
Monitoring Air Pollution Variability during Disasters


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Area, Population, Timeframe, and Methods
2.2. Mobile Data and Instruments
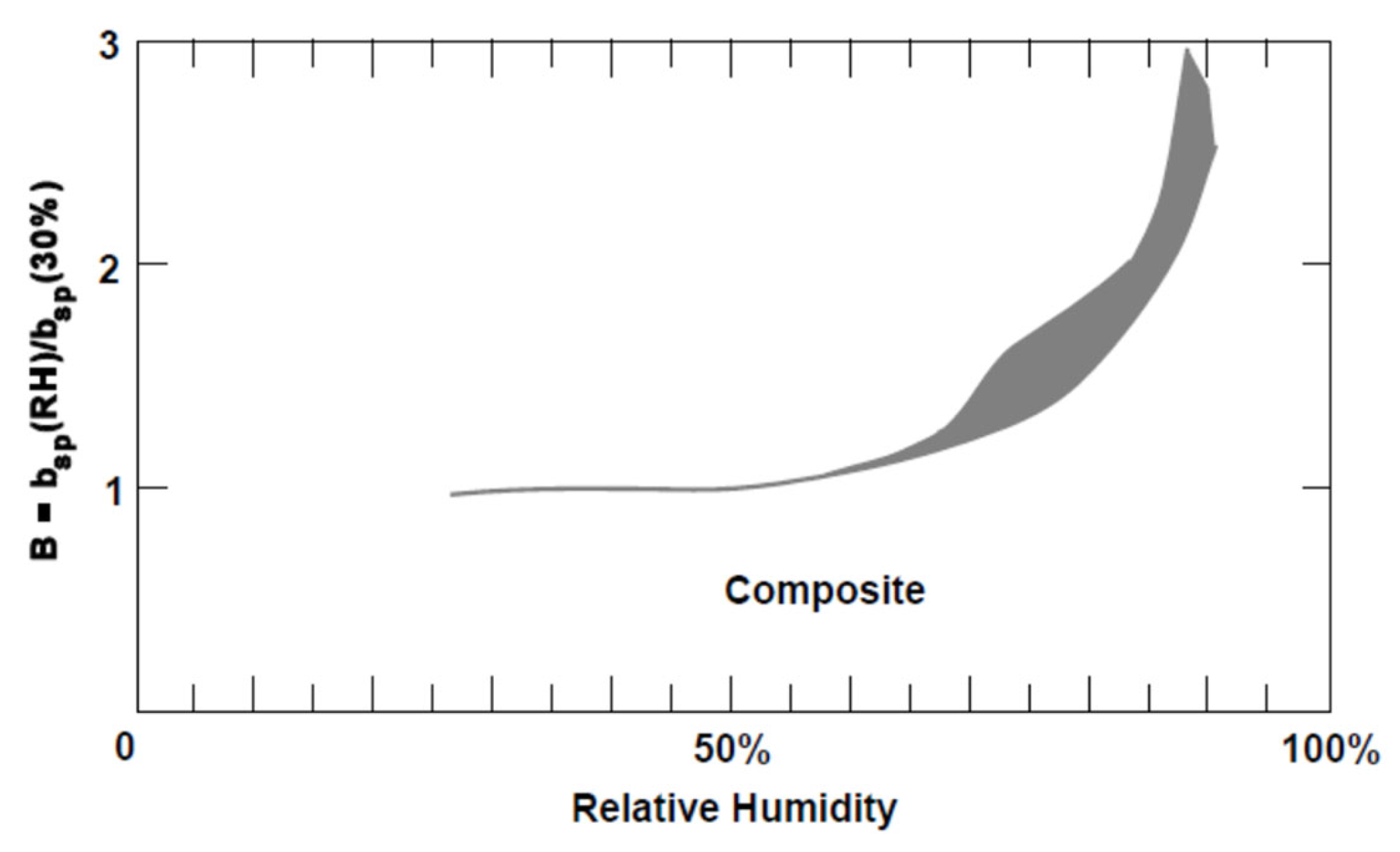
2.3. Humidity Adjustments

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parish | Land Area (Square Miles) | Population (2010 Census) | Adjusted Deaths (May–Dec, 2010) |
|---|---|---|---|
| Jefferson | 296 | 432,552 | 1353 |
| La Fourche | 1068 | 96,318 | 300 |
| Orleans | 169 | 343,829 | 559 |
| Plaquemines | 780 | 23,042 | - |
| St. Bernard | 378 | 35,897 | - |
| Terrebonne | 1232 | 111,860 | 222 |
| Region | 3923 | 1,043,498 | 2434 |
| Methods Used | LDEQ Data | EPA Daily Data | EPA Hourly Data | CDC Data | BP Data |
|---|---|---|---|---|---|
| Context of monitoring | regulatory | emergency | emergency | research | emergency |
| Monitoring type | stationary | stationary | stationary | model | mobile |
| Monitoring location | urban | coastal | coastal | regional | regional |
| Sample size (n) | 600 | 869 | 1144 | 2472 | 101,262 |
| Humidity calibration | ✓ | ||||
| Trend evaluation (graphical observation) | ✓ | ✓ | ✓ | ✓ | ✓ |
| Normality evaluation (histogram, skew, kurtosis) | ✓ | ✓ | ✓ | ✓ | ✓ |
| Centrality evaluation (mean, median) | ✓ | ✓ | ✓ | ✓ | ✓ |
| Variability evaluation (mean absolute deviation, standard deviation, seasonal variation) | ✓ | ✓ | ✓ | ✓ | ✓ |
| Comparison of peaks (short-term PM2.5 increases) | ✓ | ✓ | ✓ | ✓ | ✓ |
| Sampling frequency analysis (samples per day compared to mean absolute deviation) | ✓ | ✓ | ✓ | ✓ | ✓ |
| Comparison of means (t-tests) | ✓ | ✓ | |||
| Comparison of variances (F-tests) | ✓ | ✓ | |||
| Comparison of probability distributions (K-S tests) | ✓ | ✓ | |||
