Assessing the Sustainability and Acceptance Rate of Cost-Effective Household Water Treatment Systems in Rural Communities of Makwane Village, South Africa


Abstract
:1. Introduction
2. Materials and Methodology
2.1. Ethical
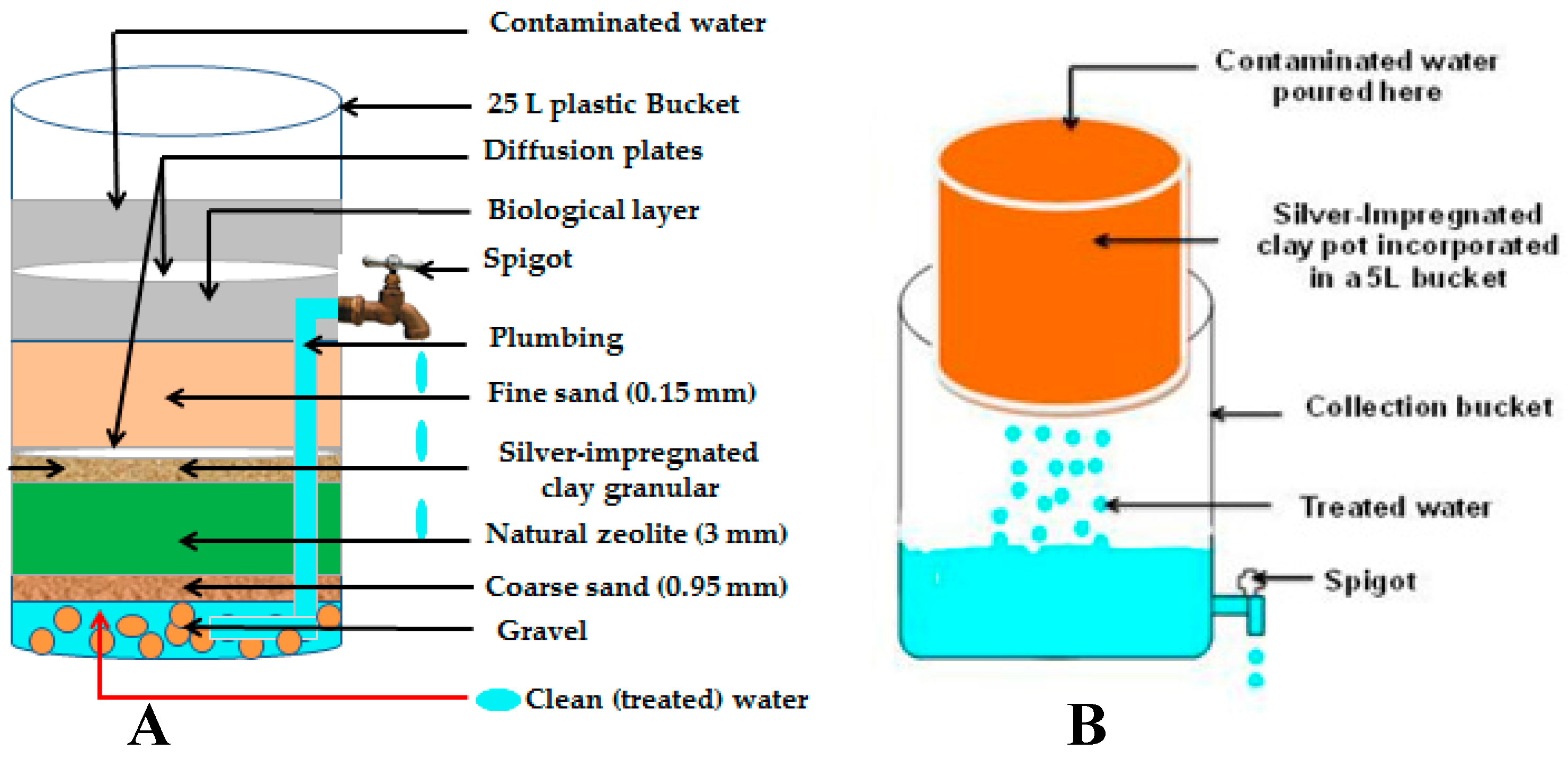
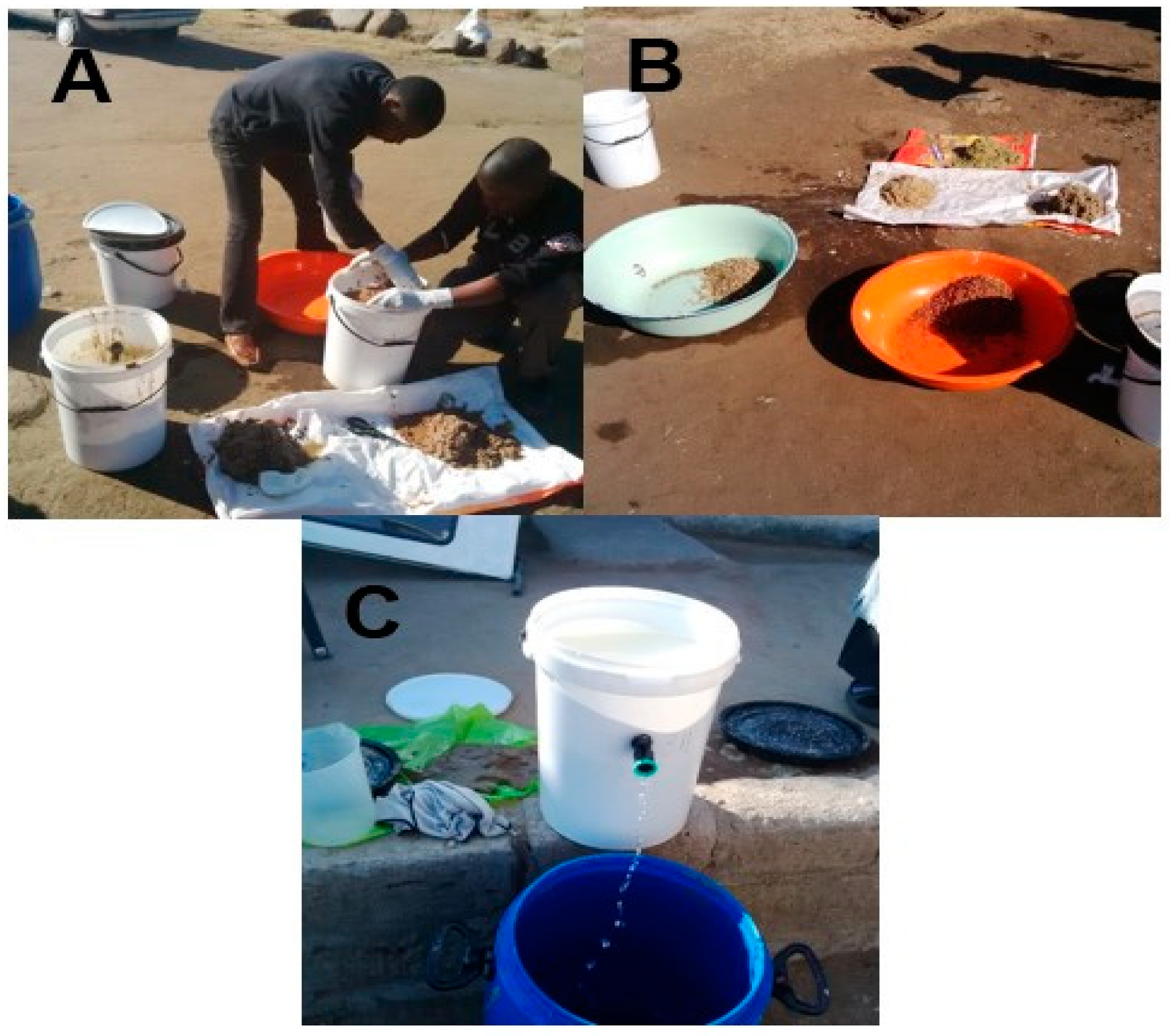
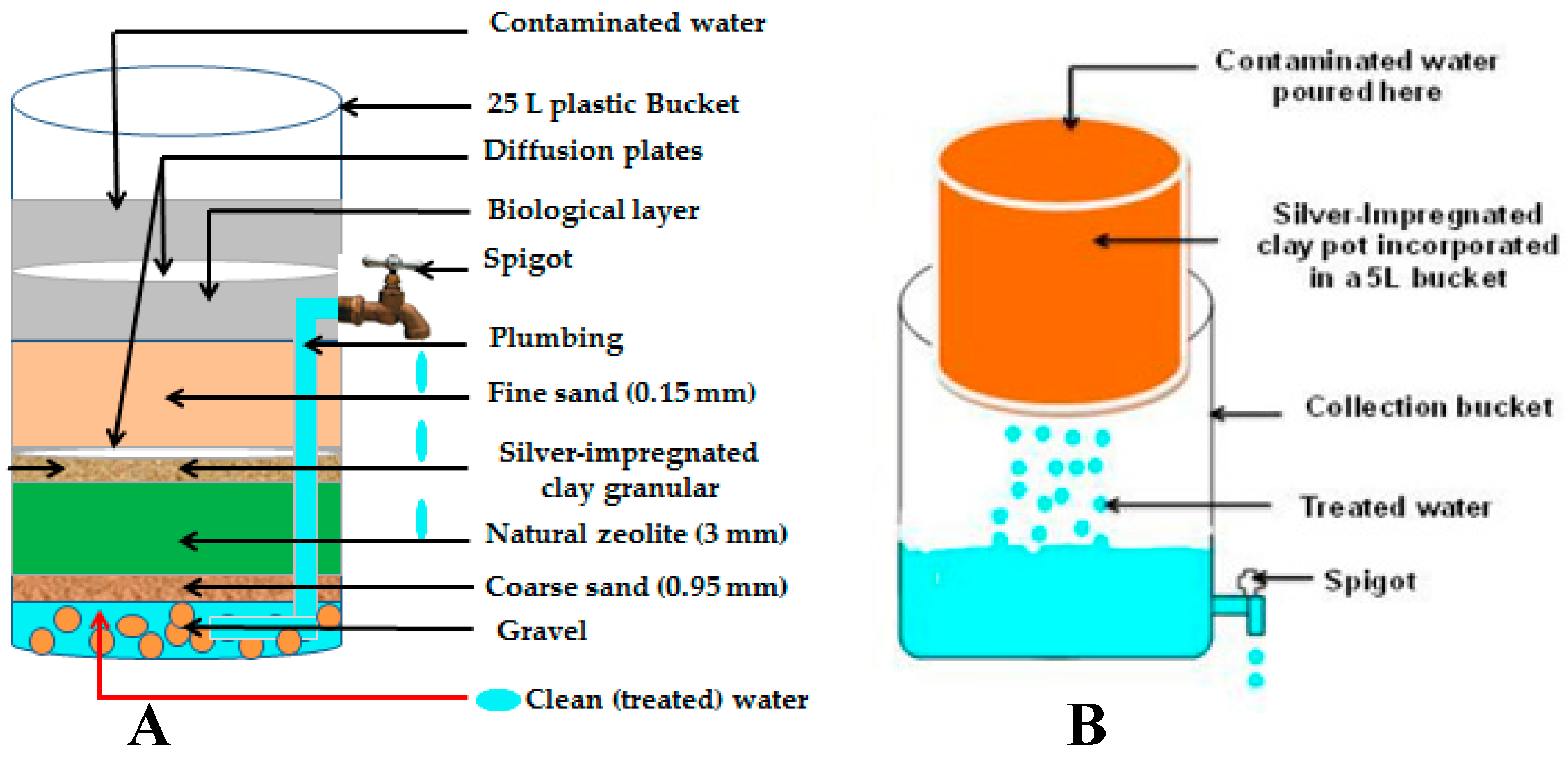
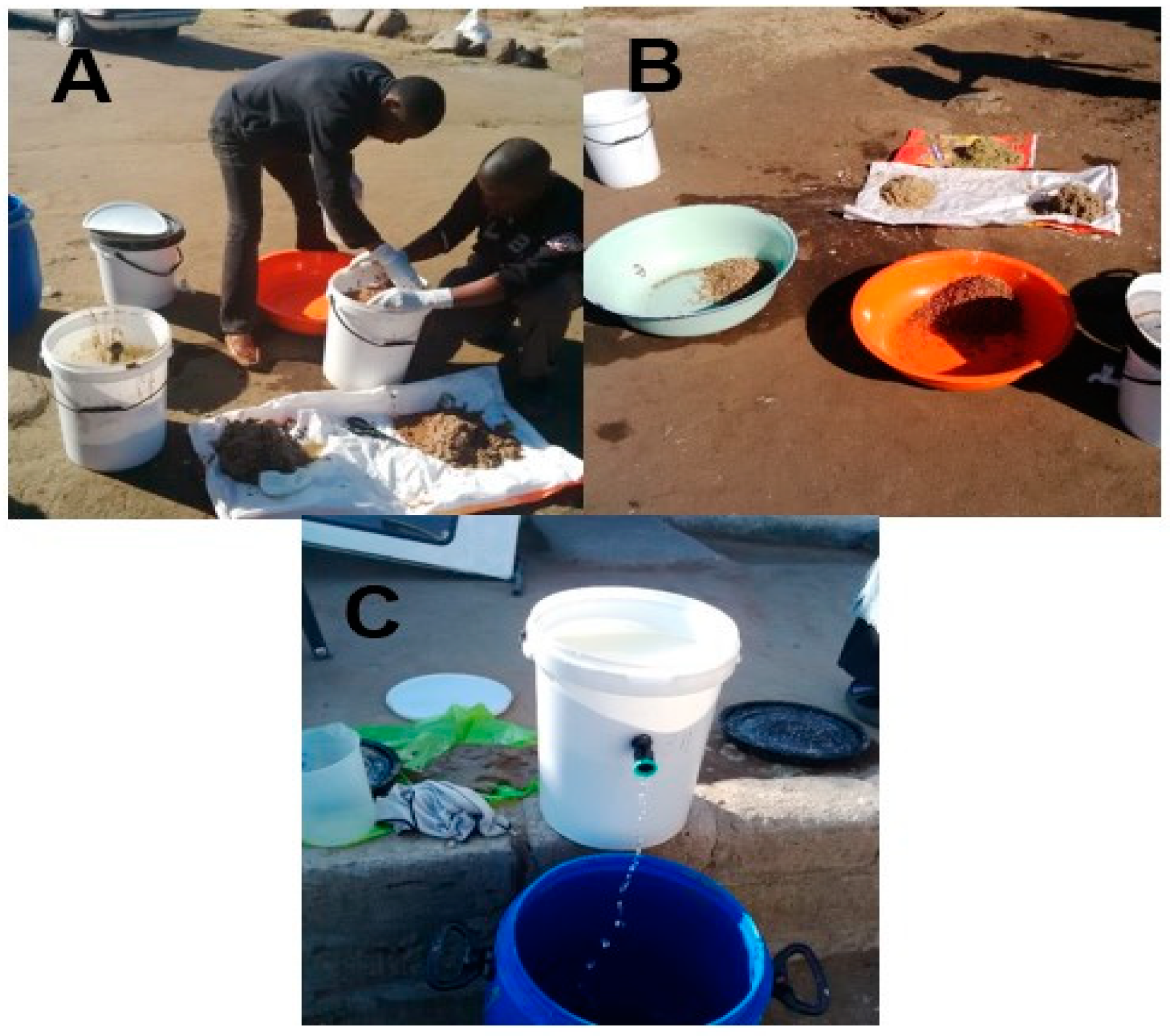
2.2. Household Water Treatment Systems Description
2.3. Data Collection
2.4. Water Quality Assessment
3. Results
3.1. Level of Education in Makwane Community during the Study Period
3.2. Level of Employment in Makwane Community during the Study Period
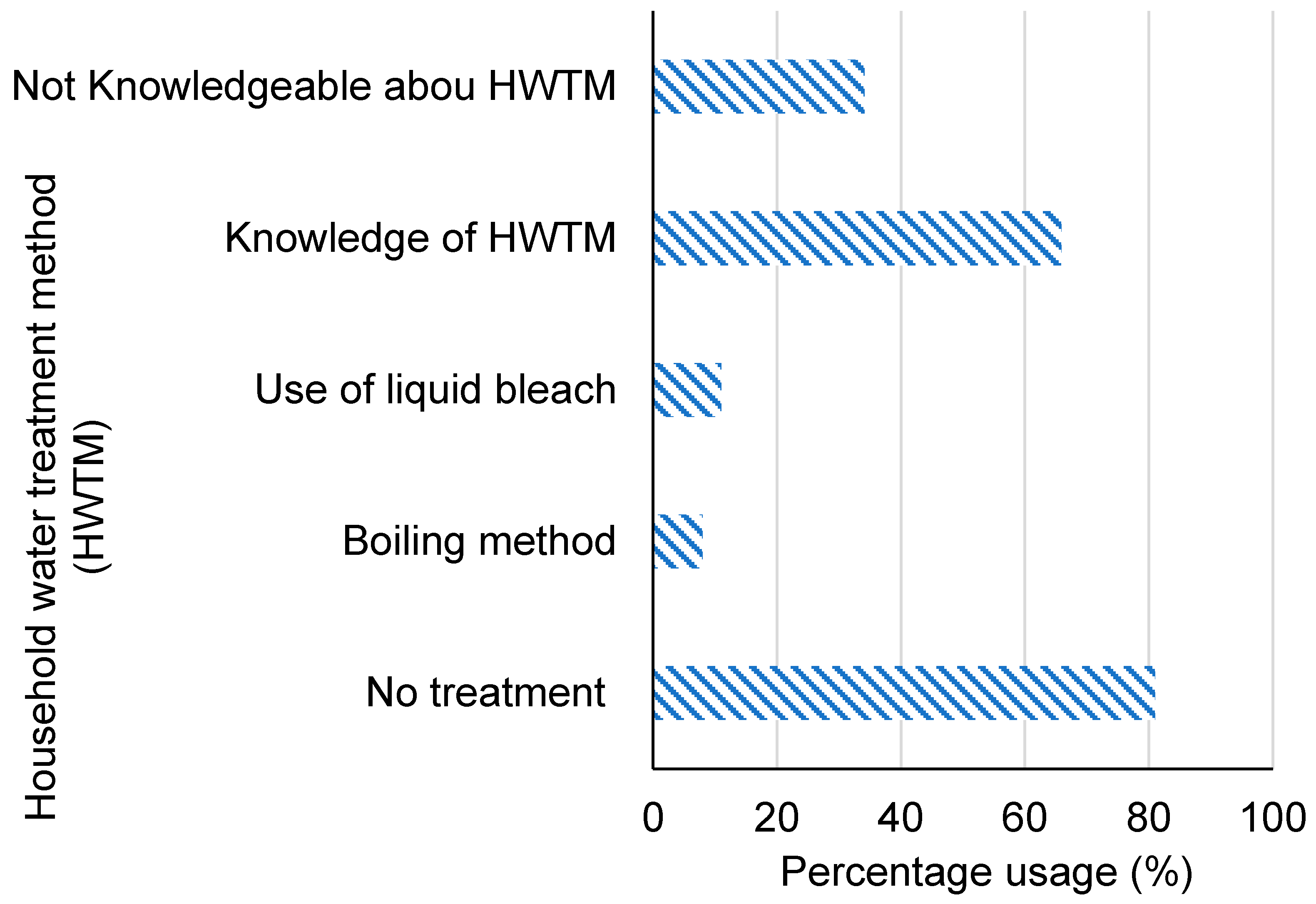
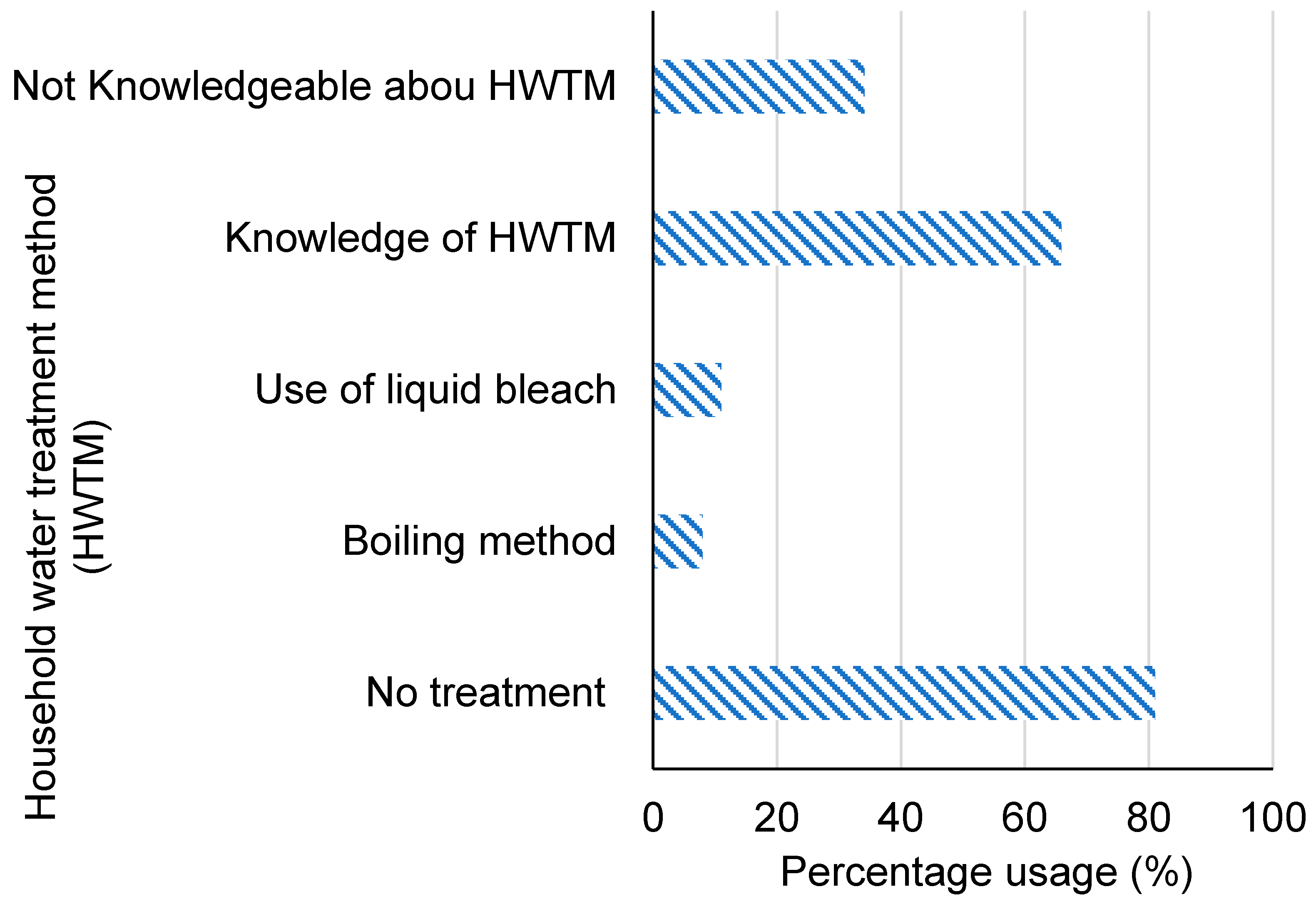
3.3. Knowledge of Water Treatment Methods and Practice in Makwane Village Prior to the Implementation of HWTS
3.4. Relationship between the Knowledge of Water Treatment Methods and Selected Demographic Profiles Prior to Implementation
