
COL5A1 RS12722 Is Associated with Temporomandibular Joint Anterior Disc Displacement without Reduction in Polish Caucasians

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics
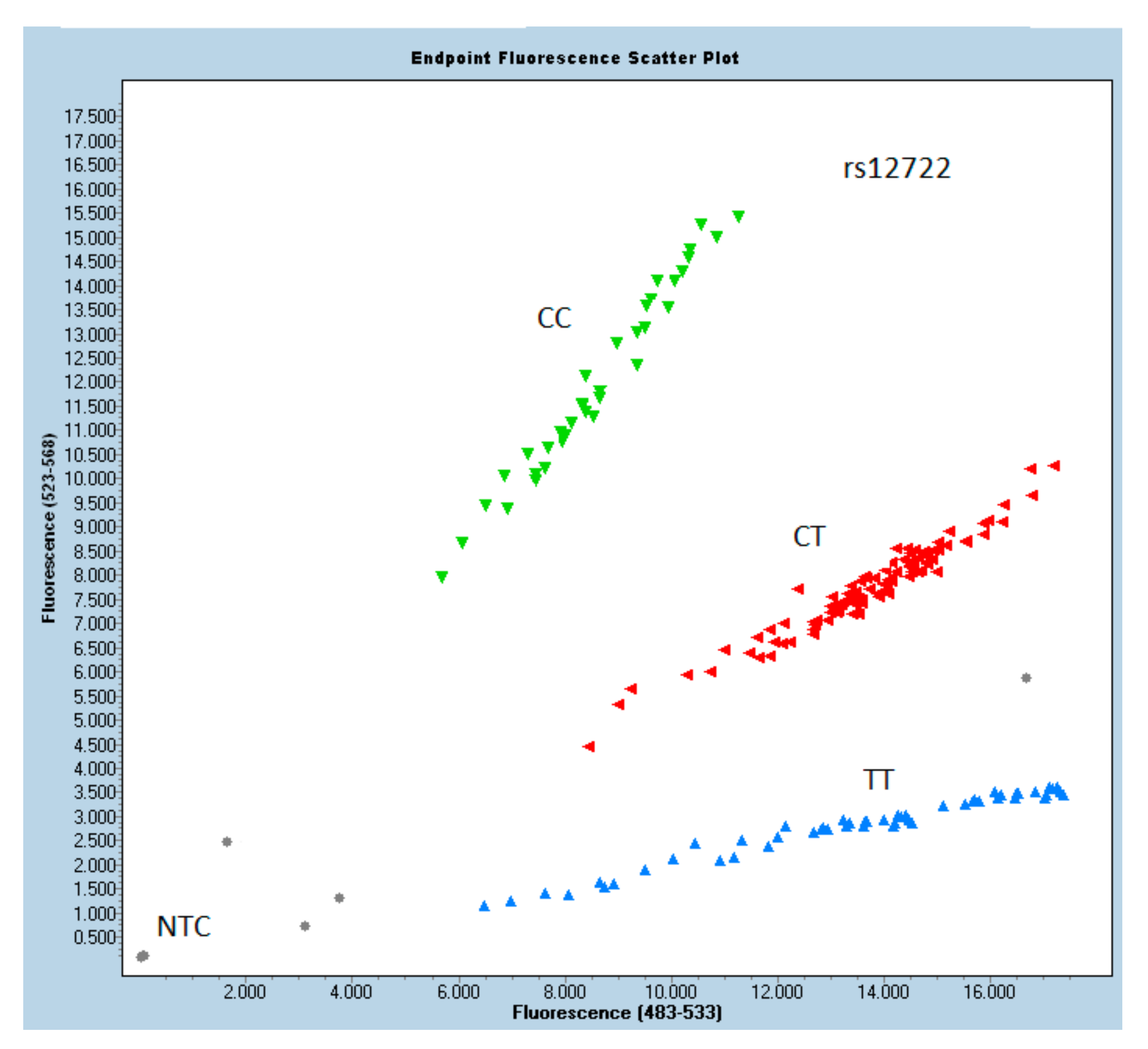
3.2. Genotyping
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACL | anterior cruciate ligament |
| ADD | anterior disc displacement |
| ADDwoR | anterior disc displacement without reduction |
| ADDwR | anterior disc displacement with reduction |
| CBCT | cone beam computed tomography |
| cEDS | classical type of Ehlers–Danlos syndrome |
| CI | confidence interval |
| CL | confidence level |
| CTS | carpal tunnel syndrome |
| DC/TMD | diagnostic criteria of temporomandibular disorder |
| EDC | estimated date of confinement |
| ICR | idiopathic condylar resorption |
| ID | internal derangement |
| LPM | lateral pterygoid muscle |
| MRI | magnetic resonance imaging |
| N | sample size |
| NTC | no template control |
| OI | osteogenesis imperfecta |
| OR | odds ratio |
| p-value | level of probability |
| PCR | polymerase chain reaction |
| SNP | single nucleotide polymorphism |
| TMD | temporomandibular disorder |
| TMJ | temporomandibular joint |
References
- Kiga, N. Histochemistry for studying structure and function of the articular disc of the human temporomandibular joint. Eur. J. Histochem. 2012, 56, e11. [Google Scholar] [CrossRef] [PubMed]
- Wadhwa, S.; Kapila, S. TMJ disorders: Future innovations in diagnostics and therapeutics. J. Dent. Educ. 2008, 72, 930–947. [Google Scholar] [CrossRef]
- Mizoguchi, I.; Nakamura, M.; Takahashi, I.; Kagayama, M.; Mitani, H. A comparison of the immunohistochemical localization of Type I and Type II collagens in craniofacial cartilages of the rat. Cells Tissues Organs 1992, 144, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Karsdal, M.A. Biochemistry of Collagens, Laminins and Elastin: Structure, Function and Biomarkers; Elsevier: Amsterdam, The Netherlands, 2019; pp. 1–389. [Google Scholar]
- Okeson, J.P. Management of Temporomandibular Disorders and Occlusion, 8th ed.; Elsevier: Amsterdam, The Netherlands, 2019. [Google Scholar]
- He, D.; Yang, X.; Wang, F.; Yang, C.; Dong, M. Acute trauma induced disc displacement without reduction and its sequelae. Sci. Rep. 2016, 6, 32684. [Google Scholar] [CrossRef] [PubMed]
- Wieckiewicz, M.; Paradowska-Stolarz, A.; Wieckiewicz, W. Psychosocial aspects of bruxism: The most paramount factor influencing teeth grinding. BioMed Res. Int. 2014, 2014, 1–7. Available online: /pmc/articles/PMC4119714/?report=abstract (accessed on 17 May 2021). [CrossRef] [PubMed]
- Lobbezoo, F.; Ahlberg, J.; Glaros, A.G.; Kato, T.; Koyano, K.; Lavigne, G.J.; De Leeuw, R.; Manfredini, D.; Svensson, P.; Winocur, E. Bruxism defined and graded: An international consensus. J. Oral Rehabil. 2012, 40, 2–4. Available online: https://pubmed.ncbi.nlm.nih.gov/23121262/ (accessed on 17 May 2021). [CrossRef]