| Statistical power (Cohen’s D, effect size r, Hedge’s G) | ✓ | ||||
| Statistical relationship between variables (linear regression, multiple regression) | ✓ | ||||
| Multicollinearity analysis (tolerance test, variance inflation factor) | ✓ |
2.4. Stationary and Modeled Data and Instruments
3. Results
3.1. Data Variability
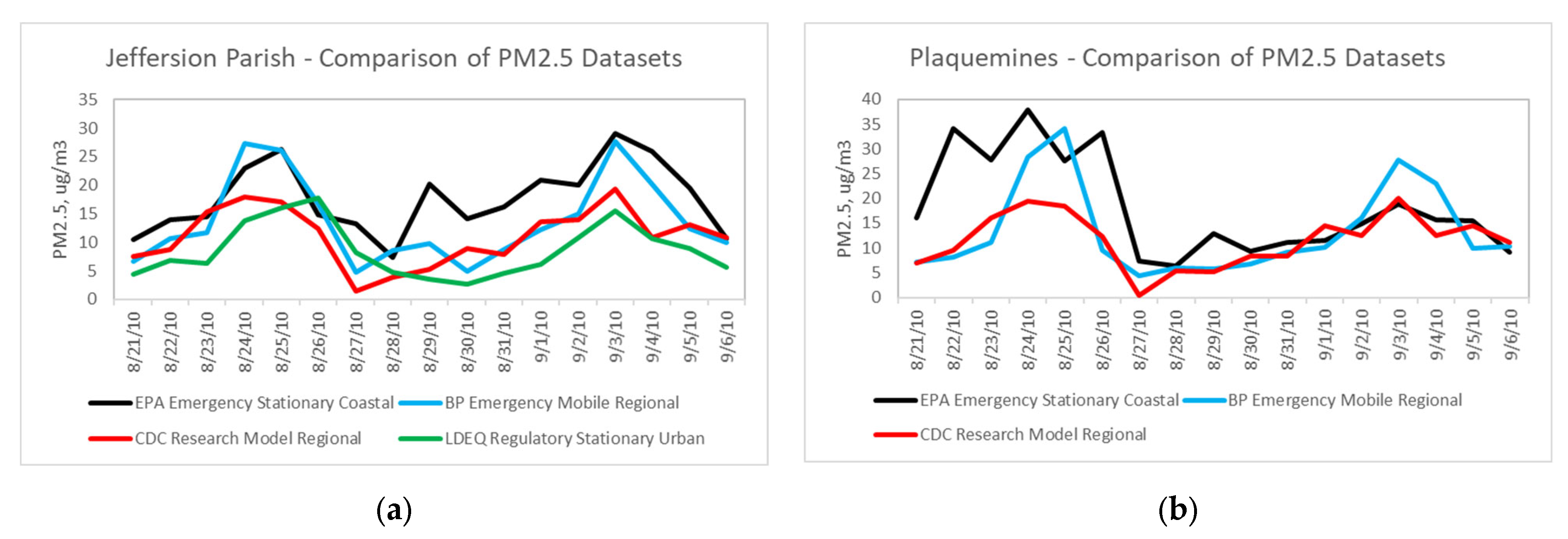
3.2. Modeled versus Mobile PM2.5 Data
3.3. Short-Term PM2.5 Increases and Mortality
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, K.; Zhang, J.; Lioy, P. Evaluation and Comparison of Continuous Fine Particulate Matter Monitors for Measurement of Ambient Aerosols. J. Air Waste Manag. Assoc. 2007, 57, 1499–1506. [Google Scholar] [CrossRef] [PubMed]
- National Commission on the BP Deepwater Horizon Oil Spill and Offshore Drilling. Deep Water: The Gulf Oil Disaster and the Future of Offshore Drilling, A Report to the President. January 2011. Available online: https://www.govinfo.gov/content/pkg/GPO-OILCOMMISSION/pdf/GPO-OILCOMMISSION.pdf (accessed on 18 March 2021).
- De Gouw, J.A.; Middlebrook, A.M.; Warneke, C.; Ahmadov, R.; Atlas, E.L.; Bahreini, R.; Blake, D.R.; Brock, C.A.; Brioude, J.; Fahey, D.W.; et al. Organic Aerosol Formation Downwind from the Deepwater Horizon Oil spill. Science 2011, 331, 1295. [Google Scholar] [CrossRef] [PubMed]
- Middlebrook, A.; Murphy, D.; Ahmadov, R.; Atlas, E.; Bahreini, R.; Blake, D.; Brioude, J.; Gouw, J.D.; Fehsenfeld, F.; Frost, G.; et al. Air Quality Implications of the Deepwater Horizon Oil spill. Proc. Natl. Acad. Sci. USA 2012, 109, 20280–20285. [Google Scholar] [CrossRef] [PubMed]
- National Oceanic and Atmospheric Administration. Insights from Oil Spill Air Pollution Study Have Implications Beyond Gulf. 11 March 2011. Available online: https://csl.noaa.gov/news/2011/92_0311.html (accessed on 20 January 2021).
