
Decoupled Glucose and Lipid Metabolic Recovery after Viral Clearance in Direct-Acting Antiviral-Treated HCV Patients: A 3-Year Prospective Cohort Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Study Design
2.3. Statistics
2.4. Informed Consent
3. Results
3.1. Baseline Characteristics of CHC Patients
3.2. Baseline Associations of CHC Patients: Lipid, Virus, Fibrosis, and IFNL3 Profiles with TC; and TC and BMI with HOMA-IR
3.3. Posttherapy Associations of SVR Patients: Lipid Profile Consistent with TC and TC Negatively with HOMA-IR
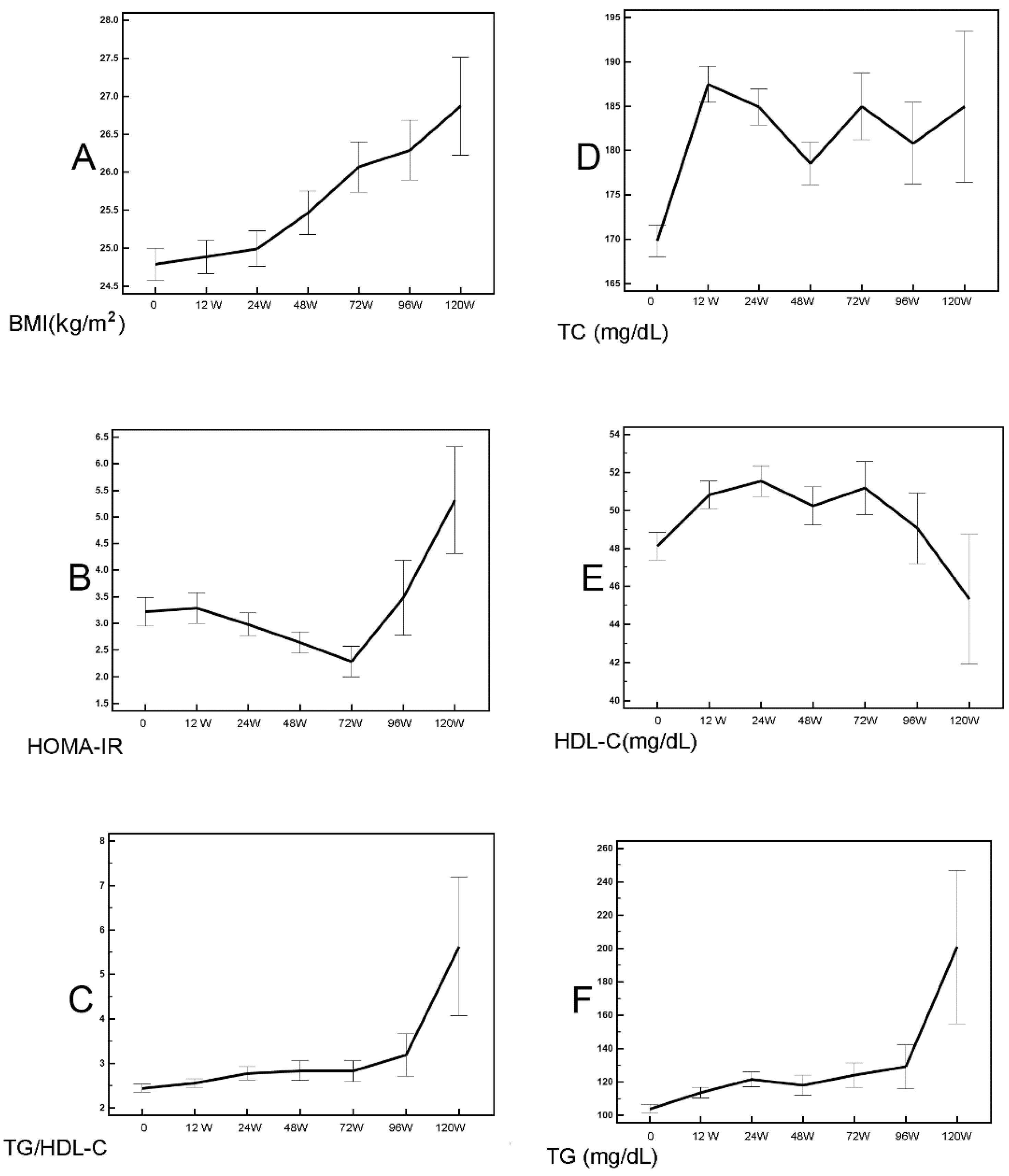
3.4. Alterations of Various Profiles in SVR Patients: Progressively Increased BMI and TG/HDL-C; HOMA-IR Reached Its Nadir at 72 Weeks Post-Therapy
3.5. Various Metabolic Profile Alteration in SVR Patients with and without Baseline IR: Increased BMI but Decreased HOMA-IR Were Noted Earlier in Patients with Than Patients without IR
3.6. Comparisons between Post-Therapy Metabolic Profiles of SVR Patients and Controls: SVR Patients Had Higher BMI and HOMA-IR Levels in the Subgroup without Baseline IR
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Borgia, S.M.; Hedskog, C.; Parhy, B.; Hyland, R.H.; Stamm, L.M.; Brainard, D.M.; Subramanian, M.G.; McHutchison, J.G.; Mo, H.; Svarovskaia, E.; et al. Identification of a novel hepatitis c virus genotype from Punjab, India: Expanding classification of hepatitis c virus into 8 genotypes. J. Infect. Dis. 2018, 218, 1722–1729. [Google Scholar] [CrossRef] [Green Version]
- Spearman, C.W.; Dusheiko, G.M.; Hellard, M.; Sonderup, M. Hepatitis C. Lancet 2019, 394, 1451–1466. [Google Scholar] [CrossRef]
- Chang, M.L. Metabolic alterations and hepatitis C: From bench to bedside. World J. Gastroenterol. 2016, 22, 1461–1476. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.L.; Yang, S.S. Metabolic signature of hepatic fibrosis: From individual pathways to systems biology. Cells 2019, 8, 1423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toyoda, H.; Kumada, T.; Tada, T.; Kiriyama, S.; Kiriyama, M.; Hisanaga, Y.; Kanamori, A.; Kitabatake, S.; Ito, T. Risk factors of hepatocellular carcinoma development in non-cirrhotic patients with sustained virologic response for chronic hepatitis C virus infection. J. Gastroenterol. Hepatol. 2015, 30, 1183–1189. [Google Scholar] [CrossRef]
- Grunt, T.W. Interacting cancer machineries: Cell signaling, lipid metabolism, and epigenetics. Trends Endocrinol. Metab. 2018, 29, 86–98. [Google Scholar] [CrossRef]
