
Strength and Surface Characteristics of 3D-Printed Resin Crowns for the Primary Molars

 , , ,
, , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
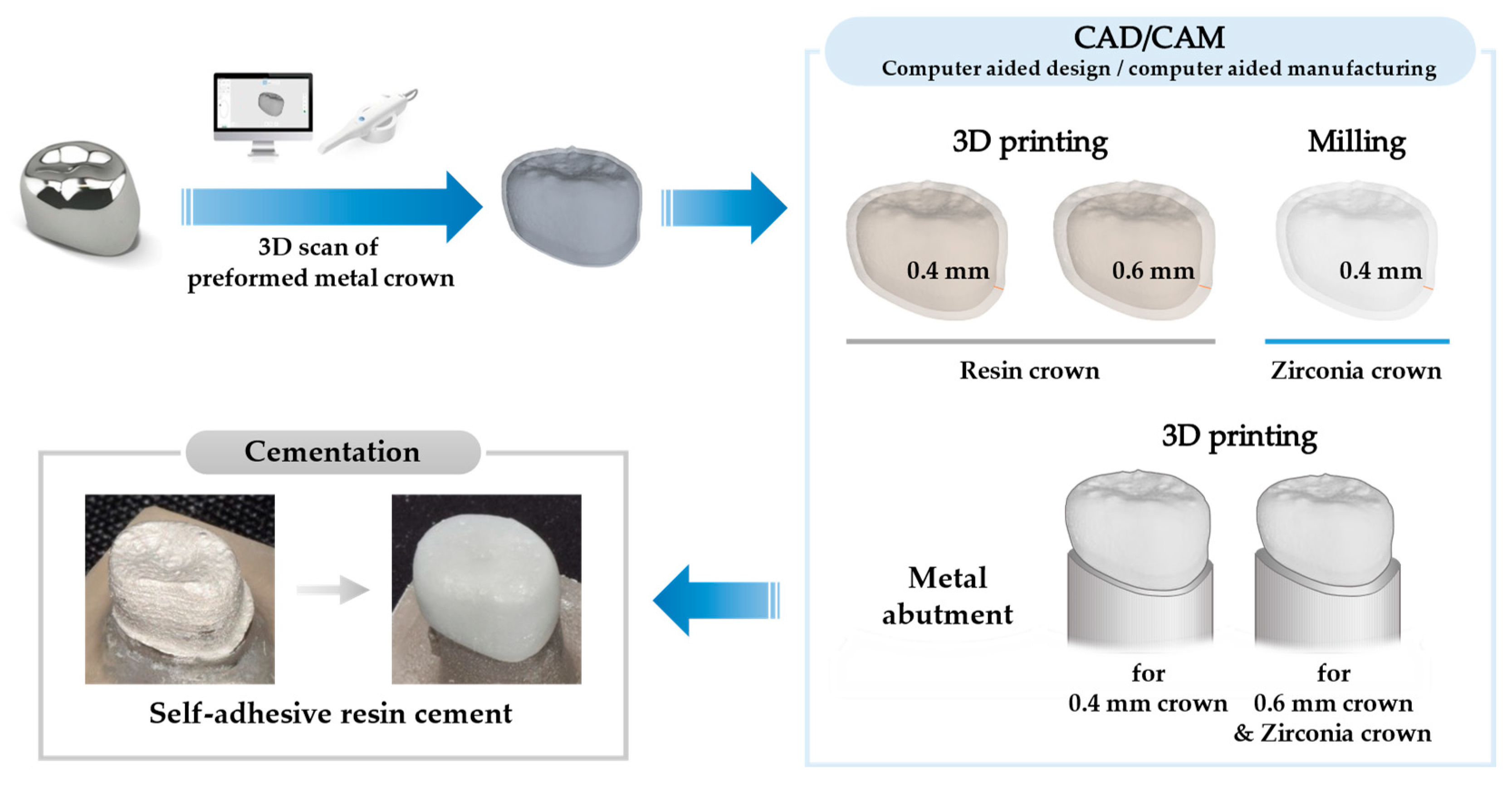
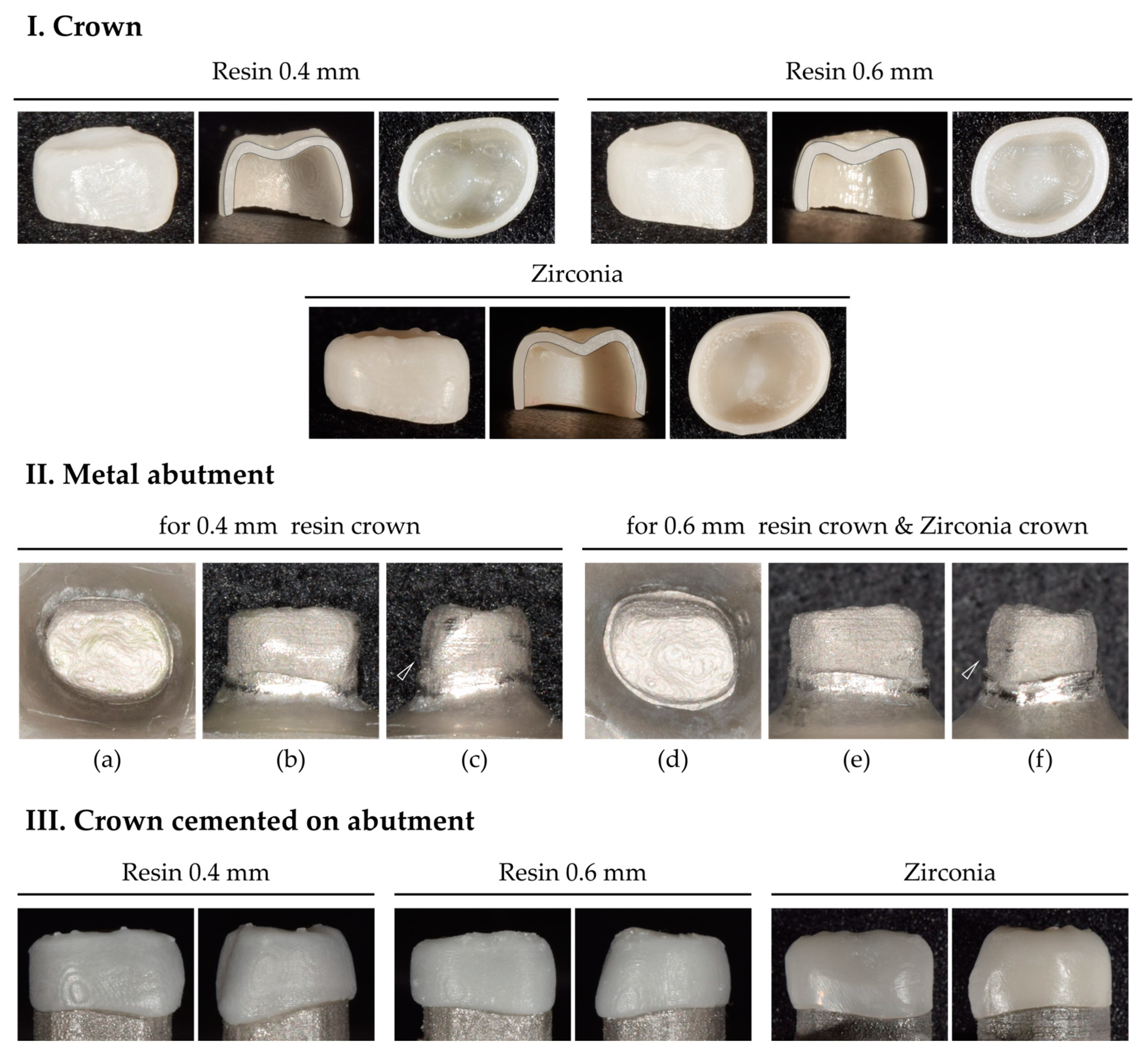
2.1. Fabrication of the Crown and Abutment
2.2. Experimental and Control Groups
2.3. Crown Cementation
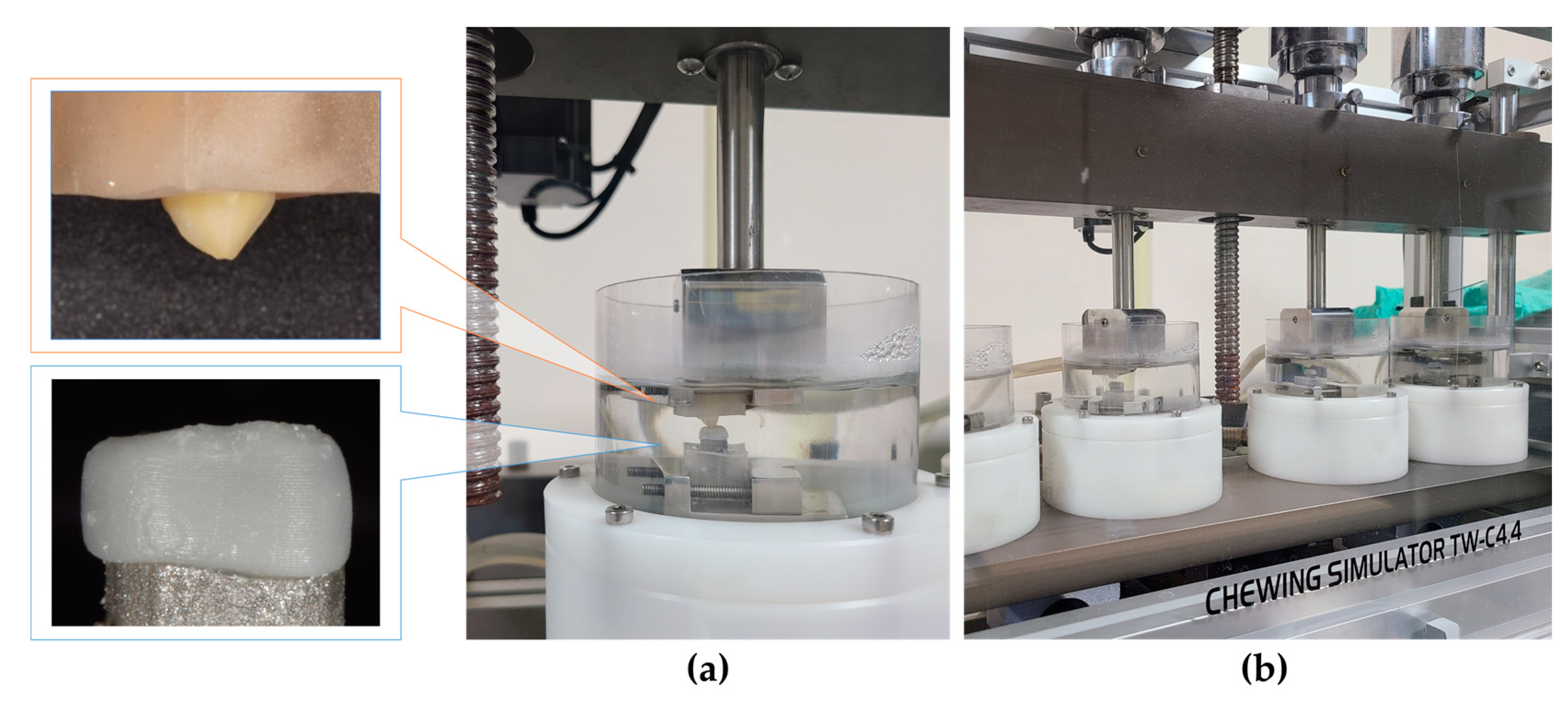
2.4. Fatigue Simulation
2.4.1. Preparation of the Antagonist
2.4.2. Chewing Simulation and Thermocycling
2.5. Field Emission Scanning Electron Microscope (FE-SEM) Analysis
2.6. Compression Strength and Fracture Pattern Analysis
2.7. Statistical Analysis
3. Results
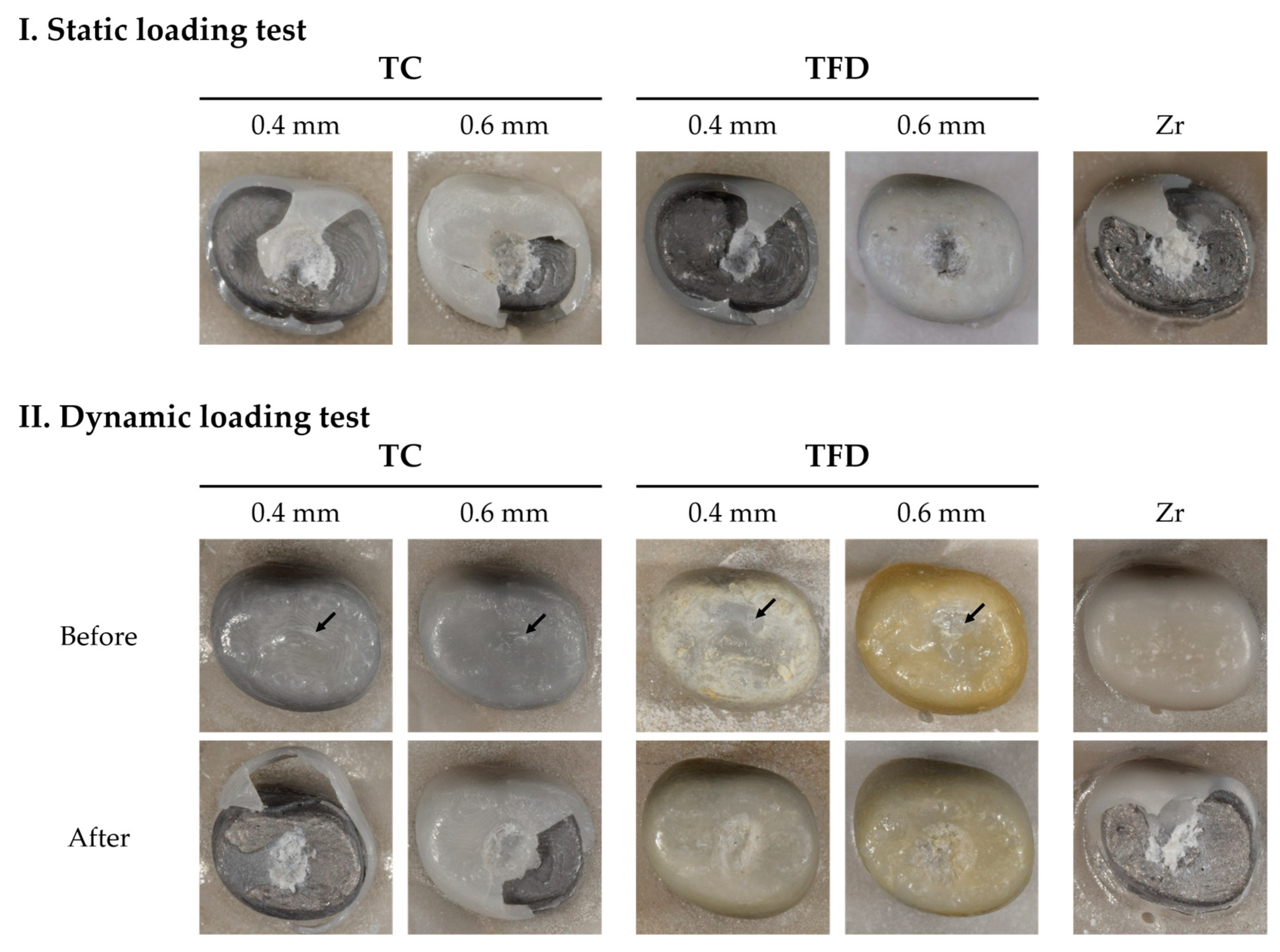
3.1. Strength
3.1.1. Static Strength
3.1.2. Dynamic Strength
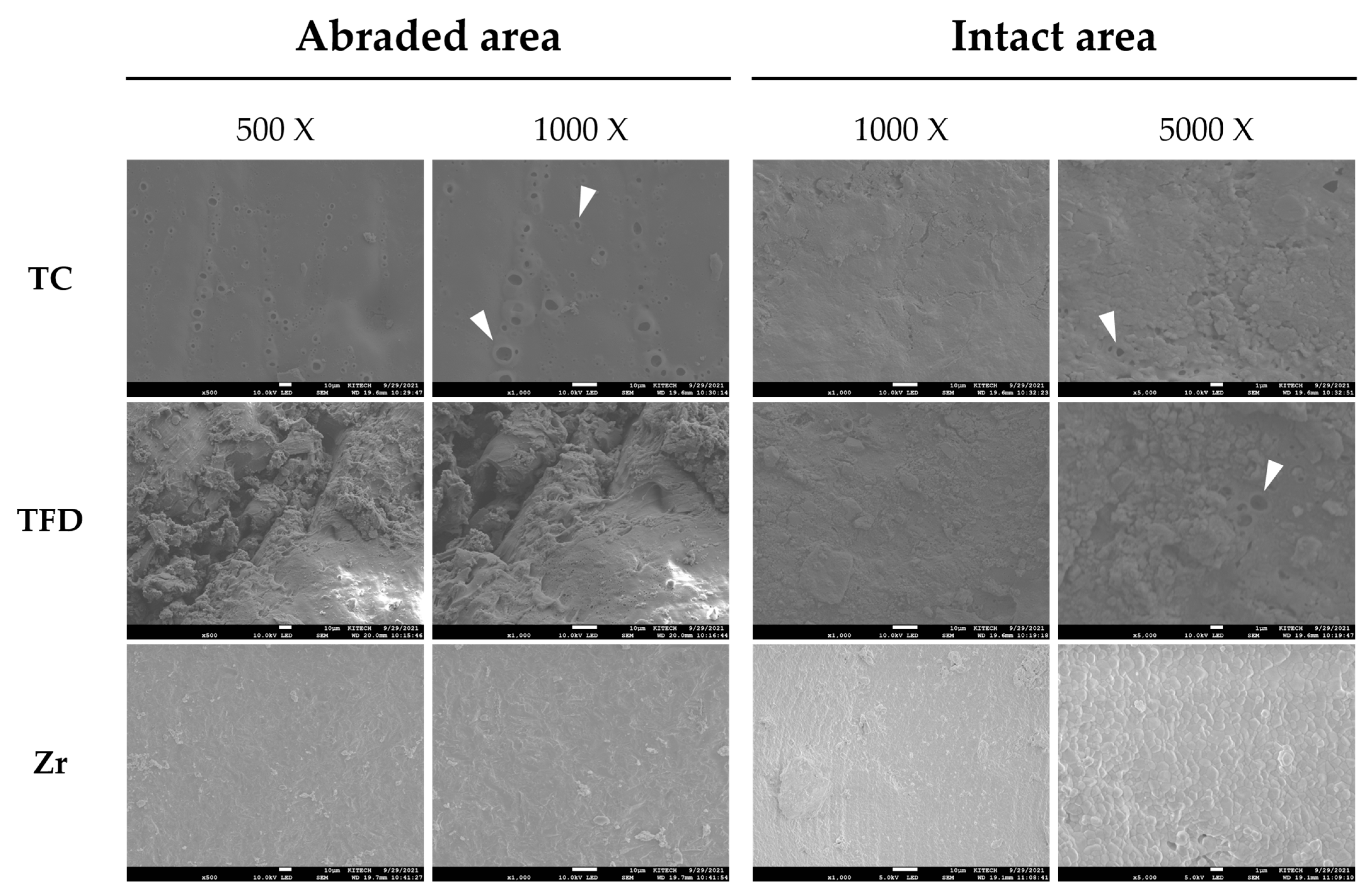
3.2. Surface Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Petersen, P.E. The world oral health report 2003: Continuous improvement of oral health in the 21st century—The approach of the who global oral health programme. Community Dent. Oral Epidemiol. 2003, 31 (Suppl. S1), 3–23. [Google Scholar] [CrossRef] [PubMed]
- Innes, N.P.; Ricketts, D.; Chong, L.Y.; Keightley, A.J.; Lamont, T.; Santamaria, R.M. Preformed crowns for decayed primary molar teeth. Cochrane Database Syst. Rev. 2015, 2015, Cd005512. [Google Scholar] [CrossRef] [PubMed]
- Seale, N.S.; Randall, R. The use of stainless steel crowns: A systematic literature review. Pediatr. Dent. 2015, 37, 145–160. [Google Scholar] [PubMed]
