

Molecular Aspects of Allergen-Specific Immunotherapy in Patients with Seasonal Allergic Rhinitis

 ,
,  , , , ,
, , , , 
Abstract
1. Introduction
2. Materials and Methods
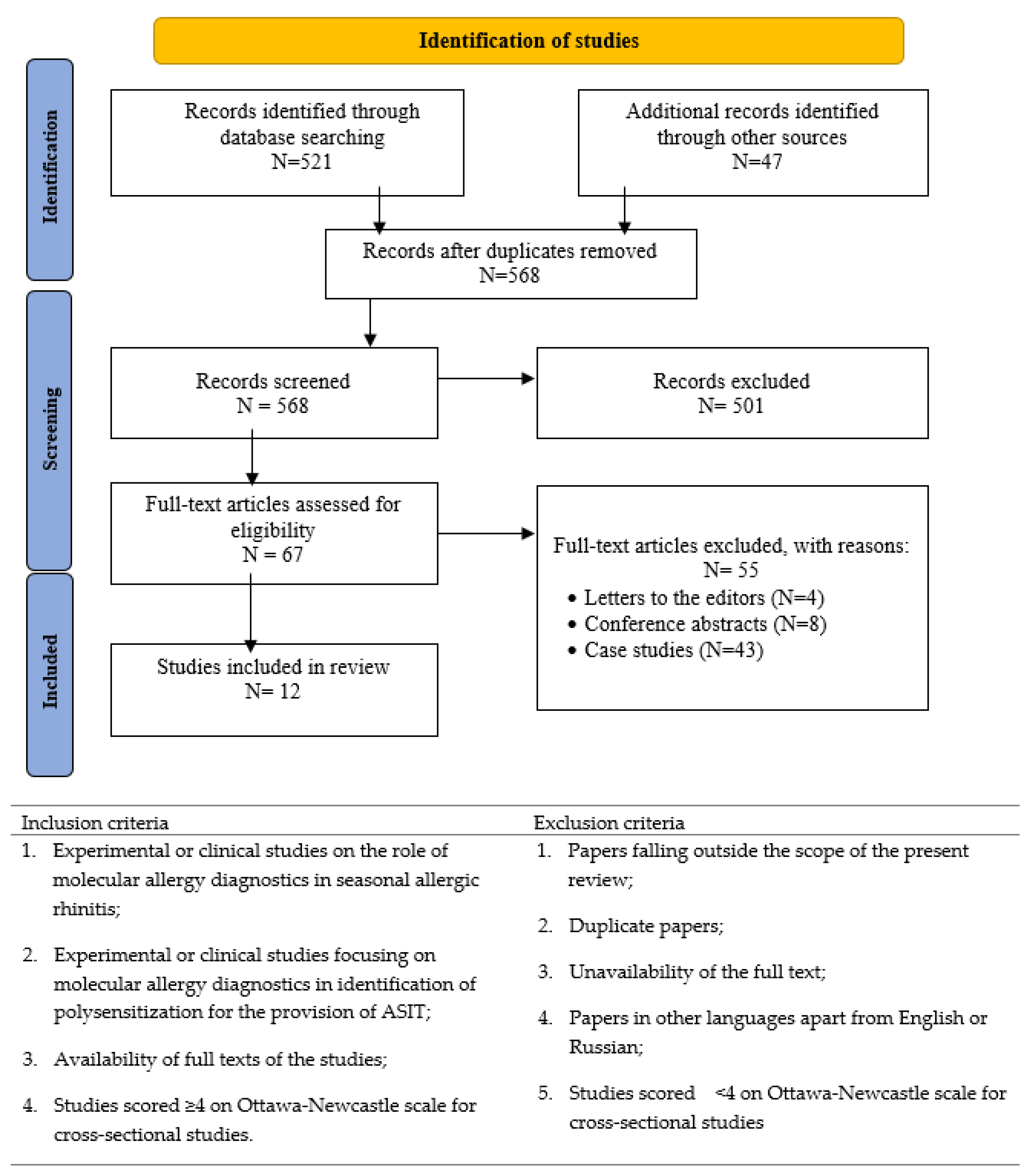
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Data Synthesis and Analysis
3. Results
3.1. Patient Characteristics
3.2. Evaluation of Component-Resolved Diagnosis
3.3. Efficiency of Component-Resolved Diagnosis for Use in ASIT
3.4. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsabouri, S.; Tseretopoulou, X.; Priftis, K.; Ntzani, E.E. Omalizumab for the Treatment of Inadequately Controlled Allergic Rhinitis: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. J. Allergy Clin. Immunol. Pract. 2014, 2, 332–340.e1. [Google Scholar] [CrossRef] [PubMed]
- Morjaria, J.B.; Caruso, M.; Emma, R.; Russo, C.; Polosa, R. Treatment of Allergic Rhinitis as a Strategy for Preventing Asthma. Curr. Allergy Asthma Rep. 2018, 18, 23. [Google Scholar] [CrossRef] [PubMed]
- Brożek, J.L.; Bousquet, J.; Agache, I.; Agarwal, A.; Bachert, C.; Bosnic-Anticevich, S.; Brignardello-Petersen, R.; Canonica, G.W.; Casale, T.; Chavannes, N.H.; et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines—2016 revision. J. Allergy Clin. Immunol. 2017, 140, 950–958. [Google Scholar] [CrossRef] [PubMed]
- Jutel, M.; Agache, I.; Bonini, S.; Burks, A.W.; Calderon, M.; Canonica, W.; Cox, L.; Demoly, P.; Frew, A.J.; O’Hehir, R.; et al. International Consensus on Allergen Immunotherapy II: Mechanisms, standardization, and pharmacoeconomics. J. Allergy Clin. Immunol. 2016, 137, 358–368. [Google Scholar] [CrossRef] [PubMed]
- Reddel, H.K.; FitzGerald, J.M.; Bateman, E.D.; Bacharier, L.B.; Becker, A.; Brusselle, G.; Buhl, R.; Cruz, A.A.; Fleming, L.; Inoue, H.; et al. GINA 2019: A fundamental change in asthma management: Treatment of asthma with short-acting bronchodilators alone is no longer recommended for adults and adolescents. Eur. Respir. J. 2019, 53, 1901046. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, K.; Mathie, R.T.; Costelloe, C.; Howick, J. Homeopathy for Allergic Rhinitis: A Systematic Review. J. Altern. Complement. Med. 2017, 23, 426–444. [Google Scholar] [CrossRef]
- Senti, G.; Freiburghaus, A.U.; Larenas-Linnemann, D.; Hoffmann, H.J.; Patterson, A.M.; Klimek, L.; Di Bona, D.; Pfaar, O.; Ahlbeck, L.; Akdis, M.; et al. Intralymphatic Immunotherapy: Update and Unmet Needs. Int. Arch. Allergy Immunol. 2019, 178, 141–149. [Google Scholar] [CrossRef]
- Larsson, O.; Hellkvist, L.; Peterson-Westin, U.; Cardell, L.O. Novel strategies for the treatment of grass pollen-induced allergic rhinitis. Expert Opin. Biol. Ther. 2016, 16, 1143–1150. [Google Scholar] [CrossRef]
- May, J.R.; Dolen, W.K. Management of Allergic Rhinitis: A Review for the Community Pharmacist. Clin. Ther. 2017, 39, 2410–2419. [Google Scholar] [CrossRef]
- Alessandri, C.; Ferrara, R.; Bernardi, M.L.; Zennaro, D.; Tuppo, L.; Giangrieco, I.; Ricciardi, T.; Tamburrini, M.; Ciardiello, M.A.; Mari, A. Molecular approach to a patient’s tailored diagnosis of the oral allergy syndrome. Clin. Transl. Allergy 2020, 10, 22. [Google Scholar] [CrossRef]
- Pablos, I.; Wildner, S.; Asam, C.; Wallner, M.; Gadermaier, G. Pollen Allergens for Molecular Diagnosis. Curr. Allergy Asthma Rep. 2016, 16, 31. [Google Scholar] [CrossRef] [PubMed]
- Crisci, C.D.; Ardusso, L.R.F. A Precision Medicine Approach to Rhinitis Evaluation and Management. Curr. Treat Options Allergy 2020, 7, 93–109. [Google Scholar] [CrossRef] [PubMed]
- Lipworth, B.; Newton, J.; Ram, B.; Small, I.; Schwarze, J. An algorithm recommendation for the pharmacological management of allergic rhinitis in the UK: A consensus statement from an expert panel. npj Prim. Care Respir. Med. 2017, 27, 3. [Google Scholar] [CrossRef] [PubMed]
- Bozek, A. Pharmacological Management of Allergic Rhinitis in the Elderly. Drugs Aging 2017, 34, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Wallace, D.V.; Dykewicz, M.S. Seasonal Allergic Rhinitis: A focused systematic review and practice parameter update. Curr. Opin. Allergy Clin. Immunol. 2017, 17, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Hoyte, F.C.L.; Nelson, H.S. Recent advances in allergic rhinitis [version 1; peer review: 2 approved]. F1000Research 2018, 7, 1333. [Google Scholar] [CrossRef]
