
Heat Shock Protein 27 Is an Emerging Predictor of Contrast-Induced Acute Kidney Injury on Patients Subjected to Percutaneous Coronary Interventions

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. Percutaneous Coronary Interventions
2.3. Acute Kidney Injury Assessment
2.4. Clinical Data and Biochemical Measurements
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. The Influence of Radiographic Contrast Media on Serum Creatinine Levels
3.3. Differences between Patients with and without CI-AKI
3.4. Univariate and Multivariate Analyses for the Prediction for CI-AKI
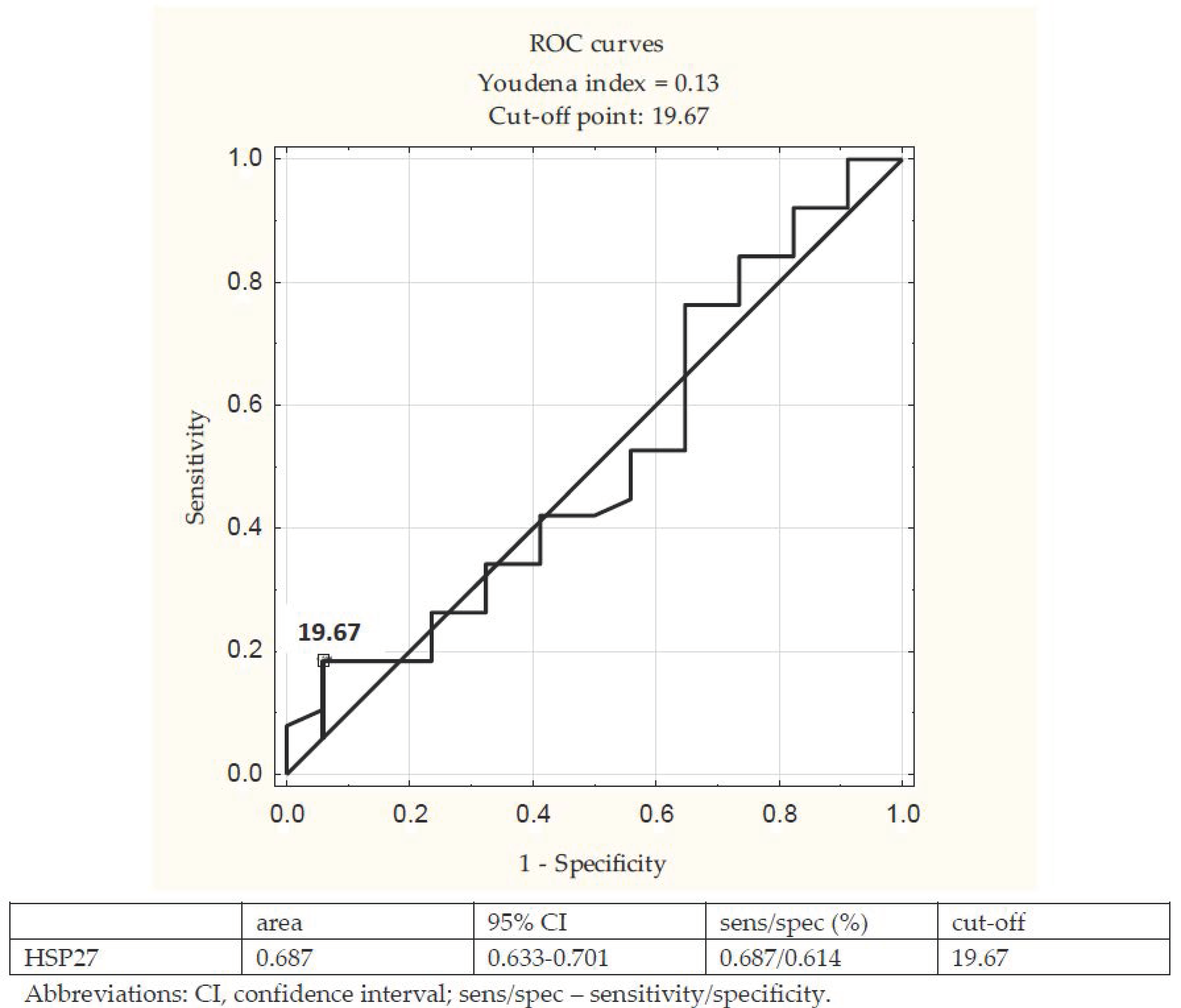
3.5. ROC Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability
Conflicts of Interest
References
- Tsai, T.; Patel, U.; Chang, T.; Kennedy, K.; Masoudi, F.; Matheny, M.; Kosiborod, M.; Amin, A.; Messenger, J.; Rumsfeld, J.; et al. Contemporary incidence, predictors, and outcomes of acute kidney injury in patients undergoing percuta-neous coronary interventions: Insights from the NCDR Cath-PCI registry. JACC Cardio. Int. 2014, 7, 1–9. [Google Scholar] [CrossRef]
- Andreucci, M.; Faga, T.; Pisani, A. Prevention of Contrast-Induced Nephropathy through a Knowledge of Its Pathogene-sis and Risk Factors. Sci. World J. 2014, 2014, 823169. [Google Scholar] [CrossRef]
- Krasinski, Z.; Krasińska, B.; Olszewska, M.; Pawlaczyk, K. Acute Renal Failure/Acute Kidney Injury (AKI) Associated with Endovascular Procedures. Diagnostics 2020, 10, 274. [Google Scholar] [CrossRef]
- Mamoulakis, C.; Tsarouhas, K.; Fragkiadoulaki, I.; Heretis, I.; Wilks, M.F.; Spandidos, D.A.; Tsitsimpikou, C.; Tsatsakis, A. Contrast-induced nephropathy: Basic concepts, pathophysiological implications and prevention strategies. Pharmacol. Ther. 2017, 180, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Gassanov, N.; Nia, A.M.; Caglayan, E.; Er, F. Remote Ischemic Preconditioning and Renoprotection: From Myth to a Novel Therapeutic Option? J. Am. Soc. Nephrol. 2013, 25, 216–224. [Google Scholar] [CrossRef]
- Matsumoto, T.; Urushido, M.; Ide, H.; Ishihara, M.; Hamada-Ode, K.; Shimamura, Y.; Ogata, K.; Inoue, K.; Taniguchi, Y.; Taguchi, T.; et al. Small Heat Shock Protein Beta-1 (HSPB1) Is Upregulated and Regulates Autophagy and Apoptosis of Renal Tubular Cells in Acute Kidney Injury. PLoS ONE 2015, 10, e0126229. [Google Scholar] [CrossRef] [PubMed]
- Pistolesi, V.; Regolisti, G.; Morabito, S.; Gandolfini, I.; Corrado, S.; Piotti, G.; Fiaccadori, E. Contrast medium induced acute kidney injury: A narrative review. J. Nephrol. 2018, 31, 797–812. [Google Scholar] [CrossRef]
