
Osteosarcoma in Adolescents and Young Adults

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Statistical Analyses
3. Results
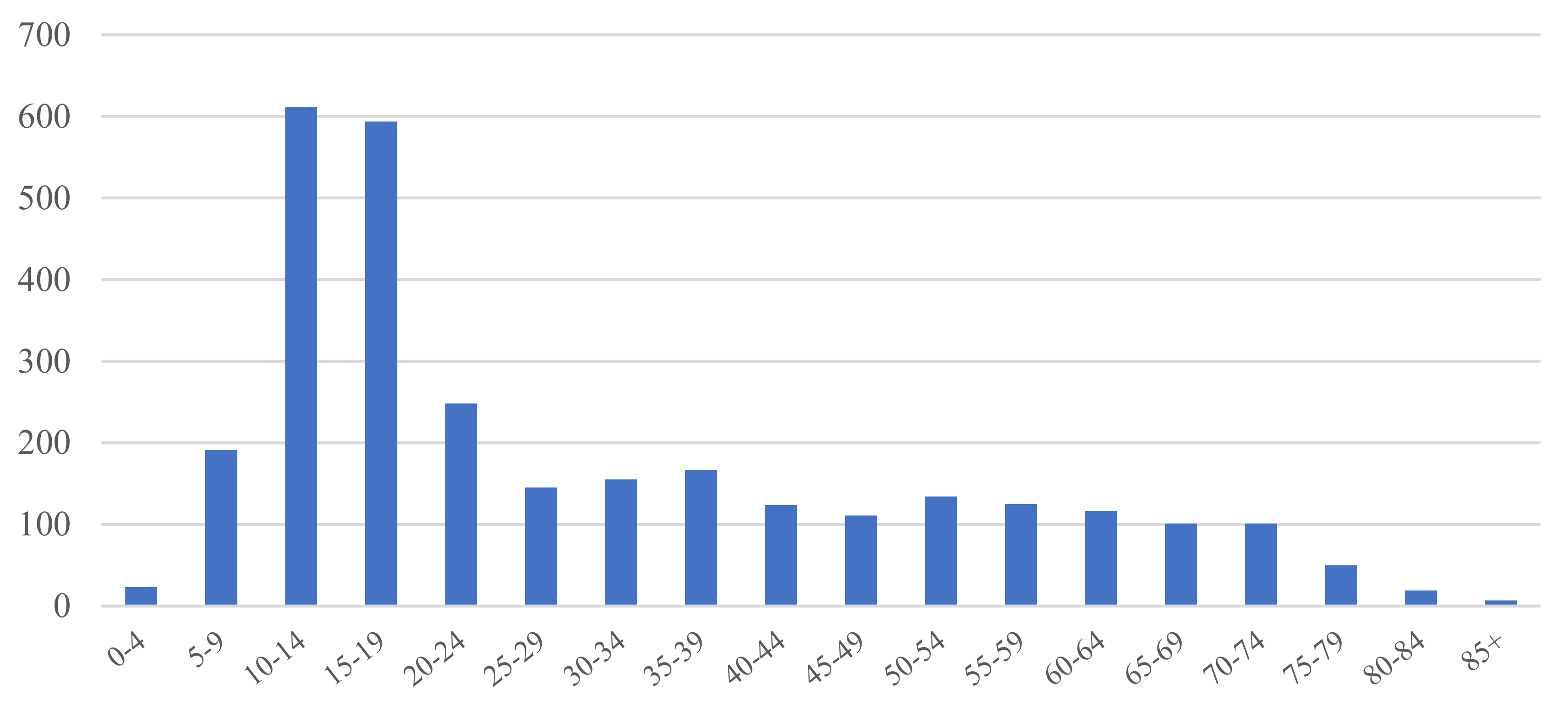
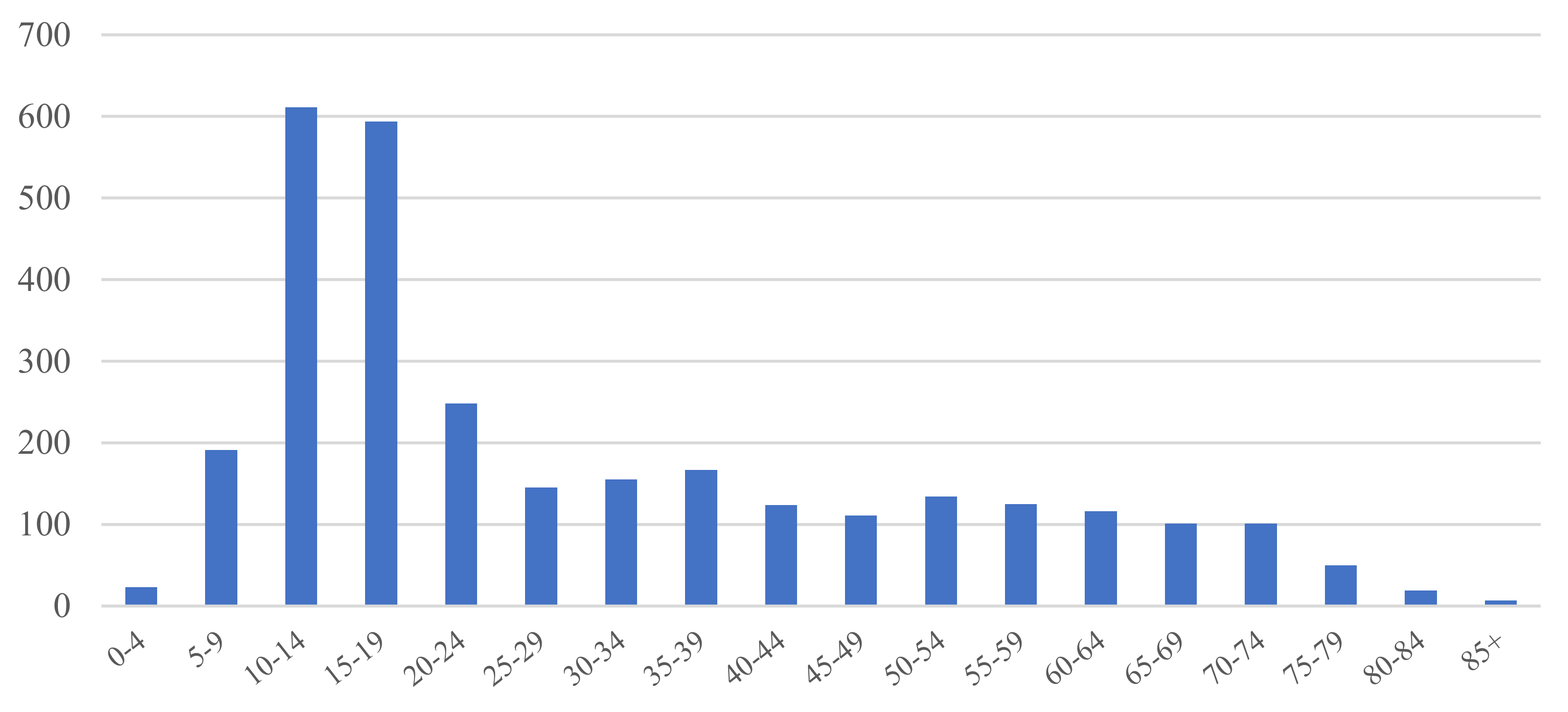
3.1. Osteosarcoma in the KCCR Database
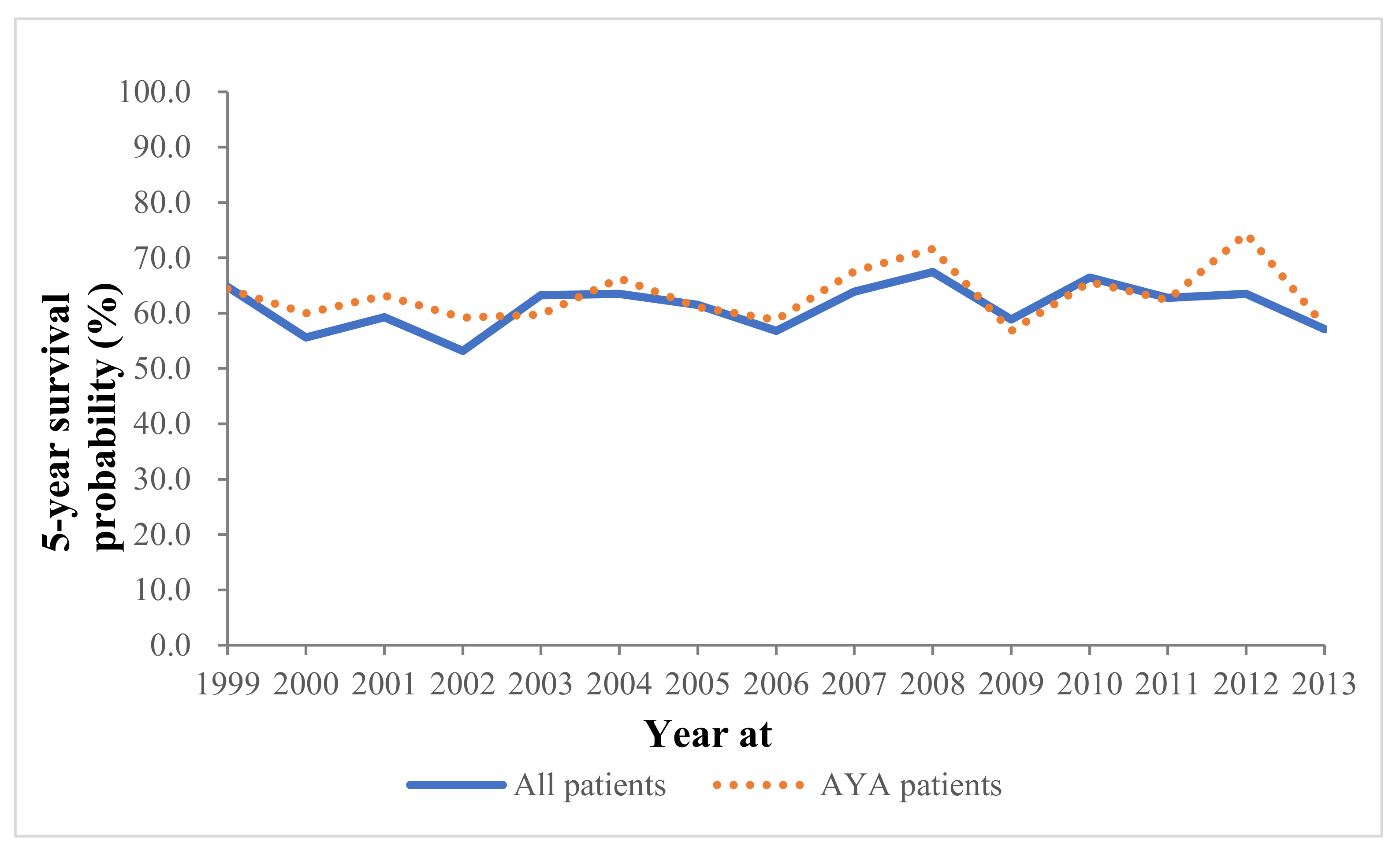
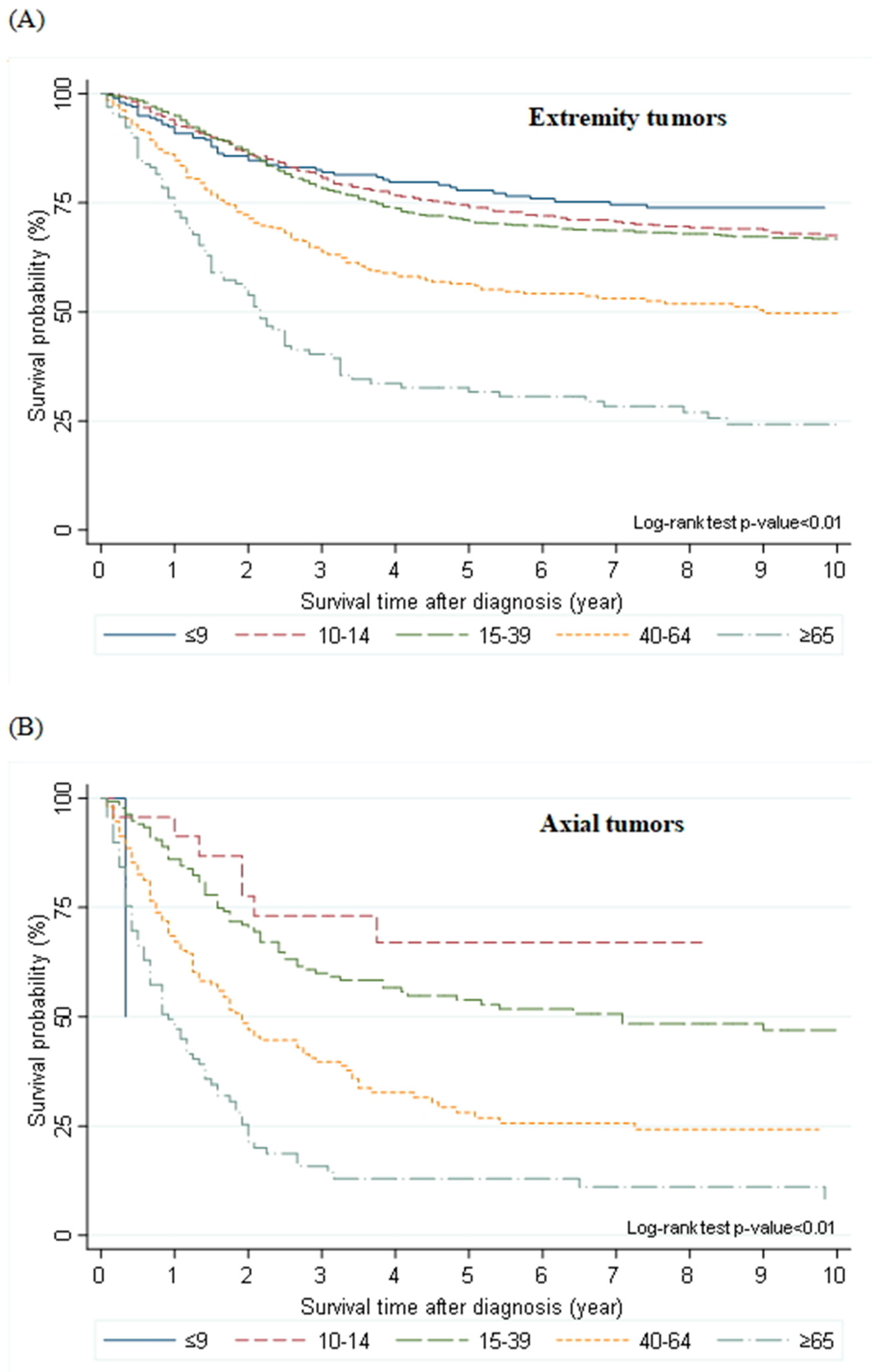
3.2. Comparisons of AYA Patients with Other Age Groups
3.3. Age-Based Subgroups Analysis of AYA Patients
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Longhi, A.; Errani, C.; De Paolis, M.; Mercuri, M.; Bacci, G. Primary Bone Osteosarcoma in the Pediatric Age: State of the Art. Cancer Treat. Rev. 2006, 32, 423–436. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, S.; Bertoni, F.; Mercuri, M.; Picci, P.; Giacomini, S.; Longhi, A.; Bacci, G. Predictive