- British Petroleum. Data Publication Summary Report: Community Air Sampling and Monitoring Data. Reference No. OTH-04v01-02. 2014. Available online: https://data.gulfresearchinitiative.org/data/BP.x750.000:0024 (accessed on 20 April 2019).
- Centers for Disease Control and Prevention. Monitor + Model Air Data. National Environmental Public Health Tracking. 2019. Available online: https://ephtracking.cdc.gov/showAirMonModData (accessed on 20 January 2021).
- Environmental Protection Agency. Final Rule on the Implementation of the New Source Review Provisions for Particulate Matter Less Than 2.5 Microns (PM2.5); 77 FR 65107; U.S. Environmental Protection Agency: Washington, DC, USA, 2012. Available online: https://www.epa.gov/sites/production/files/2015-12/documents/20080508_fs.pdf (accessed on 25 December 2020).
- Environmental Protection Agency. Quality Assurance Sampling Plan for British Petroleum Oil Spill. 2010. Available online: https://archive.epa.gov/emergency/bpspill/web/pdf/appendixe-data_management_plan_5-30.pdf (accessed on 20 April 2019).
- Louisiana Department of Environmental Quality. Ambient Air Monitoring Stations. 2011. Available online: https://www.deq.louisiana.gov/page/ambient-air-monitoring-data-reports (accessed on 20 November 2013).
- Nance, E.; King, D.; Wright, B.; Bullard, R.D. Ambient air concentrations exceeded health-based standards for fine particulate matter and benzene during the Deepwater Horizon oil spill. J. Air Waste Manag. Assoc. 2016, 66, 224–236. [Google Scholar] [CrossRef] [PubMed]
- Air Now. Air Quality Index (AQI)—A Guide to Air Quality and Your Health. 2013. Available online: http://airnow.gov/index.cfm?action=aqibasics.aqi (accessed on 5 October 2013).