- Chesné, J.; Schmidt-Weber, C.B.; von-Bieren, J.E. The Use of Adjuvants for Enhancing Allergen Immunotherapy Efficacy. Immunol. Allergy Clin. North Am. 2016, 36, 125–145. [Google Scholar] [CrossRef]
- Ciprandi, G.; Incorvaia, C.; Frati, F. Management of polysensitized patient: From molecular diagnostics to biomolecular immunotherapy. Expert Rev. Clin. Immunol. 2015, 11, 973–976. [Google Scholar] [CrossRef]
- Jutel, M.; Kosowska, A.; Smolinska, S. Allergen Immunotherapy: Past, Present, and Future. Allergy Asthma Immunol. Res. 2016, 8, 191–197. [Google Scholar] [CrossRef]
- Dretzke, J.; Meadows, A.; Novielli, N.; Huissoon, A.; Fry-Smith, A.; Meads, C. Subcutaneous and sublingual immunotherapy for seasonal allergic rhinitis: A systematic review and indirect comparison. J. Allergy Clin. Immunol. 2013, 131, 1361–1366. [Google Scholar] [CrossRef]
- Casale, T.B.; Cox, L.S.; Wahn, U.; Golden, D.B.K.; Bons, B.; Didier, A. Safety Review of 5-Grass Pollen Tablet from Pooled Data of Clinical Trials. J. Allergy Clin. Immunol. Pract. 2017, 5, 1717–1727.e1. [Google Scholar] [CrossRef] [PubMed]
- Arasi, S.; Corsello, G.; Villani, A.; Pajno, G.B. The future outlook on allergen immunotherapy in children: 2018 and beyond. Ital. J. Pediatr. 2018, 44, 80. [Google Scholar] [CrossRef] [PubMed]
- Pfaar, O.; Alvaro, M.; Cardona, V.; Hamelmann, E.; Mösges, R.; Kleine-Tebbe, J. Clinical trials in allergen immunotherapy: Current concepts and future needs. Allergy 2018, 73, 1775–1783. [Google Scholar] [CrossRef] [PubMed]
- Jutel, M.; Agache, I.; Bonini, S.; Burks, A.W.; Calderon, M.; Canonica, W.; Cox, L.; Demoly, P.; Frew, A.J.; O’Hehir, R.; et al. International consensus on allergy immunotherapy. J. Allergy Clin. Immunol. 2015, 136, 556–568. [Google Scholar] [CrossRef]
- Bousquet, J.; Khaltaev, N.; Cruz, A.A.; Denburg, J.; Fokkens, W.J.; Togias, A.; Zuberbier, T.; Canonica, G.W.; Weel, C.V.; Agache, I.; et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008. Prim. Care 2008, 63, 8–160. [Google Scholar]
- Jutel, M.; Bartkowiak-Emeryk, M.; Bręborowicz, A.; Cichocka-Jarosz, E.; Emeryk, A.; Gawlik, R.; Gonerko, P.; Rogala, B.; Nowak-Węgrzyn, A.; Samoliński, B. Sublingual immunotherapy (SLIT)—Indications, mechanism, and efficacy: Position paper prepared by the section of immunotherapy, polish society of allergy. Ann. Agric. Environ. Med. 2016, 23, 44–53. [Google Scholar] [CrossRef]
- Passalacqua, G.; Canonica, G.W. AIT (allergen immunotherapy): A model for the “precision medicine”. Clin. Mol. Allergy 2015, 13, 24. [Google Scholar] [CrossRef]
- Curin, M.; Khaitov, M.; Karaulov, A.; Namazova-Baranova, L.; Campana, R.; Garib, V.; Valenta, R. Next-Generation of Allergen-Specific Immunotherapies: Molecular Approaches. Curr. Allergy Asthma Rep. 2018, 18, 39. [Google Scholar] [CrossRef]
- Varadé, J.; Magadán, S.; González-fernández, Á. Human immunology and immunotherapy: Main achievements and challenges. Cell. Mol. Immunol. 2020, 18, 805–828. [Google Scholar] [CrossRef]
- Cardona, V.; Luengo, O.; Labrador-Horrillo, M. Immunotherapy in allergic rhinitis and lower airway outcomes. Allergy Eur. J. Allergy Clin. Immunol. 2017, 72, 35–42. [Google Scholar] [CrossRef]
- Petalas, K.; Durham, S.R. Allergen immunotherapy for allergic rhinitis. Rhinology 2013, 51, 99–110. [Google Scholar] [CrossRef]
- Zuberbier, T.; Bachert, C.; Bousquet, P.J.; Passalacqua, G.; Canonica, G.W.; Merk, H.; Worm, M.; Wahn, U.; Bousquet, J. GA2LEN/EAACI pocket guide for allergen-specific immunotherapy for allergic rhinitis and asthma. Allergy Eur. J. Allergy Clin. Immunol. 2010, 65, 1525–1530. [Google Scholar] [CrossRef] [PubMed]
- Shamji, M.H.; Kappen, J.H.; Akdis, M.; Jensen-Jarolim, E.; Knol, E.F.; Kleine-Tebbe, J.; Bohle, B.; Chaker, A.M.; Till, S.J.; Valenta, R.; et al. Biomarkers for monitoring clinical efficacy of allergen immunotherapy for allergic rhinoconjunctivitis and allergic asthma: An EAACI Position Paper. Allergy Eur. J. Allergy Clin. Immunol. 2017, 72, 1156–1173. [Google Scholar] [CrossRef] [PubMed]
- Incorvaia, C. Preventive capacity of allergen immunotherapy on the natural history of allergy. J. Prev. Med. Hyg. 2013, 54, 71–74. [Google Scholar] [CrossRef]
