
Effects of Microbeam Irradiation on Rodent Esophageal Smooth Muscle Contraction

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Preparation of Isolated Rat Esophageal Segments for Isometric Contraction Measurement in the Organ Bath
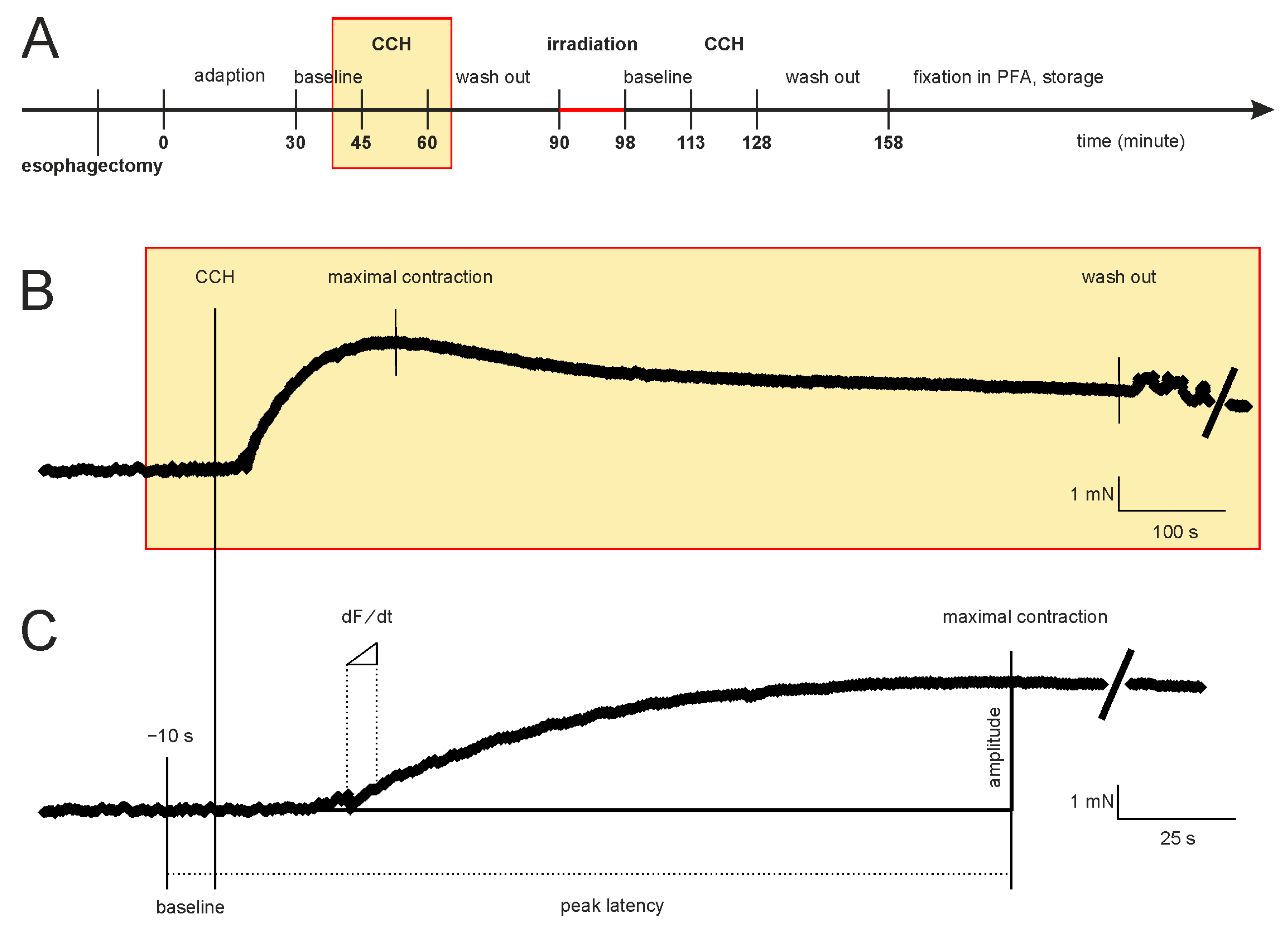
2.2. Time Course of the Experiments
2.3. Calculation of Parameters for Characterization of Isometric Contraction
2.4. Irradiation Protocol
2.5. Immunofluorescence Labelling
2.6. Statistical Analysis
3. Results
3.1. Concentration-Response Relationship for Carbachol
3.2. The Three Experimental Groups Were Homogeneously Randomised
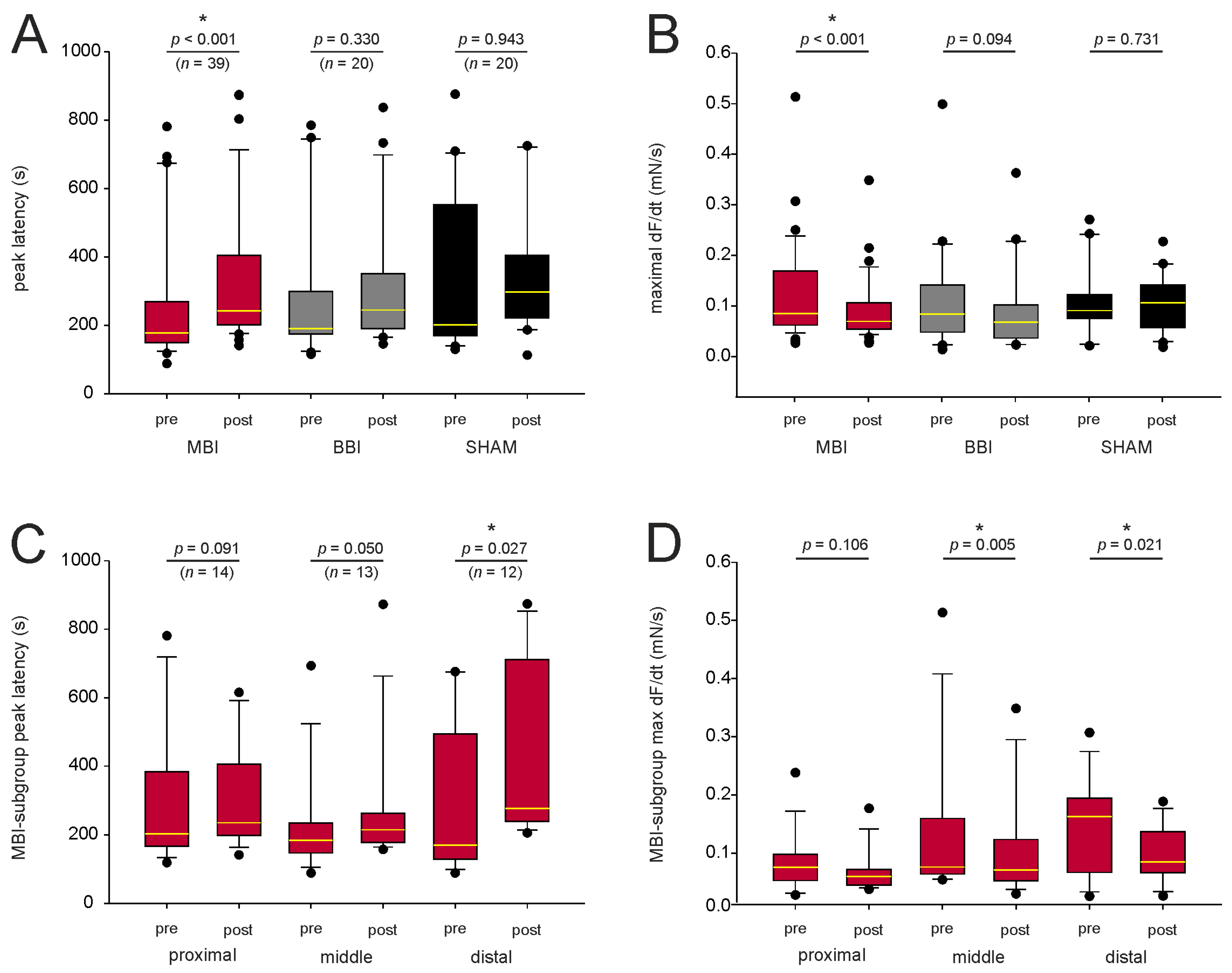
3.3. MBI Significantly Increased Peak Latency and Decreased Maximal Force Change
3.4. Subgroup Analysis of the Peak Latency and Maximal Force Change
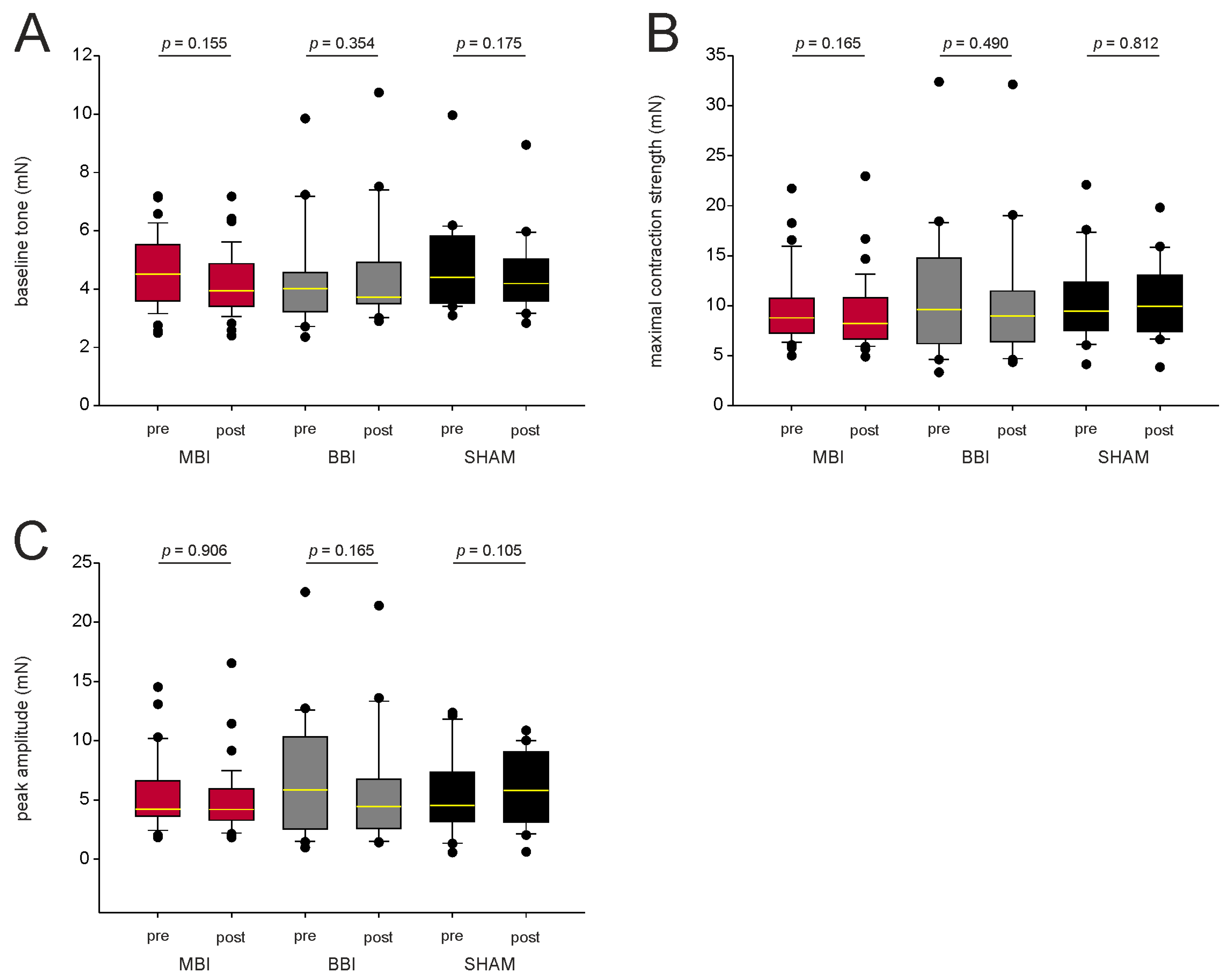
3.5. MBI Did Not Affect Baseline Tone, Maximal Contraction Strength, and Peak Amplitude
3.6. Dosimetric Characteristics
3.7. Visualization of Dose Deposition in the Esophagus after Microbeam Irradiation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Simone, C.B. Thoracic Radiation Normal Tissue Injury. Semin. Radiat. Oncol. 2017, 27, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.; Movsas, B. Radiation esophagitis: Predictive factors and preventive strategies. Semin. Radiat. Oncol. 2004, 14, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.; Movsas, B. Radiation pneumonitis and esophagitis in thoracic irradiation. Cancer Treat. Res. 2006, 128, 43–64. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, F.B.; Geinitz, H.; Feldmann, H.J. Therapy and prophylaxis of acute and late radiation-induced sequelae of the esophagus. Strahlenther. Onkol. 1998, 174 (Suppl. S3), 78–81. [Google Scholar] [PubMed]
- Murro, D.; Jakate, S. Radiation esophagitis. Arch. Pathol. Lab. Med. 2015, 139, 827–830. [Google Scholar] [CrossRef]
- Hirota, S.; Tsujino, K.; Hishikawa, Y.; Watanabe, H.; Kono, K.; Soejima, T.; Obayashi, K.; Takada, Y.; Kono, M.; Abe, M. Endoscopic findings of radiation esophagitis in concurrent chemoradiotherapy for intrathoracic malignancies. Radiother. Oncol. 2001, 58, 273–278. [Google Scholar] [CrossRef]
- Yeoh, E.; Holloway, R.H.; Russo, A.; Tippett, M.; Bermingham, H.; Chatterton, B.; Horowitz, M. Effects of mediastinal irradiation on oesophageal function. Gut 1996, 38, 166–170. [Google Scholar] [CrossRef]