- Dalewski, B.; Kamińska, A.; Szydłowski, M.; Kozak, M.; Sobolewska, E. Comparison of early effectiveness of three different intervention methods in patients with chronic orofacial pain: A randomized, controlled clinical trial. Pain Res. Manag. 2019, 2019, 7954291. [Google Scholar] [CrossRef]
- Kamińska, A.; Dalewski, B.; Sobolewska, E. The usefulness of the pressure algometer in the diagnosis and treatment of orofacial pain patients: A systematic review. Occup. Ther. Int. 2020, 2020, 5168457. [Google Scholar] [CrossRef]
- Dolwick, M.; Lipton, J.; Warner, M.; Williams, V.F. Sagittal anatomy of the human temporomandibular joint spaces: Normal and abnormal findings. J. Oral Maxillofac. Surg. 1983, 41, 86–88. [Google Scholar] [CrossRef]
- Shaffer, S.M.; Brismée, J.-M.; Sizer, P.S.; Courtney, C.A. Narrative review temporomandibular disorders. Part 1: Anatomy and examination/diagnosis. J. Man. Manip. Ther. 2014, 22, 2–12. [Google Scholar] [CrossRef]
- Bag, A.K. Imaging of the temporomandibular joint: An update. World J. Radiol. 2014, 6, 567–582. [Google Scholar] [CrossRef]
- Mokone, G.G.; Schwellnus, M.P.; Noakes, T.D.; Collins, M. The COL5A1 gene and Achilles tendon pathology. Scand. J. Med. Sci. Sports 2006, 16, 19–26. [Google Scholar] [CrossRef]
- September, A.V.; Cook, J.; Handley, C.J.; Van Der Merwe, L.; Schwellnus, M.P.; Collins, M. Variants within the COL5A1 gene are associated with Achilles tendinopathy in two populations. Br. J. Sports Med. 2008, 43, 357–365. [Google Scholar] [CrossRef]
- Posthumus, M.; September, A.V.; O’Cuinneagain, D.; Van Der Merwe, W.; Schwellnus, M.P.; Collins, M. The COL5A1 gene is associated with increased risk of anterior cruciate ligament ruptures in female participants. Am. J. Sports Med. 2009, 37, 2234–2240. [Google Scholar] [CrossRef]
- O’Connell, K.; Knight, H.; Ficek, K.; Leonska-Duniec, A.; Maciejewska-Karlowska, A.; Sawczuk, M.; Stepien-Slodkowska, M.; O’Cuinneagain, D.; van der Merwe, W.; Posthumus, M.; et al. Interactions between collagen gene variants and risk of anterior cruciate ligament rupture. Eur. J. Sport Sci. 2015, 15, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Altinisik, J.; Meric, G.; Erduran, M.; Ates, O.; Ulusal, A.E.; Akseki, D. The BstUI and DpnII variants of the COL5A1 gene are associated with tennis elbow. Am. J. Sports Med. 2015, 43, 1784–1789. [Google Scholar] [CrossRef] [PubMed]
- Junkiert-Czarnecka, A.; Pilarska-Deltow, M.; Bąk, A.; Heise, M.; Haus, O. New variants in COL5A1 gene among Polish patients with Ehlers-Danlos syndrome—Analysis of nine cases. Adv. Dermatol. Allergol. 2019, 36, 29–33. Available online: /pmc/articles/PMC6409875/?report=abstract (accessed on 22 August 2020). [CrossRef] [PubMed]
