
Increased Risk of Hereditary Prostate Cancer in Italian Families with Hereditary Breast and Ovarian Cancer Syndrome Harboring Mutations in BRCA and in Other Susceptibility Genes
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Mutational Analysis
2.3. Genetic Variant Classification
3. Results
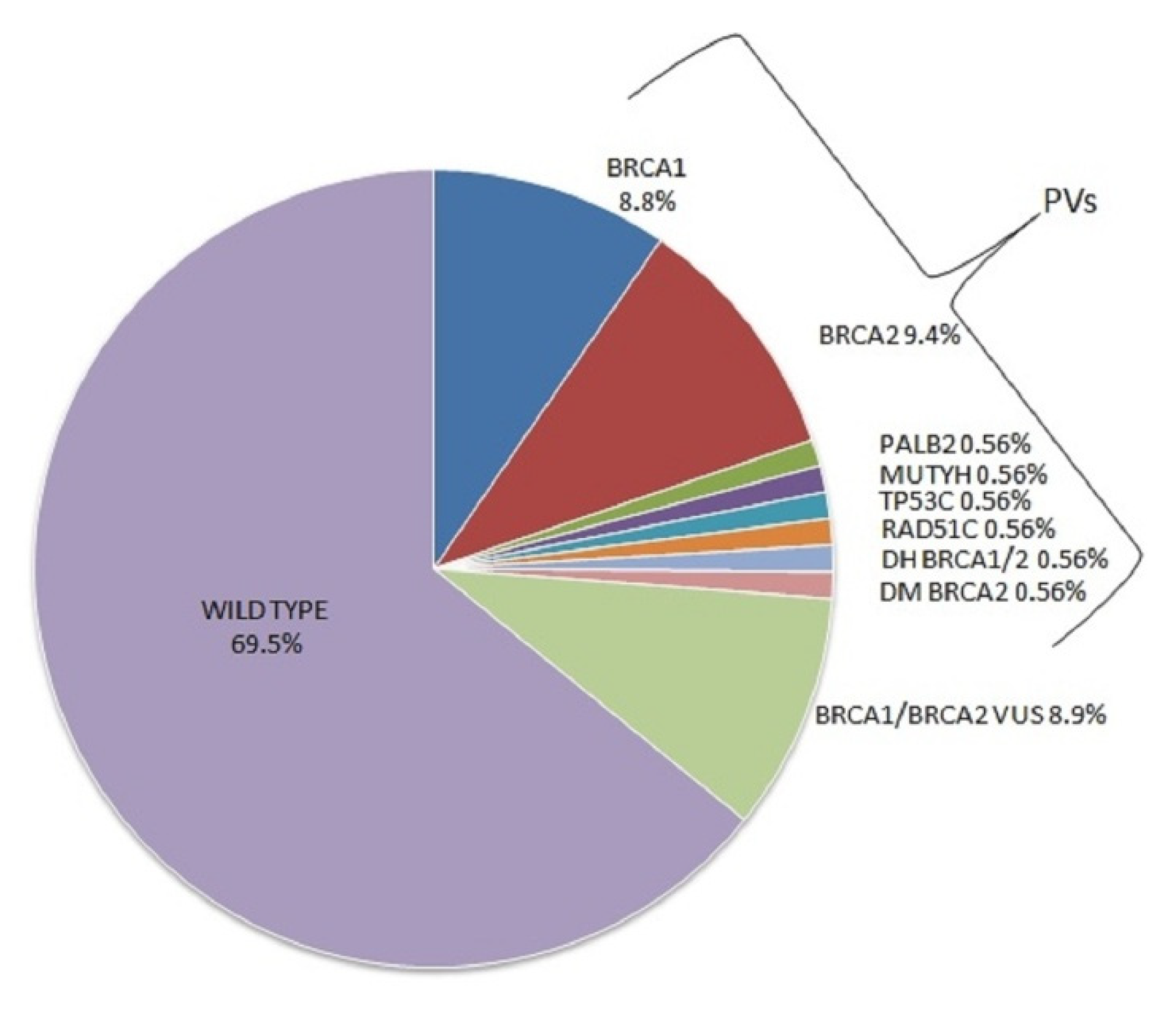
3.1. Mutations in DNA Damage Repair Genes
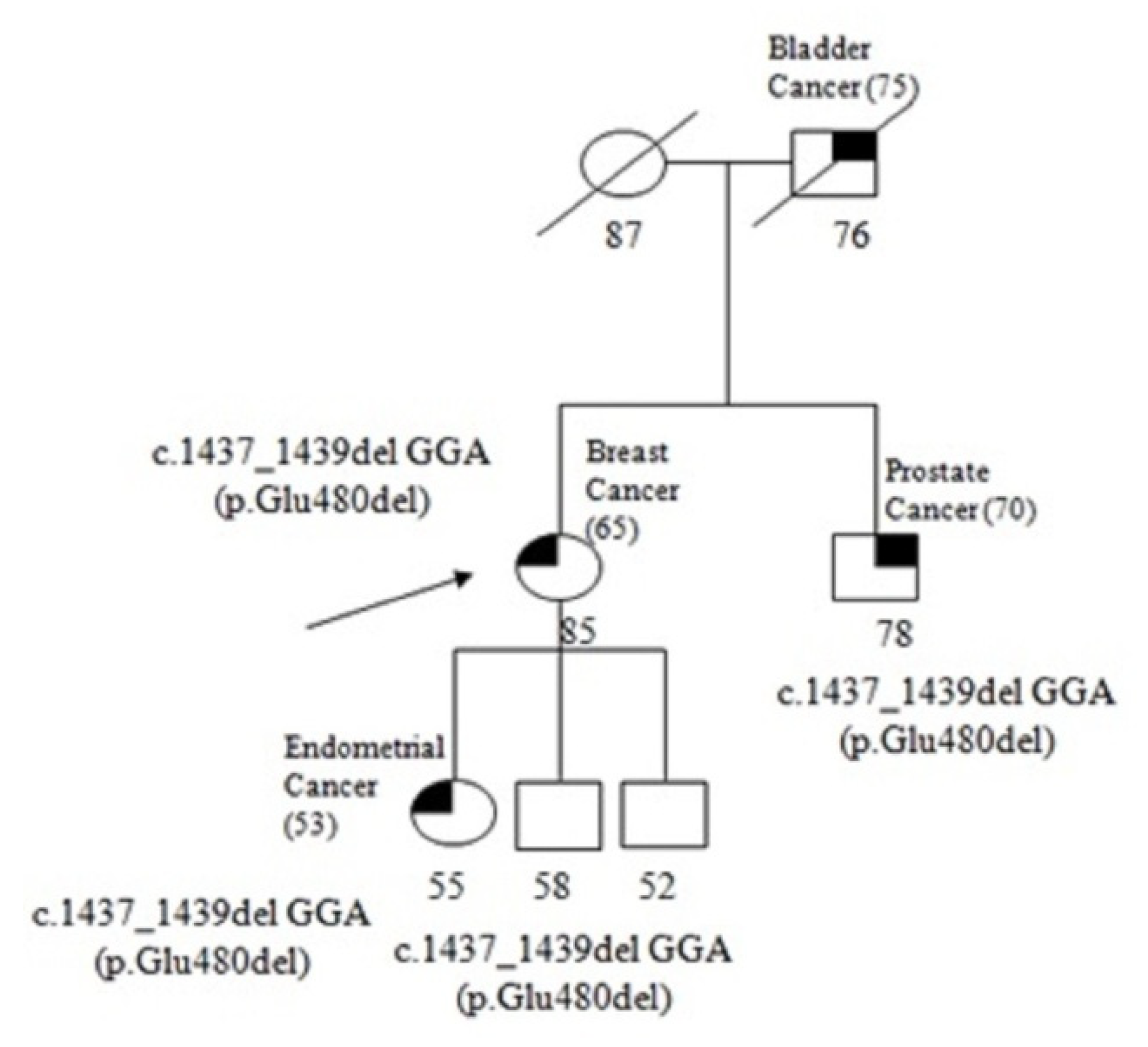
3.2. Mutations in Base Excision Repair Gene
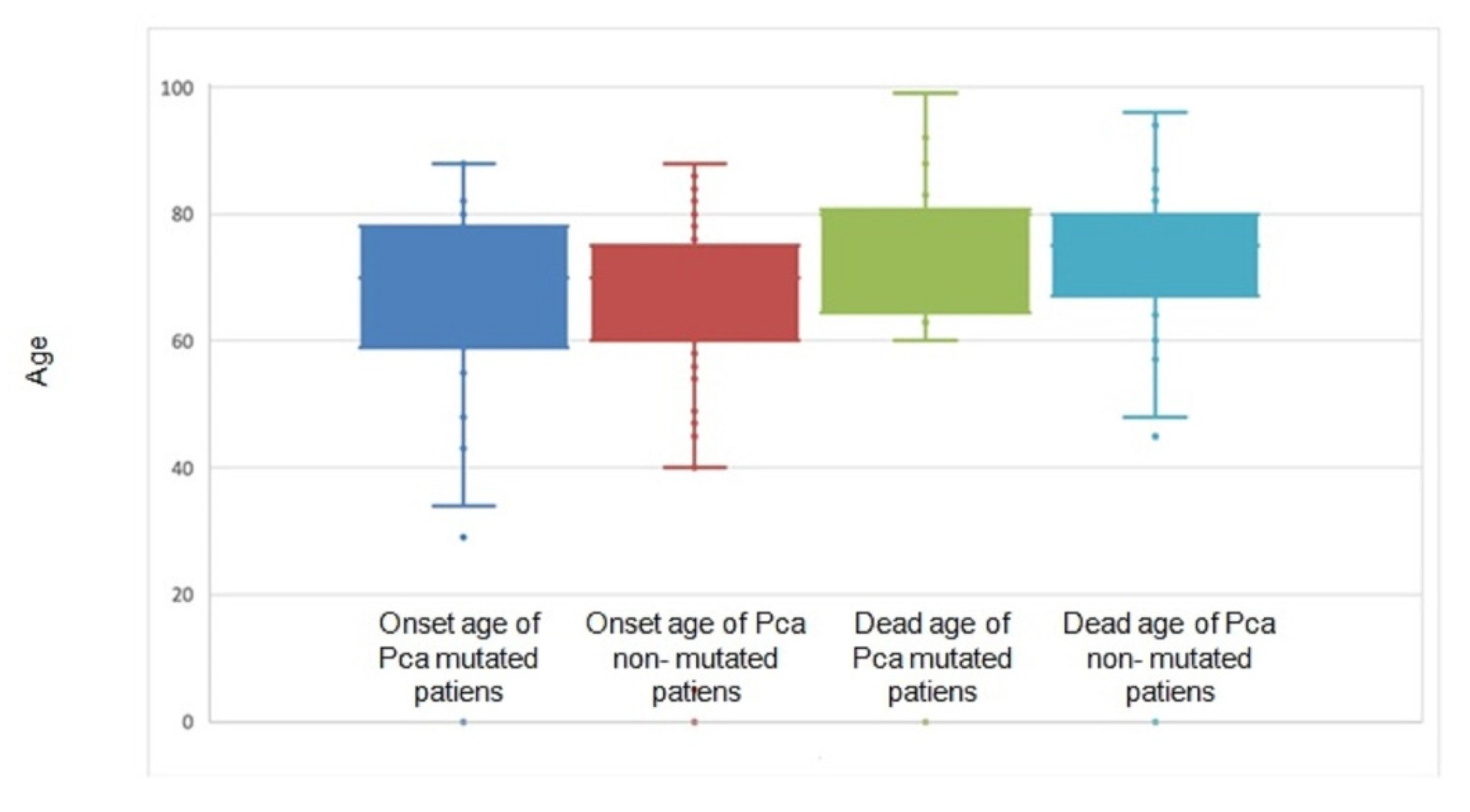
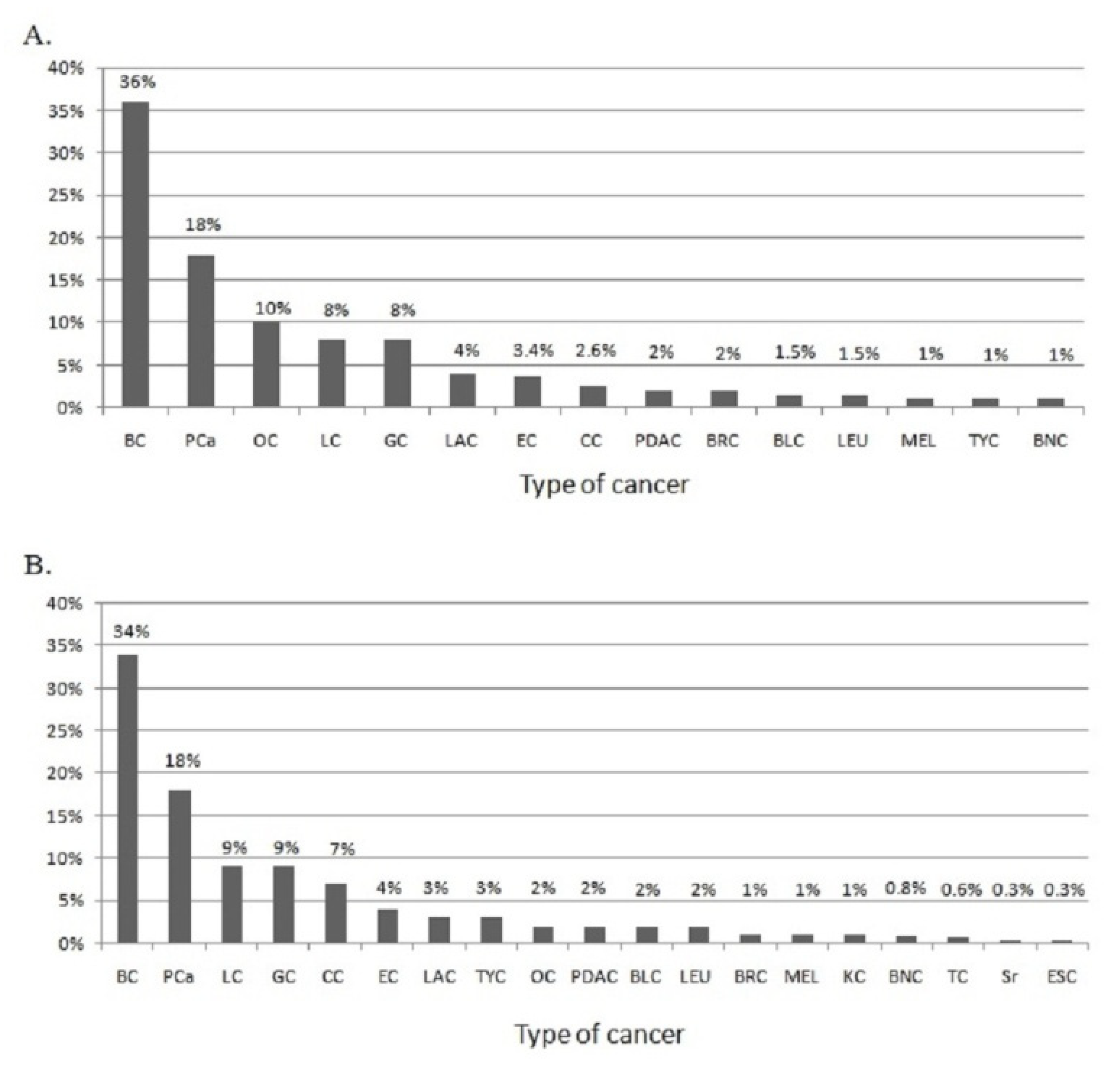
3.3. Genotype–Phenotype Correlation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rebello, R.J.; Oing, C.; Knudsen, K.E.; Loeb, S.; Johnson, D.C.; Reiter, R.E.; Gillessen, S.; Van der Kwast, T.; Bristow, R.G. Prostate cancer. Nat. Rev. Dis. Prim. 2021, 7, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Heidegger, I.; Tsaur, I.; Borgmann, H.; Surcel, C.; Kretschmer, A.; Mathieu, R.; De Visschere, P.; Valerio, M.; Bergh, R.C.V.D.; Ost, P.; et al. EAU-YAU Prostate Cancer Working Party. Hereditary prostate cancer—Primetime for genetic testing? Cancer Treat. Rev. 2019, 81, 101927. [Google Scholar] [CrossRef] [PubMed]
- Vietri, M.; D’Elia, G.; Caliendo, G.; Resse, M.; Casamassimi, A.; Passariello, L.; Albanese, L.; Cioffi, M.; Molinari, A. Hereditary Prostate Cancer: Genes Related, Target Therapy and Prevention. Int. J. Mol. Sci. 2021, 22, 3753. [Google Scholar] [CrossRef] [PubMed]
- Rebbeck, T.R. Prostate Cancer Genetics: Variation by Race, Ethnicity, and Geography. Semin. Radiat. Oncol. 2016, 27, 3–10. [Google Scholar] [CrossRef]
- Barber, L.E.; Gerke, T.; Markt, S.C.; Peisch, S.F.; Wilson, K.M.; Ahearn, T.U.; Giovannucci, E.L.; Parmigiani, G.; Mucci, L.A. Family History of Breast or Prostate Cancer and Prostate Cancer Risk. Clin. Cancer Res. 2018, 24, 5910–5917. [Google Scholar] [CrossRef]
- Vietri, M.T.; D’Elia, G.; Caliendo, G.; Casamassimi, A.; Resse, M.; Passariello, L.; Cioffi, M.; Molinari, A.M. Double mutation of APC and BRCA1 in an Italian family. Cancer Genet. 2020, 244, 32–35. [Google Scholar] [CrossRef]
- Vietri, M.T.; D’Elia, G.; Caliendo, G.; Casamassimi, A.; Federico, A.; Passariello, L.; Cioffi, M.; Molinari, A.M. Prevalence of mutations in BRCA and MMR genes in patients affected with hereditary endometrial cancer. Med. Oncol. 2021, 38, 1–10. [Google Scholar] [CrossRef]
- Vietri, M.T.; Molinari, A.M.; De Paola, M.L.; Cantile, F.; Fasano, M.; Cioffi, M. Identification of a novel in-frame deletion in BRCA2 and analysis of variants of BRCA1/2 in Italian patients affected with hereditary breast and ovarian cancer. Clin. Chem. Lab. Med. (CCLM) 2012, 50, 2171–2180. [Google Scholar] [CrossRef]
- Vietri, M.T.; D’Elia, G.; Benincasa, G.; Ferraro, G.; Caliendo, G.; Nicoletti, G.F.; Napoli, C. DNA methylation and breast cancer: A way forward (Review). Int. J. Oncol. 2021, 59, 1–12. [Google Scholar] [CrossRef]