- Coia, L.R.; Myerson, R.J.; Tepper, J.E. Late effects of radiation therapy on the gastrointestinal tract. Int. J. Radiat. Oncol. Biol. Phys. 1995, 31, 1213–1236. [Google Scholar] [CrossRef]
- Gaze, M.N.; Wilson, J.A.; Gilmour, H.M.; MacDougall, R.H.; Maran, A.G. The effect of laryngeal irradiation on pharyngoesophageal motility. Int. J. Radiat. Oncol. Biol. Phys. 1991, 21, 1315–1320. [Google Scholar] [CrossRef]
- Seeman, H.; Gates, J.A.; Traube, M. Esophageal motor dysfunction years after radiation therapy. Dig. Dis. Sci. 1992, 37, 303–306. [Google Scholar] [CrossRef]
- Vitton, V.; Andrianjafy, C.; Luciano, L.; Gonzalez, J.-M.; Padovani, L. Radio-induced esophageal motility disorders: An unrecognized diagnosis. Cancer Radiother. 2021, 25, 249–253. [Google Scholar] [CrossRef]
- Goldstein, H.M.; Rogers, L.F.; Fletcher, G.H.; Dodd, G.D. Radiological manifestations of radiation-induced injury to the normal upper gastrointestinal tract. Radiology 1975, 117, 135–140. [Google Scholar] [CrossRef] [PubMed]
- LaManna, M.M.; Parker, J.A.; Wolodzko, J.G.; Zekavat, P.P.; Popky, G.L. Radionuclide esophageal and intestinal transit scintigraphy in patients undergoing radiation therapy. Radiat. Med. 1985, 3, 13–16. [Google Scholar] [PubMed]
- Lepke, R.A.; Libshitz, H.I. Radiation-induced injury of the esophagus. Radiology 1983, 148, 375–378. [Google Scholar] [CrossRef]
- Brandt-Mainz, K.; Von Mallek, D.; Pöttgen, C.; Eising, E.G.; Bockisch, A.; Stuschke, M.; Sack, H. Parametric oesophageal multiple swallow scintigraphy for validation of dysphageal symptoms during external beam irradiation of mediastinal tumours. Eur. J. Nucl. Med. 2001, 28, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Sasso, G.; Rambaldi, P.; Sasso, F.S.; Cuccurullo, V.; Murino, P.; Puntieri, P.; Marsiglia, H.R.; Mansi, L. Scintigraphic evaluation of oesophageal transit during radiotherapy to the mediastinum. BMC Gastroenterol. 2008, 8, 51. [Google Scholar] [CrossRef]
- Türkölmez, S.; Atasever, T.; Akmansu, M. Effects of radiation therapy on oesophageal transit in patients with inner quadrant breast tumour. Nucl. Med. Commun. 2005, 26, 721–726. [Google Scholar] [CrossRef]
- Werner-Wasik, M.; Yorke, E.; Deasy, J.; Nam, J.; Marks, L.B. QUANTEC Radiation dose-volume effects in the esophagus. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S86–S93. [Google Scholar] [CrossRef]