3.4.1. Number of Household Water Treatment Systems in Use during the Study Period and Reasons for Not Being in Use for the Determination of Acceptance Rate
3.4.2. Survey Subsequent to the Implementation of the HWTS Devices in Makwane Village for the Determination of Acceptance and Adoption Rates
3.5. Long-Term Effectiveness of the HWTS Based on Their Performance
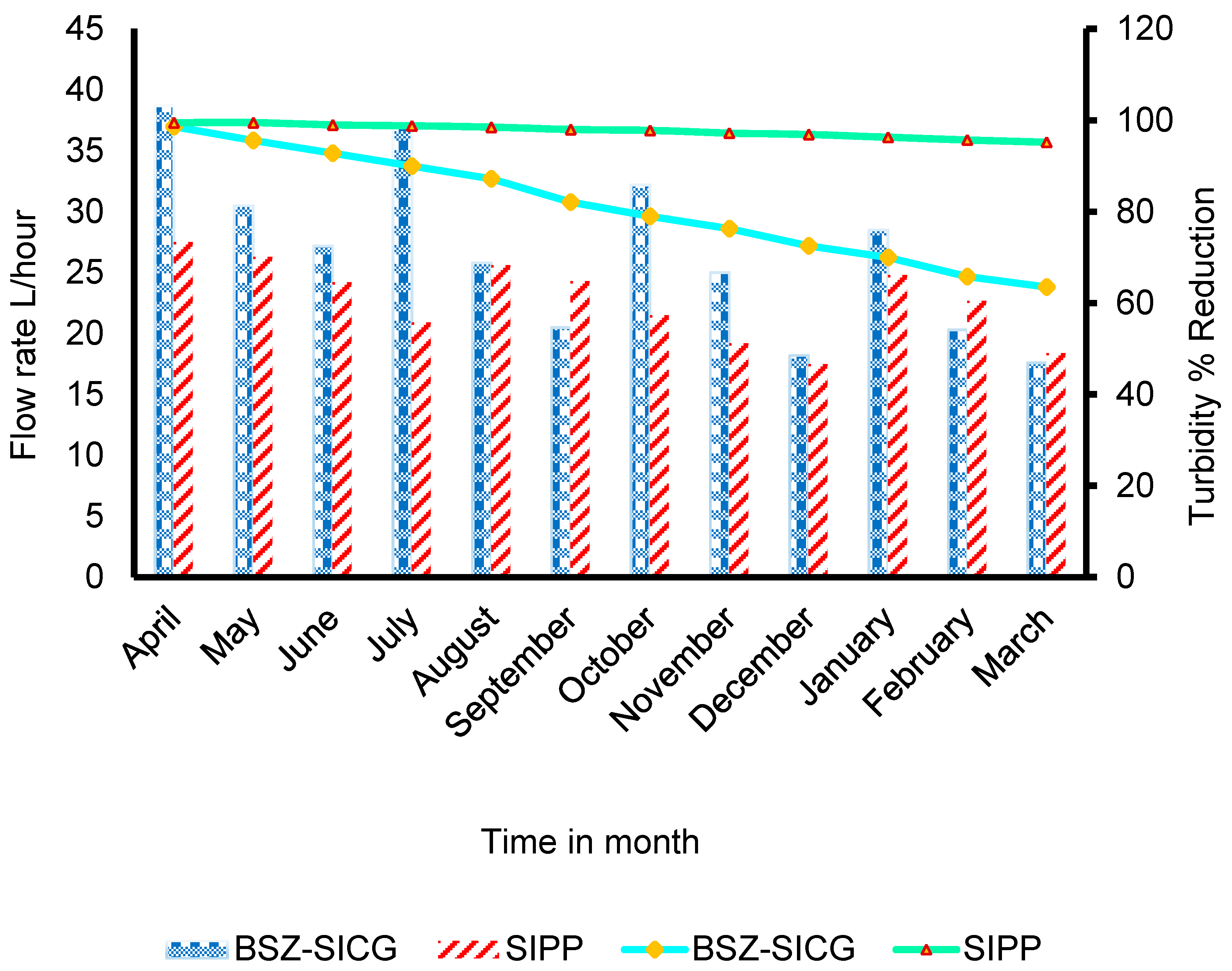
3.5.1. Long-Term Effectiveness Based on the Flow Rate and Turbidity Removal
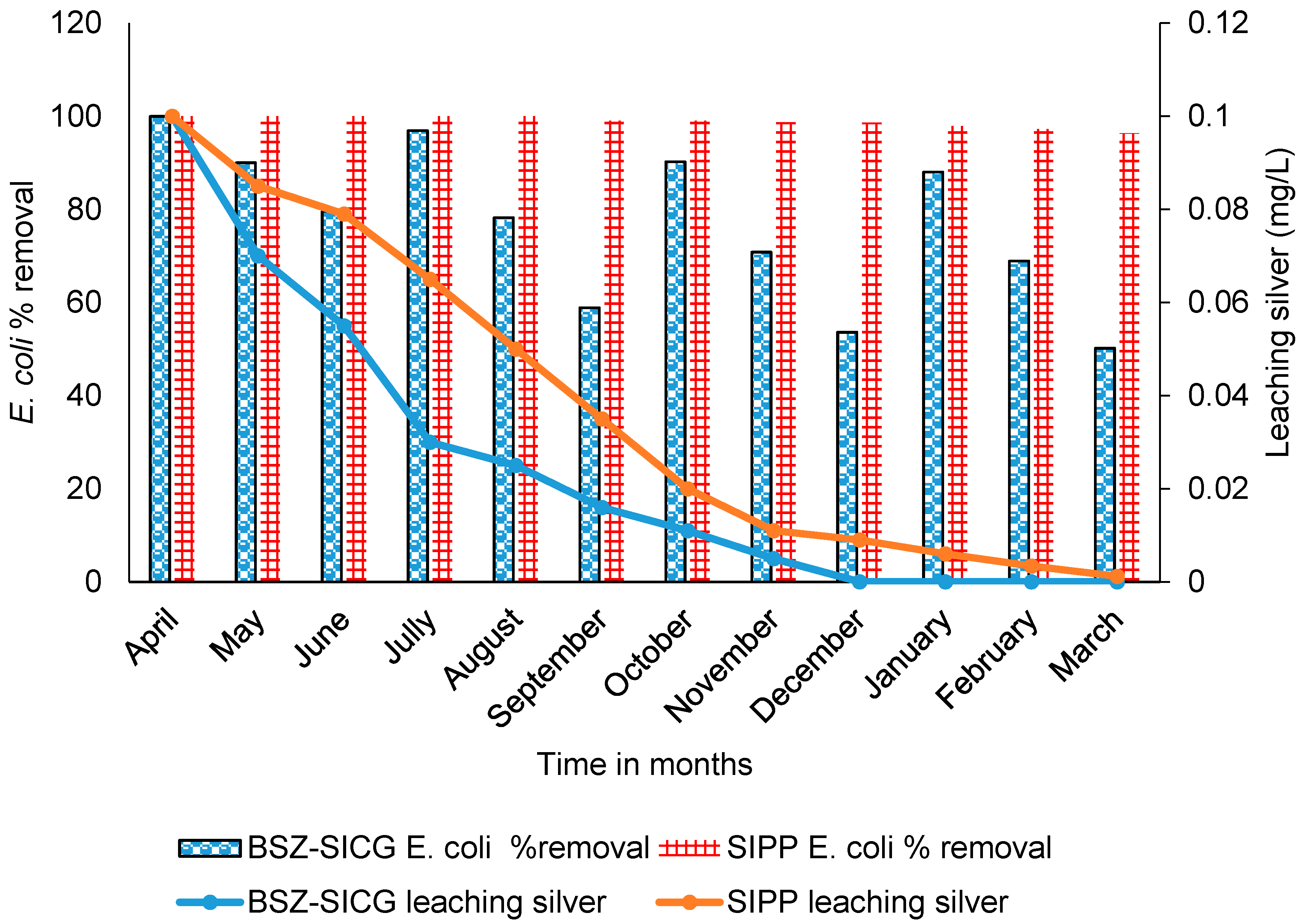
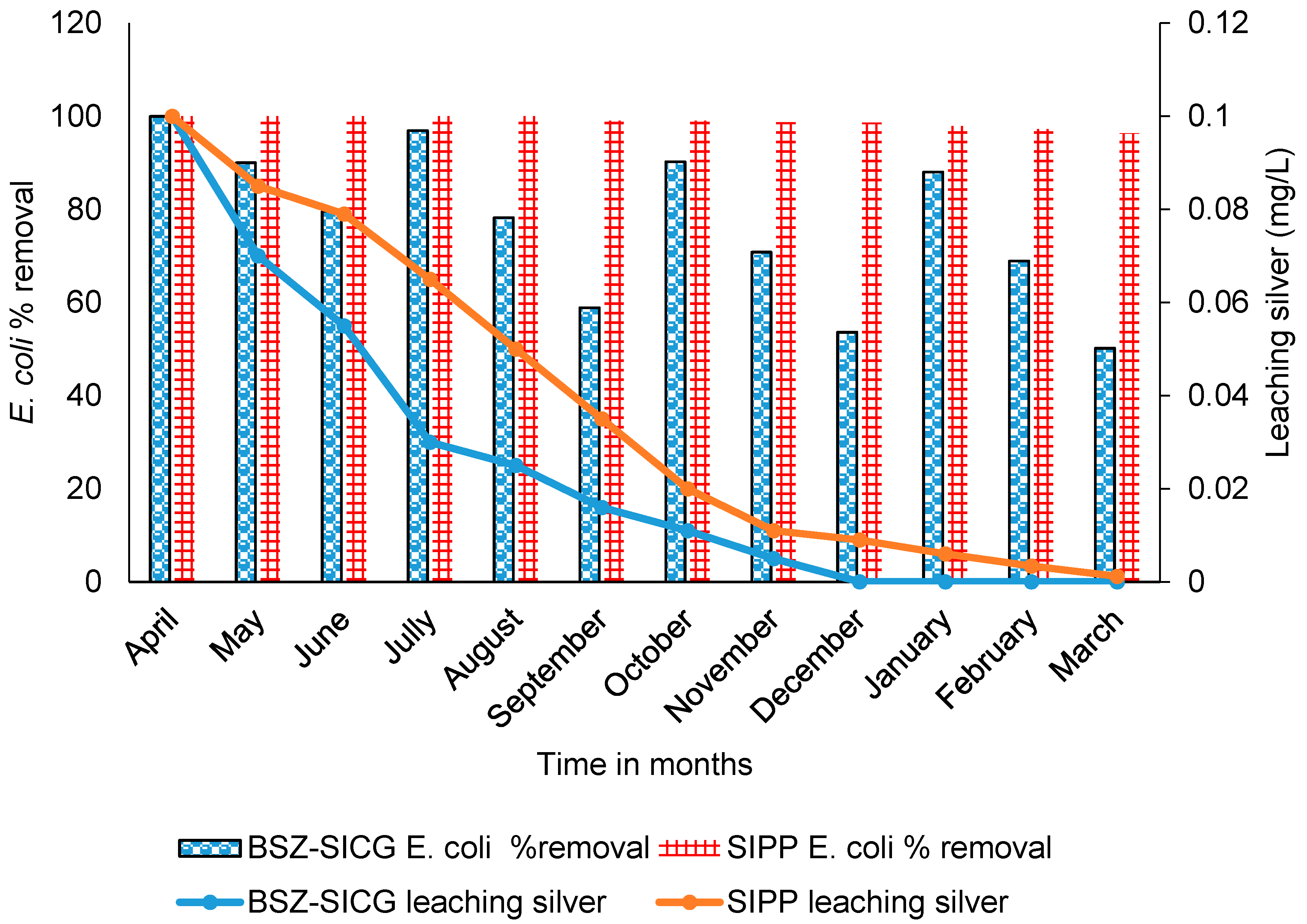
3.5.2. Long-Term Effectiveness Based on the E. coli Removal Efficiency and Leaching of Silver in Treated Water
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ojomo, E.; Elliott, M.; Goodyear, L.; Forson, M.; Bartram, J. Effectiveness and scale-up of household water treatment and safe storage practices: Enablers and barriers to effective implementation. Int. J. Hyg. Environ. Health 2015, 8, 