
A Review of PRESAGE Radiochromic Polymer and the Compositions for Application in Radiotherapy Dosimetry

 ,
,
Abstract
1. Introduction
1.1. Radiotherapy Dosimetry
1.2. Radiochromic Dosimeters
1.2.1. Fricke Gel Dosimeter
1.2.2. Polymer Gel Dosimeter
1.2.3. Radiochromic Polymer Dosimeter
2. The Components of PRESAGE
3. Radiological Properties of PRESAGE
3.1. The Role of Effective Atomic Number of Elements
3.2. The Effect of Metal Compounds
3.3. The Effect of Radical Initiator
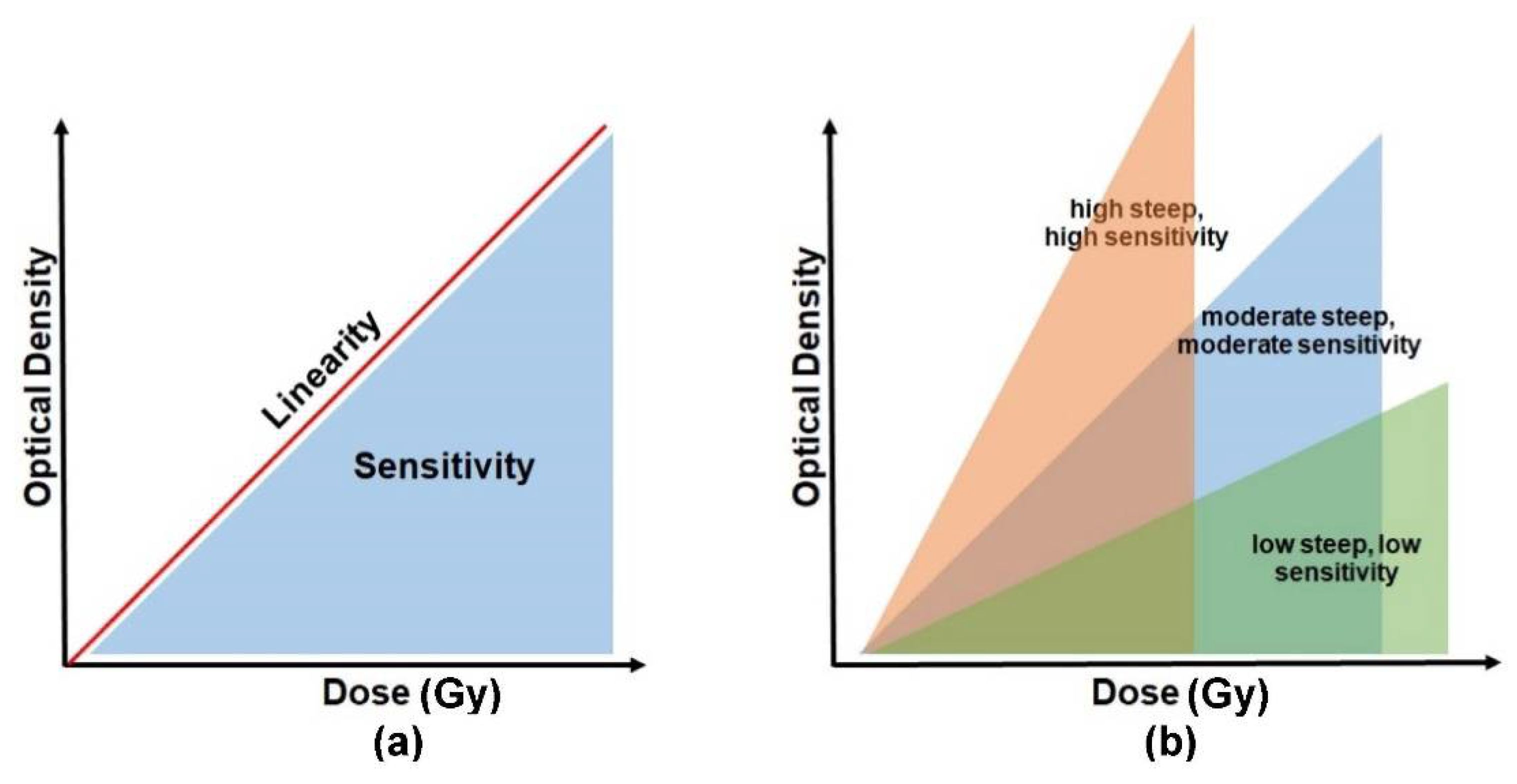
4. Sensitivity and Linearity of PRESAGE
4.1. The Effect of Radical Initiator Concentration on the Sensitivity
4.2. The Effect of Metal Compounds on the Sensitivity
4.3. Linearity of PRESAGE
5. Dose Rate and Energy Dependency
5.1. The Dose Rate Dependency
5.2. The Energy Dependency
6. Stability of PRESAGE
6.1. The Effect of Radical Initiator
6.2. The Effect of Metal Compound
7. Reusability and Reproducibility
8. Readout Modalities
8.1. Magnetic Resonance Imaging (MRI)
8.2. Ultrasound
8.3. X-ray Computed Tomography (X-ray CT)
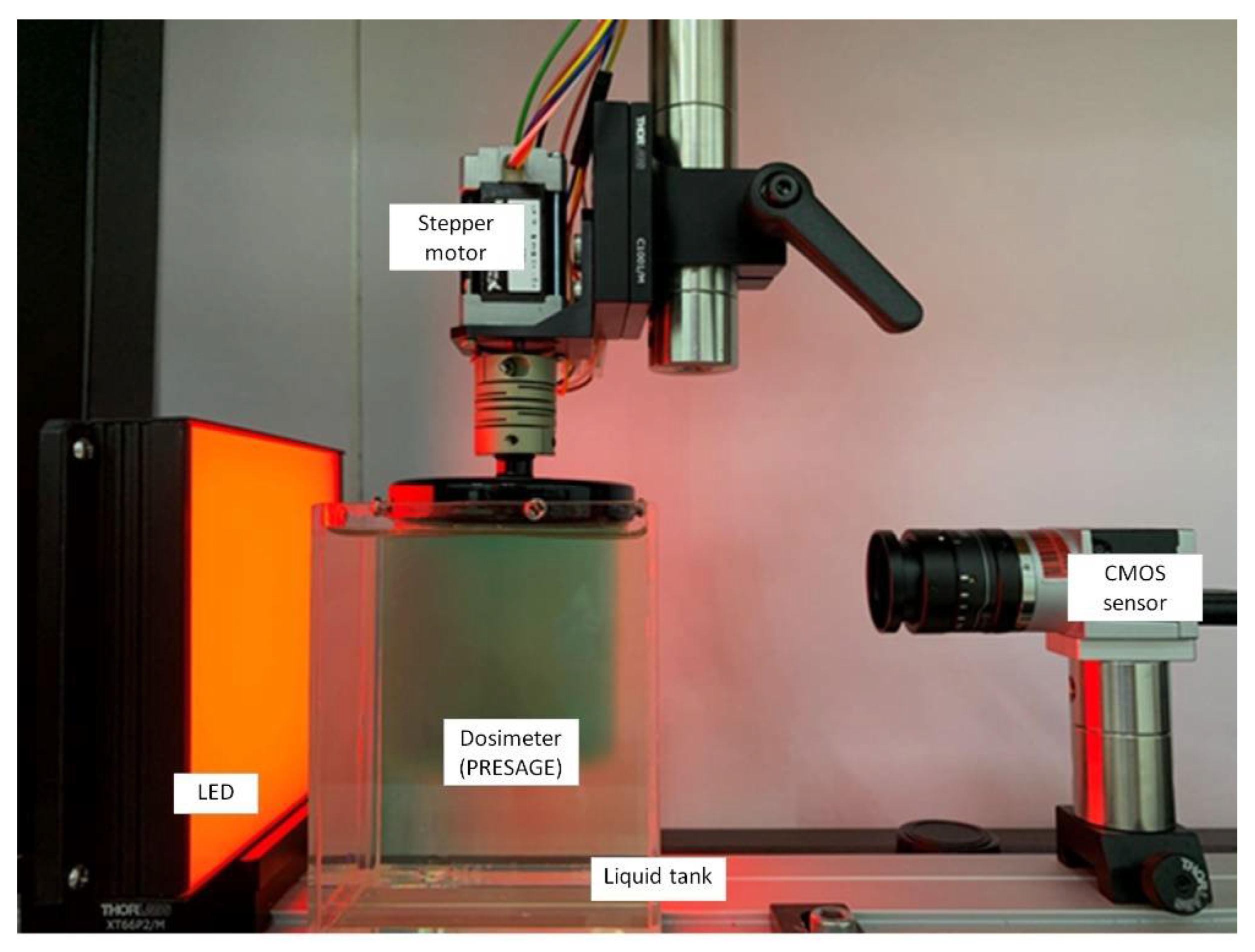
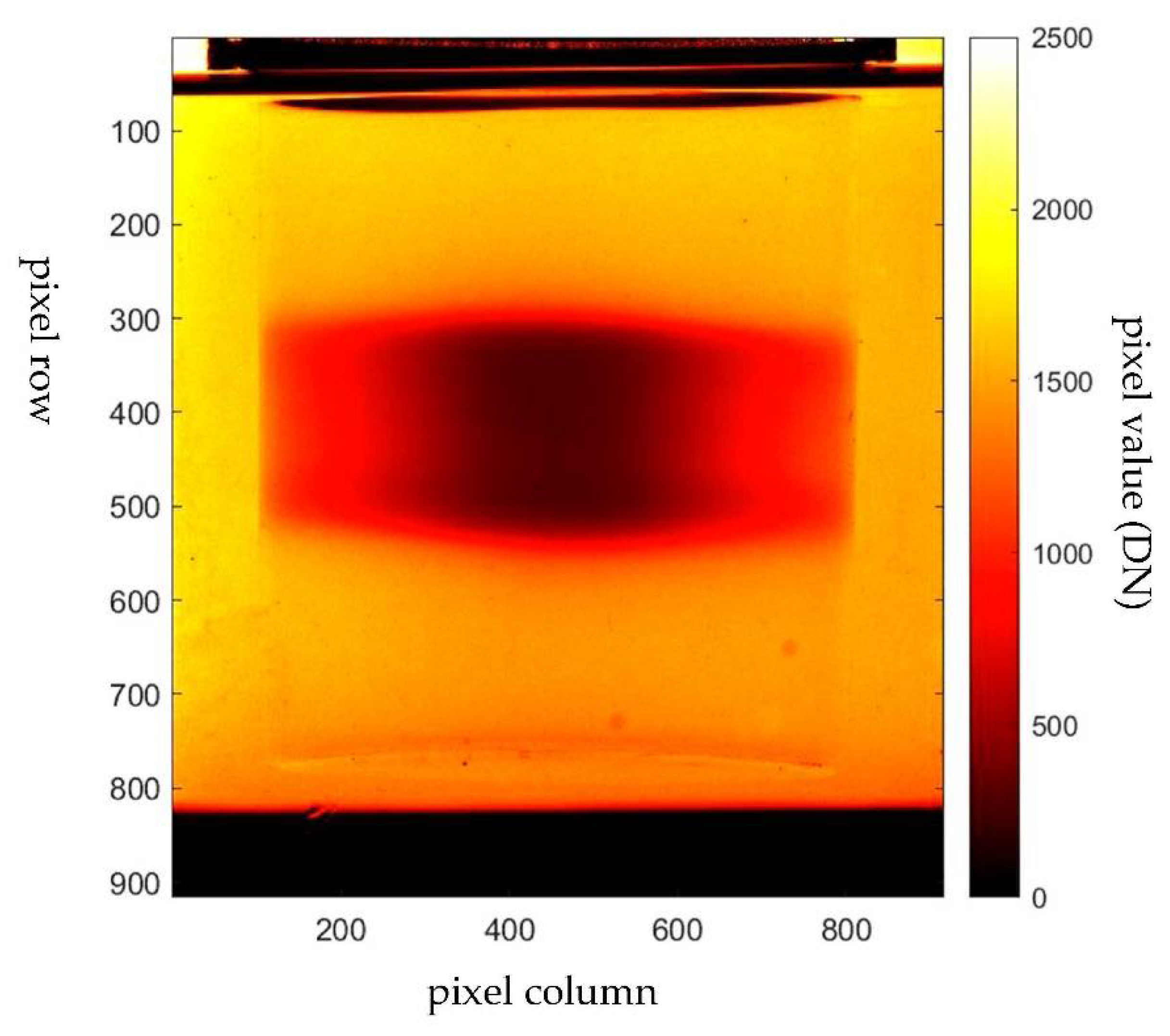
8.4. Optical Computed Tomography (OCT)
9. Dosimetry Applications
9.1. Applications in Radiotherapy Dosimetry
9.2. The Challenge in Small Field Dosimetry
9.3. Application in Brachytherapy
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Ervik, M.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.; Forman, D.; Bray, F. Cancer Incidence and Mortality Worldwide: IARC Cancer Base; International Agency for Research on Cancer: Lyon, France, 2012. [Google Scholar]
- Bourhis, J.; Montay-Gruel, P.; Jorge, P.G.; Bailat, C.; Petit, B.; Ollivier, J.; Jeanneret-Sozzi, W.; Ozsahin, M.; Bochud, F.; Moeckli, R. Clinical translation of FLASH radiotherapy: Why and how? Radiother. Oncol. 2019, 139, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Pucci, C.; Martinelli, C.; Ciofani, G. Innovative approaches for cancer treatment: Current perspectives and new challenges. Ecancermedicalscience 2019, 13, 961. [Google Scholar] [CrossRef]
- Schirrmacher, V. From chemotherapy to biological therapy: A review of novel concepts to reduce the side effects of systemic cancer treatment. Int. J. Oncol. 2019, 54, 407–419. [Google Scholar] [PubMed]
- Hanna, T.P.; King, W.D.; Thibodeau, S.; Jalink, M.; Paulin, G.A.; Harvey-Jones, E.; O’Sullivan, D.E.; Booth, C.M.; Sullivan, R.; Aggarwal, A. Mortality due to cancer treatment delay: Systematic review and meta-analysis. BMJ 2020, 371, m4087. [Google Scholar] [CrossRef] [PubMed]
- Kearney, V.; Chan, J.W.; Valdes, G.; Solberg, T.D.; Yom, S.S. The application of artificial intelligence in the IMRT planning process for head and neck cancer. Oral Oncol. 2018, 87, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Chiavassa, S.; Bessieres, I.; Edouard, M.; Mathot, M.; Moignier, A. Complexity metrics for IMRT and VMAT plans: A review of current literature and applications. Br. J. Radiol. 2019, 92, 20190270. [Google Scholar] [CrossRef]
- Antoine, M.; Ralite, F.; Soustiel, C.; Marsac, T.; Sargos, P.; Cugny, A.; Caron, J. Use of metrics to quantify IMRT and VMAT treatment plan complexity: A systematic review and perspectives. Phys. Med. 2019, 64, 98–108. [Google Scholar] [CrossRef]
- Gerhard, S.G.; Palma, D.A.; Arifin, A.J.; Louie, A.V.; Li, G.J.; Al-Shafa, F.; Cheung, P.; Rodrigues, G.B.; Bassim, C.W.; Corkum, M.T. Organ at risk dose constraints in SABR: A systematic review of active clinical trials. Pract. Radiat. Oncol. 2021, 11, e355–e365. [Google Scholar] [CrossRef]
- Dieterich, S.; Green, O.; Booth, J. SBRT targets that move with respiration. Phys. Med. 2018, 56, 19–24. [Google Scholar] [CrossRef]
- Cho, B. Intensity-modulated radiation therapy: A review with a physics perspective. Radiat. Oncol. J. 2018, 36, 1–10. [Google Scholar] [CrossRef]
- Bockel, S.; Espenel, S.; Sun, R.; Dumas, I.; Gouy, S.; Morice, P.; Chargari, C. Image-guided brachytherapy for salvage reirradiation: A systematic review. Cancers 2021, 13, 1226. [Google Scholar] [CrossRef]
- Tanderup, K.; Nesvacil, N.; Kirchheiner, K.; Serban, M.; Spampinato, S.; Jensen, N.B.K.; Schmid, M.; Smet, S.; Westerveld, H.; Ecker, S. Evidence-based dose planning aims and dose prescription in image-guided brachytherapy combined with radiochemotherapy in locally advanced cervical cancer. Proc. Semin. Radiat. Oncol. 2020, 30, 311–327. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.L. Automated radiotherapy treatment planning. Proc. Semin. Radiat. Oncol. 2019, 29, 209–218. [Google Scholar] [CrossRef]
- Clements, M.; Schupp, N.; Tattersall, M.; Brown, A.; Larson, R. Monaco treatment planning system tools and optimization processes. Med. Dosim. 2018, 43, 106–117. [Google Scholar] [CrossRef] [PubMed]
- Schreiner, L. True 3D chemical dosimetry (gels, plastics): Development and clinical role. J. Phys. Conf. Ser. 2015, 573, 1742–6596. [Google Scholar] [CrossRef]
- Jaffray, D.A.; Gospodarowicz, M.K. Radiation Therapy for Cancer. Cancer Dis. Control. Priorities 2015, 3, 239–248. [Google Scholar]
- Watanabe, Y.; Warmington, L.; Gopishankar, N. Three-dimensional radiation dosimetry using polymer gel and solid radiochromic polymer: From basics to clinical applications. World J. Radiol. 2017, 9, 112. [Google Scholar] [CrossRef]