- Di, Q.; Dai, L.; Wang, Y.; Zanobetti, A.; Choirat, C.; Schwartz, J.D.; Dominici, F. Association of short-term exposure to air pollution with mortality in older adults. JAMA 2017, 318, 2446–2456. [Google Scholar] [CrossRef]
- Schwartz, J. Air Pollution and Daily Mortality: A Review and Meta Analysis. Environ. Res. 1994, 64, 36–52. [Google Scholar] [CrossRef]
- Kim, S.E.; Hijioka, Y.; Nagashima, T.; Kim, H. Particulate Matter and Its Impact on Mortality among Elderly Residents of Seoul, South Korea. Atmosphere 2020, 11, 18. [Google Scholar] [CrossRef]
- Staniswalis, J.G.; Parks, N.J.; Bader, J.O.; Maldonado, Y.M. Temporal Analysis of Airborne Particulate Matter Reveals a Dose-Rate Effect on Mortality in El Paso: Indications of Differential Toxicity for Different Particle Mixtures. J. Air Waste Manag. Assoc. 2005, 55, 893–902. [Google Scholar] [CrossRef][Green Version]
- Krudysz, M.; Moore, K.; Geller, M.; Sioutas, C.; Froines, J. Intra-community Spatial Variability of Particulate Matter Size Distributions in Southern California/Los Angeles. Atmos. Chem. Phys. 2009, 9, 1061–1075. [Google Scholar] [CrossRef]
- Zhu, Y.; Hinds, W.C.; Kim, S.; Sioutas, C. Concentration and Size Distribution of Ultrafine Particles near a Major Highway. J. Air Waste Manag. Assoc. 2002, 52, 1032–1042. [Google Scholar] [CrossRef] [PubMed]
- Peters, J.; Theunis, J.; Van Poppel, M.; Berghmans, P. Monitoring PM10 and Ultrafine Particles in Urban Environments Using Mobile Measurements. Aerosol Air Qual. Res. 2013, 13, 509–522. [Google Scholar] [CrossRef]
- Gulev, S.K. Climatologically significant effects of space–time averaging in the North Atlantic sea–air heat flux fields. J. Clim. 1997, 10, 2743–2763. [Google Scholar] [CrossRef][Green Version]
- Hughes, P.J.; Bourassa, M.A.; Rolph, J.J.; Smith, S.R. Averaging-Related Biases in Monthly Latent Heat Fluxes. J. Atmos. Ocean. Technol. 2012, 29, 974–986. [Google Scholar] [CrossRef]
- Kaiser, J. Epidemiology. How dirty air hurts the heart. Science 2005, 307, 1858–1859. [Google Scholar] [CrossRef]
- Conroy, D.; McWilliams, A. Challenges and Issues with Reporting the AQI for PM2.5 on a Real-time Basis (slides). Environmental Protection Agency. 2001. Available online: https://slideplayer.com/slide/4160546/ (accessed on 20 March 2021).
- Environmental Protection Agency. Outdoor Air Quality Data. 2020. Available online: https://www.epa.gov/outdoor-air-quality-data (accessed on 22 December 2020).
- Yuval, D.M.; Broday, Y.C. Mapping spatiotemporal variables: The impact of the time-averaging window width on the spatial accuracy. Atmos. Environ. 2005, 39, 3611–3619. [Google Scholar] [CrossRef]
- Evangelista, M. Investigation of 1-hour PM2.5 Mass Concentration Data from EPA-Approved Continuous Federal Equivalent Method Analyzers. Environmental Protection Agency Office of Air Quality Planning and Standards. 2011. Available online: https://www3.epa.gov/ttn/naaqs/standards/pm/data/Evangelista040511.pdf (accessed on 20 December 2013).