- Fitzhugh, D.J.; Lockey, R.F. Allergen immunotherapy: A history of the first 100 years. Curr. Opin. Allergy Clin. Immunol. 2011, 11, 554–559. [Google Scholar] [CrossRef]
- Didier, A.; Malling, H.J.; Worm, M.; Horak, F.; Sussman, G.; Melac, M.; Soulié, S.; Zeldin, R.K. Post-treatment efficacy of discontinuous treatment with 300IR 5-grass pollen sublingual tablet in adults with grass pollen-induced allergic rhinoconjunctivitis. Clin. Exp. Allergy 2013, 43, 568–577. [Google Scholar] [CrossRef]
- Würtzen, P.A.; Gupta, S.; Brand, S.; Andersen, P.S. Grass pollen immunotherapy: Where are we now. Immunotherapy 2016, 8, 399–411. [Google Scholar] [CrossRef]
- Komlósi, Z.I.; Kovács, N.; Sokolowska, M.; van de Veen, W.; Akdis, M.; Akdis, C.A. Highlights of Novel Vaccination Strategies in Allergen Immunotherapy. Immunol. Allergy Clin. N. Am. 2020, 40, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Durham, S.R.; Penagos, M. Sublingual or subcutaneous immunotherapy for allergic rhinitis? J. Allergy Clin. Immunol. 2016, 137, 339–349.e10. [Google Scholar] [CrossRef] [PubMed]
- Demoly, P.; Emminger, W.; Rehm, D.; Backer, V.; Tommerup, L.; Kleine-Tebbe, J. Effective treatment of house dust mite-induced allergic rhinitis with 2 doses of the SQ HDM SLIT-tablet: Results from a randomized, double-blind, placebo-controlled phase III trial. J. Allergy Clin. Immunol. 2016, 137, 444–451.e8. [Google Scholar] [CrossRef]
- Mosbech, H.; Canonica, G.W.; Backer, V.; De Blay, F.; Klimek, L.; Broge, L.; Ljørring, C. SQ house dust mite sublingually administered immunotherapy tablet (ALK) improves allergic rhinitis in patients with house dust mite allergic asthma and rhinitis symptoms. Ann. Allergy, Asthma Immunol. 2015, 114, 134–140.e1. [Google Scholar] [CrossRef] [PubMed]
- Dorofeeva, Y.; Shilovskiy, I.; Tulaeva, I.; Focke-tejkl, M.; Flicker, S.; Kudlay, D.; Khaitov, M.; Karsonova, A.; Riabova, K.; Karaulov, A.; et al. Past, present, and future of allergen immunotherapy vaccines. Allergy Eur. J. Allergy Clin. Immunol. 2021, 76, 131–149. [Google Scholar] [CrossRef] [PubMed]
- Di Bona, D.; Plaia, A.; Leto-Barone, M.S.; La Piana, S.; Di Lorenzo, G. Efficacy of subcutaneous and sublingual immunotherapy with grass allergens for seasonal allergic rhinitis: A meta-analysis-based comparison. J. Allergy Clin. Immunol. 2012, 130, 1097–1107.e2. [Google Scholar] [CrossRef]
- Calderon, M.A.; Cox, L.; Casale, T.B.; Moingeon, P.; Demoly, P. Multiple-allergen and single-allergen immunotherapy strategies in polysensitized patients: Looking at the published evidence. J. Allergy Clin. Immunol. 2012, 129, 929–934. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, J.; Anto, J.M.; Wickman, M.; Keil, T.; Valenta, R.; Haahtela, T.; Lodrup, K.; Wright, J.; Zuberbier, T.; Arshad, S.H.; et al. Are allergic multimorbidities and IgE polysensitization associated with the persistence or re-occurrence of foetal type 2 signalling? The MeDALL hypothesis. Allergy 2015, 70, 1062–1078. [Google Scholar] [CrossRef] [PubMed]
- Kalic, T.; Breiteneder, H. Advances and novel developments in molecular allergology. Allergy 2020, 75, 3027–3038. [Google Scholar] [CrossRef]
- Cox, L.; Nelson, H.; Lockey, R.; Spector, S.L.; Tilles, S.; Wallace, D. Task force report Allergen immunotherapy: A practice parameter third update. J. Allergy Clin. Immunol. 2011, 127, S1–S55. [Google Scholar] [CrossRef]
- Bousquet, J.; Pfaar, O.; Togias, A.; Schünemann, H.J.; Ansotegui, I.; Papadopoulos, N.G.; Tsiligianni, I.; Agache, I.; Anto, J.M.; Bachert, C.; et al. 2019 ARIA Care pathways for allergen immunotherapy. Allergy Eur. J. Allergy Clin. Immunol. 2019, 74, 2087–2102. [Google Scholar] [CrossRef]
- Klimek, L.; Bachert, C.; Pfaar, O.; Becker, S.; Bieber, T.; Brehler, R.; Buhl, R.; Casper, I.; Chaker, A.; Czech, W.; et al. ARIA guideline 2019: Treatment of allergic rhinitis in the German health system. Allergol. J. Int. 2019, 28, 255–276. [Google Scholar] [CrossRef]
- Alvaro-Lozano, M.; Akdis, C.A.; Akdis, M.; Alviani, C.; Angier, E.; Arasi, S.; Arzt-Gradwohl, L.; Barber, D.; Bazire, R.; Cavkaytar, O.; et al. Allergen Immunotherapy in Children User’s Guide. Pediatr. Allergy Immunol. 2020, 31, 1–101. [Google Scholar] [CrossRef]