- Jordan, K. Review of recent advances in radiochromic materials for 3D dosimetry. J. Phys. Conf. Ser. 2010, 250, 012043. [Google Scholar] [CrossRef]
- Khezerloo, D.; Nedaie, H.A.; Takavar, A.; Zirak, A.; Farhood, B.; Movahedinejhad, H.; Banaee, N.; Ahmadalidokht, I.; Knuap, C. PRESAGE® as a solid 3-D radiation dosimeter: A review article. Radiat. Phys. Chem. 2017, 141, 88–97. [Google Scholar] [CrossRef]
- Stathakis, S.; Myers, P.; Esquivel, C.; Mavroidis, P.; Papanikolaou, N. Characterization of a novel 2D array dosimeter for patient-specific quality assurance with volumetric arc therapy. Med. Phys. 2013, 40, 071731. [Google Scholar] [CrossRef]
- Zhao, Y.; Hinds, M.; Moritz, T.; Gunn, J.; Pogue, B.; Davis, S. A 2D imaging dosimeter for photodynamic therapy. In Proceedings of the Optical Methods for Tumor Treatment and Detection: Mechanisms and Techniques in Photodynamic Therapy XXVIII, San Francisco, CA, USA, 28 February 2019; p. 108600. [Google Scholar]
- Mohamed, I.E.; Ibrahim, A.G.; Zidan, H.M.; El-Bahkiry, H.S.; El-sahragti, A.Y. Physical dosimetry of volumetric modulated arc therapy (VMAT) using EPID and 2D array for quality assurance. Egypt. J. Radiol. Nucl. Med. 2018, 49, 477–484. [Google Scholar] [CrossRef]
- Muir, B.; Nahum, A. Ionisation Chambers. In Handbook of Radiotherapy Physics; CRC Press: Boca Raton, FL, USA, 2021; pp. 321–338. [Google Scholar]
- Santos, T.; Ventura, T.; do Carmo Lopes, M. A review on radiochromic film dosimetry for dose verification in high energy photon beams. Radiat. Phys. Chem. 2021, 179, 109217. [Google Scholar] [CrossRef]
- Casolaro, P. Radiochromic films for the two-dimensional dose distribution assessment. Appl. Sci. 2021, 11, 2132. [Google Scholar] [CrossRef]
- Hoppe, R.; Phillips, T.L.; Roach, M. Leibel and Phillips Textbook of Radiation Oncology-E-Book: Expert Consult; Elsevier Health Sciences: Amsterdam, The Netherlands, 2010. [Google Scholar]
- 5 Luminescence Dosimetry. J. ICRU 2019, 19, 69–87. [CrossRef]
- Rosenfeld, A.B.; Biasi, G.; Petasecca, M.; Lerch, M.L.; Villani, G.; Feygelman, V. Semiconductor dosimetry in modern external-beam radiation therapy. Phys. Med. Biol. 2020, 65, 16TR01. [Google Scholar] [CrossRef]
- Karmakar, A.; Wang, J.; Prinzie, J.; De Smedt, V.; Leroux, P. A review of semiconductor based ionising radiation sensors used in Harsh radiation environments and their applications. Radiation 2021, 1, 194–217. [Google Scholar] [CrossRef]
- Chaikh, A.; Gaudu, A.; Balosso, J. Monitoring methods for skin dose in interventional radiology. Int. J. Cancer Ther. Oncol. 2014, 3, 03011. [Google Scholar] [CrossRef][Green Version]
- Olaciregui-Ruiz, I.; Vivas-Maiques, B.; Kaas, J.; Perik, T.; Wittkamper, F.; Mijnheer, B.; Mans, A. Transit and non-transit 3D EPID dosimetry versus detector arrays for patient specific QA. J. Appl. Clin. Med. Phys. 2019, 20, 79–90. [Google Scholar] [CrossRef]
- Alhazmi, A.; Gianoli, C.; Neppl, S.; Martins, J.; Veloza, S.; Podesta, M.; Verhaegen, F.; Reiner, M.; Belka, C.; Parodi, K. A novel approach to EPID-based 3D volumetric dosimetry for IMRT and VMAT QA. Phys. Med. Biol. 2018, 63, 115002. [Google Scholar] [CrossRef]
- Chan, G.H.; Chin, L.C.; Abdellatif, A.; Bissonnette, J.P.; Buckley, L.; Comsa, D.; Granville, D.; King, J.; Rapley, P.L.; Vandermeer, A. Survey of patient-specific quality assurance practice for IMRT and VMAT. J. Appl. Clin. Med. Phys. 2021, 22, 155–164. [Google Scholar] [CrossRef]
- Rahman, A.T.A.; Rosli, N.F.; Zain, S.M.; Zin, H.M. Recent advances in Optical Computed Tomography (OCT) imaging system for three dimensional (3D) radiotherapy dosimetry. IOP Conf. Ser. Mater. Sci. Eng. 2018, 298, 012036. [Google Scholar] [CrossRef]
- Oldham, M.; Godfrey, D.; Juang, T.; Thomas, A. Two-dimensional and Three-dimensional Dosimetry. In Handbook of Radiotherapy Physics; CRC Press: Boca Raton, FL, USA, 2021; pp. 359–376. [Google Scholar]
- Marrale, M.; d’Errico, F. Hydrogels for three-dimensional ionizing-radiation dosimetry. Gels 2021, 7, 74. [Google Scholar] [CrossRef] [PubMed]
- Oldham, M.; Godfrey, D.; Das, S.; Wolbarst, A. Advances in Medical Physics. 2014; in press. [Google Scholar]
- Schreiner, L. Where does gel dosimetry fit in the clinic. J. Phys. Conf. Ser. 2009, 164, 012001. [Google Scholar] [CrossRef]
- Baldock, C.; De Deene, Y.; Doran, S.; Ibbott, G.; Jirasek, A.; Lepage, M.; McAuley, K.; Oldham, M.; Schreiner, L. Polymer gel dosimetry. Phys. Med. Biol. 2010, 55, R1. [Google Scholar] [CrossRef]
- Day, M.; Stein, G. Chemical effects of ionizing radiation in some gels. Nature 1950, 166, 146–147. [Google Scholar] [CrossRef]
- Hoecker, F.E.; Watkins, I. Radiation polymerization dosimetry. Int. J. Appl. Radiat. Isot. 1958, 3, 31–35. [Google Scholar] [CrossRef]
- Abtahi, S.; Aghamiri, S.; Khalafi, H. Optical and MRI investigations of an optimized acrylamide-based polymer gel dosimeter. J. Radioanal. Nucl. Chem. 2014, 300, 287–301. [Google Scholar] [CrossRef]
- Abtahi, S.; Zahmatkesh, M.; Khalafi, H. Investigation of an improved MAA-based polymer gel for thermal neutron dosimetry. J. Radioanal. Nucl. Chem. 2016, 307, 855–868. [Google Scholar] [CrossRef]
- Gore, J.; Kang, Y. Measurement of radiation dose distributions by nuclear magnetic resonance (NMR) imaging. Phys. Med. Biol. 1984, 29, 1189. [Google Scholar] [CrossRef]