Factors of Disease-Free Survival for Non-Metastatic Osteosarcoma of the Extremity: An Analysis of 300 Patients Treated at the Rizzoli Institute. Ann. Oncol. 2001, 12, 1145–1150. [Google Scholar] [CrossRef] [PubMed]
- Bacci, G.; Longhi, A.; Versari, M.; Mercuri, M.; Briccoli, A.; Picci, P. Prognostic Factors for Osteosarcoma of the Extremity Treated with Neoadjuvant Chemotherapy: 15-Year Experience in 789 Patients Treated at a Single Institution. Cancer 2006, 106, 1154–1161. [Google Scholar] [CrossRef] [PubMed]
- Bacci, G.; Longhi, A.; Bertoni, F.; Bacchini, P.; Ruggeri, P.; Versari, M.; Picci, P. Primary High-Grade Osteosarcoma: Comparison Between Preadolescent and Older Patients. J. Pediatr. Hematol. Oncol. 2005, 27, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Meyers, P.A.; Heller, G.; Healey, J.; Huvos, A.; Lane, J.; Marcove, R.; Applewhite, A.; Vlamis, V.; Rosen, G. Chemotherapy for Nonmetastatic Osteogenic Sarcoma: The Memorial Sloan-Kettering Experience. J. Clin. Oncol. 1992, 10, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Keegan, T.H.; Ries, L.A.; Barr, R.D.; Geiger, A.M.; Dahlke, D.V.; Pollock, B.H.; Bleyer, W.A.; National Cancer Institute Next Steps for Adolescent and Young Adult Oncology Epidemiology Working Group. Comparison of Cancer Survival Trends in the United States of Adolescents and Young Adults with Those in Children and Older Adults. Cancer 2016, 122, 1009–1016. [Google Scholar] [CrossRef] [PubMed]