704–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Fact Sheet, Drinking Water; World Health Organization: Geneva, Switzeland, 2018. [Google Scholar]
- Craun, M.F.; Craun, G.F.; Calderon, R.L.; Beach, M.J. Waterborne outbreaks reported in the United States. J. Water Health 2006, 4, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Bessong, P.O.; Odiyo, J.O.; Musekene, J.N.; Tessema, A. Spatial distribution of diarrhoea and microbial quality of domestic water during an outbreak of diarrhoea in the Tshikuwi community in Venda, South Africa. J. Health. Popul. Nutr. 2009, 27, 652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allam, R.R.; Uthappa, C.K.; Nalini, C.; Udaragudi, P.R.; Tadi, G.P.; Murhekar, M. V An outbreak of cholera due to contaminated water, Medak District, Andhra Pradesh, India, 2013. Indian J. Community Med. Off. Publ. Indian Assoc. Prev. Soc. Med. 2015, 40, 283. [Google Scholar]
- Momtaz, H.; Dehkordi, F.S.; Rahimi, E.; Asgarifar, A. Detection of Escherichia coli, Salmonella species, and Vibrio cholerae in tap water and bottled drinking water in Isfahan, Iran. BMC Public Health 2013, 13, 556. [Google Scholar] [CrossRef] [Green Version]
- Diouf, K.; Tabatabai, P.; Rudolph, J.; Marx, M. Diarrhoea prevalence in children under five years of age in rural Burundi: An assessment of social and behavioural factors at the household level. Glob. Health Action 2014, 7, 24895. [Google Scholar] [CrossRef]
- Ezeh, O.; Agho, K.; Dibley, M.; Hall, J.; Page, A. The impact of water and sanitation on childhood mortality in Nigeria: Evidence from demographic and health surveys, 2003–2013. Int. J. Environ. Res. Public Health 2014, 11, 9256–9272. [Google Scholar] [CrossRef] [Green Version]
- Ding, Z.; Zhai, Y.; Wu, C.; Wu, H.; Lu, Q.; Lin, J.; He, F. Infectious diarrheal disease caused by contaminated well water in Chinese schools: A systematic review and meta-analysis. J. Epidemiol. 2017, 27, 274–281. [Google Scholar] [CrossRef]
