Prognostic Significance of Lymph Node Examination by the OSNA Method in Lung Cancer Patients—Comparison with the Standard Histopathological Procedure

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Examination of Lymph Nodes
2.3. Statistical Analysis
3. Results
3.1. Concordance among H&E, IHC CK19 and OSNA for Groups of LNs
3.2. Concordance among H&E, IHC CK19 and OSNA for Individual Patients
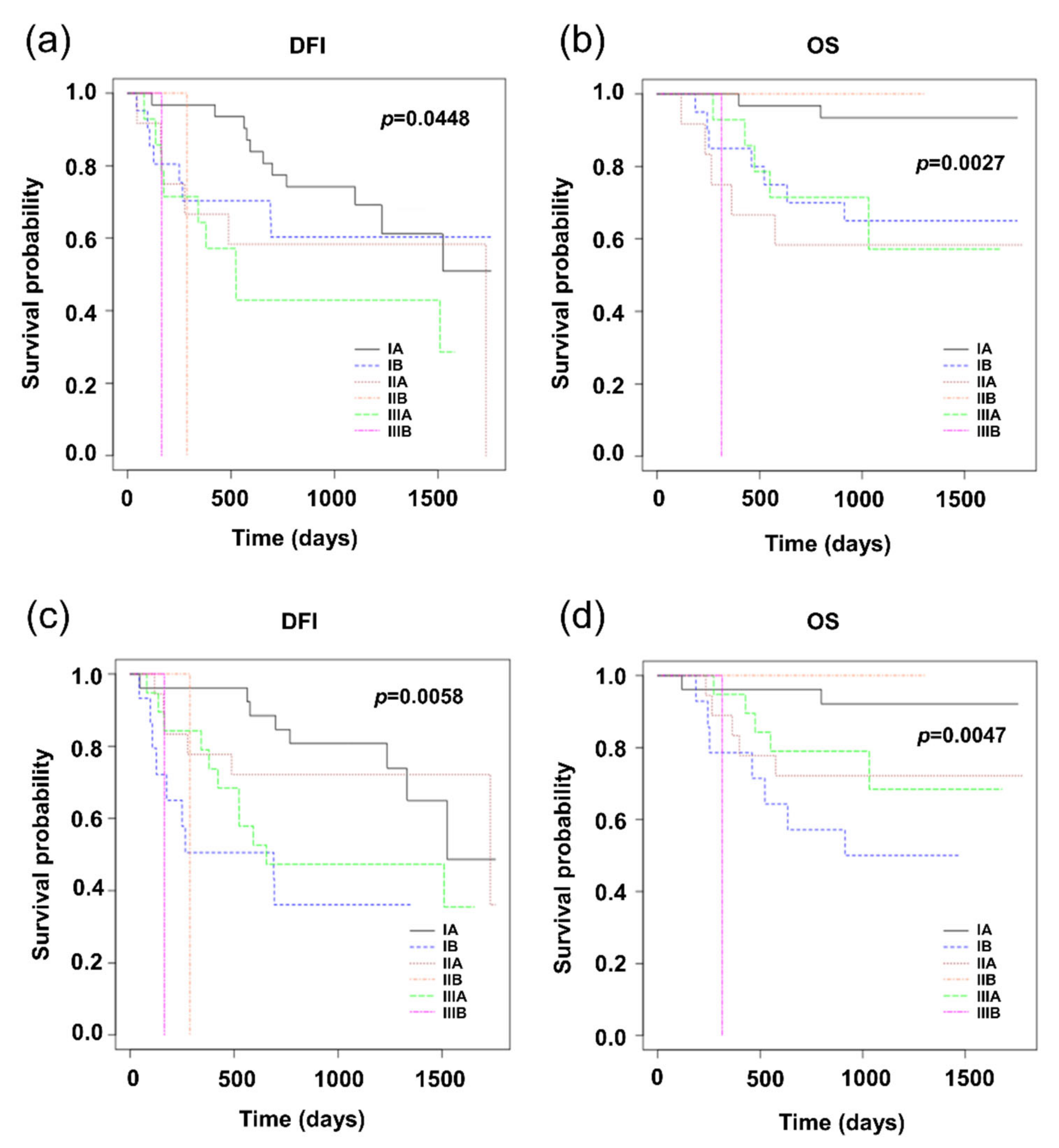
3.3. Comparison of Prognostic Significance of H&E and OSNA
3.4. Proposing a New OSNA Cut-Off Value
4. Discussion
4.1. Concordance of H&E, IHC CK19, and OSNA
4.2. Comparison of H&E and OSNA Based on Relation to Prognosis
4.3. Proposal of the OSNA New Cut-Off Value
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Croner, R.S.; Geppert, C.-I.; Bader, F.G.; Nitsche, U.; Späth, C.; Rosenberg, R.; Zettl, A.; Matias-Guiu, X.; Tarragona, J.; Güller, U.; et al. Molecular staging of lymph node-negative colon carcinomas by one-step nucleic acid amplification (OSNA) results in upstaging of a quarter of patients in a prospective, European, multicentre study. Br. J. Cancer 2014, 110, 2544–2550. [Google Scholar] [CrossRef]
- Osako, T.; Iwase, T.; Kimura, K.; Horii, R.; Akiyama, F. Sentinel node tumour burden quantified based on cytokeratin 19 mRNA copy number predicts non-sentinel node metastases in breast cancer: Molecular whole-node analysis of all removed nodes. Eur. J. Cancer 2013, 49, 1187–1195. [Google Scholar] [CrossRef]
- Hayama, M.; Chida, M.; Karube, Y.; Tamura, M.; Kobayashi, S.; Oyaizu, T.; Honma, K. One-step nucleic acid amplification for detection of lymph node metastasis in lung cancer. Ann. Thorac. Cardiovasc. Surg. 2014, 20, 181–184. [Google Scholar] [CrossRef][Green Version]
- Vogelaar, F.J.; Reimers, M.S.; van der Linden, R.L.A.; van der Linden, J.C.; Smit, V.T.H.B.M.; Lips, D.J.; van de Velde, C.J.H.; Bosscha, K. The Diagnostic Value of One-Step Nucleic acid Amplification (OSNA) for Sentinel Lymph Nodes in Colon Cancer Patients. Ann. Surg. Oncol. 2014, 21, 3924–3930. [Google Scholar] [CrossRef]
- Chaudhry, A.; Williams, S.; Cook, J.; Jenkins, M.; Sohail, M.; Calder, C.; Winters, Z.E.; Rayter, Z. The real-time intra-operative evaluation of sentinel lymph nodes in breast cancer patients using One Step Nucleic Acid Amplification (OSNA) and implications for clinical decision-making. Eur. J. Surg. Oncol. 2014, 40, 150–157. [Google Scholar] [CrossRef]
- Le Frère-Belda, M.-A.; Bats, A.-S.; Gillaizeau, F.; Poulet, B.; Clough, K.B.; Nos, C.; Peoc’h, M.; Seffert, P.; Bouteille, C.; Leroux, A.; et al. Diagnostic performance of one-step nucleic acid amplification for intraoperative sentinel node metastasis detection in breast cancer patients. Int. J. Cancer 2012, 130, 2377–2386. [Google Scholar] [CrossRef]
