
Biomarkers-in-Cardiology 8 RE-VISITED—Consistent Safety of Early Discharge with a Dual Marker Strategy Combining a Normal hs-cTnT with a Normal Copeptin in Low-to-Intermediate Risk Patients with Suspected Acute Coronary Syndrome—A Secondary Analysis of the Randomized Biomarkers-in-Cardiology 8 Trial

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Biomarker Testing
2.2. Patient Exclusion after Retesting of hs-cTnT Instead of cTnT or cTnI
2.3. Outcomes
2.4. Statistical Evaluation
3. Results
3.1. Patient Characteristics
3.2. Serial Troponin Protocol in the Overall Cohort and in the Standard of Care
3.3. Effect of Exclusion on Corresponding MACE
3.4. Protocol Deviations and Analyses per Protocol
3.5. Outcomes within 30 Days
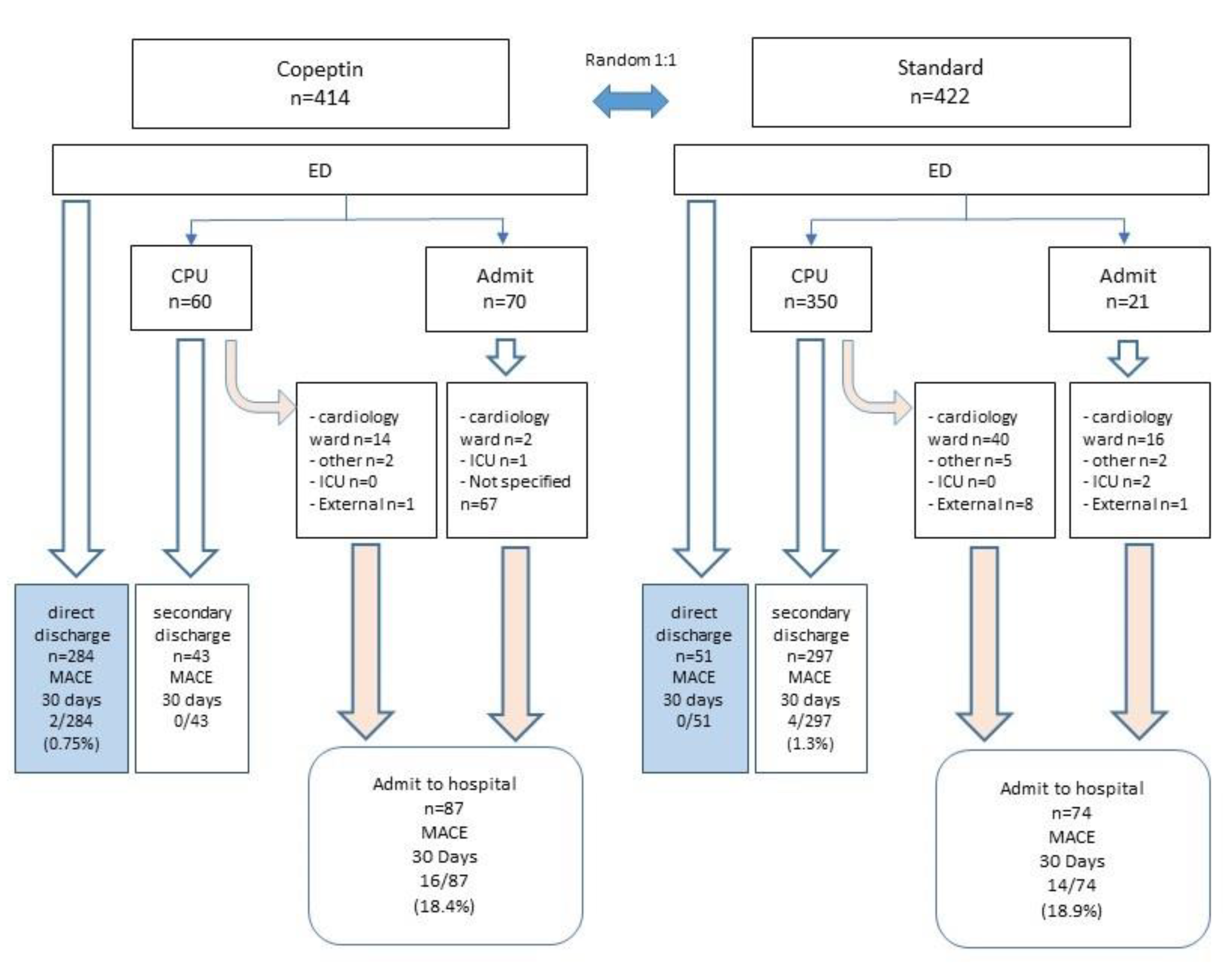
3.6. Disposition of Patients in Randomized Treatment Arms and Associated MACE Rates at 30 Days
4. Discussion
Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367, Erratum in Eur. Heart J. 2021, 42, 2298. [Google Scholar] [CrossRef]
- Giannitsis, E.; Blankenberg, S.; Christenson, R.H.; Frey, N.; von Haehling, S.; Hamm, C.W.; Inoue, K.; Katus, H.A.; Lee, C.-C.; McCord, J.; et al. Critical appraisal of the 2020 ESC guideline recommendations on diagnosis and risk assessment in patients with suspected non-ST-segment elevation acute coronary syndrome. Clin. Res. Cardiol. 2021, 110, 1353–1368. [Google Scholar] [CrossRef]
- Anand, A.; Shah, A.S.; Beshiri, A.; Jaffe, A.S.; Mills, N.L. Global Adoption of High-Sensitivity Cardiac Troponins and the Universal Definition of Myocardial Infarction. Clin. Chem. 2019, 65, 484–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stallone, F.; Schoenenberger, A.W.; Puelacher, C.; Gimenez, M.R.; Walz, B.; Devasia, A.N.; Bergner, M.; Twerenbold, R.; Wildi, K.; Reichlin, T.; et al. Incremental value of copeptin in suspected acute myocardial infarction very early after symptom onset. Eur. Heart J. Acute Cardiovasc. Care 2016, 5, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Zellweger, C.; Wildi, K.; Twerenbold, R.; Reichlin, T.; Naduvilekoot, A.; Neuhaus, J.; Balmelli, C.; Gabutti, M.; Al Afify, A.; Ballarino, P.; et al. Use of copeptin and high-sensitive cardiac troponin T for diagnosis and prognosis in patients with diabetes mellitus and suspected acute myocardial infarction. Int. J. Cardiol. 2015, 190, 190–197. [Google Scholar] [CrossRef]
- Potocki, M.; Reichlin, T.; Thalmann, S.; Zellweger, C.; Twerenbold, R.; Reiter, M.; Steuer, S.; Bassetti, S.; Drexler, B.; Stelzig, C.; et al. Diagnostic and prognostic impact of copeptin and high-sensitivity cardiac troponin T in patients with pre-existing coronary artery disease and suspected acute myocardial infarction. Heart 2012, 98, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Wildi, K.; Zellweger, C.; Twerenbold, R.; Jaeger, C.; Reichlin, T.; Haaf, P.; Faoro, J.; Gimenez, M.R.; Fischer, A.; Nelles, B.; et al. Incremental value of copeptin to highly sensitive cardiac Troponin I for rapid rule-out of myocardial infarction. Int. J. Cardiol. 