- World Health Organization (WHO) WASH (Water, Sanitation & Hygiene) and COVID-19; Water, Sanitation, Hygiene, and Waste Management for SARS-CoV-2, the Virus that Causes COVID-19. 2020. Ref. no. WHO/2019-nCoV/IPC_WASH/2020.4. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-IPC-WASH-2020.4 (accessed on 26 September 2020).
- Steele, A.; Clarke, B.; Watkins, O. Impact of jerry can disinfection in a camp environment–experiences in an IDP camp in Northern Uganda. J. Water Health 2008, 6, 559–564. [Google Scholar] [CrossRef] [Green Version]
- Rufener, S.; Mäusezahl, D.; Mosler, H.-J.; Weingartner, R. Quality of drinking-water at source and point-of-consumption—Drinking cup as a high potential recontamination risk: A field study in Bolivia. J. Health. Popul. Nutr. 2010, 28, 34. [Google Scholar] [CrossRef]
- García-Betancourt, T.; Higuera-Mendieta, D.R.; González-Uribe, C.; Cortés, S.; Quintero, J. Understanding water storage practices of urban residents of an endemic dengue area in Colombia: Perceptions, rationale and socio-demographic characteristics. PLoS ONE 2015, 10, e0129054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Healy-Profitós, J.; Lee, S.; Mouhaman, A.; Garabed, R.; Moritz, M.; Piperata, B.; Lee, J. Neighborhood diversity of potentially pathogenic bacteria in drinking water from the city of Maroua, Cameroon. J. Water Health 2016, 14, 559–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Too, J.K.; Kipkemboi Sang, W.; Ng’ang’a, Z.; Ngayo, M.O. Fecal contamination of drinking water in Kericho District, Western Kenya: Role of source and household water handling and hygiene practices. J. Water Health 2016, 14, 662–671. [Google Scholar] [CrossRef] [PubMed]
- Assembly, C. Constitution of the Republic of South Africa, 1996 (Act 108 of 1996). Pretoria Gov. Print. 1996. Available online: http://www.gov.za/aboutsa/people.htm (accessed on 26 September 2020).
