Over-Expression of βII-Tubulin and Especially Its Localization in Cell Nuclei Correlates with Poorer Outcomes in Colorectal Cancer

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Source of Patients
2.2. Tissue Samples
2.3. Immunohistochemistry
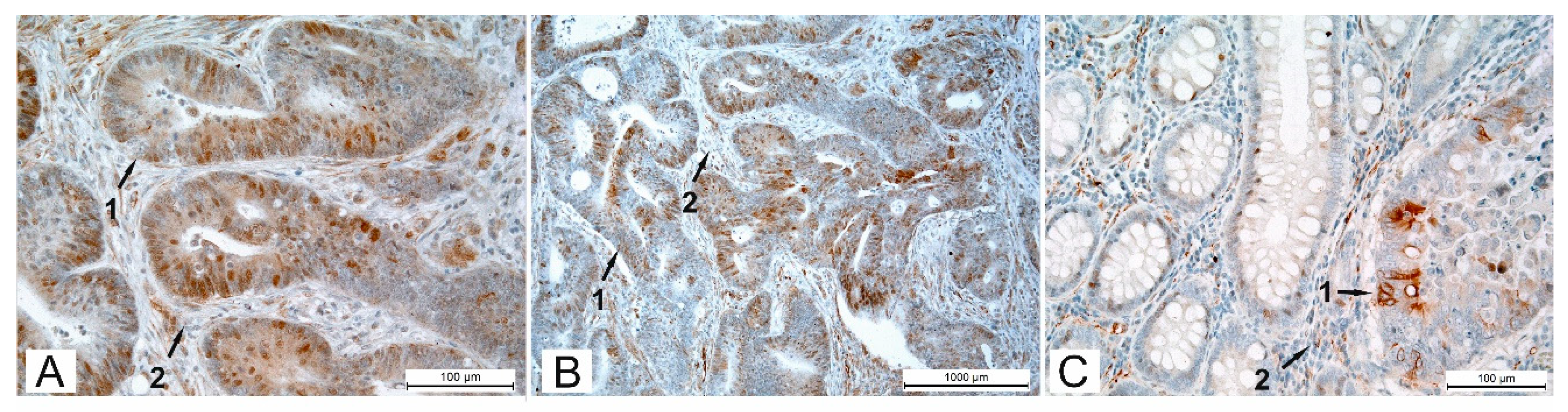
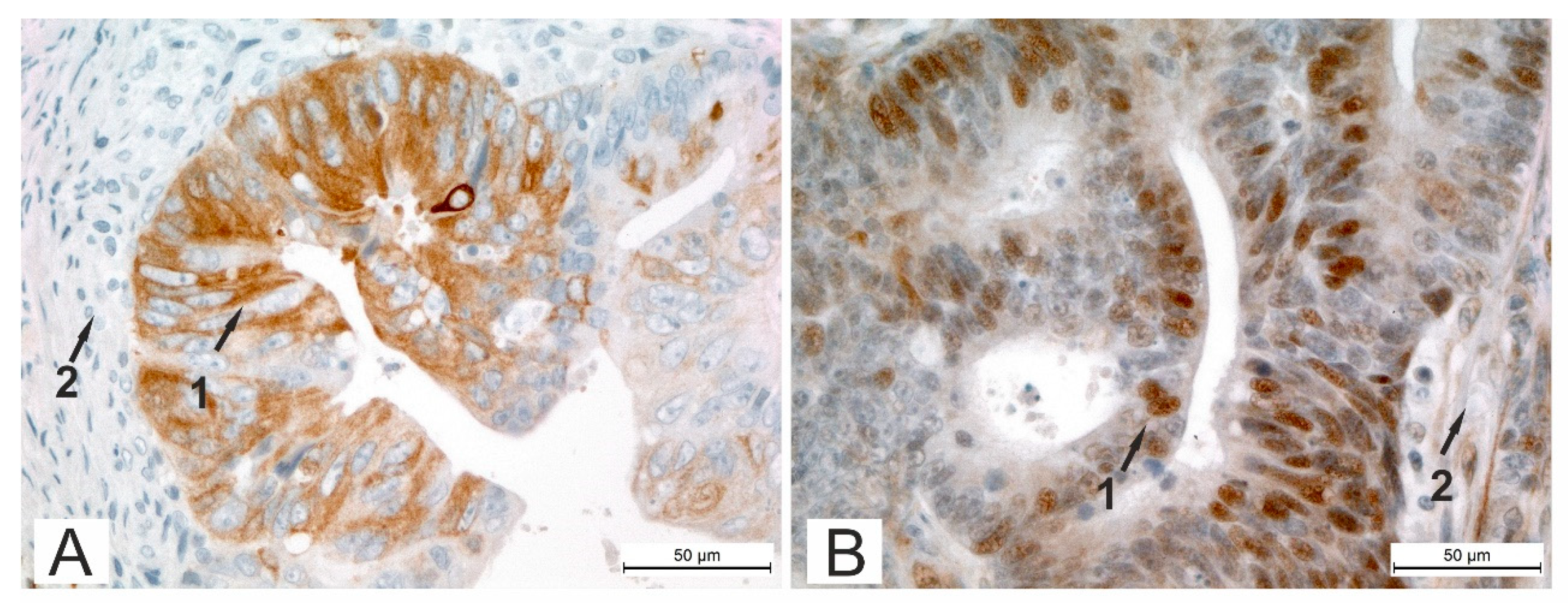
2.4. Immunohistochemistry Evaluation
2.5. Statistical Analysis
2.6. Data Sharing
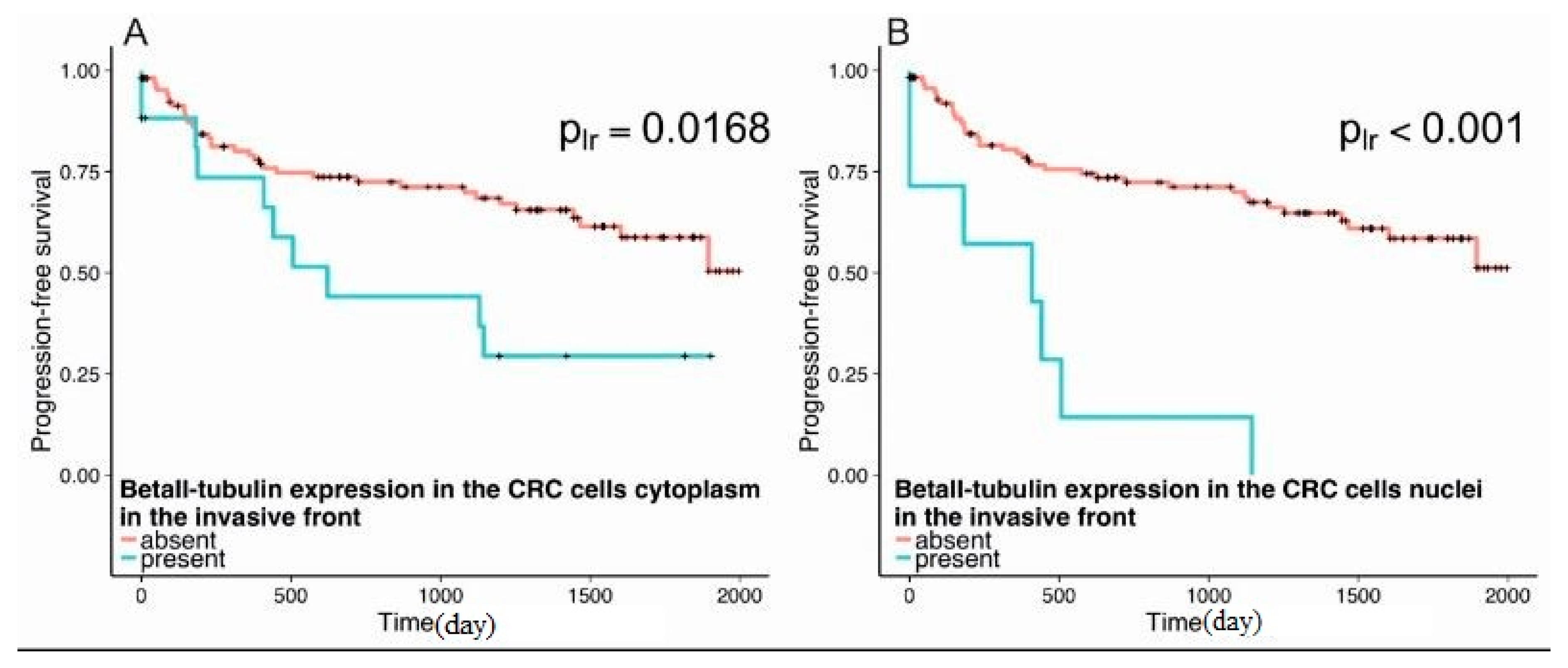
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- U.S. Cancer Statistics Working Group. United States Cancer Statistics, 1999–2014; Incidence and Mortality Web-based Report; Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute: Atlanta, GA, USA, 2017. Available online: www.cdc.gov/uscs (accessed on 1 January 2019).
- Stewart, B.W.; Wild, C.P. World Cancer Report 2014; International Agency for Research on Cancer: Lyon, France, 2014; ISBN 978-92-832-0429-9. [Google Scholar]
- Ferlay, J.; Soerjomataram, I.; Ervik, M.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11, 2013; International Agency for Research on Cancer: Lyon, France, 2013; Available online: http://globocan.iarc.fr (accessed on 6 February 2015).
- Dustin, P. Microtubules, 2nd ed.; Springer: Berlin, Germany, 1984; ISBN 3-540-13283-X. [Google Scholar]
- Kreis, T.; Vale, R. Guidebook to the Cytoskeletal and Motor Proteins, 2nd ed.; Oxford University Press: Oxford, UK, 1999; ISBN-13 978-0198599562. [Google Scholar]
- Ludueña, R.F.; Shooter, E.M.; Wilson, L. The structure of the tubulin dimer. J. Biol. Chem. 1977, 252, 7006–7014. [Google Scholar] [PubMed]
- Ludueña, R.F.; Banerjee, A. The isotypes of tubulin: Distribution and functional significance. In Cancer Drug Discovery and Development: The Role of Microtubules in Cell Biology, Neurobiology, and Oncology; Fojo, T., Ed.; Humana Press: Totowa, NJ, USA, 2008; pp. 123–175. ISBN 978-1-59745-336-3. [Google Scholar]