- Schültke, E.; Fiedler, S.; Menk, R.H.; Jaekel, F.; Dreossi, D.; Casarin, K.; Tromba, G.; Bartzsch, S.; Kriesen, S.; Hildebrandt, G.; et al. Perspectives for microbeam irradiation at the SYRMEP beamline. J. Synchrotron Radiat. 2021, 28, 410–418. [Google Scholar] [CrossRef]
- Schültke, E.; Balosso, J.; Breslin, T.; Cavaletti, G.; Djonov, V.; Esteve, F.; Grotzer, M.; Hildebrandt, G.; Valdman, A.; Laissue, J. Microbeam radiation therapy—Grid therapy and beyond: A clinical perspective. Br. J. Radiol. 2017, 90, 20170073. [Google Scholar] [CrossRef]
- Favaudon, V.; Caplier, L.; Monceau, V.; Pouzoulet, F.; Sayarath, M.; Fouillade, C.; Poupon, M.-F.; Brito, I.; Hupé, P.; Bourhis, J.; et al. Ultrahigh dose-rate FLASH irradiation increases the differential response between normal and tumor tissue in mice. Sci. Transl. Med. 2014, 6, 245ra93. [Google Scholar] [CrossRef] [PubMed]
- Favaudon, V.; Fouillade, C.; Vozenin, M.-C. Radiothérapie «flash» à très haut débit de dose: Un moyen d’augmenter l’indice thérapeutique par minimisation des dommages aux tissus sains? (Ultrahigh dose-rate, “flash” irradiation minimizes the side-effects of radiotherapy). Cancer Radiother. 2015, 19, 526–531. [Google Scholar] [CrossRef] [PubMed]
- Laissue, J.A.; Blattmann, H.; Wagner, H.P.; Grotzer, M.A.; Slatkin, D.N. Prospects for microbeam radiation therapy of brain tumours in children to reduce neurological sequelae. Dev. Med. Child Neurol. 2007, 49, 577–581. [Google Scholar] [CrossRef]
- Bouchet, A.; Lemasson, B.; Le Duc, G.; Maisin, C.; Bräuer-Krisch, E.; Siegbahn, A.; Renaud, L.; Khalil, E.; Rémy, C.; Poillot, C.; et al. Preferential effect of synchrotron microbeam radiation therapy on intracerebral 9L gliosarcoma vascular networks. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 1503–1512. [Google Scholar] [CrossRef] [PubMed]
- Bouchet, A.; Bräuer-Krisch, E.; Prezado, Y.; El Atifi, M.; Rogalev, L.; Le Clec’H, C.; Laissue, J.A.; Pelletier, L.; Le Duc, G. Better Efficacy of Synchrotron Spatially Microfractionated Radiation Therapy Than Uniform Radiation Therapy on Glioma. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 1485–1494. [Google Scholar] [CrossRef]
- Potez, M.; Bouchet, A.; Flaender, M.; Rome, C.; Collomb, N.; Grotzer, M.; Krisch, M.; Djonov, V.; Balosso, J.; Brun, E.; et al. Synchrotron X-ray Boost Delivered by Microbeam Radiation Therapy after Conventional X-ray Therapy Fractionated in Time Improves F98 Glioma Control. Int. J. Radiat. Oncol. Biol. Phys. 2020, 107, 360–369. [Google Scholar] [CrossRef]
