The Dysfunctional Immune System in Common Variable Immunodeficiency Increases the Susceptibility to Gastric Cancer

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Series
2.2. Immunohistochemistry (IHC) and Epstein-Barr Virus (EBV) In Situ Hybridization (ISH)
2.3. Digital Image Analysis
2.4. Evaluation of PD-L1 Expression
2.5. Statistical Analysis
3. Results
3.1. Clinicopathological Features of CVID Patients with Gastric Cancer
3.1.1. Clinical Data
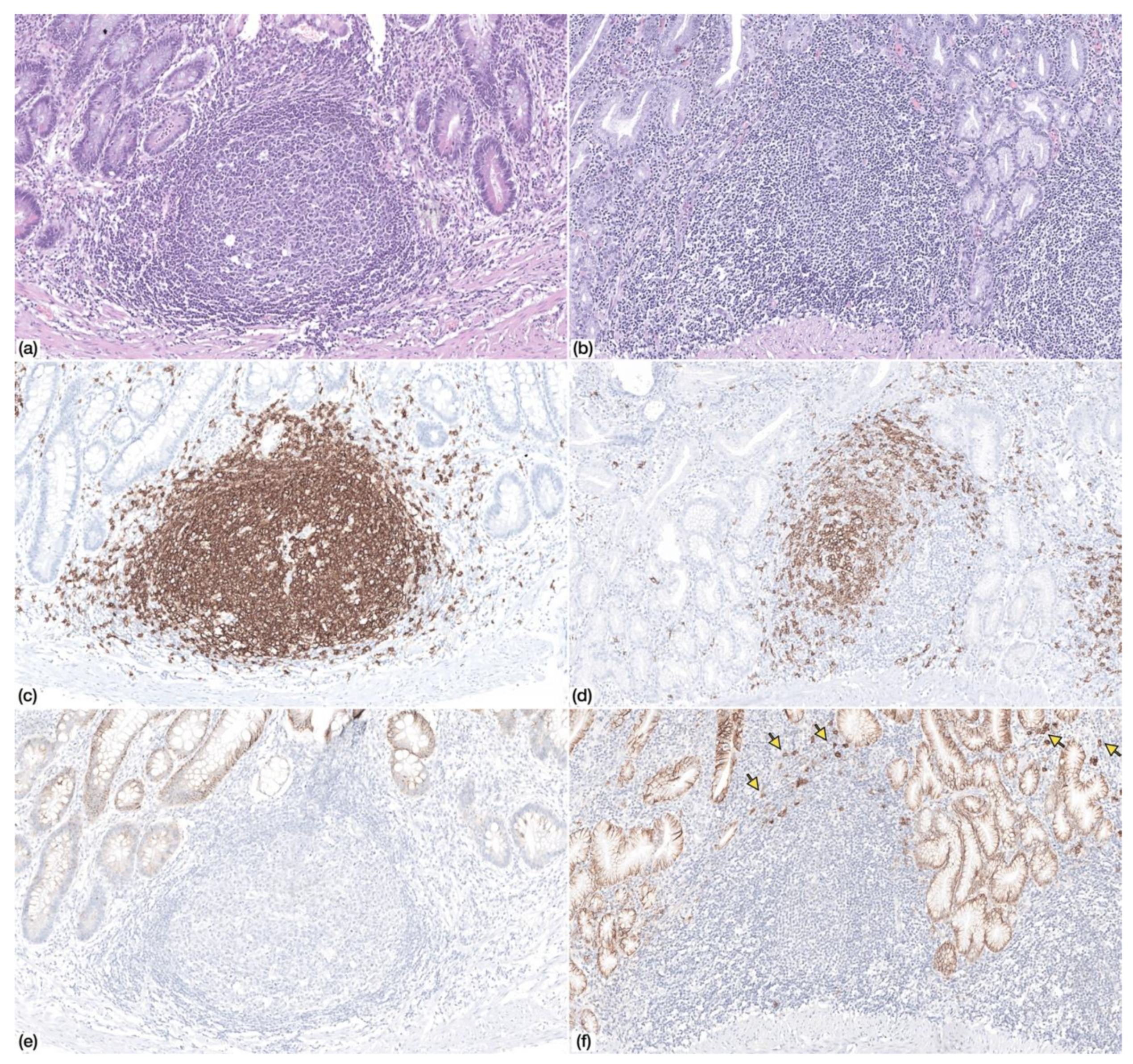
3.1.2. Histopathological Findings in Non-Neoplastic Gastric Mucosa
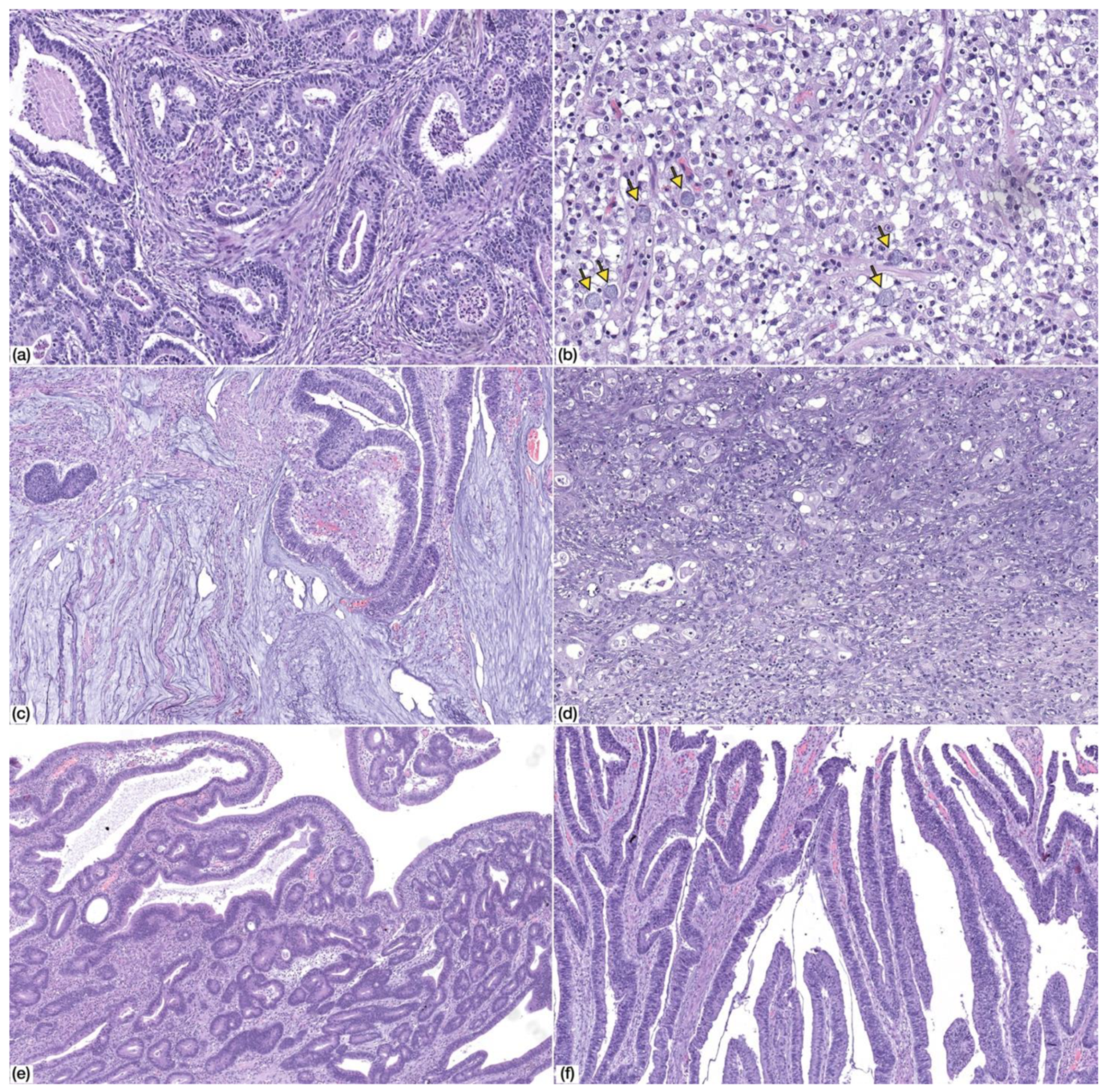
3.1.3. Histopathological Findings in Gastric Cancer
3.1.4. Histopathological Features Compared with Non-CVID Patients
3.2. EBV and CMV Were Not Detected the in Non-Neoplastic Mucosa or Gastric Cancer in CVID Patients
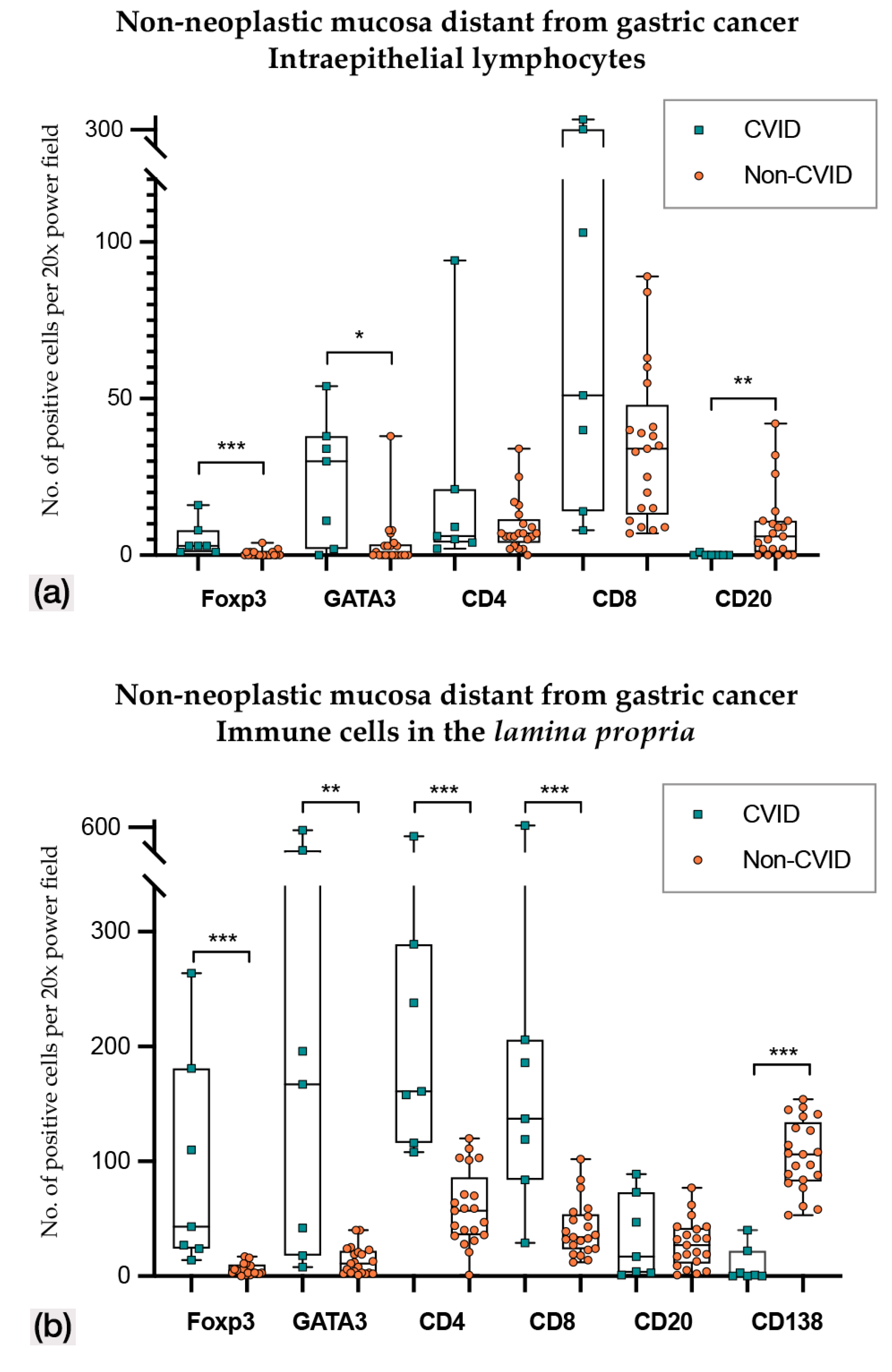
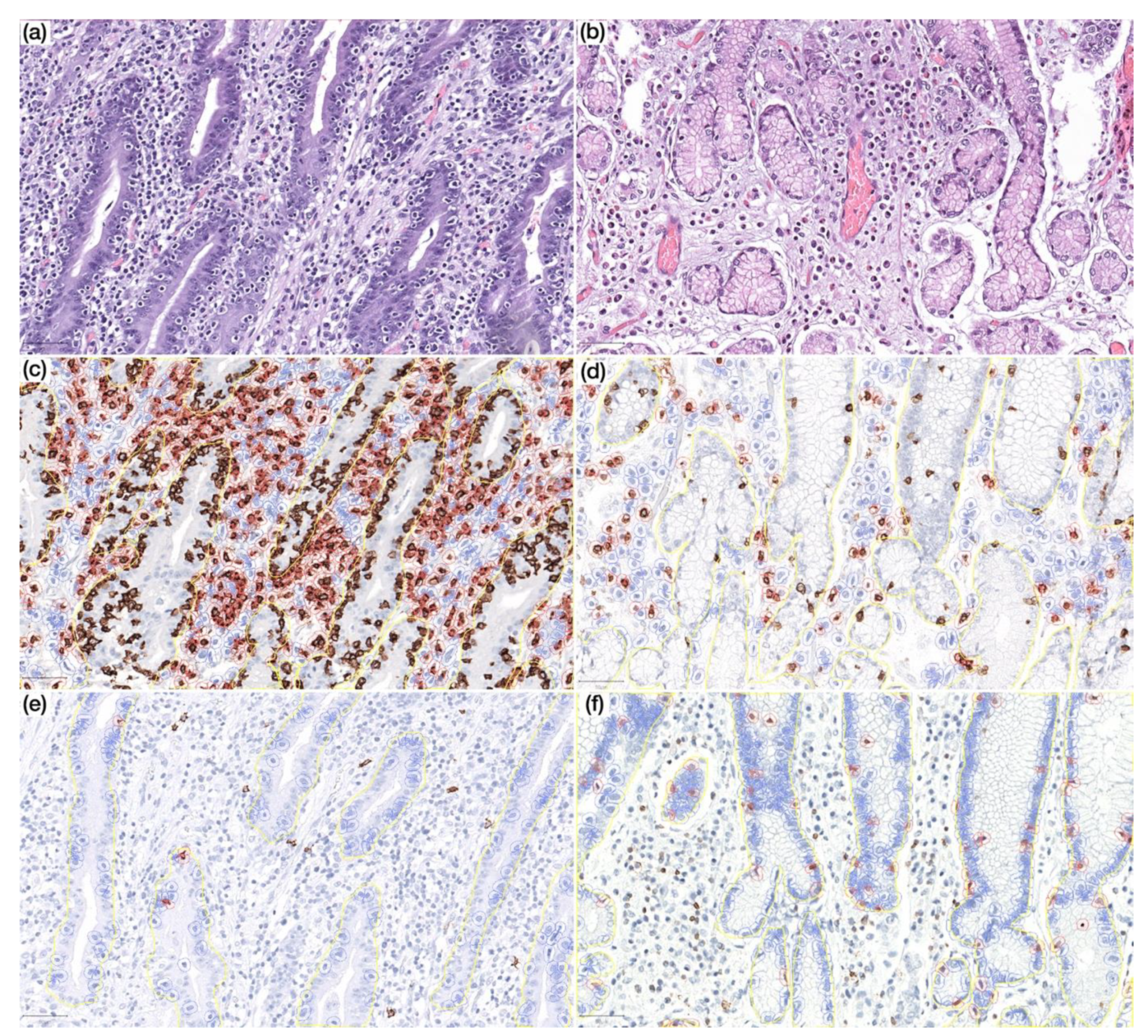
3.3. Immune Microenvironment Changes in CVID Patients Reflect Dysfunctional Immune Microenvironment
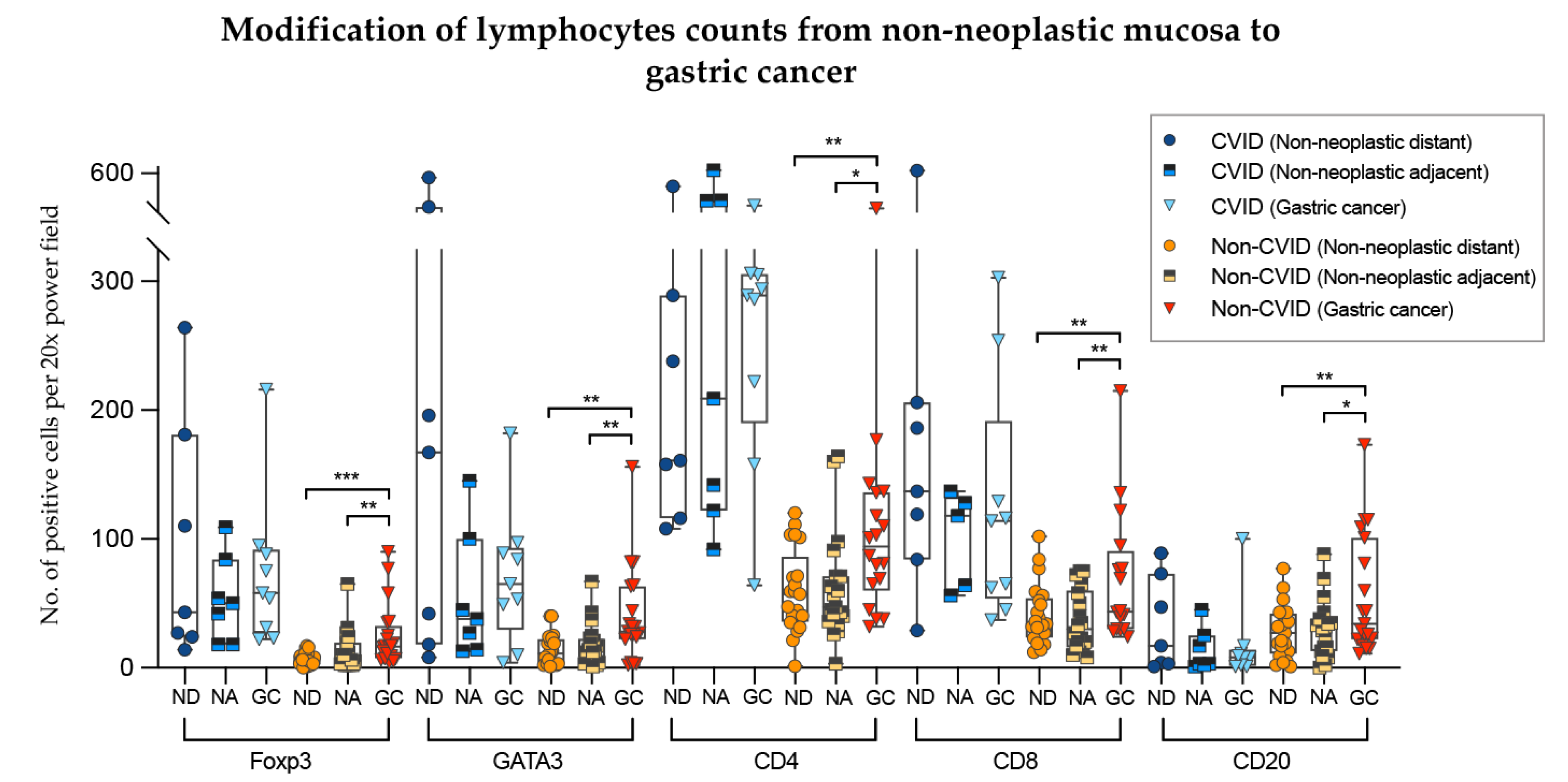
3.3.1. Continuity of Immune Disturbances along Non-Neoplastic Mucosa and Gastric Cancer in CVID
3.3.2. H. pylori Infection May Influence the Immune Microenvironment in CVID Patients.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bousfiha, A.; Jeddane, L.; Picard, C.; Al-Herz, W.; Ailal, F.; Chatila, T.; Cunningham-Rundles, C.; Etzioni, A.; Franco, J.L.; Holland, S.M.; et al. Human Inborn Errors of Immunity: 2019 Update of the IUIS Phenotypical Classification. J. Clin. Immunol. 2020, 40, 66–81. [Google Scholar] [CrossRef] [PubMed]
- Bonilla, F.A.; Barlan, I.; Chapel, H.; Costa-Carvalho, B.T.; Cunningham-Rundles, C.; De La Morena, M.T.; Espinosa-Rosales, F.J.; Hammarström, L.; Nonoyama, S.; Quinti, I.; et al. International Consensus Document (ICON): Common Variable Immunodeficiency Disorders. J. Allergy Clin. Immunol. Pr. 2015, 4, 38–59. [Google Scholar] [CrossRef] [PubMed]
- Blanco, E.; Pérez-Andrés, M.; Méndez, S.A.; Serrano, C.; Criado, I.; Del Pino-Molina, L.; Silva, S.; Madruga, I.; Bakardjieva, M.; Martins, C.; et al. Defects in memory B-cell and plasma cell subsets expressing different immunoglobulin-subclasses in patients with CVID and immunoglobulin subclass deficiencies. J. Allergy Clin. Immunol. 2019, 144, 809–824. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, R.R.; Silva, S.L.; Silva, S.P.; Melo, A.C.; Pereira-Santos, M.C.; Barata, J.; Hammarström, L.; Cascalho, M.; Sousa, A.E. Reduced BAFF-R and Increased TACI Expression in Common Variable Immunodeficiency. J. Clin. Immunol. 2014, 34, 573–583. [Google Scholar] [CrossRef]