- Das, S.; Salami, S.S.; Spratt, D.E.; Kaffenberger, S.D.; Jacobs, M.F.; Morgan, T.M. Bringing Prostate Cancer Germline Genetics into Clinical Practice. J. Urol. 2019, 202, 223–230. [Google Scholar] [CrossRef]
- González-Santiago, S.; the SEOM Hereditary Cancer Working Group; Cajal, T.R.Y.; Aguirre, E.; Alés-Martínez, J.E.; Andrés, R.; Balmaña, J.; Graña, B.; Herrero, A.; Llort, G.; et al. SEOM clinical guidelines in hereditary breast and ovarian cancer (2019). Clin. Transl. Oncol. 2019, 22, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Vietri, M.T.; Molinari, A.M.; Caliendo, G.; De Paola, M.L.; D’Elia, G.; Gambardella, A.L.; Petronella, P.; Cioffi, M. Double heterozygosity in the BRCA1 and BRCA2 genes in Italian family. Clin. Chem. Lab. Med. 2013, 51, 2319–2324. [Google Scholar] [CrossRef] [PubMed]
- Vietri, M.T.; Caliendo, G.; Schiano, C.; Casamassimi, A.; Molinari, A.M.; Napoli, C.; Cioffi, M. Analysis of PALB2 in a cohort of Italian breast cancer patients: Identification of a novel PALB2 truncating mutation. Fam. Cancer 2015, 14, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Vietri, M.T.; Caliendo, G.; Casamassimi, A.; Cioffi, M.L.; De Paola, M.; Napoli, C.; Molinari, A.M. A novel PALB2 truncating mutation in an Italian family with male breast cancer. Oncol. Rep. 2015, 33, 1243–1247. [Google Scholar] [CrossRef]
- Plon, S.E.; Eccles, D.M.; Easton, D.; Foulkes, W.D.; Genuardi, M.; Greenblatt, M.S.; Hogervorst, F.B.; Hoogerbrugge, N.; Spurdle, A.B.; Tavtigian, S.V.; et al. Sequence variant classification and reporting: Recommendations for improving the interpretation of cancer susceptibility genetic test results. Hum. Mutat. 2008, 29, 1282–1291. [Google Scholar] [CrossRef]
- Pilarski, R. The Role of BRCA Testing in Hereditary Pancreatic and Prostate Cancer Families. Am. Soc. Clin. Oncol. Educ. Book 2019, 39, 79–86. [Google Scholar] [CrossRef]
- Sokolova, A.O.; Cheng, H.H. Genetic Testing in Prostate Cancer. Curr. Oncol. Rep. 2020, 22, 5. [Google Scholar] [CrossRef]
- Zhen, J.T.; Syed, J.; Nguyen, K.A.; Leapman, M.S.; Agarwal, N.; Ms, K.B.; Llor, X.; Hofstatter, E.; Shuch, B. Genetic testing for hereditary prostate cancer: Current status and limitations. Cancer 2018, 124, 3105–3117. [Google Scholar] [CrossRef]
- Pritchard, C.C.; Mateo, J.; Walsh, M.F.; De Sarkar, N.; Abida, W.; Beltran, H.; Garofalo, A.; Gulati, R.; Carreira, S.; Eeles, R.; et al. Inherited DNA-Repair Gene Mutations in Men with Metastatic Prostate Cancer. N. Engl. J. Med. 2016, 375, 443–453. [Google Scholar] [CrossRef]
- Gandaglia, G.; Briganti, A.; Montorsi, F. Reimagining prostate cancer screening: The IMPACT of germline mutations. Lancet Oncol. 2021, 22, 1491–1492. [Google Scholar] [CrossRef]
- Costa, D.; Scognamiglio, M.; Fiorito, C.; Benincasa, G.; Napoli, C. Genetic background, epigenetic factors and dietary interventions which influence human longevity. Biogerontology 2019, 20, 605–626. [Google Scholar] [CrossRef] [PubMed]