- Diakos, C.I.; Charles, K.A.; McMillan, D.C.; Clarke, S.J. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014, 15, e493–e503. [Google Scholar] [CrossRef]
- Stone, N.J.; Robinson, J.G.; Lichtenstein, A.H.; Merz, C.N.B.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Levy, D.; Lloyd-Jones, D.M.; et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129, S1–S45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, K.; Nelson, R.A.; Wactawski-Wende, J.; Lee, D.J.; Manson, J.E.; Aragaki, A.K.; Mortimer, J.E.; Phillips, S.L.; Rohan, T.; Ho, G.Y.F.; et al. Insulin resistance and cancer-specific and all-cause mortality in postmenopausal women: The women’s health initiative. J. Natl. Cancer Inst. 2020, 112, 170–178. [Google Scholar] [CrossRef]
- Hamamoto, S.; Uchida, Y.; Wada, T.; Moritani, M.; Sato, S.; Hamamoto, N.; Ishihara, S.; Watanabe, M.; Kinoshita, Y. Changes in serum lipid concentrations in patients with chronic hepatitis C virus positive hepatitis responsive or non-responsive to interferon therapy. J. Gastroenterol. Hepatol. 2005, 20, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Teijaro, J.R. Pleiotropic roles of type 1 interferons in antiviral immune responses. Adv. Immunol. 2016, 132, 135–158. [Google Scholar]
- Halfon, P.; Locarnini, S. Hepatitis C virus resistance to protease inhibitors. J. Hepatol. 2011, 55, 192–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doyle, M.A.; Galanakis, C.; Mulvihill, E.; Crawley, A.; Cooper, C.L. Hepatitis C direct acting antivirals and ribavirin modify lipid but not glucose parameters. Cells 2019, 8, 252. [Google Scholar] [CrossRef] [Green Version]
- Mauss, S.; Berger, F.; Wehmeyer, M.H.; Ingiliz, P.; Hueppe, D.; Lutz, T.; Simon, K.G.; Schewe, K.; Rockstroh, J.K.; Baumgarten, A.; et al. Effect of antiviral therapy for HCV on lipid levels. Antivir. Ther. 2017, 21, 81–88. [Google Scholar] [CrossRef]
- Drazilova, S.; Gazda, J.; Janicko, M.; Jarcuska, P. Chronic Hepatitis C association with diabetes mellitus and cardiovascular risk in the era of DAA therapy. Can. J. Gastroenterol. Hepatol. 2018, 2018, 6150861. [Google Scholar] [CrossRef]
- Lacerda, G.S.; Medeiros, T.; Rosáriol, N.F.D.; Peralta, R.H.S.; Cabral-Castro, M.J.; Esberard, E.B.C.; de Andrade, T.G.; Xavier, A.R.; Silva, A.A. Exploring lipid and apolipoprotein levels in chronic hepatitis C patients according to their response to antiviral treatment. Clin. Biochem. 2018, 60, 17–23. [Google Scholar] [CrossRef]