- Lin, Z.; Zeng, J.; Wang, X. Compound phenotype of osteogenesis imperfecta and Ehlers-Danlos syndrome caused by combined mutations in COL1A1 and COL5A1. Biosci. Rep. 2019, 39, BSR20181409. [Google Scholar] [CrossRef]
- Schnabl, D.; Rottler, A.K.; Schupp, W.; Boisserée, W.; Grunert, I. CBCT and MRT imaging in patients clinically diagnosed with temporomandibular joint arthralgia. Heliyon 2018, 4, e00641. [Google Scholar] [CrossRef]
- Kaynak, M.; Nijman, F.; van Meurs, J.; Reijman, M.; Meuffels, D.E. Genetic Variants and Anterior Cruciate Ligament Rupture: A Systematic Review. Sports Med. 2017, 47, 1637–1650. [Google Scholar] [CrossRef]
- NCI-NHGRI Working Group on Replication in Association Studies; Chanock, S.J.; Manolio, T.; Boehnke, M.; Boerwinkle, E.; Hunter, D.; Gilles, T.; Joel, N.; Abecasis Gonçalo, R.; Altshuler, D.; et al. Replicating genotype-phenotype associations. Nature 2007, 447, 655–660. [Google Scholar]
- Hollenbach, J.A.; Mack, S.J.; Thomson, G.; Gourraud, P.A. Analytical methods for disease association studies with immunogenetic data. Methods Mol. Biol 2012, 882, 245–266. [Google Scholar] [PubMed]
- Dalewski, B.; Kamińska, A.; Białkowska, K.; Jakubowska, A.; Sobolewska, E. Association of Estrogen Receptor 1 and Tumor Necrosis Factor α Polymorphisms with Temporomandibular Joint Anterior Disc Displacement without Reduction. Dis. Markers 2020, 2020, 6351817. [Google Scholar] [CrossRef] [PubMed]
- Pabalan, N.; Tharabenjasin, P.; Phababpha, S.; Jarjanazi, H. Association of COL5A1 gene polymorphisms and risk of tendon-ligament injuries among Caucasians: A meta-analysis. Sports Med. Open 2018, 4, 46. [Google Scholar] [CrossRef] [PubMed]
- Mohmara, Y.A.; Cook, J.; Benítez-Martínez, J.C.; McPeek, E.R.; Aguilar, A.A.; Olivas, E.S.; Hernandez-Sanchez, S. Influence of genetic factors in elbow tendon pathology: A case-control study. Sci. Rep. 2020, 10, 6503. [Google Scholar] [CrossRef]
- Chen, H.; Shi, L.; Zhang, J.; Zhao, D.H.; Shi, L.; Lu, Q.N.; Zhang, Q.; Duan, Q.; Shu, S. Association of COL1A1, COL5A1 and COL12A1 genes with anterior cruciate ligament injury. Chin. J. Tissue Eng. Res. 2017, 21, 1849–1854. [Google Scholar]
- Dalewski, B.; Kaczmarek, K.; Jakubowska, A.; Szczuchniak, K.; Pałka, Ł.; Sobolewska, E. COL12A1 Single Nucleotide Polymorphisms rs240736 and rs970547 Are Not Associated with Temporomandibular Joint Disc Displacement without Reduction. Genes 2021, 12, 690. [Google Scholar] [CrossRef]
- Stępień-Słodkowska, M.; Ficek, K.; Kaczmarczyk, M.; Maciejewska-Karłowska, A.; Sawczuk, M.; Leońska-Duniec, A.; Stępiński, M.; Ziętek, P.; Król, P.; Chudecka, M.; et al. The variants within the COL5A1 gene are associated with reduced risk of anterior cruciate ligament injury in skiers. J. Hum. Kinet. 2015, 45, 103–111. [Google Scholar] [CrossRef][Green Version]