- Schreiner, L. Review of Fricke gel dosimeters. J. Phys. Conf. Ser. 2004, 3, 9. [Google Scholar] [CrossRef]
- Baldock, C.; Harris, P.; Piercy, A.; Healy, B. Experimental determination of the diffusion coefficient in two-dimensions in ferrous sulphate gels using the finite element method. Australas. Phys. Eng. Sci. Med. 2001, 24, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, T.V.; Olsen, D.R.; Skretting, A. Measurement of the ferric diffusion coefficient in agarose and gelatine gels by utilization of the evolution of a radiation induced edge as reflected in relaxation rate images. Phys. Med. Biol. 1997, 42, 1575. [Google Scholar] [CrossRef] [PubMed]
- Marini, A.; Lazzeri, L.; Cascone, M.G.; Ciolini, R.; Tana, L.; d’Errico, F. Fricke gel dosimeters with low-diffusion and high-sensitivity based on a chemically cross-linked PVA matrix. Radiat. Meas. 2017, 106, 618–621. [Google Scholar] [CrossRef]
- Maeyama, T.; Fukunishi, N.; Ishikawa, K.; Furuta, T.; Fukasaku, K.; Takagi, S.; Noda, S.; Himeno, R.; Fukuda, S. A diffusion-free and linear-energy-transfer-independent nanocomposite Fricke gel dosimeter. Radiat. Phys. Chem. 2014, 96, 92–96. [Google Scholar] [CrossRef]
- Bäck, S.Å.J.; Medin, J.; Magnusson, P.; Olsson, P.; Grusell, E.; Olsson, L.E. Ferrous sulphate gel dosimetry and MRI for proton beam dose measurements. Phys. Med. Biol. 1999, 44, 1983. [Google Scholar] [CrossRef] [PubMed]
- Gallo, S.; Pasquale, S.; Lenardi, C.; Veronese, I.; Gueli, A.M. Effect of ionizing radiation on the colorimetric properties of PVA-GTA Xylenol Orange Fricke gel dosimeters. Dye. Pigment. 2021, 187, 109141. [Google Scholar] [CrossRef]
- Boase, N.R.; Smith, S.T.; Masters, K.-S.; Hosokawa, K.; Crowe, S.B.; Trapp, J.V. Xylenol orange functionalised polymers to overcome diffusion in Fricke gel radiation dosimeters. React. Funct. Polym. 2018, 132, 81–88. [Google Scholar] [CrossRef]
- Alexander, P.; Charlesby, A.; Ross, M. The degradation of solid polymethylmethacrylate by ionizing radiation. Proc. R. Soc. Lond. Ser. A Math. Phys. Sci. 1954, 223, 392–404. [Google Scholar]
- Abtahi, S.; Aghamiri, S.; Khalafi, H.; Rahmani, F. An investigation into the potential applicability of gel dosimeters for dosimetry in boron neutron capture therapy. Int. J. Radiat. Res. 2014, 12, 149. [Google Scholar]
- Crescenti, R.A.; Scheib, S.G.; Schneider, U.; Gianolini, S. Introducing gel dosimetry in a clinical environment: Customization of polymer gel composition and magnetic resonance imaging parameters used for 3D dose verifications in radiosurgery and intensity modulated radiotherapy. Med. Phys. 2007, 34, 1286–1297. [Google Scholar] [CrossRef]
- McJury, M.; Oldham, M.; Cosgrove, V.; Murphy, P.; Doran, S.; Leach, M.; Webb, S. Radiation dosimetry using polymer gels: Methods and applications. Br. J. Radiol. 2000, 73, 919–929. [Google Scholar] [CrossRef] [PubMed]
- Hilts, M.; Audet, C.; Duzenli, C.; Jirasek, A. Polymer gel dosimetry using x-ray computed tomography: A feasibility study4. Phys. Med. Biol. 2000, 45, 2559. [Google Scholar] [CrossRef] [PubMed]
- Maryanski, M.; Zastavker, Y.; Gore, J. Radiation dose distributions in three dimensions from tomographic optical density scanning of polymer gels: II. Optical properties of the BANG polymer gel. Phys. Med. Biol. 1996, 41, 2705. [Google Scholar] [CrossRef]
- Mather, M.L.; Whittaker, A.K.; Baldock, C. Ultrasound evaluation of polymer gel dosimeters. Phys. Med. Biol. 2002, 47, 1449. [Google Scholar] [CrossRef] [PubMed]
- Guo, P.; Adamovics, J.; Oldham, M. Characterization of a new radiochromic three-dimensional dosimeter. Med. Phys. 2006, 33, 1338–1345. [Google Scholar] [CrossRef]
- Hepworth, S.; Leach, M.; Doran, S. Dynamics of polymerization in polyacrylamide gel (PAG) dosimeters:(II) modelling oxygen diffusion. Phys. Med. Biol. 1999, 44, 1875. [Google Scholar] [CrossRef][Green Version]
- Fong, P.M.; Keil, D.C.; Does, M.D.; Gore, J.C. Polymer gels for magnetic resonance imaging of radiation dose distributions at normal room atmosphere. Phys. Med. Biol. 2001, 46, 3105. [Google Scholar] [CrossRef]
- De Deene, Y.; Venning, A.; Hurley, C.; Healy, B.; Baldock, C. Dose–response stability and integrity of the dose distribution of various polymer gel dosimeters. Phys. Med. Biol. 2002, 47, 2459. [Google Scholar] [CrossRef]
- Hurley, C.; Venning, A.; Baldock, C. A study of a normoxic polymer gel dosimeter comprising methacrylic acid, gelatin and tetrakis (hydroxymethyl) phosphonium chloride (MAGAT). Appl. Radiat. Isot. 2005, 63, 443–456. [Google Scholar] [CrossRef]
- De Deene, Y.; Hurley, C.; Venning, A.; Vergote, K.; Mather, M.; Healy, B.; Baldock, C. A basic study of some normoxic polymer gel dosimeters. Phys. Med. Biol. 2002, 47, 3441. [Google Scholar] [CrossRef]
- Khan, M.; Heilemann, G.; Lechner, W.; Georg, D.; Berg, A.G. Basic Properties of a New Polymer Gel for 3D-Dosimetry at High Dose-Rates Typical for FFF Irradiation Based on Dithiothreitol and Methacrylic Acid (MAGADIT): Sensitivity, Range, Reproducibility, Accuracy, Dose Rate Effect and Impact of Oxygen Scavenger. Polymers 2019, 11, 1717. [Google Scholar] [CrossRef] [PubMed]
- De Deene, Y. Fundamental characteristics of normoxic polymer gel dosimeters. In Proceedings of the IFMBE World Congress on Medical Physics and Biomedical Engineering, Sydney, Australia, 24 August 2003. [Google Scholar]