- Randall, R.C. Preformed metal crowns for primary and permanent molar teeth: Review of the literature. Pediatr. Dent. 2002, 24, 489–500. [Google Scholar]
- Zimmerman, J.A.; Feigal, R.J.; Till, M.J.; Hodges, J.S. Parental attitudes on restorative materials as factors influencing current use in pediatric dentistry. Pediatr. Dent. 2009, 31, 63–70. [Google Scholar]
- Scheffel, D.L.S.; Jeremias, F.; Fragelli, C.M.B.; Dos Santos-Pinto, L.A.M.; Hebling, J.; de Oliveira, O.B., Jr. Esthetic dental anomalies as motive for bullying in schoolchildren. Eur. J. Dent. 2014, 8, 124–128. [Google Scholar] [CrossRef]
- Aiem, E.; Smaïl-Faugeron, V.; Muller-Bolla, M. Aesthetic preformed pediatric crowns: Systematic review. Int. J. Paediatr. Dent. 2017, 27, 273–282. [Google Scholar] [CrossRef]
- Ajayakumar, L.P.; Chowdhary, N.; Reddy, V.R.; Chowdhary, R. Use of restorative full crowns made with zirconia in children: A systematic review. Int. J. Clin. Pediatr. Dent. 2020, 13, 551–558. [Google Scholar] [CrossRef]
- Kang, H.Y.; Lee, H.; Chae, Y.K.; Hong, S.J.; Jeong, Y.Y.; Lee, K.E.; Kim, M.S.; Lee, H.S.; Choi, S.C.; Nam, O.H. Feasibility of 3-dimensional visual guides for preparing pediatric zirconia crowns: An in vitro study. Int. J. Environ. Res. Public Health 2020, 17, 5732. [Google Scholar] [CrossRef]