- Lulińska-Kuklik, E.; Rahim, M.; Domańska-Senderowska, D.; Ficek, K.; Michałowska-Sawczyn, M.; Moska, W.; Kaczmarczyk, M.; Brzeziański, M.; Brzeziańska-Lasota, E.; Cięszczyk, P.; et al. Interactions Between COL5A1 Gene and Risk of the Anterior Cruciate Ligament Rupture. J. Hum. Kinet. 2018, 62, 65–71. [Google Scholar] [CrossRef]
- Foster, B.P.; Morse, C.I.; Onambélé, G.L.; Williams, A.G. Human COL5A1 rs12722 gene polymorphism and tendon properties in vivo in an asymptomatic population. Graefe’s Arch. Clin. Exp. Ophthalmol. 2014, 114, 1393–1402. [Google Scholar] [CrossRef]
- Witzel, A.L.; Costa, J.E.D.S.; Bolzan, M.C.; De Carli, M.L.; Nunes, T.B.; Di Matteo, R.C.; De Luca, C.E.P.; Da Silveira, F.R.X. Correlation between gender, temporomandibular joint disc position and clinical findings in patients with temporomandibular disorder. Med. Express 2015, 2, 1–5. [Google Scholar] [CrossRef]
- Nebbe, B.; Major, P.W. Prevalence of TMJ disc displacement in a pre-orthodontic adolescent sample. Angle Orthod. 2000, 70, 454–463. [Google Scholar] [PubMed]
- Bagis, B.; Ayaz, E.A.; Turgut, S.; Durkan, R.; Özcan, M. Gender difference in prevalence of signs and symptoms of temporoman-dibular joint disorders: A retrospective study on 243 consecutive patients. Int. J. Med. Sci. 2012, 9, 539–544. [Google Scholar] [CrossRef]
- Ogura, I.; Kaneda, T.; Mori, S.; Sakayanagi, M.; Kato, M. Magnetic resonance characteristics of temporomandibular joint disc displacement in elderly patients. Dentomaxillofacial Radiol. 2012, 41, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.-Q.; Lei, J.; Han, J.-H.; Yap, A.U.-J.; Fu, K. Metrical analysis of disc-condyle relation with different splint treatment positions in patients with TMJ disc displacement. J. Appl. Oral Sci. 2017, 25, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Loster, J.E.; Osiewicz, M.A.; Groch, M.; Ryniewicz, W.; Wieczorek, A. The prevalence of TMD in Polish young adults. J. Prosthodont. 2017, 26, 284–288. [Google Scholar] [CrossRef]
- Tuncer, A.B.; Ergun, N.; Tuncer, A.H.; Karahan, S. Effectiveness of manual therapy and home physical therapy in patients with temporomandibular disorders: A randomized controlled trial. J. Bodyw. Mov. Ther. 2013, 17, 302–308. [Google Scholar] [CrossRef]
- Bueno, C.H.; Pereira, D.D.; Pattussi, M.P.; Grossi, P.K.; Grossi, M.L. Gender differences in temporomandibular disorders in adult populational studies: A systematic review and meta-analysis. J. Oral Rehabil. 2018, 45, 720–729. [Google Scholar] [CrossRef]
- Akhter, R. Epidemiology of temporomandibular disorder in the general population: A systematic review. Adv. Dent. Oral Health 2019, 10, 555787. [Google Scholar] [CrossRef]