- Azizi, G.; Rezaei, N.; Kiaee, F.; Tavakolinia, N.; Yazdani, R.; Mirshafiey, A.; Aghamohammadi, A. T Cell Abnormalities in Common Variable Immunodeficiency. J. Investig. Allergol. Clin. Immunol. 2016, 26, 233–243. [Google Scholar] [CrossRef]
- Viallard, J.F.; Ruiz, C.; Guillet, M.; Pellegrin, J.-L.; Moreau, J.-F. Perturbations of the CD8(+) T-cell repertoire in CVID patients with complications. Results Immunol. 2013, 3, 122–128. [Google Scholar] [CrossRef]
- Viallard, J.-F.; Camou, F.; André, M.; Liferman, F.; Moreau, J.-F.; Pellegrin, J.-L.; Blanco, P. Altered dendritic cell distribution in patients with common variable immunodeficiency. Arthritis Res. Ther. 2005, 7, R1052–R1055. [Google Scholar] [CrossRef]
- Barbosa, R.R.; Silva, S.P.; Silva, S.L.; Tendeiro, R.; Melo, A.C.; Pedro, E.; Barbosa, M.A.D.C.P.; Santos, M.C.; Victorino, R.M.; Sousa, A.E. Monocyte activation is a feature of common variable immunodeficiency irrespective of plasma lipopolysaccharide levels. Clin. Exp. Immunol. 2012, 169, 263–272. [Google Scholar] [CrossRef]
- Von Spee-Mayer, C.; Koemm, V.; Wehr, C.; Goldacker, S.; Kindle, G.; Bulashevska, A.; Proietti, M.; Grimbacher, B.; Ehl, S.; Warnatz, K. Evaluating laboratory criteria for combined immunodeficiency in adult patients diagnosed with common variable immunodeficiency. Clin. Immunol. 2019, 203, 59–62. [Google Scholar] [CrossRef]
- Ho, H.-E.; Cunningham-Rundles, C. Non-infectious Complications of Common Variable Immunodeficiency: Updated Clinical Spectrum, Sequelae, and Insights to Pathogenesis. Front. Immunol. 2020, 11, 149. [Google Scholar] [CrossRef]
- Chapel, H.; Cunningham-Rundles, C. Update in understanding common variable immunodeficiency disorders (CVIDs) and the management of patients with these conditions. Br. J. Haematol. 2009, 145, 709–727. [Google Scholar] [CrossRef] [PubMed]
- Lopes-Da-Silva, S.; Rizzo, L.V. Autoimmunity in Common Variable Immunodeficiency. J. Clin. Immunol. 2008, 28, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Mayor, P.C.; Eng, K.H.; Singel, K.L.; Abrams, S.I.; Odunsi, K.; Moysich, K.B.; Fuleihan, R.; Garabedian, E.; Lugar, P.; Ochs, H.D.; et al. Cancer in primary immunodeficiency diseases: Cancer incidence in the United States Immune Deficiency Network Registry. J. Allergy Clin. Immunol. 2018, 141, 1028–1035. [Google Scholar] [CrossRef]