- Frati, F.; Cecchi, L.; Scala, E.; Ridolo, E.; Albani, I.D.; Makrì, E.; Pajno, G.; Incorvaia, C. New product development with the innovative biomolecular sublingual immunotherapy formulations for the management of allergic rhinitis. Biol. Targets Ther. 2014, 8, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Chapman, M.D.; Wuenschmann, S.; King, E.; Pomés, A. Technological Innovations for High-Throughput Approaches to In Vitro Allergy Diagnosis. Physiol. Behav. 2019, 176, 139–148. [Google Scholar] [CrossRef]
- Matricardi, P.M.; Dramburg, S.; Potapova, E.; Skevaki, C.; Renz, H. Molecular diagnosis for allergen immunotherapy. J. Allergy Clin. Immunol. 2019, 143, 831–843. [Google Scholar] [CrossRef] [PubMed]
- Zidarn, M.; Robič, M.; Krivec, A.; Šilar, M.; Resch-Marat, Y.; Vrtala, S.; Kopač, P.; Bajrović, N.; Valenta, R.; Korošec, P. Clinical and immunological differences between asymptomatic HDM-sensitized and HDM-allergic rhinitis patients. Clin. Exp. Allergy 2019, 49, 808–818. [Google Scholar] [CrossRef] [PubMed]
- Matricardi, P.M.; Hoffmann, H.J.; Valenta, R.; Hilger, C.; Hofmaier, S.; Aalberse, R.C.; Agache, I.; Asero, R.; Barber, D.; Beyer, K.; et al. EAACI Molecular Allergology User’s Guide. Pediatr. Allergy Immunol. 2016, 27, 1–250. [Google Scholar] [CrossRef]
- Scala, E.; Alessandri, C.; Bernardi, M.L.; Ferrara, R.; Palazzo, P.; Pomponi, D.; Quaratino, D.; Rasi, C.; Zaffiro, A.; Zennaro, D.; et al. Cross-sectional survey on immunoglobulin E reactivity in 23 077 subjects using an allergenic molecule-based microarray detection system. Clin. Exp. Allergy 2010, 40, 911–921. [Google Scholar] [CrossRef]
- Liao, C.; Liang, C.; Hu, H.; Luo, W.; Wu, G.; Huang, Z.; Wu, L.; Sun, B. Major Pollen Allergen Components and CCD Detection in Bermuda Grass Sensitized Patients in Guangzhou, China. J. Asthma Allergy 2020, 13, 615–623. [Google Scholar] [CrossRef]
- Kristiansen, M.; Dhami, S.; Netuveli, G.; Halken, S.; Muraro, A.; Roberts, G.; Larenas-Linnemann, D.; Calderón, M.A.; Penagos, M.; Du Toit, G.; et al. Allergen immunotherapy for the prevention of allergy: A systematic review and meta-analysis. Pediatr. Allergy Immunol. 2017, 28, 18–29. [Google Scholar] [CrossRef]
- Santosa, A.; Andiappan, A.K.; Rotzschke, O.; Wong, H.C.; Chang, A.; Bigliardi-Qi, M.; Wang, D.Y.; Bigliardi, P.L. Evaluation of the applicability of the Immuno-solidphase allergen chip (ISAC) assay in atopic patients in Singapore. Clin. Transl. Allergy 2015, 5, 9. [Google Scholar] [CrossRef]
- González-Manceboa, E.; Domínguez-Ortegab, J.; Blanco-Bermejoc, S.; González-Secod, E.; Trujilloe, M.J.; de la Torre, F. Comparison of two diagnostic techniques, skin-prick test and component resolved diagnosis in the follow-up of a cohort of paediatric patients with pollinosis. Multicentre pilot study in a highly exposed allergenic area. Allergol. Immunopathol. 2017, 45, 121–126. [Google Scholar] [CrossRef]
- Moingeon, P. Biomarkers for Allergen Immunotherapy: A “Panoromic” View. Immunol. Allergy Clin. N. Am. 2016, 36, 161–179. [Google Scholar] [CrossRef] [PubMed]
- Baron-Bodo, V.; Horiot, S.; Lautrette, A.; Chabre, H.; Drucbert, A.S.; Danzé, P.M.; Sénéchal, H.; Peltre, G.; Galvain, S.; Zeldin, R.K.; et al. Heterogeneity of antibody responses among clinical responders during grass pollen sublingual immunotherapy. Clin. Exp. Allergy 2013, 43, 1362–1373. [Google Scholar] [CrossRef] [PubMed]
- Moingeon, P.; Lombardi, V.; Baron-Bodo, V.; Mascarell, L. Enhancing Allergen-Presentation Platforms for Sublingual Immunotherapy. J. Allergy Clin. Immunol. Pract. 2017, 5, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Van De Veen, W.; Stanic, B.; Yaman, G.; Wawrzyniak, M.; Söllner, S.; Akdis, D.G.; Rückert, B.; Akdis, C.A.; Akdis, M. IgG4 production is confined to human IL-10-producing regulatory B cells that suppress antigen-specific immune responses. J. Allergy Clin. Immunol. 2013, 131, 1204–1212. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.B.Y.; Agache, I.; Diamant, Z.; Eiwegger, T.; Traidl-hoffmann, W.J.F.C.; Nadeau, K.; Hehir, R.E.O.; Mahony, L.O.; Pfaar, O.; Torres, M.J.; et al. Biomarkers for diagnosis and prediction of therapy responses in allergic diseases and asthma. Allergy 2020, 75, 3039–3068. [Google Scholar] [CrossRef]
