


Anti-Inflammatory and Immunomodulatory Effect of High-Dose Immunoglobulins in Children: From Approved Indications to Off-Label Use
 , ,
, ,  , ,
, , 
 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
- they had to be meta-analysis, systematic reviews, reviews, clinical trials, retrospective and/or prospective observational studies, comparative studies, case series, or reports focusing on the immunomodulatory treatment of hematologic, neurologic, and inflammatory immune dysregulation disorders;
- the full text had to be available.
- they were editorials, or conference abstracts;
- the articles were written in a language other than English;
- full-text versions of the articles could not be obtained.
2.3. Study Selection
2.4. Results
3. Results
3.1. Immunoglobulins and Immune-Mediated Neurological Disorders
3.1.1. Acute and Chronic Inflammatory Neuropathies
3.1.2. Myasthenia Gravis (MG)
3.1.3. Autoimmune Encephalitis (AE)
3.1.4. Autoimmune Demyelinating Disorders of CNS
3.1.5. Myelin Oligodendrocyte Glycoprotein (MOG) Associated Disorder (MOGAD)
3.1.6. Opsoclonus-Myoclonus-Ataxia Syndrome (OMAS)
3.1.7. Other Neurological Disorders with Limited or Inconclusive Evidence
3.2. Immunoglobulins in Hematological Conditions
3.2.1. Immune Thrombocytopenia (ITP)
3.2.2. Autoimmune Hemolytic Anemia (AIHA)
3.2.3. Autoimmune Neutropenia (AIN)
3.2.4. Acquired Hemophilia (AHA)
3.2.5. Neonatal Alloimmune Thrombocytopenia (NAIT)
3.2.6. Post-Transfusion Purpura (PTP)
3.2.7. Thrombotic Thrombocytopenic Purpura (TTP)
3.3. Immunoglobulins and Inflammatory Diseases
3.3.1. Juvenile Idiopathic Arthritis (JIA)
3.3.2. Juvenile Dermatomyositis (JDM)
3.3.3. Childhood-Onset Systemic Lupus Erythematosus (cSLE)
3.3.4. Henoch-Schönlein Purpura (HSP)
3.3.5. Kawasaki Disease (KD)
3.3.6. Multisystem Inflammatory Syndrome in Children (MIS-C)
3.4. Monitoring, Prevention, and Treatment of Adverse Effects
4. Discussion
- Formulating international guidelines on which a spectrum of other global, national, regional, and local initiatives should be aligned, encompassing consensus documents, audit programs, and monitoring frameworks.
- Implementing robust data collection mechanisms for IVIG/SCIG usage, IVIG/SCIG-requiring disease prevalence and diagnoses (e.g., IEI registries), as well as dosage and clinical outcome data, thereby facilitating an evidence-based evaluation of the efficacy of IVIG-SCIG prescriptions.
- Exploring viable alternatives to IVIG/SCIG therapy to mitigate the growing demand and address supply constraints.
- Ensuring access to proficient immunologists who possess expertise in the judicious prescription of IVIG/SCIG, while also fostering collaboration among less experienced clinicians and their more seasoned counterparts to facilitate knowledge sharing and skill development.
- Refraining from utilizing IVIG/SCIG in cases where its efficacy is tenuous, uncertain, or not well-established, unless the situation involves a life-threatening condition that may potentially benefit from rescue HD-IVIG. Whenever possible and if suitable, it is preferable to explore alternative, safe, and cost-effective therapeutic options. This approach is aimed at preserving the availability of IVIG/SCIG for patients with IEI primarily suffering from antibody deficiencies, for whom IgRT serves as a crucial and life-saving treatment.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Immunoglobulins and Infectious Conditions
References
- Bruton, O.C. Agammaglobulinemia. Pediatrics 1952, 9, 722–728. [Google Scholar] [CrossRef]
- European Medicines Agency. Guideline on the Clinical Investigation of Human Immunoglobulin for Intravenous Administration (IVIg). EMA/CHMP/BPWP/94033/2007 Rev. 4. Draft Committee for Medicinal Products for Human (CHMP). 13 October 2020. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-investigation-human-normal-immunoglobulin-intravenous-administration-ivig-rev-4_en.pdf (accessed on 1 August 2023).
- Prevot, J.; Jolles, S. Global immunoglobulin supply: Steaming towards the iceberg? Curr. Opin. Allergy Clin. Immunol. 2020, 20, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Brand, A.; De Angelis, V.; Vuk, T.; Garraud, O.; Lozano, M.; Politis, D. Review of indications for immunoglobulin (IG) use: Narrowing the gap between supply and demand. Transfus. Clin. Biol. 2021, 28, 96–122. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Model List of Essential Medicines for Children, 8th List, 2021; World Health Organization: Geneva, Switzerland, 2021.
- World Health Organization Model List of Essential Medicines, 22nd List, 2021; World Health Organization: Geneva, Switzerland, 2021.
- Marchesi, A.; De Jacobis, I.T.; Rigante, D.; Rimini, A.; Malorni, W.; Corsello, G.; Bossi, G.; Buonuomo, S.; Cardinale, F.; Cortis, E.; et al. Kawasaki disease: Guidelines of the Italian Society of Pediatrics, part I—Definition, epidemiology, etiopathogenesis, clinical expression and management of the acute phase. Ital. J. Pediatr. 2018, 44, 102. [Google Scholar] [CrossRef] [PubMed]
- Parodi, E.; Russo, G.; Farruggia, P.; Notarangelo, L.D.; Giraudo, M.T.; Nardi, M.; Giona, F.; Giordano, P.; Ramenghi, U.; Barone, A.; et al. Management strategies for newly diagnosed immune thrombocytopenia in Italian AIEOP Centres: Do we overtreat? Data from a multicentre, prospective cohort study. Blood Transfus. 2020, 18, 396–405. [Google Scholar] [CrossRef] [PubMed]
- DeSouza, S.; Angelini, D. Updated guidelines for immune thrombocytopenic purpura: Expanded management options. Clevel. Clin. J. Med. 2021, 88, 664–668. [Google Scholar] [CrossRef] [PubMed]
- Eftimov, F.; Winer, J.B.; Vermeulen, M.; de Haan, R.; van Schaik, I.N. Intravenous immunoglobulin for chronic inflammatory demyelinating polyradiculoneuropathy. Cochrane Database Syst. Rev. 2013, 12, CD001797. [Google Scholar] [CrossRef] [PubMed]
- Keddie, S.; Eftimov, F.; van den Berg, L.H.; Brassington, R.; de Haan, R.J.; van Schaik, I.N. Immunoglobulin for multifocal motor neuropathy. Cochrane Database Syst. Rev. 2022, 11, CD004429. [Google Scholar] [CrossRef]
- Doets, A.Y.; Hughes, R.A.; Brassington, R.; Hadden, R.D.; Pritchard, J. Pharmacological treatment other than corticosteroids, intravenous immunoglobulin and plasma exchange for Guillain-Barré syndrome. Cochrane Database Syst. Rev. 2020, 11, CD008630. [Google Scholar] [CrossRef]
- Hughes, R.A.; Swan, A.V.; van Doorn, P.A. Intravenous immunoglobulin for Guillain-Barré syndrome. Cochrane Database Syst. Rev. 2014, 2019, CD002063. [Google Scholar] [CrossRef]
- Verboon, C.; Harbo, T.; Cornblath, D.R.; Hughes, R.A.C.; van Doorn, P.A.; Lunn, M.P.; Gorson, K.C.; Barroso, F.; Kuwabara, S.; Galassi, G.; et al. Intravenous immunoglobulin treatment for mild Guillain-Barré syndrome: An international observational study. J. Neurol. Neurosurg. Psychiatry 2021, 92, 1080–1088. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, J.H.O.; Enk, A.H. High-dose intravenous immunoglobulin in skin autoimmune disease. Front Immunol. 2019, 10, 1090. [Google Scholar] [CrossRef] [PubMed]
- Bayry, J.; Ahmed, E.A.; Toscano-Rivero, D.; Vonniessen, N.; Genest, G.; Cohen, C.G.; Dembele, M.; Kaveri, S.V.; Mazer, B.D. Intravenous Immunoglobulin: Mechanism of Action in Autoimmune and Inflammatory Conditions. J. Allergy Clin. Immunol. Pract. 2023, 11, 1688–1697. [Google Scholar] [CrossRef] [PubMed]
- Clynes, R. Immune complexes as therapy for autoimmunity. J. Clin. Investig. 2005, 115, 25–27. [Google Scholar] [CrossRef] [PubMed]
- Siragam, V.; Brinc, D.; Crow, A.R.; Song, S.; Freedman, J.; Lazarus, A.H. Can antibodies with specificity for soluble antigens mimic the therapeutic effects of intravenous IgG in the treatment of autoimmune disease? J. Clin. Investig. 2005, 115, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Samuelsson, A.; Towers, T.L.; Ravetch, J.V. Anti-inflammatory Activity of IVIG Mediated Through the Inhibitory Fc Receptor. Science 2001, 291, 484–486. [Google Scholar] [CrossRef] [PubMed]
- Debré, M.; Griscelli, C.; Bonnet, M.-C.; Carosella, E.; Philippe, N.; Reinert, P.; Vilmer, E.; Kaplan, C.; Fridman, W.; Teillaud, J.-L. Infusion of Fcγ fragments for treatment of children with acute immune thrombocytopenic purpura. Lancet 1993, 342, 945–949. [Google Scholar] [CrossRef]
- Crow, A.R.; Suppa, S.J.; Chen, X.; Mott, P.J.; Lazarus, A.H. The neonatal Fc receptor (FcRn) is not required for IVIg or anti-CD44 monoclonal antibody–mediated amelioration of murine immune thrombocytopenia. Blood 2011, 118, 6403–6406. [Google Scholar] [CrossRef]
- Anthony, R.M.; Kobayashi, T.; Wermeling, F.; Ravetch, J.V. Intravenous gammaglobulin suppresses inflammation through a novel TH2 pathway. Nature 2011, 475, 110–113. [Google Scholar] [CrossRef]
- Anthony, R.M.; Wermeling, F.; Karlsson, M.C.I.; Ravetch, J.V. Identification of a receptor required for the anti-inflammatory activity of IVIG. Proc. Natl. Acad. Sci. USA 2008, 105, 19571–19578. [Google Scholar] [CrossRef]
- Galeotti, C.; Stephen-Victor, E.; Karnam, A.; Das, M.; Gilardin, L.; Maddur, M.S.; Wymann, S.; Vonarburg, C.; Chevailler, A.; Dimitrov, J.D.; et al. Intravenous immunoglobulin induces IL-4 in human basophils by signaling through surface-bound IgE. J. Allergy Clin. Immunol. 2019, 144, 524–535.e8. [Google Scholar] [CrossRef] [PubMed]
- Das, M.; Karnam, A.; Stephen-Victor, E.; Gilardin, L.; Bhatt, B.; Sharma, V.K.; Rambabu, N.; Patil, V.; Lecerf, M.; Käsermann, F.; et al. Intravenous immunoglobulin mediates anti-inflammatory effects in peripheral blood mononuclear cells by inducing autophagy. Cell Death Dis. 2020, 11, 50. [Google Scholar] [CrossRef] [PubMed]
- Martínez, T.; Garcia-Robledo, J.E.; Plata, I.; Urbano, M.-A.; Posso-Osorio, I.; Rios-Serna, L.J.; Barrera, M.C.; Tobón, G.J. Mechanisms of action and historical facts on the use of intravenous immunoglobulins in systemic lupus erythematosus. Autoimmun. Rev. 2019, 18, 279–286. [Google Scholar] [CrossRef]
- Shoenfeld, Y. Efficacy of IVIG affinity-purified anti-double-stranded DNA anti-idiotypic antibodies in the treatment of an experimental murine model of systemic lupus erythematosus. Int. Immunol. 2002, 14, 1303–1311. [Google Scholar] [CrossRef] [PubMed]
- Rossi, F.; Dietrich, G.; Kazatchkine, M.D. Antiidiotypic suppression of autoantibodies with normal polyspecific immunoglobulins. Res. Immunol. 1989, 140, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Basta, M.; Van Goor, F.; Luccioli, S.; Billings, E.M.; Vortmeyer, A.O.; Baranyi, L.; Szebeni, J.; Alving, C.R.; Carroll, M.C.; Berkower, I.; et al. F(ab)′2-mediated neutralization of C3a and C5a anaphylatoxins: A novel effector function of immunoglobulins. Nat. Med. 2003, 9, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Spycher, M.; Matozan, K.; Minnig, K.; Zehnder, R.; Miescher, S.; Hoefferer, L.; Rieben, R. In vitro comparison of the complement-scavenging capacity of different intravenous immunoglobulin preparations. Vox Sang. 2009, 97, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Udi, N.; Yehuda, S. Intravenous immunoglobulin—Indications and mechanisms in cardiovascular diseases. Autoimmun. Rev. 2008, 7, 445–452. [Google Scholar] [CrossRef] [PubMed]
- Uozumi, R.; Iguchi, R.; Masuda, S.; Nishibata, Y.; Nakazawa, D.; Tomaru, U.; Ishizu, A. Pharmaceutical immunoglobulins reduce neutrophil extracellular trap formation and ameliorate the development of MPO-ANCA-associated vasculitis. Mod. Rheumatol. 2020, 30, 544–550. [Google Scholar] [CrossRef]
- von Gunten, S.; Vogel, M.; Schaub, A.; Stadler, B.M.; Miescher, S.; Crocker, P.R.; Simon, H.-U. Intravenous immunoglobulin preparations contain anti–Siglec-8 autoantibodies. J. Allergy Clin. Immunol. 2007, 119, 1005–1011. [Google Scholar] [CrossRef]
- McAlpine, S.M.; Roberts, S.E.; Heath, J.J.; Käsermann, F.; Issekutz, A.C.; Issekutz, T.B.; Derfalvi, B. High Dose Intravenous IgG Therapy Modulates Multiple NK Cell and T Cell Functions in Patients with Immune Dysregulation. Front. Immunol. 2021, 12, 660506. [Google Scholar] [CrossRef]
- Ebbo, M.; Audonnet, S.; Grados, A.; Benarous, L.; Mahevas, M.; Godeau, B.; Viallard, J.; Piperoglou, C.; Cognet, C.; Farnarier, C.; et al. NK cell compartment in the peripheral blood and spleen in adult patients with primary immune thrombocytopenia. Clin. Immunol. 2017, 177, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Mausberg, A.K.; Heininger, M.K.; Zu Horste, G.M.; Cordes, S.; Fleischer, M.; Szepanowski, F.; Kleinschnitz, C.; Hartung, H.-P.; Kieseier, B.C.; Stettner, M. NK cell markers predict the efficacy of IV immunoglobulins in CIDP. Neurol.-Neuroimmunol. Neuroinflamm. 2020, 7, e884. [Google Scholar] [CrossRef] [PubMed]
- Bohn, A.B.; Nederby, L.; Harbo, T.; Skovbo, A.; Vorup-Jensen, T.; Krog, J.; Jakobsen, J.; Hokland, M.E. The effect of IgG levels on the number of natural killer cells and their Fc receptors in chronic inflammatory demyelinating polyradiculoneuropathy. Eur. J. Neurol. 2011, 18, 919–924. [Google Scholar] [CrossRef] [PubMed]
- Maddur, M.S.; Sharma, M.; Hegde, P.; Lacroix-Desmazes, S.; Kaveri, S.V.; Bayry, J. Inhibitory Effect of IVIG on IL-17 Production by Th17 Cells is Independent of Anti-IL-17 Antibodies in the Immunoglobulin Preparations. J. Clin. Immunol. 2013, 33, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Maddur, M.S.; Vani, J.; Hegde, P.; Lacroix-Desmazes, S.; Kaveri, S.V.; Bayry, J. Inhibition of differentiation, amplification, and function of human TH17 cells by intravenous immunoglobulin. J. Allergy Clin. Immunol. 2011, 127, 823–830.e7. [Google Scholar] [CrossRef]
- Séïté, J.-F.; Goutsmedt, C.; Youinou, P.; Pers, J.-O.; Hillion, S. Intravenous immunoglobulin induces a functional silencing program similar to anergy in human B cells. J. Allergy Clin. Immunol. 2014, 133, 181–188.e9. [Google Scholar] [CrossRef]
- Séité, J.F.; Guerrier, T.; Cornec, D.; Jamin, C.; Youinou, P.; Hillion, S. TLR9 responses of B cells are repressed by intravenous immunoglobulin through the recruitment of phosphatase. J. Autoimmun. 2011, 37, 190–197. [Google Scholar] [CrossRef]
- Trinath, J.; Hegde, P.; Sharma, M.; Maddur, M.S.; Rabin, M.; Vallat, J.-M.; Magy, L.; Balaji, K.N.; Kaveri, S.V.; Bayry, J. Intravenous immunoglobulin expands regulatory T cells via induction of cyclooxygenase-2–dependent prostaglandin E2 in human dendritic cells. Blood 2013, 122, 1419–1427. [Google Scholar] [CrossRef]
- Kamaguchi, M.; Iwata, H.; Mori, Y.; Toyonaga, E.; Ujiie, H.; Kitagawa, Y.; Shimizu, H. Anti-idiotypic Antibodies against BP-IgG Prevent Type XVII Collagen Depletion. Front. Immunol. 2017, 8, 1669. [Google Scholar] [CrossRef]
- Patwa, H.S. Dosing and individualized treatment—Patient-centric treatment: Changing practice guidelines. Clin. Exp. Immunol. 2014, 178, 36–38. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zandman-Goddard, G.; Krauthammer, A.; Levy, Y.; Langevitz, P.; Shoenfeld, Y. Long-Term Therapy with Intravenous Immunoglobulin is Beneficial in Patients with Autoimmune Diseases. Clin. Rev. Allergy Immunol. 2012, 42, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Mdsas, M.F. Immunoglobulin Database Data Update 2020/21 September 2022 Compiled by Mark Foster MDSAS. Available online: https://igd.mdsas.com/wp-content/uploads/immunoglobulindatabasedataupdate202021.pdf (accessed on 1 August 2023).