- Marquez, E.; Sadowski, E.; Reese, S.; Vidyasagar, A.; Artz, N.; Fain, S.; Jacobson, L.; Swain, W.; Djamali, A. Serum HSP27 is associated with medullary perfusion in kidney allografts. J. Nephrol. 2012, 25, 1075–1080. [Google Scholar] [CrossRef]
- E Smoyer, W.; Ransom, R.; Harris, R.C.; Welsh, M.J.; Lutsch, G.; Benndorf, R. Ischemic acute renal failure induces differential expression of small heat shock proteins. J. Am. Soc. Nephrol. 2000, 11, 211–221. [Google Scholar]
- Inia, J.A.; O’Brien, E.R. Role of Heat Shock Protein 27 in Modulating Atherosclerotic Inflammation. J. Cardiovasc. Transl. Res. 2021, 14, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Jia, K.; Sun, D.; Yang, M. Protective effect of HSP27 in atherosclerosis and coronary heart disease by inhibiting reactive oxygen species. J. Cell. Biochem. 2018, 120, 2859–2868. [Google Scholar] [CrossRef]
- Guo, Q.; Du, X.; Zhao, Y.; Zhang, D.; Yue, L.; Wang, Z. Ischemic post conditioning prevents renal ischemia reperfusion injury through the induction of heat shock proteins in rats. Mol. Med. Rep. 2014, 10, 2875–2881. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, S.; Harrison, E.M.; Ross, J.A.; Wigmore, S.J.; Hughes, J. Heat-Shock Proteins and Acute Ischaemic Kidney Injury. Nephron 2014, 126, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Jaroszyński, A.; Jaroszyńska, A.; Siebert, J.; Dąbrowski, W.; Niedziałek, J.; Bednarek-Skublewska, A.; Zapolski, T.; Wysokiński, A.; Załuska, W.; Książek, A.; et al. The prognostic value of positive T-wave in lead aVR in hemodialy-sis patients. Clin. Exp. Nephrol. 2015, 19, 1157–1164. [Google Scholar] [CrossRef][Green Version]
- Martínez-Laorden, E.; Navarro-Zaragoza, J.; Milanés, M.V.; Laorden, M.L.; Almela, P. Cardiac Protective Role of Heat Shock Protein 27 in the Stress Induced by Drugs of Abuse. Int. J. Mol. Sci. 2020, 21, 3623. [Google Scholar] [CrossRef]
- Levine, G.; Bates, E.; Blankenship, J.; Bailey, S.; Bittl, J.; Cercek, B.; Chambers, C.; Ellis, S.; Guyton, R.; Hollenberg, S.; et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: A report of the American College of Car-diology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation 2011, 124, 574–651. [Google Scholar] [CrossRef]
- Mehta, R.L.; A Kellum, J.; Shah, S.V.; A Molitoris, B.; Ronco, C.; Warnock, D.G.; Levin, A. Acute Kidney Injury Network: Report of an initiative to improve outcomes in acute kidney injury. Crit. Care 2007, 11, R31. [Google Scholar] [CrossRef] [PubMed]
- Golshahi, J.; Nasri, H.; Gharipour, M. Contrast-induced nephropathy; A literature review. J. Nephropathol. 2014, 3, 51–56. [Google Scholar]
