
Cochlear Implant Challenges in Children with Ichthyosis: A Systematic Review

 ,
,
Abstract
1. Introduction
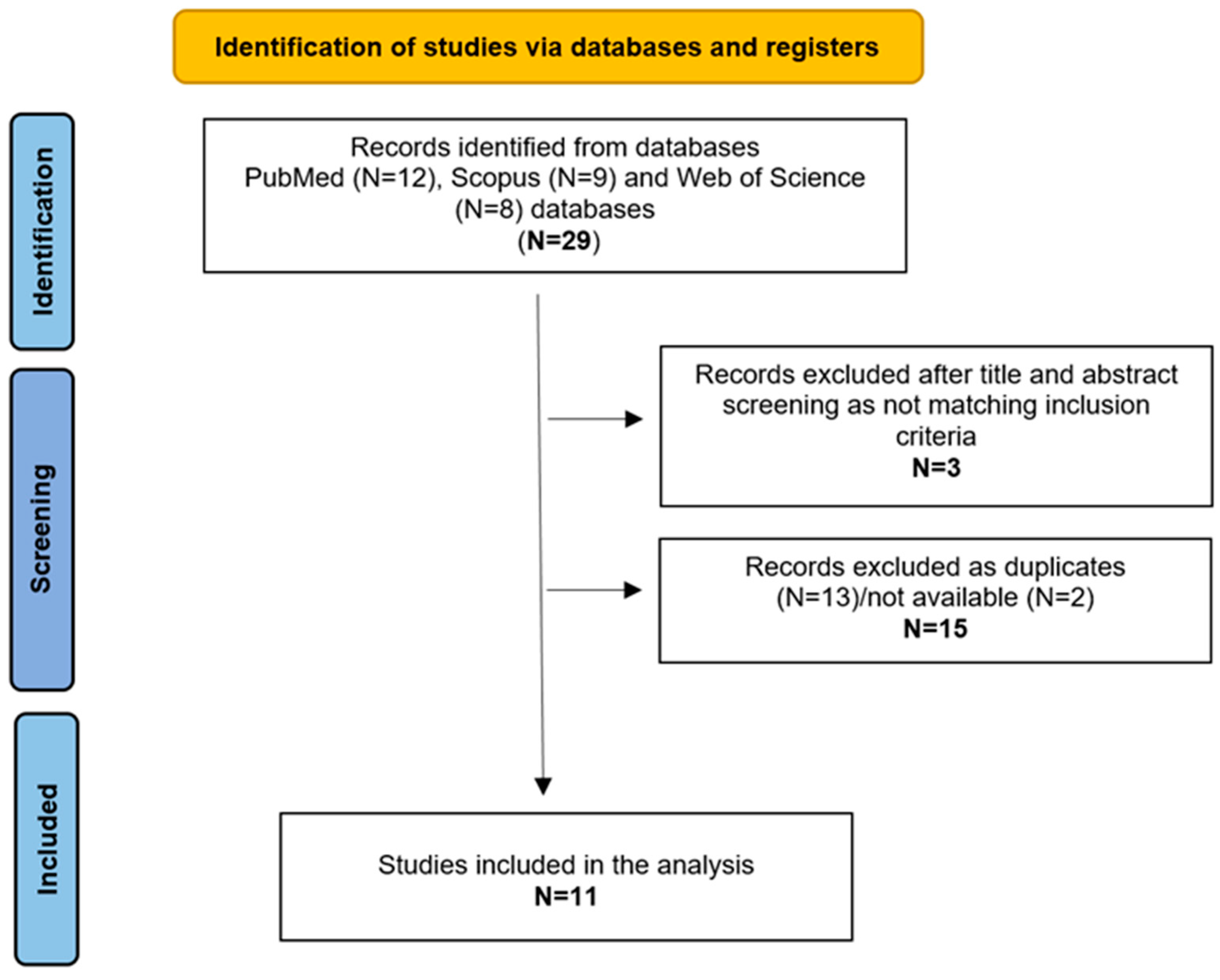
2. Materials and Methods
3. Results
3.1. Population
3.2. Genetic Analysis
3.3. Clinical Features
3.4. Imaging
3.5. Audiological Evaluation
3.6. Therapy, Auditory Rehabilitation, and Outcomes
3.7. Follow-Up and Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Traupe, H.; Fischer, J.; Oji, V. Nonsyndromic types of ichthyoses—An update. J. Dtsch. Dermatol. Ges. 2014, 12, 109–121. [Google Scholar] [CrossRef] [PubMed]
- Oji, V.; Tadini, G.; Akiyama, M.; Bardon, C.B.; Bodemer, C.; Bourrat, E.; Coudiere, P.; DiGiovanna, J.J.; Elias, P.; Fischer, J.; et al. Revised nomenclature and classification of inherited ichthyoses: Results of the First Ichthyosis Consensus Conference in Sorèze 2009. J. Am. Acad. Dermatol. 2010, 63, 607–641. [Google Scholar] [CrossRef]
- Cushing, S.L.; MacDonald, L.; Propst, E.J.; Sharma, A.; Stockley, T.; Blaser, S.L.; James, A.L.; Papsin, B.C. Successful cochlear implantation in a child with Keratosis, Icthiosis and Deafness (KID) Syndrome and Dandy-Walker malformation. Int. J. Pediatr. Otorhinolaryngol. 2008, 72, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Lamprecht, A.; Goecke, T.; Anton-Lamprecht, I.; Kuster, W. Progressive erythrokeratodermia cochlear hearing impairment: A case report review of the literature. Int. J. Pediatr. Otorhinolaryngol. 1988, 15, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Gumus, B.; Incesulu, A.; Pinarbasli, M.O. Cochlear Implantation in Patients with Keratitis-Ichthyosis-Deafness Syndrome: A Report of Two Cases. Case Rep. Otolaryngol. 2017, 2017, 3913187. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Hampton, S.M.; Toner, J.G.; Small, J. Cochlear implant extrusion in a child with keratitis, ichthyosis and deafness syndrome. J. Laryngol. Otol. 1997, 111, 465–467. [Google Scholar] [CrossRef] [PubMed]