- Ig Usage Data and Statistics—July 2022 | National Blood Authority. Available online: https://www.blood.gov.au/ig-usage-data-and-statistics (accessed on 1 August 2023).
- George, R. Nine Pints: A Journey through the Money, Medicine and Mysteries of Blood; Metropolitan Books: New York, NY, USA, 2018. [Google Scholar]
- Marketing Research Bureau. Plasma Economics: How Demand for Plasma Proteins Affects Plasma Fractionation Volumes. Available online: https://marketingresearchbureau.com/plasma-industry/plasma-economics-concept-of-plasma-market-driver/ (accessed on 1 August 2023).
- Gadian, J.; Kirk, E.; Holliday, K.; Lim, M.; Absoud, M. Systematic review of immunoglobulin use in paediatric neurological and neurodevelopmental disorders. Dev. Med. Child Neurol. 2017, 59, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Vitaliti, G.; Tabatabaie, O.; Matin, N.; Ledda, C.; Pavone, P.; Lubrano, R.; Serra, A.; Di Mauro, P.; Cocuzza, S.; Falsaperla, R. The usefulness of immunotherapy in pediatric neurodegenerative disorders: A systematic review of literature data. Hum. Vaccines Immunother. 2015, 11, 2749–2763. [Google Scholar] [CrossRef] [PubMed]
- Racosta, J.M.; Sposato, L.A.; Kimpinski, K. Subcutaneous versus intravenous immunoglobulin for chronic autoimmune neuropathies: A meta-analysis. Muscle Nerve 2017, 55, 802–809. [Google Scholar] [CrossRef] [PubMed]
- Gaspard, N.; Hirsch, L.J.; Sculier, C.; Loddenkemper, T.; van Baalen, A.; Lancrenon, J.; Emmery, M.; Specchio, N.; Farias-Moeller, R.; Wong, N.; et al. New-onset refractory status epilepticus (NORSE) and febrile infection-related epilepsy syndrome (FIRES): State of the art and perspectives. Epilepsia 2018, 59, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Kramer, U.; Chi, C.-S.; Lin, K.-L.; Specchio, N.; Sahin, M.; Olson, H.; Nabbout, R.; Kluger, G.; Lin, J.-J.; van Baalen, A. Febrile infection-related epilepsy syndrome (FIRES): Pathogenesis, treatment, and outcome. Epilepsia 2011, 52, 1956–1965. [Google Scholar] [CrossRef]
- Klein da Costa, B.; Banwell, B.L.; Sato, D.K. Treatment of MOG-IgG associated disease in paediatric patients: A systematic review. Mult. Scler. Relat. Disord. 2021, 56, 103216. [Google Scholar] [CrossRef]
- Nosadini, M.; Eyre, M.; Molteni, E.; Thomas, T.; Irani, S.R.; Dalmau, J.; Dale, R.C.; Lim, M.; Anlar, B.; Armangue, T.; et al. Use and Safety of Immunotherapeutic Management of N-Methyl-d-Aspartate Receptor Antibody Encephalitis: A Meta-analysis. JAMA Neurol. 2021, 78, 1333–1344. [Google Scholar] [CrossRef]
- de Alarcon, P.A.; Matthay, K.K.; London, W.B.; Naranjo, A.; Tenney, S.C.; Panzer, J.A.; Hogarty, M.D.; Park, J.R.; Maris, J.M.; Cohn, S.L. Intravenous immunoglobulin with prednisone and risk-adapted chemotherapy for children with opsoclonus myoclonus ataxia syndrome associated with neuroblastoma (ANBL00P3): A randomised, open-label, phase 3 trial. Lancet Child Adolesc. Health 2018, 2, 25. [Google Scholar] [CrossRef]
- Johnson, M.; Ehlers, S.; Fernell, E.; Hajjari, P.; Wartenberg, C.; Wallerstedt, S.M. Anti-inflammatory, antibacterial and immunomodulatory treatment in children with symptoms corresponding to the research condition PANS (Pediatric Acuteonset Neuropsychiatric Syndrome): A systematic review. PLoS ONE 2021, 16, e0253844. [Google Scholar] [CrossRef] [PubMed]
- Orsini, A.; Foiadelli, T.; Magistrali, M.; Carli, N.; Bagnasco, I.; Dassi, P.; Verrotti, A.; Marcotulli, D.; Canavese, C.; Nicita, F.; et al. A nationwide study on Sydenham’s chorea: Clinical features, treatment and prognostic factors: A multicenter cohort study on Sydenham’s chorea. Eur. J. Paediatr. Neurol. 2022, 36, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, S.S.; Nosadini, M.; Grattan-Smith, P.; Dale, R.C. Intravenous immunoglobulin in acute Sydenham’s chorea: A systematic review Selected studies and critical appraisal. J. Paediatr. Child Health 2015, 51, 12. [Google Scholar] [CrossRef]
- Orsini, A.; Foiadelli, T.; Sica, A.; Santangelo, A.; Carli, N.; Bonuccelli, A.; Consolini, R.; D’elios, S.; Loddo, N.; Verrotti, A.; et al. Psychopathological Impact in Patients with History of Rheumatic Fever with or without Sydenham’s Chorea: A Multicenter Prospective Study. Int. J. Environ. Res. Public Health 2022, 19, 10586. [Google Scholar] [CrossRef] [PubMed]
- Gianella-Borradori, A.; Hirt, A.; Lüthy, A.; Wagner, H.P.; Imbach, P. Haemophilia due to factor VIII inhibitors in a patient suffering from an autoimmune disease: Treatment with intravenous immunoglobulin: A case report. Blut 1984, 48, 403–407. [Google Scholar] [CrossRef]
- Sultan, Y.; Kazatchkine, M.D.; Maisonneuve, P.; Nydegger, U.E. Anti-idiotypic suppression of autoantibodies to factor VIII (antihaemophilic factor) by high-dose intravenous gammaglobulin. Lancet 1984, 2, 765–768. [Google Scholar] [CrossRef] [PubMed]
- Flores, G.; Cunningham-Rundles, C.; Newland, A.C.; Bussel, J.B. Efficacy of intravenous immunoglobulin in the treatment of autoimmune hemolytic anemia: Results in 73 patients. Am. J. Hematol. 1993, 44, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Mathai, S.S.; Bawa, K.S.; Gupta, G.; Mehrishi, R.N. Auto Immune Hemolytic Anaemia in Infancy: Case Report. Med. J. Armed Forces India 1999, 55, 61–62. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hilgartner, M.W.; Bussel, J. Use of intravenous gamma globulin for the treatment of autoimmune neutropenia of childhood and autoimmune hemolytic anemia. Am. J. Med. 1987, 83, 25–29. [Google Scholar] [CrossRef]
- Bussel, J.; Lalezari, P.; Hilgartner, M.; Partin, J.; Fikrig, S.; O’malley, J.; Barandun, S. Reversal of neutropenia with intravenous gammaglobulin in autoimmune neutropenia of infancy. Blood 1983, 62, 398–400. [Google Scholar] [CrossRef]
- Mikhail, D.B.; Zhu, J.; Pradhan, S.M.; Freiberg, A.S. Rate of Rise of Platelet Count After IVIG for Pediatric Immune Thrombocytopenia. J. Pediatr. Hematol. 2022, 44, e672–e676. [Google Scholar] [CrossRef] [PubMed]
- Heitink-Pollé, K.M.J.; Uiterwaal, C.S.P.M.; Porcelijn, L.; Tamminga, R.Y.J.; Smiers, F.J.; van Woerden, N.L.; Wesseling, J.; Vidarsson, G.; Laarhoven, A.G.; de Haas, M.; et al. Intravenous immunoglobulin vs observation in childhood immune thrombocytopenia: A randomized controlled trial. Blood 2018, 132, 883–891. [Google Scholar] [CrossRef]
- Higashide, Y.; Hori, T.; Yoto, Y.; Kabutoya, H.; Honjo, S.; Sakai, Y.; Nojima, M.; Yoda, M.; Yamamoto, M.; Tsutsumi, H. Predictive factors of response to IVIG in pediatric immune thrombocytopenic purpura. Pediatr. Int. 2018, 60, 357–361. [Google Scholar] [CrossRef] [PubMed]
- Ou, C.Y.; Hsieh, K.S.; Chiou, Y.H.; Chang, Y.H.; Ger, L.P. A comparative study of initial use of intravenous immunoglobulin and prednisolone treatments in childhood idiopathic thrombocytopenic purpur. Acta Paediatr. Taiwanica 2006, 47, 226–231. [Google Scholar]
- Gereige, R.S.; Barrios, N.J. Treatment of childhood acute immune thrombocytopenic purpura with high-dose methylprednisolone, intravenous immunoglobulin, or the combination of both. P. R. Health Sci. J. 2000, 19, 15–18. [Google Scholar] [PubMed]
- Fujisawa, K.; Iyori, H.; Ohkawa, H.; Konishi, S.; Bessho, F.; Shirahata, A.; Miyazaki, S.; Akatsuka, J. A prospective, randomized trial of conventional, dose-accelerated corticosteroids and intravenous immunoglobulin in children with newly diagnosed idiopathic thrombocytopenic purpura. Int. J. Hematol. 2000, 72, 376–383. [Google Scholar]
- Rosthøj, S.; Nielsen, S.M.; Pedersen, F.K. Randomized comparison of intravenous immunoglobulin and methylprednisolone pulse therapy in children with newly diagnosed idiopathic thrombocytic purpura. The Danish ITP Study Group. Ugeskr. Laeger 1998, 160, 1640–1644. [Google Scholar]
- Winkelhorst, D.; Oepkes, D.; Lopriore, E. Fetal and neonatal alloimmune thrombocytopenia: Evidence based antenatal and postnatal management strategies. Expert Rev. Hematol. 2017, 10, 729–737. [Google Scholar] [CrossRef]
- Mueller-Eckhardt, C.; Kiefel, V.; Grubert, A. High-dose IgG treatment for neonatal alloimmune thrombocytopenia. Blut 1989, 59, 145–146. [Google Scholar] [CrossRef]
- Ziman, A.; Klapper, E.; Pepkowitz, S.; Smith, R.; Garratty, G.; Goldfinger, D. A second case of post-transfusion purpura caused by HPA-5a antibodies: Successful treatment with intravenous immunoglobulin. Vox Sang. 2002, 83, 165–166. [Google Scholar] [CrossRef]
- Kroll, H.; Kiefel, V.; Mueller-Eckhardt, C. Post-transfusion purpura: Clinical and immunologic studies in 38 patients. Infusionsther. Transfusionsmed. 1993, 20, 198–204. [Google Scholar] [PubMed]
- Mueller-Eckhardt, C.; Kiefel, V. High-dose IgG for post-transfusion purpura-revisited. Blut 1988, 57, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Ding, J.; Baer, M.R.; Hess, J.R.; Zimrin, A.B. Intravenous immunoglobulin as salvage therapy for refractory thrombotic thrombocytopenic purpura. Am. J. Hematol. 2018, 93, E77–E79. [Google Scholar] [CrossRef] [PubMed]
- Centurioni, R.; Bobbio-Pallavicini, E.; Porta, C.; Rodeghiero, F.; Gugliotta, L.; Billio, A.; Tacconi, F.; Ascari, E. Treatment of thrombotic thrombocytopenic purpura with high-dose immunoglobulins. Results in 17 patients. Italian Cooperative Group for TTP. Haematologica 1995, 80, 325–331. [Google Scholar] [PubMed]
- Zhang, X.; Che, R.; Xu, H.; Ding, G.; Zhao, F.; Huang, S.; Zhang, A. Hemoperfusion and intravenous immunoglobulins for refractory gastrointestinal involvement in pediatric Henoch-Schönlein purpura: A single-center retrospective cohort study. BMC Pediatr. 2022, 22, 692. [Google Scholar] [CrossRef] [PubMed]
- Morotti, F.; Bracciolini, G.; Caorsi, R.; Cattaneo, L.; Gattorno, M.; Ravelli, A.; Felici, E. Intravenous immunoglobulin for corticosteroid-resistant intestinal Henoch-Schönlein purpura: Worth a controlled trial against corticosteroids? Rheumatology 2021, 60, 3868–3871. [Google Scholar] [CrossRef] [PubMed]
- Mauro, A.; Mauro, S.; Rega, R.; Martemucci, L.; Sottile, R. Successful treatment of hemorrhagic bullous Henoch-Schonlein purpura with intravenous immunoglobulins. Pediatr. Dermatol. 2019, 36, e34–e36. [Google Scholar] [CrossRef] [PubMed]
- Cherqaoui, B.; Chausset, A.; Stephan, J.L.; Merlin, E. Intravenous immunoglobulins for severe gastrointestinal involvement in pediatric Henoch-Schönlein purpura: A French retrospective study. Arch. Pediatr. 2016, 23, 584–590. [Google Scholar] [CrossRef] [PubMed]
- Fatima, A.; Gibson, D.P. Pneumatosis intestinalis associated with Henoch-Schönlein purpura. Pediatrics 2014, 134, e880–e883. [Google Scholar] [CrossRef]
- de Maddi, F.; Dinardo, R.; Buonocore, M.C.; Dinardo, M.; Bartolomei, B.; Rigante, D. Intravenous immunoglobulin in Henoch-Schönlein purpura complicated by cerebral hemorrhage. Rheumatol. Int. 2013, 33, 2451–2453. [Google Scholar] [CrossRef]
- Fagbemi, A.A.O.; Torrente, F.; Hilson, A.J.W.; Thomson, M.A.; Heuschkel, R.B.; Murch, S.H. Massive gastrointestinal haemorrhage in isolated intestinal Henoch-Schonlein purpura with response to intravenous immunoglobulin infusion. Eur. J. Pediatr. 2007, 166, 915–919. [Google Scholar] [CrossRef] [PubMed]
- Lamireau, T.; Rebouissoux, L.; Hehunstre, J.P. Intravenous immunoglobulin therapy for severe digestive manifestations of Henoch-Schönlein purpura. Acta Paediatr. 2001, 90, 1081–1082. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, R.; Charles-Schoeman, C.; Schessl, J.; Bata-Csörgő, Z.; Dimachkie, M.M.; Griger, Z.; Moiseev, S.; Oddis, C.; Schiopu, E.; Vencovský, J.; et al. Trial of Intravenous Immune Globulin in Dermatomyositis. N. Engl. J. Med. 2022, 387, 1264–1278. [Google Scholar] [CrossRef] [PubMed]
- Lam, C.G.; Manlhiot, C.; Pullenayegum, E.M.; Feldman, B.M. Efficacy of intravenous Ig therapy in juvenile dermatomyositis. Ann. Rheum. Dis. 2011, 70, 2089–2094. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.M.; Bingham, C.A.; Kahn, P.J.; Eichenfield, A.H.; Imundo, L.F. Favorable Outcome of Juvenile Dermatomyositis Treated without Systemic Corticosteroids. J. Pediatr. 2010, 156, 302–307. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Al-Mayouf, S.M.; Laxer, R.M.; Schneider, R.; Silverman, E.D.; Feldman, B.M. Intravenous immunoglobulin therapy for juvenile dermatomyositis: Efficacy and safety. J. Rheumatol. 2000, 27, 2498–2503. [Google Scholar]
- Sansome, A.; Dubowitz, V. Intravenous immunoglobulin in juvenile dermatomyositis—Four year review of nine cases. Arch. Dis. Child. 1995, 72, 25. [Google Scholar] [CrossRef][Green Version]
- Collet, K.; Dalac, S.; Maerens, B.; Courtois, J.; Izac, M.; Lambert, D. Juvenile dermatomyositis: Treatment with intravenous gammaglobulin. Br. J. Dermatol. 1994, 130, 231–234. [Google Scholar] [CrossRef]
- Dalakas, M.C.; Illa, I.; Dambrosia, J.M.; Soueidan, S.A.; Stein, D.P.; Otero, C.; Dinsmore, S.T.; McCrosky, S. A Controlled Trial of High-Dose Intravenous Immune Globulin Infusions as Treatment for Dermatomyositis. N. Engl. J. Med. 1993, 329, 1993–2000. [Google Scholar] [CrossRef]
- Lang, B.A.; Laxer, R.M.; Murphy, G.; Silverman, E.D.; Roifman, C.M. Treatment of dermatomyositis with intravenous gammaglobulin. Am. J. Med. 1991, 91, 169–172. [Google Scholar] [CrossRef]
- Roifman, C.M.; Schaffer, F.M.; Wachsmuth, S.E.; Murphy, G.; Gelfand, E.W. Reversal of Chronic Polymyositis Following Intravenous Immune Serum Globulin Therapy. JAMA 1987, 258, 513–515. [Google Scholar] [CrossRef] [PubMed]
- Broderick, C.; Kobayashi, S.; Suto, M.; Ito, S.; Kobayashi, T. Intravenous immunoglobulin for the treatment of Kawasaki disease. Cochrane Database Syst. Rev. 2023, 2023, CD014884. [Google Scholar] [CrossRef]
- Lei, W.-T.; Chang, L.-S.; Zeng, B.-Y.; Tu, Y.-K.; Uehara, R.; Matsuoka, Y.J.; Su, K.-P.; Lee, P.-C.; Cavalcante, J.L.; Stubbs, B.; et al. Pharmacologic interventions for Kawasaki disease in children: A network meta-analysis of 56 randomized controlled trials. eBioMedicine 2022, 78, 103946. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Jiang, J.; Shi, X.; Qin, J.; Dong, J.; Xu, L.; Huang, C.; Liu, Y.; Zheng, Y.; Hou, M.; et al. Nomogram to predict risk of resistance to intravenous immunoglobulin in children hospitalized with Kawasaki disease in Eastern China. Ann. Med. 2022, 54, 442–453. [Google Scholar] [CrossRef] [PubMed]
- Hamada, H.; Suzuki, H.; Onouchi, Y.; Ebata, R.; Terai, M.; Fuse, S.; Okajima, Y.; Kurotobi, S.; Hirai, K.; Soga, T.; et al. Efficacy of primary treatment with immunoglobulin plus ciclosporin for prevention of coronary artery abnormalities in patients with Kawasaki disease predicted to be at increased risk of non-response to intravenous immunoglobulin (KAICA): A randomised controlled, open-label, blinded-endpoints, phase 3 trial. Lancet 2019, 393, 1128–1137. [Google Scholar] [CrossRef] [PubMed]
