
Hydrogel- and Nanocomposite-Based Drug-Delivery Strategies in the Treatment of Vaginal Infections



Abstract
1. Introduction
2. Vaginal Infections and Treatment
2.1. Bacterial Vaginosis (BV)
2.2. Vulva Vaginal Candidiasis (VVC)
2.3. Trichomoniasis
2.4. Human Immunodeficiency Viral Infection (HIV)
2.5. Human Papilloma Viral Infection (HPV) (Low Risk and High Risk)
3. Important Considerations on Hydrogel-Based Approaches to Vaginal Drug Delivery
3.1. Injectable Dynamic Hydrogels and Rheological Considerations
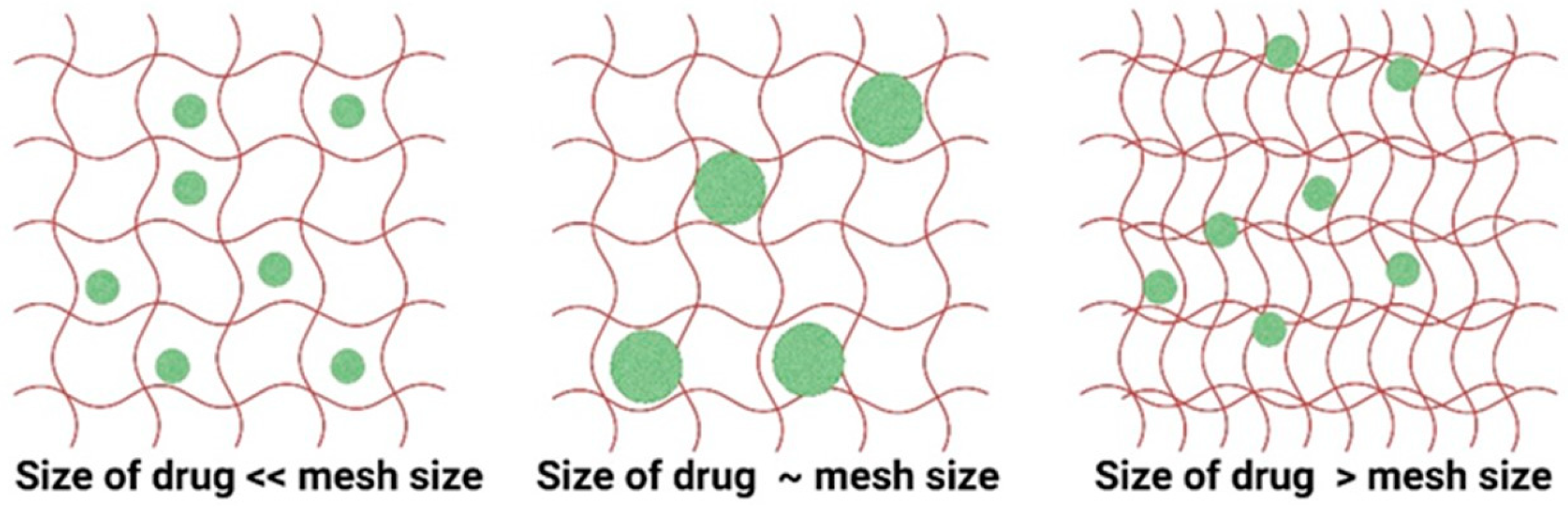
3.2. Mass-Transport Considerations
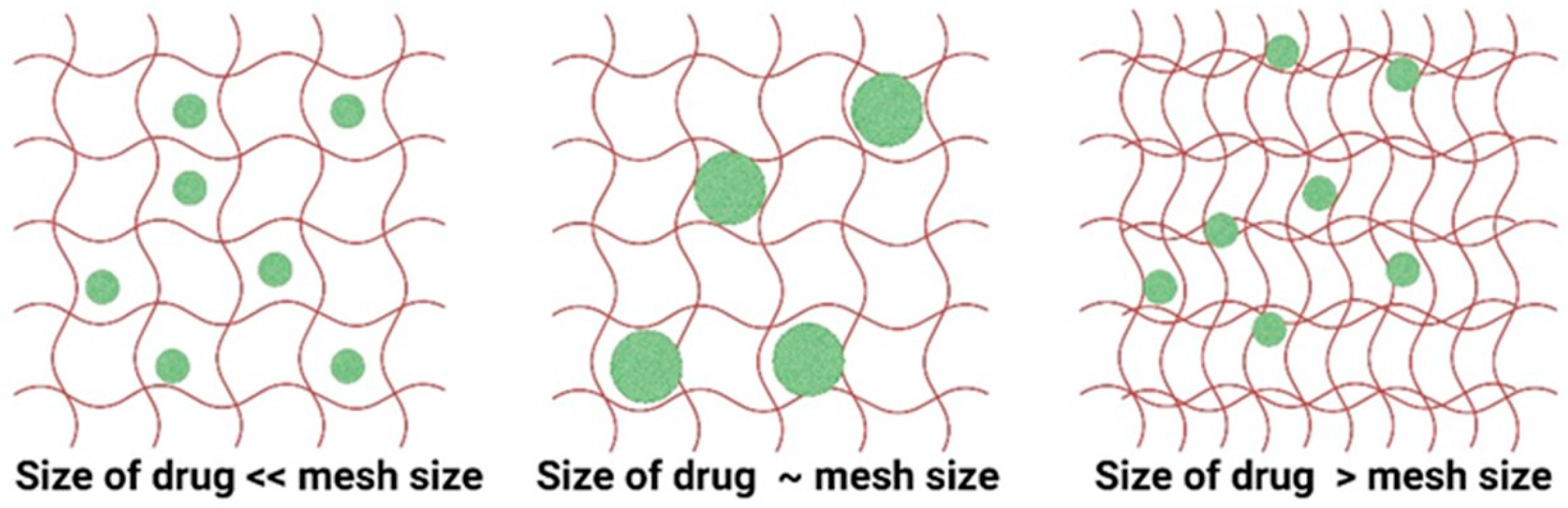
3.3. Swelling Characteristics and Diffusion Parameters
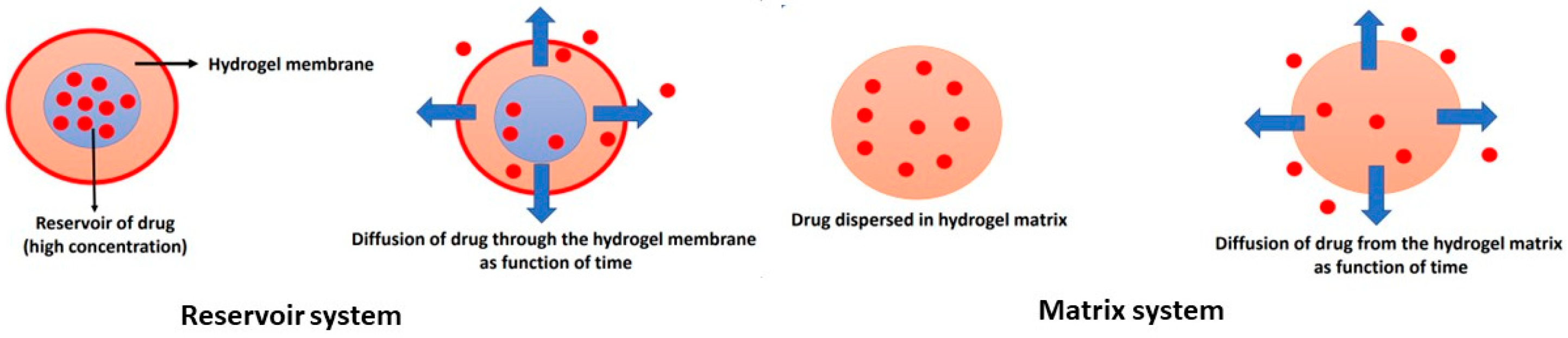
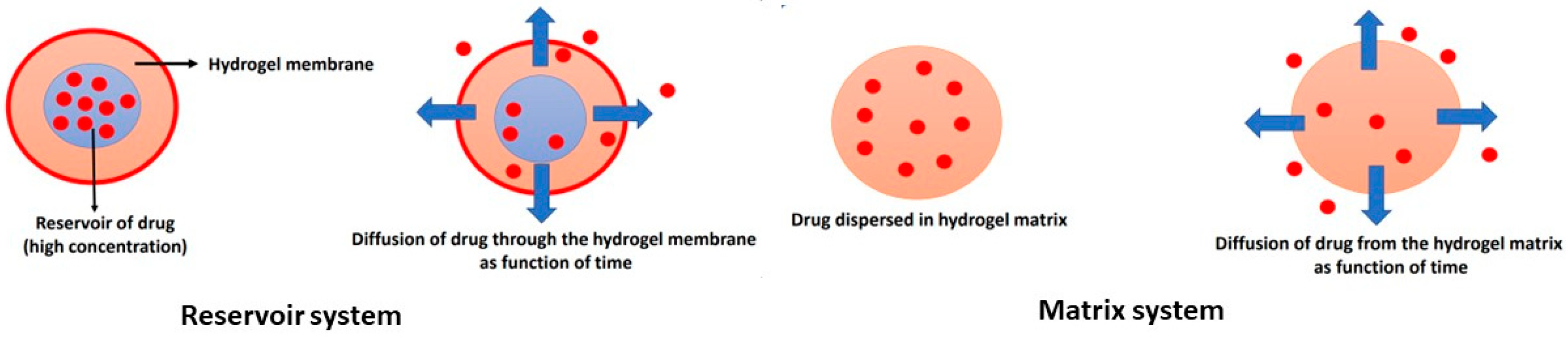
4. Mechanism of Drug Release from Hydrogel Formulations and Mathematical Models
5. Types of Hydrogel Formulations as Vaginal Drug-Delivery Systems
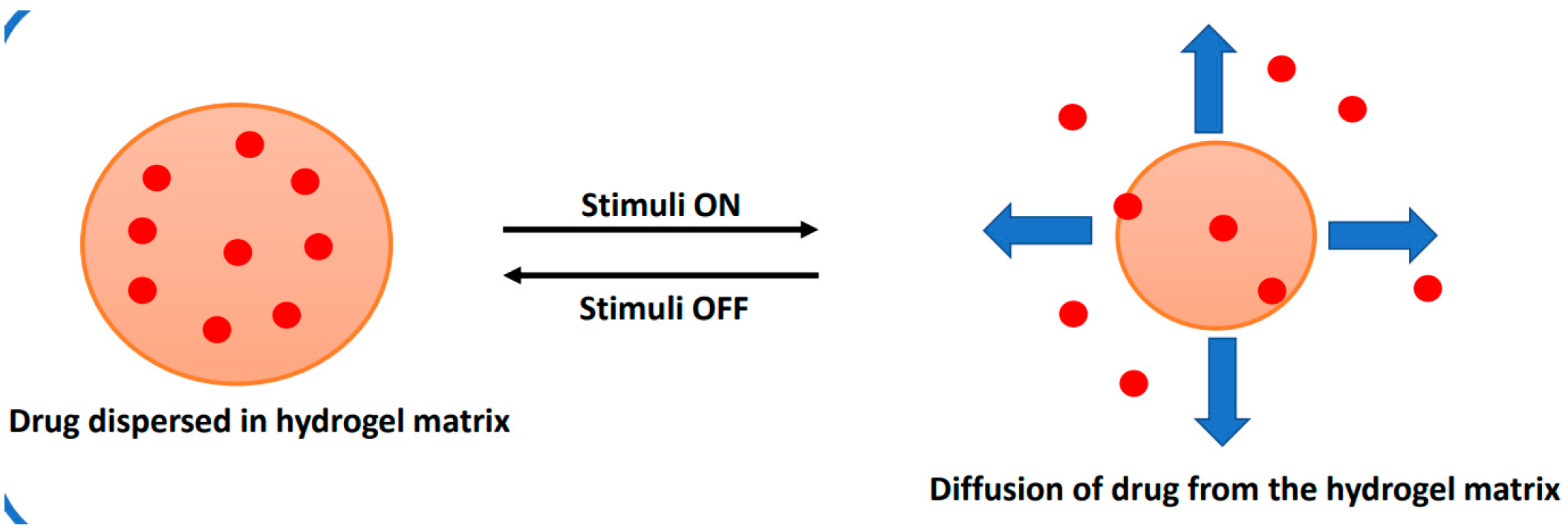
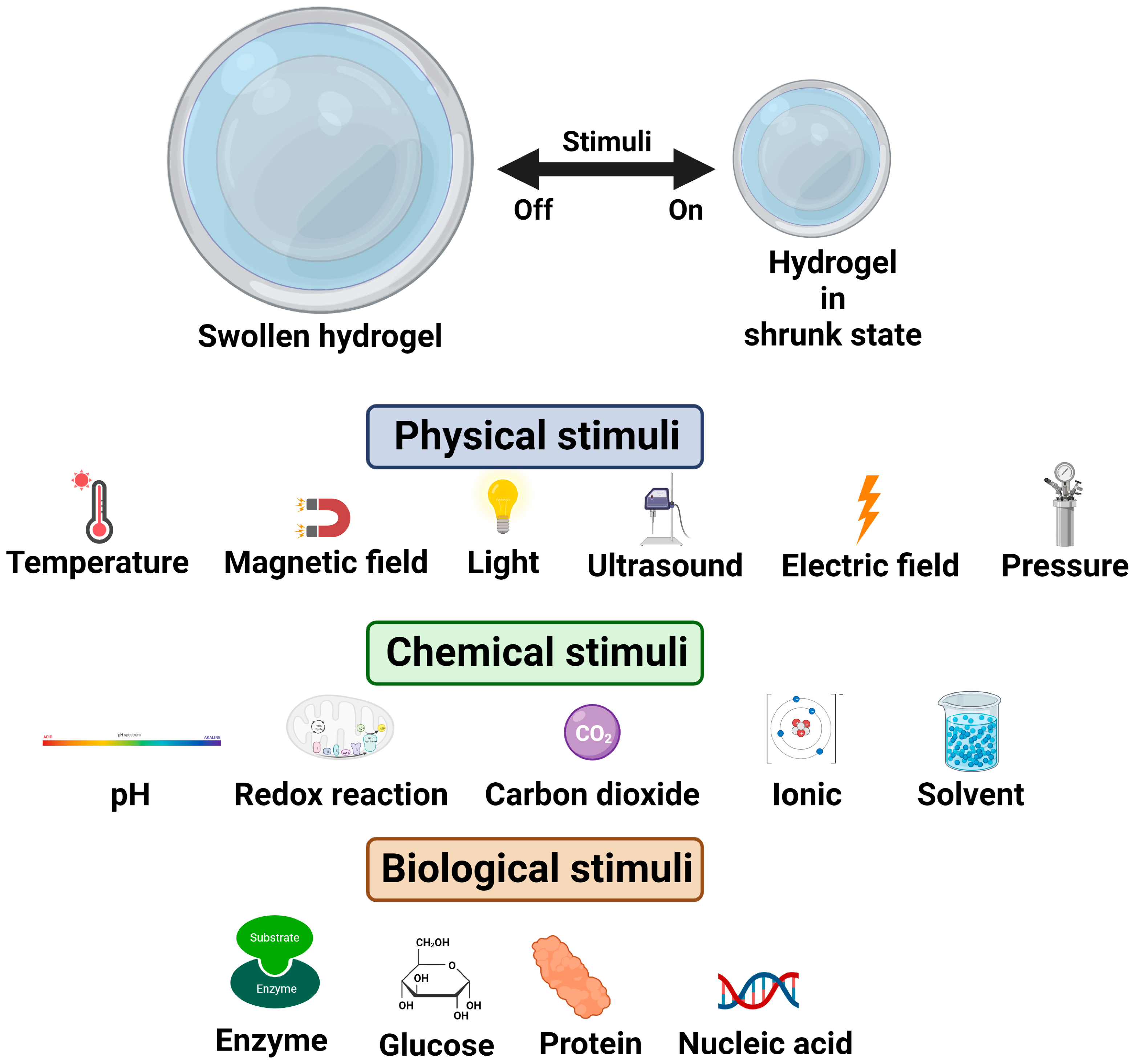
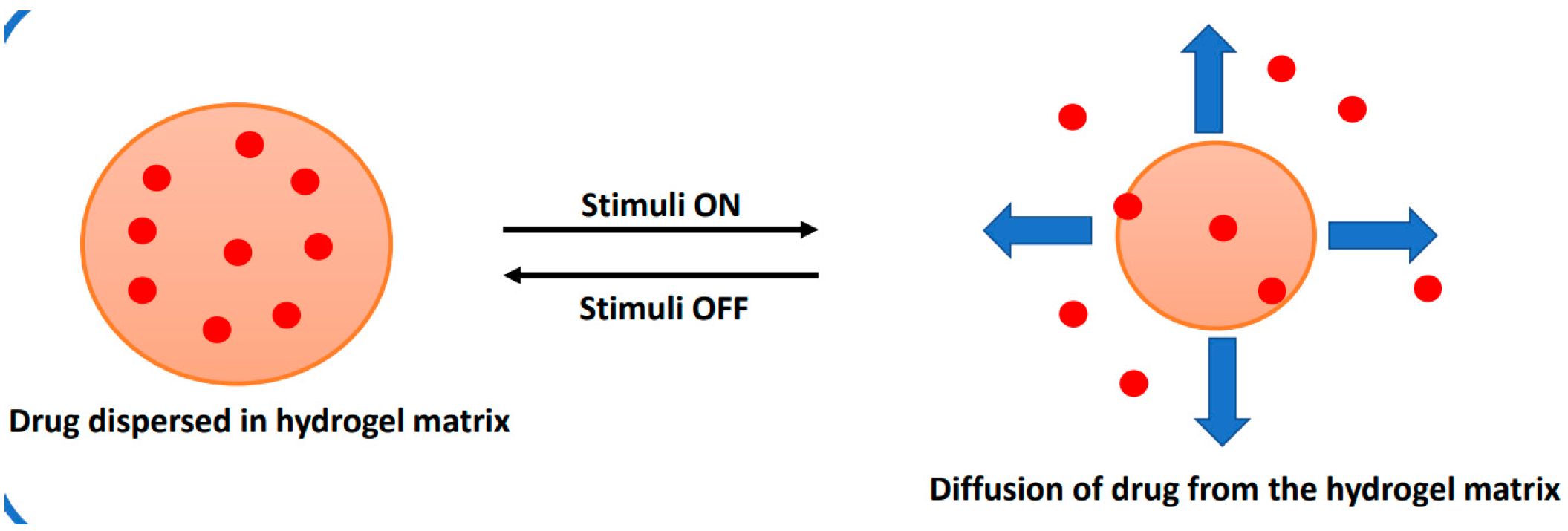
5.1. timuli-Responsive Hydrogels
5.2. Temperature-Responsive Hydrogels (Thermogelling Systems)