- Clark, L.; Wells, M.H.; Harris, E.F.; Lou, J. Comparison of amount of primary tooth reduction required for anterior and posterior zirconia and stainless steel crowns. Pediatr. Dent. 2016, 38, 42–46. [Google Scholar]
- Tahayeri, A.; Morgan, M.; Fugolin, A.P.; Bompolaki, D.; Athirasala, A.; Pfeifer, C.S.; Ferracane, J.L.; Bertassoni, L.E. 3D printed versus conventionally cured provisional crown and bridge dental materials. Dent. Mater. 2018, 34, 192–200. [Google Scholar] [CrossRef]
- Jang, G.; Kim, S.K.; Heo, S.J.; Koak, J.Y. Fit analysis of stereolithography-manufactured three-unit resin prosthesis with different 3D-printing build orientations and layer thicknesses. J. Prosthet. Dent. 2023, S0022-3913, 00703–00704. [Google Scholar] [CrossRef]
- Shim, J.S.; Kim, J.E.; Jeong, S.H.; Choi, Y.J.; Ryu, J.J. Printing accuracy, mechanical properties, surface characteristics, and microbial adhesion of 3D-printed resins with various printing orientations. J. Prosthet. Dent. 2020, 124, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Shaheen, S.R.; Sridevi, E.; Sai Sankar, A.J.; SKrishna, V.S.; Sridhar, M.; Sankar, K.S. Contemporary era of Three-dimensional printing in pediatric dentistry: An overview. J. Oral Res. Rev. 2023, 15, 72–79. [Google Scholar] [CrossRef]
- Dimova-Gabrovska, M.; Dimitrova, D.; Yordanov, B.; Yankova, M.; Peev, T. Advantages and disadvantages of pediatric crown prosthetic treatment. J. IMAB 2019, 25, 2695–2700. [Google Scholar] [CrossRef]