- Sarno, F.; the International Network Medicine Consortium; Benincasa, G.; List, M.; Barabasi, A.-L.; Baumbach, J.; Ciardiello, F.; Filetti, S.; Glass, K.; Loscalzo, J.; et al. Clinical epigenetics settings for cancer and cardiovascular diseases: Real-life applications of network medicine at the bedside. Clin. Epigenetics 2021, 13, 1–38. [Google Scholar] [CrossRef] [PubMed]
- Maiorino, M.I.; Schisano, B.; Di Palo, C.; Vietri, M.T.; Cioffi, M.; Giugliano, G.; Giugliano, D.; Esposito, K. Interleukin-20 circulating levels in obese women: Effect of weight loss. Nutr. Metab. Cardiovasc. Dis. 2010, 20, 180–185. [Google Scholar] [CrossRef]
- Cioffi, M.; Riegler, G.; Vietri, M.T.; Pilla, P.; Caserta, L.; Carratù, R.; Sica, V.; Molinari, A.M. Serum p53 antibodies in patients affected with ulcerative colitis. Inflamm. Bowel. Dis. 2004, 10, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Bellastella, G.; Maiorino, M.I.; De Bellis, A.; Vietri, M.T.; Mosca, C.; Scappaticcio, L.; Pasquali, D.; Esposito, K.; Giugliano, D. Serum but not salivary cortisol levels are influenced by daily glycemic oscillations in type 2 diabetes. Endocrine 2016, 53, 220–226. [Google Scholar] [CrossRef]
- Pritzlaff, M.; Tian, Y.; Reineke, P.; Stuenkel, A.J.; Allen, K.; Gutierrez, S.; Jackson, M.; Dolinsky, J.S.; LaDuca, H.; Xu, J.; et al. Diagnosing hereditary cancer predisposition in men with prostate cancer. Genet. Med. 2020, 22, 1517–1523. [Google Scholar] [CrossRef]
- Vietri, M.T.; Caliendo, G.; D’Elia, G.; Resse, M.; Casamassimi, A.; Minucci, P.B.; Ioio, C.D.; Cioffi, M.; Molinari, A.M. Five Italian Families with Two Mutations in BRCA Genes. Genes 2020, 11, 1451. [Google Scholar] [CrossRef]
- Iversen, E.S.; Lipton, G.; Hart, S.N.; Lee, K.Y.; Hu, C.; Polley, E.C.; Pesaran, T.; Yussuf, A.; LaDuca, H.; Chao, E.; et al. An integrative model for the comprehensive classification of BRCA1 and BRCA2 variants of uncertain clinical significance. npj Genom. Med. 2022, 7, 1–8. [Google Scholar] [CrossRef]
- Lyra, P.C.M.; Nepomuceno, T.C.; de Souza, M.L.M.; Machado, G.F.; Veloso, M.F.; Henriques, T.B.; dos Santos, D.Z.; Ribeiro, I.G.; Ribeiro, R.S.; Rangel, L.B.A.; et al. Integration of functional assay data results provides strong evidence for classification of hundreds of BRCA1 variants of uncertain significance. Genet. Med. 2020, 23, 306–315. [Google Scholar] [CrossRef]
- Edwards, S.M.; Evans, D.G.; Hope, Q.; Norman, A.R.; Barbachano, Y.; Bullock, S.; Kote-Jarai, Z.; Meitz, J.; Falconer, A.; Osin, P.; et al. UK Genetic Prostate Cancer Study Collaborators and BAUS Section of Oncology. Pros-tate cancer in BRCA2 germline mutation carriers is associated with poorer prognosis. Br. J. Cancer 2010, 7, 918–924. [Google Scholar] [CrossRef]
- Patel, V.L.; Busch, E.L.; Friebel, T.M.; Cronin, A.; Leslie, G.; McGuffog, L.; Adlard, J.; Agata, S.; Agnarsson, B.A.; Ahmed, M.; et al. Association of Genomic Domains in BRCA1 and BRCA2 with Prostate Cancer Risk and Aggressiveness. Cancer Res. 2020, 80, 624–638. [Google Scholar] [CrossRef] [PubMed]