5.3. pH-Responsive Hydrogels
5.4. Ion-Responsive Hydrogels
5.5. Multi-Stimuli-Responsive Hydrogels
5.6. Liquid Crystalline Hydrogels
5.7. Astrodimer Gel and Metronidazole in the Treatment of Bacterial Vaginosis
5.8. Nanocarriers: Liposomes, Polymer Nanoparticles, Fibers, and Gels
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Loveless, M.; Myint, O. Vulvovaginitis—Presentation of more common problems in pediatric and adolescent gynecology. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 48, 14–27. [Google Scholar] [CrossRef]
- Gosecka, M.; Gosecki, M. Antimicrobial-polymer-based hydrogels for the intravaginal therapies—Engineering considerations. Pharmaceutics 2021, 13, 1393. [Google Scholar] [CrossRef] [PubMed]
- Cook, M.; Brown, M.B. Polymeric gels for intravaginal drug delivery. J. Control. Release 2018, 270, 145–157. [Google Scholar] [CrossRef] [PubMed]
- Palmeira-de-Oliveira, R.; Palmeira-de-Oliveira, A.; Martinez-de-Oliveira, J. New strategies for local treatment of vaginal infection. Adv. Drug Deli. Rev. 2015, 92, 105–122. [Google Scholar] [CrossRef] [PubMed]