- Ebrahimi, M.; Dashti, H.; Mehrabkhani, M.; Arghavani, M.; Daneshvar-Mozafari, A. Temporomandibular disorders and related factors in a group of Iranian adolescents: A cross-sectional survey. J. Dent. Res. Dent. Clin. Dent. Prospect. 2011, 5, 123–127. [Google Scholar]
- Pedroni, C.R.; De Oliveira, A.S.; Guaratini, M.I. Prevalence study of signs and symptoms of temporomandibular disorders in university students. J. Oral Rehabil. 2003, 30, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Bernhardt, O.; Gesch, D.; Schwahn, C.; Bitter, K.; Mundt, T.; Mack, F.; Kocher, T.; Meyer, G.; Hensel, E.; John, U. Signs of temporomandibular disorders in tinnitus patients and in a population-based group of volunteers: Results of the Study of Health in Pomerania. J. Oral Rehabil. 2004, 31, 311–319. [Google Scholar] [CrossRef]
- Minghelli, B.; Morgado, M.; Caro, T. Association of temporomandibular disorder symptoms with anxiety and depression in Portuguese college students. J. Oral Sci. 2014, 56, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Thilander, B.; Rubio, G.; Pena, L.; de Mayorga, C. Prevalence of temporomandibular dysfunction and its association with malocclusion in children and adolescents: An epidemiologic study related to specified stages of dental development. Angle Orthod. 2002, 72, 146–154. [Google Scholar]
- LeResche, L.; Mancl, L.; Sherman, J.J.; Gandara, B.; Dworkin, S.F. Changes in temporomandibular pain and other symptoms across the menstrual cycle. Pain 2003, 106, 253–261. [Google Scholar] [CrossRef]
- LeResche, L.; Saunders, K.; Von Korff, M.R.; Barlow, W.; Dworkin, S.F. Use of exogenous hormones and risk of temporomandibular disorder pain. Pain 1997, 69, 153–160. [Google Scholar] [CrossRef]
- Ribeiro-Dasilva, M.C.; Line, S.R.P.; Dos Santos, M.C.L.G.; Arthuri, M.T.; Hou, W.; Fillingim, R.B.; Rizzatti-Barbosa, C.M. Estrogen Receptor-α Polymorphisms and Predisposition to TMJ Disorder. J. Pain 2009, 10, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Cairns, B.E. Pathophysiology of TMD pain—Basic mechanisms and their implications for pharmacotherapy. J. Oral Rehabil. 2010, 37, 391–410. [Google Scholar] [CrossRef] [PubMed]
- Bergström, I.; List, T.; Magnusson, T. A follow-up study of subjective symptoms of temporomandibular disorders in patients who received acupuncture and/or interocclusal appliance therapy 18–20 years earlier. Acta Odontol. Scand. 2008, 66, 88–92. [Google Scholar] [CrossRef]
- Abrahams, Y.; Laguette, M.J.; Prince, S.; Collins, M. Polymorphisms within the COL5A1 3′-UTR that alters mRNA structure and the MIR608 gene are associated with achilles tendinopathy. Ann. Hum. Genet. 2013, 77, 204–214. [Google Scholar] [CrossRef]