2015, 190, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Boeddinghaus, J.; Reichlin, T.; Nestelberger, T.; Twerenbold, R.; Meili, Y.; Wildi, K.; Hillinger, P.; Gimenez, M.R.; Cupa, J.; Schumacher, L.; et al. Early diagnosis of acute myocardial infarction in patients with mild elevations of cardiac troponin. Clin. Res. Cardiol. 2017, 106, 457–467. [Google Scholar] [CrossRef] [PubMed]
- Wildi, K.; Boeddinghaus, J.; Nestelberger, T.; Twerenbold, R.; Badertscher, P.; Wussler, D.; Giménez, M.R.; Puelacher, C.; Lavallaz, J.D.F.D.; Dietsche, S.; et al. Comparison of fourteen rule-out strategies for acute myocardial infarction. Int. J. Cardiol. 2019, 283, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Mueller-Hennessen, M.; Lindahl, B.; Giannitsis, E.; Vafaie, M.; Biener, M.; Haushofer, A.C.; Seier, J.; Christ, M.; Alquézar-Arbé, A.; Defilippi, C.R.; et al. Combined testing of copeptin and high-sensitivity cardiac troponin T at presentation in comparison to other algorithms for rapid rule-out of acute myocardial infarction. Int. J. Cardiol. 2019, 276, 261–267. [Google Scholar] [CrossRef]
- Reichlin, T.; Schindler, C.; Drexler, B.; Twerenbold, R.; Reiter, M.; Zellweger, C.; Moehring, B.; Ziller, R.; Hoeller, R.; Gimenez, M.R.; et al. One-Hour Rule-out and Rule-in of Acute Myocardial Infarction Using High-Sensitivity Cardiac Troponin T. Arch. Intern. Med. 2012, 172, 1211–1218. [Google Scholar] [CrossRef]
- Shah, A.S.; Anand, A.; Sandoval, Y.; Lee, K.K.; Smith, S.W.; Adamson, P.D.; Chapman, A.R.; Langdon, T.; Sandeman, D.; Vaswani, A.; et al. High-sensitivity cTn I at presentation in patients with suspected acute coronary syndrome: A cohort study. Lancet 2015, 386, 2481–2488. [Google Scholar] [CrossRef] [Green Version]
- Neumann, J.T.; Sörensen, N.A.; Schwemer, T.; Ojeda, F.; Bourry, R.; Sciacca, V.; Schaefer, S.; Waldeyer, C.; Sinning, C.; Renné, T.; et al. Diagnosis of Myocardial Infarction Using a High-Sensitivity Troponin I 1-Hour Algorithm. JAMA Cardiol. 2016, 1, 397–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiang, C.-H.; Lee, G.H.; Gi, W.-T.; Wu, Y.-K.; Huang, S.-S.; Yeo, Y.H.; Giannitsis, E.; Lee, C.-C. Safety and efficacy of the European Society of Cardiology 0/1-hour algorithm for diagnosis of myocardial infarction: Systematic review and meta-analysis. Heart 2020, 106, 985–991. [Google Scholar] [CrossRef] [PubMed]
- Stoyanov, K.M.; Hund, H.; Biener, M.; Gandowitz, J.; Riedle, C.; Löhr, J.; Mueller-Hennessen, M.; Vafaie, M.; A Katus, H.; Giannitsis, E. RAPID-CPU: A prospective study on implementation of the ESC 0/1-hour algorithm and safety of discharge after rule-out of myocardial infarction. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 39–51. [Google Scholar] [CrossRef] [Green Version]