- Chappell, C.A.; Rohan, L.C.; Moncia, B.J.; Wang, I.; Meyn, L.A.; Bunge, K.; Hillier, S.L. The effects of reproductive hormones on the physical properties of cervicovaginal fluid. Am. J. Obstet. Gynecol. 2014, 211, 226e1–226e7. [Google Scholar] [CrossRef]
- Martins dos Santos, A.; Carvalho, S.G.; Sousa Araujo, V.H.; Carvalho, G.C.; Daflon, G.; Chorilli, M. Recent advances in hydrogels as a strategy for drug delivery intended to vaginal infections. Int. J. Pharmaceut. 2020, 590, 119867–119878. [Google Scholar] [CrossRef]
- Arpa, M.D.; Yoltas, A.; Onay Tarlan, E.; Senyuz, C.S.; Siphai, H.; Aydin, A.; Ustundag Okur, N. New therapeutic system based on hydrogels for vaginal candidiasis management: Formulation-characterization and in in vitro evaluation based on vaginal irritation and direct contact test. Pharm. Dev. Technol. 2020, 25, 1238–1248. [Google Scholar] [CrossRef]
- Vazquez, F.; Fernández-Blázquez, A.; García, B. Vaginosis. Vaginal microbiota. Enferm. Infec. Microbiol. Clin. 2019, 37, 592–601. [Google Scholar] [CrossRef]
- Gonçalves, B.; Ferreira, C.; Alves, C.T.; Henriques, M.; Azeredo, J.; Silva, S. Vulvovaginal candidiasis: Epidemiology, microbiology and risk factors. Crit. Rev. Microbiol. 2016, 42, 905–927. [Google Scholar] [CrossRef]
- Workowski, K. Bacterial Vaginosis-2015 STD Treatment Guidelines. 2015. Available online: https://www.cdc.gov/std/tg2015/bv.htm (accessed on 4 January 2024).
- Jones, A. Bacterial vaginosis: A review of treatment, recurrence, and disparities. J. Nurse Pract. 2019, 15, 420–423. [Google Scholar] [CrossRef]
- Denning, D.W.; Kneale, M.; Sobel, J.D.; Rautemaa-Richardson, R. Global burden of recurrent vulvovaginal candidiasis: A systematic review. Lancet Infect. Dis. 2018, 18, e339–e347. [Google Scholar] [CrossRef]
- Chatzivasileiou, P.; Vyzantiadis, T.A. Vaginal yeast colonisation: From a potential harmless condition to clinical implications and management approaches—A literature review. Mycoses 2019, 62, 638–650. [Google Scholar] [CrossRef] [PubMed]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 62, e1–e50. [Google Scholar] [CrossRef] [PubMed]
- Vulvovaginal Candidiasis—2015 STD Treatment Guidelines. 2015. Available online: https://www.cdc.gov/std/tg2015/candidiasis.htm (accessed on 4 January 2024).