- Mortaz, E.; Tabarsi, P.; Mansouri, D.; Khosravi, A.; Garssen, J.; Velayati, A.; Adcock, I.M. Cancers Related to Immunodeficiencies: Update and Perspectives. Front. Immunol. 2016, 7, 197. [Google Scholar] [CrossRef] [PubMed]
- Mellemkjær, L.; Hammarström, L.; Andersen, V.; Yuen, J.; Heilmann, C.; Barington, T.; Björkander, J.; Olsen, J.H. Cancer risk among patients with IgA deficiency or common variable immunodeficiency and their relatives: A combined Danish and Swedish study. Clin. Exp. Immunol. 2002, 130, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Kiaee, F.; Azizi, G.; Rafiemanesh, H.; Zainaldain, H.; Rizvi, F.S.; Alizadeh, M.; Jamee, M.; Mohammadi, S.; Habibi, S.; Sharifi, L.; et al. Malignancy in common variable immunodeficiency: A systematic review and meta-analysis. Expert Rev. Clin. Immunol. 2019, 15, 1105–1113. [Google Scholar] [CrossRef]
- Pulvirenti, F.; Pecoraro, A.; Cinetto, F.; Milito, C.; Valente, M.; Santangeli, E.; Crescenzi, L.; Rizzo, F.; Tabolli, S.; Spadaro, G.; et al. Gastric Cancer Is the Leading Cause of Death in Italian Adult Patients With Common Variable Immunodeficiency. Front. Immunol. 2018, 9, 9. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- De Petris, G.; Dhungel, B.M.; Chen, L.; Chang, Y.-H.H. Gastric Adenocarcinoma in Common Variable Immunodeficiency. Int. J. Surg. Pathol. 2014, 22, 600–606. [Google Scholar] [CrossRef]
- Leone, P.; Vacca, A.; Dammacco, F.; Racanelli, V. Common Variable Immunodeficiency and Gastric Malignancies. Int. J. Mol. Sci. 2018, 19, 451. [Google Scholar] [CrossRef]
- Manesh, A.T.; Azizi, G.; Heydari, A.; Kiaee, F.; Shaghaghi, M.; Hossein-Khannazer, N.; Yazdani, R.; Abolhassani, H.; Aghamohammadi, A. Epidemiology and pathophysiology of malignancy in common variable immunodeficiency? Allergol. Et Immunopathol. 2017, 45, 602–615. [Google Scholar] [CrossRef] [PubMed]
- Dhalla, F.; Da Silva, S.P.; Lucas, M.; Travis, S.; Chapel, H. Review of gastric cancer risk factors in patients with common variable immunodeficiency disorders, resulting in a proposal for a surveillance programme. Clin. Exp. Immunol. 2011, 165, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lauren, P. The two histological main types of gastric carcinoma: Diffuse and so-called intestinal-type carcinoma. an attempt at a histo-clinical classification. Acta Pathol. Microbiol. Scand. 1965, 64, 31–49. [Google Scholar] [CrossRef] [PubMed]
- WHO Classification of Tumours. Digestive System Tumours, 5th ed.; WHO Classification of Tumours Editorial Board: Lyon, France, 2019. [Google Scholar]