- Isa, M. Heading for Murky Waters. FinWeek; Fin24, South Africa. 2016. Available online: https://www.news24.com/fin24/finweek/featured/heading-for-murky-waters-20161124 (accessed on 26 September 2020).
- WHO/UNICEF. Progress on Sanitation and Drinking Water—2015 Update and MDG Assessment; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- StatSA. The State of Basic Service Delivery in South Africa: In-Depth Analysis of the Community Survey 2016 Data, Report 03-01-22/; Pretoria Gov. Print, South Africa. 2016. Available online: http://www.statssa.gov.za/publications/Report%2003-01-22/Report%2003-01-222016.pdf (accessed on 26 September 2020).
- UNDP. Sustainable Development Goals (SDGs). Goal 6: Ensure Access to Water and Sanitation for All. New York, NY, USA, 2015. Available online: https://www.un.org/sustainabledevelopment/water-and-sanitation/ (accessed on 26 September 2020).
- Momba, M.N.B.; Offringa, G.; Nameni, G.; Brouckaert, B. Development of a Prototype Nanotechnology-Based Clay Filter Pot to Purify Water for Drinking and Cooking in Rural Homes; WRC Report No. KV 244/10; Water Research Commission: Pretoria, South Africa, 2010; pp. 27–32. [Google Scholar]
- Mwabi, J.K.; Adeyemo, F.E.; Mahlangu, T.O.; Mamba, B.B.; Brouckaert, B.M.; Swartz, C.D.; Offringa, G.; Mpenyana-Monyatsi, L.; Momba, M.N.B. Household water treatment systems: A solution to the production of safe drinking water by the low-income communities of Southern Africa. Phys. Chem. Earth Parts A/B/C 2011, 36, 1120–1128. [Google Scholar] [CrossRef]
- Mahlangu, T.O.; Mamba, B.B.; Momba, M.N.B. A comparative assessment of chemical contaminant removal by three household water treatment filters. Water SA 2012, 38, 39–48. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.; Clasen, T. High adherence is necessary to realize health gains from water quality interventions. PLoS ONE 2012, 7, e36735. [Google Scholar] [CrossRef] [Green Version]
- Hunter, P.R. Household water treatment in developing countries: Comparing different intervention types using meta-regression. Environ. Sci. Technol. 2009, 43, 8991–8997. [Google Scholar] [CrossRef]
- Moropeng, R.; Budeli, P.; Mpenyana-Monyatsi, L.; Momba, M. Dramatic Reduction in Diarrhoeal Diseases through Implementation of Cost-Effective Household Drinking Water Treatment Systems in Makwane Village, Limpopo Province, South Africa. Int. J. Environ. Res. Public Health 2018, 15, 410. [Google Scholar] [CrossRef] [Green Version]
- Brözel, V.S.; Cloete, T.E. Effect of Storage Time and Temperature on the Aerobic Plate Count and on the Community Structure of Two Water Samples; Institutional Repository of the University of Pretoria, South Africa. 1991. Available online: http://hdl.handle.net/2263/4198 (accessed on 26 September 2020).
- Wolf, J.; Prüss-Ustün, A.; Cumming, O.; Bartram, J.; Bonjour, S.; Cairncross, S.; Clasen, T.; Colford, J.M., Jr.; Curtis, V.; De France, J. Systematic review: Assessing the impact of drinking water and sanitation on diarrhoeal disease in low-and middle-income settings: Systematic review and meta-regression. Trop. Med. Int. Health 2014, 19, 928–942. [Google Scholar] [CrossRef]
- Makutsa, P.; Nzaku, K.; Ogutu, P.; Barasa, P.; Ombeki, S.; Mwaki, A.; Quick, R.E. Challenges in implementing a point-of-use water quality intervention in rural Kenya. Am. J. Public Health 2001, 91, 1571–1573. [Google Scholar] [CrossRef] [PubMed]
- Luby, S.P.; Mendoza, C.; Keswick, B.H.; Chiller, T.M.; Hoekstra, R.M. Difficulties in bringing point-of-use water treatment to scale in rural Guatemala. Am. J. Trop. Med. Hyg. 2008, 78, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Arnold, B.; Arana, B.; Mäusezahl, D.; Hubbard, A.; Colford, J.M., Jr. Evaluation of a pre-existing, 3-year household water treatment and handwashing intervention in rural Guatemala. Int. J. Epidemiol. 2009, 38, 1651–1661. [Google Scholar] [CrossRef] [PubMed]
- Firth, J.; Balraj, V.; Muliyil, J.; Roy, S.; Rani, L.M.; Chandresekhar, R.; Kang, G. Point-of-use interventions to decrease contamination of drinking water: A randomized, controlled pilot study on efficacy, effectiveness, and acceptability of closed containers, Moringa oleifera, and in-home chlorination in rural South India. Am. J. Trop. Med. Hyg. 2010, 82, 759–765. [Google Scholar] [CrossRef]
- Wright, J.A.; Cronin, A.; Okotto-Okotto, J.; Yang, H.; Pedley, S.; Gundry, S.W. A spatial analysis of pit latrine density and groundwater source contamination. Environ. Monit. Assess. 2013, 185, 4261–4272. [Google Scholar] [CrossRef]
- Clasen, T.; Schmidt, W.-P.; Rabie, T.; Roberts, I.; Cairncross, S. Interventions to improve water quality for preventing diarrhoea: Systematic review and meta-analysis. BMJ 2007, 334, 782. [Google Scholar] [CrossRef] [Green Version]
- Waddington, H.; Snilstveit, B. Effectiveness and sustainability of water, sanitation, and hygiene interventions in combating diarrhoea. J. Dev. Eff. 2009, 1, 295–335. [Google Scholar] [CrossRef]
- Cairncross, S.; Hunt, C.; Boisson, S.; Bostoen, K.; Curtis, V.; Fung, I.C.H.; Schmidt, W.-P. Water, sanitation and hygiene for the prevention of diarrhoea. Int. J. Epidemiol. 2010, 39, i193–i205. [Google Scholar] [CrossRef] [Green Version]
- Trevett, A.F.; Carter, R.C.; Tyrrel, S.F. The importance of domestic water quality management in the context of faecal–oral disease transmission. J. Water Health 2005, 3, 259–270. [Google Scholar] [CrossRef]