- Shamji, M.H.; Ljørring, C.; Francis, J.N.; A Calderon, M.; Larché, M.; Kimber, I.; Frew, A.J.; Ipsen, H.; Lund, K.; Würtzen, P.A.; et al. Functional rather than immunoreactive levels of IgG4 correlate closely with clinical response to grass pollen immunotherapy. Allergy Eur. J. Allergy Clin. Immunol. 2012, 67, 217–226. [Google Scholar] [CrossRef]
- Patelis, A.; Borres, M.P.; Kober, A.; Berthold, M. Multiplex component-based allergen microarray in recent clinical studies. Clin. Exp. Allergy 2016, 46, 1022–1032. [Google Scholar] [CrossRef] [PubMed]
- Sastre, J.; Sastre-Ibañez, M. Molecular diagnosis and immunotherapy. Curr. Opin. Allergy Clin. Immunol. 2016, 16, 565–570. [Google Scholar] [CrossRef]
- Lee, J.; Kim, S.; Choi, H.; Jung, C.; Ban, G.; Shin, Y.S.; Nahm, D.; Park, H.; Ye, Y. A Retrospective Study of Clinical Response Predictors in Subcutaneous Allergen Immunotherapy With House Dust Mites for Allergic Rhinitis. Allergy Asthma Immunol. Res. 2018, 10, 18–24. [Google Scholar] [CrossRef]
- Canonica, G.W.; Bachert, C.; Hellings, P.; Ryan, D.; Valovirta, E.; Wickman, M.; De Beaumont, O.; Bousquet, J. Allergen Immunotherapy (AIT): A prototype of Precision Medicine. World Allergy Organ. J. 2015, 8, 31. [Google Scholar] [CrossRef]
- Van Hage, M.; Schmid-Grendelmeier, P.; Skevaki, C.; Plebani, M.; Canonica, W.; Kleine-Tebbe, J.; Nystrand, M.; Jafari-Mamaghani, M.; Jakob, T. Performance evaluation of ImmunoCAP® ISAC 112: A multi-site study. Clin. Chem. Lab. Med. 2017, 55, 571–577. [Google Scholar] [CrossRef]
- Movérare, R.; Larsson, H.; Carlsson, R.; Holmquist, I. Mugwort-Sensitized Individuals from North Europe, South Europe and North America Show Different IgE Reactivity Patterns. Int. Arch. Allergy Immunol. 2011, 154, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Sastre, J.; Landivar, M.E.; Ruiz-García, M.; Andregnette-Rosigno, M.V.; Mahillo, I. How Molecular Diagnosis Can Change Allergen-Specific Immunotherapy Prescription in a Complex Pollen Area. Allergy 2012, 67, 709–711. [Google Scholar] [CrossRef] [PubMed]
- Letrán, A.; Espinazo, M.; Moreno, F. Measurement of IgE to Pollen Allergen Components Is Helpful in Selecting Patients for Immunotherapy. Ann. Allergy, Asthma Immunol. 2013, 111, 295–297. [Google Scholar] [CrossRef] [PubMed]
- Moreno, C.; Justicia, J.L.; Quiralte, J.; Moreno-Ancillo, Á.; Iglesias-Cadarso, A.; Torrecillas, M.; Labarta, N.; García, M.A.; Dávila, I. Olive, Grass or Both? Molecular Diagnosis for the Allergen Immunotherapy Selection in Polysensitized Pollinic Patients. Allergy 2014, 69, 1357–1363. [Google Scholar] [CrossRef]
- Stringari, G.; Tripodi, S.; Caffarelli, C.; Dondi, A.; Asero, R.; Bellini, F.; Maiello, N.; Frediani, T.; Peparini, I.; Dascola, P.; et al. The effect of component-resolved diagnosis on specific immunotherapy prescription in children with hay fever. J. Allergy Clin. Immunol. 2014, 134, 75–81. [Google Scholar] [CrossRef]
- Darsow, U.; Brockow, K.; Pfab, F.; Jakob, T.; Petersson, C.J.; Borres, M.P.; Ring, J.; Behrendt, H.; Huss-Marp, J. Heterogeneity of Molecular Sensitization Profiles in Grass Pollen Allergy—Implications for Immunotherapy? Clin. Exp. Allergy 2014, 44, 778–786. [Google Scholar] [CrossRef]
- Schmid, J.M.; Würtzen, P.A.; Dahl, R.; Hoffmann, H.J. Pretreatment IgE Sensitization Patterns Determine the Molecular Profile of the IgG4 Response during Updosing of Subcutaneous Immunotherapy with Timothy Grass Pollen Extract. J. Allergy Clin. Immunol. 2016, 137, 562–570. [Google Scholar] [CrossRef]
- Luo, W.; Pan, G.; Huang, H.; Zheng, P.; Wei, N.; Zhang, Y.; Zeng, G.; Sun, B. A Component-Resolved Diagnostic Approach for a Study on Grass Pollen Allergens in Chinese Southerners with Allergic Rhinitis and/or Asthma. J. Vis. Exp. 2017, 2017, e55723. [Google Scholar] [CrossRef]
- Martinez-Cañavate, A.; Torres Borrego, J.; Terán, A.B.M.; Higueras, J.L.C.; Figueroa, B.E.G.; Pacheco, R.R.; Aguilar, C.D.I.M. Molecular Sensitization Patterns and Influence of Molecular Diagnosis in Immunotherapy Prescription in Children Sensitized to Both Grass and Olive Pollen. Int. J. Lab. Hematol. 2018, 29, 369–374. [Google Scholar] [CrossRef]