- The ad-hoc Working Group of ERBP; Fliser, D.; Laville, M.; Covic, A.; Fouque, D.; Vanholder, R.; Juillard, L.; Van Biesen, W. A European Renal Best Practice (ERBP) position statement on the Kidney Disease Improving Global Outcomes (KDIGO) Clinical Practice Guidelines on Acute Kidney Injury: Part 1: Definitions, conservative management and contrast-induced nephropathy. Nephrol. Dial. Transplant. 2012, 27, 4263–4272. [Google Scholar] [CrossRef] [PubMed]
- Negishi, Y.; Tanaka, A.; Ishii, H.; Takagi, K.; Inoue, Y.; Uemura, Y.; Umemoto, N.; Yoshioka, N.; Morishima, I.; Asano, H.; et al. Contrast-Induced Nephropathy and Long-Term Clinical Outcomes Following Percutaneous Coronary Intervention in Patients With Advanced Renal Dysfunction (Estimated Glomerular Filtration Rate < 30 mL/min/1.73 m2). Am. J. Cardiol. 2019, 123, 361–367. [Google Scholar]
- Wu, R.; Kong, Y.; Yin, J.; Liang, R.; Lu, Z.; Wang, N.; Zhao, Q.; Zhou, Y.; Yan, C.; Wang, F.; et al. Antithrombin Ⅲ is a Novel Predictor for Contrast Induced Nephropathy After Coronary Angiography. Kidney Blood Press. Res. 2018, 43, 170–180. [Google Scholar] [CrossRef]
- Demir, O.; Lombardo, F.; Poletti, E.; Laricchia, A.; Beneduce, A.; Maccagni, D.; Slavich, M.; Giannini, F.; Carlino, M.; Margonato, A.; et al. Contrast-Induced Nephropathy After Percutaneous Coronary Intervention for Chronic Total Occlu-sion Versus Non-Occlusive Coronary Artery Disease. Am. J. Cardiol. 2018, 122, 1837–1842. [Google Scholar] [CrossRef] [PubMed]
- Chebotareva, N.; Bobkova, I.; Shilov, E. Heat shock proteins and kidney disease: Perspectives of HSP therapy. Cell Stress Chaperones 2017, 22, 319–343. [Google Scholar] [CrossRef]
- Tian, X.; Zhao, L.; Song, X.; Yan, Y.; Liu, N.; Li, T.; Yan, B.; Liu, B. HSP27 Inhibits Homocysteine-Induced Endothelial Apoptosis by Modulation of ROS Production and Mitochondrial Caspase-Dependent Apoptotic Pathway. BioMed Res. Int. 2016, 2016, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Lun, M.; Schworer, C.; Blasick, T.; Marker, K.; Jones, J.; Carey, D. Heat-shock protein expression is highly sen-sitive to ischemia reperfusion injury in rat kidneys. Ann. Clin. Lab. Sci. 2008, 38, 57–64. [Google Scholar] [PubMed]
- Rodríguez-Iturbe, B.; Johnson, R.J. Heat shock proteins and cardiovascular disease. Physiol. Int. 2018, 105, 19–37. [Google Scholar] [CrossRef]
- Bellamy, C.O.; O’Neill, S.; Ingman, T.G.; Wigmore, S.J.; Harrison, E.M. Differential expression of heat shock proteins in healthy and diseased human renal allografts. Ann. Transplant. 2013, 18, 550–557. [Google Scholar] [CrossRef]