- Ludueña, R.F.; Yeh, I.T.; Joe, P.; Guo, J. Functional significance of vertebrate β-tubulin isotypes. Meditsina 2011, 72, 50–57. (In Russian) [Google Scholar]
- Walss, C.; Kreisberg, J.I.; Luduena, R.F. Presence of the βII-isotype of tubulin in the nuclei of cultured rat kidney mesangial cells. Cell Motil. Cytoskeleton 1999, 42, 274–284. [Google Scholar] [CrossRef]
- Walss-Bass, C.; Prasad, V.; Kreisberg, J.I.; Ludueña, R.F. Interaction of the βIV-tubulin isotype with actin stress fibers in cultured rat kidney mesangial cells. Cell Motil. Cytoskeleton 2001, 49, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Kourmouli, N.; Dialynas, G.; Petraki, C.; Pyrpasopoulou, A.; Singh, P.M.; Georgatos, S.D.; Theodoropoulos, P.A. Binding of heterochromatin protein 1 to the nuclear envelope is regulated by a soluble form of tubulin. J. Biol. Chem. 2001, 276, 13007–13014. [Google Scholar] [CrossRef] [PubMed]
- Carré, M.; André, N.; Carles, G.; Borghi, H.; Brichese, L.; Briand, C.; Braguer, D. Tubulin is an inherent component of mitochondrial membranes that interacts with the voltage-dependent anion channel. J. Biol. Chem. 2002, 277, 33664–33669. [Google Scholar] [CrossRef] [PubMed]
- Yanagida, M.; Hayano, T.; Yamauchi, Y.; Shinkawa, T.; Natsume, T.; Isobe, T.; Takahashi, N. Human fibrillarin forms a sub-complex with splicing factor 2-associated p32, protein arginine methyltransferases, and tubulins α3 and β1 that is independent of its association with preribosomal ribonucleoprotein complexes. J. Biol. Chem. 2004, 279, 1607–1614. [Google Scholar] [CrossRef]
- McIntosh, J.R.; Grishchuk, E.; Morphew, M.K.; Efremov, A.K.; Zhudenkov, K.; Volkov, V.A.; Cheeseman, I.M.; Desai, A.; Mastronarde, D.N.; Ataullakhanov, A.I. Fibrils connect microtubule tips with kinetochores: A mechanism to couple tubulin dynamics to chromosome motion. Cell 2008, 135, 322–333. [Google Scholar] [CrossRef]
- Banerjee, A.; Roach, M.C.; Wall, K.A.; Lopata, M.A.; Cleveland, D.W.; Ludueña, R.F. A monoclonal antibody against the type II isotype of β-tubulin. Preparation of isotypically altered tubulin. J. Biol. Chem. 1988, 263, 3029–3034. [Google Scholar]