- Steinle, S.; Reis, S.; Sabel, C.E. Quantifying human exposure to air pollution—Moving from static monitoring to spatiotemporally resolved personal exposure assessment. Sci. Total Environ. 2013, 443, 184–193. [Google Scholar] [CrossRef]
- Perring, A.E.; Schwarz, J.P.; Spackman, J.R.; Bahreini, R.; de Gouw, J.A.; Gao, R.S.; Holloway, J.S.; Lack, D.A.; Langridge, J.M.; Peischl, J.; et al. Characteristics of Black Carbon Aerosol from a Surface Oil Burn During the Deepwater Horizon Oil spill. Geophys. Res. Lett. 2011, 38, 17. [Google Scholar] [CrossRef]
- Kumar, P.; Morawska, L.; Birmili, W.; Paasonen, P.; Hu, M.; Kulmala, M.; Harrison, R.M.; Norford, L.; Britter, R. Ultrafine particles in cities. Environ. Int. 2014, 66, 1–10. [Google Scholar] [CrossRef]
- Sabaliauskas, K.; Jeong, C.H.; Yao, X.; Jun, Y.S.; Jadidian, P.; Evans, G.J. Five-year roadside measurements of ultrafine particles in a major Canadian city. Atmos. Environ. 2012, 49, 245–256. [Google Scholar] [CrossRef]
- Heal, M.R.; Kumar, P.; Harrison, R.M. Particles, air quality, policy and health. Chem. Soc. Rev. 2012, 41, 6606–6630. [Google Scholar] [CrossRef]
- Birmili, W.; Tomsche, L.; Sonntag, A.; Opelt, C.; Weinhold, K.; Nordmann, S.; Schmidt, W. Variability of aerosol particles in the urban atmosphere of Dresden (Germany). Effects of spatial scale and particle size. Meteorol. Z. 2013, 22, 195–211. [Google Scholar] [CrossRef]
- Costabile, F.; Birmili, W.; Klose, S.; Tuch, T.; Wehner, B.; Wiedensohler, A.; Franck, U.; König, K.; Sonntag, A. Spatiotemporal variability and principal components of the particle number size distribution in an urban atmosphere. Atmos. Chem. Phys. 2009, 9, 3163–3195. [Google Scholar] [CrossRef]
- Ross, Z.; Ito, K.; Johnson, S.; Yee, M.; Pezeshki, G.; Clougherty, J.E.; Savitz, D.; Matte, T. Spatial and temporal estimation of air pollutants in New York City: Exposure assignment for use in a birth outcomes study. Environ. Health 2013, 12, 1–13. Available online: http://www.ehjournal.net/content/12/1/51 (accessed on 11 July 2014). [CrossRef] [PubMed]
- Peres, L.C.; Trapido, E.; Rung, A.L.; Harrington, D.J.; Oral, E.; Fang, Z.; Fontham, E.; Peters, E.S. The Deepwater Horizon Oil Spill and Physical Health among Adult Women in Southern Louisiana: The Women and Their Children’s Health (WaTCH) Study. Environ. Health Perspect. 2016, 124, 1208–1213. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. FastStats: Older Persons’ Health. National Center for Health Statistics. 2021. Available online: https://www.cdc.gov/nchs/fastats/older-american-health.htm (accessed on 15 February 2021).
- GIS Geography. Open Source Louisiana Parish Map. 2021. Available online: https://gisgeography.com/louisiana-parish-map/ (accessed on 23 March 2021).
- Environmental Protection Agency. List of Designated Reference and Equivalent Methods. Office of Research and Development. 2014. Available online: www.epa.gov/ttn/amtic/criteria.html (accessed on 28 July 2014).
- Hernandez, G.; Berry, T.-A.; Wallis, S.L.; Poyner, D. Temperature and Humidity Effects on Particulate Matter Concentrations in a Sub-Tropical Climate During Winter. Proc. Int. Conf. Environ. Chem. Biol. 2017, 102, 41–49. [Google Scholar] [CrossRef]
- Index Mundi. Louisiana Land Area in Square Miles, 2010 by County. 2019. Available online: https://www.indexmundi.com/facts/united-states/quick-facts/louisiana/land-area#map (accessed on 24 February 2019).
- U.S. Census Bureau. County Population Totals: 2010–2019. 2020. Available online: https://www.census.gov/data/tables/time-series/demo/popest/2010s-counties-total.html (accessed on 1 February 2021).
- Louisiana State Center for Health Statistics. Louisiana State Office of Public Health, New Orleans, LA. (Data by Request, Received on 4 February 2021). Available online: https://ldh.la.gov/index.cfm/page/647 (accessed on 25 January 2021).