- Schültke, E.; Juurlink, B.H.; Ataelmannan, K.; Laissue, J.; Blattmann, H.; Bräuer-Krisch, E.; Bravin, A.; Minczewska, J.; Crosbie, J.; Taherian, H.; et al. Memory and survival after microbeam radiation therapy. Eur. J. Radiol. 2008, 68, S142–S146. [Google Scholar] [CrossRef]
- Schültke, E.; Bräuer-Krisch, E.; Blattmann, H.; Requardt, H.; Laissue, J.A.; Hildebrandt, G. Survival of rats bearing advanced intracerebral F 98 tumors after glutathione depletion and microbeam radiation therapy: Conclusions from a pilot project. Radiat. Oncol. 2018, 13, 89. [Google Scholar] [CrossRef]
- Jaekel, F.; Bräuer-Krisch, E.; Bartzsch, S.; Laissue, J.; Blattmann, H.; Scholz, M.; Soloviova, J.; Hildebrandt, G.; Schültke, E. Microbeam Irradiation as a Simultaneously Integrated Boost in a Conventional Whole-Brain Radiotherapy Protocol. Int. J. Mol. Sci. 2022, 23, 8319. [Google Scholar] [CrossRef]
- Adam, J.-F.; Balosso, J.; Bayat, S.; Berkvens, P.; Berruyer, G.; Bräuer-Krisch, E.; Brochard, T.; Chamel, G.; Desagneaux, A.; Drevon-Gaud, R.; et al. Toward Neuro-Oncologic Clinical Trials of High-Dose-Rate Synchrotron Microbeam Radiation Therapy: First Treatment of a Spontaneous Canine Brain Tumor. Int. J. Radiat. Oncol. Biol. Phys. 2022, 113, 967–973. [Google Scholar] [CrossRef]
- Schültke, E.; Bayat, S.; Bartzsch, S.; Bräuer-Krisch, E.; Djonov, V.; Fiedler, S.; Fernandez-Palomo, C.; Jaekel, F.; Pellicioli, P.; Trappetti, V.; et al. A Mouse Model for Microbeam Radiation Therapy of the Lung. Int. J. Radiat. Oncol. Biol. Phys. 2020, 110, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Trappetti, V.; Fernandez-Palomo, C.; Smyth, L.; Klein, M.; Haberthür, D.; Butler, D.; Barnes, M.; Shintani, N.; de Veer, M.; Laissue, J.A.; et al. Synchrotron Microbeam Radiation Therapy for the Treatment of Lung Carcinoma: A Preclinical Study. Int. J. Radiat. Oncol. Biol. Phys. 2021, 111, 1276–1288. [Google Scholar] [CrossRef] [PubMed]
- Schültke, E.; Lerch, M.; Kirschstein, T.; Lange, F.; Porath, K.; Fiedler, S.; Davis, J.; Paino, J.; Engels, E.; Barnes, M.; et al. Modification of the Langendorff system of the isolated beating heart for experimental radiotherapy at a synchrotron: 4000 Gy in a heart beat. J. Synchrotron Radiat. 2022, 29, 1027–1032. [Google Scholar] [CrossRef] [PubMed]
- Lange, F.; Kirschstein, T.; Davis, J.; Paino, J.; Barnes, M.; Klein, M.; Porath, K.; Stöhlmacher, P.; Fiedler, S.; Frank, M.; et al. Microbeam irradiation of the beating rodent heart: An ex vivo study of acute and subacute effects on cardiac function. Int. J. Radiat. Oncol. Biol. Phys. 2022, 114, 143–152. [Google Scholar] [CrossRef]