- Paulo, P.; Pinto, P.; Peixoto, A.; Santos, C.; Pinto, C.; Rocha, P.; Veiga, I.; Soares, G.; Machado, C.; Ramos, F.; et al. Validation of a Next-Generation Sequencing Pipeline for the Molecular Diagnosis of Multiple Inherited Cancer Predisposing Syndromes. J. Mol. Diagn. 2017, 19, 502–513. [Google Scholar] [CrossRef] [PubMed]
- Horak, P.; Weischenfeldt, J.; von Amsberg, G.; Beyer, B.; Schütte, A.; Uhrig, S.; Gieldon, L.; Klink, B.; Feuerbach, L.; Hübschmann, D.; et al. Response to olaparib in a PALB2 germline mutated prostate cancer and genetic events associated with resistance. Mol. Case Stud. 2019, 5, a003657. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Guo, H.; Zhu, Y.; Xia, Y.; Cui, J.; Shi, K.; Fan, Y.; Shi, B.; Chen, S. TP53 alterations of hormone-naïve prostate cancer in the Chinese population. Prostate Cancer Prostatic Dis. 2020, 24, 482–491. [Google Scholar] [CrossRef]
- Teroerde, M.; Nientiedt, C.; Duensing, A.; Hohenfellner, M.; Stenzinger, A.; Duensing, S.; Bott, S.R.J.; Ng, K.L. Revisiting the Role of p53 in Prostate Cancer. In Prostate Cancer; Exon Publications: Brisbane, Australia, 2021; Chapter 8. [Google Scholar]
- D’Elia, G.; Caliendo, G.; Casamassimi, A.; Cioffi, M.; Molinari, A.M.; Vietri, M.T. APC and MUTYH Analysis in FAP Patients: A Novel Mutation in APC Gene and Genotype-Phenotype Correlation. Genes 2018, 9, 322. [Google Scholar] [CrossRef]
- Vietri, M.T.; D’Elia, G.; Caliendo, G.; Albanese, L.; Signoriello, G.; Napoli, C.; Molinari, A.M. Pancreatic Cancer with Mutation in BRCA1/2, MLH1, and APC Genes: Phenotype Correlation and Detection of a Novel Germline BRCA2 Mutation. Genes 2022, 13, 321. [Google Scholar] [CrossRef]
- Nicolosi, P.; Ledet, E.; Yang, S.; Michalski, S.; Freschi, B.; O’Leary, E.; Esplin, E.D.; Nussbaum, R.L.; Sartor, O. Prevalence of Germline Variants in Prostate Cancer and Implications for Current Genetic Testing Guidelines. JAMA Oncol. 2019, 5, 523–528. [Google Scholar] [CrossRef]
- Thalgott, M.; Kron, M.; Brath, J.M.; Ankerst, D.P.; Thompson, I.M.; Gschwend, J.E.; Herkommer, K. Men with family history of prostate cancer have a higher risk of disease recurrence after radical prostatectomy. World J. Urol. 2017, 36, 177–185. [Google Scholar] [CrossRef]
- Castro, E.; Goh, C.; Olmos, D.; Saunders, E.; Leongamornlert, D.; Tymrakiewicz, M.; Mahmud, N.; Dadaev, T.; Govindasami, K.; Guy, M.; et al. Germline BRCA Mutations Are Associated with Higher Risk of Nodal Involvement, Distant Metastasis, and Poor Survival Outcomes in Prostate Cancer. J. Clin. Oncol. 2013, 31, 1748–1757. [Google Scholar] [CrossRef]
- Castro, E.; Goh, C.; Leongamornlert, D.; Saunders, E.; Tymrakiewicz, M.; Dadaev, T.; Govindasami, K.; Guy, M.; Ellis, S.; Frost, D.; et al. Effect of BRCA Mutations on Metastatic Relapse and Cause-specific Survival After Radical Treatment for Localised Prostate Cancer. Eur. Urol. 2015, 68, 186–193. [Google Scholar] [CrossRef]
- Narod, S.A.; Neuhausen, S.; Vichodez, G.; Armel, S.; Lynch, H.T.; Ghadirian, P.; Cummings, S.; Olopade, O.; Stoppa-Lyonnet, D.; Couch, F.; et al. Rapid progression of prostate cancer in men with a BRCA2 mutation. Br. J. Cancer 2008, 99, 371–374. [Google Scholar] [CrossRef] [PubMed]
