
Osteochondral Lesions of the Ankle Treated with Bone Marrow Concentrate with Hyaluronan and Fibrin: A Single-Centre Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Bone Marrow Aspirate Concentrate (BMC)
2.3. Surgical Technique
2.4. Post-Operative Protocol
2.5. Outcome Measures
2.6. Statistical Analysis
3. Results
3.1. Demographics
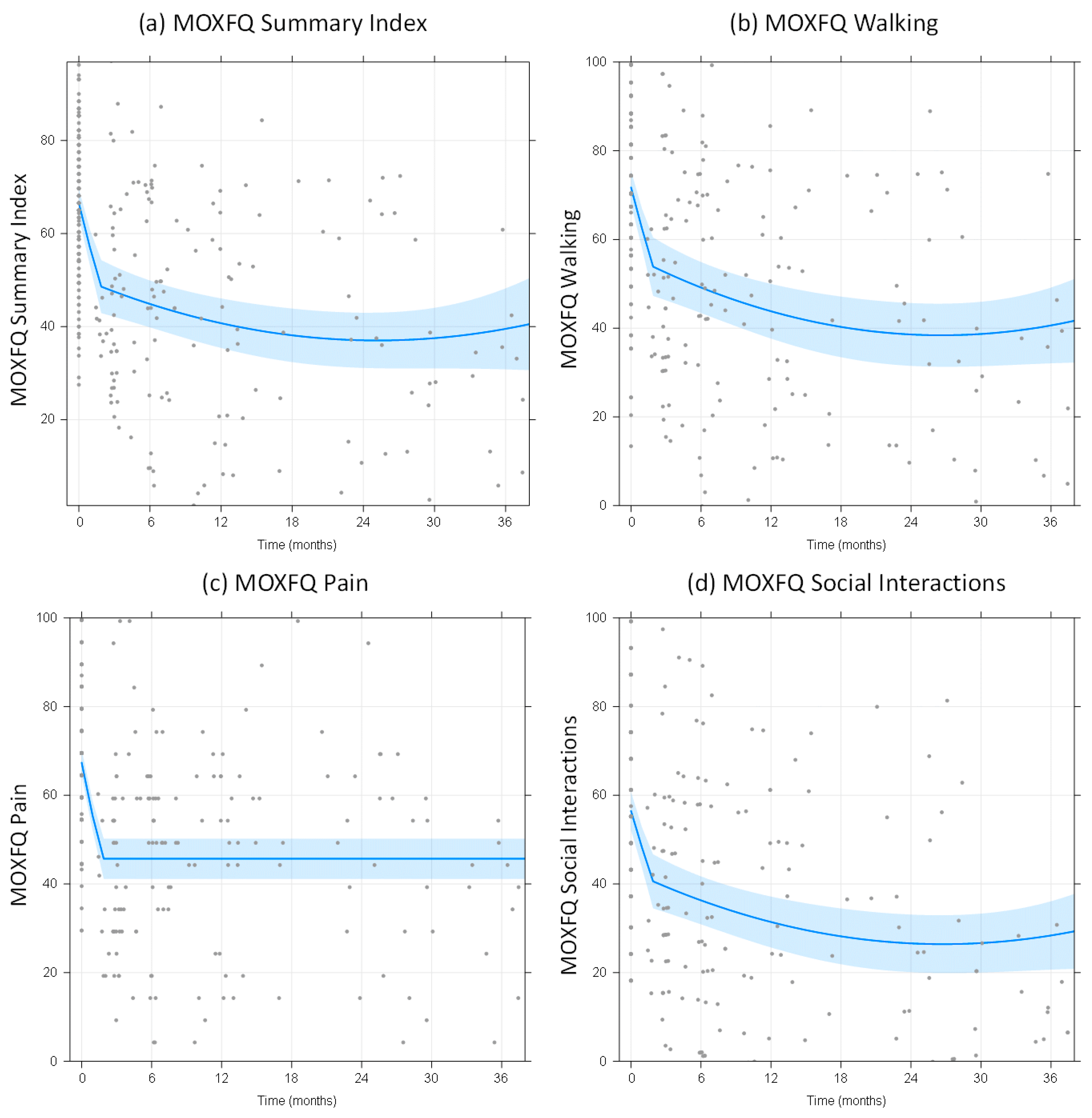
3.2. MOXFQ Scores and EQ-5D Scores (Patient-Related Outcome Measures)
3.3. Predictors of Improvement in MOXFQ-Summary Index
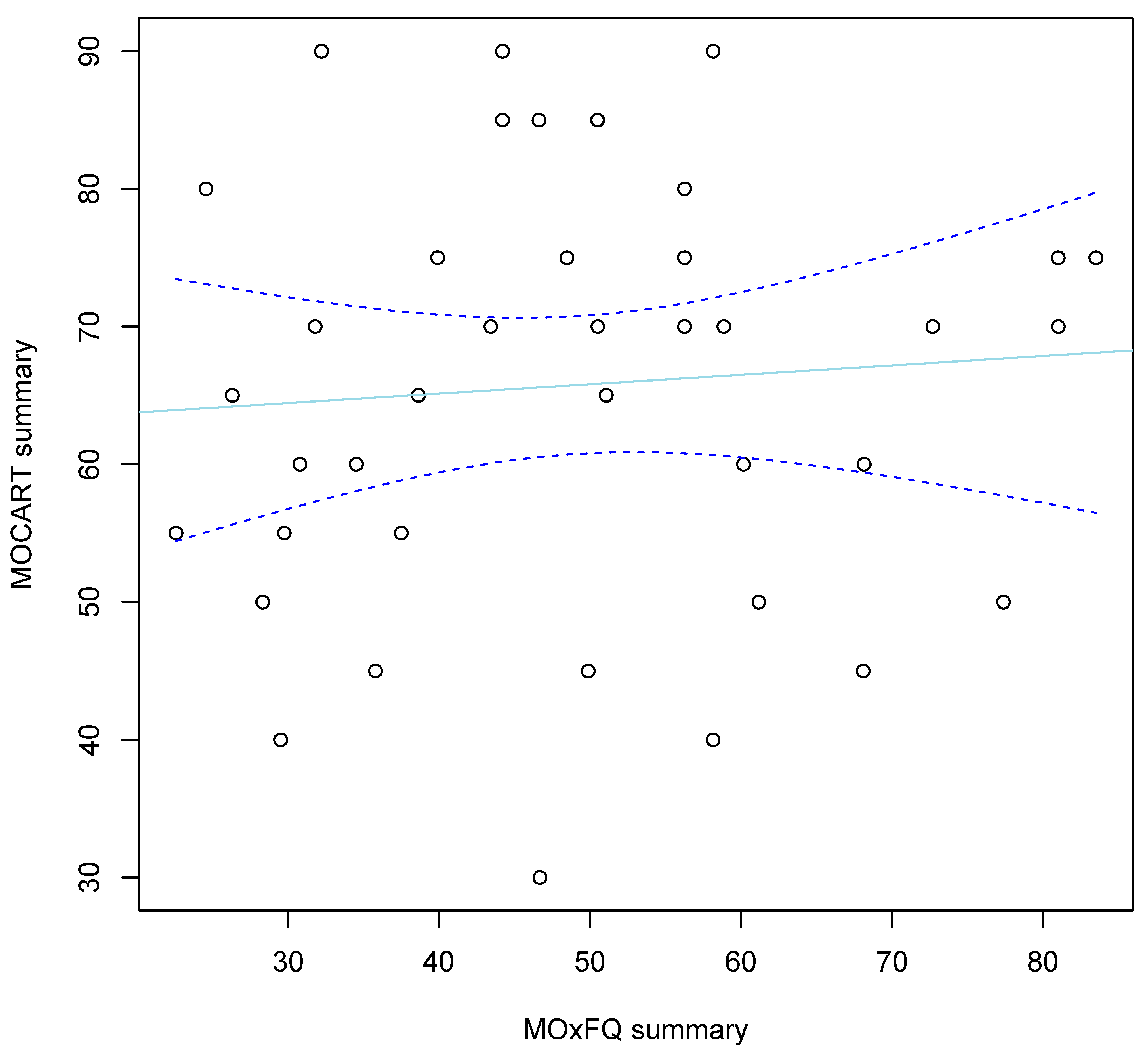
3.4. Post-Operative MRI Scan Findings
3.5. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Section or Topic | Item No | Checklist Item | Reported on Page No. |
|---|---|---|---|
| Study Design | 1 | Study conducted in accordance with CONSORT (RCT), STROBE (cohort, case-control, or cross-sectional), or PRISMA (meta-analysis) guidelines | 3 |
| 2 | Relevant institutional and ethical approval | 15 | |
| Recipient Details | 3 | Recipient demographics (including age and sex) | 4, 5 |
| 4 | Comorbidities (including underlying diabetes, inflammatory conditions, pre-existing joint pathology, and smoking status) | 4, 5 | |
| 5 | Current anti-inflammatory medications | 4, 5 | |
| Injury details | 6 | Diagnosis (including relevant grading system and chronicity) | 3, 4 |
| 7 | Previous treatments for current injury | 5 | |
| Intervention Details | 8 | Surgical intervention described sufficiently to enable replication | 3, 4 |
| 9 | Operative findings | 4, 5 | |
| Donor Age | 10 | Donor Age | 4 |
| Tissue Harvest | 11 | Tissue harvest described sufficiently to enable replication (including anatomical source, equipment, reagents, storage media, and environment) | 3 |
| 12 | Time between tissue harvest and processing | 3 | |
| Processing | 13 | Description of tissue processing that makes replication of the experiment possible (including digestion solution concentrations and volumes, duration, agitation and temperature of digestion phase, and name of commercial system) | 3 |
| 14 | If performed, purification described sufficiently to enable replication (including combination and concentration of antibodies, equipment, and method of confirming purity) | N/A | |
| 15 | Yield with respect to volume of tissue processed | 3 | |
| Cell culture | 16 | If performed, cell culture described sufficiently to enable replication (including conditions and number of freeze-thaw cycles) | N/A |
| 17 | If performed, pre-differentiation described sufficiently to enable replication | N/A | |
| MSC characteristics | 18 | MSC preparation and source described in title and abstract (e.g., BM-MSC and ADSC) | 1, 3 |
| 19 | Cellular composition and/or heterogeneity | 3 | |
| 20 | Immunophenotype and details of in vitro differentiation tested on batch | N/A | |
| 21 | Passage and percentage viability | N/A | |
| Delivery | 22 | MSC delivery described sufficiently to enable replication (including point of delivery, volume of suspension, and media used as vehicle) | 3 |