- Dionne, A.; Le, C.-K.; Poupart, S.; Autmizguine, J.; Meloche-Dumas, L.; Turgeon, J.; Fournier, A.; Dahdah, N. Profile of resistance to IVIG treatment in patients with Kawasaki disease and concomitant infection. PLoS ONE 2018, 13, e0206001. [Google Scholar] [CrossRef] [PubMed]
- Akca, U.K.; Aydin, E.A.; Aykan, H.H.; Serin, O.; Sag, E.; Demir, S.; Atalay, E.; Kasap, M.; Batu, E.D.; Karagoz, T.; et al. Comparison of IVIG resistance predictive models in Kawasaki disease. Pediatr. Res. 2022, 91, 621–626. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.T.; Sun, L.C.; Wu, E.T.; Wang, J.K.; Lue, H.C.; Wu, M.H. Acute and late coronary outcomes in 1073 patients with Kawasaki disease with and without intravenous γ-immunoglobulin therapy. Arch. Dis. Child. 2015, 100, 542–547. [Google Scholar] [CrossRef]
- Newburger, J.W.; Takahashi, M.; Burns, J.C.; Beiser, A.S.; Chung, K.J.; Duffy, C.E.; Glode, M.P.; Mason, W.H.; Reddy, V.; Sanders, S.P.; et al. The treatment of Kawasaki syndrome with intravenous gamma globulin. N. Engl. J. Med. 1986, 315, 341–347. [Google Scholar] [CrossRef]
- Furusho, K.; Sato, K.; Soeda, T.; Matsumoto, H.; Okabe, T.; Hirota, T.; Kawada, S. High-dose intravenous gammaglobulin for kawasaki disease. Lancet 1983, 322, 1359. [Google Scholar] [CrossRef]
- Mahmoud, S.; El-Kalliny, M.; Kotby, A.; El-Ganzoury, M.; Fouda, E.; Ibrahim, H. Treatment of MIS-C in Children and Adolescents. Curr. Pediatr. Rep. 2022, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Son, M.B.F.; Murray, N.; Friedman, K.; Young, C.C.; Newhams, M.M.; Feldstein, L.R.; Loftis, L.L.; Tarquinio, K.M.; Singh, A.R.; Heidemann, S.M.; et al. Multisystem Inflammatory Syndrome in Children—Initial Therapy and Outcomes. N. Engl. J. Med. 2021, 385, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Ouldali, N.; Toubiana, J.; Antona, D.; Javouhey, E.; Madhi, F.; Lorrot, M.; Léger, P.-L.; Galeotti, C.; Claude, C.; Wiedemann, A.; et al. Association of Intravenous Immunoglobulins Plus Methylprednisolone vs Immunoglobulins Alone with Course of Fever in Multisystem Inflammatory Syndrome in Children. JAMA 2021, 325, 855. [Google Scholar] [CrossRef] [PubMed]
- Belhadjer, Z.; Auriau, J.; Méot, M.; Oualha, M.; Renolleau, S.; Houyel, L.; Bonnet, D. Addition of Corticosteroids to Immunoglobulins Is Associated with Recovery of Cardiac Function in Multi-Inflammatory Syndrome in Children. Circulation 2020, 142, 2282–2284. [Google Scholar] [CrossRef] [PubMed]
- Giannini, E.H.; Lovell, D.J.; Silverman, E.D.; Sundel, R.P.; Tague, B.L.; Ruperto, N. Intravenous immunoglobulin in the treatment of polyarticular juvenile rheumatoid arthritis: A phase I/II study. Pediatric Rheumatology Collaborative Study Group. J. Rheumatol. 1996, 23, 919–924. [Google Scholar] [PubMed]
- Uziel, Y.; Laxer, R.M.; Schneider, R.; Silverman, E.D. Intravenous immunoglobulin therapy in systemic onset juvenile rheumatoid arthritis: A followup study. J. Rheumatol. 1996, 23, 910–918. [Google Scholar] [PubMed]
- Silverman, E.D.; Cawkwell, G.D.; Lovell, D.J.; Laxer, R.M.; Lehman, T.J.; Passo, M.H.; Zemel, L.S.; Giannini, E.H. Intravenous immunoglobulin in the treatment of systemic juvenile rheumatoid arthritis: A randomized placebo controlled trial. Pediatric Rheumatology Collaborative Study Group. J. Rheumatol. 1994, 21, 2353–2358. [Google Scholar] [PubMed]
- Silverman, E.D.; Laxer, R.M.; Greenwald, M.; Gelfand, E.; Shore, A.; Stein, L.D.; Roifman, C.M. Intravenous gamma globulin therapy in systemic juvenile rheumatoid arthritis. Arthritis Rheum. 1990, 33, 1015–1022. [Google Scholar] [CrossRef]
- Prieur, A.M.; Adleff, A.; Debre, M.; Boulate, P.; Griscelli, C. High dose immunoglobulin therapy in severe juvenile chronic arthritis: Long-term follow-up in 16 patients. Clin. Exp. Rheumatol. 1990, 8, 603–608. [Google Scholar]
- Shi, N.; Wang, X.; Zou, L.; Yang, X.; Ma, Q.; Lu, M. Case Report: Macrophage Activation Syndrome and Widespread Neuroimaging Abnormality in Childhood-Onset Systemic Lupus Erythematosus. Front. Pediatr. 2021, 9, 767115. [Google Scholar] [CrossRef]
- Akca, Ü.K.; Batu, E.D.; Kısaarslan, A.P.; Poyrazoğlu, H.; Ayaz, N.A.; Sözeri, B.; Sağ, E.; Atalay, E.; Demir, S.; Karadağ, Ş.G.; et al. Hematological involvement in pediatric systemic lupus erythematosus: A multi-center study. Lupus 2021, 30, 1983–1990. [Google Scholar] [CrossRef] [PubMed]
- Baglan, E.; Ozdel, S.; Yazıcı, M.U.; Azapağası, E.; Çelik, H.; Yüksel, D.; Uçan, B.; Karakaya, D.; Bulbul, M. A novel therapeutic approach using the Zipper method to treat chorea in a pediatric-onset systemic lupus erythematosus patient. Lupus 2021, 30, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Lube, G.E.; Ferriani, M.P.L.; Campos, L.M.A.; Terreri, M.T.; Bonfá, E.; Magalhães, C.S.; Aikawa, N.E.; Piotto, D.P.; Peracchi, O.A.B.; dos Santos, M.C.; et al. Evans Syndrome at Childhood-Onset Systemic Lupus Erythematosus Diagnosis: A Large Multicenter Study. Pediatr. Blood Cancer 2016, 63, 1238–1243. [Google Scholar] [CrossRef]
- Brogna, C.; Manna, R.; Contaldo, I.; Romeo, D.M.; Stefanini, M.C.; Chiaretti, A.; Mercuri, E.; Mariotti, P. Intravenous immunoglobulin for Pediatric Neuropsychiatric Lupus Triggered by Epstein-Barr Virus Cerebral Infection. Isr. Med. Assoc. J. 2016, 18, 763–766. [Google Scholar] [PubMed]
- Friedman, D.M.; Llanos, C.; Izmirly, P.M.; Brock, B.; Byron, J.; Copel, J.; Cummiskey, K.; Dooley, M.A.; Foley, J.; Graves, C.; et al. Evaluation of fetuses in a study of intravenous immunoglobulin as preventive therapy for congenital heart block: Results of a multicenter, prospective, open-label clinical trial. Arthritis Rheum. 2010, 62, 1138–1146. [Google Scholar] [CrossRef] [PubMed]
- Pisoni, C.N.; Brucato, A.; Ruffatti, A.; Espinosa, G.; Cervera, R.; Belmonte-Serrano, M.; Sánchez-Román, J.; García-Hernández, F.G.; Tincani, A.; Bertero, M.T.; et al. Failure of intravenous immunoglobulin to prevent congenital heart block: Findings of a multicenter, prospective, observational study. Arthritis Rheum. 2010, 62, 1147–1152. [Google Scholar] [CrossRef] [PubMed]
- Miyagawa, S.; Nakajima, M.; Nishio, K.; Sogami, J.; Tsubakimoto, A.; Yoshioka, A.; Shirai, T. Guillain-Barre syndrome in a child with systemic lupus erythematosus and anti-Ro/SSA and anti-La/SSB autoantibodies. Br. J. Dermatol. 2000, 143, 1050–1054. [Google Scholar] [CrossRef]
- Nosadini, M.; Mohammad, S.S.; Suppiej, A.; Sartori, S.; Dale, R.C. Intravenous immunoglobulin in paediatric neurology: Safety, adherence to guidelines, and long-term outcome. Dev. Med. Child Neurol. 2016, 58, 1180–1192. [Google Scholar] [CrossRef]
- Schafflick, D.; Kieseier, B.C.; Wiendl, H.; Meyer zu Horste, G. Novel pathomechanisms in inflammatory neuropathies. J. Neuroinflamm. 2017, 14, 232. [Google Scholar] [CrossRef]
- Querol, L.; Lleixà, C. Novel Immunological and Therapeutic Insights in Guillain-Barré Syndrome and CIDP. Neurotherapeutics 2021, 18, 2222–2235. [Google Scholar] [CrossRef]
- Korinthenberg, R.; Trollmann, R.; Felderhoff-Müser, U.; Bernert, G.; Hackenberg, A.; Hufnagel, M.; Pohl, M.; Hahn, G.; Mentzel, H.; Sommer, C.; et al. Diagnosis and treatment of Guillain-Barré Syndrome in childhood and adolescence: An evidence- and consensus-based guideline. Eur. J. Paediatr. Neurol. 2020, 25, 5–16. [Google Scholar] [CrossRef] [PubMed]
- Maeda, H.; Ishii, R.; Kusunoki, S.; Chiyonobu, T. Childhood-onset multifocal motor neuropathy with IgM antibodies to GM2 and GalNac-GD1a. Brain Dev. 2020, 42, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Dalakas, M.C. Update on Intravenous Immunoglobulin in Neurology: Modulating Neuro-autoimmunity, Evolving Factors on Efficacy and Dosing and Challenges on Stopping Chronic IVIg Therapy. Neurotherapeutics 2021, 18, 2397–2418. [Google Scholar] [CrossRef]
- Lünemann, J.D.; Quast, I.; Dalakas, M.C. Efficacy of Intravenous Immunoglobulin in Neurological Diseases. Neurotherapeutics 2015, 13, 34–46. [Google Scholar] [CrossRef] [PubMed]
- Korinthenberg, R.; Schessl, J.; Kirschner, J.; Mönting, J.S. Intravenously administered immunoglobulin in the treatment of childhood Guillain-Barré syndrome: A randomized trial. Pediatrics 2005, 116, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Kanra, G.; Ozon, A.; Vajsar, J.; Castagna, L.; Secmeer, G.; Topaloglu, H. Intravenous immunoglobulin treatment in children with Guillain-Barré syndrome. Eur. J. Paediatr. Neurol. 1997, 1, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Hughes, R. The role of IVIg in autoimmune neuropathies: The latest evidence. J. Neurol. 2008, 255, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Ram, D.; Aziz, M. G99(P) IVIG for Guillain-Barré syndrome: Which regimen should I choose? Arch. Dis. Child. 2016, 101 (Suppl. 1), A57. [Google Scholar] [CrossRef]
- Ramdas, S.; Della Marina, A.; Ryan, M.M.; McWilliam, K.; Klein, A.; Jacquier, D.; Alabaf, S.; Childs, A.-M.; Parasuraman, D.; Beeson, D.; et al. Rituximab in juvenile myasthenia gravis-an international cohort study and literature review. Eur. J. Paediatr. Neurol. 2022, 40, 5–10. [Google Scholar] [CrossRef]
- Liew, W.K.M.; Kang, P.B. Update on juvenile myasthenia gravis. Curr. Opin. Pediatr. 2013, 25, 694–700. [Google Scholar] [CrossRef]
- Dalmau, J.; Graus, F. Antibody-Mediated Encephalitis. N. Engl. J. Med. 2018, 378, 840–851. [Google Scholar] [CrossRef] [PubMed]
- Armangue, T.; Petit-Pedrol, M.; Dalmau, J. Autoimmune Encephalitis in Children. J. Child Neurol. 2012, 27, 1460–1469. [Google Scholar] [CrossRef] [PubMed]
- Cellucci, T.; Van Mater, H.; Graus, F.; Muscal, E.; Gallentine, W.; Klein-Gitelman, M.S.; Benseler, S.M.; Frankovich, J.; Gorman, M.P.; Van Haren, K.; et al. Clinical approach to the diagnosis of autoimmune encephalitis in the pediatric patient. Neurol.-Neuroimmunol. Neuroinflamm. 2020, 7, e663. [Google Scholar] [CrossRef] [PubMed]
- Rossor, T.; Yeh, E.A.; Khakoo, Y.; Angelini, P.; Hemingway, C.; Irani, S.R.; Schleiermacher, G.; Santosh, P.; Lotze, T.; Dale, R.C.; et al. Diagnosis and Management of Opsoclonus-Myoclonus-Ataxia Syndrome in Children: An International Perspective. Neurol.-Neuroimmunol. Neuroinflamm. 2022, 9, e1153. [Google Scholar] [CrossRef] [PubMed]
- Armangué, T.; Sabater, L.; Torres-Vega, E.; Martínez-Hernández, E.; Ariño, H.; Petit-Pedrol, M.; Planagumà, J.; Bataller, L.; Dalmau, J.; Graus, F. Clinical and immunological features of opsoclonus-myoclonus syndrome in the era of neuronal cell surface antibodies. JAMA Neurol. 2016, 73, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Nosadini, M.; Mohammad, S.S.; Ramanathan, S.; Brilot, F.; Dale, R.C. Immune therapy in autoimmune encephalitis: A systematic review. Expert Rev. Neurother. 2015, 15, 1391–1419. [Google Scholar] [CrossRef] [PubMed]
- Nosadini, M.; Thomas, T.; Eyre, M.; Anlar, B.; Armangue, T.; Benseler, S.M.; Cellucci, T.; Deiva, K.; Gallentine, W.; Gombolay, G.; et al. International Consensus Recommendations for the Treatment of Pediatric NMDAR Antibody Encephalitis. Neurol.-Neuroimmunol. Neuroinflamm. 2021, 8, e1052. [Google Scholar] [CrossRef] [PubMed]
- Rossor, T.; Benetou, C.; Wright, S.; Duignan, S.; Lascelles, K.; Robinson, R.; Das, K.; Ciccarelli, O.; Wassmer, E.; Hemingway, C.; et al. Early predictors of epilepsy and subsequent relapse in children with acute disseminated encephalomyelitis. Mult. Scler. J. 2020, 26, 333–342. [Google Scholar] [CrossRef]
- Santoro, J.D.; Chitnis, T. Diagnostic Considerations in Acute Disseminated Encephalomyelitis and the Interface with MOG Antibody. Neuropediatrics 2019, 50, 273–279. [Google Scholar] [CrossRef]
- Krupp, L.B.; Tardieu, M.; Amato, M.P.; Banwell, B.; Chitnis, T.; Dale, R.C.; Ghezzi, A.; Hintzen, R.; Kornberg, A.; Pohl, D.; et al. International Pediatric Multiple Sclerosis Study Group criteria for pediatric multiple sclerosis and immune-mediated central nervous system demyelinating disorders: Revisions to the 2007 definitions. Mult. Scler. J. 2013, 19, 1261–1267. [Google Scholar] [CrossRef]
- Baumann, M.; Bartels, F.; Finke, C.; Adamsbaum, C.; Hacohen, Y.; Rostásy, K.; E.U. Paediatric Mog Consortium; Bruijstens, A.L.; Wendel, E.-M.; Lechner, C.; et al. E.U. paediatric MOG consortium consensus: Part 2—Neuroimaging features of paediatric myelin oligodendrocyte glycoprotein antibody-associated disorders. Eur. J. Paediatr. Neurol. 2020, 29, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Massa, S.; Fracchiolla, A.; Neglia, C.; Argentiero, A.; Esposito, S. Update on Acute Disseminated Encephalomyelitis in Children and Adolescents. Children 2021, 8, 280. [Google Scholar] [CrossRef] [PubMed]
- Pohl, D.; Alper, G.; Van Haren, K.; Kornberg, A.J.; Lucchinetti, C.F.; Tenembaum, S.; Belman, A.L. Acute disseminated encephalomyelitis. Neurology 2016, 87 (Suppl. 2), S38–S45. [Google Scholar] [CrossRef] [PubMed]
- Wingerchuk, D.M.; Banwell, B.; Bennett, J.L.; Cabre, P.; Carroll, W.; Chitnis, T.; De Seze, J.; Fujihara, K.; Greenberg, B.; Jacob, A.; et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology 2015, 85, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Banwell, B.; Fadda, G.; Armangue, T.; Hacohen, Y.; Chitnis, T. Paediatric Multiple Sclerosis and Antibody-Associated Demyelination: Clinical, Imaging, and Biological Considerations for Diagnosis and Care. Lancet Neurol. 2021, 20, 136–149. [Google Scholar]
- Magraner, M.J.; Coret, F.; Casanova, B. The effect of intravenous immunoglobulin on neuromyelitis optica. Neurologia 2013, 28, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Elsone, L.; Panicker, J.; Mutch, K.; Boggild, M.; Appleton, R.; Jacob, A. Role of intravenous immunoglobulin in the treatment of acute relapses of neuromyelitis optica: Experience in 10 patients. Mult. Scler. J. 2013, 20, 501–504. [Google Scholar] [CrossRef]
- Pena, J.A.; Lotze, T.E. Pediatric Multiple Sclerosis: Current Concepts and Consensus Definitions. Autoimmune Dis. 2013, 2013, 673947. [Google Scholar] [CrossRef]
- Jancic, J.; Nikolic, B.; Ivancevic, N.; Djuric, V.; Zaletel, I.; Stevanovic, D.; Peric, S.; Anker, J.N.V.D.; Samardzic, J. Multiple Sclerosis in Pediatrics: Current Concepts and Treatment Options. Neurol. Ther. 2016, 5, 131. [Google Scholar] [CrossRef]
- Armangue, T.; Olivé-Cirera, G.; Martínez-Hernandez, E.; Sepulveda, M.; Ruiz-Garcia, R.; Muñoz-Batista, M.; Ariño, H.; González-Álvarez, V.; Felipe-Rucián, A.; Martínez-González, M.J.; et al. Associations of paediatric demyelinating and encephalitic syndromes with myelin oligodendrocyte glycoprotein antibodies: A multicentre observational study. Lancet Neurol. 2020, 19, 234–246. [Google Scholar] [CrossRef]