- Janeway, K.A.; Barkauskas, D.A.; Krailo, M.D.; Meyers, P.A.; Schwartz, C.L.; Ebb, D.H.; Seibel, N.L.; Grier, H.E.; Gorlick, R.; Marina, N. Outcome for Adolescent and Young Adult Patients with Osteosarcoma: A Report from the Children’s Oncology Group. Cancer 2012, 118, 4597–4605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollock, B.H.; Birch, J.M. Registration and Classification of Adolescent and Young Adult Cancer Cases. Pediatr. Blood Cancer 2008, 50, 1090–1093. [Google Scholar] [CrossRef] [PubMed]
- US Department of Health and Human Services; National Institutes of Health; National Cancer Institute; LIVESTRONG Young Adult Alliance. Closing the Gap: Research and Care Imperatives for Adolescents and Young Adults with Cancer; Report of the Adolescent and Young Adult Oncology Progress Review Group; NIH Pub. No. 06–6067; National Institutes of Health: Bethesda, MD, USA, 2006.
- Children’s Oncology Group; SEER Program (National Cancer Institute [U.S.]). Cancer Epidemiology in Older Adolescents and Young Adults 15 to 29 Years of Age, Including SEER Incidence and Survival: 1975–2000; U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute: Bethesda, MD, USA, 2006; p. 205.
- Herzog, C.E. Overview of Sarcomas in the Adolescent and Young Adult Population. J. Pediatr. Hematol. Oncol. 2005, 27, 215–218. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Classification of Diseases for Oncology, 3rd ed.; Fritz, A.P., Percy, C., Jack, A., Shanmugaratnam, K., Sobin, L., Parkin, D.M., Whelan, S., Eds.; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Daejeon: Statistics Korea. 2018. Available online: http://kosis.kr. (accessed on 28 February 2020).