- Twerenbold, R.; Costabel, J.P.; Nestelberger, T.; Campos, R.; Wussler, D.; Arbucci, R.; Cortes, M.; Boeddinghaus, J.; Baumgartner, B.; Nickel, C.H.; et al. Outcome of Applying the ESC 0/1-hour Algorithm in Patients With Suspected Myocardial Infarction. J. Am. Coll. Cardiol. 2019, 74, 483–494. [Google Scholar] [CrossRef]
- Chew, D.; Lambrakis, K.; Blyth, A.; Seshadri, A.; Edmonds, M.; Briffa, T.; Cullen, L.A.; Quinn, S.; Karnon, J.; Chuang, A.; et al. A Randomized Trial of a 1-Hour Troponin T Protocol in Suspected Acute Coronary Syndromes. Circulation 2019, 140, 1543–1556. [Google Scholar] [CrossRef] [PubMed]
- Möckel, M.; Searle, J.; Hamm, C.; Slagman, A.; Blankenberg, S.; Huber, K.; Katus, H.; Liebetrau, C.; Müller, C.; Muller, R.; et al. Early discharge using single cardiac troponin and copeptin testing in patients with suspected acute coronary syndrome (ACS): A randomized, controlled clinical process study. Eur. Heart J. 2015, 36, 369–376. [Google Scholar] [CrossRef]
- Morgenthaler, N.G.; Struck, J.; Alonso, C.; Bergmann, A. Assay for the Measurement of Copeptin, a Stable Peptide Derived from the Precursor of Vasopressin. Clin. Chem. 2006, 52, 112–119. [Google Scholar] [CrossRef] [Green Version]
- Morgenthaler, N.G.; Müller, B.; Struck, J.; Bergmann, A.; Redl, H.; Christ-Crain, M. COPEPTIN, A Stable Peptide of the Arginine Vasopressin Precursor, is Elevated in Hemorrhagic and Septic Shock. Shock. 2007, 28, 219–226. [Google Scholar] [CrossRef]
- Reichlin, T.; Hochholzer, W.; Stelzig, C.; Laule, K.; Freidank, H.; Morgenthaler, N.G.; Bergmann, A.; Potocki, M.; Noveanu, M.; Breidthardt, T.; et al. Incremental Value of Copeptin for Rapid Rule Out of Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2009, 54, 60–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giannitsis, E.; Huber, K.; Hamm, C.W.; Möckel, M. Instant rule-out of suspected non-ST-segment elevation myocardial infarction using high-sensitivity cardiac troponin T with Copeptin versus a single low high-sensitivity cardiac troponin T: Findings from a large pooled individual data analysis on 10,329 patients. Clin. Res. Cardiol. 2021, 110, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Giannitsis, E.; Slagman, A.; Hamm, C.W.; Gehrig, S.; Vollert, J.O.; Huber, K. Copeptin combined with either non-high sensitivity or high sensitivity cardiac troponin for instant rule-out of suspected non-ST segment elevation myocardial infarction. Biomarkers 2020, 25, 649–658. [Google Scholar] [CrossRef]
- Saenger, A.; Beyrau, R.; Braun, S.; Cooray, R.; Dolci, A.; Freidank, H.; Giannitsis, E.; Gustafson, S.; Handy, B.; Katus, H.; et al. Multicenter analytical evaluation of a high-sensitivity troponin T assay. Clin. Chim. Acta 2011, 412, 748–754. [Google Scholar] [CrossRef] [PubMed]
- Keller, T.; Tzikas, S.; Zeller, T.; Czyz, E.; Lillpopp, L.; Ojeda, F.M.; Roth, A.; Bickel, C.; Baldus, S.; Sinning, C.R.; et al. Copeptin Improves Early Diagnosis of Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2010, 55, 2096–2106. [Google Scholar] [CrossRef] [Green Version]