- Kirschstein, T.; Rehberg, M.; Bajorat, R.; Tokay, T.; Porath, K.; Köhling, R. High K+-induced contraction requires depolarization-induced Ca2+ release from internal stores in rat gut smooth muscle. Acta Pharmacol. Sin. 2009, 30, 1123–1131. [Google Scholar] [CrossRef]
- Kirschstein, T.; Protzel, C.; Porath, K.; Sellmann, T.; Köhling, R.; Hakenberg, O.W. Age-dependent contribution of Rho kinase in carbachol-induced contraction of human detrusor smooth muscle in vitro. Acta Pharmacol. Sin. 2014, 35, 74–81. [Google Scholar] [CrossRef]
- Wilde, F.; Ogurreck, M.; Greving, I.; Hammel, J.U.; Beckmann, F.; Hipp, A.; Lottermoser, L.; Khokhriakov, I.; Lytaev, P.; Dose, T.; et al. Micro-CT at the imaging beamline P05 at PETRA III. In Proceedings of the 12th International Conference on Synchrotron Radiation Instrumentation, New York, NY, USA, 6–10 July 2015; p. 30035. [Google Scholar]
- Buhr, H.; Büermann, L.; Gerlach, M.; Krumrey, M.; Rabus, H. Measurement of the mass energy-absorption coefficient of air for X-rays in the range from 3 to 60 keV. Phys. Med. Biol. 2012, 57, 8231–8247. [Google Scholar] [CrossRef]
- Veatch, W.; Okada, S. Radiation-induced breaks of DNA in cultured mammalian cells. Biophys. J. 1969, 9, 330–346. [Google Scholar] [CrossRef][Green Version]
- Rogakou, E.P.; Pilch, D.R.; Orr, A.H.; Ivanova, V.S.; Bonner, W.M. DNA double-stranded breaks induce histone H2AX phosphorylation on serine 139. J. Biol. Chem. 1998, 273, 5858–5868. [Google Scholar] [CrossRef]
- Kuo, L.J.; Yang, L.-X. Gamma-H2AX—A novel biomarker for DNA double-strand breaks. In Vivo 2008, 22, 305–309. [Google Scholar]
- Fernandez-Palomo, C.; Mothersill, C.; Bräuer-Krisch, E.; Laissue, J.; Seymour, C.; Schültke, E. γ-H2AX as a marker for dose deposition in the brain of wistar rats after synchrotron microbeam radiation. PLoS ONE 2015, 10, e0119924. [Google Scholar] [CrossRef] [PubMed]
- Giglio, D.; Podmolíková, L.; Tobin, G. Changes in the Neuronal Control of the Urinary Bladder in a Model of Radiation Cystitis. J. Pharmacol. Exp. Ther. 2018, 365, 327–335. [Google Scholar] [CrossRef] [PubMed]
- McDonnell, B.M.; Buchanan, P.J.; Prise, K.M.; McCloskey, K.D. Acute radiation impacts contractility of guinea-pig bladder strips affecting mucosal-detrusor interactions. PLoS ONE 2018, 13, e0193923. [Google Scholar] [CrossRef] [PubMed]