- Jin, S.; Choi, J.W.; Jeong, C.M.; Huh, J.B.; Lee, S.H.; Lee, H.; Yun, M.J. Evaluating the wear of resin teeth by different opposing restorative materials. Materials 2019, 12, 3684–3694. [Google Scholar] [CrossRef]
- Corbani, K.; Hardan, L.; Skienhe, H.; Özcan, M.; Alharbi, N.; Salameh, Z. Effect of material thickness on the fracture resistance and failure pattern of 3d-printed composite crowns. Int. J. Comput. Dent. 2020, 23, 225–233. [Google Scholar]
- Kadokawa, A.; Suzuki, S.; Tanaka, T. Wear evaluation of porcelain opposing gold, composite resin, and enamel. J. Prosthet. Dent. 2006, 96, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Özcan, M.; Jonasch, M. Effect of cyclic fatigue tests on aging and their translational implications for survival of all-ceramic tooth-borne single crowns and fixed dental prostheses. J. Prosthodont. 2018, 27, 364–375. [Google Scholar] [CrossRef] [PubMed]
- van der Linden, F.P.G.M. Development of the Human Dentition, 1st ed.; Quintessence Publishing Co., Inc.: Batavia, IL, USA, 2016; pp. 65–72. [Google Scholar]
- Kamegai, T.; Tatsuki, T.; Nagano, H.; Mitsuhashi, H.; Kumeta, J.; Tatsuki, Y.; Kamegai, T.; Inaba, D. A determination of bite force in northern Japanese children. Eur. J. Orthod. 2005, 27, 53–57. [Google Scholar] [CrossRef]