| 23 | If performed, details of co-delivered growth factors, scaffolds, or carriers | 4 | |
| Outcome | 24 | Rehabilitation protocol sufficiently described to enable replication (including immobilization and physical therapy) | 4 |
| 25 | Outcome assessments include functional outcomes and recording of complications (including infection and tumour); if performed, radiographic outcomes, physical examination findings, return to activities, and satisfaction | 4, 5 |
Appendix B
| Item No. | Recommendation | Page No. | |
|---|---|---|---|
| Title and abstract | 1 | (a) Indicate the study’s design with a commonly used term in the title or the abstract | 1 |
| (b) Provide in the abstract an informative and balanced summary of what was done and what was found | 1 | ||
| Introduction | |||
| Background/rationale | 2 | Explain the scientific background and rationale for the investigation being reported | 1–3 |
| Objectives | 3 | State specific objectives, including any prespecified hypotheses | 3 |
| Methods | |||
| Study design | 4 | Present key elements of study design early in the paper | 3 |
| Setting | 5 | Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection | 3–5 |
| Participants | 6 | Cohort study—Give the eligibility criteria, and the sources and methods of selection of participants. Describe methods of follow-up Case-control study—Give the eligibility criteria, and the sources and methods of case ascertainment and control selection. Give the rationale for the choice of cases and controls Cross-sectional study—Give the eligibility criteria, and the sources and methods of selection of participants | 3, 4 |
| Variables | 7 | Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if applicable | 3, 4 |
| Data sources/ measurement | 8 * | For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of assessment methods if there is more than one group | 4 |
| Bias | 9 | Describe any efforts to address potential sources of bias | 4, 5, 10 |
| Study size | 10 | Explain how the study size was arrived at | 5 |
| Quantitative variables | 11 | Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why | 4, 5 |
| Statistical methods | 12 | (a) Describe all statistical methods, including those used to control for confounding | 5 |
| (b) Describe any methods used to examine subgroups and interactions | N/A | ||
| (c) Explain how missing data were addressed | 4 | ||
| (d) Cohort study—If applicable, explain how loss to follow-up was addressed | 11 | ||
| (e) Describe any sensitivity analyses | 5 | ||
| Participants | 13 * | (a) Report numbers of individuals at each stage of study—e.g. numbers potentially eligible, examined for eligibility, confirmed eligible, included in the study, completing follow-up, and analysed | 5, 6, 10 |
| (b) Give reasons for non-participation at each stage | 5, 6, 10, 11 | ||
| (c) Consider use of a flow diagram | N/A | ||