- Kim, S.K.; Roos, T.R.; Roos, A.K.; Kleimeyer, J.P.; Ahmed, M.A.; Goodlin, G.T.; Fredericson, M.; Ioannidis, J.P.A.; Avins, A.L.; Dragoo, J.L. Genome-wide association screens for Achilles tendon and ACL tears and tendinopathy. PLoS ONE 2017, 12, e0170422. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.L.; Seale, K.B.; El Khoury, L.Y.; Posthumus, M.; Ribbans, W.J.; Raleigh, S.M.; Colins, M.; September, A.V. Polymorphisms within the COL5A1 gene and regulators of the extracellular matrix modify the risk of Achilles tendon pathology in a British case-control study. J. Sports Sci. 2017, 35, 1475–1483. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total n = 250 | Case n = 124 | Control n = 126 | p-Value Case vs. Control * | |||||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |||
| Sex | Females | 200 | 80.00 | 104 | 83.87 | 96 | 76.19 | 0.129 |
| Males | 50 | 20.00 | 20 | 16.13 | 30 | 23.81 | ||
| Age | Mean | 38.15 | 32.36 | 43.86 | <0.0001 | |||
| SD | 17.03 | 13.03 | 18.56 | |||||
| Case | Control | OR | CI 95% | p-Value ** | |||
|---|---|---|---|---|---|---|---|
| rs13946—COL5A1 | |||||||
| reference | TT | 50 (40.7%) | 65 (52.4%) | 1 | |||
| CC | 19 (15.4%) | 14 (11.3%) | 0.5668 | 0.2591 | 1.2397 | 0.1551 | |
| CT | 54 (43.9%) | 45 (36.3%) | 0.641 | 0.3737 | 1.1009 | 0.1070 | |
| rs12722—COL5A1 | |||||||
| reference | TT | 66 (53.2%) | 45 (36.9%) | 1 | |||
| CC | 27 (21.8%) | 26 (21.3%) | 1.4123 | 0.7311 | 2.7284 | 0.1334 | |
| CT | 31 (25.0%) | 51 (41.8%) | 2.4129 | 1.3436 | 4.3333 | 0.0032 * | |
| Rs12722 | aOR | aOR 95% CI | p |
|---|---|---|---|
| CT | 2.413 | 1.344–4.333 | 0.003 |
| CC | 1.708 | 0.849–3.439 | 0.133 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dalewski, B.; Białkowska, K.; Pałka, Ł.; Jakubowska, A.; Kiczmer, P.; Sobolewska, E. COL5A1 RS12722 Is Associated with Temporomandibular Joint Anterior Disc Displacement without Reduction in Polish Caucasians. Cells 2021, 10, 2423. https://doi.org/10.3390/cells10092423
Dalewski B, Białkowska K, Pałka Ł, Jakubowska A, Kiczmer P, Sobolewska E. COL5A1 RS12722 Is Associated with Temporomandibular Joint Anterior Disc Displacement without Reduction in Polish Caucasians. Cells. 2021; 10(9):2423. https://doi.org/10.3390/cells10092423
Chicago/Turabian StyleDalewski, Bartosz, Katarzyna Białkowska, Łukasz Pałka, Anna Jakubowska, Paweł Kiczmer, and Ewa Sobolewska. 2021. "COL5A1 RS12722 Is Associated with Temporomandibular Joint Anterior Disc Displacement without Reduction in Polish Caucasians" Cells 10, no. 9: 2423. https://doi.org/10.3390/cells10092423
APA StyleDalewski, B., Białkowska, K., Pałka, Ł., Jakubowska, A., Kiczmer, P., & Sobolewska, E. (2021). COL5A1 RS12722 Is Associated with Temporomandibular Joint Anterior Disc Displacement without Reduction in Polish Caucasians. Cells, 10(9), 2423. https://doi.org/10.3390/cells10092423