- Dominguez-Muñoz, J.E. The Obestatin/G protein-coupled receptor 39 system regulates pepsinogen I secretion in human stomach. In AJCC Cancer Staging Manual; Morressier: Berlin, Germany, 2017. [Google Scholar]
- Bankhead, P.; Loughrey, M.B.; Fernández, J.A.; Dombrowski, Y.; McArt, D.G.; Dunne, P.D.; McQuaid, S.; Gray, R.T.; Murray, L.J.; Coleman, H.G.; et al. QuPath: Open source software for digital pathology image analysis. Sci. Rep. 2017, 7, 16878. [Google Scholar] [CrossRef]
- Kulangara, K.; Zhang, N.; Corigliano, E.; Guerrero, L.; Waldroup, S.; Jaiswal, D.; Ms, M.J.; Shah, S.; Hanks, D.; Wang, J.; et al. Clinical Utility of the Combined Positive Score for Programmed Death Ligand-1 Expression and the Approval of Pembrolizumab for Treatment of Gastric Cancer. Arch. Pathol. Lab. Med. 2019, 143, 330–337. [Google Scholar] [CrossRef]
- Barbosa, R.R.; Silva, S.P.; Silva, S.L.; Melo, A.C.; Pedro, E.; Barbosa, M.A.D.C.P.; Santos, M.C.; Victorino, R.M.; Sousa, A.E. Primary B-Cell Deficiencies Reveal a Link between Human IL-17-Producing CD4 T-Cell Homeostasis and B-Cell Differentiation. PLoS ONE 2011, 6, e22848. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, A.; Lauwers, G.Y. Pathology of non-infective gastritis. Histopathol. 2007, 50, 15–29. [Google Scholar] [CrossRef] [PubMed]
- Gullo, I.; Oliveira, P.; Athelogou, M.; Gonçalves, G.; Pinto, M.L.; Carvalho, J.; Valente, A.; Pinheiro, H.; Andrade, S.; Almeida, G.M.; et al. New insights into the inflamed tumor immune microenvironment of gastric cancer with lymphoid stroma: From morphology and digital analysis to gene expression. Gastric Cancer 2018, 22, 77–90. [Google Scholar] [CrossRef]
- Oliveira, C.; Pinheiro, H.; Figueiredo, J.; Seruca, R.; Carneiro, F. Familial gastric cancer: Genetic susceptibility, pathology, and implications for management. Lancet Oncol. 2015, 16, e60–e70. [Google Scholar] [CrossRef]
- Durães, C.; Almeida, G.M.; Seruca, R.; Oliveira, C.; Carneiro, F. Biomarkers for gastric cancer: Prognostic, predictive or targets of therapy? Virchows Arch. 2014, 464, 367–378. [Google Scholar] [CrossRef]
- Paquin-Proulx, D.; Sandberg, J.K. Persistent Immune Activation in CVID and the Role of IVIg in Its Suppression. Front. Immunol. 2014, 5, 5. [Google Scholar] [CrossRef]