| Descriptive data | 14 * | (a) Give characteristics of study participants (e.g. demographic, clinical, social) and information on exposures and potential confounders | 6 |
| (b) Indicate number of participants with missing data for each variable of interest | 6 | ||
| (c) Cohort study—Summarise follow-up time (e.g., average and total amount). | 7 | ||
| Outcome data | 15 * | Cohort study—Report numbers of outcome events or summary measures over time | 7–10 |
| Main results | 16 | (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (e.g., 95% confidence interval). Make clear which confounders were adjusted for and why they were included | 7–11 |
| (b) Report category boundaries when continuous variables were categorized | 7–11 | ||
| (c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period | N/A | ||
| Other analyses | 17 | Report other analyses done—e.g. analyses of subgroups and interactions, and sensitivity analyses | 5 |
| Discussion | |||
| Key results | 18 | Summarise key results with reference to study objectives | 12 |
| Limitations | 19 | Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude of any potential bias | 12, 13 |
| Interpretation | 20 | Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar studies, and other relevant evidence | 13 |
| Generalisability | 21 | Discuss the generalisability (external validity) of the study results | 13 |
| OtherInformation | |||
| Funding | 22 | Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the present article is based | 14 |
References
- Saxena, A.; Eakin, C. Articular talar injuries in athletes: Results of microfracture and autogenous bone graft. Am. J. Sports Med. 2007, 35, 1680–1687. [Google Scholar] [CrossRef] [PubMed]
- Looze, C.A.; Capo, J.; Ryan, M.K.; Begly, J.P.; Chapman, C.; Swanson, D.; Singh, B.C.; Strauss, E.J. Evaluation and Management of Osteochondral Lesions of the Talus. Cartilage 2017, 8, 19–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phemister, D.B. The causes of and changes in loose bodies arising from the articular surface of the joint. J. Bone Jt. Surg. 1924, 6, 278–315. [Google Scholar]
- Berndt, A.L.; Harty, M. Transchondral fractures (osteochondritis dissecans) of the talus. J. Bone Jt. Surg. Am. 1959, 41, 988–1020. [Google Scholar] [CrossRef]
- Doherty, C.; Delahunt, E.; Caulfield, B.; Hertel, J.; Ryan, J.; Bleakley, C. The incidence and prevalence of ankle sprain injury: A systematic review and meta-analysis of prospective epidemiological studies. Sports Med. 2014, 44, 123–140. [Google Scholar] [CrossRef]
- Zengerink, M.; Struijs, P.A.; Tol, J.L.; van Dijk, C.N. Treatment of osteochondral lesions of the talus: A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 238–246. [Google Scholar] [CrossRef] [Green Version]
- Buckwalter, J.; Maw, V.; Ratcliffe, A. Restoration of injured or degenerated articular cartilage. J. Am. Acad. Orthop. Surg. 1994, 2, 92–201. [Google Scholar] [CrossRef]
- Lan, T.; McCarthy, H.S.; Hulme, C.H.; Wright, K.T.; Makwana, N. The management of talar osteochondral lesions—Current concepts. Arthrosc. Jt. Surg. 2021, 8, 231–237. [Google Scholar] [CrossRef]