- Walss-Bass, C.; Xu, K.; David, S.; Fellous, A.; Ludueña, R.F. Occurrence of nuclear βII-tubulin in cultured cells. Cell Tissue Res. 2002, 308, 215–223. [Google Scholar] [CrossRef]
- Xu, K.; Ludueña, R.F. Characterization of nuclear βII-tubulin in tumor cells: A possible novel target for taxol. Cell Motil. Cytoskeleton 2002, 53, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Yeh, I.-T.; Ludueña, R.F. The βII isotype of tubulin is present in the cell nuclei of a variety of cancers. Cell Motil. Cytoskeleton 2004, 57, 96–106. [Google Scholar] [CrossRef] [PubMed]
- Derry, W.B.; Wilson, L.; Khan, I.A.; Ludueña, R.F.; Jordan, M.A. Taxol differentially modulates the dynamics of microtubules assembled from unfractionated and purified β-tubulin isotypes. Biochemistry 1997, 36, 3554–3562. [Google Scholar] [CrossRef] [PubMed]
- Khan, I.A.; Ludueña, R.F. Different effects of vinblastine on the polymerization of isotypically purified tubulins from bovine brain. Investig. New Drugs 2003, 21, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Roach, M.C.; Boucher, V.L.; Walss, C.; Ravdin, P.M.; Ludueña, R.F. Preparation of a monoclonal antibody specific for the class I isotype of β-tubulin: The β isotypes of tubulin differ in their cellular distributions within human tissues. Cell Motil. Cytoskeleton 1998, 39, 273–285. [Google Scholar] [CrossRef]
- Oda, E.; Nakamura, Y.; Yamamoto, M.; Kojiro, M. Immunohistochemical distribution of tubulin beta II in human normal and neoplastic tissues. Kurume Med. J. 2005, 52, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Dhamodharan, R.; Jordan, M.A.; Thrower, D.; Wilson, L.; Wadsworth, P. Vinblastine suppresses dynamics of individual microtubules in living interphase cells. Mol. Biol. Cell 1995, 6, 1215–1229. [Google Scholar] [CrossRef]