- Wan, Y. GATA3: A master of many trades in immune regulation. Trends Immunol. 2014, 35, 233–242. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Wang, C.; Cong, L.; Marjanovic, N.D.; Kowalczyk, M.S.; Zhang, H.; Nyman, J.; Sakuishi, K.; Kurtulus, S.; Gennert, D.; et al. A Distinct Gene Module for Dysfunction Uncoupled from Activation in Tumor-Infiltrating T Cells. Cell 2016, 166, 1500.e9–1511.e9. [Google Scholar] [CrossRef] [PubMed]
- Medsger, T.A.; Ivanco, D.E.; Kardava, L.; Morel, P.A.; Lucas, M.R.; Fuschiotti, P. GATA-3 up-regulation in CD8+ T cells as a biomarker of immune dysfunction in systemic sclerosis, resulting in excessive interleukin-13 production. Arthritis Rheum. 2011, 63, 1738–1747. [Google Scholar] [CrossRef] [PubMed]
- Sowell, R.T.; Kaech, S.M. Probing the Diversity of T Cell Dysfunction in Cancer. Cell 2016, 166, 1362–1364. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.R. Transcriptional regulation of T helper type 2 differentiation. Immunol. 2014, 141, 498–505. [Google Scholar] [CrossRef]
- Sugimoto, M.; Yamaoka, Y.; Furuta, T. Influence of interleukin polymorphisms on development of gastric cancer and peptic ulcer. Worldj. Gastroenterol. 2010, 16, 1188–1200. [Google Scholar] [CrossRef]
- Liu, X.; Cao, K.; Xu, C.; Hu, T.; Zhou, L.; Cao, D.; Xiao, J.; Luo, L.; Guo, Y.; Qi, Y. GATA-3 augmentation down-regulates Connexin43 in Helicobacter pylori associated gastric carcinogenesis. Cancer Biol. Ther. 2015, 16, 987–996. [Google Scholar] [CrossRef]
- Hasan, S.; Hemmige, V.; Forbes, L.R.; Orange, J.S.; Hajjar, J. Gastric Adenocarcinoma in the Setting of X-Linked Agammaglobulinemia (XLA) and HIV. J. Allergy Clin. Immunol. 2015, 135, AB184. [Google Scholar] [CrossRef]
- Lackmann, G.M.; Niehues, T.; Wahn, V. 143 Gastric Adenocarcinoma In a Boy with X-Linked Agammaglobulinemia. Pediatr. Res. 2004, 56, 488. [Google Scholar] [CrossRef]
- Boone, A.T.S.; Martínez, M.G.T.; Herrera, G.L.; Portilla, J.O.D.L.; Padilla, S.E.E.; Rosales, F.J.E.; Reyes, S.O.L. Gastric Adenocarcinoma in the Context of X-linked Agammaglobulinemia. J. Clin. Immunol. 2013, 34, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Hajjar, J.; Hasan, S.; Forbes, L.R.; Hemmige, V.; Orange, J.S. Gastric Adenocarcinoma in a Patient with X-Linked Agammaglobulinemia and HIV: Case Report and Review of the Literature. Front. Pediatr. 2016, 4, 142. [Google Scholar] [CrossRef] [PubMed]