- Karnovsky, S.C.; DeSandis, B.; Haleem, A.M.; Sofka, C.M.; O’Malley, M.; Drakos, M.C. Comparison of juvenile allogenous articular cartilage and bone marrow aspirate concentrate versus microfracture with and without bone marrow aspirate concentrate in arthroscopic treatment of talar osteochondral lesions. Foot Ankle Int. 2018, 39, 393–405. [Google Scholar] [CrossRef]
- Loomer, R.; Fisher, C.; Lloyd-Smith, R.; Sisler, J.; Cooner, T. Osteochondral lesions of the talus. Am. J. Sports Med. 1993, 21, 13–19. [Google Scholar] [CrossRef]
- Hepple, S.; Winson, I.G.; Glew, D. Osteochondral lesions of the talus: A revised classification. Foot Ankle Int. 1999, 20, 789–793. [Google Scholar] [CrossRef] [PubMed]
- Tol, J.L.; Struijs, P.A.; Bossuyt, P.M.; Verhagen, R.A.; van Dijk, C.N. Treatment strategies in osteochondral defects of the talar dome: A systematic review. Foot Ankle Int. 2000, 21, 119–126. [Google Scholar] [CrossRef]
- Ferkel, R.D.; Zanotti, R.M.; Komenda, G.A.; Sgaglione, N.A.; Cheng, M.S.; Applegate, G.R.; Dopirak, R.M. Arthroscopic treatment of chronic osteochondral lesions of the talus: Long-term results. Am. J. Sports Med. 2008, 36, 1750–1762. [Google Scholar] [CrossRef] [PubMed]
- Hannon, C.P.; Murawski, C.D.; Fansa, A.M.; Smyth, N.A.; Do, H.; Kennedy, J.G. Microfracture for osteochondral lesions of the talus: A systematic review of reporting of outcome data. Am. J. Sports Med. 2013, 41, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Shimozono, Y.; Coale, M.; Yasui, Y.; O’Halloran, A.; Deyer, T.W.; Kennedy, J.G. Subchondral bone degradation after microfracture for osteochondral lesions of the talus: An MRI analysis. Am. J. Sports Med. 2018, 46, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.Y.; Lee, K.B. Arthroscopic microfracture for osteochondral lesion of the talus. Second-look arthroscopic and magnetic resonance analysis of cartilage repair tissue outcomes. J. Bone Jt. Am. 2020, 102, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Valderrabano, V.; Leumann, A.; Rasch, H.; Egelhof, T.; Hintermann, B.; Pagenstert, G. Kneeto-ankle mosaicplasty for the treatment of osteochondral lesions of the ankle joint. Am. J. Sports Med. 2009, 37 (Suppl. 1), 105S–111S. [Google Scholar] [CrossRef]
- Emre, T.Y.; Ege, T.; Cift, H.T.; Demircioglu, D.T.; Seyhan, B.; Uzun, M. Open mosaicplasty in osteochondral lesions of the talus: A prospective study. J. Foot Ankle Surg. 2012, 51, 556–560. [Google Scholar] [CrossRef]
- Kraeutler, M.J.; Chahla, J.; Dean, C.S.; Mitchell, J.J.; Santini-Araujo, M.G.; Pinney, S.J.; Pascual-Garrido, C. Current concepts review update: Osteochondral lesions of the talus. Foot Ankle Int. 2017, 38, 331–342. [Google Scholar] [CrossRef]
- Whittaker, J.P.; Smith, G.; Makwana, N.; Roberts, S.; Harrison, P.E.; Laing, P.; Richardson, J.B. Early results of autologous chondrocyte implantation in the talus. J. Bone Jt. Surg. Br. 2005, 87, 179–183. [Google Scholar] [CrossRef] [Green Version]