- Łaniewski, P.; Herbst-Kralovetz, M. Vagina. Encycl. Reprod. 2018, 2, 353–359. [Google Scholar]
- Kissinger, P. Trichomonas vaginalis: A review of epidemiologic, clinical and treatment issues. BMC Infect. Dis. 2015, 15, 307. [Google Scholar] [CrossRef] [PubMed]
- Workowski, K.A.; Bolan, G.A. Sexually transmitted diseases treatment guidelines, 2015. Mmwr Recomm. Rep. 2015, 64, 137. [Google Scholar]
- Deeks, S.G.; Overbaugh, J.; Phillips, A.; Buchbinder, S. HIV Infection. Nat. Rev. Dis. Prim. 2015, 1, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Fitzmaurice, C.; Dicker, D.; Pain, A.; Hamavid, H.; Moradi-Lakeh, M.; MacIntyre, M.F.; Allen, C.; Hansen, G.; Woodbrook, R.; Wolfe, C.; et al. The global burden of cancer 2013. JAMA Oncol. 2015, 1, 505–527. [Google Scholar] [CrossRef]
- . Torcia, M.G. Interplay among vaginal microbiome, immune response, and sexually transmitted viral infections. Int. J. Mol. Sci. 2019, 20, 266. [Google Scholar] [CrossRef]
- Yarbrough, V.L.; Winkle, S.; Herbst-Kralovetz, M.M. Antimicrobial peptides in the female reproductive tract: A critical component of the mucosal immune barrier with physiological and clinical implications. Hum. Reprod. Update 2015, 21, 353–377. [Google Scholar] [CrossRef]
- World Health Organisation. Human Papillomavirus (HPV) and Cervical Cancer. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/human-papillomavirus-(hpv)-and-cervical-cancer (accessed on 4 January 2024).
- Knuth, K.; Amiji, M.; Robinson, J.R. Hydrogel delivery systems for vaginal and oral applications—Formulation and biological considerations. Adv. Drug Deliv. Rev. 1993, 11, 137–167. [Google Scholar] [CrossRef]
- Badulescu, O.V.; Mocanu, M.; Iancu, C.E.; Constantin, M.M.L.; Badescu, M. Assessment of hematological toxicity in case f oral administration of metronidazole. Rev. Chim. Buchar. 2016, 67, 1137–1139. [Google Scholar]
- Capparelli, E.V.; Bricker-Ford, R.; Rogers, M.J.; McKerrow, J.H.; Reed, S.L. Phase I clinical trial results of auranofin, a novel antiparasitic agent. Antimicrob. Agents Chemother. 2017, 61, 450–455. [Google Scholar] [CrossRef] [PubMed]
- Narayanaswamy, R.; Torchilin, V.P. Hydrogels and their applications in targeted drug delivery. Molecules 2019, 24, 603. [Google Scholar] [CrossRef]
- Alessin, C.; Nyijessy, P. Management of resistant trichomoniasis. Curr. Infect. Dis. Rep. 2019, 21, 567–572. [Google Scholar]
- Long, L.; Hu, C.; Liu, W.; Wu, C.; Lu, L.; Yang, L.; Wang, Y. Injectable multifunctional hyaluronic acid/methylcellulose hydrogels for chronic wounds repairing. Carb. Polym. 2022, 289, 119456–119470. [Google Scholar] [CrossRef]
- Cabane, E.; Zhang, X.; Langowska, K.; Palivan, C.G.; Meier, W. Stimuli-responsive polymers and their applications in nanomedicine. Biointerphases 2012, 7, 9–22. [Google Scholar] [CrossRef]
- Zhang, C.; Li, Y.; Xue, X.; Chu, P.; Liu, C.; Yang, K.; Jiang, Y.; Chen, W.Q.; Zou, G.; Liang, X.J. A smart pH-switchable luminescent hydrogel. Chem. Commun. 2015, 51, 4168–4171. [Google Scholar] [CrossRef]
- Tan, H.-L.; Teow, S.-Y.; Pushpamalar, J. Application of metal nanoparticle-hydrogel composites in tissue regeneration. Bioengineering 2019, 6, 17. [Google Scholar] [CrossRef]
- Mei, L.L.; Chen, J.T.; Yu, S.Q.; Huang, Y.; Xie, Y.C.; Wang, H.; Pan, X.; Wu, C.B. Expansible thermal gelling foam aerosol for vaginal drug delivery. Drug Deliv. 2017, 24, 1325–1337. [Google Scholar] [CrossRef]
- Ghicha, M.V.; Hirjau, M.; Lupuleasa, D.; Dinnu-Piravu, C.E. Flow and thixotropic parameters for rheological characterization of hydrogels. Molecules 2016, 21, 786. [Google Scholar] [CrossRef]
- Von Tomme, S.R.; Storm, G.; Hennink, W.E. In situ gelling hydrogels for pharmaceutical and biomedical applications. Int. J. Pharm. 2008, 355, 1–18. [Google Scholar] [CrossRef]
- Siepmann, J.; Siepmann, F. Mathematical modeling of drug delivery. Int. J. Pharm. 2008, 364, 328–343. [Google Scholar] [CrossRef]
- Li, H.; Luo, R.; Lam, K.Y. Modeling of environmentally sensitive hydrogels for drug delivery: An overview and recent developments. Front. Drug Des. Discov. 2006, 2, 295–331. [Google Scholar]
- Thang, N.H.; Chien, T.B.; Cuong, D.X. Polymer-based hydrogels applied in drug delivery: An overview. Gels 2023, 9, 523. [Google Scholar] [CrossRef]
- Choi, H.G.; Jung, J.H.; Ryu, J.M.; Yoon, S.J.; Oh, Y.K.; Kim, C.K. Development of in situ gelling and mucoadhesive acetaminophen liquid suppository. Int. J. Pharm. 1998, 165, 33–44. [Google Scholar] [CrossRef]
- Siepmann, J.; Gopferich, A. Mathematical modeling of bio erodible, polymeric drug delivery systems. Adv. Drug Del. Rev. 2001, 48, 229–247. [Google Scholar] [CrossRef] [PubMed]
- Modrzejewska, Z.; Nawrotek, K. Drug release from hydrogel matrices. Ecol. Chem. Eng. 2010, 17, 1–10. [Google Scholar]
- Lin, C.; Metters, A.T. Hydrogels in controlled release formulations: Network design and mathematical modeling. Adv. Drug Deliv. Rev. 2006, 58, 1379–1408. [Google Scholar] [CrossRef]