- Bruno, G.; Zaccari, P.; Rocco, G.; Scalese, G.; Panetta, C.; Porowska, B.; Pontone, S.; Severi, C. Proton pump inhibitors and dysbiosis: Current knowledge and aspects to be clarified. Worldj. Gastroenterol. 2019, 25, 2706–2719. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, R.M.; Marques, J.P.; Pinto-Ribeiro, I.; Costa, J.L.; Carneiro, F.; Machado, J.C.; Figueiredo, C. Gastric microbial community profiling reveals a dysbiotic cancer-associated microbiota. Gut 2017, 67, 226–236. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | CVID Patients n = 9 | Non-CVID Patients n = 21 | p Value |
|---|---|---|---|
| Median value (range) | Median value (range) | ||
| Age | 43 (27–62) | 75 (45–84) | 0.000 * |
| N (%) | N (%) | ||
| Gender Female Male | 5/9 (55.6%) 4/9 (44.4%) | 11/21 (52.4%) 10/21 (47.6%) | 1.000 |
| Helicobacter pylori infection Positive Negative | 8/9 (88.9%) 1/9 (11.1%) | 6/14 (42.9%) 8/14 (57.1%) | 0.036 * |
| Histopathological Findings in Non-Neoplastic Mucosa | |||
| Lymphocitic gastritis Present Absent NA | 7/7 (100.0%) 0/7 (0.0%) 2 | 1/21 (4.8%) 20/21 (95.2%) 0 | 0.000 * |
| Lymphoid follicles Present Absent NA | 4/7 (57.1%) 3/7 (42.9%) 2 | 21/21 (100.0%) 0/21 (0.0%) 0 | 0.011 * |
| Neutrophilic activity Present Absent NA | 2/7 (28.6%) 5/7 (71.4%) 2 | 0/21 (0.0%) 21/21 (100%) 0 | 0.056 |
| Intestinal metaplasia Present Absent NA | 7/7 (100.0%) 0/7 (0.0%) 2 | 21/21 (100.0%) 0/21 (0.0%) 0 | NA |
| Histopathological features of gastric cancer | |||
| pT stage (AJCC 8th Ed) [25] pT1a pT1b pT2 NA | 4/7 (57.1%) 2/7 (28.6%) 1/7 (14.3) 2 | 15/21 (71.4%) 6/21 (28.6%) 0/21 0 | 0.21 |
| Laurén classification [23] Intestinal Diffuse Mixed Indeterminate | 6/9 (66.7%) 1/9 (11.1%) 0/9 (0.0%) 2/9 (22.2%) | 13/21 (61.9%) 1/21 (4.8%) 4/21 (19.0%) 3/21 (14.3%) | 0.502 |
| WHO classification (2019) [24] Tubular/papillary Poorly cohesive Mucinous Mixed GCLS | 6/9 (66.7%) 1/9 (11.1%) 2/9 (22.2%) 0/9 (0.0%) 0/9 (0.0%) | 13/21 (61.9%) 1/21 (4.8%) 0/21 (0.0%) 4/21 (19.0%) 3/21 (14.3%) | 0.089 |
| Precursor lesions Present (adenoma) Absent NA | 2/7 (28.6%) 5/7 (71.4%) 2 | 5/21 (23.8%) 16/21 (76.2%) 0 | 1.000 |
| EBV and CMV infection | |||
| EBV infection (EBER-ISH) Positive Negative | 0/9 (0.0%) 9/9 (100.0%) | 1/21 (4.8%) 20/21 (95.2%) | 1.000 |
| CMV infection (IHC) Positive Negative | 0/9 (0.0%) 9/9 (100.0%) | 0/21 (0.0%) 21/21 (100.0%) | NA |
| Immune Cell Biomarker | CVID Patients n = 9 | Non-CVID Patients n = 21 | p Value |
|---|---|---|---|
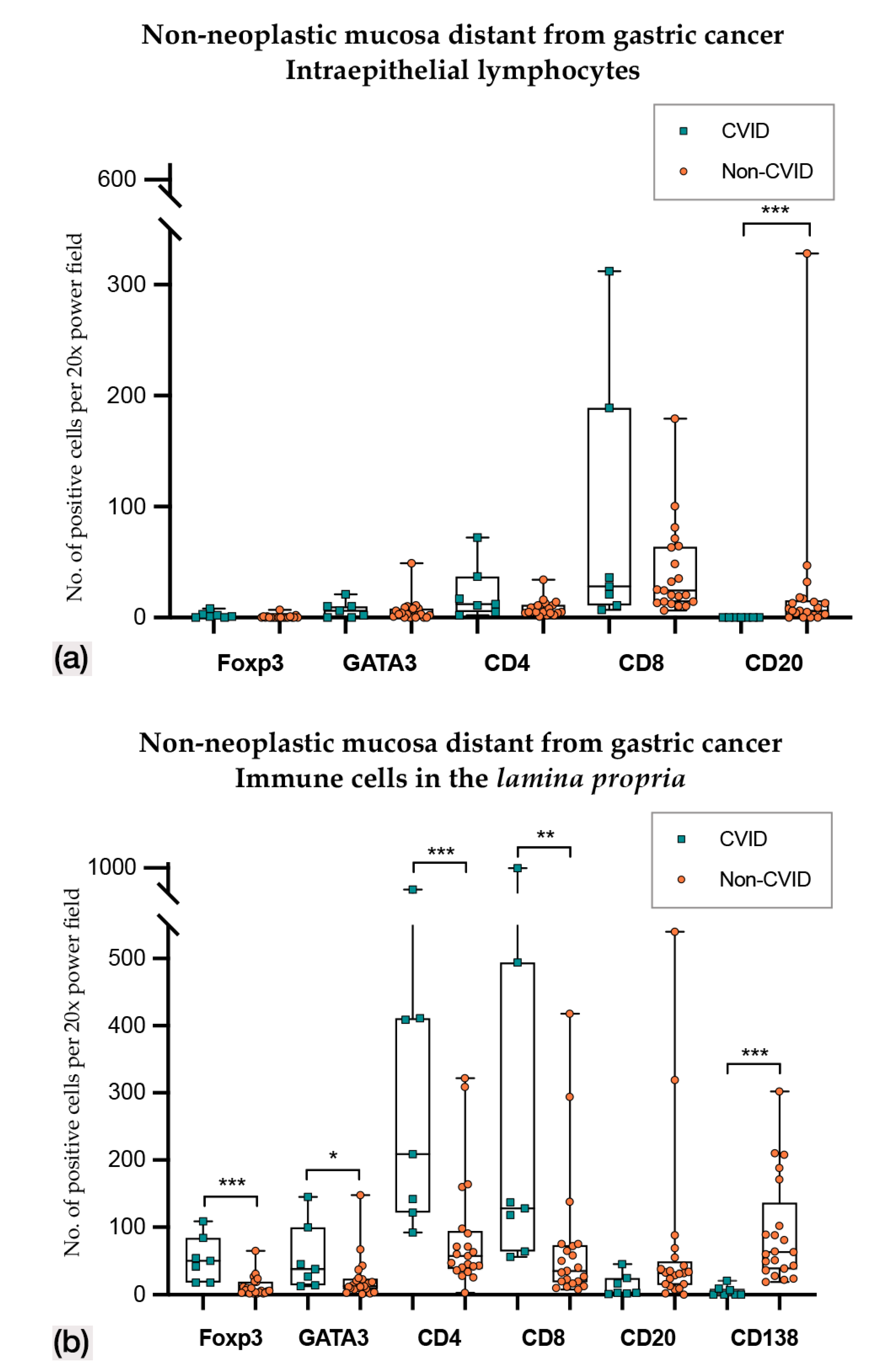
| 1. Non-neoplastic mucosa distant from gastric cancer (intraepithelial) | |||
| n = 7/9 Median value (95% CI) (No. positive cells per 20× PF) | n = 21/21 Median value (95% CI) (No positive cells per 20× PF) | ||
| Foxp3 | 3.0 (1.0–8.0) | 0.0 (0.0–1.0) | 0.000 * |