- Bruijstens, A.L.; Lechner, C.; Flet-Berliac, L.; Deiva, K.; Neuteboom, R.F.; Hemingway, C.; Wassmer, E.; Wendel, E.M.; Breu, M.; de Chalus, A.; et al. paediatric MOG consortium consensus: Part 1—Classification of clinical phenotypes of paediatric myelin oligodendrocyte glycoprotein antibody-associated disorders. Eur. J. Paediatr. Neurol. 2020, 29, 2–13. [Google Scholar] [CrossRef] [PubMed]
- Nosadini, M.; Eyre, M.; Giacomini, T.; Valeriani, M.; Della Corte, M.; Praticò, A.D.; Annovazzi, P.; Cordani, R.; Cordelli, D.M.; Crichiutti, G.; et al. Early Immunotherapy and Longer Corticosteroid Treatment Are Associated with Lower Risk of Relapsing Disease Course in Pediatric MOGAD. Neurol.-Neuroimmunol. Neuroinflamm. 2023, 10, e200065. [Google Scholar] [CrossRef] [PubMed]
- Bruijstens, A.L.; Wendel, E.-M.; Lechner, C.; Bartels, F.; Finke, C.; Breu, M.; Flet-Berliac, L.; de Chalus, A.; Adamsbaum, C.; Capobianco, M.; et al. E.U. paediatric MOG consortium consensus: Part 5—Treatment of paediatric myelin oligodendrocyte glycoprotein antibody-associated disorders. Eur. J. Paediatr. Neurol. 2020, 29, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Varadkar, S.; Bien, C.G.; Kruse, C.A.; Jensen, F.E.; Bauer, J.; Pardo, C.A.; Vincent, A.; Mathern, G.W.; Cross, J.H. Rasmussen’s encephalitis: Clinical features, pathobiology, and treatment advances. Lancet Neurol. 2014, 13, 195–205. [Google Scholar] [CrossRef] [PubMed]
- Bien, C.G.; Tiemeier, H.; Sassen, R.; Kuczaty, S.; Urbach, H.; von Lehe, M.; Becker, A.J.; Bast, T.; Herkenrath, P.; Karenfort, M.; et al. Rasmussen encephalitis: Incidence and course under randomized therapy with tacrolimus or intravenous immunoglobulins. Epilepsia 2013, 54, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Ramesha, K.; Rajesh, B.; Ashalatha, R.; Kesavadas, C.; Abraham, M.; Radhakrishnan, V.; Sarma, P.; Radhakrishnan, K. Rasmussen’s encephalitis: Experience from a developing country based on a group of medically and surgically treated patients. Seizure 2009, 18, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Granata, T.; Fusco, L.; Gobbi, G.; Freri, E.; Ragona, F.; Broggi, G.; Mantegazza, R.; Giordano, L.; Villani, F.; Capovilla, G.; et al. Experience with immunomodulatory treatments in Rasmussen’s encephalitis. Neurology 2003, 61, 1807–1810. [Google Scholar] [CrossRef] [PubMed]
- Specchio, N.; Pietrafusa, N. New-onset refractory status epilepticus and febrile infection-related epilepsy syndrome. Dev. Med. Child Neurol. 2020, 62, 897–905. [Google Scholar] [CrossRef]
- Hirsch, L.J.; Gaspard, N.; van Baalen, A.; Nabbout, R.; Demeret, S.; Loddenkemper, T.; Navarro, V.; Specchio, N.; Lagae, L.; Rossetti, A.O.; et al. Proposed consensus definitions for new-onset refractory status epilepticus (NORSE), febrile infection-related epilepsy syndrome (FIRES), and related conditions. Epilepsia 2018, 59, 739–744. [Google Scholar] [CrossRef]
- Gofshteyn, J.S.; Wilfong, A.; Devinsky, O.; Bluvstein, J.; Charuta, J.; Ciliberto, M.A.; Laux, L.; Marsh, E.D. Cannabidiol as a Potential Treatment for Febrile Infection-Related Epilepsy Syndrome (FIRES) in the Acute and Chronic Phases. J. Child Neurol. 2017, 32, 35–40. [Google Scholar] [CrossRef]
- Specchio, N.; Fusco, L.; Claps, D.; Vigevano, F. Epileptic encephalopathy in children possibly related to immune-mediated pathogenesis. Brain Dev. 2010, 32, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Frankovich, J.; Swedo, S.; Murphy, T.; Dale, R.C.; Agalliu, D.; Williams, K.; Daines, M.; Hornig, M.; Chugani, H.; Sanger, T.; et al. Clinical Management of Pediatric Acute-Onset Neuropsychiatric Syndrome: Part II—Use of Immunomodulatory Therapies. J. Child Adolesc. Psychopharmacol. 2017, 27, 574–593. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.; Frankovich, J.; Cunningham, M.W.; Latimer, M.E.; Murphy, T.K.; Thienemann, M.; Williams, K.; Walter, J.; Swedo, S.E. Clinical Evaluation of Youth with Pediatric Acute-Onset Neuropsychiatric Syndrome (PANS): Recommendations from the 2013 PANS Consensus Conference. J. Child Adolesc. Psychopharmacol. 2015, 25, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Kühne, T. Diagnosis and management of immune thrombocytopenia in childhood. Hamostaseologie 2017, 37, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Provan, D.; Arnold, D.M.; Bussel, J.B.; Chong, B.H.; Cooper, N.; Gernsheimer, T.; Ghanima, W.; Godeau, B.; González-López, T.J.; Grainger, J.; et al. Updated international consensus report on the investigation and management of primary immune thrombocytopenia. Blood Adv. 2019, 3, 3780–3817. [Google Scholar] [CrossRef] [PubMed]
- Papagianni, A.; Economou, M.; Tragiannidis, A.; Karatza, E.; Tsatra, I.; Gombakis, N.; Athanassiadou-Piperopoulou, F.; Athanasiou-Metaxa, M. Standard-dose intravenous anti-D immunoglobulin versus intravenous immunoglobulin in the treatment of newly diagnosed childhood primary immune thrombocytopenia. J. Pediatr. Hematol. Oncol. 2011, 33, 265–269. [Google Scholar] [CrossRef]
- Neunert, C.; Terrell, D.R.; Arnold, D.M.; Buchanan, G.; Cines, D.B.; Cooper, N.; Cuker, A.; Despotovic, J.M.; George, J.N.; Grace, R.F.; et al. American Society of Hematology 2019 guidelines for immune thrombocytopenia. Blood Adv. 2019, 3, 3829–3866. [Google Scholar] [CrossRef]
- Carcao, M.; Silva, M.; David, M.; Klaassen, R.J.; Steele, M.; Price, V.; Wakefield, C.; Kim, L.; Stephens, D.; Blanchette, V.S. IVMP+IVIG raises platelet counts faster than IVIG alone: Results of a randomized, blinded trial in childhood ITP. Blood Adv. 2020, 4, 1492–1500. [Google Scholar] [CrossRef]
- Aladjidi, N.; Jutand, M.; Beaubois, C.; Fernandes, H.; Jeanpetit, J.; Coureau, G.; Gilleron, V.; Kostrzewa, A.; Lauroua, P.; Jeanne, M.; et al. Reliable assessment of the incidence of childhood autoimmune hemolytic anemia. Pediatr. Blood Cancer 2017, 64, e26683. [Google Scholar] [CrossRef]
- Voulgaridou, A.; Kalfa, T.A. Autoimmune hemolytic anemia in the pediatric setting. J. Clin. Med. 2021, 10, 216. [Google Scholar] [CrossRef]
- Zanella, A.; Barcellini, W. Treatment of autoimmune hemolytic anemias. Haematologica 2014, 99, 1547–1554. [Google Scholar] [CrossRef] [PubMed]
- Zeerleder, S. Autoimmune haemolytic anaemia—A practical guide to cope with a diagnostic and therapeutic challenge. Neth. J. Med. 2011, 69, 177–184. [Google Scholar] [PubMed]
- Fan, J.; He, H.; Zhao, W.; Wang, Y.; Lu, J.; Li, J.; Li, J.; Xiao, P.; Lu, Y.; Chai, Y.; et al. Clinical Features and Treatment Outcomes of Childhood Autoimmune Hemolytic Anemia: A Retrospective Analysis of 68 Cases. J. Pediatr. Hematol. 2016, 38, e50–e55. [Google Scholar] [CrossRef] [PubMed]
- Afzal, W.; Owlia, M.B.; Hasni, S.; Newman, K.A. Autoimmune Neutropenia Updates: Etiology, Pathology, and Treatment. South Med. J. 2017, 110, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Charlebois, J.; Rivard, G.É.; St-Louis, J. Management of acquired hemophilia A: Review of current evidence. Transfus. Apher. Sci. 2018, 57, 717–720. [Google Scholar] [CrossRef] [PubMed]
- Kruse-Jarres, R.; Kempton, C.L.; Baudo, F.; Collins, P.W.; Knoebl, P.; Leissinger, C.A.; Tiede, A.; Kessler, C.M. Acquired hemophilia A: Updated review of evidence and treatment guidance. Am. J. Hematol. 2017, 92, 695–705. [Google Scholar] [CrossRef] [PubMed]
- Collins, P.; Baudo, F.; Knoebl, P.; Lévesque, H.; Nemes, L.; Pellegrini, F.; Marco, P.; Tengborn, L.; Huth-Kühne, A. Immunosuppression for acquired hemophilia A: Results from the European Acquired Haemophilia Registry (EACH2). Blood 2012, 120, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Bussel, J.B.; Vander Haar, E.L.; Berkowitz, R.L. New developments in fetal and neonatal alloimmune thrombocytopenia. Am. J. Obstet. Gynecol. 2021, 225, 120–127. [Google Scholar] [CrossRef]
- Lieberman, L.; Greinacher, A.; Murphy, M.F.; Bussel, J.; Bakchoul, T.; Corke, S.; Kjaer, M.; Kjeldsen-Kragh, J.; Bertrand, G.; Oepkes, D.; et al. Fetal and neonatal alloimmune thrombocytopenia: Recommendations for evidence-based practice, an international approach. Br. J. Haematol. 2019, 185, 549–562. [Google Scholar] [CrossRef]
- Ouwehand, W.H.; Smith, G.; Ranasinghe, E. Management of severe alloimmune thrombocytopenia in the newborn. Arch. Dis. Child.-Fetal Neonatal Ed. 2000, 82, 173F–175F. [Google Scholar] [CrossRef]
- de Kruijff, E.; van Gammeren, A.J.; Porcelijn, L.; van Esser, J.W.J. Post-transfusion purpura in a woman with acute myeloid leukemia. Neth. J. Med. 2019, 77, 81–83. [Google Scholar] [PubMed]
- Hamblin, T.J.; Abidi, S.M.N.; Nee, P.A.; Copplestone, A.; Mufti, G.J.; Oscier, D.G. Successful Treatment of Post-Transfusion Purpura with High Dose Immunoglobulins after Lack of Response to Plasma Exchange. Vox Sang. 1985, 49, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Joly, B.S.; Coppo, P.; Veyradier, A. Pediatric thrombotic thrombocytopenic purpura. Eur. J. Haematol. 2018, 101, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Joly, B.S.; Coppo, P.; Veyradier, A. An update on pathogenesis and diagnosis of thrombotic thrombocytopenic purpura. Expert Rev. Hematol. 2019, 12, 383–395. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.C.; Arnold, D.M.; Leber, B.F.; Clare, R.; Molnar, G.J.; Kelton, J.G. Intravenous immunoglobulin as an adjunct to plasma exchange for the treatment of chronic thrombotic thrombocytopenic purpura. Vox Sang. 2007, 93, 173–175. [Google Scholar] [CrossRef] [PubMed]
- Lovell, D.J.; Ruperto, N.; Giannini, E.H.; Martini, A. Advances from clinical trials in juvenile idiopathic arthritis. Nat. Rev. Rheumatol. 2013, 9, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Onel, K.B.; Horton, D.B.; Lovell, D.J.; Shenoi, S.; Cuello, C.A.; Angeles-Han, S.T.; Becker, M.L.; Cron, R.Q.; Feldman, B.M.; Ferguson, P.J.; et al. 2021 American College of Rheumatology Guideline for the Treatment of Juvenile Idiopathic Arthritis: Therapeutic Approaches for Oligoarthritis, Temporomandibular Joint Arthritis, and Systemic Juvenile Idiopathic Arthritis. Arthritis Rheumatol. 2022, 74, 553–569. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.J.Y.; Schneider, R. Systemic Juvenile Idiopathic Arthritis. Pediatr. Clin. N. Am. 2018, 65, 691–709. [Google Scholar] [CrossRef]
- Bayry, J.; Negi, V.S.; Kaveri, S.V. Intravenous immunoglobulin therapy in rheumatic diseases. Nat. Rev. Rheumatol. 2011, 7, 349–359. [Google Scholar] [CrossRef]
- Feldman, B.M.; Rider, L.G.; Reed, A.M.; Pachman, L.M. Juvenile dermatomyositis and other idiopathic inflammatory myopathies of childhood. Lancet 2008, 371, 2201–2212. [Google Scholar] [CrossRef]
- Kobayashi, I.; Akioka, S.; Kobayashi, N.; Iwata, N.; Takezaki, S.; Nakaseko, H.; Sato, S.; Nishida, Y.; Nozawa, T.; Yamasaki, Y.; et al. Clinical practice guidance for juvenile dermatomyositis (JDM) 2018-Update. Mod. Rheumatol. 2020, 30, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Enders, F.B.; Bader-Meunier, B.; Baildam, E.; Constantin, T.; Dolezalova, P.; Feldman, B.M.; Lahdenne, P.; Magnusson, B.; Nistala, K.; Ozen, S.; et al. Consensus-based recommendations for the management of juvenile dermatomyositis. Ann. Rheum. Dis. 2017, 76, 329–340. [Google Scholar] [CrossRef] [PubMed]
- Waldman, R.; DeWane, M.E.; Lu, J. Dermatomyositis: Diagnosis and treatment. J. Am. Acad. Dermatol. 2020, 82, 283–296. [Google Scholar] [CrossRef] [PubMed]
- Zandman-Goddard, G.; Levy, Y.; Shoenfeld, Y. Intravenous Immunoglobulin Therapy and Systemic Lupus Erythematosus. Clin. Rev. Allergy Immunol. 2005, 29, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, M.M.; Wagner-Weiner, L. Intravenous Immunoglobulin in Pediatric Rheumatology: When to Use It and What Is the Evidence. Pediatr. Ann. 2017, 46, e19–e24. [Google Scholar] [CrossRef] [PubMed]
- Santos, F.P.S.T.; Nascimento, B.R.; Calderaro, D.C.; Ferreira, G.A.; Correa, H. Neuropsychiatric Syndromes in Childhood-Onset Systemic Lupus Erythematosus: A Systematic Review and Meta-analysis. J. Clin. Rheumatol. 2021, 27, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Brogna, C.; Mariotti, P.; Manna, R. Conventional and intravenous immunoglobulin therapy in paediatric antiphospholipid antibodies-related chorea. Lupus 2014, 23, 1449–1451. [Google Scholar] [CrossRef]
- Papachristos, D.A.; Oon, S.; Hanly, J.G.; Nikpour, M. Management of inflammatory neurologic and psychiatric manifestations of systemic lupus erythematosus: A systematic review. Semin. Arthritis Rheum. 2021, 51, 49–71. [Google Scholar] [CrossRef]
- Oni, L.; Sampath, S. Childhood IgA vasculitis (Henoch Schonlein Purpura)-advances and knowledge gaps. Front. Pediatr. 2019, 7, 257. [Google Scholar] [CrossRef]
- Rostoker, G.; Desvaux-Belghiti, D.; Pilatte, Y.; Petit-Phar, M.; Philippon, C.; Deforges, L.; Terzidis, H.; Intrator, L.; Andre, C.; Adnot, S.; et al. High-dose immunoglobulin therapy for severe IgA nephropathy and Henoch- Schonlein purpura. Ann. Intern. Med. 1994, 120, 476–484. [Google Scholar] [CrossRef]
- Hahn, D.; Hodson, E.M.; Craig, J.C. Interventions for preventing and treating kidney disease in IgA vasculitis. Cochrane Database Syst. Rev. 2023, 2023, CD005128. [Google Scholar] [CrossRef]
- Nothhaft, M.; Klepper, J.; Kneitz, H.; Meyer, T.; Hamm, H.; Morbach, H. Hemorrhagic Bullous Henoch-Schönlein Purpura: Case Report and Review of the Literature. Front. Pediatr. 2019, 6, 413. [Google Scholar] [CrossRef] [PubMed]
- McCrindle, B.W.; Rowley, A.H.; Newburger, J.W.; Burns, J.C.; Bolger, A.F.; Gewitz, M.; Baker, A.L.; Jackson, M.A.; Takahashi, M.; Shah, P.B.; et al. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals from the American Heart Association. Circulation 2017, 135, e927–e999. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.; Yang, H.W.; Lin, T.Y.; Yang, K.D. Perspective of Immunopathogenesis and Immunotherapies for Kawasaki Disease. Front. Pediatr. 2021, 9, 697632. [Google Scholar] [CrossRef]
- Wang, N.; Chen, Z.; Zhang, F.; Zhang, Q.; Sun, L.; Lv, H.; Wang, B.; Shen, J.; Zhou, X.; Chen, F.; et al. Intravenous Immunoglobulin Therapy Restores the Quantity and Phenotype of Circulating Dendritic Cells and CD4+ T Cells in Children with Acute Kawasaki Disease. Front. Immunol. 2022, 13, 802690. [Google Scholar] [CrossRef] [PubMed]
- Tremoulet, A.H. Adjunctive therapies in Kawasaki disease. Int. J. Rheum Dis. 2018, 21, 76–79. [Google Scholar] [CrossRef]
- Riphagen, S.; Gomez, X.; Gonzalez-Martinez, C.; Wilkinson, N.; Theocharis, P. Hyperinflammatory shock in children during COVID-19 pandemic. Lancet 2020, 395, 1607–1608. [Google Scholar] [CrossRef] [PubMed]
- Toubiana, J.; Poirault, C.; Corsia, A.; Bajolle, F.; Fourgeaud, J.; Angoulvant, F.; Debray, A.; Basmaci, R.; Salvador, E.; Biscardi, S.; et al. Kawasaki-like multisystem inflammatory syndrome in children during the COVID-19 pandemic in Paris, France: Prospective observational study. BMJ 2020, 369, m2094. [Google Scholar] [CrossRef]