- Senden, R.; De Jean, P.; McAuley, K.; Schreiner, L. Polymer gel dosimeters with reduced toxicity: A preliminary investigation of the NMR and optical dose–response using different monomers. Phys. Med. Biol. 2006, 51, 3301. [Google Scholar] [CrossRef]
- Hilts, M. X-ray computed tomography imaging of polymer gel dosimeters. J. Phys. Conf. Ser. 2006, 56, 95. [Google Scholar] [CrossRef]
- Adamovics, J.; Maryanski, M. Characterisation of PRESAGE™: A new 3-D radiochromic solid polymer dosemeter for ionising radiation. Radiat. Prot. Dosim. 2006, 120, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.; Venning, A.; De Deene, Y.; Vial, P.; Oliver, L.; Adamovics, J.; Baldock, C. Radiological properties of the PRESAGE and PAGAT polymer dosimeters. Appl. Radiat. Isot. 2008, 66, 1970–1974. [Google Scholar] [CrossRef]
- Alqathami, M.; Blencowe, A.; Ibbott, G. An investigation into the potential influence of oxygen on the efficiency of the PRESAGE® dosimeter. J. Phys. Conf. Ser. 2015, 573, 12044. [Google Scholar] [CrossRef]
- Adamovics, J.; Guo, P.; Burgess, D.; Manzoor, A.; Oldham, M. PRESAGETM-Development and optimization studies of a 3D radiochromic plastic dosimeter–Part 2. J. Phys. Conf. Ser. 2006, 56, 021. [Google Scholar]
- Khezerloo, D.; Nedaie, H.A.; Takavar, A.; Zirak, A.; Farhood, B.; Banaee, N.; Alidokht, E. Dosimetric properties of new formulation of PRESAGE® with tin organometal catalyst: Development of sensitivity and stability to megavoltage energy. J. Cancer Res. Ther. 2018, 14, 308. [Google Scholar]
- Jackson, J.; Juang, T.; Adamovics, J.; Oldham, M. An investigation of PRESAGE® 3D dosimetry for IMRT and VMAT radiation therapy treatment verification. Phys. Med. Biol. 2015, 60, 2217. [Google Scholar] [CrossRef]
- Adamovics, J.; Jordan, K.; Dietrich, J. PRESAGETM-Development and optimization studies of a 3D radiochromic plastic dosimeter–Part 1. J. Phys. Conf. Ser. 2006, 56, 020. [Google Scholar]
- Adamovics, J.; Maryanski, M. A new approach to radiochromic three-dimensional dosimetry-polyurethane. J. Phys. Conf. Ser. 2004, 3, 020. [Google Scholar] [CrossRef]
- Khezerloo, D.; Nedaie, H.A.; Farhood, B.; Zirak, A.; Takavar, A.; Banaee, N.; Ahmadalidokht, I.; Kron, T. Optical computed tomography in PRESAGE® three-dimensional dosimetry: Challenges and prospective. J. Cancer Res. Ther. 2017, 13, 419. [Google Scholar] [PubMed]
- Mostaar, A.; Hashemi, B.; Zahmatkesh, M.; Aghamiri, S.; Mahdavi, S. A basic dosimetric study of PRESAGE: The effect of different amounts of fabricating components on the sensitivity and stability of the dosimeter. Phys. Med. Biol. 2010, 55, 903. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.B. March’s Advanced Organic Chemistry: Reactions, Mechanisms, and Structure; John Wiley & Sons: Hoboken, NJ, USA, 2020. [Google Scholar]
- Strukul, G. Catalytic Oxidations with Hydrogen Peroxide as Oxidant; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2013; Volume 9. [Google Scholar]
- Alqathami, M.; Adamovics, J.; Benning, R.; Qiao, G.; Geso, M.; Blencowe, A. Evaluation of ultra-sensitive leucomalachite dye derivatives for use in the PRESAGE® dosimeter. Radiat. Phys. Chem. 2013, 85, 204–209. [Google Scholar] [CrossRef]
- Gorjiara, T.; Hill, R.; Kuncic, Z.; Adamovics, J.; Bosi, S.; Kim, J.H.; Baldock, C. Investigation of radiological properties and water equivalency of PRESAGE® dosimeters. Med. Phys. 2011, 38, 2265–2274. [Google Scholar] [CrossRef]
- Khan, F.M. The Physics of Radiation Therapy; Wolters Kluwer Health: Philadelphia, PA, USA, 2012. [Google Scholar]
- Kobayashi, K.; Usami, N.; Porcel, E.; Lacombe, S.; Le Sech, C. Enhancement of radiation effect by heavy elements. Mutat. Res. Rev. Mutat. Res. 2010, 704, 123–131. [Google Scholar] [CrossRef]
- Compton, A.H. A quantum theory of the scattering of X-rays by light elements. Phys. Rev. 1923, 21, 483. [Google Scholar] [CrossRef]
- Hubbell, J.H.; Seltzer, S.M. Tables of X-ray Mass Attenuation Coefficients and Mass Energy-Absorption Coefficients 1 keV to 20 MeV for Elements Z = 1 to 92 and 48 Additional Substances of Dosimetric Interest; National Inst. of Standards and Technology-PL: Gaithersburg, MD, USA, 1995.
- Brown, S.; Venning, A.; De Deene, Y.; Vial, P.; Oliver, L.; Adamovics, J.; Baldock, C. Radiological properties of the pagat gel dosimeter and the presage polymer dosimeter. Australas. Phys. Eng. Sci. Med. 2007, 30, 436. [Google Scholar]
- Gagliardi, F.M.; Day, L.; Poole, C.M.; Franich, R.D.; Geso, M. Water equivalent PRESAGE® for synchrotron radiation therapy dosimetry. Med. Phys. 2018, 45, 1255–1265. [Google Scholar] [CrossRef]
- Alqathami, M.; Blencowe, A.; Qiao, G.; Adamovics, J.; Geso, M. Optimizing the sensitivity and radiological properties of the PRESAGE® dosimeter using metal compounds. Radiat. Phys. Chem. 2012, 81, 1688–1695. [Google Scholar] [CrossRef]
- Alqathami, M.; Blencowe, A.; Geso, M.; Ibbott, G. Characterization of novel water-equivalent PRESAGE® dosimeters for megavoltage and kilovoltage X-ray beam dosimetry. Radiat. Meas. 2015, 74, 12–19. [Google Scholar] [CrossRef]
- Alqathami, M.; Blencowe, A.; Qiao, G.; Butler, D.; Geso, M. Optimization of the sensitivity and stability of the PRESAGE™ dosimeter using trihalomethane radical initiators. Radiat. Phys. Chem. 2012, 81, 867–873. [Google Scholar] [CrossRef]