- Ren, Z.-J.; Cao, D.-H.; Zhang, Q.; Ren, P.-W.; Liu, L.-R.; Wei, Q.; Wei, W.-R.; Dong, Q. First-degree family history of breast cancer is associated with prostate cancer risk: A systematic review and meta-analysis. BMC Cancer 2019, 19, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Vietri, M.T.; Caliendo, G.; D’Elia, G.; Resse, M.; Casamassimi, A.; Minucci, P.B.; Cioffi, M.; Molinari, A.M. BRCA and PALB2 mutations in a cohort of male breast cancer with one bilateral case. Eur. J. Med Genet. 2020, 63, 103883. [Google Scholar] [CrossRef]
- Marabelle, A.; Le, D.T.; Ascierto, P.A.; Di Giacomo, A.M.; De Jesus-Acosta, A.; Delord, J.-P.; Geva, R.; Gottfried, M.; Penel, N.; Hansen, A.R.; et al. Efficacy of Pembrolizumab in Patients with Noncolorectal High Microsatellite Instability/Mismatch Repair–Deficient Cancer: Results From the Phase II KEYNOTE-158 Study. J. Clin. Oncol. 2020, 38, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Montisci, A.; Vietri, M.T.; Palmieri, V.; Sala, S.; Donatelli, F.; Napoli, C. Cardiac Toxicity Associated with Cancer Immunotherapy and Biological Drugs. Cancers 2021, 13, 4797. [Google Scholar] [CrossRef] [PubMed]
- Montisci, A.; Palmieri, V.; Liu, J.E.; Vietri, M.T.; Cirri, S.; Donatelli, F.; Napoli, C. Severe Cardiac Toxicity Induced by Cancer Therapies Requiring Intensive Care Unit Admission. Front. Cardiovasc. Med. 2021, 8, 713694. [Google Scholar] [CrossRef]
- Carreira, S.; Porta, N.; Arce-Gallego, S.; Seed, G.; Llop-Guevara, A.; Bianchini, D.; Rescigno, P.; Paschalis, A.; Bertan, C.; Baker, C.; et al. Biomarkers Associating with PARP Inhibitor Benefit in Prostate Cancer in the TOPARP-B Trial. Cancer Discov. 2021, 11, 2812–2827. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Syndrome | No. of Families | No. and Tumor Type of Probands | No. of PCa Cases |
|---|---|---|---|
| Hereditary breast and ovarian cancer syndrome (HBOC) | 180 | 154 breast cancers | 217 |
| 8 ovarian cancers | |||
| 3 colorectal cancers | |||
| 3 melanomas | |||
| 2 prostate cancers | |||
| 2 prostate and colorectal cancers | |||
| 2 prostate, colorectal and bladder cancers | |||
| 2 endometrial cancers | |||
| 2 ovarian and colorectal cancers | |||
| 1 pancreatic cancer | |||
| 1 gastric cancer |
| Family | Gene | Mutation | Exon | Family Members (Diagnosis) | Age | Mutational Analysis |
|---|---|---|---|---|---|---|
| 1 | BRCA1 | c.117_118del (p.Cys39_Asp40delinsTer) | 3 | Proband (Ovarian Cancer) | 65 | Mutated |
| Daughter (Unaffected) | 41 | Wild Type | ||||
| 2 | BRCA1 | c.181T > G (p.Cys61Gly) | 5 | Proband (Breast Cancer) | 30 | Mutated |
| Father (Prostate Cancer) | 52 | Mutated | ||||
| Sister (Unaffected) | 31 | Wild Type | ||||
| Sister (Unaffected) | 27 | Wild Type | ||||
| Sister (Unaffected) | 21 | Wild Type | ||||
| 3 | BRCA1 | c.213-11T > G (IVS5-11T > G) | 6 | Proband (Ovarian Cancer) | 55 | Mutated |