- Smyth, C.M.; Sinnathuray, A.R.; Hughes, A.E.; Toner, J.G. Cochlear implantation in keratitis-ichthyosis-deafness syndrome: 10-year follow-up of two patients. Cochlear. Implants Int. 2012, 13, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, S.; McKenna, K. Keratitis-ichthyosis-deafness syndrome and carotenaemia. Clin. Exp. Dermatol. 2003, 28, 394–396. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.P.; Peng, J.J.; Zheng, H. Cochlear implantation in child with keratitis-ichthyosis-deafness syndrome: A case report. Asian J. Surg. 2023, 46, 903–904. [Google Scholar] [CrossRef]
- Choung, Y.H.; Shin, Y.R.; Kim, H.J.; Kim, Y.C.; Ahn, J.H.; Choi, S.J.; Jeong, S.Y.; Park, K. Cochlear implantation and connexin expression in the child with keratitis-ichthyosis-deafness syndrome. Int. J. Pediatr. Otorhinolaryngol. 2008, 72, 911–915. [Google Scholar] [CrossRef] [PubMed]
- Arndt, S.; Aschendorff, A.; Schild, C.; Beck, R.; Maier, W.; Laszig, R.; Birkenhäger, R. A novel dominant and a de novo mutation in the GJB2 gene (connexin-26) cause keratitis-ichthyosis-deafness syndrome: Implication for cochlear implantation. Otol. Neurotol. 2010, 31, 210–215. [Google Scholar] [CrossRef]
- Barker, E.J.; Briggs, R.J. Cochlear implantation in children with keratitis-ichthyosis-deafness (KID) syndrome: Outcomes in three cases. Cochlear. Implants Int. 2009, 10, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Sinnathuray, A.R.; Toner, J.G.; Geddis, A.; Clarke-Lyttle, J.; Patterson, C.C.; Hughes, A.E. Auditory perception and speech discrimination after cochlear implantation in patients with connexin 26 (GJB2) gene-related deafness. Otol. Neurotol. 2004, 25, 930–934. [Google Scholar] [CrossRef]
- Markova, T.G.; Brazhkina, N.B.; Bliznech, E.A.; Bakhshinyan, V.V.; Polyakov, A.V.; Tavartkiladze, G.A. Phenotype in a patient with p.D50N mutation in GJB2 gene resemble both KID and Clouston syndromes. Int. J. Pediatr. Otorhinolaryngol. 2016, 81, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Krogmann, R.J.; Al Khalili, Y. Cochlear Implants. [Updated 2023 Jul 24]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK544280/ (accessed on 28 November 2024).