- Alghadhban, S.; Youn, S.; Na, Y.; Kim, K.; Ye, S.-J. Optimization of bromine-based radical initiators using leucomalachite green and solvents in PRESAGE® dosimeter. Radiat. Phys. Chem. 2022, 194, 109985. [Google Scholar] [CrossRef]
- Eznaveh, Z.S.; Zahamtkesh, M.; Asl, A.K.; Bagheri, S. Sensitivity optimization of PRESAGE polyurethane based dosimeter. Radiat. Meas. 2010, 45, 89–91. [Google Scholar] [CrossRef]
- Carroll, M.; Alqathami, M.; Ibbott, G. The quenching effect in PRESAGE® by a proton beam: Investigation of formulation dependence. J. Phys. Conf. Ser. 2017, 847, 012027. [Google Scholar] [CrossRef]
- Tran, J.; Agelou, M.; Amiot, M.-N.; Boissonnat, G.; Dehe-Pittance, C.; Girard, H.; Lazaro, D.; Simic, V.; Tromson, D. Flexible radiochromic dosimeters development for complex irradiation beams. J. Phys. Conf. Ser. 2022, 2167, 012002. [Google Scholar] [CrossRef]
- Cho, J.D.; Son, J.; Choi, C.H.; Kim, J.S.; Wu, H.-G.; Park, J.M.; Kim, J.-I. Improvement in sensitivity of radiochromic 3D dosimeter based on rigid polyurethane resin by incorporating tartrazine. PLoS ONE 2020, 15, e0230410. [Google Scholar] [CrossRef] [PubMed]
- Yates, E.S.; Balling, P.; Petersen, J.B.; Christensen, M.N.; Skyt, P.S.; Bassler, N.; Kaiser, F.-J.; Muren, L.P. Characterization of the optical properties and stability of Presage™ following irradiation with photons and carbon ions. Acta Oncol. 2011, 50, 829–834. [Google Scholar] [CrossRef]
- Alqathami, M.; Adamovics, J.; Benning, R.; Blencowe, A. An investigation into ultra-sensitive substituted leucomalachite dye derivatives for use in the PRESAGE® dosimeter. J. Phys. Conf. Ser. 2013, 444, 012034. [Google Scholar] [CrossRef]
- Wang, Z.; Thomas, A.; Newton, J.; Ibbott, G.; Deasy, J.; Oldham, M. Dose verification of stereotactic radiosurgery treatment for trigeminal neuralgia with presage 3D dosimetry system. J. Phys. Conf. Ser. 2010, 250, 012058. [Google Scholar] [CrossRef]
- Al-Nowais, S.; Nisbet, A.; Adamovics, J.; Doran, S.J. An attempt to determine the saturation dose for PRESAGE™. J. Phys. Conf. Ser. 2009, 164, 012043. [Google Scholar] [CrossRef]
- Gagliardi, F.M.; Franich, R.D.; Geso, M. Dose response and stability of water equivalent PRESAGE® dosimeters for synchrotron radiation therapy dosimetry. Phys. Med. Biol. 2018, 63, 235027. [Google Scholar] [CrossRef] [PubMed]
- Alqathami, M.; Blencowe, A.; Ibbott, G. Experimental determination of the influence of oxygen on the PRESAGE® dosimeter. Phys. Med. Biol. 2016, 61, 813. [Google Scholar] [CrossRef]
- Chang, K.H.; Lee, S.; Cao, Y.J.; Shim, J.B.; Lee, J.E.; Lee, N.K.; Lee, J.A.; Yang, D.S.; Park, Y.J.; Yoon, W.S. Comparison of the BANGkit™ and the PRESAGE™ gel dosimeters for use with a CCD-based optical CT scanner. J. Korean Phys. Soc. 2014, 64, 740–745. [Google Scholar] [CrossRef]
- Adamovics, J.; Farfán, E.B.; Coleman, J.R. Improving the Presage® Polymer Radiosensitivity for Hot Cell and Glovebox 3D Characterization. Health Phys. 2013, 104, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Park, J.M.; Park, S.-Y.; Choi, C.H.; Chun, M.; Han, J.H.; Cho, J.D.; Kim, J.-I. Dosimetric characteristics of a reusable 3D radiochromic dosimetry material. PLoS ONE 2017, 12, e0180970. [Google Scholar] [CrossRef]
- De Deene, Y. How important is the dose rate sensitivity of 2D and 3D radiation dosimeters? J. Phys. Conf. Ser. 2019, 1305, 012059. [Google Scholar] [CrossRef]
- Pappas, E.; Zoros, E.; Zourari, K.; Hourdakis, C.; Papagiannis, P.; Karaiskos, P.; Pantelis, E. PO-0774: Investigation of dose-rate dependence at an extensive range for PRESAGE radiochromic dosimeter. Radiother. Oncol. 2017, 123, S410. [Google Scholar] [CrossRef]
- Jensen, M.B.; Balling, P.; Doran, S.J.; Petersen, J.B.; Wahlstedt, I.H.; Muren, L.P. Dose response of three-dimensional silicone-based radiochromic dosimeters for photon irradiation in the presence of a magnetic field. Phys. Imaging Radiat. Oncol. 2020, 16, 81–84. [Google Scholar] [CrossRef]
- Clift, C.; Thomas, A.; Adamovics, J.; Chang, Z.; Das, I.; Oldham, M. Toward acquiring comprehensive radiosurgery field commissioning data using the PRESAGE®/optical-CT 3D dosimetry system. Phys. Med. Biol. 2010, 55, 1279. [Google Scholar] [CrossRef]
- Wang, Y.F.; Dona, O.; Liu, K.; Adamovics, J.; Wuu, C.S. Dosimetric characterization of a body-conforming radiochromic sheet. J. Appl. Clin. Med. Phys. 2020, 21, 167–177. [Google Scholar] [CrossRef]
- Wang, Y.-F.; Liu, K.; Adamovics, J.; Wuu, C.-S. An Investigation of dosimetric accuracy of a novel PRESAGE radiochromic sheet and its clinical applications. J. Phys. Conf. Ser. 2019, 1305, 012041. [Google Scholar] [CrossRef]
- Youkahana, E.Q.; Gagliardi, F.; Geso, M. Two-dimensional scanning of PRESAGE® dosimetry using UV/VIS spectrophotometry and its potential application in radiotherapy. Biomed. Phys. Eng. Express 2016, 2, 045009. [Google Scholar] [CrossRef]
- Zhao, L.; Newton, J.; Oldham, M.; Das, I.J.; Cheng, C.-W.; Adamovics, J. Feasibility of using PRESAGE® for relative 3D dosimetry of small proton fields. Phys. Med. Biol. 2012, 57, N431. [Google Scholar] [CrossRef]