- Giannitsis, E.; Clifford, P.; Slagman, A.; Ruedelstein, R.; Liebetrau, C.; Hamm, C.; Honnart, D.; Huber, K.; Vollert, J.O.; Simonelli, C.; et al. Multicentre cross-sectional observational registry to monitor the safety of early discharge after rule-out of acute myocardial infarction by copeptin and troponin: The Pro-Core registry. BMJ Open 2019, 9, e028311. [Google Scholar] [CrossRef]
- Lindahl, B.; Venge, P.; James, S. The new high-sensitivity cardiac troponin T assay improves risk assessment in acute coronary syndromes. Am. Heart J. 2010, 160, 224–229, Erratum in Am. Heart J. 2011, 161, 425. [Google Scholar] [CrossRef]
- Celik, S.; Giannitsis, E.; Wollert, K.C.; Schwöbel, K.; Lossnitzer, D.; Hilbel, T.; Lehrke, S.; Zdunek, D.; Hess, A.; Januzzi, J.L.; et al. Cardiac troponin T concentrations above the 99th percentile value as measured by a new high-sensitivity assay predict long-term prognosis in patients with acute coronary syndromes undergoing routine early invasive strategy. Clin. Res. Cardiol. 2011, 100, 1077–1085. [Google Scholar] [CrossRef]
- Eggers, K.M.; Lindahl, B.; Melki, D.; Jernberg, T. Consequences of implementing a cardiac troponin assay with improved sensitivity at Swedish coronary care units: An analysis from the SWEDEHEART registry. Eur. Heart J. 2016, 37, 2417–2424. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| All Patients (n = 836) | Standard Group (n = 422) | Copeptin Group (n = 414) | |
|---|---|---|---|
| Patients’ characteristics | |||
| Age (years) (mean ± SD) | 53.3 ± 15.4 | 53.2 ± 14.9 | 53.4 ± 16.0 |
| Male sex | 62.0 (518) | 64.2 (271) | 59.7 (247) |
| Risk factors | |||
| BMI | 27.3 ± 4.79 | 27.3 ± 4.56 | 27.2 ± 5.00 |
| Diabetes | 12.9 (107) | 13.2 (55) | 12.6 (52) |
| Hypertension | 56.8 (469) | 56.7 (236) | 56.8 (233) |
| Hyperlipidaemia | 43.6 (354) | 45.1 (184) | 42.1 (170) |
| Family history of MI | 27.4 (214) | 24.5 (95) | 30.4 (119) ** |
| Smoker | 33.2 (270) | 35.1 (144) | 31.2 (126) |
| Ex-smoker | 31.1 (253) | 29.8 (122) | 32.4 (131) |
| GRACE-score (mean ± SD) | 78.76 ± 26.7 | 78.12 ± 26.4 | 79.42 ± 27.1 |
| TIMI risk score (Median/IQR) | 1 (0–2) | 1 (0–2) | 1 (0–2) |
| Medical history | |||
| Known CAD | 25.2 (207) | 24.5 (101) | 26.0 (106) |
| Prior MI | 13.3 (110) | 14.4 (60) | 12.2 (50) |
| Prior PCI | 21.3 (176) | 21.3 (88) | 21.4 (88) |
| Prior CABG | 4.3 (36) | 3.1 (13) | 5.6 (23) ** |
| Chronic heart failure | 5.6 (46) | 3.9 (16) | 7.4 (30) * |
| Primary valve disease | 7.0 (57) | 7.1 (29) | 6.9 (28) |
| Prior valve surgery | 1.2 (10) | 1.0 (4) | 1.5 (6) |
| Cardiomyopathy | 1.8 (15) | 0.5 (2) | 3.2 (13) * |
| Renal disease | 4.9 (40) | 3.6 (15) | 6.1 (25) |
| Time since symptom onset | |||
| 0–3 h (less or equal 3) | 35.2 (294) | 36.7 (155) | 33.6 (139) |
| <6 h | 42.5 (355) | 44.1 (186) | 40.8 (169) |
| <12 h | 52.3 (437) | 51.9 (219) | 52.7 (218) |
| unknown | 170 | 79 | 91 |