- Güller, U.; Zettl, A.; Worni, M.; Langer, I.; Cabalzar-Wondberg, D.; Viehl, C.T.; Demartines, N.; Zuber, M. Molecular investigation of lymph nodes in colon cancer patients using one-step nucleic acid amplification (OSNA): A new road to better staging? Cancer 2012, 118, 6039–6045. [Google Scholar] [CrossRef]
- Osako, T.; Iwase, T.; Kimura, K.; Masumura, K.; Horii, R.; Akiyama, F. Incidence and possible pathogenesis of sentinel node micrometastases in ductal carcinoma in situ of the breast detected using molecular whole lymph node assay. Br. J. Cancer 2012, 106, 1675–1681. [Google Scholar] [CrossRef]
- Remoundos, D.D.; Ng, V.V.; Wilson, H.A.; Ahmed, F.; Chia, Y.; Cunnick, G.H. The use of one step nucleic-acid amplification (OSNA) in clinical practice: A single-centre study. Breast 2013, 22, 162–167. [Google Scholar] [CrossRef]
- Yamamoto, N.; Daito, M.; Hiyama, K.; Ding, J.; Nakabayashi, K.; Otomo, Y.; Tsujimoto, M.; Matsuura, N.; Kato, Y. An Optimal mRNA Marker for OSNA (One-step Nucleic Acid Amplification) Based Lymph Node Metastasis Detection in Colorectal Cancer Patients. Jpn. J. Clin. Oncol. 2013, 43, 264–270. [Google Scholar] [CrossRef]
- Kosťun, J.; Pešta, M.; Sláma, J.; Slunéčko, R.; Vlasák, P.; Bouda, J.; Novotný, Z.; Topolčan, O.; Kučera, R.; Kulda, V.; et al. One-step nucleic acid amplification vs ultrastaging in the detection of sentinel lymph node metastasis in endometrial cancer patients. J. Surg. Oncol. 2019, 119, 361–369. [Google Scholar] [CrossRef]
- Gęca, K.; Rawicz-Pruszyński, K.; Mielko, J.; Mlak, R.; Sędłak, K.; Polkowski, W.P. Rapid Detection of Free Cancer Cells in Intraoperative Peritoneal Lavage Using One-Step Nucleic Acid Amplification (OSNA) in Gastric Cancer Patients. Cells 2020, 9, 2168. [Google Scholar] [CrossRef]
- Del Carmen, S.; Gatius, S.; Franch-Arcas, G.; Baena, J.A.; Gonzalez, O.; Zafon, C.; Cuevas, D.; Valls, J.; Pérez, A.; Martinez, M.; et al. Concordance study between one-step nucleic acid amplification and morphologic techniques to detect lymph node metastasis in papillary carcinoma of the thyroid. Hum. Pathol. 2016, 48, 132–141. [Google Scholar] [CrossRef]
- Medas, F.; Coni, P.; Podda, F.; Salaris, C.; Cappellacci, F.; Faa, G.; Calò, P.G. Evaluation of accuracy of one-step nucleic acid amplification (OSNA) in diagnosis of lymph node metastases of papillary thyroid carcinoma. Diagnostic study. Ann. Med. Surg. 2012 2019, 46, 17–22. [Google Scholar] [CrossRef]