- Niemeyer, P.; Salzmann, G.; Schmal, H.; Mayr, H.; Sudkamp, N.P. Autologous chondrocyte implantation for the treatment of chondral and osteochondral defects of the talus: A meta-analysis of available evidence. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 1696–1703. [Google Scholar] [CrossRef] [PubMed]
- Verhagen, R.A.; Struijs, P.A.; Bossuyt, P.M.; van Dijk, C.N. Systematic review of treatment strategies for osteochondral defects of the talar dome. Foot Ankle Clin. 2003, 8, 233–242. [Google Scholar] [CrossRef]
- Loveday, D.; Clifton, R.; Robinson, A. Interventions for treating osteochondral defects of the talus in adults. Cochrane Database Syst Rev. 2010, 8, CD008104. [Google Scholar] [CrossRef] [PubMed]
- Friedenstein, A.J.; Piatetzky, I.I.S.; Petrakova, K.V. Osteogenesis in transplants of bone marrow cells. J. Embryol. Exp. Morphol. 1966, 16, 381–390. [Google Scholar] [CrossRef]
- Shetty, A.A.; Kim, S.J.; Shetty, V.; Stelzeneder, D.; Shetty, N.; Bilagi, P.; Lee, H.J. Autologous bone-marrow mesenchymal cell induced chondrogenesis: Single-stage arthroscopic cartilage repair. Tissue Eng. Regen. Med. 2014, 11, 247–253. [Google Scholar] [CrossRef]
- Allison, D.D.; Grande-Allen, K.J. Review. Hyaluronan: A powerful tissue engineering tool. Tissue Eng. 2006, 12, 2131–2140. [Google Scholar] [CrossRef]
- Burdick, J.A.; Chung, C.; Jia, X.; Randolph, M.A.; Langer, R. Controlled degradation and mechanical behavior of photopolymerized hyaluronic acid networks. Biomacromolecules 2005, 6, 86–91. [Google Scholar] [CrossRef] [Green Version]
- Strauss, E.; Schachter, A.; Frenkel, S.; Rosen, J. The efficacy of intra-articular hyaluronan injection after the microfracture technique for the treatment of articular cartilage lesions. Am. J. Sports Med. 2009, 37, 720–726. [Google Scholar] [CrossRef]
- Sage, A.; Chang, A.A.; Schumacher, B.L.; Sah, R.L.; Watson, D. Cartilage outgrowth in fibrin scaffolds. Am. J. Rhinol. Allergy 2009, 23, 486–491. [Google Scholar] [CrossRef]
- Murphy, E.P.; McGoldrick, N.P.; Curtin, M.; Kearns, S.R. A prospective evaluation of bone marrow aspirate concentrate and microfracture in the treatment of osteochondral lesions of the talus. Foot Ankle Surg. 2019, 25, 441–448. [Google Scholar] [CrossRef]
- Murray, I.R.; Geeslin, A.G.; Goudie, E.B.; Petrigliano, F.A.; LaPrade, R.F. Minimum information for studies evaluating biologics in orthopaedics (MIBO): Platelet-rich plasma and mesenchymal stem cells. J. Bone Jt. Surg. 2017, 99, 809–819. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)statement: Guidelines for reporting observational studies. J. Clin Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morley, D.; Jenkinson, C.; Doll, H.; Lavis, G.; Sharp, R.; Cooke, P.; Dawson, J. The Manchester–Oxford Foot Questionnaire (MOXFQ) development and validation of a summary index score. Bone Jt. Res. 2013, 2, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Van Reenen, M.; Janssen, B. EQ-5D-5L User Guide; EuroQol Research Foundation: Rotterdam, The Netherlands, 2015. [Google Scholar]