| Son (Unaffected) | 28 | Wild Type | ||||
| Daughter (Unaffected) | 24 | Mutated | ||||
| Sister (Unaffected) | 59 | Mutated | ||||
| 4 | BRCA1 | c.547 + 2T > A (IVS8 + 2T > A) | 8 | Proband (Breast Cancer) | 52 | Mutated |
| Mother (Breast Cancer) | 45 † | Mutated | ||||
| Aunt (Prostate Cancer) | 60 † | Mutated | ||||
| Aunt (Breast Cancer) | 48 † | Mutated | ||||
| 5 | BRCA1 | c.798_799delTT (p.Ser267Lysfs) | 11 | Proband (Breast and Ovarian Cancer) | 56 | Mutated |
| Son (Unaffected) | 28 | Mutated | ||||
| Sister (Unaffected) | 65 | Wild Type | ||||
| Brother (Unaffected) | 61 | Mutated | ||||
| 6 | BRCA1 | c.1796_1800del (p.Ser599*) | 11 | Proband (Ovarian Cancer) | 58 | Mutated |
| Sister (Unaffected) | 55 | Wild Type | ||||
| 7 | BRCA1 | c.3351dup (p.Gln1118fs) | 11 | Proband (Breast Cancer) | 50 | Mutated |
| Cousin (Prostate Cancer) | 53 | Mutated | ||||
| 8 | BRCA1 | c.3607 C > T (p.Arg1203Ter) | 11 | Proband (Breast Cancer) | 40 | Mutated |
| Sister (Unaffected) | 39 | Mutated | ||||
| Niece (Unaffected) | 18 | Wild Type | ||||
| 9 | BRCA1 | c.3756_3759delGTCT (p.Ser1253ArgfsTer10) | 11 | Proband (Ovarian Cancer) | 59 | Mutated |
| Son (Unaffected) | 36 | Wild Type | ||||
| Daughter (Unaffected) | 39 | Wild Type | ||||
| 10 | BRCA1 | c.5123C > A (p.Ala1708Glu) | 18 | Proband (Breast and Ovarian Cancer) | 52 | Mutated |
| Sister (Unaffected) | 54 | Mutated | ||||
| Brother (Unaffected) | 51 | Wild Type | ||||
| 11 | BRCA1 | c.5123C > A (p.Ala1708Glu) | 18 | Proband (Ovarian Cancer) | 52 | Mutated |
| Sister (Melanoma) | 55 | Mutated | ||||
| Sister (Unaffected) | 47 | Wild Type | ||||
| Cousin (Unaffected) | 50 | Wild Type | ||||
| 12 | BRCA1 | c.5123C > A (p.Ala1708Glu) | 18 | Proband (Colon Cancer) | 54 | Mutated |
| Sister (Unaffected) | 55 | Mutated | ||||
| Sister (Unaffected) | 59 | Mutated | ||||
| Cousin (Colon Cancer) | 54 | Wild Type | ||||
| 13 | BRCA1 | c.5266dupC (p.Gln1756Profs) | 20 | Proband (Breast and Ovarian Cancer) | 64 | Mutated |
| Daughter (Unaffected) | 36 | Wild Type | ||||
| Son (Unaffected) | 38 | Mutated | ||||
| Brother (Unaffected) | 66 | Mutated | ||||
| Niece (Breast Cancer) | 32 | Mutated | ||||
| Niece (Prostate Cancer) | 41 | Mutated | ||||
| 14 | BRCA1 | c.5266dupC (p.Gln1756Profs) | 20 | Proband (Breast Cancer) | 51 | Mutated |
| Daughter (Unaffected) | 28 | Mutated | ||||
| 15 | BRCA1 | c.5266dupC (p.Gln1756Profs) | 20 | Proband (Ovarian Cancer) | 43 | Mutated |
| Sister (Unaffected) | 27 | Wild Type | ||||
| Brother (Unaffected) | 39 | Mutated | ||||
| Cousin (Breast and Ovarian Cancer) | 46 | Mutated | ||||
| Cousin (Unaffected) | 57 | Wild Type | ||||
| Cousin (Unaffected) | 54 | Wild Type | ||||
| Cousin (Prostate Cancer) | 50 | Mutated | ||||
| 16 | BRCA1 BRCA2 | c.547 + 2T > A (IVS8 + 2T > A) c.2830A > T (p.Lys944Ter) | 8 11 | Proband (Bilateral Breast Cancer) | 32 | Mutated |
| Sister (Unaffected) | 48 | Wild Type | ||||
| Mother (Unaffected) | 68 | Wild Type | ||||