- Yvon, A.C.; Wadsworth, P.; Jordan, M.A. Taxol suppresses dynamics of individual microtubules in living human tumor cells. Mol. Biol. Cell 1999, 10, 947–959. [Google Scholar] [CrossRef]
- Rathinasamy, K.; Jindal, B.; Asthana, J.; Singh, P.; Balaji, P.V.; Panda, D. Griseofulvin stabilizes microtubule dynamics, activates p53 and inhibits the proliferation of MCF-7 cells synergistically with vinblastine. BMC Cancer 2010, 10, 213. [Google Scholar] [CrossRef]
- Edge, S.B.; Byrd, D.R.; Compton, C.C.; Fritz, A.G.; Greene, F.L.; Trotti, A. AJCC Cancer Staging Manual, 7th ed.; Springer: New York, NY, USA, 2009; ISBN-13 978-1845974749. [Google Scholar]
- Portyanko, A.; Kovalev, P.; Gorgun, J.; Cherstvoy, E. Beta(III)-tubulin at the invasive margin of colorectal cancer: Possible link to invasion. Virchows Archiv. 2009, 454, 541–548. [Google Scholar] [CrossRef]
- Compton, C.C.; Fielding, L.P.; Burgart, L.J.; Conley, B.; Cooper, H.S.; Hamilton, S.R.; Hammond, M.E.H.; Henson, D.E.; Hutter, R.V.P.; Nagle, R.B.; et al. Prognostic factors in colorectal cancer: College of American Pathologists Consensus Statement 1999. Arch. Pathol. Lab. Med. 2000, 124, 979–994. [Google Scholar] [CrossRef] [PubMed]
- De Divitiis, C.; Nasti, G.; Montano, M.; Fisichella, R.; Iaffaioli, R.V.; Berretta, M. Prognostic and predictive response factors in colorectal cancer patients: Between hope and reality. World J. Gastroenterol. 2014, 20, 15049–15059. [Google Scholar] [CrossRef] [PubMed]
- Hiser, L.; Aggarwal, A.; Young, R.; Frankfurter, A.; Spano, A.; Correia, J.J.; Lobert, S. Comparison of β-tubulin mRNA and protein levels in 12 human cancer cell lines. Cell Motil. Cytoskeleton 2006, 63, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Cerami, E.; Gao, J.; Dogrusoz, U.; Gross, B.E.; Sumer, S.U.; Aksoy, B.A.; Jacobsen, A.; Byrne, C.J.; Heuer, M.L.; Larsson, E.; et al. The cBio Cancer Genomics Portal: An open platform for exploring multidimensional cancer genomics data. Cancer Discov. 2012, 2, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Aksov, B.A.; Dogrusog, U.; Dresdner, G.; Gross, B.; Sumer, S.O.; Sun, Y.; Jacobsen, A.; Sinha, R.; Larsson, E.; et al. Integrative analysis of complex cancer genomics and clinical profiles using the cBioPortal. Sci. Signal. 2013, 2, 6. [Google Scholar] [CrossRef] [PubMed]