- Inoue, M.; Hiyama, K.; Nakabayashi, K.; Morii, E.; Minami, M.; Sawabata, N.; Shintani, Y.; Nakagiri, T.; Susaki, Y.; Maeda, J.; et al. An accurate and rapid detection of lymph node metastasis in non-small cell lung cancer patients based on one-step nucleic acid amplification assay. Lung Cancer 2012, 78, 212–218. [Google Scholar] [CrossRef]
- Masai, K.; Nakagawa, K.; Yoshida, A.; Sakurai, H.; Watanabe, S.; Asamura, H.; Tsuta, K. Cytokeratin 19 expression in primary thoracic tumors and lymph node metastases. Lung Cancer 2014, 86, 318–323. [Google Scholar] [CrossRef]
- Nakagawa, K.; Asamura, H.; Tsuta, K.; Nagai, K.; Yamada, E.; Ishii, G.; Mitsudomi, T.; Ito, A.; Higashiyama, M.; Tomita, Y.; et al. The novel one-step nucleic acid amplification (OSNA) assay for the diagnosis of lymph node metastasis in patients with non-small cell lung cancer (NSCLC): Results of a multicenter prospective study. Lung Cancer 2016, 97, 1–7. [Google Scholar] [CrossRef]
- Vodicka, J.; Mukensnabl, P.; Vejvodova, S.; Spidlen, V.; Kulda, V.; Topolcan, O.; Pesta, M. A more sensitive detection of micrometastases of NSCLC in lymph nodes using the one-step nucleic acid amplification (OSNA) method. J. Surg. Oncol. 2018, 117, 163–170. [Google Scholar] [CrossRef]
- Rusch, V.W.; Asamura, H.; Watanabe, H.; Giroux, D.J.; Rami-Porta, R.; Goldstraw, P. The IASLC Lung Cancer Staging Project: A Proposal for a New International Lymph Node Map in the Forthcoming Seventh Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 2009, 4, 568–577. [Google Scholar] [CrossRef]
- Tamaki, Y. One-step nucleic acid amplification (OSNA): Where do we go with it? Int. J. Clin. Oncol. 2017, 22, 3–10. [Google Scholar] [CrossRef]
- Buglioni, S.; Di Filippo, F.; Terrenato, I.; Casini, B.; Gallo, E.; Marandino, F.; Maini, C.L.; Pasqualoni, R.; Botti, C.; Di Filippo, S.; et al. Quantitative molecular analysis of sentinel lymph node may be predictive of axillary node status in breast cancer classified by molecular subtypes. PLoS ONE 2013, 8, e58823. [Google Scholar] [CrossRef]
- Tateishi, M.; Fukuyama, Y.; Hamatake, M.; Kohdono, S.; Ishida, T.; Sugimachi, K. Skip mediastinal lymph node metastasis in non-small cell lung cancer. J. Surg. Oncol. 1994, 57, 139–142. [Google Scholar] [CrossRef]
- Wang, L.; Zhan, C.; Gu, J.; Xi, J.; Lin, Z.; Xue, L.; Ge, D.; Wang, Q. Role of Skip Mediastinal Lymph Node Metastasis for Patients With Resectable Non-small-cell Lung Cancer: A Propensity Score Matching Analysis. Clin. Lung Cancer 2019, 20, e346–e355. [Google Scholar] [CrossRef]