- Young, J.L., Jr.; Roffers, S.; Ries, L.; Fritz, A.; Hurlbut, A.A. SEER Summary Staging Manual −2000: Codes and Coding Instructions; National Cancer Institute, National Institutes of Health: Bethesda, MD, USA, 2001.
- Coccia, P.F. Overview of Adolescent and Young Adult Oncology. J. Oncol. Pract. 2019, 15, 235–237. [Google Scholar] [CrossRef] [PubMed]
- Smeland, S.; Bielack, S.S.; Whelan, J.; Bernstein, M.; Hogendoorn, P.; Krailo, M.D.; Gorlick, R.; Janeway, K.A.; Ingleby, F.C.; Anninga, J.; et al. Survival and prognosis with osteosarcoma: Outcomes in more than 2000 patients in the EURAMOS-1 (European and American Osteosarcoma Study) cohort. Eur. J. Cancer 2019, 109, 36–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukushima, T.; Ogura, K.; Akiyama, T.; Takeshita, K.; Kawai, A. Descriptive Epidemiology and Outcomes of Bone Sarcomas in Adolescent and Young Adult Patients in Japan. BMC Musculoskelet. Disord. 2018, 19, 297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, M.; Lim, J.; Lee, J.A.; Park, B.K.; Jung, K.W.; Won, Y.J.; Park, H.J. Cancer Incidence and Survival Among Adolescents and Young Adults in Korea: An Update for 2016. Cancer Res. Treat. 2021, 53, 32–44. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.A. Osteosarcoma in Korean Children and Adolescents. Korean J. Pediatr. 2015, 58, 123–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casali, P.G.; Bielack, S.; Abecassis, N.; Aro, H.; Bauer, S.; Biagini, R.; Bonvalot, S.; Boukovinas, I.; Bovee, J.V.M.G.; Brennan, B.; et al. Bone sarcomas: ESMO–PaedCan–EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv79–iv95. [Google Scholar] [CrossRef] [PubMed]
- Bacci, G.; Forni, C.; Ferrari, S.; Longhi, A.; Bertoni, F.; Mercuri, M.; Donati, D.; Capanna, R.; Bernini, G.; Briccoli, A.; et al. Neoadjuvant Chemotherapy for Osteosarcoma of the Extremity: Intensification of Preoperative Treatment Does Not Increase the Rate of Good Histologic Response to the Primary Tumor or Improve the Final Outcome. J. Pediatr. Hematol. Oncol. 2003, 25, 845–853. [Google Scholar] [CrossRef] [PubMed]
| Variables | No. | Median Survival Time (Month) | 5-Year Survival (%)÷(CI) | Univariate | Multivariate | |||
|---|---|---|---|---|---|---|---|---|
| HR | p-Value | HR | p-Value | |||||
| Sex | Male Female | 1684 1333 | -÷- | 62 (59–64) | Reference | 0.9198 | Reference | 0.1549 |
| 62 (59–64) | 1.01 (0.89–1.13) | 0.92 (0.81–1.03) | ||||||
| Location | Extremity | 2291 | - | 68 (66–70) | Reference | <0.0001÷ | Reference | <0.0001 |
| Axial | 403 | 25 | 36 (31–41) | 2.72 (2.33–3.17) | 0.91 (1.62–2.24) | |||
| Elsewhere | 323 | 54 | 49 (43–55) | 1.77 (1.48–2.12) | 1.31 (1.09–1.58) | |||