- Shimizu, K.; Soroida, Y.; Sato, M.; Hikita, H.; Kobayashi, T.; Endo, M.; Sato, M.; Gotoh, H.; Iwai, T.; Tateishi, R.; et al. Eradication of hepatitis C virus is associated with the attenuation of steatosis as evaluated using a controlled attenuation parameter. Sci. Rep. 2018, 8, 7845. [Google Scholar] [CrossRef]
- Sun, H.Y.; Cheng, P.N.; Tseng, C.Y.; Tsai, W.J.; Chiu, Y.C.; Young, K.C. Favouring modulation of circulating lipoproteins and lipid loading capacity by direct antiviral agents grazoprevir/elbasvir or ledipasvir/sofosbuvir treatment against chronic HCV infection. Gut 2018, 67, 1342–1350. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, S.; Yatsuhashi, H.; Abiru, S.; Yamasaki, K.; Komori, A.; Nagaoka, S.; Saeki, A.; Uchida, S.; Bekki, S.; Kugiyama, Y.; et al. Rapid increase in serum low-density lipoprotein cholesterol concentration during hepatitis c interferon-free treatment. PLoS ONE. 2016, 11, e0163644. [Google Scholar] [CrossRef]
- Alsebaey, A.; Elhelbawy, M.; Abdel-Razek, W.; Hashim, M.; Elshenawy, H.; Waked, I. HCV treatment with direct acting antivirals improves the insulin sensitivity. Expert Rev. Anti-Infect. Ther. 2019, 17, 749–754. [Google Scholar] [CrossRef] [PubMed]
- Adinolfi, L.E.; Nevola, R.; Guerreral, B.; D’Alterio, G.; Marrone, A.; Giordano, M.; Rinaldi, L. Hepatitis C virus clearance by direct-acting antiviral treatments and impact on insulin resistance in chronic hepatitis C patients. J. Gastroenterol. Hepatol. 2018, 33, 1379–1382. [Google Scholar] [CrossRef] [PubMed]
- Weidner, P.; Boettche, D.; Zimmerer, T.; Burgermeister, E.; Teufel, A.; Ebert, M.; Antoni, C. Impact of direct acting antiviral (DAA) treatment on glucose metabolism and reduction of pre-diabetes in patients with chronic hepatitis C. J. Gastrointestin. Liver Dis. 2018, 27, 281–289. [Google Scholar] [CrossRef] [Green Version]
- Beig, J.; Orr, D.; Harrison, B.; Gane, E. Hepatitis C virus eradication with new interferon-free treatment improves metabolic profile in hepatitis c virus-related liver transplant recipients. Liver Transpl. 2018, 24, 1031–1039. [Google Scholar] [CrossRef] [Green Version]
- Petta, S.; Adinolfi, L.E.; Fracanzani, A.L.; Rini, F.; Caldarella, R.; Calvaruso, V.; Cammà, C.; Cammà, M.; Marco, V.D.; Grimaudo, S.; et al. Hepatitis C virus eradication by direct-acting antiviral agents improves carotid atherosclerosis in patients with severe liver fibrosis. J. Hepatol. 