| GATA3 | 30.0 (2.1–43.9) | 0.0 (0.0–6.9) | 0.014 * |
| CD4 | 6.0 (2.1–21.0) | 7.0 (5.0–10.0) | 0.917 |
| CD8 | 51.0 (11.1–303.0) | 34.0 (15.0–41.0) | 0.172 |
| CD20 | 0.0 (0.0–0.5) | 6.0 (2.0–11.0) | 0.003 * |
| 2. Non-neoplastic mucosa distant from gastric cancer (lamina propria) | |||
| n = 7/9 Median value (95% CI) (No. positive cells per 20× PF) | n = 21/21 Median value (95% CI) (No. positive cells per 20× PF) | ||
| Foxp3 | 43.0 (24.0–262.6) | 5.0 (2.0–8.0) | 0.000 * |
| GATA3 | 167.0 (18.4–570.0) | 11.0 (4.0–23.5) | 0.002 * |
| CD4 | 161.0 (108.3–289.0) | 57.0 (36.1–69.8) | 0.000 * |
| CD8 | 137.0 (84.0–206.0) | 34.0 (24.1–48.9) | 0.001 * |
| CD20 | 17.0 (1.1–73.0) | 27.0 (17.0–33.0) | 0.876 |
| CD138 | 1.0 (0.0–22.0) | 106.0 (84.1–139.6) | 0.000 * |
| 3. Non-neoplastic mucosa adjacent to gastric cancer (intraepithelial) | |||
| n = 7/9 Median value (95% CI) (No. positive cells per 20× PF) | n = 21/21 Median value (95% CI) (No. positive cells per 20× PF) | ||
| Foxp3 | 1.0 (0.0–4.4) | 0.0 (0.0–0.0) | 0.172 |
| GATA3 | 6.0 (0.0–15.3) | 3.0 (1.0–6.0) | 0.604 |
| CD4 | 12.0 (5.0–37.0) | 5.0 (4.0–11.4) | 0.113 |
| CD8 | 28.0 (11.0–248.4) | 24.0 (16.5–48.0) | 0.678 |
| CD20 | 0.0 (0.0–0.0) | 6.0 (3.0–13.0) | 0.001 * |
| 4. Non-neoplastic mucosa adjacent to gastric cancer (lamina propria) | |||
| n = 7/9 Median value (95% CI) (No. positive cells per 20× PF) | n = 21/21 Median value (95% CI) (No. positive cells per 20× PF) | ||
| Foxp3 | 50.0 (18.0–108.2) | 6.0 (4.0–19.8) | 0.001 * |
| GATA3 | 38.0 (14.0–143.5) | 13.0 (11.0–23.0) | 0.023 * |
| CD4 | 209.0 (117.2–615.9) | 57.0 (42.0–90.3) | 0.001 * |
| CD8 | 128.0 (64.0–739.9) | 35.0 (20.1–71.8) | 0.007 * |
| CD20 | 3.0 (2.0–25.0) | 32.0 (20.1–44.8) | 0.055 |
| CD138 | 0.0 (0.0–10.5) | 63.0 (41.2–89.0) | 0.000 * |
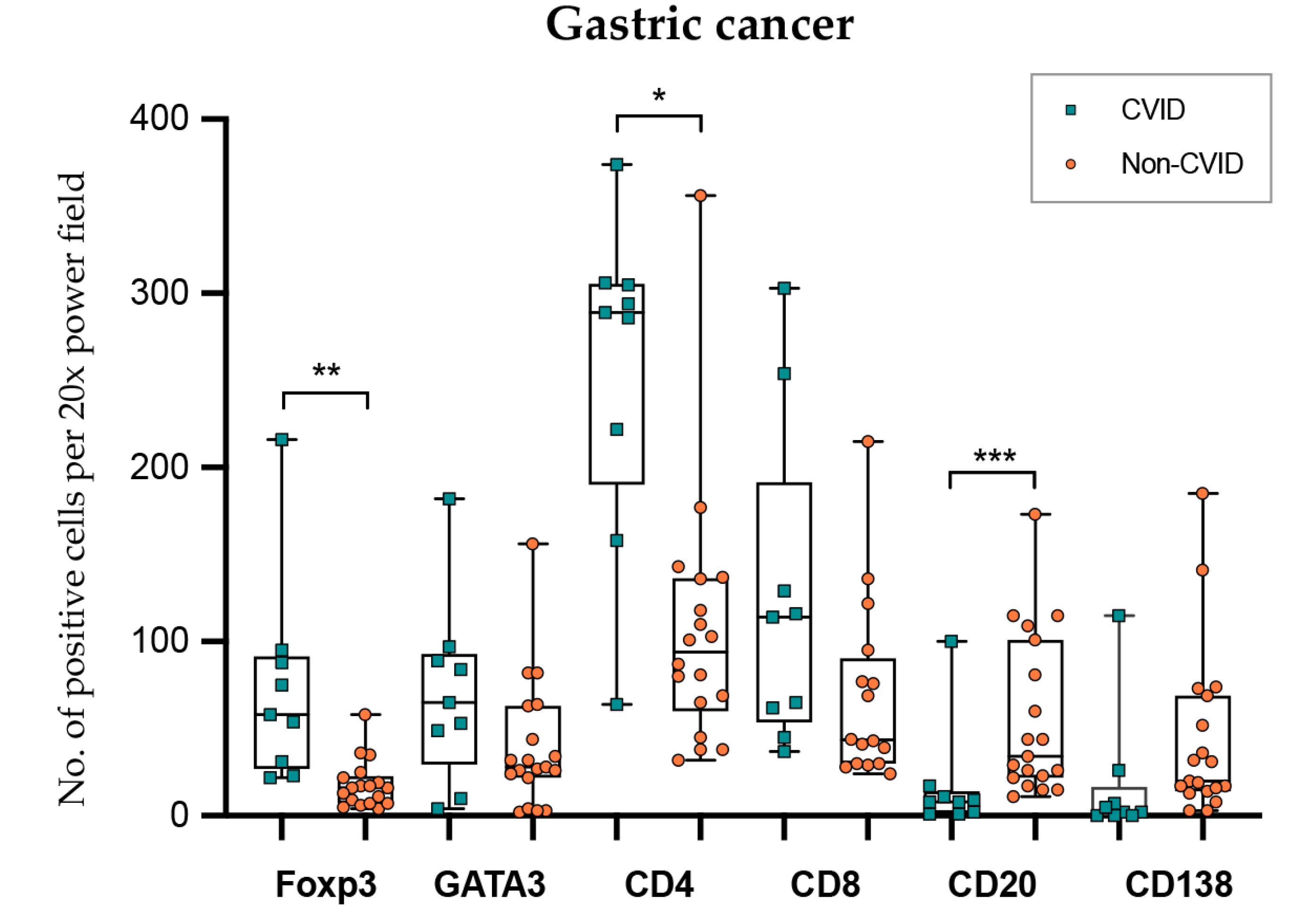
| 5. Gastric cancer (intraepithelial and stromal compartments) | |||
| n = 9/9 Median value (95% CI) (No. positive cells per 20× PF) | n = 21/21 Median value (95% CI) (No. positive cells per 20× PF) | ||
| Foxp3 | 58.0 (23.1–88.0) | 16.5 (6.6–25.0) | 0.002 * |
| GATA3 | 65.0 (11.4–90.4) | 30.0 (15.3–34.0) | 0.178 |
| CD4 | 289.0 (222.0–305.0) | 102.0 (69.3–137.0) | 0.040 * |
| CD8 | 114.0 (45.0–254.0) | 72.5 (39.1–122.0) | 0.689 |
| CD20 | 8.0 (1.0–17.0) | 39.0 23.1–99.6) | 0.000 * |
| CD138 | 2.0 (0.0–25.6) | 31.0 (15.0–68.4) | 0.003 * |
| Feature | CVID Patients | Non-CVID Patients | p Value |
|---|---|---|---|
| 1. Non-neoplastic mucosa distant from gastric cancer (intraepithelial) | |||