- Casari, F.A.; Germann, C.; Weigelt, L.; Wirth, S.; Viehöfer, A.; Ackermann, J. The role of magnetic resonance imaging in autologous matrix-induced chondrogenesis for osteochondral lesions of the talus: Analyzing MOCART 1 and 2.0. Cartilage 2021, 13, 639S–645S. [Google Scholar] [CrossRef] [PubMed]
- Bhosale, A.M.; Kuiper, J.H.; Johnson, W.E.; Harrison, P.E.; Richardson, J.B. Midterm to long-term longitudinal outcome of autologous chondrocyte implantation in the knee joint: A multilevel analysis. Am. J. Sports Med. 2009, 37 (Suppl. 1), 131–138. [Google Scholar] [CrossRef] [PubMed]
- Kierkegaard, S.; Langeskov-Christensen, M.; Lund, B.; Naal, F.D.; Mechlenburg, I.; Dalgas, U.; Casartelli, N.C. Pain, activities of daily living and sport function at different time points after hip arthroscopy in patients with femoroacetabular impingement: A systematic review with meta-analysis. Br. J. Sports Med. 2017, 51, 572–579. [Google Scholar] [CrossRef]
- Muggeo, V.M.; Atkins, D.C.; Gallop, R.J.; Dimidjian, S. Segmented mixed models with random changepoints: A maximum likelihood approach with application to treatment for depression study. Stat. Model. 2014, 14, 293–313. [Google Scholar] [CrossRef]
- Bouras, T.; Kuiper, J.H.; Barnett, A. Isolated medial patellofemoral ligament reconstruction significantly improved quality of life in patients with recurrent patella dislocation: A response to Hiemstra et al.’s letter to the editor. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 3735–3737. [Google Scholar] [CrossRef]
- Heinze, G.; Wallisch, C.; Dunkler, D. Variable selection—A review and recommendations for the practicing statistician. Biom. J. 2018, 60, 431–449. [Google Scholar] [CrossRef] [Green Version]
- Ranstam, J.; Kärrholm, J.; Pulkkinen, P.; Mäkelä, K.; Espehaug, B.; Pedersen, A.B.; Mehnert, F.; Furnes, O.; NARAStudy Group. Statistical analysis of arthroplasty data: I.I. Guidelines. Acta Orthop. 2011, 82, 258–267. [Google Scholar] [CrossRef] [Green Version]
- Dawson, J.; Boller, I.; Doll, H.; Lavis, G.; Sharp, R.; Cooke, P.; Jenkinson, C. Minimally important change was estimated for the Manchester–Oxford Foot Questionnaire after foot/ankle surgery. J. Clin. Epidemiol. 2014, 67, 697–705. [Google Scholar] [CrossRef] [PubMed]
- Shearer, C.; Loomer, R.; Clement, D. Nonoperatively managed stage 5 osteochondral talar lesions. Foot Ankle Int. 2002, 23, 651–654. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.-B.; Bai, L.-B.; Yoon, T.-R.; Jung, S.-T.; Seon, J.-K. Second-look arthroscopic findings and clinical outcomes after microfracture for osteochondral lesions of the talus. Am. J. Sports Med. 2009, 37 (Suppl. 1), 63S–70S. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.H.; Hui, J.H. The potential of stem cells in orthopaedic surgery. J. Bone Jt. Surg. Br. 2006, 88, 841–851. [Google Scholar] [CrossRef] [PubMed]