- Mountain, G.; Wood, D.; Toumba, J. Bite force measurement in children with primary dentition. Int. J. Paediatr. Dent. 2011, 21, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Baldissara, P.; Ozcan, M.; Melilli, D.; Valandro, L.F. Effect of cyclic loading on fracture strength and microleakage of a quartz fiber dowel with different adhesive, cement and resin core material combinations. Minerva Stomatol. 2010, 59, 407–414. [Google Scholar]
- Kobayashi, F.Y.; Furlan, N.F.; Barbosa, T.S.; Castelo, P.M.; Gavião, M.B. Evaluation of masticatory performance and bite force in children with sleep bruxism. J. Oral Rehabil. 2012, 39, 776–784. [Google Scholar] [CrossRef]
- Braun, S.; Hnat, W.P.; Freudenthaler, J.W.; Marcotte, M.R.; Hönigle, K.; Johnson, B.E. A study of maximum bite force during growth and development. Angle Orthod. 1996, 66, 261–264. [Google Scholar] [CrossRef]
- Fink, J.K. Materials, Chemicals and Methods for Dental Applications; John Wiley & Sons: Hoboken, NJ, USA, 2018. [Google Scholar]
- Kim, N.Y.; Kim, H.; Kim, I.H.; Lee, J.H.; Lee, K.E.; Lee, H.S.; Kim, J.H.; Song, J.S.; Shin, Y.S. Novel 3D Printed Resin Crowns for Primary Molars: In Vitro Study of Fracture Resistance, Biaxial Flexural Strength, and Dynamic Mechanical Analysis. Children 2022, 9, 1445. [Google Scholar] [CrossRef]
- Rossi, S.; Benaglia, M.; Brenna, D.; Porta, R.; Orlandi, M. Three dimensional (3d) printing: A straightforward, user-friendly protocol to convert virtual chemical models to real-life objects. J. Chem. Educ. 2015, 92, 1398–1401. [Google Scholar] [CrossRef]