- Arifin, D.Y.; Lee, L.Y.; Wang, C.H. Mathematical modeling and simulation of drug release from microspheres: Implications to drug delivery systems. Adv. Drug Deliv. Rev. 2006, 58, 1247–1325. [Google Scholar] [CrossRef]
- Costa, P.; Sousa Lobo, J.M. Modeling and comparison of dissolution profiles. Eur. J. Pharm. Sci. 2001, 13, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Grassi, M.; Grassi, G. Mathematical modeling and controlled drug delivery: Matrix system. Curr. Drug Deliv. 2005, 2, 97–116. [Google Scholar] [CrossRef]
- Yang, T.-T.; Cheng, Y.-Z.; Qin, M.; Wang, Y.-H.; Yu, H.-L.; Wang, A.-L.; Zhang, W.-F. Thermosensitive chitosan hydrogels containing polymeric microspheres for vaginal drug delivery. Biomed. Res. Int. 2017, 2017, 12. [Google Scholar] [CrossRef] [PubMed]
- Malli, S.; Bories, C.; Pradines, B.; Loiseau, P.M.; Ponchel, G.; Bouchemal, K. In situ forming pluronic® F127/chitosan hydrogel limits metronidazole transmucosal absorption. Eur. J. Pharm. Biopharm. 2017, 112, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Timur, S.S.; Şahin, A.; Aytekin, E.; Öztürk, N.; Polat, K.H.; Tezel, N.; Gürsoy, R.N.; Çalış, S. Design and in vitro evaluation of tenofovir-loaded vaginal gels for the prevention of HIV infections. Pharm. Dev. Technol. 2018, 23, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Nikhar, S.; Bansode, D.A.; Mahadik, K.R. Thermosensitive in situ gel of tinidazole in treatment of bacterial vaginosis: Formulation and evaluation. Int. J. Ayurveda Pharma Res. 2020, 8, 1–12. [Google Scholar]
- Sosa, L.; Calpena, A.C.; Silva-Abreu, M.; Espinoza, L.C.; Rincón, M.; Bozal, N.; Domenech, O.; Rodríguez-Lagunas, M.J.; Clares, B. Thermoreversible gel-loaded amphotericin B for the treatment of dermal and vaginal candidiasis. Pharmaceutics 2019, 11, 312. [Google Scholar] [CrossRef]
- Martín-Illana, A.; Notario-Pérez, F.; Cazorla-Luna, R.; Ruiz-Caro, R.; Veiga, M.D. Smart freeze-dried bigels for the prevention of the sexual transmission of HIV by accelerating the vaginal release of tenofovir during intercourse. Pharmaceutics 2019, 11, 232. [Google Scholar] [CrossRef]
- Kim, S.; Traore, Y.L.; Chen, Y.; Ho, E.A.; Liu, S. Switchable on-demand release of a nanocarrier from a segmented reservoir type intravaginal ring filled with a ph-responsive supramolecular polyurethane hydrogel. ACS Appl. Biol. Mater. 2018, 1, 652–662. [Google Scholar] [CrossRef]
- Osmari, B.F.; Giuliani, L.M.; Reolon, J.B.; Rigo, G.V.; Tasca, T.; Cruz, L. Gellan gum-based hydrogel containing nanocapsules for vaginal indole-3-carbinol delivery in trichomoniasis treatment. Eur. J. Pharm. Sci. 2020, 151, 928–987. [Google Scholar] [CrossRef]
- Cheaburu-Yilmaz, C.N.; Yilmaz, O.; Kose, F.A.; Bibire, N. Chitosan-graft-poly(N-isopropylacrylamide)/PVA cryogels as carriers for mucosal delivery of voriconazole. Polymers 2019, 11, 1432. [Google Scholar] [CrossRef]
- Yenkar, P.; Mayee, R.; Nawale, R.; Chavan, R.; Salunke, T.; Bhoyar, V. Bio responsive in situ gel of clindamycin for vaginal application. Res. Rev. J. Pharm. Pharm. Sci. 2013, 2, 26–32. [Google Scholar]
- Esposito, C.L.; Kirilov, P.; Roullin, V.G. Organogels, promising drug delivery systems: An update of state-of-the-art and recent applications. J. Control. Release 2018, 271, 1–20. [Google Scholar] [CrossRef]
- de Araújo, P.R.; Calixto, G.M.; da Silva, I.C.; de Paula Zago, L.H.; Oshiro, J.A.J.; Pavan, F.R.; Ribeiro, A.O.; Fontana, C.R.; Chorilli, M. Mucoadhesive in situ gelling liquid crystalline precursor system to improve the vaginal administration of drugs. AAPS Pharmscitech 2019, 20, 225. [Google Scholar] [CrossRef]
- Chavoustie, S.E.; Carter, B.A.; Waldbaum, A.S.; Donders, G.G.G.; Peters, K.H.; Schwebke, J.R.; Paull, J.R.A.; Price, C.F.; Bogdanov, A.; Raffai, T.; et al. Castellarnau, A.; McCloud, P.; et al. Two phase 3, double-blind, placebo-controlled studies of the efficacy and safety of Astodrimer 1% Gel for the treatment of bacterial vaginosis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 245, 13–18. [Google Scholar] [CrossRef]
- Abbas, A.M.; Shabaan, S.O. Once daily in-situ forming versus twice-daily conventional metronidazole vaginal gels for treatment of bacterial vaginosis: A randomized controlled trial. J. Genit. Syst. Disord. 2015, 4, 1–5. [Google Scholar] [CrossRef]
- Vanić, Z.; Rukavina, Z.; Manner, S.; Fallarero, A.; Uzelac, L.; Kralj, M.; Klarić, D.A.; Bogdanocv, A.; Raffai, T.; Viropk, D.P.; et al. Azithromycin-liposomes as a novel approach for localized therapy of cervicovaginal bacterial infections. Int. J. Nanomed. 2019, 14, 5957–5976. [Google Scholar] [CrossRef]
- Jøraholmen, M.W.; Basnet, P.; Acharya, G.; Škalko-Basnet, N. PEGylated liposomes for topical vaginal therapy improve delivery of interferon alpha. Eur. J. Pharm. Biopharma. 2017, 113, 132–139. [Google Scholar] [CrossRef]