- Soneja, S.; Chen, C.; Tielsch, J.M.; Katz, J.; Zeger, S.L.; Checkley, W.; Curriero, F.C.; Breysse, P.N. Humidity and gravimetric equivalency adjustments for nephelometer-based particulate matter measurements of emissions from solid biomass fuel use in cookstoves. Int. J. Environ. Res. Public Health 2014, 11, 6400–6416. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Bo, H.; Changhe, C.; Ping, D.; Lei, Z.; Guanghong, F. Scattering properties of atmospheric aerosols over Lanzhou City and applications using an integrating nephelometer. Adv. Atmos. Sci. 2004, 21, 848–856. [Google Scholar] [CrossRef]
- Sioutas, C.; Kim, S.; Chang, M.; Terrell, L.L.; Gong, H., Jr. Field evaluation of a modified DataRAM MIE scattering monitor for real-time PM2. 5 mass concentration measurements. Atmos. Environ. 2000, 34, 4829–4838. [Google Scholar] [CrossRef]
- Chakrabarti, B.; Fine, P.M.; Delfino, R.; Sioutas, C. Performance evaluation of the active-flow personal DataRAM PM2. 5 mass monitor (Thermo Anderson pDR-1200) designed for continuous personal exposure measurements. Atmos. Environ. 2004, 38, 3329–3340. [Google Scholar] [CrossRef]
- Covert, D.S.; Waggoner, A.P.; Weiss, R.E.; Ahlquist, N.C.; Charlson, R.J. Atmospheric aerosols, humidity, and visibility. In The Character and Origins of Smog Aerosols: A Digest of Results from the California Aerosol Characterization Experiment (ACHEX); Advances in Environmental Science and Technology: V. 9; Hidy, G.M., Mueller, P.K., Grosjean, D., Appel, B.R., Wesolowski, J.J., Eds.; John Wiley & Sons, Inc.: New York, NY, USA, 1980; pp. 559–581. [Google Scholar]
- Environmental Protection Agency. Air Quality Criteria for Particulate Matter; EPA/600/P-95/001bF; Office of Research and Development: Washington, DC, USA, 1996; Volume II of III. [Google Scholar]
- National Oceanic and Atmospheric Administration. National Centers for Environmental Information (formerly National Climatic Data Center). Available online: https://www.ncdc.noaa.gov/cdo-web/ (accessed on 20 December 2020).
- Environmental Protection Agency. EPA Response to the BP Oil Spill in the Gulf of Mexico. 2013. Available online: https://archive.epa.gov/emergency/bpspill/web/html/epa.html (accessed on 27 May 2015).
- Gorard, S. Revisiting a 90-year-old debate: The advantages of the mean deviation. Br. J. Educ. Stud. 2005, 53, 417–430. [Google Scholar] [CrossRef]
- Leys, C.; Delacre, M.; Mora, Y.L.; Lakens, D.; Ley, C. How to classify, detect, and manage univariate and multivariate outliers, with emphasis on pre-registration. Int. Rev. Soc. Psychol. 2019, 32, 1–10. [Google Scholar] [CrossRef]
- Russell, M.; Allen, D.T.; Collins, D.R.; Fraser, M.P. Daily, Seasonal, and Spatial Trends in PM2.5 Mass and Composition in Southeast Texas Special Issue of Aerosol Science and Technology on Findings from the Fine Particulate Matter Supersites Program. Aerosol Sci. Technol. 2004, 38, 14–26. [Google Scholar] [CrossRef][Green Version]
- Chen, R.; Peng, R.D.; Meng, X.; Zhou, Z.; Chen, B.; Kan, H. Seasonal variation in the acute effect of particulate air pollution on mortality in the China Air Pollution and Health Effects Study (CAPES). Sci. Total Environ. 2013, 450–451, 259–265. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Air Quality Measures on the National Environmental Health Tracking Network. 2018. Available online: https://data.cdc.gov/Environmental-Health-Toxicology/Air-Quality-Measures-on-the-National-Environmental/cjae-szjv (accessed on 20 March 2021).