- Camacho, G.D.-R.; Arjona, A.M.M.; Padial, J.F.-C.; Catalán, J.R. How Molecular Diagnosis May Modify Immunotherapy Prescription in Multi-Sensitized Pollen-Allergic Children. Allergol. Immunopathol. 2018, 46, 552–556. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Luo, W.; Wu, Z.; Cai, C.; Huang, H.; Sun, B. A Pilot Study on the Allergen-Speci Fi c IgE to Molecular Components on Polysensitized Mite Allergic Asthmatic Patients in Guangzhou, China. Mol. Immunol. 2019, 105, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Haidar, L.; Tamas, T.-P.; Stolz, F.; Patrascu, R.F.P.; Chen, K.-W.; Panaitescu, C. Symptom Patterns and Comparison of Diagnostic Methods in Ragweed Pollen Allergy. Exp. Ther. Med. 2021, 21, 525. [Google Scholar] [CrossRef]
- Villalta, D.; Tonutti, E.; Bizzaro, N.; Brusca, I.; Sargentini, V.; Asero, R.; Bilò, M.B.; Manzotti, G.; Murzilli, F.; Cecchi, L.; et al. Recommendations for the Use of Molecular Diagnostics in the Diagnosis of Allergic Diseases. Eur. Ann. Allergy Clin. Immunol. 2018, 50, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Canonica, G.W.; Ansotegui, I.J.; Pawankar, R.; Schmid-Grendelmeier, P.; Van Hage, M.; Baena-Cagnani, C.E.; Melioli, G.; Nunes, C.; Passalacqua, G.; Rosenwasser, L.; et al. A WAO-ARIA-GA2LEN Consensus Document on Molecular-Based Allergy Diagnostics. World Allergy Organ. J. 2013, 6, 17. [Google Scholar] [CrossRef]
- Sastre, J. Molecular Diagnosis in Allergy. Clin. Exp. Allergy 2010, 40, 1442–1460. [Google Scholar] [CrossRef]
- Dodig, S.; Čepelak, I. The Potential of Component-Resolved Diagnosis in Laboratory Diagnostics of Allergy. Biochem. Medica 2018, 28, 020501. [Google Scholar] [CrossRef]
- Akarsu, A.; Ocak, M.; Sahiner, U.M.; Soyer, O.; Sekerel, B.E. Multiplex Component-Based Allergen Macroarray Test Is Useful to Predict Clinical Reactivity to Tree Nuts in Children. Allergol. Int. 2022, 71, 236–247. [Google Scholar] [CrossRef]
- Hoover, H.; Leatherman, B.; Ryan, M.; McMains, K.; Veling, M. Evidence-Based Dosing of Maintenance Subcutaneous Immunotherapy: A Contemporary Review of State-of-the-Art Practice. Int. Forum Allergy Rhinol. 2018, 8, 806–816. [Google Scholar] [CrossRef]
- Roberts, G.; Pfaar, O.; Akdis, C.A.; Ansotegui, I.J.; Durham, S.R.; van Wijk, R.G.; Halken, S.; Larenas-Linnemann, D.; Pawankar, R.; Pitsios, C.; et al. EAACI Guidelines on Allergen Immunotherapy: Allergic Rhinoconjunctivitis. Allergy Eur. J. Allergy Clin. Immunol. 2018, 73, 765–798. [Google Scholar] [CrossRef]
- Calderon, M.A.; Demoly, P.; Van Wijk, R.G.; Bousquet, J.; Sheikh, A.; Frew, A.; Scadding, G.; Bachert, C.; Malling, H.J.; Valenta, R.; et al. EAACI: A European Declaration on Immunotherapy. Designing the Future of Allergen Specific Immunotherapy. Clin. Transl. Allergy 2012, 2, 20. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author, Year of Publication | Age of Patients | Sample Size | Type of Allergy | Country | Main Findings | Ottawa-Newcastle Score |
|---|---|---|---|---|---|---|
| Movérare, 2011 [72] | All ages | 110 | Mugwort allergy | Sweden, Estonia, Switzerland, Spain, Greece, United States, Canada | This research indicates a role for cross-reactive IgE antibodies in positive test results for mugwort in these subjects. Mugwort-sensitized subjects have different IgE reactivity profiles to weed allergens (Art v 3, Amb a 1, Par j 2, Sal k 1, Bet v 2, Bet v 4, CCDs). CRD in clinical practice leads to more detailed information on IgE reactivity at the molecular level that could be helpful to choose appropriate pollen extracts for ASIT *. | 4 |
| Sastre, 2012 [73] | All ages | 141 | Allergic rhinitis/asthma | Spain | There was a very low agreement between indications and use of allergens for specific immunotherapy before and after performing Component-resolved diagnosis (46% of patients). | 4 |
| Letrán, 2013 [74] | 6–62 years | 175 | Seasonal pollen-allergic rhinoconjunctivitis and/or asthma | Spain | The use of Component-resolved diagnosis helped to carefully select allergens for ASIT. CRD # changed the selection of allergens for ASIT in more than 50% of cases, as compared with the baseline selection. | 4 |
| Moreno, 2014 [75] | 5–65 years | 1263 | Seasonal allergic rhinitis, asthma, allergic conjunctivitis | Spain | The majority of patients (922 patients, 73%) would have been indicated for a mixture of grass and olive pollens for the provision of allergen immunotherapy. In 56.8% of patients, there was noncoincidence in the composition of allergen immunotherapy that would be selected before and after the investigation. CRD could help improve the selection of AIT in polysensitized patients. | 4 |