- Jøraholmen, M.W.; Škalko-Basnet, N.; Acharya, G.; Basnet, P. Resveratrol-loaded liposomes for topical treatment of vaginal inflammation and infections. Eur. J. Pharm. Sci. 2015, 79, 112–121. [Google Scholar] [CrossRef]
- Martinez-perez, B.; Quintanar-Guerrero, D.; Tapia-Tapia, M.; Cisneros-Tamayo, R.; Zambrano-Zaragova, M.L.; Alcal-Alcala, S.; Mendoza-Munoz, N.; Pinon-Segundo, E. Controlled release biodegradable nanoparticles: From preparation to vaginal applications. Eur. J. Pharm. Sci. 2018, 115, 185–195. [Google Scholar] [CrossRef]
- Amaral, A.C.; Saavedra, P.H.V.; Oliveira Souza, A.C.; de Melo, M.T.; Tedesco, A.C.; Morais, P.C.; Soares Felipe, M.S.; Bocca, A.L. Miconazole loaded chitosan-based nanoparticles for local treatment of vulvovaginal candidiasis fungal infections. Colloids Surf. B Biointerfaces 2019, 174, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Calvo, N.L.; Sreekumar, S.; Svetaz, L.A.; Lamas, M.C.; Moerschbacher, B.M.; Leonardi, D. Design and characterization of chitosan nano formulations for the delivery of antifungal agents. Int. J. Mol. Sci. 2019, 20, 3686. [Google Scholar] [CrossRef]
- Abdellatiff, M.M.; Khalil, I.A.; Elakkad, Y.E.; Eliwa, H.A.; Samir, T.M.; Al-Mokaddem, A.K. Formulation and characterization of sertaconazole nitrate mucoadhesive liposomes for vaginal candidiasis. Int. J. Nanomed. 2020, 15, 4079–4090. [Google Scholar] [CrossRef]
- Tugcu-Demiroz, F. Vaginal delivery of benzydamine hydrochloride through liposomes dispersed in mucoadhesive gels. Chem. Pharm. Bull. 2017, 65, 660–667. [Google Scholar] [CrossRef]
- Abilova, G.K.; Kaldybekov, D.B.; Irmukhametova, G.S.; Kazybayeva, D.S.; Iskakbayeva, Z.A.; Kudaibergenov, S.E.; Khutoryanskiy, V.V. Chitosan/poly(2-ethyl-2-oxazoline) films with ciprofloxacin for application in vaginal drug delivery. Materials 2020, 13, 1709. [Google Scholar] [CrossRef]
- Cazorla-Luna, R.; Notario-Perez, F.; Martin-Illana, A.; Bedoya, L.M.; Tamayo, A.; Rubio, J.; Ruiz-Caro, R.; Veiga, M.D. Development and in vitro/ex vivo characterization of vaginal mucoadhesive bilayer film based on ethylcellulose and biopolymers for vaginal sustained release of tenofovir. Biomacromolecules 2020, 21, 2309–2319. [Google Scholar] [CrossRef]
- Anderson, D.J.; Maathe, J.; Pudney, J.; Anderson, D. The structure of the human vaginal stratum corneum and its role in immune defense HHS public access. Am. J. Reprod. Immunol. 2014, 71, 618–623. [Google Scholar] [CrossRef]
- Kenechukwu, F.C.; Attama, A.A.; Ibezim, E.C.; Nnamani, P.O.; Umeyor, C.E.; Uronnachi, E.M.; Gugu, T.H.; Momoh, M.A.; Ofokansi, K.C.; Akpa, P.A. Surface-modified mucoadhesive microgels as controlled release system for miconazole nitrate to improve localized treatment of vulvovaginal candidiasis. Eur. J. Pharm. Sci. 2018, 111, 358–375. [Google Scholar] [CrossRef]
- Khattab, A.; Ismail, S. Formulation and evaluation of oxiconazole-nitrate mucoadhesive nanoemulsion based gel for treatment of fungal vaginal infection. Int. J. Pharm. Pharm. Sci. 2016, 8, 33–40. [Google Scholar]
- Pandey, M.; Choudhury, H.; Abdul-Aziz, A.; Bhattamisra, S.K.; Gorain, B.; Carine, T.; Toong, T.W.; Yi, N.J.; Win Yi, L. Promising drug delivery approaches to treat microbial infections in the vagina: A recent update. Polymers 2021, 12, 26–50. [Google Scholar]
- Melo, C.M.; Cardoso, J.F.; Perassoli, F.B.; de Oliveira Neto, A.S.; Pinto, L.M.; de Freitas Marques, M.B.; de Nova Mussel, W.; Magalhaes, J.T.; de Lima Moura, S.A.; de Freitas Araujo, M.G.; et al. Amphotericin b-loaded eudragit RL100 nanocapsules coated with hyaluronic acid for the treatment of vulvovaginal candidiasis. Carbohydr. Polym. 2020, 230, 115608. [Google Scholar] [CrossRef] [PubMed]
- Jeckson, T.A.; Neo, Y.P.; Sisinthy, S.P.; Gorain, B. Delivery of therapeutics from layer-by-layer electrospun nanofiber matrix for wound healing: An update. J. Pharm. Sci. 2020, 110, 635–653. [Google Scholar] [CrossRef] [PubMed]
- Nematpour, N.; Moradipour, P.; Zangeneh, M.M.; Arkan, E.; Abdoli, M.; Behbood, L. The application of nanomaterial science in the formulation of a novel antibiotic: Assessment of the antifungal properties of mucoadhesive clotrimazole loaded nanofiber versus vaginal films. Mater. Sci. Eng. C. 2020, 110, 110635. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formulation | Polymer | Gelation Temperature (°C) | Infection |
|---|---|---|---|
| Foam aerosol (thermal gelling) with silver nanoparticles | Pluronics, Carbopol | 35.7 | Vaginitis |
| In situ thermal gel with benzydamine hydrochloride | Poloxamer, chitosan | 31.8 | Vaginitis |
| Vaginal gel with clotrimazole | Pluronics F127, F68 and polycarbophil | 31 | Candidiasis |
| Thermoreversible gel with amphotericin | Pluronic P407 | 32 | Candidiasis |
| Vaginal suppository with miconazole nitrate | Pluronics F188, P407 and HPMC | Candidiasis | |