- LaBonte, M.J.; Wilson, P.M.; Fazzone, W.; Groshen, S.; Lenz, H.J.; Ladner, R.D. DNA microarray profiling of genes differentially regulated by the histone deacetylase inhibitors vorinostat and LBH589 in colon cancer cell lines. BMC Med. Genom. 2009, 2, 67. [Google Scholar] [CrossRef] [PubMed]
- Dessein, A.F.; Stechly, L.; Jonckheere, N.; Dumont, P.; Monté, D.; Leteurtre, E.; Truant, S.; Pruvot, F.R.; Figeac, M.; Hebbar, M.; et al. Autocrine induction of invasive and metastatic phenotypes by the MIF-CRCR4 axis in drug-resistant human colon cancer cells. Cancer Res. 2010, 70, 4644–4654. [Google Scholar] [CrossRef]
- Cirillo, L.; Gotta, M.; Meraldi, P. The elephant in the room: The role of microtubules in cancer. In Cell Division Machinery and Disease; Gotta, M., Meraldi, P., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 93–124. ISBN 978-3-319-57125-6. [Google Scholar]
- Guo, J.; Walss-Bass, C.; Ludueña, R.F. The beta isotypes of tubulin in neuronal differentiation. Cytoskeleton 2010, 67, 431–441. [Google Scholar] [CrossRef]
- Guo, J.; Qiang, M.; Ludueña, R.F. The distribution of β-tubulin isotypes in cultured neurons from embryonic, newborn, and adult mouse brains. Brain Res. 2011, 1420, 8–18. [Google Scholar] [CrossRef]
- Georgatos, S.D.; Theodoropoulos, P.A. Rules to remodel by: What drives nuclear envelope disassembly and reassembly during mitosis? Crit. Rev. Eukaryot. Gene Expr. 1999, 9, 373–381. [Google Scholar] [CrossRef]
- Rashid, A.; Pizer, E.S.; Moga, M.; Milgraum, L.Z.; Zahurak, M.; Pasternack, G.R.; Kuhajda, F.P.; Hamilton, S.R. Elevated expression of fatty acid synthase and fatty acid synthetic activity in colorectal neoplasia. Am. J. Pathol. 1997, 150, 201–208. [Google Scholar] [PubMed]