| Stringari, 2014 [76] | 4–18 years | 651 | Allergic rhinitis, asthma | Italy | The decision on prescription or composition of specific immunotherapy was changed in 277 (42%) of 651 children or 315 (48%) of 651 children, depending on the European or American approach, respectively. | 4 |
| Darsow, 2014 [77] | >18 years | 101 | Allergic rhinoconjunctivitis | Germany | There was significant heterogeneity in molecular sensitization profiles. None of the patients exactly matched the allergen composition of previous specific immunotherapy, containing Phl p 1, Phl p 2, Phl p 5a/b, and Phl p 6, the selection of which was based on conjunctival and nasal provocation tests. | 4 |
| Schmid, 2016 [78] | All ages | 24 | Seasonal rhinoconjunctivitis | Denmark | CRD suggests a personalized approach to ASIT. Change in IgE and IgG4 levels may be used as an early biomarker for ASIT effectiveness. | 7 |
| Luo, 2017 [79] | All ages | 346 | Allergic rhinitis and/or asthma | China | Only 17.1% of patients were sensitized to major allergens Phl p 1 and Phl p 5, and 100.0% of patients were sensitized to cross-reactive component Phl p 4. The authors conclude that ASIT is not indicated to all patients with timothy grass pollen sensitization. | 4 |
| Martínez-Cañavate Burgos, 2018 [80] | 5–18 years | 281 | Seasonal allergic rhinitis | Spain | Double sensitization to grass and olive pollen allergens was found in vitro in 76% of children for an IgE cutoff point of 0.35 kU/L. When the component-resolved diagnosis results were known, the composition of the prescribed immunotherapy was changed in 52.87% of cases. | 4 |
| Del-Río Camacho, 2018 [81] | 8–12 years | 70 | Allergic rhinitis and/or asthma | Spain | CRD led to a modified immunotherapy prescription in 54.3% of patients. Indications to the single-allergen therapy increased from 18% to 51% when the component-resolved diagnosis was included. The decision to prescribe immunotherapy was reversed following component-resolved diagnosis in 9.3% of cases. | 4 |
| Hu, 2019 [82] | 1–85 years | 57 | Allergic rhinitis, asthma | China | CRD identified the main dust mite allergen components leading to sensitization (nDer p 1, rDer p 2, nDer f 1, and rDer f 2) as well as cross-reactive components rDer p 10, which helped to make a meaningful selection of allergens for ASIT. | 4 |
| Haidar, 2021 [83] | All ages | 83 | Rhinitis, conjunctivitis, asthma | Romania | Most patients were polysensitized (62.65%), especially to other pollens, house dust mites, and animal danders. Only 90% of the patients with positive skin prick test to ragweed pollen extract also had increased specific serum IgE to Amb a 1. | 4 |
| Allergen Type (Source) | Allergenic Molecule | Group Type | Marker Type | Cross-Reactive Allergens |
|---|---|---|---|---|
| Major Components of Airborne Allergens | ||||
| Grass pollens | ||||
| Bermuda grass | nCyn d 1 | Group 1 | Major allergen | Grass pollen |
| Timothy grass | rPhl p 1 | Group 2 | Major allergen | Grass pollen |
| rPhl p 2 | Group 2 | Minor allergen | Grass pollen | |
| rPhl p 4 | Berberine bridge enzyme | Minor allergen | Grass pollen | |
| rPhl p 5 | Group 5 | Major allergen | Grass pollen | |
| rPhl p 6 | Group 6 | Minor allergen | Grass pollen | |
| rPhl p 11 | Ole-e-1-related protein | Minor allergen | Grass pollen | |
| Tree pollens | ||||
| Birch | rBet v 1 | PR-10 protein | Major allergen | Fruits, vegetables, nuts, seeds, beans, tree pollens (birch, alder, hazel, hornbeam), carrot, celery, apple, apricot, cherry, pear, spices |
| Japanese cedar | nCry j 1 | Pectate lyase | Major allergen | Tree pollens |
| Cypress | nCup a 1 | Pectate lyase | Major allergen | Tree pollens (cypress family: juniper, cypress, cedar) |
| Olive | rOle e 1 | General olive group 5 | Major allergen | Tree pollens It is a marker of a high degree of cross-reactivity with ash, privet, lilac, and angustifolia, although these pollens are not identical. rOle e1 is homologous with proteins of sycamore, plantain, saffron, and cereal crop: timothy grass, rye, and corn. |
| rOle e 9 | 1,3-beta-glucanase | Minor allergen | Tree pollen | |
| Platanus acerifolia, Plane tree | rPla a 1 | Invertase inhibitor | Major allergen | Tree pollen |