2018, 69, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.L.; Kuo, C.J.; Pao, L.H.; Hsu, C.M.; Chiu, C.T. The evolving relationship between adiponectin and insulin sensitivity in hepatitis C patients during viral clearance. Virulence 2017, 8, 1255–1264. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.C.; Cheng, H.H.; Chen, S.C.; Shen, W.C.; Huang, Y.T. Pre-treatment high body mass index is associated with poor survival in Asian premenopausal women with localized breast cancer. J. Cancer 2021, 12, 4488–4496. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 2. Classification and diagnosis of diabetes: Standards of medical care in diabetes—2019. Diabetes Care. 2019, 42 (Suppl. S1), S13–S28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, X.L.; Jiang, L.S.; Wu, C.S.; Pan, L.Y.; Lou, Z.Q.; Peng, C.T.; Dong, Y.; Ruan, B. The role of fibrosis index FIB-4 in predicting liver fibrosis stage and clinical prognosis: A diagnostic or screening tool? J. Formos. Med. Assoc. 2021. [Google Scholar] [CrossRef]
- da Luz, P.L.; Favarato, D.; Faria-Neto, J.R., Jr.; Lemos, P.; Chagas, A.C. High ratio of triglycerides to HDL-cholesterol predicts extensive coronary disease. Clinics 2008, 63, 427–432. [Google Scholar] [CrossRef] [Green Version]
- Yeh, W.C.; Tsao, Y.C.; Li, W.C.; Tzeng, I.; Chen, L.S.; Chen, J.Y. Elevated triglyceride-to-HDL cholesterol ratio is an indicator for insulin resistance in middle-aged and elderly Taiwanese population: A cross-sectional study. Lipids Health Dis. 2019, 18, 176. [Google Scholar] [CrossRef] [Green Version]
- Pantoja-Torres, B.; Toro-Huamanchumo, C.J.; Urrunaga-Pastor, D.; Guarnizo-Poma, M.; Lazaro-Alcantara, H.; Paico-Palacios, S.; Ranilla-Seguin, V.d.C.; Benites-Zapata, V.A.; Insulin Resistance and Metabolic Syndrome Research Group. High triglycerides to HDL-cholesterol ratio is associated with insulin resistance in normal-weight healthy adults. Diabetes Metab. Syndr. 2019, 13, 382–388. [Google Scholar] [CrossRef]
- Chrostek, L.; Supronowicz, L.; Panasiuk, A.; Cylwik, B.; Gruszewska, E.; Flisiak, R. The effect of the severity of liver cirrhosis on the level of lipids and lipoproteins. Clin. Exp. Med. 2014, 14, 417–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.H.; Lao, X.Q.; Tillmann, H.L.; Rowell, J.; Patel, K.; Thompson, A.; Suchindran, S.; Muir, A.J.; Guyton, J.R.; Gardner, S.D.; et al. Interferon-lambda genotype and low serum low-density lipoprotein cholesterol levels in patients with chronic hepatitis C infection. Hepatology 2010, 51, 1904–1911. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, A.; Fukushima, M.; Sakai, M.; Kataoka, K.; Nagata, I.; Doi, K.; Arakawa, H.; Nagasaka, S.; Tokuyama, K.; Nakai, Y. The role of the body mass index and triglyceride levels in identifying insulin-sensitive and insulin-resistant variants in Japanese non-insulin-dependent diabetic patients. Metabolism 2000, 49, 1001–1005. [Google Scholar] [CrossRef]