- Hunt, S.A.; Sherman, O. Arthroscopic treatment of osteochondral lesions of the talus with correlation of outcome scoring systems. Arthroscopy 2003, 9, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Fortier, L.A.; Potter, H.G.; Rickey, E.J.; Schnabel, L.V.; Foo, L.F.; Chong, L.R. Concentrated bone marrow aspirate improves full-thickness cartilage repair compared with microfracture in the equine model. J. Bone Jt. Surg. Am. 2010, 92, 1927–1937. [Google Scholar] [CrossRef] [Green Version]
- Corr, D.; Raikin, J.; O’Neil, J.; Raikin, S. Long-term Outcomes of Microfracture for Treatment of Osteochondral Lesions of the Talus. Foot Ankle Int. 2021, 42, 833–840. [Google Scholar] [CrossRef]
- Drakos, M.C.; Eble, S.K.; Cabe, T.N.; Patel, K.; Hansen, O.B.; Sofka, C.; Deland, J.T. Comparison of Functional and Radiographic Outcomes of Talar Osteochondral Lesions Repaired with Micronized Allogenic Cartilage Extracellular Matrix and Bone Marrow Aspirate Concentrate vs Microfracture. Foot Ankle Int. 2021, 42, 841–850. [Google Scholar] [CrossRef]
- Pradhan, A.; Lever, C.; Makwana, N.; Kuiper, J.H.; Roberts, S.; Parker, J.; Harrison, P.; Laing, P.; Richardson, J.B. Autologous Chondrocyte Implantation in Osteochondral Defects of the Talus: Up to Fourteen Years Follow-Up Study. In Proceedings of the 18th EFORT Congress, Vienna, Austria, 31 May–2 June 2017. [Google Scholar]
- Johnson, B.; Lever, C.; Roberts, S.; Harrison, P.; Laing, P.; Richardson, J.B. Cell cultured chondrocyte implantation and scaffold techniques for osteochondral talar lesions. Foot Ankle Clin. 2013, 18, 135–150. [Google Scholar] [CrossRef]

| Parameter | Level | Mean (SD), Median [Range] or n (%) |
|---|---|---|
| Number of patients (ankles) | 94 (96) | |
| Age (mean (SD)) | 37.3 (14.4) | |
| Sex(%) | M | 51 (54) |
| F | 43 (45) | |
| BMI (mean (SD)) | 29.3 (5.6) | |
| Bone affected (%) | Talus | 83 (88) |
| Both Talus and Tibia | 8 (8) | |
| Tibia | 3 (3) | |
| Location (%) | Medial Talus | 65 (76) |
| Lateral Talus | 16 (19) | |
| Both Medial and Lateral Talus | 3 (4) | |
| Central Talus | 1 (1) | |
| Known history of injury (%) | Yes | 70 (74) |
| No | 24 (26) | |
| Months from symptoms onset (median [range]) | 66.5 [19, 372] | |
| Injury mechanism (%) | Fall | 37 (54) |
| Sport | 29 (41) | |
| Horse | 2 (3) | |
| Road/Traffic Accident | 2 (3) | |
| Months from injury (median [range]) | 60 [8, 480] | |
| Previous surgery (%) | Yes | 62 (65) |
| No | 34 (35) | |
| Bone oedemas (%) | Yes | 75 (79) |
| No | 20 (21) | |
| OA (%) | No | 75 (79) |
| Yes | 20 (21) | |
| Cysts (%) | Yes | 63 (66) |
| No | 33 (34) | |
| Area (cm2; mean (SD) [range]) | 1.5 (0.7) [0.4 to 4] | |
| Osteotomy (%) | No | 83 (88) |
| Yes | 13 (15) |
| Previous Surgery | n = 62 |
|---|---|
| Arthroscopy and microfracture | 31 |
| Arthroscopy | 27 |
| Open debridement | 2 |
| Open reduction and internal fixation for fracture | 2 |
| 1 × previous procedure | 23 |
| 2 × previous procedures | 31 |