| rPla a 2 | Polygalacturonase | Minor allergen | Tree pollen | |
| Weed pollens | ||||
| Ambrosia | Amb a 1 | Pectate lyase | Major allergen | Weed pollens It is a marker of true sensitization to ambrosia and cross-reactivity with cereal crop and weed pollens. |
| Artemisia vulgaris | Art v 1 | Defensin | Major allergen | Weed, grass, and tree pollens. It is responsible for cross-reactivity with pollens of various plants: ragweed, daisy, chamomile, dandelion, sunflower, calendula, elecampane, string, coltsfoot, citrus fruits, kiwi, mango, sunflower seed, honey, chicory, parsley, carrots, tomatoes, peas, dill, hazelnuts, peanuts, red pepper. |
| Chenopodium album | rChe a 1 | Ole-e-1-related protein | Major allergen | Weed pollens |
| Pellitory | rPar j 2 | Lipid transport proteins (nsLTP) | Major allergen | Weed pollens |
| Plantain | rPla I 1 | Ole-e-1-related protein | Major allergen | Weed pollens |
| Kali tragus | nSal k 1 | Pectin methyl esterase | Major allergen | Weed pollens |
| Species-specific and cross-reactive components | ||||
| Olive pollen | Ole e 7 | Lipid transport proteins (nsLTP) | Minor allergens | Fruits, vegetables, nuts, seeds, beans, cereal crop, spices, tree, and weed pollens |
| Plane tree | Pla a 3 | |||
| Birch | Bet v 1 | PR-10 protein | Major allergens | Fruits, vegetables, nuts, seeds, beans, tree pollens (alder, hazel, hornbeam), carrot, celery, apple, peach, cherry, pear, spices, and peanuts. |
| Alder | Aln g 1 | |||
| Hazel | rCor a 1.0101 | |||
| Birch | rBet v 2 | Profilin | Minor allergens | Fruits, vegetables, nuts, seeds, beans, cereal crop, spices, latex, weed, grass, and tree pollens (olive, bermudagrass, pellitory, sunflower, date fruit, banana, pineapple, and exotic fruits) |
| Forest grass | rMer a 1 | |||
| Timothy grass | rPhl p 12 | |||
| Birch | rBet v 4 | Polcalcin | Minor allergens | Weed, grass, and tree pollens (Timothy grass, bermudagrass, turnip, rape, European olives, black alder) and could serve as a marker of polyvalent sensitization to plant allergens. |
| Timothy grass | rPhl p 7 | Weed, grass, and tree pollens (beech family: birch and olives) | ||
| Group Type | Degree of Cross-Reactivity | Properties | Inhalant Allergens |
|---|---|---|---|
| Polcalcins (calcium-binding proteins) | High | - | Bet v4, Phl p7 |
| Profilins | High | Susceptible to high temperatures and digestive enzymes | Bet v2, rMer a 1, Phl p12 |
| Nonspecific lipid transport proteins (nsLTP) | Various | Resistant to high temperatures and digestive enzymes | Art v 3, Ole e 7, Pla a 3 |
| Pathogenesis-related protein family 10 (PR-10), Bet v 1 homolog | High | Susceptible to high temperatures and digestive enzymes | Bet v 1, Aln g 1, rCor a 1.0101 |
| Cross-reactive carbo-hydrate determinants (CCD) | High | Resistant to high temperatures | nCyn d1, nOle e1, nCup a 1, nSal k 1, nPla a 2, nArt v 1, Phl p 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Izmailovich, M.; Semenova, Y.; Abdushukurova, G.; Mukhamejanova, A.; Dyussupova, A.; Faizova, R.; Gazaliyeva, M.; Akhvlediani, L.; Glushkova, N.; Kalmakhanov, S.; et al. Molecular Aspects of Allergen-Specific Immunotherapy in Patients with Seasonal Allergic Rhinitis. Cells 2023, 12, 383. https://doi.org/10.3390/cells12030383
Izmailovich M, Semenova Y, Abdushukurova G, Mukhamejanova A, Dyussupova A, Faizova R, Gazaliyeva M, Akhvlediani L, Glushkova N, Kalmakhanov S, et al. Molecular Aspects of Allergen-Specific Immunotherapy in Patients with Seasonal Allergic Rhinitis. Cells. 2023; 12(3):383. https://doi.org/10.3390/cells12030383
Chicago/Turabian StyleIzmailovich, Marina, Yuliya Semenova, Gulzada Abdushukurova, Ainur Mukhamejanova, Azhar Dyussupova, Raida Faizova, Meruert Gazaliyeva, Leila Akhvlediani, Natalya Glushkova, Sundetgali Kalmakhanov, and et al. 2023. "Molecular Aspects of Allergen-Specific Immunotherapy in Patients with Seasonal Allergic Rhinitis" Cells 12, no. 3: 383. https://doi.org/10.3390/cells12030383
APA StyleIzmailovich, M., Semenova, Y., Abdushukurova, G., Mukhamejanova, A., Dyussupova, A., Faizova, R., Gazaliyeva, M., Akhvlediani, L., Glushkova, N., Kalmakhanov, S., & Bjørklund, G. (2023). Molecular Aspects of Allergen-Specific Immunotherapy in Patients with Seasonal Allergic Rhinitis. Cells, 12(3), 383. https://doi.org/10.3390/cells12030383