- Gundry, S.W.; Wright, J.A.; Conroy, R.; Du Preez, M.; Genthe, B.; Moyo, S.; Mutisi, C.; Ndamba, J.; Potgieter, N. Contamination of drinking water between source and point-of-use in rural households of South Africa and Zimbabwe: Implications for monitoring the Millennium Development Goal for water. Water Pract. Technol. 2006, 1. [Google Scholar] [CrossRef]
- Onabolu, B.; Jimoh, O.D.; Igboro, S.B.; Sridhar, M.K.C.; Onyilo, G.; Gege, A.; Ilya, R. Source to point of use drinking water changes and knowledge, attitude and practices in Katsina State, Northern Nigeria. Phys. Chem. Earth Parts A/B/C 2011, 36, 1189–1196. [Google Scholar] [CrossRef]
- Momba, M.N.B.; Tyafa, Z.; Makala, N. Rural water treatment plants fail to provide potable water to their consumers: The Alice water treatment plant in the Eastern Cape province of South Africa. S. Afr. J. Sci. 2004, 100, 307–310. [Google Scholar]
- Momba, M.N.B.; Notshe, T.L. The microbiological quality of groundwater-derived drinking water after long storage in household containers in a rural community of South Africa. J. Water Supply Res. Technol. 2003, 52, 67–77. [Google Scholar] [CrossRef]
- Budeli, P.; Moropeng, R.C.; Mpenyana-Monyatsi, L.; Momba, M.N.B. Inhibition of biofilm formation on the surface of water storage containers using biosand zeolite silver-impregnated clay granular and silver impregnated porous pot filtration systems. PLoS ONE 2018, 13, e0194715. [Google Scholar] [CrossRef] [Green Version]
- Mwabi, J.K.; Mamba, B.B.; Momba, M.M.B. Removal of waterborne bacteria from surface water and groundwater by cost-effective household water treatment systems (HWTS): A sustainable solution for improving water quality in rural communities of Africa. Water SA 2013, 39, 445–456. [Google Scholar] [CrossRef] [Green Version]
- Edokpayi, J.N.; Odiyo, J.O.; Msagati, T.; Potgieter, N. Temporal variations in physico-chemical and microbiological characteristics of Mvudi River, South Africa. Int. J. Environ. Res. Public Health. 2015, 12, 4128–4140. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N = 70 | ||
|---|---|---|
| Category | Frequency | Percentage |
| Primary school | 30 | 31.4 |
| Secondary/high school | 47 | 52.9 |
| Tertiary institution | 3 | 4.3 |
| None | 8 | 11.4 |
| N = 70 | |||
|---|---|---|---|
| Category | Frequency | Percentage | |
| Employed | Professional jobs | 3 | 4.3 |
| Non-professional jobs | 25 | 35.7 | |
| Unemployed | Social welfare grant | 38 | 54.3 |
| Other | 4 | 5.7 | |
| Variables | Knowledge of Boiling and Liquid Bleach Methods N = 70 | ||
|---|---|---|---|
| Age Group | Good | Fair | Poor |
| Frequency (%) | Frequency (%) | Frequency (%) | |
| 17–21 | 2 (22.1) | 1 (11.1) | 6 (66.7) |
| 22–26 | 8 (44.4) | 3 (16.7) | 7 (38.9) |
| 27–31 | 7 (50) | 2 (14.3) | 5 (35.7) |
| 32–36 | 12 (57) | 5 (24) | 4 (19) |
| ≥37 | 3 (37.5) | 1 (12.5) | 4 (50) |
| Level of education | |||
| Primary | 3 (12.5) | 3 (12.5) | 18(75) |
| Secondary/High school | 27 (71.1) | 8 (21.0) | 3 (7.9) |
| Tertiary level | 3 (100) | 0 (0) | 0 (0) |
| none | 2 (40) | 2 (40) | 1 (20) |
| Assessment Period | Bsz-Sicg Filters N = 35 | Sipp Filters N = 35 | Reason for Not in Use |
|---|---|---|---|
| April–June 2015 | 35 (100%) | 35 (100%) | N/A |
| July–September 2015 | 29 (82.9%) | 35 (97.1%) | BSZ-SICG: Water had bad smell. SIPP: Filters got damaged. |
| October–December 2015 | 16 (45.7%) | 22 (66.9%) | BSZ-SICG: Bad smell, no time for maintenance (time consuming), broken spigot. SIPP: Damaged. |
| January–March 2016 | 07 (20.0%) | 19 (54.3%) | BSZ-SICG: Bad smell, time consuming during maintenance, no time for treating water. SIPP: Damaged, flow rate too slow (time consuming). |
| Survey Questions | Participant’s Responds N = 70 | |
|---|---|---|
| How often do they treat their water with implemented HWTS? | When needed | 54 (77.1%) |
| On a daily basis | 4 (5.7%) | |
| Never | 12 (17.1%) | |
| How do they store treated water? | Improved storage container | 8 (11.4%) |
| Unimproved storage container | 11 (15.7%) | |
| Other | 51 (72.9%) | |
| How often do they wash the storage containers? | When dirty (visible dirt) | 56 (80%) |
| Once a week | 8 (11.4%) | |
| Never | 6 (8.6%) | |
| Are they willing to buy one of the HWTS? | Yes | 4 (5.7%) |
| No | 59 (84.3%) | |
| Not sure | 7 (10%) | |
| Time in Month | Influent Turbidity (NTU) | Effluent Turbidity (NTU) | |
|---|---|---|---|
| SIPP Filters | BSZ-SIGC Filters | ||
| April | 86.7 | 0.43 | 1.21 |
| May | 66.9 | 0.33 | 2.94 |
| June | 65.0 | 0.65 | 4.68 |
| July | 33 | 0.40 | 3.3 |
| August | 28.67 | 0.43 | 3.67 |
| September | 26.82 | 0.54 | 4.8 |
| October | 12.24 | 0.23 | 2.57 |
| November | 16.67 | 0.47 | 3.95 |
| December | 15.75 | 0.49 | 4.33 |
| January | 12.33 | 0.47 | 3.7 |
| February | 13.37 | 0.57 | 4.68 |
| March | 13.42 | 0.64 | 4.9 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moropeng, R.C.; Momba, M.N.B. Assessing the Sustainability and Acceptance Rate of Cost-Effective Household Water Treatment Systems in Rural Communities of Makwane Village, South Africa. Crystals 2020, 10, 872. https://doi.org/10.3390/cryst10100872
Moropeng RC, Momba MNB. Assessing the Sustainability and Acceptance Rate of Cost-Effective Household Water Treatment Systems in Rural Communities of Makwane Village, South Africa. Crystals. 2020; 10(10):872. https://doi.org/10.3390/cryst10100872
Chicago/Turabian StyleMoropeng, Resoketswe Charlotte, and Maggy Ndombo Benteke Momba. 2020. "Assessing the Sustainability and Acceptance Rate of Cost-Effective Household Water Treatment Systems in Rural Communities of Makwane Village, South Africa" Crystals 10, no. 10: 872. https://doi.org/10.3390/cryst10100872