- Turner, A.C.; Powers, S.A.; Odom, M.R.; Pak, E.S.; Ashcraft, K.A.; Koontz, B.F.; Hannan, J.L. Impact of prostatic radiation therapy on bladder contractility and innervation. Neurourol. Urodyn. 2021, 40, 1470–1478. [Google Scholar] [CrossRef]
- Lorenzi, B.; Brading, A.F.; Martellucci, J.; Cetta, F.; Mortensen, N.J.M. Short-term effects of neoadjuvant chemoradiotherapy on internal anal sphincter function: A human in vitro study. Dis. Colon Rectum 2012, 55, 465–472. [Google Scholar] [CrossRef]
- Molls, M.; Stadler, P.; Becker, A.; Feldmann, H.J.; Dunst, J. Relevance of oxygen in radiation oncology. Mechanisms of action, correlation to low hemoglobin levels. Strahlenther. Onkol. 1998, 174 (Suppl. S4), 13–16. [Google Scholar]
- Frerker, B.; Rohde, M.; Müller, S.; Bien, C.G.; Köhling, R.; Kirschstein, T. Distinct Effects of Stereotactically Injected Human Cerebrospinal Fluid Containing Glutamic Acid Decarboxylase Antibodies into the Hippocampus of Rats on the Development of Spontaneous Epileptic Activity. Brain Sci. 2020, 10, 123. [Google Scholar] [CrossRef]
- Mitoma, H.; Song, S.-Y.; Ishida, K.; Yamakuni, T.; Kobayashi, T.; Mizusawa, H. Presynaptic impairment of cerebellar inhibitory synapses by an autoantibody to glutamate decarboxylase. J. Neurol. Sci. 2000, 175, 40–44. [Google Scholar] [CrossRef]
- Hackert, J.K.; Müller, L.; Rohde, M.; Bien, C.G.; Köhling, R.; Kirschstein, T. Anti-GAD65 Containing Cerebrospinal Fluid Does not Alter GABAergic Transmission. Front. Cell. Neurosci. 2016, 10, 130. [Google Scholar] [CrossRef]
- Skrzypiec-Spring, M.; Grotthus, B.; Szelag, A.; Schulz, R. Isolated heart perfusion according to Langendorff---still viable in the new millennium. J. Pharmacol. Toxicol. Methods 2007, 55, 113–126. [Google Scholar] [CrossRef]
- Wuest, M.; Hecht, J.; Christ, T.; Braeter, M.; Schoeberl, C.; Hakenberg, O.W.; Wirth, M.P.; Ravens, U. Pharmacodynamics of propiverine and three of its main metabolites on detrusor contraction. Br. J. Pharmacol. 2005, 145, 608–619. [Google Scholar] [CrossRef] [PubMed]