- Verdoni, L.; Mazza, A.; Gervasoni, A.; Martelli, L.; Ruggeri, M.; Ciuffreda, M.; Bonanomi, E.; D’Antiga, L. An outbreak of severe Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2 epidemic: An observational cohort study. Lancet 2020, 395, 1771–1778. [Google Scholar] [CrossRef]
- Henderson, L.A.; Canna, S.W.; Friedman, K.G.; Gorelik, M.; Lapidus, S.K.; Bassiri, H.; Behrens, E.M.; Ferris, A.; Kernan, K.F.; Schulert, G.S.; et al. American College of Rheumatology Clinical Guidance for Multisystem Inflammatory Syndrome in Children Associated With SARS-CoV-2 and Hyperinflammation in Pediatric COVID-19: Version 2. Arthritis Rheumatol. 2021, 73, e13–e29. [Google Scholar] [CrossRef]
- McArdle, A.J.; Vito, O.; Patel, H.; Seaby, E.G.; Shah, P.; Wilson, C.; Broderick, C.; Nijman, R.; Tremoulet, A.H.; Munblit, D.; et al. Treatment of Multisystem Inflammatory Syndrome in Children. N. Engl. J. Med. 2021, 385, 11–22. [Google Scholar] [CrossRef]
- Rauniyar, R.; Mishra, A.; Kharel, S.; Giri, S.; Rauniyar, R.; Yadav, S.; Chaudhary, G. IVIG plus Glucocorticoids versus IVIG Alone in Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with COVID-19: A Systematic Review and Meta-Analysis. Can. J. Infect. Dis. Med. Microbiol. 2022, 2022, 9458653. [Google Scholar] [CrossRef] [PubMed]
- Law, Y.M.; Lal, A.K.; Chen, S.; Čiháková, D.; Cooper, L.T.; Deshpande, S.; Godown, J.; Grosse-Wortmann, L.; Robinson, J.D.; Towbin, J.A.; et al. Diagnosis and Management of Myocarditis in Children. Circulation 2021, 144, E123–E135. [Google Scholar] [CrossRef] [PubMed]
- Henderson, L.A.; Canna, S.W.; Friedman, K.G.; Gorelik, M.; Lapidus, S.K.; Bassiri, H.; Behrens, E.M.; Kernan, K.F.; Schulert, G.S.; Seo, P.; et al. American College of Rheumatology Clinical Guidance for Multisystem Inflammatory Syndrome in Children Associated With SARS–CoV-2 and Hyperinflammation in Pediatric COVID-19: Version 3. Arthritis Rheumatol. 2022, 74, E1–E20. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.P.; Shamie, I.; Lee, J.C.; Nowell, C.J.; Peng, W.; Angulo, S.; Le, L.N.; Liu, Y.; Miao, H.; Xiong, H.; et al. Immune response to intravenous immunoglobulin in patients with Kawasaki disease and MIS-C. J. Clin. Investig. 2021, 131, e147076. [Google Scholar] [CrossRef] [PubMed]
- Ganigara, M.; Sharma, C.; Bayry, J. Unraveling the mechanisms of IVIG immunotherapy in MIS-C. Cell Rep. Med. 2021, 2, 100431. [Google Scholar] [CrossRef] [PubMed]
- Syrimi, E.; Fennell, E.; Richter, A.; Vrljicak, P.; Stark, R.; Ott, S.; Murray, P.G.; Al-Abadi, E.; Chikermane, A.; Dawson, P.; et al. The immune landscape of SARS-CoV-2-associated Multisystem Inflammatory Syndrome in Children (MIS-C) from acute disease to recovery. iScience 2021, 24, 103215. [Google Scholar] [CrossRef] [PubMed]
- Galeotti, C.; Kaveri, S.V.; Bayry, J. IVIG-mediated effector functions in autoimmune and inflammatory diseases. Int. Immunol. 2017, 29, 491–498. [Google Scholar] [CrossRef]
- Ravelli, A.; Minoia, F.; Davì, S.; Horne, A.; Bovis, F.; Pistorio, A.; Aricò, M.; Avcin, T.; Behrens, E.M.; De Benedetti, F.; et al. 2016 Classification Criteria for Macrophage Activation Syndrome Complicating Systemic Juvenile Idiopathic Arthritis: A European League Against Rheumatism/American College of Rheumatology/Paediatric Rheumatology International Trials Organisation Collaborative Initiative. Arthritis Rheumatol. 2016, 68, 566–576. [Google Scholar] [CrossRef]
- Lee, P.Y.; Day-Lewis, M.; Henderson, L.A.; Friedman, K.G.; Lo, J.; Roberts, J.E.; Lo, M.S.; Platt, C.D.; Chou, J.; Hoyt, K.J.; et al. Distinct clinical and immunological features of SARS-CoV-2-induced multisystem inflammatory syndrome in children. J. Clin. Investig. 2020, 130, 5942–5950. [Google Scholar] [CrossRef]
- Rodriguez-Smith, J.J.; Verweyen, E.L.; Clay, G.M.; Esteban, Y.M.; de Loizaga, S.R.; Baker, E.J.; Do, T.; Dhakal, S.; Lang, S.M.; Grom, A.A.; et al. Inflammatory biomarkers in COVID-19-associated multisystem inflammatory syndrome in children, Kawasaki disease, and macrophage activation syndrome: A cohort study. Lancet Rheumatol. 2021, 3, e574–e584. [Google Scholar] [CrossRef] [PubMed]
- Yener, G.O.; Kısaarslan, A.P.; Ulu, K.; Atalay, E.; Haşlak, F.; Özdel, S.; Yücel, B.B.; Yıldırım, D.G.; Çakmak, F.; Öztürk, K.; et al. Differences and similarities of multisystem inflammatory syndrome in children, Kawasaki disease and macrophage activating syndrome due to systemic juvenile idiopathic arthritis: A comparative study. Rheumatol. Int. 2022, 42, 879–889. [Google Scholar] [CrossRef] [PubMed]
- Valverde, I.; Singh, Y.; Sanchez-De-Toledo, J.; Theocharis, P.; Chikermane, A.; Di Filippo, S.; Kuciñska, B.; Mannarino, S.; Tamariz-Martel, A.; Gutierrez-Larraya, F.; et al. Acute Cardiovascular Manifestations in 286 Children with Multisystem Inflammatory Syndrome Associated With COVID-19 Infection in Europe. Circulation 2021, 143, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Patel, T.; Kelleman, M.; West, Z.; Peter, A.; Dove, M.; Butto, A.; Oster, M.E. Comparison of Multisystem Inflammatory Syndrome in Children-Related Myocarditis, Classic Viral Myocarditis, and COVID-19 Vaccine-Related Myocarditis in Children. J. Am. Heart Assoc. 2022, 11, e024393. [Google Scholar] [CrossRef]
- Maisch, B. Cardio-Immunology of Myocarditis: Focus on Immune Mechanisms and Treatment Options. Front. Cardiovasc. Med. 2019, 6, 48. [Google Scholar] [CrossRef]
- Huang, X.; Sun, Y.; Su, G.; Li, Y.; Shuai, X. Intravenous Immunoglobulin Therapy for Acute Myocarditis in Children and Adults. Int. Heart J. 2019, 60, 359–365. [Google Scholar] [CrossRef]
- Robinson, J.; Hartling, L.; Vandermeer, B.; Sebastianski, M.; Klassen, T.P. Intravenous immunoglobulin for presumed viral myocarditis in children and adults. Cochrane Database Syst. Rev. 2020, 2020, CD004370. [Google Scholar] [CrossRef]
- Caforio, A.L.P.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648. [Google Scholar] [CrossRef]
- Guo, Y.; Tian, X.; Wang, X.; Xiao, Z. Adverse Effects of Immunoglobulin Therapy. Front. Immunol. 2018, 9, 1299. [Google Scholar] [CrossRef]
- Dantal, J. Intravenous Immunoglobulins: In-Depth Review of Excipients and Acute Kidney Injury Risk. Am. J. Nephrol. 2013, 38, 275–284. [Google Scholar] [CrossRef]
- Jiang, M.; Kimber, J.S.; Gupta, A.; Kovoor, J.; Stretton, B.; Ravindran, J.; Hissaria, P.; Smith, W.B.; Bacchi, S. Adverse Reactions Associated with Intravenous Immunoglobulin Administration in the Treatment of Neurological Disorders: A Systematic Review. Int. Arch. Allergy Immunol. 2023, 184, 513–528. [Google Scholar] [CrossRef]
- Freeman, C.M.; Squire, J.D.; Joshi, A.Y. Immunoglobulin treatment for B-cell immunodeficiencies. J. Immunol. Methods 2022, 509, 113336. [Google Scholar] [CrossRef] [PubMed]
- Sandler, S.G.; Eder, A.F.; Goldman, M.; Winters, J.L. The entity of immunoglobulin A-related anaphylactic transfusion reactions is not evidence based. Transfusion 2015, 55, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Tacquard, C.; Boudjedir, K.; Carlier, M.; Muller, J.Y.; Gomis, P.; Mertes, P.M. Hypersensitivity transfusion reactions due to IgA deficiency are rare according to French hemovigilance data. J. Allergy Clin. Immunol. 2017, 140, 884–885. [Google Scholar] [CrossRef] [PubMed]
- Yanagihashi, M.; Okamoto, R.; Morioka, H.; Sawada, M.; Matsumoto, S.; Ikeda, T.; Kano, O. Coronary spastic angina after the administration of intravenous immunoglobulin in myasthenia gravis: A case report. BMC Neurol. 2020, 20, 319. [Google Scholar] [CrossRef] [PubMed]
- Binitha, M.; Nandakumar, G.; Thomas, D. Suspected cardiac toxicity to intravenous immunoglobulin used for treatment of scleromyxedema. Indian J. Dermatol. Venereol. Leprol. 2008, 74, 248. [Google Scholar] [CrossRef] [PubMed]
- Benadiba, J.; Robitaille, N.; Lambert, G.; Itaj, N.K.; Pastore, Y. Intravenous immunoglobulin-associated thrombosis: Is it such a rare event? Report of a pediatric case and of the Quebec Hemovigilance System. Transfusion 2015, 55, 571–575. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, J.; Al Amri, A.; Ghatasheh, G. Transfusion-Related Acute Lung Injury After Immunoglobulin Infusion for Kawasaki Disease: A Case Report and Literature Review. Glob. Pediatr. Health 2017, 4, 2333794X1774654. [Google Scholar] [CrossRef]
- Baudel, J.L.; Vigneron, C.; Pras-Landre, V.; Joffre, J.; Marjot, F.; Ait-Oufella, H.; Bigé, N.; Maury, E.; Guidet, B.; Fain, O.; et al. Transfusion-related acute lung injury (TRALI) after intravenous immunoglobulins: French multicentre study and literature review. Clin. Rheumatol. 2020, 39, 541–546. [Google Scholar] [CrossRef]
- Yu, Y.; Lian, Z. Update on transfusion-related acute lung injury: An overview of its pathogenesis and management. Front. Immunol. 2023, 14, 1175387. [Google Scholar] [CrossRef]
- Cappell, K.M.; Sherry, R.M.; Yang, J.C.; Goff, S.L.; Vanasse, D.A.; McIntyre, L.; Rosenberg, S.A.; Kochenderfer, J.N. Long-Term Follow-Up of Anti-CD19 Chimeric Antigen Receptor T-Cell Therapy. J. Clin. Oncol. 2020, 38, 3805–3815. [Google Scholar] [CrossRef] [PubMed]
- Makatsori, M.; Kiani-Alikhan, S.; Manson, A.L.; Verma, N.; Leandro, M.; Gurugama, N.P.; Longhurst, H.J.; Grigoriadou, S.; Buckland, M.; Kanfer, E.; et al. Hypogammaglobulinaemia after rituximab treatment—Incidence and outcomes. QJM 2014, 107, 821–828. [Google Scholar] [CrossRef]
- Stohl, W.; Schwarting, A.; Okada, M.; Scheinberg, M.; Doria, A.; Hammer, A.E.; Kleoudis, C.; Groark, J.; Bass, D.; Fox, N.L.; et al. Efficacy and Safety of Subcutaneous Belimumab in Systemic Lupus Erythematosus: A Fifty-Two–Week Randomized, Double-Blind, Placebo-Controlled Study. Arthritis Rheumatol. 2017, 69, 1016–1027. [Google Scholar] [CrossRef]
- Yusof, Y.M.; Vital, E.M.; McElvenny, D.M.; Hensor, E.M.A.; Das, S.; Dass, S.; Rawstron, A.C.; Buch, M.H.; Emery, P.; Savic, S. Predicting Severe Infection and Effects of Hypogammaglobulinemia During Therapy with Rituximab in Rheumatic and Musculoskeletal Diseases. Arthritis Rheumatol. 2019, 71, 1812–1823. [Google Scholar] [CrossRef] [PubMed]
- Galli, E.; Fresa, A.; Bellesi, S.; Metafuni, E.; Maiolo, E.; Pansini, I.; Frioni, F.; Autore, F.; Limongiello, M.A.; Innocenti, I.; et al. Hematopoiesis and immune reconstitution after CD19 directed chimeric antigen receptor T-cells (CAR-T): A comprehensive review on incidence, risk factors and current management. Eur. J. Haematol. 2023, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Lucas, M.; Lee, M.; Lortan, J.; Lopez-Granados, E.; Misbah, S.; Chapel, H. Infection outcomes in patients with common variable immunodeficiency disorders: Relationship to immunoglobulin therapy over 22 years. J. Allergy Clin. Immunol. 2010, 125, 1354–1360.e4. [Google Scholar] [CrossRef]
- Khan, S.; Davies, L.; Cowley, D.; Wild, G.; Sewell, W.A.C. Anti-acetylcholine receptor antibody reactivity of IgG in commercial immunoglobulin preparations. Clin. Neurol. Neurosurg. 2010, 112, 835–836. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Sims, S.; Raine, D.; Sewell, W.A.C. Both autoantibodies and pathogen-specific antibodies are present in immunoglobulin preparations and reflect characteristics of the donor population. J. Am. Acad. Dermatol. 2008, 59, 1089–1090. [Google Scholar] [CrossRef]
- Smith, T.D.; Cunningham-Rundles, C. Detection of anti–glutamic acid decarboxylase antibodies in immunoglobulin products. J. Allergy Clin. Immunol. Pract. 2018, 6, 260–261. [Google Scholar] [CrossRef]
- Grüter, T.; Ott, A.; Meyer, W.; Jarius, S.; Kinner, M.; Motte, J.; Pitarokoili, K.; Gold, R.; Komorowski, L.; Ayzenberg, I. Effects of IVIg treatment on autoantibody testing in neurological patients: Marked reduction in sensitivity but reliable specificity. J. Neurol. 2020, 267, 715–720. [Google Scholar] [CrossRef]
- van der Molen, R.G.; Hamann, D.; Jacobs, J.F.; van der Meer, A.; de Jong, J.; Kramer, C.; Strengers, P.F.; van der Meer, J.W. Anti-SSA antibodies are present in immunoglobulin preparations. Transfusion 2015, 55, 832–837. [Google Scholar] [CrossRef] [PubMed]
- Burbelo, P.D.; Castagnoli, R.; Shimizu, C.; Delmonte, O.M.; Dobbs, K.; Discepolo, V.; Vecchio, A.L.; Guarino, A.; Licciardi, F.; Ramenghi, U.; et al. Autoantibodies Against Proteins Previously Associated with Autoimmunity in Adult and Pediatric Patients With COVID-19 and Children With MIS-C. Front. Immunol. 2022, 13, 841126. [Google Scholar] [CrossRef] [PubMed]
- Dimitriadou, M.M.; Alexopoulos, H.; Akrivou, S.; Gola, E.; Dalakas, M.C. Anti-Neuronal Antibodies Within the IVIg Preparations: Importance in Clinical Practice. Neurotherapeutics 2020, 17, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Fnu, Z.; Uddin, A.; Navetta-Modrov, B.; Patnaik, A.; Kaell, A. Inpatient Rheumatology Consultation Prompted by Positive Autoantibodies in Patients Receiving Intravenous Immunoglobulin Therapy: A Case Series and Literature Review. Cureus 2023, 15, e37008. [Google Scholar] [CrossRef] [PubMed]
- Imbach, P.; Barandun, S.; Baumgartner, C.; Hirt, A.; Hofer, F.; Wagner, H.P. High-dose intravenous gammaglobulin therapy of refractory, in particular idiopathic thrombocytopenia in childhood. Helv. Paediatr. Acta 1981, 36, 81–86. [Google Scholar] [PubMed]
- Imbach, P.; D’Apuzzo, V.; Hirt, A.; Rossi, E.; Vest, M.; Barandun, S.; Baumgartner, C.; Morell, A.; Schöni, M.; Wagner, H. High-dose intravenous gammaglobulin for idiopathic thrombocytopenic purpura in childhood. Lancet 1981, 317, 1228–1231. [Google Scholar] [CrossRef] [PubMed]
- Fateh-Moghadam, A.; Wick, M.; Besinger, U.; Geursen, R.G. High-dose intravenous gammaglobulin for myasthenia gravis. Lancet 1984, 323, 848–849. [Google Scholar] [CrossRef]
- Péchadre, J.; Sauvezie, B.; Osier, C.; Gibert, J. Traitement des encéphalopathies épileptiques de l’enfant par les gamma-globulines Résultats préliminaires. Rev. D’electroencéphalograph. Neurophysiol. Clin. 1977, 7, 443–447. [Google Scholar] [CrossRef]
- Więsik-Szewczyk, E.; Ziętkiewicz, M.; Radziwilska-Muc, A.; Jahnz-Różyk, K. Increased Access to Immunoglobulin Replacement Therapy for Patients with Primary Immunodeficiency in Poland Based on Clinical Usage Data of Immunoglobulin G over a 5-Year Period. J. Clin. Med. 2023, 12, 2431. [Google Scholar] [CrossRef]
- EMA. Guideline on the Clinical Investigation of Human Normal Immunoglobulin for Intravenous Administration (IVIg); EMA: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Criteria for Clinical Use of Immunoglobulin in Australia. Available online: https://www.criteria.blood.gov.au/checkeligibility (accessed on 1 August 2023).