| 3 × previous procedures | 8 |
| Kellgren-Lawrence Classification | n = 20 |
|---|---|
| 0 (no OA) | 1 |
| 1 (doubtful) | 5 |
| 2 (mild) | 13 |
| 3 (moderate) | 1 |
| 4 (severe) | 0 |
| Outcome | Baseline | 12 Months | p-Value (vs. Baseline) | 36 Months | p-Value (vs. 12 m) |
|---|---|---|---|---|---|
| MOXFQ | |||||
| Summary | 66.5 (63.4 to 69.7) | 40.8 (35.3 to 46.2) | <0.001 | 39.5 (30.7 to 48.4) | 0.79 |
| Walking | 71.7 (67.9 to 75.5) | 43.8 (37.6 to 50.0) | <0.001 | 40.6 (32.0 to 49.2) | 0.41 |
| Pain | 67.3 (64.3 to 70.3) | 45.6 (41.0 to 50.2) | <0.001 | 42.7 (35.3 to 50.1) | 0.31 |
| Social | 56.5 (52.1 to 60.8) | 31.4 (25.6 to 37.2) | <0.001 | 28.4 (20.6 to 36.2) | 0.37 |
| EQ-5D | 0.53 (0.48 to 0.57) | 0.70 (0.65 to 0.75) | <0.001 | 0.61 (0.52 to 0.70) | 0.06 |
| Predictor | Coefficient (95% CI) | p-Value |
|---|---|---|
| Full model | ||
| Age (per year) | −0.12 (−0.65 to 0.41) | 0.65 |
| Male | −3.6 (−15.3 to 8.1) | 0.54 |
| BMI | 0.6 (−0.7 to 1.9) | 0.36 |
| Known history of injury a | 16.3 (2.8 to 29.8) | 0.017 |
| Time from symptom onset (per year) | 0.7 (−0.03 to 1.4) | 0.057 |
| Previous surgery a | 11.3 (−1.6 to 24.2) | 0.084 |
| Bone oedemas | −3.4 (−17.0 to 10.3) | 0.63 |
| OA a | 6.9 (−7.4 to 21.3) | 0.34 |
| Bone affected b | - | 0.42 |
| Location b | - | 0.71 |
| Defect area (per cm2) | −6.5 (−15.5 to 2.4) | 0.15 |
| Cysts | 3.3 (−13.3 to 19.9) | 0.69 |
| Osteotomy | −5.0 (−21.1 to 11.1) | 0.54 |
| Final model | ||
| Known history of injury a | 8.1 (−0.8 to 17.1) | 0.073 |
| Time from symptom onset (per year) | 0.7 (0.1 to 1.2) | 0.013 |
| Previous surgery a | 7.7 (−1.4 to 16.8) | 0.095 |
| OA a | 7.9 (−1.3 to 17.1) | 0.092 |
| Defect area (per cm2) | −6.7 (−11.9 to −1.5) | 0.012 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abas, S.; Kuiper, J.H.; Roberts, S.; McCarthy, H.; Williams, M.; Bing, A.; Tins, B.; Makwana, N. Osteochondral Lesions of the Ankle Treated with Bone Marrow Concentrate with Hyaluronan and Fibrin: A Single-Centre Study. Cells 2022, 11, 629. https://doi.org/10.3390/cells11040629
Abas S, Kuiper JH, Roberts S, McCarthy H, Williams M, Bing A, Tins B, Makwana N. Osteochondral Lesions of the Ankle Treated with Bone Marrow Concentrate with Hyaluronan and Fibrin: A Single-Centre Study. Cells. 2022; 11(4):629. https://doi.org/10.3390/cells11040629
Chicago/Turabian StyleAbas, Sameera, Jan Herman Kuiper, Sally Roberts, Helen McCarthy, Mike Williams, Andrew Bing, Bernhard Tins, and Nilesh Makwana. 2022. "Osteochondral Lesions of the Ankle Treated with Bone Marrow Concentrate with Hyaluronan and Fibrin: A Single-Centre Study" Cells 11, no. 4: 629. https://doi.org/10.3390/cells11040629
APA StyleAbas, S., Kuiper, J. H., Roberts, S., McCarthy, H., Williams, M., Bing, A., Tins, B., & Makwana, N. (2022). Osteochondral Lesions of the Ankle Treated with Bone Marrow Concentrate with Hyaluronan and Fibrin: A Single-Centre Study. Cells, 11(4), 629. https://doi.org/10.3390/cells11040629