- Mehrpouya, M.; Pourhashem, Z.; Yardehnavi, N.; Oladnabi, M. Evaluation of cytokeratin 19 as a prognostic tumoral and metastatic marker with focus on improved detection methods. J. Cell. Physiol. 2019, 234, 21425–21435. [Google Scholar] [CrossRef]
- Noorlag, R.; van Es, R.J.J.; de Bree, R.; Willems, S.M. Cytokeratin 19 expression in early oral squamous cell carcinoma and their metastasis: Inadequate biomarker for one-step nucleic acid amplification implementation in sentinel lymph node biopsy procedure: One-step nucleic acid amplification in early oral cancer. Head Neck 2017, 39, 1864–1868. [Google Scholar] [CrossRef]
- Deambrogio, C.; Castellano, I.; Paganotti, A.; Zorini, E.O.; Corsi, F.; Bussone, R.; Franchini, R.; Antona, J.; Miglio, U.; Sapino, A.; et al. A new clinical cut-off of cytokeratin 19 mRNA copy number in sentinel lymph node better identifies patients eligible for axillary lymph node dissection in breast cancer. J. Clin. Pathol. 2014, 67, 702–706. [Google Scholar] [CrossRef]
- Terrenato, I.; D’Alicandro, V.; Casini, B.; Perracchio, L.; Rollo, F.; De Salvo, L.; Di Filippo, S.; Di Filippo, F.; Pescarmona, E.; Maugeri-Saccà, M.; et al. A cut-off of 2150 cytokeratin 19 mRNA copy number in sentinel lymph node may be a powerful predictor of non-sentinel lymph node status in breast cancer patients. PLoS ONE 2017, 12, e0171517. [Google Scholar] [CrossRef]
- Ren, Y.; Zhang, L.; Xie, H.; She, Y.; Su, H.; Xie, D.; Zheng, H.; Zhang, L.; Jiang, G.; Wu, C.; et al. Lymph Node Micrometastasis Prognosticates Survival for Patients with Stage 1 Bronchogenic Adenocarcinoma. Ann. Surg. Oncol. 2018, 25, 3812–3819. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Number of Patients | % |
|---|---|---|
| Gender | ||
| Male | 50 | 62.5 |
| Female | 30 | 37.5 |
| Type of operation | ||
| Pneumonectomy | 6 | 7.5 |
| Bi-lobectomy | 7 | 8.8 |
| Lobectomy | 67 | 83.7 |
| Histology of NSCLC | ||
| Adenocarcinoma | 45 | 56.3 |
| Squamous cell carcinoma | 33 | 41.2 |
| Adenosquamous carcinoma | 2 | 2.5 |
| Pathological T status of NSCLC 1 | ||
| T1a | 20 | 25.0 |
| T1b | 22 | 27.5 |
| T2a | 26 | 32.5 |
| T2b | 6 | 7.5 |
| T3 | 5 | 6.3 |
| T4 | 1 | 1.2 |
| Adjuvant chemotherapy | ||
| No | 52 | 65.0 |
| Yes | 28 | 35.0 |
| Variables | Number of Patients | % |
|---|---|---|
| Gender | ||
| Male | 13 | 65.0 |
| Female | 7 | 35.0 |
| Adjuvant chemotherapy | ||
| no | 12 | 60.0 |
| yes | 8 | 40.0 |
| NSCLC (80 Patients) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Concordance of H&E, IHC CK19 and OSNA assay | 61 patients (76.3%) | |||||||
| Differences between H&E, IHC CK19 and OSNA assay | 19 patients (23.7%) | |||||||
| H&E | IHC CK19 | OSNA | Cases | Commentary | ||||