- Kessler, A.; Reymus, M.; Hickel, R.; Kunzelmann, K.H. Three-body wear of 3d printed temporary materials. Dent. Mater. 2019, 35, 1805–1812. [Google Scholar] [CrossRef] [PubMed]
- Ligon, S.C.; Liska, R.; Stampfl, J.; Gurr, M.; Mülhaupt, R. Polymers for 3d printing and customized additive manufacturing. Chem. Rev. 2017, 117, 10212–10290. [Google Scholar] [CrossRef]
- Oysaed, H.; Ruyter, I.E. Water sorption and filler characteristics of composites for use in posterior teeth. J. Dent. Res. 1986, 65, 1315–1318. [Google Scholar] [CrossRef]
- Choi, J.W.; Bae, I.H.; Noh, T.H.; Ju, S.W.; Lee, T.K.; Ahn, J.S.; Jeong, T.S.; Huh, J.B. Wear of primary teeth caused by opposed all-ceramic or stainless steel crowns. J. Adv. Prosthodont. 2016, 8, 43–52. [Google Scholar] [CrossRef]
- Vichi, A.; Balestra, D.; Scotti, N.; Louca, C.; Paolone, G. Translucency of CAD/CAM and 3D Printable Composite Materials for Permanent Dental Restorations. Polymers 2023, 15, 1443. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | Abbreviation | Product (Lot No.) | Composition | Content (%) | Flexural Strength (MPa) | Flexural Modulus (MPa) | Manufacturer |
|---|---|---|---|---|---|---|---|
| 3D-printed polymer | TC | TC-80DP (B1220K11-003) | α,α′-[(1-Methylethylidene)di-4,1-phenylene]bis[ω-[(2-methyl-1-oxo-2-propenyl)oxy]poly(oxy-1,2-ethanediyl) | 0–20 | ≥220 | ≥4500 | Graphy, Seoul, Korea |
| 1,4-Butanediol polymer with α-hydro-ω-hydroxypoly(oxy-1,4-butanediyl) and 1,1′-methylendbis [4-isocyanatobenzene] | 20–60 | ||||||