- Jaroszyński, A.; Jaroszyńska, A.; Zaborowski, T.; Drelich-Zbroja, A.; Zapolski, T.; Dąbrowski, W. Serum heat shock pro-tein 27 levels predict cardiac mortality in hemodialysis patients. BMC Nephrol. 2018, 19, 359. [Google Scholar] [CrossRef]
- Kim, M.; Park, S.; Kim, M.; Chen, S.; Gerthoffer, W.; D‘Agati, V.; Lee, H. Selective renal over expression of human heat shock protein 27 reduces renal ischemia-reperfusion injury in mice. Am. J. Physiol. Renal Physiol. 2010, 299, 347–358. [Google Scholar] [CrossRef]
- Fujigaki, Y.; Sun, Y.; Fujikura, T.; Sakao, Y.; Togawa, A.; Suzuki, H.; Yasuda, H.; Hishida, A. Immunohistochemical study of heat shock protein 27 with respekt to survival and regeneration of proximal tubular cells after uranylacetate-induced acute tubular injury in rats. Ren. Fail. 2010, 32, 119–125. [Google Scholar] [CrossRef]


{kind=link}
| Parameter | All Patients n = 343 | CI-AKI n = 32 | Non CI-AKI n = 311 | p |
|---|---|---|---|---|
| Age (years) | 66.36 ± 7.32 | 72.8 ± 6.72 | 64.4 ± 6.95 | <0.001 |
| Female gender (%) | 38.2 | 46.9 | 37.3 | 0.021 |
| Prior MI (%) | 25.9 | 27.3 | 25.8 | 0.496 |
| Diabete smellitus (%) | 48.0 | 63.4 | 45.1 | 0.011 |
| Hypertension (%) | 83.7 | 81.1 | 83.9 | 0.504 |
| Smoking (%) | 18.1 | 17.8 | 18.2 | 0.687 |
| EF (%) | 54.83 ± 5.33 | 52.70 ± 5.21 | 55.14 ± 5.56 | 0.165 |
| Hemoglobin (g/dL) | 11.68 ± 1.09 | 10.43 ± 1.08 | 11.98 ±1.02 | 0.091 |
| Total cholesterol (mg/dL) | 188.3 ± 37.35 | 188.2 ± 35.15 | 188.3 ± 37.35 | 0.674 |
| LDL cholesterol (mg/dL) | 114.8 ± 30.11 | 116.2 ± 29.19 | 114.7 ± 29.08 | 0.544 |
| HDL cholesterol (mg/dL) | 43.82 ± 17.08 | 43.41 ± 16.89 | 43.85 ± 16.45 | 0.715 |
| Triglycerides (mg/dL) | 176.3 ± 59.27 | 170.2 ± 59.03 | 176.6 ± 58.9 | 0.314 |
| Hypotension during PCI (%) | 9.5 | 22.7 | 8.1 | <0.001 |
| RCM volume (mL) | 179 ± 58 | 198 ± 41 | 175.2 ± 52 | 0.006 |
| CV > MACD (%) | 20.1 | 28.1 | 19.4 | <0.001 |
| Number of diseased vessels (n) | 2.3 ± 0.7 | 2.6 ± 0.8 | 2.2 ± 0.7 | 0.002 |
| eGFR (mL/min/1.73 m2) | 62.7 ± 9.04 | 59.9 ± 8.31 | 62.90 ± 8.91 | 0.114 |
| Albuminuria (%) | 18.1 | 25.0 | 17.7 | 0.004 |
| HSP27 (µg/L) | 32.7 ± 8.14 | 21.19 ± 7.87 | 35.3 ± 8.11 | <0.001 |
| ACE/ARB (%) | 86.0 | 87.5 | 85.6 | 0.327 |
| Beta blockers (%) | 75.8 | 78.1 | 74.9 | 0.213 |
| Statins (%) | 82.2 | 81.3 | 82.90 | 0.614 |
| Diuretics (%) | 19.0 | 18.8 | 19.1 | 0.799 |
| Parameter | Univariate OR (95% CI) | p | Multivariate OR (95% CI) | p |
|---|---|---|---|---|
| Age (years) | 1.31 (1.07–1.1.58) | <0.001 | 1.18 (0.98–1.92) | 0.104 |
| Female gender (%) | 1.26 (0.98–2.17) | 0.021 | 1.23 (0.79–2.31) | 0.113 |
| Prior MI (%) | 1.12 (0.64–2.23) | 0.187 | ||
| Diabete mellitus (%) | 1.09 (0.73–1.549 | 0.016 | 1.11 (0.63–1.83) | 0.247 |