| Extent of disease÷(since 2006) | Localized | 910 | - | 73 (69–76) | Reference | <0.0001 | Reference | <0.0001 |
| Metastasis | 644 | 41 | 44 (40–48) | 2.60 (2.19–3.10) | 2.40 (2.03–2.84) | |||
| Unknown | 413 | - | 71 (66–75) | 0.98 (0.78–1.24) | 1.57 (1.34–1.83) | |||
| Age group | Young children | 214 | - | 78 (71–83) | Reference | <0.0001 | Reference | <0.0001 |
| Pubertal children | 610 | - | 73 (70–77) | 1.24 (0.90–1.70) | 1.22 (0.89–1.67) | |||
| AYA | 1307 | - | 68 (65–71) | 1.47 (1.09–1.98) | 1.35 (1.00–1.82) | |||
| Adults | 608 | 44 | 47 (43–51) | 3.06 (2.64–4.16) | 2.55 (1.87–3.47) | |||
| Elderly | 278 | 20 | 25 (20–31) | 5.88 (4.28–8.08) | 4.69 (3.39–6.49) | |||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number (n = 3022) | % | |
|---|---|---|---|
| Sex | Male | 1689 | 55.89 |
| female | 1333 | 44.11 | |
| Male to female ratio | 1.27 | ||
| Location | Extremity (upper, lower) | 2294 | 75.91 |
| Axial (pelvis, spine) | 404 | 13.37 | |
| Elsewhere | 324 | 10.72 | |
| Age group | Young children (≤9 years) | 214 | 7.08 |
| Pubertal children (10–14 years) | 611 | 20.22 | |
| AYA (15–39 years) | 1309 | 43.32 | |
| Adults (40–64 years) | 610 | 20.19 | |
| Elderly (≥65 years) | 278 | 9.20 | |
| Diagnostic period | 1999–2003 | 764 | 25.28 |
| 2004–2008 | 764 | 25.28 | |
| 2009–2013 | 812 | 26.87 | |
| 2014–2017 | 682 | 22.57 | |
| Extent of disease (n = 1972, since 2006) | Localized | 911 | 46.20 |
| Metastasis | 648 | 32.86 | |
| Unknown | 413 | 20.94 | |
| Treatment | Surgery only | 650 | 21.51 |
| RT only | 26 | 0.86 | |
| Surgery + RT | 44 | 1.46 | |
| Surgery + CTx | 1360 | 45.00 | |
| CTx + RT | 34 | 1.13 | |
| Surgery + CTx + RT | 92 | 3.04 | |
| Unknown | 816 | 27.00 | |
| Variables | Age | ||||||
|---|---|---|---|---|---|---|---|
| Young Children (n = 214) | Pubertal Children (n = 611) | AYA (n = 1309) | Adults (n = 610) | Elderly (n = 278) | p-Value | ||
| Sex | Male | 123 | 327 | 808 | 302 | 129 | <0.0001 |
| Female | 91 | 284 | 501 | 308 | 149 | ||
| Male to female ratio | 1.35 | 1.15 | 1.61 | 0.98 | 0.87 | ||
| Location | Extremity | 198 | 573 | 1051 | 340 | 132 | <0.0001 |
| Axial | 2 | 23 | 138 | 151 | 90 | ||
| Elsewhere | 14 | 15 | 120 | 119 | 56 | ||
| Extent of disease (since 2006) | Localized | 56 | 175 | 396 | 197 | 87 | 0.0010 |
| Metastasis | 35 | 115 | 245 | 161 | 92 | ||
| Unknown | 33 | 103 | 159 | 82 | 36 | ||
| Treatment | Surgery only | 22 | 51 | 261 | 185 | 131 | <0.0001 |
| RT only | 0 | 2 | 9 | 4 | 11 | ||
| Surgery + RT | 0 | 1 | 5 | 16 | 22 | ||
| Surgery + CTx | 109 | 356 | 633 | 214 | 48 | ||
| CTx + RT | 1 | 4 | 11 | 16 | 2 | ||
| Surgery + CTx + RT | 3 | 8 | 37 | 35 | 9 | ||
| Unknown | 79 | 189 | 353 | 140 | 55 | ||
| Variables | No. | Median Survival Time (Month) | 5-Year Survival (%) (CI) | Univariate | Multivariate | |||