- Patel, S.; Jinjuvadia, R.; Patel, R.; Liangpunsakul, S. Insulin resistance is associated with significant liver fibrosis in chronic hepatitis c patients: A systemic review and meta-analysis. J. Clin. Gastroenterol. 2016, 50, 80–84. [Google Scholar] [CrossRef] [Green Version]
- Ripoli, M.; Pazienza, V. Impact of HCV genetic differences on pathobiology of disease. Expert Rev. Anti. Infect. Ther. 2011, 9, 747759. [Google Scholar] [CrossRef] [PubMed]
- Shousha, H.I.; Abdelaziz, R.A.; Azab, S.M.; Khairy, M.; Afifi, S.A.; Mehrez, M.I.; Eshra, M.A.; Abdelrahim, A.Y. Effect of treatment with direct acting antivirals on body mass index and hepatic steatosis in chronic hepatitis C. J. Med. Virol. 2018, 90, 1099–1105. [Google Scholar] [CrossRef]
- Palaniappan, L.; Carnethon, M.R.; Wang, Y.; Hanley, A.J.; Fortmann, S.P.; Haffner, S.M.; Wagenknecht, L. Predictors of the incident metabolic syndrome in adults: The insulin resistance atherosclerosis study. Diabetes Care 2004, 27, 788–793. [Google Scholar] [CrossRef] [Green Version]
- Martinez, K.E.; Tucker, L.A.; Bailey, B.W.; LeCheminant, J.D. Expanded normal weight obesity and insulin resistance in US adults of the national health and nutrition examination survey. J. Diabetes Res. 2017, 2017, 9502643. [Google Scholar] [CrossRef]
- Tokarz, V.L.; MacDonald, P.E.; Klip, A. The cell biology of systemic insulin function. J. Cell Biol. 2018, 217, 2273–2289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kachhawa, P.; Kachhawa, K.; Agrawal, D.; Sinha, V.; Sarkar, P.D.; Kumar, S. Association of dyslipidemia, increased insulin resistance, and serum CA 15-3 with increased risk of breast cancer in urban areas of north and central India. J. Midlife Health. 2018, 9, 85–91. [Google Scholar] [PubMed]
- Cho, J.; Hong, H.; Park, S.; Kim, S.; Kang, H. Insulin resistance and its association with metabolic syndrome in Korean children. Biomed. Res. Int. 2017, 2017, 8728017. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 415) | Baseline IR (+) (n = 168) | Baseline IR (−) (n = 247) | p Values | |
|---|---|---|---|---|
| Sex (Male), n (%) | 191 (46) | 85 (50.6) | 102 (43.6) | 0.099 |