| 2-Hydroxyethyl methacrylate | 30–80 | ||||||
| Phenylbis(2,4,6-trimethylbenzoyl)phosphine oxide | 0–10 | ||||||
| Butylhydroxytoluene | 0–1 | ||||||
| Titanium dioxide | 0–1 | ||||||
| Pigment | 0–1 | ||||||
| TFD | TFD-23-5 (prototype) | α,α′-[(1-Methylethylidene)di-4,1-phenylene]bis[ω-[(2-methyl-1-oxo-2-propenyl)oxy]poly(oxy-1,2-ethanediyl) | 0–20 | ≥100 | ≥2850 | Graphy, Seoul, Korea | |
| 1,4-Butanediol polymer with α-hydro-ω-hydroxypoly(oxy-1,4-butanediyl) and 1,1′-methylendbis[4-isocyanatobenzene] | 20–60 | ||||||
| 2-Hydroxyethyl methacrylate | 30–80 | ||||||
| Phenylbis(2,4,6-trimethylbenzoyl)phosphine oxide | 0–10 | ||||||
| Titanium dioxide | 0–1 | ||||||
| Pigment | 0–1 | ||||||
| Zirconia | Zr | Luxen Enamel (201113-10E2P-7) | ZrO2 + HfO2 + Y2O3 | >99.8 wt.% | Dentalmax, Cheonan, Korea | ||
| (Y2O3) | (4–6 wt.%) |
| Static Fracture Load (N) | Dynamic Fracture Load (N) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean | SD | Max | Min | n | Mean | SD | Max | Min | |
| TC04 | 10 | 3079.20 | 955.57 | 4435.58 | 2152.53 | 10 | 2472.78 | 576.25 | 3265.73 | 1537.46 |
| TFD04 | 10 | 3533.92 | 644.19 | 4440.78 | 2958.33 | 10 | 3260.17 | 915.38 | 4469.83 | 2065.35 |
| Zr | 10 | 3632.71 | 596.74 | 4435.97 | 2643.25 | 10 | 2585.75 | 665.54 | 3632.56 | 1823.38 |
| p | 0.119 | 0.113 | ||||||||
| Static Fracture Load (N) | Dynamic Fracture Load (N) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean | SD | Max | Min | n | Mean | SD | Max | Min | |