| TNM | Stage | TNM | Stage | TNM | Stage | |||
| T2aN0 | IB | T2aN1 | IIA | T2aN1 | IIA | 1 | higher stage by both OSNA and IHC CK19 | |
| T1aN0 | IA | T1aN0 | IA | T1aN2 | IIIA | 2 | higher stage by OSNA | |
| T1bN0 | IA | T1bN0 | IA | T1bN1 | IIA | 4 | ||
| T1bN0 | IA | T1bN0 | IA | T1bN2 | IIIA | 1 | ||
| T2aN0 | IB | T2aN0 | IB | T2aN1 | IIA | 2 | ||
| T2aN0 | IB | T2aN0 | IB | T2aN2 | IIIA | 4 | ||
| T1aN1 | IIA | T1aN1 | IIA | T1aN0 | IA | 1 | lower stage by OSNA | |
| T2aN2 | IIIA | T2aN2 | IIIA | T2aN0 | IB | 1 | ||
| T1aN2 | IIIA | T1aN2 | IIIA | T1aN0 | IA | 1 | ||
| T3N2 | IIIA | T3N0 | IIB | T3N0 | IIB | 1 | lower stage by both OSNA and IHC CK19 | |
| T1bN0 | IA | T1bN2 | IIIA | T1bN0 | IA | 1 | higher stage by IHC CK19 | |
| Lung metastases of colorectal carcinoma (20 patients) | ||||||||
| Concordance of H&E, IHC CK19 and OSNA assay | 17 patients (85.0%) | |||||||
| Differences between H&E, IHC CK19 and OSNA assay | 3 patients (15.0%) | |||||||
| H&E | IHC CK19 | OSNA | Cases | Commentary | ||||
| N-stage | N-stage | N-stage | ||||||
| N0 | N0 | N1 | 2 | higher N-stage by OSNA | ||||
| N0 | N0 | N2 | 1 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vodicka, J.; Pesta, M.; Kulda, V.; Houfkova, K.; Vankova, B.; Sebek, J.; Skala, M.; Fichtl, J.; Prochazkova, K.; Topolcan, O. Prognostic Significance of Lymph Node Examination by the OSNA Method in Lung Cancer Patients—Comparison with the Standard Histopathological Procedure. Cells 2020, 9, 2611. https://doi.org/10.3390/cells9122611
Vodicka J, Pesta M, Kulda V, Houfkova K, Vankova B, Sebek J, Skala M, Fichtl J, Prochazkova K, Topolcan O. Prognostic Significance of Lymph Node Examination by the OSNA Method in Lung Cancer Patients—Comparison with the Standard Histopathological Procedure. Cells. 2020; 9(12):2611. https://doi.org/10.3390/cells9122611
Chicago/Turabian StyleVodicka, Josef, Martin Pesta, Vlastimil Kulda, Katerina Houfkova, Bohuslava Vankova, Jakub Sebek, Martin Skala, Jakub Fichtl, Kristyna Prochazkova, and Ondrej Topolcan. 2020. "Prognostic Significance of Lymph Node Examination by the OSNA Method in Lung Cancer Patients—Comparison with the Standard Histopathological Procedure" Cells 9, no. 12: 2611. https://doi.org/10.3390/cells9122611
APA StyleVodicka, J., Pesta, M., Kulda, V., Houfkova, K., Vankova, B., Sebek, J., Skala, M., Fichtl, J., Prochazkova, K., & Topolcan, O. (2020). Prognostic Significance of Lymph Node Examination by the OSNA Method in Lung Cancer Patients—Comparison with the Standard Histopathological Procedure. Cells, 9(12), 2611. https://doi.org/10.3390/cells9122611