- Marschark, M.; Spencer, L.J.; Durkin, A.; Borgna, G.; Convertino, C.; Machmer, E.; Kronenberger, W.G.; Trani, A. Understanding language, hearing status, and visual-spatial skills. J. Deaf Stud. Deaf Educ. 2015, 20, 310–330. [Google Scholar] [CrossRef] [PubMed]
- Cohen, N.L.; Hoffman, R.A. Complications of cochlear implant surgery in adults and children. Ann. Otol. Rhinol. Laryngol. 1991, 100 Pt 1, 708–711. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Reference | N and Gender | Genetic Analysis | PTA | Imaging | Comorbidity (except for common otological and skin problems connected to the disease itself) | PA e CI (Age) | Outcome with CI: PTA and/or Language | Complications | Follow-Up |
| Hampton et al., 1997 [7] | 1 F | NR | Profound bilateral SNHL | NR | None | HAs, CI (unspecified whether mono-or bilateral) | Improved PTA Discrimination, speech and imitation improved steadily. | Infection and extensive wound dehiscence | NR |
| Smyth et al., 2012 [8] | 2 (1M, 1F) | D50N: c.148G>A | Profound bilateral HL | CT neative | Shortening of Achilles tendon | HAs, Monolateral CI (for both patients) | Improved PTA and Speech. Poor discrimination, use of sign language | Otitis externa, progressive extensive wound dehiscence, CI explantation, intermittent ottorrhoea, TM perforation | 10 y |
| Ahmadi et al., 2003 [9] | 1 F | NR | SNHL | NR | Prematurity, carotenaemia, encephalomyelitis, shortening of Achilles tendon, | CI (9 m) (unspecified whether mono-or bilateral) | Unsuccessful CI | Poor wound healing | NR |
| Wang et al., 2023 [10] | 1 F | D50N: c.50C>T p.S17F | Profound SNHL | Negative | Elderlylike appearance, photophobia | Monolateral CI | Improved PTA | Mild incision irritating, incision infection | NR |
| Choung et al., 2008 [11] | 1 M | D50N: c.148G>A | Profound SNHL | Negative | Tongue with ulcerative and angular cheilitis, severely decreased visual acuity, neovascularization, corneal scarring, photophobia | HAs (1 y), Monolateral CI | Improved PTA | Difficulties in hearing rehabilitation due to low visual impairment, skin irritation | NR |
| Gumus et al., 2017 [5] | 2 (1M, 1F) | NR | Severe -Profound SNHL | NR | Motor growth retardation | HAs (4 y;10 m), Monolateral CI (7 y; 5 y) | Improved PTA, perception and speech | None | 1 y; 20 m |
| Arndt et al., 2010 [12] | 2 F | D50N: c.89 T>A; GAC9AAC: p.Asp50Asn. | Severe progressive bilateral SNHL | NR | Skin manifestations, bright light sensitivity | - HA (16y), Sequential CI (20 y–25 y); - HAs (3 m), Sequential CI (14m-planned) | Improved open-speech comprehension awarness | Changes in skin morphology under the transmitter coil, skin necrosis, wound dehiscence and partial extrusion of the implant | 7 m |
| Cushing et al., 2008 [3] | 1 (gender unspecified) | D50A: c.149A>C | Profound bilateral SNHL | MRI: hypoplasia of the inferior cerebellar vermis and the fourth ventricle, large posterior fossa midline cyst; CT: hypoplastic cochlea, deficient roof of the SSC on the left and a small modiolus on the right. | Blepharitis, bilateral corneal pannus, mild vascularization, corneal | HAs (5 m), CI (1 y) | Improved PTA, perception and speech. Difficult in open set testing | Incision infection | 4 y |
| Barker et al., 2009 [13] | 3 (gender unspecified) | NR | Severe-Profound bilateral SNHL | NR | Gait problems, Shortening of Achilles tendon, calf and knee muscles, recurrent corneal infections, photophobia | HAs, - Sequential CIs (14 m, 47 m); - Monolateral CI (28 m); - Sequential CI (39 m, 62 m) | Improved speech and language | Abscess of the external ear canal and parotid, recurrent otitis media with otorrhoea, middle ear effusion, skin thickening over the site of the device, mastoiditis | 42 m; 26 m; 12 m |
| Sinnathuray et al., 2004 [14] | 32 (gender unspecified) | D50N: c.35G; D50N: c.35G/169C>T; deletion in GJB6; GJB2-unrelated deafness (20) | Profound SNHL | NR | NR | NR | Improved perception GJB2-related deafness> GJB2-unrelated deafness | NR | NR |
| Markova et al., 2016 [15] | 1F | D50N | Severe bilateral SNHL | NR | None | HAs (30 m), Monolateral CI (42 m) | Improved PTA, perception speech and language | NR | 7 y |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caragli, V.; Luppi, L.; Tegmeyer, N.C.; Genovese, E.; Soloperto, D. Cochlear Implant Challenges in Children with Ichthyosis: A Systematic Review. Genes 2025, 16, 129. https://doi.org/10.3390/genes16020129
Caragli V, Luppi L, Tegmeyer NC, Genovese E, Soloperto D. Cochlear Implant Challenges in Children with Ichthyosis: A Systematic Review. Genes. 2025; 16(2):129. https://doi.org/10.3390/genes16020129
Chicago/Turabian StyleCaragli, Valeria, Laura Luppi, Nicole Carrie Tegmeyer, Elisabetta Genovese, and Davide Soloperto. 2025. "Cochlear Implant Challenges in Children with Ichthyosis: A Systematic Review" Genes 16, no. 2: 129. https://doi.org/10.3390/genes16020129
APA StyleCaragli, V., Luppi, L., Tegmeyer, N. C., Genovese, E., & Soloperto, D. (2025). Cochlear Implant Challenges in Children with Ichthyosis: A Systematic Review. Genes, 16(2), 129. https://doi.org/10.3390/genes16020129