| n = 7/9 | n = 21/21 | ||
| Positive intraepithelial lymphocytes Negative | 3/7 (42.9%) 4/7 (57.1%) | 0/21 (0.0%) 21/21 (100.0%) | 0.011 * |
| 2. Non-neoplastic mucosa distant from gastric cancer (lamina propria) | |||
| n = 7/9 | n = 21/21 | ||
| <10% positive immune cells ≥10% positive immune cells | 4/7 (57.1%) 3/7 (42.9%) | 21/21 (100.0%) 0/21 (0.0%) | 0.011 * |
| 3. Non-neoplastic mucosa adjacent to gastric cancer (intraepithelial) | |||
| n = 7/9 | n = 21/21 | ||
| Positive intraepithelial lymphocytes Negative | 3/7 (42.9%) 4/7 (57.1%) | 1/21 (4.8%) 20/21 (95.2%) | 0.038 * |
| 4. Non-neoplastic mucosa adjacent to gastric cancer (lamina propria) | |||
| n = 7/9 | n = 21/21 | ||
| <10% positive immune cells ≥10% positive immune cells | 5/7 (71.4%) 2/7 (28.6 %) | 21/21 (100.0%) 0/21 (0.0%) | 0.056 |
| 5. Gastric cancer (combined positive score) [27] | |||
| n = 9/9 | n = 21/21 | ||
| <1% 1–50% >50% | 2 (22.2%) 7 (77.8%) 0 (0.0%) | 10 (47.6%) 8 (38.1%) 3 (14.3%) | 0.117 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gullo, I.; Costa, C.; Silva, S.L.; Ferreira, C.; Motta, A.; Silva, S.P.; Ferreira, R.D.; Rosmaninho, P.; Faria, E.; Costa, J.T.d.; et al. The Dysfunctional Immune System in Common Variable Immunodeficiency Increases the Susceptibility to Gastric Cancer. Cells 2020, 9, 1498. https://doi.org/10.3390/cells9061498
Gullo I, Costa C, Silva SL, Ferreira C, Motta A, Silva SP, Ferreira RD, Rosmaninho P, Faria E, Costa JTd, et al. The Dysfunctional Immune System in Common Variable Immunodeficiency Increases the Susceptibility to Gastric Cancer. Cells. 2020; 9(6):1498. https://doi.org/10.3390/cells9061498
Chicago/Turabian StyleGullo, Irene, Catarina Costa, Susana L. Silva, Cristina Ferreira, Adriana Motta, Sara P. Silva, Rúben Duarte Ferreira, Pedro Rosmaninho, Emília Faria, José Torres da Costa, and et al. 2020. "The Dysfunctional Immune System in Common Variable Immunodeficiency Increases the Susceptibility to Gastric Cancer" Cells 9, no. 6: 1498. https://doi.org/10.3390/cells9061498
APA StyleGullo, I., Costa, C., Silva, S. L., Ferreira, C., Motta, A., Silva, S. P., Ferreira, R. D., Rosmaninho, P., Faria, E., Costa, J. T. d., Câmara, R., Gonçalves, G., Santos-Antunes, J., Oliveira, C., Machado, J. C., Carneiro, F., & Sousa, A. E. (2020). The Dysfunctional Immune System in Common Variable Immunodeficiency Increases the Susceptibility to Gastric Cancer. Cells, 9(6), 1498. https://doi.org/10.3390/cells9061498