| TC04 | 10 | 3079.20 | 955.57 | 4435.58 | 2152.53 | 10 | 2472.78 | 576.25 | 3265.73 | 1537.46 |
| TC06 | 10 | 1333.23 | 717.57 | 2994.81 | 764.78 | 10 | 1824.10 | 1346.70 | 4428.30 | 616.00 |
| p | 0.000 | 0.035 | ||||||||
| TFD04 | 10 | 3533.92 | 644.19 | 4440.78 | 2958.33 | 10 | 3260.17 | 915.38 | 4469.83 | 2065.35 |
| TFD06 | 10 | 3991.88 | 443.30 | 4405.87 | 2891.68 | 10 | 3800.15 | 764.96 | 4566.61 | 2224.63 |
| p | 0.353 | 0.280 | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.; Cho, W.; Lee, H.; Bae, J.; Jeong, T.; Huh, J.; Shin, J. Strength and Surface Characteristics of 3D-Printed Resin Crowns for the Primary Molars. Polymers 2023, 15, 4241. https://doi.org/10.3390/polym15214241
Park S, Cho W, Lee H, Bae J, Jeong T, Huh J, Shin J. Strength and Surface Characteristics of 3D-Printed Resin Crowns for the Primary Molars. Polymers. 2023; 15(21):4241. https://doi.org/10.3390/polym15214241
Chicago/Turabian StylePark, Soyoung, Wontak Cho, Hyeonjong Lee, Jihyeon Bae, Taesung Jeong, Jungbo Huh, and Jonghyun Shin. 2023. "Strength and Surface Characteristics of 3D-Printed Resin Crowns for the Primary Molars" Polymers 15, no. 21: 4241. https://doi.org/10.3390/polym15214241
APA StylePark, S., Cho, W., Lee, H., Bae, J., Jeong, T., Huh, J., & Shin, J. (2023). Strength and Surface Characteristics of 3D-Printed Resin Crowns for the Primary Molars. Polymers, 15(21), 4241. https://doi.org/10.3390/polym15214241