- AIFA. Documento di Indirizzo Sull’uso Delle Immunoglobuline Umane in Condizioni di Carenza; AIFA: Rome, Italy, 2022. [Google Scholar]
- Na, I.; Buckland, M.; Agostini, C.; Edgar, J.D.M.; Friman, V.; Michallet, M.; Sánchez-Ramón, S.; Scheibenbogen, C.; Quinti, I. Current clinical practice and challenges in the management of secondary immunodeficiency in hematological malignancies. Eur. J. Haematol. 2019, 102, 447–456. [Google Scholar] [CrossRef]
- Cinetto, F.; Francisco, I.E.; Fenchel, K.; Scarpa, R.; Montefusco, V.; Pluta, A.; Wolf, H.M. Use of immunoglobulin replacement therapy in patients with secondary antibody deficiency in daily practice: A European expert Q&A-based review. Expert Rev. Hematol. 2023, 16, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Kobayashi, R.H.; Litzman, J.; Cherwin, L.; Hoeller, S.; Kreuwel, H. Subcutaneous immunoglobulin 16.5% for the treatment of pediatric patients with primary antibody immunodeficiency. Expert Rev. Clin. Immunol. 2023, 19, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Gardulf, A.; Bjorvell, H.; Andersen, V.; Bjorkander, J.; Ericson, D.; Froland, S.S.; Gustafson, R.; Hammarstrom, L.; Nystrom, T.; Soeberg, B.; et al. Lifelong treatment with gammaglobulin for primary antibody deficiencies: The patients’ experiences of subcutaneous self-infusions and home therapy. J. Adv. Nurs. 1995, 21, 917–927. [Google Scholar] [CrossRef] [PubMed]
- Hammarstrom, L.; Gardulf, A.; Edvard Smith, C.I.; Gardulf, A. Home treatment of hypogammaglobulinaemia with subcutaneous gammaglobulin by rapid infusion. Lancet 1991, 338, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Gardulf, A.; Björvell, H.; Gustafson, R.; Hammarström, L.; Smith, C.I. Safety of rapid subcutaneous gammaglobulin infusions in patients with primary antibody deficiency. Immunodeficiency 1993, 4, 81–84. [Google Scholar] [PubMed]
- Gaspar, J.; Gerritsen, B.; Jones, A. Immunoglobulin replacement treatment by rapid subcutaneous infusion. Arch. Dis. Child. 1998, 79, 48–51. [Google Scholar] [CrossRef] [PubMed]
- Chouksey, A.; Duff, K.; Wasserbauer, N.; Berger, M. Subcutaneous Immunoglobulin-G Replacement Therapy with Preparations Currently Available in the United States for Intravenous or Intramuscular Use: Reasons and Regimens. Allergy Asthma Clin. Immunol. 2005, 1, 120. [Google Scholar] [CrossRef] [PubMed]
- Gammon, R.; Katz, L.M.; Strauss, D.; Rowe, K.; Menitove, J.; Benjamin, R.J.; Goel, R.; Borge, D.; Reichenberg, S.; Smith, R. Beyond COVID-19 and lessons learned in the United States. Transfus. Med. 2023, 33, 6–15. [Google Scholar] [CrossRef]
- Chapel, H.M.; Spickett, G.P.; Ericson, D.; Engl, W.; Eibl, M.M.; Bjorkander, J. The comparison of the efficacy and safety of intravenous versus subcutaneous immunoglobulin replacement therapy. J. Clin. Immunol. 2000, 20, 94–100. [Google Scholar] [CrossRef]
- Gul, Y.; Kapakli, H.; Guner, S.N.; Alan, H.B.; Hazar, E.; Keles, S.; Reisli, I. Long-Term Experience of Subcutaneous Immunoglobulin Therapy in Pediatric Primary Immunodeficient Patients with Low and Normal Body Weight. J. Clin. Immunol. 2022, 42, 64–71. [Google Scholar] [CrossRef]
- Hagan, J.B.; Fasano, M.B.; Spector, S.; Wasserman, R.L.; Melamed, I.; Rojavin, M.A.; Zenker, O.; Orange, J.S. Efficacy and Safety of a New 20% Immunoglobulin Preparation for Subcutaneous Administration, IgPro20, in Patients with Primary Immunodeficiency. J. Clin. Immunol. 2010, 30, 734–745. [Google Scholar] [CrossRef] [PubMed]
- Ochs, H.D.; Gupta, S.; Kiessling, P.; Nicolay, U.; Berger, M. Safety and Efficacy of Self-Administered Subcutaneous Immunoglobulin in Patients with Primary Immunodeficiency Diseases. J. Clin. Immunol. 2006, 26, 265–273. [Google Scholar] [CrossRef]
- Alsina, L.; Montoro, J.B.; Moral, P.M.; Neth, O.; Pica, M.O.; Sánchez-Ramón, S.; Presa, M.; Oyagüez, I.; Casado, M.; González-Granado, L.I. Cost-minimization analysis of immunoglobulin treatment of primary immunodeficiency diseases in Spain. Eur. J. Health Econ. 2022, 23, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Perraudin, C.; Bourdin, A.; Vicino, A.; Kuntzer, T.; Bugnon, O.; Berger, J. Home-based subcutaneous immunoglobulin for chronic inflammatory demyelinating polyneuropathy patients: A Swiss cost-minimization analysis. PLoS ONE 2020, 15, e0242630. [Google Scholar] [CrossRef] [PubMed]
- Perraudin, C.; Bourdin, A.; Spertini, F.; Berger, J.; Bugnon, O. Switching Patients to Home-Based Subcutaneous Immunoglobulin: An Economic Evaluation of an Interprofessional Drug Therapy Management Program. J. Clin. Immunol. 2016, 36, 502–510. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, B.; Martins, K.J.B.; Tran, D.T.; Blain, H.; Richer, L.; Klarenbach, S.W. Economic impact of self-administered subcutaneous versus clinic-administered intravenous immunoglobulin G therapy in Alberta, Canada: A population-based cohort study. Allergy Asthma Clin. Immunol. 2022, 18, 99. [Google Scholar] [CrossRef] [PubMed]
- Fu, L.W.; Song, C.; Isaranuwatchai, W.; Betschel, S. Home-based subcutaneous immunoglobulin therapy vs hospital-based intravenous immunoglobulin therapy: A prospective economic analysis. Ann. Allergy Asthma Immunol. 2018, 120, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.; Romberg, N. High cost of immunoglobulin replacement therapy. Ann. Allergy Asthma Immunol. 2022, 129, 645. [Google Scholar] [CrossRef]
- Garraud, O. Injectable immunoglobulins, immunodeficiency and off-label clinical trials, source plasma and ethical concerns and debates. Transfus. Apher. Sci. 2019, 58, 529–530. [Google Scholar] [CrossRef]
- Costagliola, G.; Peroni, D.G.; Consolini, R. Beyond Infections: New Warning Signs for Inborn Errors of Immunity in Children. Front. Pediatr. 2022, 10, 855445. [Google Scholar] [CrossRef]
- Lindahl, H.; Bryceson, Y.T. Neuroinflammation Associated with Inborn Errors of Immunity. Front. Immunol. 2022, 12, 827815. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Zhu, L.-N.; Hou, H.-M.; Wang, S.; Zhang, S.; Wang, G.-G.; Guo, Z.-Y. FcRn inhibitors: A novel option for the treatment of myasthenia gravis. Neural Regen. Res. 2022, 18, 1637–1644. [Google Scholar] [CrossRef] [PubMed]
- Briani, C.; Visentin, A. Therapeutic Monoclonal Antibody Therapies in Chronic Autoimmune Demyelinating Neuropathies. Neurotherapeutics 2022, 19, 874–884. [Google Scholar] [CrossRef] [PubMed]
- Heo, Y.A. Satralizumab: First Approval. Drugs 2020, 80, 1477–1482. [Google Scholar] [CrossRef] [PubMed]
- Frampton, J.E. Inebilizumab: First Approval. Drugs 2020, 80, 1259–1264. [Google Scholar] [CrossRef] [PubMed]
- Conti, F.; Gottardi, F.; Moratti, M.; Belotti, T.; Ferrari, S.; Selva, P.; Bassi, M.; Zama, D.; Pession, A. Refractory immune thrombocytopenia successfully treated with bortezomib in a child with 22q11.2 deletion syndrome, complicated by Evans syndrome and hypogammaglobulinemia. Platelets 2022, 33, 801–806. [Google Scholar] [CrossRef] [PubMed]
- Dodig, D.; Genge, A.; Selchen, D.; Freedman, M.S. Complement Inhibition in Myasthenia Gravis and Neuromyelitis Optica Spectrum Disorder. Can. J. Neurol. Sci. J. Can. Des Sci. Neurol. 2023, 50, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Werdan, K. Pathophysiology of Septic Shock and Multiple Organ Dysfunction Syndrome and Various Therapeutic Approaches with Special Emphasis on Immunoglobulins. Ther. Apher. Dial. 2001, 5, 115–122. [Google Scholar] [CrossRef]
- Friedman, C.; Wender, D.; Temple, D.; Rawson, J. Intravenous Gamma Globulin as Adjunct Therapy for Severe Group B Streptococcal Disease in the Newborn. Am. J. Perinatol. 1990, 7, 1–4. [Google Scholar] [CrossRef]
- Kaul, R.; McGeer, A.; Norrby-Teglund, A.; Kotb, M.; Schwartz, B.; O’Rourke, K.; Talbot, J.; Low, D.E. Intravenous Immunoglobulin Therapy for Streptococcal Toxic Shock Syndrome—A Comparative Observational Study. Clin. Infect. Dis. 1999, 28, 800–807. [Google Scholar] [CrossRef]
- Jenson, H.B.; Pollock, B.H. The role of intravenous immunoglobulin for the prevention and treatment of neonatal sepsis. Semin. Perinatol. 1998, 22, 50–63. [Google Scholar] [CrossRef] [PubMed]
- INIS Collaborative Group. Treatment of Neonatal Sepsis with Intravenous Immune Globulin. N. Engl. J. Med. 2011, 365, 1201–1211. [Google Scholar] [CrossRef] [PubMed]
- Alejandria, M.M.; Lansang, M.A.D.; Dans, L.F.; Mantaring, J.B., III. Intravenous immunoglobulin for treating sepsis, severe sepsis and septic shock. Cochrane Database Syst. Rev. 2013, 2018, CD001090. [Google Scholar] [CrossRef] [PubMed]
- Perricone, C.; Triggianese, P.; Bursi, R.; Cafaro, G.; Bartoloni, E.; Chimenti, M.S.; Gerli, R.; Perricone, R. Intravenous Immunoglobulins at the Crossroad of Autoimmunity and Viral Infections. Microorganisms 2021, 9, 121. [Google Scholar] [CrossRef]
- Pinto, A.K.; Hassert, M.; Han, X.; Barker, D.; Carnelley, T.; Branche, E.; Steffen, T.L.; Stone, E.T.; Geerling, E.; Viramontes, K.M.; et al. The Ability of Zika virus Intravenous Immunoglobulin to Protect from or Enhance Zika Virus Disease. Front. Immunol. 2021, 12, 717425. [Google Scholar] [CrossRef] [PubMed]
- Castaldo, P.; D’alanno, G.; Biserni, G.B.; Moratti, M.; Conti, F.; Fabi, M.; Lanari, M. Exploring Factors Influencing Changes in Incidence and Severity of Multisystem Inflammatory Syndrome in Children. Pathogens 2023, 12, 997. [Google Scholar] [CrossRef]
- Mosca, M.; Bacchetta, J.; Chamouard, V.; Rascle, P.; Dubois, V.; Paul, S.; Mekki, Y.; Picard, C.; Bertholet-Thomas, A.; Ranchin, B.; et al. IVIg therapy in the management of BK virus infections in pediatric kidney transplant patients. Arch. Pédiatr. 2023, 30, 165–171. [Google Scholar] [CrossRef]


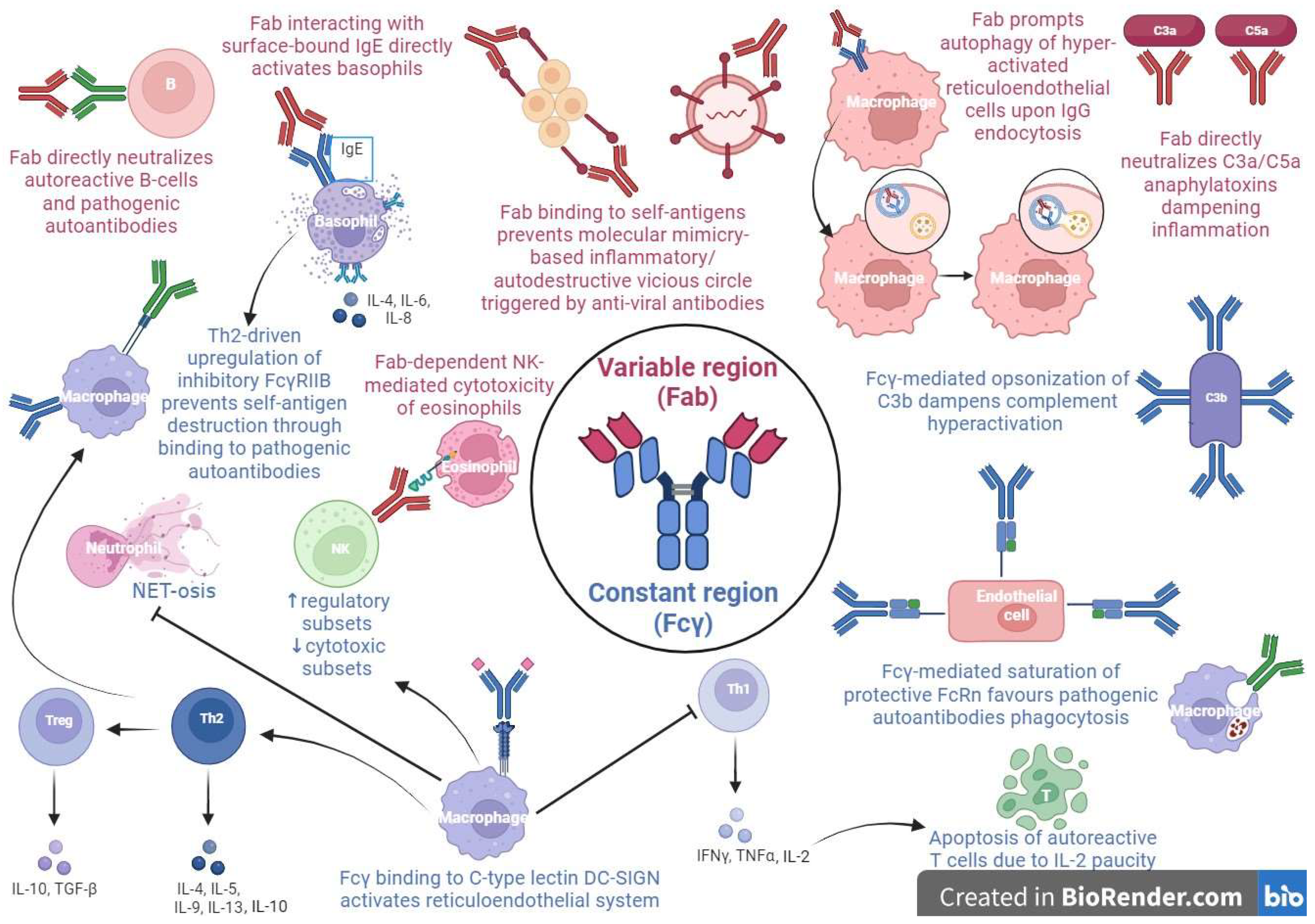{kind=link}
| Author | Year | Type of Study | Objective | Outcome |
|---|---|---|---|---|
| Neurologic Conditions | ||||
| Acute disseminated encephalomyelitis (ADEM) | ||||
| Gadian J et al. [50] | 2017 | Systematic review without meta-analysis | Comparison between IVIG and
| IVIG and steroids can improve recovery in initial treatment of ADEM |
| Vitaliti G et al. [51] | 2015 | Systematic review without meta-analysis | Effects of corticosteroids in terms of complete recovery | IVIG is a possible treatment for ADEM, especially for the steroid-resistant/dependent form, although there is insufficient evidence about its effectiveness |
| Chronic inflammatory demyelinating polyneuropathy (CIDP) | ||||
| Racosta JM et al. [52] | 2017 | Systematic review with meta-analysis | Comparison between IVIG and subcutaneous (SCIG) immunoglobulin in terms of symptoms [baseline change in the Medical Research Council Sum Score (MRC-SS)], efficacy, safety, adverse effects, and conditions of use for the different treatments | No statistically significant difference between IVIG and SCIG on the MRC-SS for muscle strength |
| Gadian J et al. [50] | 2017 | Systematic review without meta-analysis | Comparison between IVIG and PLEX/corticosteroids in terms of sensory and motor function, assessed by the Modified Rankin Scale, neurological and/or electrophysiological tests | IVIG is a potential efficacious first-choice therapy for chronic inflammatory demyelinating polyneuropathy (78% rate of response), when compared with corticosteroids (70% rate of response) and PLEX (14% rate of response) in terms of sensory and motor function |
| Febrile infection-related epilepsy syndrome (FIRES) | ||||
| Gaspard N et al. [53] | 2018 | Critical review and invited commentary | The First International Symposium regarding new-onset refractory status epilepticus (NORSE) and FIRES to improve patient management | Among 225 patients with FIRES, positive effects were reported in 11/63 (17%) treated with steroids, 5/94 (5%) with IVIG, 19/35 (54%) with ketogenic diet, 2/18 (11%) with plasmapheresis, 3/5 (60%) with hypothermia, and 1/3 (33%) with rituximab |
| Kramer U et al. [54] | 2011 | Retrospective multicenter study | To search for the correlations between different therapies (IVIG, steroids, barbiturate, ketogenic diet) and outcome in 77 children with FIRES | IVIG, ketogenic diet, and a barbiturate-induced coma were the only efficacious treatment modalities for FIRES in two, one, and one patients, respectively |
| Guillain–Barré syndrome (GBS) | ||||
| Gadian J et al. [50] | 2017 | Systematic review without meta-analysis | Comparison between IVIG and PLEX/supportive care/no treatment in terms of time to improvement/recovery | IVIG speeds up recovery, reducing time until function improvement, but does not affect maximal disability score |
| Vitaliti G et al. [51] | 2015 | Systematic review without meta-analysis | Comparison between IVIG and PLEX/supportive care/no treatment in terms of time to improvement/recovery | IVIGs are a possible therapy for GBS in comparison with PLEX or supportive care |
| Hughes RA et al. [13] | 2014 | Systematic review with meta-analysis | Explore the differences between IVIG and PLEX/placebo/no treatment in terms of time to recovery and improvement in disability grade 4 weeks after the randomization | Addition of IVIG hastens recovery, significantly improving disability grade 4 weeks after randomization compared with supportive care alone |
| Myasthenia gravis (MG) | ||||
| Gadian J et al. [50] | 2017 | Systematic review without meta-analysis | Comparison between IVIG and corticosteroids in terms of clinical response to treatment | IVIG may improve responses in patients with MG, although the evidence about itstheir effectiveness in the disease’s exacerbation is low |
| Myelin oligodendrocyte glycoprotein (MOG) antibody-associated disease (MOGAD) | ||||
| Klein da Costa et al. [55] | 2021 | Systematic review | To perform a review on treatment of children with MOGAD |
|
| N-methyl D-aspartate receptor antibody encephalitis (NMDARE) | ||||
| Nosadini et al. [56] | 2021 | Meta-analysis | To assess the safety of immunotherapies in individuals with NMDARE; to identify early predictors of relapse and poor functional outcome; to assess variations in immunotherapy employment and disease course since NMDARE was first reported 14 years before |
|
| Gadian J et al. [50] | 2017 | Systematic review without meta-analysis | To evaluate effectiveness of IVIG, with or without adjunctive immunomodulatory therapies, in terms of recovery in patients with NMDARE |
|
| Opsoclonus-myoclonus-ataxia syndrome (OMAS) | ||||
| de Alarcon PA et al. [57] | 2018 | A randomised, prospective, open-label, phase III therapeutic trial | To evaluate the response to prednisone and check if IVIG adjunction further ameliorates response in 53 pediatric patients with neuroblastoma-related OMAS |
|
| Gadian J et al. [50] | 2017 | Systematic Review without meta-analysis | To evaluate the effectiveness of IVIG, steroids, and rituximab/cyclophosphamide in comparison with corticosteroids/ACTH alone in terms of recovery in patients with opsoclonus myoclonus syndrome |
|
| Pediatric acute-onset neuropsychiatric syndrome (PANS) | ||||
| Johnson M et al. [58] | 2021 | Systematic review without meta-analysis | To assess effects of treatment in children with PANS |
|
| Rasmussen’s encephalitis | ||||
| Gadian J et al. [50] | 2017 | Systematic review without meta-analysis | To evaluate the effectiveness of IVIG, tacrolimus, corticosteroids, PLEX, ACTH, interferon, and surgery, alone or in combination, in terms of recovery in patients with Rasmussen’s encephalitis |
|
| Sydenham’s chorea | ||||