- Oda, H. New developments in the stabilization of leuco dyes: Effect of UV absorbers containing an amphoteric counter-ion moiety on the light fastness of color formers. Dye. Pigment. 2005, 66, 103–108. [Google Scholar] [CrossRef]
- Pierquet, M.; Thomas, A.; Adamovics, J.; Oldham, M. An investigation into a new re-useable 3D radiochromic dosimetry material, PresageREU. J. Phys. Conf. Ser. 2010, 250, 012047. [Google Scholar] [CrossRef] [PubMed]
- Juang, T.; Adamovics, J.; Oldham, M. Characterization of a reusable PRESAGE® 3D dosimeter. J. Phys. Conf. Ser. 2015, 573, 012039. [Google Scholar] [CrossRef]
- Juang, T.; Newton, J.; Niebanck, M.; Benning, R.; Adamovics, J.; Oldham, M. Customising PRESAGE® for diverse applications. J. Phys. Conf. Ser. 2013, 444, 012029. [Google Scholar] [CrossRef]
- Juang, T.; Adamovics, J.; Oldham, M. TH-C-19A-05: Evaluation of a New Reusable 3D Dosimeter. Med. Phys. 2014, 41, 548. [Google Scholar] [CrossRef]
- Wuu, C.-S.; Xu, Y. 3-D dosimetry with optical CT scanning of polymer gels and radiochromic plastic dosimeter. Radiat. Meas. 2011, 46, 1903–1907. [Google Scholar] [CrossRef]
- Thomas, A.; Oldham, M. Fast, large field-of-view, telecentric optical-CT scanning system for 3D radiochromic dosimetry. J. Phys. Conf. Ser. 2010, 250, 012007. [Google Scholar] [CrossRef] [PubMed]
- Sakhalkar, H.; Adamovics, J.; Ibbott, G.; Oldham, M. A comprehensive evaluation of the PRESAGE/optical-CT 3D dosimetry system. Med. Phys. 2009, 36, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Oldham, M. 3D dosimetry by optical-CT scanning. J. Phys. Conf. Ser. 2006, 56, 006. [Google Scholar] [CrossRef]
- Rathnayaka, K.; Momot, K.I.; Noser, H.; Volp, A.; Schuetz, M.A.; Sahama, T.; Schmutz, B. Quantification of the accuracy of MRI generated 3D models of long bones compared to CT generated 3D models. Med. Eng. Phys. 2012, 34, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Hilts, M.; Jirasek, A.; Duzenli, C. Technical considerations for implementation of x-ray CT polymer gel dosimetry. Phys. Med. Biol. 2005, 50, 1727. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, R.; Lotan, Y. Cost consideration in utilization of multiparametric magnetic resonance imaging in prostate cancer. Transl. Androl. Urol. 2017, 6, 345. [Google Scholar] [CrossRef] [PubMed]
- Masoumi, H.; Mokhtari-Dizaji, M.; Arbabi, A.; Bakhshandeh, M. Determine the dose distribution using ultrasound parameters in MAGIC-f polymer gels. Dose-Response 2016, 14, 1559325815625647. [Google Scholar] [CrossRef]
- Khoei, S.; Trapp, J.V.; Langton, C.M. Ultrasound attenuation computed tomography assessment of PAGAT gel dose. Phys. Med. Biol. 2014, 59, N129. [Google Scholar] [CrossRef]
- Khoei, S.; Trapp, J.; Langton, C. Quantitative evaluation of polymer gel dosimeters by broadband ultrasound attenuation. J. Phys. Conf. Ser. 2013, 444, 012084. [Google Scholar] [CrossRef]
- Sakhalkar, H.; Oldham, M. Fast, high-resolution 3D dosimetry utilizing a novel optical-CT scanner incorporating tertiary telecentric collimation. Med. Phys. 2008, 35, 101–111. [Google Scholar] [CrossRef]
- Doran, S.J. The history and principles of optical computed tomography for scanning 3-D radiation dosimeters: 2008 update. J. Phys. Conf. Ser. 2009, 164, 12020. [Google Scholar] [CrossRef]
- Lopatiuk-Tirpak, O.; Langen, K.; Meeks, S.; Kupelian, P.; Zeidan, O.; Maryanski, M. Performance evaluation of an improved optical computed tomography polymer gel dosimeter system for 3D dose verification of static and dynamic phantom deliveries. Med. Phys. 2008, 35, 3847–3859. [Google Scholar] [CrossRef] [PubMed]
- Wolodzko, J.G.; Marsden, C.; Appleby, A. CCD imaging for optical tomography of gel radiation dosimeters. Med. Phys. 1999, 26, 2508–2513. [Google Scholar] [CrossRef] [PubMed]
- Jordan, K.; Battista, J. Small, medium and large optical cone beam CT. J. Phys. Conf. Ser. 2006, 56, 214. [Google Scholar] [CrossRef]
- Jordan, K.; Battista, J. A stable black-refractive-index-matching liquid for optical CT scanning of hydrogels. J. Phys. Conf. Ser. 2009, 164, 012045. [Google Scholar] [CrossRef]
- Doran, S.; Krstajic, N.; Adamovics, J.; Jenneson, P. Optical CT scanning of PRESAGE™ polyurethane samples with a CCD-based readout system. J. Phys. Conf. Ser. 2004, 3, 240. [Google Scholar] [CrossRef]
- Rosli, N.F.; Zin, H.M.; Rahman, A.T.A. Development of a CMOS-based optical computed tomography system (CMOS-OCT) for 3D radiotherapy dosimetry. Health Technol. 2018, 8, 189–196. [Google Scholar] [CrossRef]
- Mohyedin, M.Z.; Zin, H.M.; Hashim, S.; Bradley, D.A.; Aldawood, S.; Alkhorayef, M.; Sulieman, A.; Abdul Rahman, A.T. 2D and 3D dose analysis of PRESAGE® dosimeter using a prototype 3DmicroHD-OCT imaging system. Radiat. Phys. Chem. 2022, 2022, 110312. [Google Scholar] [CrossRef]
- Zin, H.M.; Rahman, A.T.A. Application of an in-house developed complementary metal-oxide-semiconductor-based optical computed tomography (CMOS-OCT) imaging system for stereotactic radiosurgery dosimetry using a PRESAGE® dosimeter. Radiat. Phys. Chem. 2022, 194, 110029. [Google Scholar] [CrossRef]
- Zin, H.M.; Konstantinidis, A.C.; Harris, E.J.; Osmond, J.P.; Olivo, A.; Bohndiek, S.E.; Clark, A.T.; Turchetta, R.; Guerrini, N.; Crooks, J. Characterisation of regional variations in a stitched CMOS active pixel sensor. Nucl. Instrum. Methods Phys. Res. Sect. A Accel. Spectrometers Detect. Assoc. Equip. 2010, 620, 540–548. [Google Scholar] [CrossRef]