| Nanocomposite gel with auranofin | Chitosan, Pluronic F127, P407 | 32 °C | Trichomoniasis |
| Vaginal gel with tenofovir | Pluronics F127, Chitosan | 26 °C | HIV |
| Blended hydrogel with curcumin | Pluronic P407, Chitosan, HPMC | 32.8 | Vaginal mucosal inflammation, HPV |
| Formulation | Polymer | pH | Infection |
|---|---|---|---|
| Bigels with tenofovir | Pectin | 4–12 | HIV |
| Vaginal film with tenofovir | Chitosan citrate, Eudragit S100 | 2–3 | HIV |
| Intravaginal ring (hydrogel) with siRNA | PEG, polyurethane | 4–7 | HIV |
| Intravaginal ring (with polymer membrane) with SiRNA | PEG, phenyl isocyanate, 1,4-bis(2-hyroxy ethyl piperazine) | 4.5–7.0 | HIV |
| Synthetic mucin like | Phenylboronic acid, salicylhydroxamic acid, crosslinked polymers | 4.8–7.0 | HIV |
| Formulation | Polymer | Drug | Infection |
|---|---|---|---|
| Vaginal gel | Gellan gum | Clindamycin | BV |
| Vaginal gel/solution | Gellan gum, HPMC | Clindamycin | Vaginitis |
| Vaginal gel | Gellan gum | Secnidazole | Trichomoniasis |
| Formulation | Polymer | Stimuli | Infection |
|---|---|---|---|
| Gel with clindamycin | Gellan gum, pluronics | Temperature and ions | BV |
| Hydrogel with oxytetracycline | Sodium alginate, NIPAM | Temperature and pH | BV |
| In situ gel with polymer flakes and ketoconazole | Pluronic Pf127, chitosan, gellan gum | Temperature and ions | VVD |
| In situ gel with amphotericin | Copolymers | Temperature and pH | VVD |
| In situ gel with voriconazole | Grafted copolymers of NIPAM and PVA | Temperature and pH | BV and VVD |
| Organogel (palm oil-based) with maraviroc | Hyaluronic acid | Temperature and enzyme | HIV |
| Vaginal osmotic pump with antiretroviral drugs | Carbopol | Osmotic pressure and pH | HIV |
| Liposome gel with acrtigenin | Pluronics P407, PF188 | Temperature and pH | VVD and HIV |
| Formulation | Composition | Drug | Disease |
|---|---|---|---|
| Liquid-crystal precursor | Carbopol 974P, polycarbophil, water | Syngonanthus nitens | VVD with Candida krusei |
| Liquid-crystal precursor | Carbopol 974P, polycarbophil, water | Syngonanthus nitens | VVD with Candida albicans |
| Liquid-crystal gel based on phytantriol | Phytantriol, ethanol, water | Sinomenine hydrochloride | Cervical cancer |
| Liquid-crystal gel | Pluronic P407 | Hypericin | BV, cervical and vaginal cancers |
| Formulation Type | Polymer | Drug | Infection |
|---|---|---|---|
| Conventional liposomes | Phosphatidylcholine and hydrogenated phosphatidylcholine | azithromycin | E. coli related vaginal infection |
| Liposomes | Chitosan and phosphatidylcholine | Resveratrol | Vaginal inflammation and infection |
| Liposomes | Phosphatidylcholine, monoacyl phosphatidylcholine, and propylene glycol | azithromycin | E. coli related vaginal infections |
| Liposomes (mucus penetrating) | Cholesterol, phosphatidylcholine, methoxy poly(ethylene glycol)-modified lipids | azithromycin | Vaginal candidiasis |
| Nanoparticles | Poly(lactic-co-glycolic acid) | Clotrimazole | Candida albicans |
| Nanoparticle | Chitosan | Miconazole | Vaginal candidiasis |
| Nanoparticle | Eudragit RL100 and hyaluronic acid | Ampicillin | Vaginal candidiasis |
| Nanocapsules | Chitosan and lecithin | Tioconazole, Econazole | Vaginal candidiasis |
| Mucoadhesive Liposomal gel | Phosphatidylcholine, cholesterol, pectin, and dimethyldidodecyl ammonium bromide | Sertaconazole | Vaginal candidiasis |
| Lipogel | Carbopol, hydroxy propyl methyl cellulose | Benzydamide hydrochloride | Vaginitis |
| Microgel | Polycarbophil | Miconazole nitrate | Vaginal candidiasis |
| Nanofibers | Polyvinyl pyrrolidone | Metronidazole | Vaginal candidiasis |
| Nanofibers | Dextran, sodium alginate, PVA | Clotrimazole | Vaginal candidiasis |
| Film/membrane | Chitosan and poly(2-ethyl-2-oxazoline) | Ciprofloxacin | Bacterial vaginosis |
| Film/membrane | Alginate, chitosan | Metronidazole | Bacterial vaginosis |
| Film/membrane | Modified gellan gum | Metronidazole | Bacterial vaginosis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlAnsari, R.; Hasan, B.; Deen, G.R.; Torsten, U. Hydrogel- and Nanocomposite-Based Drug-Delivery Strategies in the Treatment of Vaginal Infections. Polymers 2024, 16, 775. https://doi.org/10.3390/polym16060775
AlAnsari R, Hasan B, Deen GR, Torsten U. Hydrogel- and Nanocomposite-Based Drug-Delivery Strategies in the Treatment of Vaginal Infections. Polymers. 2024; 16(6):775. https://doi.org/10.3390/polym16060775
Chicago/Turabian StyleAlAnsari, Renad, Bushra Hasan, G. Roshan Deen, and Uwe Torsten. 2024. "Hydrogel- and Nanocomposite-Based Drug-Delivery Strategies in the Treatment of Vaginal Infections" Polymers 16, no. 6: 775. https://doi.org/10.3390/polym16060775
APA StyleAlAnsari, R., Hasan, B., Deen, G. R., & Torsten, U. (2024). Hydrogel- and Nanocomposite-Based Drug-Delivery Strategies in the Treatment of Vaginal Infections. Polymers, 16(6), 775. https://doi.org/10.3390/polym16060775