| Orsini A et al. [59] | 2022 | Multicenter cohort study | To provide high-quality evidence of the management and prognostic markers of Sydenham’s chorea in 171 pediatric patients | Immunomodulatory therapy (IVIG and steroids) is not associated with a medium-term higher efficacy, but it shows a slightly reduced risk of relapse in comparison with symptomatic therapy (anti-seizure medication, dopamine antagonists) |
| Mohammad SS et al. [60,61] | 2015 | Systematic review | To compare effectiveness of IVIG, corticosteroids, PLEX and symptomatic treatment in terms of chorea score reduction and of shorter need for symptomatic treatment considering two randomized controlled studies |
|
| Hematologic conditions | ||||
| Acquired hemophilia (AHA) | ||||
| Gianella-Borradori et al. [62] | 1984 | Case report | To describe a case of AHA in a boy of 13 years | Vincristine and steroids controlled the hemophilia, but this therapy was discontinued due to side effects. For this reason, he had to start therapy with IVIG Treatment with IVIG resulted in a slow rise in factor VIII and in a reduction in factor VIII inhibitors |
| Sultan Y et al. [63] | 1984 | Case series | To describe the cases of two patients with high-titer antihemophilic factor (VIII) autoantibodies, treated with IVIG | The treatment with IVIG produced rapid and durable antibody suppression |
| Autoimmune hemolytic anemia (AIHA) | ||||
| Flores G et al. [64] | 1993 | Separate pilot studies at 3 institutions (37 patients), combined with a review of 36 cases of AIHA treated with IVIG reported in the literature | To assess warm antibody AIHA responsiveness to IVIG | Overall, 29 of 73 (39.7%) patients were responsive to IVIG treatment Hepatomegaly and a low level of hemoglobin pre-treatment (<6–7 g/dL) strongly correlated with IVIG efficacy |
| Mathai et al. [65] | 1990 | Case report | To describe IVIG efficacy in the management of hemolytic anemia through the case of a newborn with hemolytic anemia refractory to steroid treatment | An excellent response was detected in the patient, achieving complete remission with IVIG (dose of 2 g/kg over 5 days) |
| Autoimmune neutropenia (AIN) | ||||
| Hilgartner et al. [66] | 1987 | Case series | To describe the cases of six children aged <2 years presenting with a neutrophil count less than 300/mmc and severe infections, treated with 1 g/kg of IVIG until their neutrophil counts reached more than 1000/mmc | Efficacy was reached with a dose of 3 g/kg given over 5 to 7 days; all children recovered from their infections and reached persistent normal neutrophil counts |
| Bussel et al. [67] | 1983 | Case report | To describe two cases of children affected by AIN who showed a good response after IVIG treatment | With the initial IVIG therapy, the neutrophil count raised significantly in both patients; one patient achieved remission |
| Immune thrombocytopenia (ITP) | ||||
| Mikhail D. et al. [68] | 2022 | Monocentric retrospective study | To calculate the rate of rise in the platelet count with IVIG therapy and the impact of demographic and clinical characteristics on the rate of rise. To provide a nomogram showing when to expect a meaningful rise in the platelet count after IVIG therapy | A rate of rise of over +0.5 K/µL/h was seen in 78% of patients. There was not a statistically significant correlation between the rate of rise in the platelet count and age or sex |
| Heitink-Pollé KMJ et al. [69] | 2018 | Multicenter randomized controlled trial | To demonstrate IVIG efficacy at a single dose in reducing the chronicization rate in children with the first episode of ITP. 206 children with new-onset ITP, <20 × 109 platelets/L and mild to moderate bleeding randomly received either a single IVIG infusion (0.8 g/kg) (n = 102) or no therapy (n = 104) |
|
| Higashide Y et al. [70] | 2018 | Multicentered retrospective study | To identify new predictive factors for determining responses to IVIG treatment in newly diagnosed ITP. | Age ≥23 months (p = 0.020) and platelet count <9.0 × 109/L (p = 0.018) were considered to be unfavorable factors for short-term response. Age ≥23 months (p = 0.020) was the only unfavorable factor for long-term response to IVIG therapy |
| Ou CY et al. [71] | 2006 | Comparative study | To compare the increase in platelet count and to assess the risk for persistent severe thrombocytopenia in 87 children with ITP treated with IVIG or prednisolone. 54 patients received IVIG for two days, followed by prednisolone, while 33 patients received prednisolone for 14–21 days |
|
| Gereige RS et al. [72] | 2000 | Retrospective study | To compare the effectiveness of 3 regimens: IVIG only, HD methylprednisolone (HDMP) only and IVIG and HDMP in association in the management of 148 children of ITP |
|
| Fujisawa K et al. [73] | 2000 | Prospective randomized trial | To determine the minimal essential treatment for acute ITP in patients with <10 × 103 platelets/mmc or 10 to 29 × 103 platelets/mmc and mucosal bleeding. Patients randomly received IVIG at 1 to 2 g/kg, conventional oral prednisolone, intravenous methylprednisolone (MPSL), or pulsed intravenous methylprednisolone (P-MPSL) | IVIG offered faster platelet enhancement compared with other therapies |
| Rosthøj S et al. [74] | 1998 | Randomized study | To compare IVIG with P-MPSL in 43 new-onset pediatric cases of ITP |
|
| Neonatal alloimmune thrombocytopenia (NAIT) | ||||
| Winkelhorst D et al. [75] | 2017 | Review | An overview about the available evidence for both pre- and post-natal treatment alternatives in NAIT | For the postnatal treatment of NAIT, matched platelet transfusion represents a potential treatment, which may be combined with IVIG |
| Mueller C et al. [76] | 1989 | Case series | To describe 12 cases of NAIT treated with IVIG. | Of the 12 infants, 10 had a good response (response rate 70–80%), confirming that IVIG can represent a rescue therapy in NAIT in case of unavailable compatible platelets |
| Post-transfusion purpura (PTP) | ||||
| Ziman A et al. [77] | 2002 | Case report | To describe the case of a female of 61 years of age who developed severe PTP | The patient was effectively treated with IVIG |
| Kroll H et al. [78] | 1993 | Retrospective study | To analyze clinical and therapeutic data regarding 38 adult patients with PTP | Of the patients, 74% were responsive to IVIG |
| Mueller C et al. [79] | 1988 | Retrospective multicenter study | To assess IVIG efficacy in 19 PTP cases in adults | A good or excellent response was detected in 17/19 patients receiving IVIG |
| Thrombotic thrombocytopenic purpura (TTP) | ||||
| Ding J et al. [80] | 2017 | Retrospective registry study | To examinate IVIG response in patients with refractory TTP |
|
| Centurioni R. et al. [81] | 1995 | Retrospective observational study | To demonstrate the role of IVIG in the treatment of TTP through the analysis of 17 cases of PLEX-resistant TTP treated with IVIG |
|
| Inflammatory conditions | ||||
| Henoch–Schönlein purpura (HSP) | ||||
| Zhang X et al. [82] | 2022 | Single-center retrospective cohort study | Clinical trial on 64 HSP patients with refractory gastrointestinal manifestation, divided into three groups with different treatment strategies: IVIG and steroid; hemoperfusion and steroid; and IVIG, hemoperfusion and steroid. | Improvement in gastrointestinal symptoms was found in all three groups. IVIG treatment showed better results in young children. |
| Morotti F et al. [83] | 2020 | Case reports | Two clinical cases (11- and 5-year-old boys) of severe HSP gastrointestinal vasculitis refractory to HD intravenous corticosteroids | Rapid clinical gastrointestinal response to IVIG therapy, observing complete resolution within a few days |
| Mauro A et al. [84] | 2019 | Case report | Clinical case of HSP showing severe cutaneous lesions refractory to corticosteroid therapy | An 11-year-old girl was successfully cured with HD-IVIG with prompt symptom recovery |
| Cherqaoui B et al. [85] | 2016 | Retrospective study | Study on the outcomes of HSP patients showing severe gastrointestinal manifestations and undergoing nonsteroidal immunomodulatory treatments |
|
| Fatima A et al. [86] | 2014 | Case report | Clinical case of a 2-year-old girl with HSP showing gastrointestinal involvement (small bowel thickening, colic pneumatosis) | Abdominal pain improved after total parenteral nutrition, antibiotics, and HD-IVIG. Computed tomography scan confirmed normalization of the radiologic signs |
| De Maddi F et al. [87] | 2013 | Case report | Clinical report of boy of 8 years of age with HSP (purpuric rash, polyarticular arthralgias, abdominal pain) who developed acute cerebral hemorrhage |
|
| Fagbemi AA et al. [88] | 2007 | Case report | Clinical case of a 9-year-old affected by HSP, with life-threatening gastrointestinal hemorrhage from multiple intestinal sites. Endoscopy demonstrated aspects of severe gastritis and corticosteroids use was precluded | IVIG use was beneficial for a sustained remission of clinical manifestations. Therefore, this treatment could represent an effective alternative to corticosteroids in these cases |
| Lamireau T et al. [89] | 2001 | Case report | Clinical report of a 10-year-old boy with HSP experiencing sever persistent abdominal pain and bleeding 2 months after diagnosis | After HD-IVIG gastrointestinal manifestations resolved within 3 days, feeding via mouth began on day 7, and he stopped steroid therapy within 1 month. No symptoms were reported during a 3-year follow-up |
| Juvenile dermatomyositis (JDM) | ||||
| Aggarwal R et al. [90] | 2022 | Clinical trial | Randomized, placebo-controlled trial on 95 adult patients showing active dermatomyositis, divided in a 1:1 ratio and receiving IVIG (2 g/kg) or placebo, every 4 weeks for 16 weeks. | Disease improvement (based on a clinical score) was significantly higher in the IVIG-treated patients, despite adverse events |
| Lam CG et al. [91] | 2011 | Retrospective study | Study to define if patients with JDM who receive IVIG reach quiescence sooner with a reduced disease activity compared to controls. For SD patients, to compare IVIG-treated patients to IVIG-naive ones and define disease activity in the two groups | Similar or lower disease activity was noted among IVIG patients compared to controls from 30 days to 4 years post-diagnosis. Steroid-resistant patients showed the best response. Among steroid-dependent patients, IVIG recipients had lower disease activity |
| Levy et al. [92] | 2010 | Retrospective study | Clinical course of eight patients with JDM cured successfully without the use of systemic corticosteroids | IVIG was the first-line treatment (75%) alongside methotrexate (50%), with a favorable response in all and no serious side effects |
| Al-Mayouf SM et al. [93] | 2000 | Retrospective study | To evaluate the role of IVIG in the management of JDM in 18 steroid-resistant or steroid-dependent patients or with unacceptable side effects. Ten patients underwent second-line treatments (methotrexate, azathioprine, cyclosporine, or cyclophosphamide) |
|
| Sansome A et al. [94] | 1995 | Case series | Evaluation of IVIG therapy (2 g/kg for 3 days, then same dose in 5 consecutive days) in nine children with JDM, failing conventional treatments or with intolerable side effects, followed for a 4-year period. The patients were treated with prednisolone, azathioprine, and cyclosporin |
|
| Collet et al. [95] | 1994 | Case report | Two patients (7-year-old and 12-year-old) with refractory JDM and steroid toxicity, treated with HD-IVIG for 9 months | Improvement in muscle mass and reduced muscular damage, cutaneous lesions, discontinuation of steroid therapy |
| Dalakas MC et al. [96] | 1993 | Randomized controlled trial | Evaluation of IVIG treatment in 15 patients (18 to 55 years of age) diagnosed with resistant dermatomyositis diagnosed through biopsy. Randomization between HD-IVIG or placebo per month for three months while taking steroids, with the possibility of crossing over to the alternative therapy for three months in addition | Improvement in muscle strength and repeated muscular biopsies, neuromuscular symptoms |
| Lang BA et al. [97] | 1991 | Pilot study | Evaluation of HD-IVIG in 5 JDM patients, with persistent muscular weakness despite daily corticosteroids. Toxicity to steroid or immunosuppressive therapy was reported by some of the patients | Improved muscle mass and reduced cutaneous rash in all patients. Discontinuation or reduction in steroid therapy |
| Roifman et al. [98] | 1987 | Case report | Evaluation of response to IVIG treatment in a patient of 15 years of age presenting with diffuse myositis and normal immunity, not responding to treatment with steroids, methotrexate, or cyclophosphamide | Improvement in muscle strength, cardiac ejection fraction, pulmonary function tests; reduction in steroid dosage |
| Kawasaki disease (KD) | ||||
| Broderick C et al. [99] | 2023 | Systematic review with meta analysis | To assess IVIG safety and efficacy in the treatment and prevention of KD cardiac complications |
|
| Lei WT et al. [100] | 2022 | Network meta-analysis | To make a comparison about the efficacy and safety of the alternative treatments for the initial and refractory stages of KD, examining 56 randomized controlled trials involving 6486 participants | Medium-dosage IVIG (1 g) + aspirin + infliximab was compared with high-dosage IVIG (2 g min) + aspirin, showing a shorter fever duration (mean difference = −1.8 days) and a smaller incidence of coronary artery anomalies in the initial-stage KD (odds ratio = 0.50, 95% confidence interval: 0.18–1.37) High-dosage IVIG (2 g min) + pulse steroid in comparison with high-dosage IVIG (2 g min) alone showed a better rate of fever decline in refractory-stage KD (odds ratio = 0.04, 95% confidence interval: 0.00–0.43). High-dosage IVIG (2 g min) + ciclosporin in respect to high-dosage IVIG alone (2 g min) exhibited a smaller incidence of coronary artery anomalies in refractory-stage KD (odds ratio = 0.05, 95% confidence interval: 0.00–1.21) Infliximab in comparison with high-dosage IVIG (2 g min) alone improved resolution in refractory-stage KD (odds ratio = 0.20, 95% confidence interval: 0.07–0.62) |
| Huang H et al. [101] | 2022 | Retrospective and prospective cohort study | To develop a nomogram predictive for IVIG resistance enrolling retrospectively 1293 children with KD in eastern China, with IVIG resistance defined as persistent or recrudescent fever ≥36 h after the stop of IVIG infusion | Low haemoglobin, high percentage of neutrophils, high C-reactive protein level, high platelet count, low serum albumin, high serum sodium, high serum alkaline phosphatase, low coronary artery damage, and uncomplete Kawasaki disease represent risk factors for IVIG resistance. The nomogram based on these factors showed a good discriminatory power (area under curve (AUC), 0.75), sensitivity (0.74) and specificity (0.64). In the prospective (209 patients) and external (205 patients) data, the AUC was 0.83 and 0.66, respectively, the sensitivity was 1 and 0.86, respectively, and the specificity was 0.60 and 0.49, respectively. |
