.012 | 0.011 | 0.066 | 1.110 | 0.268 | −0.010 | 0.034 | 0.058 | 0.055 | 0.687 | 1.455 | |
| Variables | Unstandardized Coefficients | Standardized Coefficients | t | Sig. | 95. 0% Confidence Interval for B | ||
|---|---|---|---|---|---|---|---|
| B | Std. Error | Beta | Lower Bound | Upper Bound | |||
| (Constant) | −0.304 | 0.255 | −1.194 | 0.233 | −0.805 | 0.197 | |
| Population Density | 0.025 | 0.014 | 0.194 | 1.763 | 0.079 | −0.003 | 0.053 |
| Temple weight | 0.006 | 0.010 | 0.040 | 0.603 | 0.547 | −0.014 | 0.026 |
| Building Density | 0.026 | 0.020 | 0.192 | 1.321 | 0.188 | −0.013 | 0.066 |
| Greenery Density | −0.056 | 0.011 | −0.415 | −5.019 | 0.000 ** | −0.079 | −0.034 |
| Road Density | −0.028 | 0.018 | −0.212 | −1.552 | 0.122 | −0.064 | 0.008 |
| Water Density | 0.042 | 0.011 | 0.262 | 3.827 | 0.000 ** | 0.020 | 0.063 |
| NO2 | −0.006 | 0.002 | −0.229 | −3.454 | 0.001 ** | −0.010 | −0.003 |
| PM2.5 | 0.036 | 0.014 | 0.178 | 2.655 | 0.008 ** | 0.009 | 0.063 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cai, W.H.; Wong, P.P.Y. Associations between Incense-Burning Temples and Respiratory Mortality in Hong Kong. Atmosphere 2021, 12, 774. https://doi.org/10.3390/atmos12060774
Cai WH, Wong PPY. Associations between Incense-Burning Temples and Respiratory Mortality in Hong Kong. Atmosphere. 2021; 12(6):774. https://doi.org/10.3390/atmos12060774
Chicago/Turabian StyleCai, Wen Hui, and Paulina Pui Yun Wong. 2021. "Associations between Incense-Burning Temples and Respiratory Mortality in Hong Kong" Atmosphere 12, no. 6: 774. https://doi.org/10.3390/atmos12060774
APA StyleCai, W. H., & Wong, P. P. Y. (2021). Associations between Incense-Burning Temples and Respiratory Mortality in Hong Kong. Atmosphere, 12(6), 774. https://doi.org/10.3390/atmos12060774