| Age (years) | 60.33 ±12.83 | 59.14 ± 12.95 | 61.38 ± 12.64 | 0.085 |
| BMI (kg/m2) | 24.69 ±34.92 | 26.72 ± 4.04 | 23.29 ± 3.18 | <0.001 |
| HCV genotype 1, n (%) | 244 (58.8) | 107 (63.7) | 131 (56.0) | 0.031 |
| HCV genotype 2, n (%) | 122 (29.4) | 42 (25.0) | 76 (32.5) | 0.088 |
| Log HCV RNA (logIU/mL) | 5.98 ± 0.87 | 6.01 ± 0.87 | 5.97 ± 0.88 | 0.612 |
| ALT(U/L) | 80.93 ± 91.26 | 93.83 ± 118.9 | 73.12 ± 65.99 | 0.027 |
| HOMA-IR | 3.21 ± 4.96 | 5.47 ± 7.07 | 1.59 ± 0.54 | <0.001 |
| HDL-C (mg/dL) | 48.27 ± 13.82 | 44.02 ± 10.97 | 51.10 ±14.67 | <0.001 |
| TG (mg/dL) | 102.26 ± 52.47 | 120.1 ± 63.3 | 89.57 ± 38.81 | <0.001 |
| TC (mg/dL) | 169.46 ± 34.91 | 169.7 ± 33.92 | 168.44 ± 34.38 | 0.716 |
| Liver cirrhosis, n (%) | 90 (21.6) | 48 (28.57) | 42 (17) | 0.007 |
| Diabetes mellitus, n (%) | 52 (12.5) | 48 (28.5) | 4 (1.6) | 0.004 |
| FIB-4 | 3.52 ±3.39 | 3.56 ± 3.44 | 3.58 ± 3.42 | 0.955 |
| IFNL3-rs12979860 CC genotype, n (%) | 351 (84.6) | 141 (83.3) | 210 (85) | 0.527 |
| HOMA-IR | TC (mg/dL) | |||
|---|---|---|---|---|
| Beta (95% CI of Beta) | p Values | Beta (95% CI of Beta) | p Values | |
| Sex (male) | 0.693 (−0.643~2.029) | 0.308 | −2.612 (−9.588~4.364) | 0.462 |
| Age (years) | −0.033 (−0.087~0.021) | 0.225 | −0.039 (−0.32 ~0.242) | 0.787 |
| BMI (kg/m2) | 0.187 (0.018~0.357) | 0.03 | 0.371 (−5.19~1.261) | 0.412 |
| Genotype 1 (yes) | −0.879 (−2.23~0.474) | 0.202 | 6.293 (−0.749~13.334) | 0.08 |
| Log HCV RNA (logIU/mL) | 0.521 (0.397~1.439) | 0.265 | 4.944 (0.182~9.706) | 0.042 |
| ALT(U/L) | −0.001 (−0.007~0.006) | 0.869 | 0.012 (−0.022~0.047) | 0.478 |
| HDL-C (mg/dL) | −0.008 (−0.07~0.054) | 0.807 | 1.282 (1.000~1.564) | <0.001 |
| TG (mg/dL) | 0.019 (0.004~0.033) | 0.011 | 0.222 (0.15~0.294) | <0.001 |
| TC (mg/dL) | −0.002 (−0.016~0.013) | 0.851 | NA | |
| HOMA-IR | NA | −0.061 (−6.99~0.577) | 0.851 | |
| Liver cirrhosis (yes) | −0.067 (−1.699~1.564) | 0.935 | −6.967 (−15.433~1.500) | 0.106 |
| FIB-4 | 0.054 (−0.155~0.262) | 0.612 | −1.459 (−2.53~−0.386) | 0.008 |
| IFNL3 CC genotype (yes) | 0.06 (−1.744~1.863) | 0.948 | 10.24 (0.919~19.565) | 0.031 |
| 12-Week Posttherapy vs. Baseline (n = 360) | 24-Week Posttherapy vs. Baseline (n = 317) | 48-Week Posttherapy vs. Baseline (n = 248) | 72-Week Posttherapy vs. Baseline (n = 191) | 96-Week Posttherapy vs. Baseline (n = 159) | 120-Week Posttherapy vs. Baseline (n = 96) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Difference | p Values | Difference | p Values | Difference | p Values | Difference | p Values | Difference | p Values | Difference | p Values | |