- Gautam, B. Literature review on IMRT and VMAT for prostate cancer. Am. J. Cancer Rev. 2014, 2, 1–5. [Google Scholar]
- Menzel, H.-G. International commission on radiation units and measurements. J. ICRU 2014, 14, 1–2. [Google Scholar] [CrossRef]
- Agnew, C.E.; McGarry, C.K. A tool to include gamma analysis software into a quality assurance program. Radiother. Oncol. 2016, 118, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, K.; Ibbott, G.S.; Lafratta, R.G.; Gifford, K.A.; Buzdar, S.A. Dosimetric characterisation of anthropomorphic PRESAGE® dosimeter and EBT2 film for partial breast radiotherapy. J. Radiother. Pract. 2018, 17, 96–103. [Google Scholar] [CrossRef]
- Buzdar, S.A.; Jabeen, S.; Iqbal, K. Review on the feasibility of using PRESAGE® dosimeter in various radiotherapy techniques. J. Radiother. Pract. 2021, 20, 230–237. [Google Scholar]
- ur Rehman, J.; Isa, M.; Ahmad, N.; Gilani, Z.A.; Chow, J.C.; Afzal, M.; Ibbott, G.S. Quality assurance of volumetric-modulated arc therapy head and neck cancer treatment using PRESAGE® dosimeter. J. Radiother. Pract. 2018, 17, 441–446. [Google Scholar] [CrossRef]
- Costa, F.; Menten, M.J.; Doran, S.; Adamovics, J.; Hanson, I.M.; Nill, S.; Oelfke, U. Dose verification of dynamic MLC-tracked radiotherapy using small PRESAGE® 3D dosimeters and a motion phantom. J. Phys. Conf. Ser. 2019, 1305, 012068. [Google Scholar] [CrossRef]
- Tajaldeen, A.; Alghamdi, S. Investigation of dosimetric impact of organ motion in static and dynamic conditions for three stereotactic ablative body radiotherapy techniques: 3D conformal radiotherapy, intensity modulated radiation therapy, and volumetric modulated arc therapy by using PRESAGE 3D dosimeters. Exp. Oncol. 2019, 41, 153–159. [Google Scholar]
- Na, Y.H.; Wang, Y.F.; Black, P.J.; Velten, C.; Qian, X.; Lin, S.C.; Adamovics, J.; Wuu, C.S. Dosimetric and geometric characteristics of a small animal image-guided irradiator using 3D dosimetry/optical CT scanner. Med. Phys. 2018, 45, 3330–3339. [Google Scholar] [CrossRef]
- Xu, A.Y.; Wang, Y.-F.; Admovics, J.; Wuu, C.-S. Assessing CBCT-based patient positioning accuracy on the Gamma Knife IconTM via Presage® 3D absolute dosimetry. J. Phys. Conf. Ser. 2019, 1305, 012026. [Google Scholar] [CrossRef]
- Wuu, C.-S.; Wang, Y.-F.; Xu, A.Y.; Adamovics, J. Pre-clinical and small field dosimetry. J. Phys. Conf. Ser. 2019, 1305, 012023. [Google Scholar] [CrossRef]
- Ibbott, G.S.; Le, H.J.; Roe, Y. The MD Anderson experience with 3D dosimetry and an MR-linac. J. Phys. Conf. Ser. 2019, 1305, 012011. [Google Scholar] [CrossRef]
- Sakhalkar, H.; Sterling, D.; Adamovics, J.; Ibbott, G.; Oldham, M. Investigation of the feasibility of relative 3D dosimetry in the Radiologic Physics Center Head and Neck IMRT phantom using Presage/optical-CT. Med. Phys. 2009, 36, 3371–3377. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, K.; Ibbott, G.S.; Lafratta, R.G.; Gifford, K.A.; Akram, M.; Buzdar, S.A. Dosimetric feasibility of an anthropomorphic three-dimensional PRESAGE® dosimeter for verification of single entry hybrid catheter accelerated partial breast brachytherapy. J. Radiother. Pract. 2018, 17, 403–410. [Google Scholar] [CrossRef]
- Iqbal, K.; Gifford, K.A.; Ibbott, G.; Grant, R.L.; Buzdar, S.A. Comparison of an anthropomorphic PRESAGE® dosimeter and radiochromic film with a commercial radiation treatment planning system for breast IMRT: A feasibility study. J. Appl. Clin. Med. Phys. 2014, 15, 363–374. [Google Scholar] [CrossRef]
- Collins, C.; Kodra, J.; Yoon, S.W.; Coakley, R.; Adamovics, J.; Oldham, M. Preliminary investigation of a reusable radiochromic sheet for radiation dosimetry. J. Phys. Conf. Ser. 2019, 1305, 012032. [Google Scholar] [CrossRef]
- Thomas, A.; Yan, H.; Oldham, M.; Juang, T.; Adamovics, J.; Yin, F. The effect of motion on IMRT–looking at interplay with 3D measurements. J. Phys. Conf. Ser. 2013, 444, 012049. [Google Scholar] [CrossRef]
- Thomas, A.; Niebanck, M.; Juang, T.; Wang, Z.; Oldham, M. A comprehensive investigation of the accuracy and reproducibility of a multitarget single isocenter VMAT radiosurgery technique. Med. Phys. 2013, 40, 121725. [Google Scholar] [CrossRef]
- Rehman, J.; Iqbal, T.; Tailor, R.; Majid, A.; Ashraf, J.; Khan, I.; Afzal, M.; Ibbott, G. Dosimetric comparison among different head and neck radiotherapy techniques using PRESAGE® dosimeter. Int. J. Cancer Oncol. 2015, 3, 349. [Google Scholar] [CrossRef][Green Version]
- Touch, M.; Wu, Q.; Oldham, M. SU-E-J-80: Interplay Effect Between VMAT Intensity Modulation and Tumor Motion in Hypofractioned Lung Treatment, Investigated with 3D Pressage Dosimeter. Med. Phys. 2014, 41, 173–174. [Google Scholar] [CrossRef]
- Tello, V.; Tailor, R.; Hanson, W. How water equivalent are water-equivalent solid materials for output calibration of photon and electron beams? Med. Phys. 1995, 22, 1177–1189. [Google Scholar] [CrossRef]
- Klawikowski, S.J.; Yang, J.N.; Adamovics, J.; Ibbott, G.S. PRESAGE 3D dosimetry accurately measures Gamma Knife output factors. Phys. Med. Biol. 2014, 59, N211. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Tailor, R.; Ibbott, G.; Lampe, S.; Bivens Warren, W.; Tolani, N. Dosimetric characterization of a brachytherapy source by thermoluminescence dosimetry in liquid water. Med. Phys. 2008, 35, 5861–5868. [Google Scholar] [CrossRef] [PubMed]