- Rowinsky, E.K.; Donehower, R.C. Drug therapy: Paclitaxel (Taxol). N. Engl. J. Med. 1995, 332, 1004–1014. [Google Scholar] [CrossRef] [PubMed]
- Walss-Bass, C.; Kreisberg, J.I.; Ludueña, R.F. Effect of the anti-tumor drug vinblastine on nuclear βII-tubulin in cultured rat kidney mesangial cells. Investig. New Drugs 2003, 21, 15–26. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Intensity of Staining | βII-Tubulin Expression | |||||
|---|---|---|---|---|---|---|
| Tumor Center | Invasive Front | Normal Mucosa | ||||
| N | % | N | % | N | % | |
| Negative | 95 | 76.0 | 106 | 84.8 | 34 | 58.6 |
| Positive | 30 | 24.0 | 19 | 15.2 | 24 | 41.4 |
| All | 125 | 100 | 125 | 100 | 58 | 100 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruksha, K.; Mezheyeuski, A.; Nerovnya, A.; Bich, T.; Tur, G.; Gorgun, J.; Luduena, R.; Portyanko, A. Over-Expression of βII-Tubulin and Especially Its Localization in Cell Nuclei Correlates with Poorer Outcomes in Colorectal Cancer. Cells 2019, 8, 25. https://doi.org/10.3390/cells8010025
Ruksha K, Mezheyeuski A, Nerovnya A, Bich T, Tur G, Gorgun J, Luduena R, Portyanko A. Over-Expression of βII-Tubulin and Especially Its Localization in Cell Nuclei Correlates with Poorer Outcomes in Colorectal Cancer. Cells. 2019; 8(1):25. https://doi.org/10.3390/cells8010025
Chicago/Turabian StyleRuksha, Kseniya, Artur Mezheyeuski, Alexander Nerovnya, Tatyana Bich, Gennady Tur, Julia Gorgun, Richard Luduena, and Anna Portyanko. 2019. "Over-Expression of βII-Tubulin and Especially Its Localization in Cell Nuclei Correlates with Poorer Outcomes in Colorectal Cancer" Cells 8, no. 1: 25. https://doi.org/10.3390/cells8010025
APA StyleRuksha, K., Mezheyeuski, A., Nerovnya, A., Bich, T., Tur, G., Gorgun, J., Luduena, R., & Portyanko, A. (2019). Over-Expression of βII-Tubulin and Especially Its Localization in Cell Nuclei Correlates with Poorer Outcomes in Colorectal Cancer. Cells, 8(1), 25. https://doi.org/10.3390/cells8010025