| Father (Unaffected) | 78 | Mutated | ||||
| Aunt (Unaffected) | 74 | Wild Type | ||||
| Cousin (Unaffected) | 50 | Wild Type | ||||
| Cousin (Breast Cancer) | 52 | Mutated | ||||
| Niece (Unaffected) | 25 | Mutated | ||||
| Nephew (Unaffected) | 27 | Mutated | ||||
| Nephew (Unaffected) | 21 | Mutated | ||||
| 17 | BRCA2 | c.67 + 1G > A (IVS2 + 1G > A) | 2 | Proband (Breast Cancer) | 60 | Mutated |
| Son (Unaffected) | 56 | Mutated | ||||
| Daughter (Unaffected) | 54 | Wild Type | ||||
| Daughter (Unaffected) | 51 | Wild Type | ||||
| 18 | BRCA2 | c.1238delT (p.Leu413HisfsX17) | 10 | Proband (Breast Cancer) | 65 | Mutated |
| Son (Unaffected) | 42 | Mutated | ||||
| Son (Unaffected) | 38 | Mutated | ||||
| Son (Unaffected) | 37 | Mutated | ||||
| Brother (Unaffected) | 71 | Mutated | ||||
| Nephew (Unaffected) | 37 | Wild Type | ||||
| 19 | BRCA2 | c.1496_1497delAG (p.Gln499fs) | 10 | Proband (Breast Cancer) | 41 | Mutated |
| Son (Unaffected) | 21 | Mutated | ||||
| Daughter (Unaffected) | 24 | Mutated | ||||
| Sister (Breast Cancer) | 55 | Mutated | ||||
| Nephew (Unaffected) | 24 | Mutated | ||||
| Niece (Unaffected) | 36 | Mutated | ||||
| Niece (Unaffected) | 35 | Mutated | ||||
| Cousin (Prostate Cancer) | 47 | Mutated | ||||
| Cousin (Unaffected) | 41 | Wild Type | ||||
| 20 | BRCA2 | c.4322_4323delAG (p.Glu1441ValfsTer3) | 11 | Proband (Breast Cancer) | 62 | Mutated |
| Father (Prostate Cancer) | 73 | Mutated | ||||
| 21 | BRCA2 | c.5796_5797delTA (p.His1932Glnfs) | 11 | Proband (Breast Cancer) | 72 | Mutated |
| Cousin (Prostate Cancer) | 72 | Mutated | ||||
| Cousin (Breast Cancer) | 68 | Wild Type | ||||
| 22 | BRCA2 | c.6037A > T (p.Lys2013Ter) | 11 | Proband (Ovarian Cancer) | 66 | Mutated |
| Daughter (Unaffected) | 28 | Mutated | ||||
| 23 | BRCA2 | c.6450dup (p.Val2151fs) | 11 | Proband (Breast Cancer) | 54 | Mutated |
| Son (Unaffected) | 24 | Wild Type | ||||
| Daughter (Unaffected) | 21 | Mutated | ||||
| 24 | BRCA2 | c.6468_6469delTC (p.Gln2157Ilefs) | 11 | Proband (Ovarian and Colon Cancer) | 62 | Mutated |
| Daughter (Unaffected) | 40 | Wild Type | ||||
| 25 | BRCA2 | c.6468_6469delTC (p.Gln2157Ilefs) | 11 | Proband (Breast Cancer) | 49 | Mutated |
| Sister (Ovarian Cancer) | 53 | Mutated | ||||
| 26 | BRCA2 | c.6486_6489delACAA (p.Lys2162Asnfs) | 11 | Proband (Breast Cancer) | 50 | Mutated |
| Daughter (Unaffected) | 30 | Mutated | ||||
| Daughter (Unaffected) | 28 | Mutated | ||||
| Sister (Unaffected) | 52 | Wild Type | ||||
| Brother (Unaffected) | 49 | Mutated | ||||
| 27 | BRCA2 | c.7007G > A (p.Arg2336His) | 13 | Proband (Breast Cancer) | 32 | Mutated |
| Mother (Unaffected) | 57 | Wild type | ||||
| Father (Prostate Cancer) | 63 | Mutated | ||||
| Sister (Unaffected) | 27 | Wild type | ||||
| 28 | BRCA2 | c.7857G > A (p.Trp2619Ter) | 17 | Proband (Breast Cancer) | 45 | Mutated |
| Sister (Unaffected) | 48 | Wild Type | ||||
| 29 | BRCA2 | c.8954_8955delGTTinsAA | 23 | Proband (Colon Cancer) | 76 | Mutated |