| Hamada H et al. [102] | 2019 | Randomized controlled, open-label, blinded-endpoints, phase 3 trial | To compare safety and efficacy of IVIG + ciclosporin (5 mg/kg per day for 5 days) and IVIG in 175 KD patients at high risk for IVIG resistance according to Kobayashi’s scoring system (PMID: 16735679). The primary outcome was incidence of coronary artery anomalies during the 3-month trial. | Incidence of coronary artery anomalies was lower in the IVIG + ciclosporin group than in the IVIG group—with a significant risk ratio (0.46; 95% confidence interval 0.25–0.86; p = 0.010)—in KD patients at high risk for IVIG resistance, with no difference as concerns incidence of adverse effects |
| Dionne A et al. [103] | 2018 | Monocentric retrospective cohort study | To compare 154 KD children with and without a concomitant infection in terms of need for a second IVIG course, C-reactive protein level, and prevalence of coronary complications | KD children with a concomitant infection showed a higher prevalence of IVIG resistance (p = 0.05), of need for a second IVIG course (p = 0.04), and higher inflammatory markers prior to (p = 0.04) and after (p = 0.003) IVIG administration. Prevalence of coronary complications was not statistically different between the two groups |
| Kaya Akca U et al. [104] | 2018 | Monocentric retrospective cohort study | To compare different prognostic scoring system predictive for IVIG resistance in Turkish children with KD | Low platelet count and increased serum gamma-glutamyl transferase levels were unfavorable factors for response to IVIG therapy |
| Lin MT et al. [105] | 2015 | Retrospective cohort study | Evaluation of IVIG effectiveness in terms of coronary heart complication reversal in patients diagnosed with KD between the groups with and without IVIG | Insufficient evidence about the effectiveness of IVIG in KD in terms of coronary heart complication reversal, with a significant improvement in the early subgroup but not in the late subgroup |
| Newburger JW et al. [106] | 1986 | Multicenter randomized trial | Comparison between IVIG + aspirin and aspirin only in terms of prevalence of coronary–artery abnormalities at a timepoint of 2 and 7 weeks after enrollment | IVIG safely and effectively reduces, in a statistically significant manner, the rate of coronary–artery abnormalities if administered early in the course of KD |
| Furusho K et al. [107] | 1983 | Case–control study | Comparison between IVIG and aspirin in terms of duration of fever, time to phlogosis indexes negativization, and aneurysm formation | IVIG prevents coronary aneurysm formation, providing an anti-inflammatory effect reducing significantly fever duration and time to negativization of phlogosis indexes |
| Multisystem inflammatory syndrome in children (MIS-C) | ||||
| Mahmoud S et al. [108] | 2022 | Review | An overview about the available evidence and recommendations for MIS-C treatment in children and adolescents | IVIG ± glucocorticoids represent the first-tier immunomodulatory therapy. In case of refractoriness, a switch to biologic agents such as anakinra, tocilizumab, and infliximab is warranted |
| Son MB et al. [109] | 2021 | Comparative study | To compare the effectiveness of IVIG + steroids and IVIG alone in 518 patients with MIS-C <21 years of life, considering cardiac dysfunction in terms of need for vasopressors on or after day 2 of therapy as primary outcome and adjunctive treatment (glucocorticoids in patients receiving IVIG alone, a second course of IVIG, or a biologic) on or after day 1, and fever on or after day 2, peristent or recurrent, as secondary outcomes | IVIG + steroids therapy carries a lower risk of new or persistent cardiac dysfunction than IVIG only. |
| Ouldali N et al. [110] | 2021 | Retrospective cohort study | Comparison between IVIG + methylprednisolone and IVIG alone in terms of fever duration | IVIG + methylprednisolone treatment significantly reduces rate of unresponsiveness, described as persistent fever after 48 h of first-line therapy or fever relapse within a week |
| Belhadjer Z et al. [111] | 2020 | Observational study | Comparison between IVIG + methylprednisolone and IVIG alone in terms of recovery of cardiac function | IVIG + methylprednisolone treatment significantly reduces time to recovery, described as isovolumic relaxation time >90 milliseconds for diastolic function and left ventricle ejection fraction >55% |
| Polyarthritis (rheumatoid factor positive) | ||||
| Giannini EH et al. [112] | 1996 | Clinical trial (randomized, withdrawal, double-blind, placebo-controlled) | Evaluation about efficacy and safety of IVIG therapy in the treatment of resistant polyarticular juvenile idiopathic arthritis | Three-fourths of patients with poly-JIA experienced clinical improvement with IVIG during open administration, more likely in those with a history of disease shorter than 3 years than those with a more prolonged illness (>5 years). The beneficial effect was short after discontinuation of IVIG therapy |
| Systemic juvenile idiopathic arthritis (JIA) | ||||
| Uziel Y et al. [113] | 1996 | Clinical trial (open-label) | To assess the short- and long-term consequences of IVIG therapy among 27 patients affected by systemic onset juvenile idiopathic arthritis (SOJIA) |
|
| Silverman ED et al. [114] | 1994 | Clinical trial (multicenter, randomized, double-blind, placebo-controlled) | Evaluation of safety and efficacy of IVIG therapy in 31 patients with juvenile idiopathic arthritis (dosage of 1.5 g/kg every 2 weeks for 2 months, then every month for 4 months). Comparison with placebo (0.1% albumin) |
|
| Silverman ED et al. [115] | 1990 | Clinical trial (open-label) | Evaluation of HD-IVIG treatment in eight patients affected by systemic juvenile idiopathic arthritis considering articular and extraarticular symptoms, laboratory exams, corticosteroid therapy, and global evaluation | Improvement in articular and extraarticular symptoms; prednisone dosage; blood exams (hemoglobin, albumin, serum immunoglobulin, platelet count, and erythrocyte sedimentation rate levels) |
| Prieur AM et al. [116] | 1990 | Clinical trial (open-label) | Evaluation of HD-IVIG treatment in 16 patients with severe forms of juvenile chronic arthritis | Improvement in laboratory abnormalities. No difference among short- and long-term therapy |
| Systemic lupus erythematosus (SLE) | ||||
| Shi N et al. [117] | 2021 | Case report | Clinical case of an 11-year-old girl presenting Childhood-Onset SLE (cSLE)-associated MAS and neuroimaging anomalies as onset symptoms, treated with HD methylprednisolone, and cyclophosphamide and HD-IVIG every two weeks. | The patient showed clinical and neuroimaging improvement on day 25. |
| Akca U et al. [118] | 2021 | Retrospective multicenter study | To assess hematological features in pediatric SLE patients |
|
| Baglan E et al. [119] | 2021 | Case report | Clinical case of a boy of 10 years of age with cSLE showing chorea and delirium, who underwent Zipper method treatment (consecutive PLEX and IVIG) given the resistance to conventional therapy and rapidly progressing neurological involvement | First cSLE case involving central nervous system, showing resistance to steroids and cyclophosphamide, and resolved by the Zipper method |
| Lube GE et al. [120] | 2016 | Retrospective multicenter cohort study | Evaluation of prevalence, clinical manifestations, laboratory exams, and outcomes in a childhood-onset SLE cohort with Evans Syndrome at diagnosis |
|
| Brogna C et al. [121] | 2016 | Case report | Clinical report of a boy of 7 years of age showing severe neuropsychiatric lupus erythematosus provoked by reactivation of EBV cerebral infection, effectively responding to IVIG |
|
| Friedman DL et al. [122] | 2010 | Prospective multicenter open-label study | To assess the function of IVIG as prevention treatment for congenital heart block, given its potential role in reducing maternal autoantibody levels and fetal inflammatory activation | IVIG protocol was completed in twenty women before the limit of 3 cases of advanced congenital heart block was observed. No signs of neonatal lupus were observed in sixteen children at birth. No substantial variations in maternal antibody levels were noticed. There were no safety issues |
| Pisoni CL et al. [123] | 2010 | Prospective multicenter observational study | Evaluation of IVIG therapy in congenital heart block prevention among neonates born from high-risk pregnancies | IVIG therapy (dosed as follows: 400 mg/kg at weeks 12, 15, 18, 21, and 24 of pregnancy) did not demonstrate any effect as a prophylaxis for congenital heart block in high-risk women |
| Miyagawa S et al. [124] | 2000 | Case report | Clinical case of a girl of 7 years of age with SLE and probable diagnosis of Sjögren’s syndrome who developed Guillain-Barré syndrome 6 years after diagnosis | The patient condition resolved with aggressive treatment, involving HD steroids, PLEX, and IVIG therapy |
| Major Adverse Event | Monitoring and Treatment | Preventive Measures | Cost-Effective Commercial Preparations * |
|---|---|---|---|
| Acute renal failure [237,238,239] | Monitoring: Urine output, creatinine, and blood urea nitrogen dosage before and after IVIG employment. Treatment: Immediate IVIG cessation. Intravenous hydration post infusion. Dialysis | Avoidance of sucrose-stabilized (e.g., Carimune, Cytogam, Gammar-IV, Sandoglobulin IVIG) and/or hyperosmolar (e.g., Asceniv, Bivigam, Gammagard S/D, Gammaplex 5%, Venoglobulin-I 10% IVIG; Cutaquig or Xembify SCIG) products, especially in case of concomitant nephrotoxic therapies (e.g., inhibitors of the renin-angiotensin system, NSAIDs), diabetes mellitus, pre-existing renal disease, sepsis, hypovolemia. Prehydration | CUVITRU SCIG 200 mg/mL 5 g: $459.54 = 415.90 EUR Hizentra SCIG 200 mg/mL 5 g: $500.99 = 453.86 EUR HYQVIA SCIG 100 mg/mL 5 g: $500.99 = 453.86 EUR Privigen IVIG 100 mg/mL 5 g: $500.99 = 453.86 EUR Gammagard IVIG 5 g/96 mL 5 g: $500.99 = 453.86 EUR Flebogamma IVIG 50 mg/mL 5 g: $500.99 = 453.86 EUR Octagam 5% IVIG 50 mg/mL 5 g: $500.99 = 453.86 EUR Gamunex-C IVIG/SCIG 5 g/50 mL 5 g: $768.35 = 695.37 EUR Gammagard liquid SCIG 5 g/50 mL 5 g: $897.55 = 812.30 EUR Gammaked IVIG/SCIG 1 g /10 mL 5 g: $998.32 = 904.01 EUR PANZYGA IVIG 100 mg/mL 5 g: $1087.88 = 985.20 EUR Gammaplex 10% IVIG 50 mg/mL 5 g: $1091.09 = 988.38 EUR Gamimune N 5%–10% IVIG (out of production) Venoglobulin-I 5% IVIG (out of production) Venoglobulin-S IVIG (out of production) |
| Anaphylaxis [238,239,240,241] | Treatment: Immediate IVIG cessation. | Employment of IgA-depleted products (e.g., Gammagard S/D or Gammaplex IVIG; Cutaquig or Xembify SCIG even better), although the presence of anti-IgA antibodies is neither a necessary nor a sufficient cause of transfusion-related anaphylaxis | Cutaquig SCIG 165 mg/mL 5 g: $637.62 = 577.64 EUR Xembify SCIG 1 g/5 mL–4 g/20 mL 5 g: $946.69 = 857.17 EUR Gammaplex IVIG 50 mg/mL 5 g: $1091.09 = 988.38 EUR Gammagard S/D IVIG 5 g/96 mL 5 g: $1144.79 = 1036.08 EUR |
| Hemolytic anemia [125,238,239] | Monitoring: Hemoglobin dosage up to 96 h after IVIG. Treatment: Immediate IVIG cessation. Adequate hydration. Red blood cell transfusions. B12 and folate supplementation. Plasmapheresis or hemodialysis as rescue therapies. | Avoidance of amino acid-stabilized products (e.g., Asceniv, Bivigam, Gammagard Liquid-S/D, Gammaked, Gammaplex 10%, Gamunex-C, PANZYGA or Privigen IVIG; CUVITRU, Gammagard Liquid, Gammaked, Gamunex-C, Hizentra, HYQVIA, Xembify SCIG), especially in the case of non-O blood group recipients or concomitant assumption of NSAIDs, gastro-intestinal medications, and broad-spectrum antibiotics. Prehydration | Flebogamma IVIG 50 mg/mL 5 g: $500.99 = 453.86 EUR Octagam 5% IVIG 50 mg/mL 5 g: $500.99 = 453.86 EUR Cutaquig SCIG 165 mg/mL 5 g: $637.62 = 577.64 EUR Gammaplex 5% IVIG 50 mg/mL 5 g: $1091.09 = 988.38 EUR Cytogam IVIG 50 mg/mL 5 g: $3718.92 = 3368.65 EUR Carimune IVIG (out of production) Gamimune N 5% IVIG (out of production) Gammar-IV IVIG (out of production) Venoglobulin-I IVIG (out of production) Venoglobulin-S IVIG (out of production) |
| Myocardial infarction, coronary spastic angina (reported only in non-pediatric patients) [238,239,242,243] | Treatment: Immediate IVIG cessation. | Avoidance of high-sodium-containing (e.g., Asceniv, Bivigam, Gammagard S/D, Gammaplex 5%, Venoglobulin-I 10%, Gammar-IV 10% IVIG) and hyperosmolar (e.g., Carimune 6%–12% IVIG; Cutaquig or Xembify SCIG) products, particularly in case of pre-existent cardiac dysfunction and/or hypertension. | Flebogamma IVIG 50 mg/mL 5 g: $500.99 = 453.86 EUR Octagam 5% IVIG 50 mg/mL 5 g: $500.99 = 453.86 EUR Gamunex-C IVIG 100 mg/mL 5 g: $730.38 = 661.02 EUR Gammagard liquid IVIG 5 g/50 mL 5 g: $897.55 = 812.30 EUR Gammaked IVIG 1 g/10 mL 5 g: $998.32 = 904.01 EUR PANZYGA IVIG 100 mg/mL 5 g: $1087.88 = 985.20 EUR Gammaplex 10% IVIG 50 mg/mL 5 g: $1091.09 = 988.38 EUR Cytogam IVIG 50 mg/mL 5 g: $3718.92 = 3368.65 EUR Carimune 3% IVIG (out of production) Gamimune N 5%–10% IVIG (out of production) Gammar-IV 5% IVIG (out of production) Venoglobulin-I 5% IVIG (out of production) Venoglobulin-S IVIG (out of production) |
| Thromboembolic events [238,239,244] | Monitoring: Pre and post infusion D-dimer levels Treatment: Immediate IVIG cessation or dose fragmentation and/or lower infusion rate. Discuss low-molecular-weight heparin (1 mg/kg/dose twice a day at an anticoagulation dose). Interruption of pro-thrombotic agents (e.g., oral contraceptive). | Removal of pro-thrombotic factors, such as obesity and oral contraceptives. | |
| Transfusion-related acute lung injury (TRALI) [238,239,245,246,247] | Treatment: Immediate IVIG cessation. Oxygen supply. Ventilation. Extracorporeal membrane oxygenation. Intravenous ascorbic acid (2.5 g/6 h for 96 h). | No robust evidence available on preventive strategies, although leukoreduction and pathogen reduction technologies, removing membrane lipid structures, and pathogenic nucleic acids in donor samples could have a role in preventing TRALI |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conti, F.; Moratti, M.; Leonardi, L.; Catelli, A.; Bortolamedi, E.; Filice, E.; Fetta, A.; Fabi, M.; Facchini, E.; Cantarini, M.E.; et al. Anti-Inflammatory and Immunomodulatory Effect of High-Dose Immunoglobulins in Children: From Approved Indications to Off-Label Use. Cells 2023, 12, 2417. https://doi.org/10.3390/cells12192417
Conti F, Moratti M, Leonardi L, Catelli A, Bortolamedi E, Filice E, Fetta A, Fabi M, Facchini E, Cantarini ME, et al. Anti-Inflammatory and Immunomodulatory Effect of High-Dose Immunoglobulins in Children: From Approved Indications to Off-Label Use. Cells. 2023; 12(19):2417. https://doi.org/10.3390/cells12192417
Chicago/Turabian StyleConti, Francesca, Mattia Moratti, Lucia Leonardi, Arianna Catelli, Elisa Bortolamedi, Emanuele Filice, Anna Fetta, Marianna Fabi, Elena Facchini, Maria Elena Cantarini, and et al. 2023. "Anti-Inflammatory and Immunomodulatory Effect of High-Dose Immunoglobulins in Children: From Approved Indications to Off-Label Use" Cells 12, no. 19: 2417. https://doi.org/10.3390/cells12192417
APA StyleConti, F., Moratti, M., Leonardi, L., Catelli, A., Bortolamedi, E., Filice, E., Fetta, A., Fabi, M., Facchini, E., Cantarini, M. E., Miniaci, A., Cordelli, D. M., Lanari, M., Pession, A., & Zama, D. (2023). Anti-Inflammatory and Immunomodulatory Effect of High-Dose Immunoglobulins in Children: From Approved Indications to Off-Label Use. Cells, 12(19), 2417. https://doi.org/10.3390/cells12192417