- George, D.; Mallery, M. SPSS for Windows Step by Step: A Simple Guide and Reference, 10th ed.; 17.0 Update; Pearson: Boston, MA, USA, 2010. [Google Scholar]
- Gravetter, F.; Wallnau, L. Essentials of Statistics for the Behavioral Sciences, 8th ed.; Belmont, CA: Wadsworth, OH, USA, 2014. [Google Scholar]
- Ghasemi, A.; Zahediasl, S. Normality Tests for Statistical Analysis: A Guide for Non-Statisticians. Int. J. Endocrinol. Metab. 2012, 10, 486–489. [Google Scholar] [CrossRef]
- Hair, J.F., Jr.; Babin, B.; Anderson, R.E. Multivariate Analysis: A Global Perspective; Kennesaw State University: Kennesaw, GA, USA, 2010. [Google Scholar]
- Liu, Y.; Pan, J.; Zhang, H.; Shi, C.; Li, G.; Peng, Z.; Ma, J.; Zhou, Y.; Zhang, L. Short-term exposure to ambient air pollution and asthma mortality. Am. J. Respir. Crit. Care Med. 2019, 200, 24–32. [Google Scholar] [CrossRef]
- Goldstein, B.D.; Osofsky, H.J.; Lichtveld, M.Y. The Gulf Oil Spill. N. Engl. J. Med. 2011, 364, 1334–1348. [Google Scholar] [CrossRef]





| Modeled Data | Mobile Data | |||||||
|---|---|---|---|---|---|---|---|---|
| Sample Size, n | Mean μg/m3 | Median μg/m3 | Short-term Increases STI | Sample Size, n | Mean μg/m3 | Median μg/m3 | Short-term Increases STI | |
| Jefferson | 403 | 13.03 | 13.03 | 3 | 19,106 | 15.97 | 13.50 | 1932 |
| Lafourche | 563 | 12.87 | 13.03 | 3 | 32,967 | 17.28 | 14.40 | 4290 |
| Orleans | 223 | 13.13 | 12.78 | 3 | 4681 | 17.45 | 14.50 | 722 |
| Plaquemines | 572 | 13.38 | 13.20 | 2 | 18,478 | 14.64 | 12.00 | 2029 |
| St. Bernard | 320 | 13.95 | 13.88 | 3 | 10,255 | 16.62 | 13.60 | 1140 |
| Terrebonne | 391 | 12.75 | 12.89 | 2 | 15,775 | 16.62 | 14.00 | 1477 |
| Region | 2472 | 13.22 | 13.18 | 16 | 101,262 | 16.39 | 13.60 | 11,590 |
| OLS Regression | n | R | R2 | Adj. R2 | SE | β | ρ | 95% CI |
|---|---|---|---|---|---|---|---|---|
| Simple | ||||||||
| Jefferson | 31 | 0.46 | 0.21 | 0.18 | 14.37 | 0.1799 | 0.0096 ** | (0.05,0.31) |
| Lafourche | 33 | 0.44 | 0.19 | 0.16 | 3.485 | 0.0164 | 0.0113 * | (0.00,0.03) |
| Terrebonne | 26 | 0.41 | 0.17 | 0.13 | 3.248 | 0.0326 | 0.0326 * | (0.00,0.06) |
| Multiple | 33 | 0.71 | 0.51 | 0.46 | 16.09 | |||
| Jefferson | 0.1679 | 0.0443 * | (0.01,0.33) | |||||
| Lafourche | 0.0632 | 0.0496 * | (0.00,0.13) | |||||
| Terrebonne | 0.1868 | 0.0116 * | (0.04,0.33) | |||||
| Simple | ||||||||
| Unaggregated | 33 | 0.66 | 0.43 | 0.41 | 16.77 | 0.1046 | 3.53E-5 *** | (0.06,0.15) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nance, E. Monitoring Air Pollution Variability during Disasters. Atmosphere 2021, 12, 420. https://doi.org/10.3390/atmos12040420
Nance E. Monitoring Air Pollution Variability during Disasters. Atmosphere. 2021; 12(4):420. https://doi.org/10.3390/atmos12040420
Chicago/Turabian StyleNance, Earthea. 2021. "Monitoring Air Pollution Variability during Disasters" Atmosphere 12, no. 4: 420. https://doi.org/10.3390/atmos12040420
APA StyleNance, E. (2021). Monitoring Air Pollution Variability during Disasters. Atmosphere, 12(4), 420. https://doi.org/10.3390/atmos12040420