- Nath, R.; Anderson, L.L.; Luxton, G.; Weaver, K.A.; Williamson, J.F.; Meigooni, A.S. Dosimetry of interstitial brachytherapy sources: Recommendations of the AAPM Radiation Therapy Committee Task Group No. 43. Med. Phys. 1995, 22, 209–234. [Google Scholar] [CrossRef] [PubMed]
- Vidovic, A.; Juang, T.; Meltsner, S.; Adamovics, J.; Chino, J.; Steffey, B.; Craciunescu, O.; Oldham, M. An investigation of a PRESAGE® in vivo dosimeter for brachytherapy. Phys. Med. Biol. 2014, 59, 3893. [Google Scholar] [CrossRef][Green Version]
- Gorjiara, T.; Hill, R.; Kuncic, Z.; Baldock, C. Water equivalency evaluation of PRESAGE® dosimeters for dosimetry of Cs-137 and Ir-192 brachytherapy sources. J. Phys. Conf. Ser. 2010, 250, 012093. [Google Scholar] [CrossRef]
- Gifford, K.A.; Iqbal, K.; Grant, R.L.; Buzdar, S.A.; Ibbott, G.S. Dosimetric verification of a commercial brachytherapy treatment planning system for a single Entry APBI Hybrid Catheter Device by PRESAGE® and Radiochromic Film. Brachytherapy 2013, 12, 11–77. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Effective Atomic Number (Zeff) | Low-Energy Cross-Section Deviation from Water | High Energy Cross-Section Deviation from Water | |
|---|---|---|---|---|
| Water | 3.3428 | 7.417 | - | - |
| PRESAGE (original) [72] | 3.2826 | 8.650 | 81% | <5% |
| PRESAGE (Formulation A) [84] | 3.2669 | 7.688 | 40% | 3% |
| PRESAGE (Formulation B) [84] | 3.2754 | 7.740 | 49% | 4% |
| PRESAGE (Formulation C) [84] | 3.2670 | 8.652 | 117% | 2% |
| PRESAGE (Iodoform) [93] | 3.2611 | 16.03 | 96% | <4% |
| PRESAGE (MOD3) [92] | 3.2768 | 7.416 | <18% | N/A (small) |
| PRESAGE (DBTDL) [90] | N/A | N/A | 2% | N/A (small) |
| PRESAGE (Bromine-based RI, F2) [94] | 3.4420 | 7.425 | 8% | N/A (small) |
| PRESAGE (Bromine-based RI, F5) [94] | 3.6580 | 9.657 | >50% | N/A (small) |
| Material | Density (g/cm3) | Effective Atomic Number (Zeff) | Slope Value (Sensitivity, Gy−1) |
|---|---|---|---|
| PRESAGE (LMG) [100] | 1.048 | 7.45 | 0.00890 |
| PRESAGE (MeO-LMG) [100] | 1.052 | 7.46 | 0.01802 |
| PRESAGE (Cl-LMG) [100] | 1.054 | 7.50 | 0.03027 |
| PRESAGE (Br-LMG) [100] | 1.057 | 8.10 | 0.04018 |
| PRESAGE (Bi Neo) [91] | 1.085 | 7.90 | 0.00787 |
| PRESAGE (DBTDL) [91] | 1.084 | 7.65 | 0.00681 |
| PRESAGE (Zn OCT) [91] | 1.083 | 7.49 | 0.00658 |
| PRESAGE (Iodoform) [93] | 1.047 | 16.03 | 0.02333 |
| PRESAGE (Bromoform) [93] | 1.076 | 9.96 | 0.01616 |
| PRESAGE (Chloroform) [93] | 1.102 | 6.62 | 0.00570 |
| PRESAGE (Organometallic catalyst) [75] | 1.100 | 7.72 | 0.01400 |
| PRESAGE (MOD 1) [92] | 1.039 | 7.410 | 0.00557 |
| PRESAGE (MOD 2) [92] | 1.042 | 7.415 | 0.00646 |
| PRESAGE (MOD 3) [92] | 1.044 | 7.416 | 0.00722 |
| PRESAGE (tartrazine) [98] | N/A | 11.100 | 0.10100 |
| PRESAGE (bromine-based RI, F5) [94] | 1.135 | 9.657 | 0.11090 |
| PRESAGE (bromine-based RI, F2) [94] | 1.058 | 7.380 | 0.02440 |
| Material | Dose Range | Correlation Coefficient |
|---|---|---|
| PRESAGE (LMG) [100] | 0 Gy–30 Gy | 0.9946 |
| PRESAGE (MeO-LMG) [100] | 0 Gy–30 Gy | 0.9963 |
| PRESAGE (Cl-LMG) [100] | 0 Gy–30 Gy | 0.9985 |
| PRESAGE (Br-LMG) [100] | 0 Gy–30 Gy | 0.9997 |
| PRESAGE (Bi Neo) [91] | 0 Gy–30 Gy | 0.9999 |
| PRESAGE (DBTDL) [91] | 0 Gy–30 Gy | 0.9999 |
| PRESAGE (Zn OCT) [91] | 0 Gy–30 Gy | 0.9999 |
| PRESAGE (Iodoform) [93] | 0 Gy–30 Gy | 0.9988 |
| PRESAGE (Bromoform) [93] | 0 Gy–30 Gy | 0.9996 |
| PRESAGE (Chloroform) [93] | 0 Gy–30 Gy | 0.9980 |
| PRESAGE (Organometallic catalyst) [75] | 0 Gy–20 Gy | 0.9700 |
| PRESAGE (MOD 1) [92] | 0 Gy–50 Gy | 0.9984 |
| PRESAGE (MOD 2) [92] | 0 Gy–50 Gy | 0.9993 |
| PRESAGE (MOD 3) [92] | 0 Gy–50 Gy | 0.9989 |
| PRESAGE (deoxygenation) [104] | 0 Gy–30 Gy | 0.9981 |
| PRESAGE (no deoxygenation) [104] | 0 Gy–30 Gy | 0.9972 |
| Material | Rate of Optical Clearing | Reusability | Reproducibility |
|---|---|---|---|
| PRESAGEREU [117] | >12 days | 5 times | 80% |
| PRESAGE® [119] | 14 days | N/A | N/A |
| PRESAGE-RU [118] | 5–7 days | 5 times | 60% |
| PRESAGE-RU [120] | 10 days | 3 times | 66% |
| PRESAGEREU (room temperature) [107] | 2 days | 2 times | 50% |
| PRESAGEREU (low temperature) [107] | 2 days | 3 times | 75% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohyedin, M.Z.; Zin, H.M.; Adenan, M.Z.; Abdul Rahman, A.T. A Review of PRESAGE Radiochromic Polymer and the Compositions for Application in Radiotherapy Dosimetry. Polymers 2022, 14, 2887. https://doi.org/10.3390/polym14142887
Mohyedin MZ, Zin HM, Adenan MZ, Abdul Rahman AT. A Review of PRESAGE Radiochromic Polymer and the Compositions for Application in Radiotherapy Dosimetry. Polymers. 2022; 14(14):2887. https://doi.org/10.3390/polym14142887
Chicago/Turabian StyleMohyedin, Muhammad Zamir, Hafiz Mohd Zin, Mohd Zulfadli Adenan, and Ahmad Taufek Abdul Rahman. 2022. "A Review of PRESAGE Radiochromic Polymer and the Compositions for Application in Radiotherapy Dosimetry" Polymers 14, no. 14: 2887. https://doi.org/10.3390/polym14142887
APA StyleMohyedin, M. Z., Zin, H. M., Adenan, M. Z., & Abdul Rahman, A. T. (2022). A Review of PRESAGE Radiochromic Polymer and the Compositions for Application in Radiotherapy Dosimetry. Polymers, 14(14), 2887. https://doi.org/10.3390/polym14142887