| BMI (kg/m2) | 0.09 ± 0.06 | 0.111 | 0.2 ± 0.07 | 0.007 | 0.48 ± 0.10 | <0.001 | 0.76 ± 0.12 | <0.001 | 0.97 ± 0.183 | <0.001 | 1.57 ± 0.292 | <0.001 |
| ALT(U/L) | −58.9 ± 4.62 | <0.001 | −60.2 ± 4.94 | <0.001 | −66.6 ± 6.44 | <0.001 | −59.8 ± 5.00 | <0.001 | −57.7 ± 7.18 | <0.001 | −63.7 ± 10.6 | <0.001 |
| FIB-4 | −0.71 ± 0.08 | <0.001 | −0.32 ± 0.15 | <0.001 | −1.25 ± 0.214 | <0.001 | −1.12 ± 0.40 | <0.001 | −1.82 ± 0.37 | <0.001 | −1.05 ± 3.14 | 0.007 |
| TC (mg/dL) | 17.6 ± 1.44 | <0.001 | 14.4 ± 1.60 | <0.001 | 10.3 ± 1.84 | <0.001 | 14.5 ± 3.05 | <0.001 | 13.4 ± 3.72 | 0.001 | 22.3 ± 8.63 | 0.018 |
| TG (mg/dL) | 9.82 ± 2.58 | <0.001 | 18.7 ± 3.63 | <0.001 | 19.4 ± 5.11 | <0.001 | 25.6 ± 5.61 | <0.001 | 29.6 ± 8.45 | <0.001 | 38.9 ± 9.6 | <0.001 |
| HDL-C (mg/dL) | 2.86 ± 0.48 | <0.001 | 3.09 ± 5.21 | <0.001 | 1.80 ± 0.64 | 0.005 | 2.89 ± 0.92 | 0.002 | 2.13 ± 0.97 | 0.004 | −0.48 ± 2.01 | 0.034 |
| TG/HDL-C | 0.10 ± 0.07 | 0.191 | 0.38 ± 0.11 | 0.001 | 0.55 ± 0.18 | 0.003 | 0.53 ± 0.16 | 0.001 | 0.77 ± 0.29 | 0.011 | 2.76 ± 1.10 | 0.021 |
| HOMA-IR | 0.11 ± 0.23 | 0.626 | −0.22 ± 0.31 | 0.479 | −0.77 ± 0.52 | 0.147 | −0.41 ± 0.19 | 0.039 | 0.38 ± 0.14 | 0.436 | 1.03 ± 0.68 | 0.16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.; Chien, R.-N.; Pao, L.-H.; Kuo, C.-J.; Huang, P.-H.; Chang, M.-L. Decoupled Glucose and Lipid Metabolic Recovery after Viral Clearance in Direct-Acting Antiviral-Treated HCV Patients: A 3-Year Prospective Cohort Study. Cells 2021, 10, 2934. https://doi.org/10.3390/cells10112934
Lee H, Chien R-N, Pao L-H, Kuo C-J, Huang P-H, Chang M-L. Decoupled Glucose and Lipid Metabolic Recovery after Viral Clearance in Direct-Acting Antiviral-Treated HCV Patients: A 3-Year Prospective Cohort Study. Cells. 2021; 10(11):2934. https://doi.org/10.3390/cells10112934
Chicago/Turabian StyleLee, Heng, Rong-Nan Chien, Li-Heng Pao, Chia-Jung Kuo, Po-Han Huang, and Ming-Ling Chang. 2021. "Decoupled Glucose and Lipid Metabolic Recovery after Viral Clearance in Direct-Acting Antiviral-Treated HCV Patients: A 3-Year Prospective Cohort Study" Cells 10, no. 11: 2934. https://doi.org/10.3390/cells10112934
APA StyleLee, H., Chien, R.-N., Pao, L.-H., Kuo, C.-J., Huang, P.-H., & Chang, M.-L. (2021). Decoupled Glucose and Lipid Metabolic Recovery after Viral Clearance in Direct-Acting Antiviral-Treated HCV Patients: A 3-Year Prospective Cohort Study. Cells, 10(11), 2934. https://doi.org/10.3390/cells10112934