| Standard Group (n = 422) | Copeptin Group (n = 414) | Absolute Differenc in MACE Proportion | ||||
|---|---|---|---|---|---|---|
| MACE at 30 days | ||||||
| Yes | 18 | 18 | ||||
| No | 398 | 388 | ||||
| Unknown (lost to FU) | 6 | 8 | ||||
| MACE % (95% CI) | ||||||
| Intention to treat analysis | 4.27 (2.55–6.66) (18/422) | 4.34 (2.60–6.78) (18/414) | −0.08 (−2.83) | |||
| HR = 1.019 (95% CI: 0.523 to 1.987), p = 0.99 (chi2) | ||||||
| Exclusions per protocol deviation | 32 | 74 | ||||
| MACE after Exclusions | ||||||
| Yes | 17 | 7 | ||||
| No | 367 | 325 | ||||
| Unknown | 6 | 8 | ||||
| MACE % (95% CI) | ||||||
| Per protocol analysis | 4.35 (2.56–6.88) (17/390) | 2.05 (0.83–4.20) (7/340) | 2.30 (−0.23) | |||
| HR = 0.472 (95% CI: 0.193 to 1.153), p = 0.09 (chi2) | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giannitsis, E.; Garfias-Veitl, T.; Slagman, A.; Searle, J.; Müller, C.; Blankenberg, S.; von Haehling, S.; Katus, H.A.; Hamm, C.W.; Huber, K.; et al. Biomarkers-in-Cardiology 8 RE-VISITED—Consistent Safety of Early Discharge with a Dual Marker Strategy Combining a Normal hs-cTnT with a Normal Copeptin in Low-to-Intermediate Risk Patients with Suspected Acute Coronary Syndrome—A Secondary Analysis of the Randomized Biomarkers-in-Cardiology 8 Trial. Cells 2022, 11, 211. https://doi.org/10.3390/cells11020211
Giannitsis E, Garfias-Veitl T, Slagman A, Searle J, Müller C, Blankenberg S, von Haehling S, Katus HA, Hamm CW, Huber K, et al. Biomarkers-in-Cardiology 8 RE-VISITED—Consistent Safety of Early Discharge with a Dual Marker Strategy Combining a Normal hs-cTnT with a Normal Copeptin in Low-to-Intermediate Risk Patients with Suspected Acute Coronary Syndrome—A Secondary Analysis of the Randomized Biomarkers-in-Cardiology 8 Trial. Cells. 2022; 11(2):211. https://doi.org/10.3390/cells11020211
Chicago/Turabian StyleGiannitsis, Evangelos, Tania Garfias-Veitl, Anna Slagman, Julia Searle, Christian Müller, Stefan Blankenberg, Stephan von Haehling, Hugo A. Katus, Christian W. Hamm, Kurt Huber, and et al. 2022. "Biomarkers-in-Cardiology 8 RE-VISITED—Consistent Safety of Early Discharge with a Dual Marker Strategy Combining a Normal hs-cTnT with a Normal Copeptin in Low-to-Intermediate Risk Patients with Suspected Acute Coronary Syndrome—A Secondary Analysis of the Randomized Biomarkers-in-Cardiology 8 Trial" Cells 11, no. 2: 211. https://doi.org/10.3390/cells11020211
APA StyleGiannitsis, E., Garfias-Veitl, T., Slagman, A., Searle, J., Müller, C., Blankenberg, S., von Haehling, S., Katus, H. A., Hamm, C. W., Huber, K., Vollert, J. O., & Möckel, M. (2022). Biomarkers-in-Cardiology 8 RE-VISITED—Consistent Safety of Early Discharge with a Dual Marker Strategy Combining a Normal hs-cTnT with a Normal Copeptin in Low-to-Intermediate Risk Patients with Suspected Acute Coronary Syndrome—A Secondary Analysis of the Randomized Biomarkers-in-Cardiology 8 Trial. Cells, 11(2), 211. https://doi.org/10.3390/cells11020211