- Mader, F.; Krause, L.; Tokay, T.; Hakenberg, O.W.; Köhling, R.; Kirschstein, T. P2Y receptor-mediated transient relaxation of rat longitudinal ileum preparations involves phospholipase C activation, intracellular Ca(2+) release and SK channel activation. Acta Pharmacol. Sin. 2016, 37, 617–628. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ackbar, R.; Malvasio, V.; Holzer, P.; Saxena, A.K. In vitro effect of bethanechol and suberyldicholine on regions of guinea pig esophagus. J. Surg. Res. 2012, 174, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Shim, J.H.; Kim, M.; Sun, Y.H.; Kwak, H.S.; Yan, X.; Choi, B.-C.; Im, C.; Sim, S.S.; Jeong, J.H.; et al. MLCK and PKC Involvements via Gi and Rho A Protein in Contraction by the Electrical Field Stimulation in Feline Esophageal Smooth Muscle. Korean J. Physiol. Pharmacol. 2010, 14, 29–35. [Google Scholar] [CrossRef]
- Park, S.Y.; Song, H.J.; Sohn, U.D. Participation of Rho-associated kinase in electrical stimulated and acetylcholine-induced contraction of feline esophageal smooth muscle. Eur. J. Pharmacol. 2009, 607, 220–225. [Google Scholar] [CrossRef]
- Stoner, G.D.; Pettis, W.; Haugen, A.; Jackson, F.; Harris, C.C. Explant culture of rat esophagus in a chemically defined medium. In Vitro 1981, 17, 681–688. [Google Scholar] [CrossRef]
- Sohn, U.D.; Cao, W.; Tang, D.-C.; Stull, J.T.; Haeberle, J.R.; Wang, C.-L.A.; Harnett, K.M.; Behar, J.; Biancani, P. Myosin light chain kinase- and PKC-dependent contraction of LES and esophageal smooth muscle. Am. J. Physiol. Gastrointest. Liver Physiol. 2001, 281, G467–G478. [Google Scholar] [CrossRef]
- Strüder, D.; Hellwig, S.; Rennau, H.; van Bonn, S.; Schraven, S.P.; Mlynski, R.; Hildebrandt, G.; Schuldt, T. Screening for irradiation vasculopathy by intima-media thickness sonography in head and neck cancer patients. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 2017–2026. [Google Scholar] [CrossRef]
- van der Sanden, B.; Bräuer-Krisch, E.; Siegbahn, E.A.; Ricard, C.; Vial, J.-C.; Laissue, J. Tolerance of arteries to microplanar X-ray beams. Int. J. Radiat. Oncol. 2010, 77, 1545–1552. [Google Scholar] [CrossRef]
- Milliat, F.; François, A.; Isoir, M.; Deutsch, E.; Tamarat, R.; Tarlet, G.; Atfi, A.; Validire, P.; Bourhis, J.; Sabourin, J.-C.; et al. Influence of endothelial cells on vascular smooth muscle cells phenotype after irradiation: Implication in radiation-induced vascular damages. Am. J. Pathol. 2006, 169, 1484–1495. [Google Scholar] [CrossRef]
- Levesque, L.; Lam, M.; Allaire, P.; Mondat, M.; Houle, S.; Beaudoin, G.; Donath, D.; Leclerc, G. Effects of radiation therapy on vascular responsiveness. J. Cardiovasc. Pharmacol. 2001, 37, 381–393. [Google Scholar] [CrossRef] [PubMed]