| Hypertension (%) | 1.13 (0.73–2.051) | 0.285 | ||
| Smoking (%) | 1.35 (0.77–2.87) | 0.297 | ||
| EF (%) | 0.85 (0.51–1.18) | 0.009 | 0.96 (0.65–2.01) | 0.237 |
| Hemoglobin (g/dL) | 0.89 (0.74–1.43) | 0.022 | 0.88 (0.62–2.41) | 0.211 |
| Total cholesterol (mg/dL) | 1.09 (0.78–2.67) | 0.477 | ||
| LDL cholesterol (mg/dL) | 1.28 (0.73–2.05) | 0.201 | ||
| HDL cholesterol (mg/dL) | 0.91 (0.69–1.57) | 0.286 | ||
| Triglycerides (mg/dL) | 1.17 (0.82–1.84) | 0.366 | ||
| ACE/ARB (%) | 1.02 (0.45–2.04) | 0.527 | ||
| Beta blockers (%) | 0.97 (0.54–2.36) | 0.525 | ||
| Statins (%) | 0.92 (0.56–2.11) | 0.218 | ||
| Diuretics (%) | 1.03 (0.44–2.11) | 0.233 | ||
| Albuminuria (%) | 1.11 (0.86–2.01) | 0.014 | 1.08 (0.69–3.02) | 0.171 |
| Hypotension during PCI (%) | 1.21 (1.03–2.13) | 0.013 | 1.18 (0.93–2.57) | 0.089 |
| CV > MACD (%) | 1.39 (1.05–2.17) | <0.001 | 1.23 (0.99–2.11) | 0.001 |
| Number of diseased vessels (n) | 1.33 (1.03–2.18) | 0.004 | 1.27 (0.99–2.03) | 0.006 |
| eGFR (mL/min/1.73 m2) | 0.80 (0.37–1.81) | 0.189 | ||
| HSP27 (µg/L) | 0.78 (0.53–1.11) | <0.001 | 0.81 (0.51–1.37) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaroszyński, A.; Zaborowski, T.; Głuszek, S.; Zapolski, T.; Sadowski, M.; Załuska, W.; Cedro, A.; Małecka-Massalska, T.; Dąbrowski, W. Heat Shock Protein 27 Is an Emerging Predictor of Contrast-Induced Acute Kidney Injury on Patients Subjected to Percutaneous Coronary Interventions. Cells 2021, 10, 684. https://doi.org/10.3390/cells10030684
Jaroszyński A, Zaborowski T, Głuszek S, Zapolski T, Sadowski M, Załuska W, Cedro A, Małecka-Massalska T, Dąbrowski W. Heat Shock Protein 27 Is an Emerging Predictor of Contrast-Induced Acute Kidney Injury on Patients Subjected to Percutaneous Coronary Interventions. Cells. 2021; 10(3):684. https://doi.org/10.3390/cells10030684
Chicago/Turabian StyleJaroszyński, Andrzej, Tomasz Zaborowski, Stanisław Głuszek, Tomasz Zapolski, Marcin Sadowski, Wojciech Załuska, Anna Cedro, Teresa Małecka-Massalska, and Wojciech Dąbrowski. 2021. "Heat Shock Protein 27 Is an Emerging Predictor of Contrast-Induced Acute Kidney Injury on Patients Subjected to Percutaneous Coronary Interventions" Cells 10, no. 3: 684. https://doi.org/10.3390/cells10030684
APA StyleJaroszyński, A., Zaborowski, T., Głuszek, S., Zapolski, T., Sadowski, M., Załuska, W., Cedro, A., Małecka-Massalska, T., & Dąbrowski, W. (2021). Heat Shock Protein 27 Is an Emerging Predictor of Contrast-Induced Acute Kidney Injury on Patients Subjected to Percutaneous Coronary Interventions. Cells, 10(3), 684. https://doi.org/10.3390/cells10030684