| Son (Unaffected) | 39 | Wild Type | ||||
| Daughter (Unaffected) | 44 | Mutated | ||||
| Father (Breast Cancer) | 76 | Mutated | ||||
| Sister (Thyroid Cancer) | 70 | Mutated | ||||
| Brother (Prostate Cancer) | 66 | Mutated | ||||
| Niece (Unaffected) | 44 | Mutated | ||||
| Niece (Unaffected) | 23 | Wild type | ||||
| Nephew (Unaffected) | 42 | Wild type | ||||
| Nephew (Unaffected) | 44 | Mutated | ||||
| 30 | BRCA2 BRCA2 | c.631G > A (p.Val221Ile) c.7008-2A > T (IVS13-2A > T) | 7 14 | Proband (Breast Cancer) | 46 | Mutated |
| Daughter (Unaffected) | 23 | Mutated | ||||
| Daughter (Unaffected) | 22 | Mutated | ||||
| Daughter (Unaffected) | 18 | Wild Type | ||||
| Sister (Unaffected) | 46 | Mutated | ||||
| Sister (Unaffected) | 42 | Wild Type | ||||
| Sister (Unaffected) | 36 | Wild Type | ||||
| 31 | PALB2 | c.1919C > A (p.Ser640Ter) | 5 | Proband (Breast Cancer) | 30 | Mutated |
| Father (Prostate Cancer) | 70 | Mutated | ||||
| 32 | MUTYH | c.1437_1439del GGA (p.Glu480del) | 14 | Proband (Breast Cancer) | 85 | Mutated |
| Brother (Prostate Cancer) | 78 | Mutated | ||||
| Daughter (Endometrial Cancer) | 55 | Mutated | ||||
| Son (Unaffected) | 58 | Mutated | ||||
| 33 | RAD51C | c.(705 + 1_706-1)_(837 + 1_838-1)del | 5 | Proband (Gastric Cancer) | 58 | Mutated |
| Cousin (Endometrial Cancer) | 54 | Mutated | ||||
| 34 | TP53 | c.817C > T (p.Arg273Cys) | 8 | Proband (Breast Cancer) | 46 | Mutated |
| Daughter (Unaffected) | 20 | Mutated | ||||
| Son (Unaffected) | 24 | Mutated |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Elia, G.; Caliendo, G.; Tzioni, M.-M.; Albanese, L.; Passariello, L.; Molinari, A.M.; Vietri, M.T. Increased Risk of Hereditary Prostate Cancer in Italian Families with Hereditary Breast and Ovarian Cancer Syndrome Harboring Mutations in BRCA and in Other Susceptibility Genes. Genes 2022, 13, 1692. https://doi.org/10.3390/genes13101692
D’Elia G, Caliendo G, Tzioni M-M, Albanese L, Passariello L, Molinari AM, Vietri MT. Increased Risk of Hereditary Prostate Cancer in Italian Families with Hereditary Breast and Ovarian Cancer Syndrome Harboring Mutations in BRCA and in Other Susceptibility Genes. Genes. 2022; 13(10):1692. https://doi.org/10.3390/genes13101692
Chicago/Turabian StyleD’Elia, Giovanna, Gemma Caliendo, Maria-Myrsini Tzioni, Luisa Albanese, Luana Passariello, Anna Maria Molinari, and Maria Teresa Vietri. 2022. "Increased Risk of Hereditary Prostate Cancer in Italian Families with Hereditary Breast and Ovarian Cancer Syndrome Harboring Mutations in BRCA and in Other Susceptibility Genes" Genes 13, no. 10: 1692. https://doi.org/10.3390/genes13101692
APA StyleD’Elia, G., Caliendo, G., Tzioni, M.-M., Albanese, L., Passariello, L., Molinari, A. M., & Vietri, M. T. (2022). Increased Risk of Hereditary Prostate Cancer in Italian Families with Hereditary Breast and Ovarian Cancer Syndrome Harboring Mutations in BRCA and in Other Susceptibility Genes. Genes, 13(10), 1692. https://doi.org/10.3390/genes13101692