- Mollà, M.; Gironella, M.; Miquel, R.; Tovar, V.; Engel, P.; Biete, A.; Piqué, J.M.; Panés, J. Relative roles of ICAM-1 and VCAM-1 in the pathogenesis of experimental radiation-induced intestinal inflammation. Int. J. Radiat. Oncol. Biol. Phys. 2003, 57, 264–273. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Experimental Group | Irradiation | Pharmacological Intervention | Esophageal Segments |
|---|---|---|---|
| I | 225 ± 15 Gy | carbachol before and after MBI | proximal (n = 14) middle (n = 13) distal (n = 12) |
| II | 3.5 ± 0.5 Gy | carbachol before and after BBI | proximal (n = 6) middle (n = 8) distal (n = 6) |
| III | SHAM irradiation | carbachol before and after SHAM | proximal (n = 5) middle (n = 7) distal (n = 8) |
| Parameter | MBI | BBI | Sham | p-Value * |
|---|---|---|---|---|
| segment length (cm) | 0.48 ± 0.02 | 0.52 ± 0.04 | 0.53 ± 0.02 | 0.215 |
| baseline tone (mN) | 4.54 ± 0.19 | 4.35 ± 0.39 | 4.80 ± 0.35 | 0.327 |
| maximal contraction strength (mN) | 9.91 ± 0.59 | 10.94 ± 1.49 | 10.28 ± 0.95 | 0.939 |
| peak amplitude (mN) | 5.37 ± 0.47 | 6.59 ± 1.18 | 5.48 ± 0.74 | 0.983 |
| peak latency (s) | 260 ± 30 | 295 ± 50 | 343 ± 53 | 0.305 |
| maximal force change (mN/s) | 0.12 ± 0.02 | 0.11 ± 0.02 | 0.11 ± 0.02 | 0.770 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frerker, B.; Fiedler, S.; Kirschstein, T.; Lange, F.; Porath, K.; Sellmann, T.; Kutzner, L.; Wilde, F.; Moosmann, J.; Köhling, R.; et al. Effects of Microbeam Irradiation on Rodent Esophageal Smooth Muscle Contraction. Cells 2023, 12, 176. https://doi.org/10.3390/cells12010176
Frerker B, Fiedler S, Kirschstein T, Lange F, Porath K, Sellmann T, Kutzner L, Wilde F, Moosmann J, Köhling R, et al. Effects of Microbeam Irradiation on Rodent Esophageal Smooth Muscle Contraction. Cells. 2023; 12(1):176. https://doi.org/10.3390/cells12010176
Chicago/Turabian StyleFrerker, Bernd, Stefan Fiedler, Timo Kirschstein, Falko Lange, Katrin Porath, Tina Sellmann, Leonie Kutzner, Fabian Wilde, Julian Moosmann, Rüdiger Köhling, and et al. 2023. "Effects of Microbeam Irradiation on Rodent Esophageal Smooth Muscle Contraction" Cells 12, no. 1: 176. https://doi.org/10.3390/cells12010176
APA StyleFrerker, B., Fiedler, S., Kirschstein, T., Lange, F., Porath, K., Sellmann, T., Kutzner, L., Wilde, F., Moosmann, J., Köhling, R., Hildebrandt, G., & Schültke, E. (2023). Effects of Microbeam Irradiation on Rodent Esophageal Smooth Muscle Contraction. Cells, 12(1), 176. https://doi.org/10.3390/cells12010176