|---|---|---|---|---|---|---|---|---|
| HR | p-Value | HR | p-Value | |||||
| Sex | Male Female | 1684 1333 | - - | 62 (59–64) | Reference | 0.9198 | Reference | 0.1549 |
| 62 (59–64) | 1.01 (0.89–1.13) | 0.92 (0.81–1.03) | ||||||
| Location | Extremity | 2291 | - | 68 (66–70) | Reference | <0.0001 | Reference | <0.0001 |
| Axial | 403 | 25 | 36 (31–41) | 2.72 (2.33–3.17) | 0.91 (1.62–2.24) | |||
| Elsewhere | 323 | 54 | 49 (43–55) | 1.77 (1.48–2.12) | 1.31 (1.09–1.58) | |||
| Extent of disease (since 2006) | Localized | 910 | - | 73 (69–76) | Reference | <0.0001 | Reference | <0.0001 |
| Metastasis | 644 | 41 | 44 (40–48) | 2.60 (2.19–3.10) | 2.40 (2.03–2.84) | |||
| Unknown | 413 | - | 71 (66–75) | 0.98 (0.78–1.24) | 1.57 (1.34–1.83) | |||
| Age group | Young children | 214 | - | 78 (71–83) | Reference | <0.0001 | Reference | <0.0001 |
| Pubertal children | 610 | - | 73 (70–77) | 1.24 (0.90–1.70) | 1.22 (0.89–1.67) | |||
| AYA | 1307 | - | 68 (65–71) | 1.47 (1.09–1.98) | 1.35 (1.00–1.82) | |||
| Adults | 608 | 44 | 47 (43–51) | 3.06 (2.64–4.16) | 2.55 (1.87–3.47) | |||
| Elderly | 278 | 20 | 25 (20–31) | 5.88 (4.28–8.08) | 4.69 (3.39–6.49) | |||
| Variables | Age (Years) | ||||||
|---|---|---|---|---|---|---|---|
| 15–19 (n = 594) | 20–24 (n = 248) | 25–29 (n = 145) | 30–34 (n = 155) | 35–39 (n = 167) | p-Value | ||
| Sex | Male | 389 | 172 | 77 | 78 | 92 | <0001 |
| Female | 205 | 76 | 68 | 77 | 75 | ||
| Location | Extremity | 533 | 207 | 105 | 98 | 108 | <0001 |
| Axial | 43 | 25 | 13 | 24 | 33 | ||
| Elsewhere | 18 | 16 | 27 | 33 | 26 | ||
| Extent of disease (since 2006) | Localized | 171 | 71 | 49 | 51 | 54 | 0.7419 |
| Metastasis | 110 | 45 | 30 | 27 | 33 | ||
| Unknown | 75 | 29 | 12 | 25 | 18 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.A.; Lim, J.; Jin, H.Y.; Park, M.; Park, H.J.; Park, J.W.; Kim, J.H.; Kang, H.G.; Won, Y.-J. Osteosarcoma in Adolescents and Young Adults. Cells 2021, 10, 2684. https://doi.org/10.3390/cells10102684
Lee JA, Lim J, Jin HY, Park M, Park HJ, Park JW, Kim JH, Kang HG, Won Y-J. Osteosarcoma in Adolescents and Young Adults. Cells. 2021; 10(10):2684. https://doi.org/10.3390/cells10102684
Chicago/Turabian StyleLee, Jun Ah, Jiwon Lim, Hye Young Jin, Meerim Park, Hyeon Jin Park, Jong Woong Park, June Hyuk Kim, Hyun Guy Kang, and Young-Joo Won. 2021. "Osteosarcoma in Adolescents and Young Adults" Cells 10, no. 10: 2684. https://doi.org/10.3390/cells10102684
APA StyleLee, J. A., Lim, J., Jin, H. Y., Park, M., Park, H. J., Park, J. W., Kim, J. H., Kang, H. G., & Won, Y.-J. (2021). Osteosarcoma in Adolescents and Young Adults. Cells, 10(10), 2684. https://doi.org/10.3390/cells10102684