Exergame Experience of Young and Old Individuals Under Different Difficulty Adjustment Methods

 , ,
, ,
Abstract
1. Introduction
2. Related Work
2.1. Purposing of Games for Health
2.2. Difficulty Adjustments in Exergames
3. Materials and Methods
3.1. Hypotheses
- Q1.
- Do traditional approaches fail to provide a satisfactory play experience?
- Q2.
- Do flow experience of young and old individuals differ from each other under similar exergaming conditions?
- Q3.
- Is there a difference between difficulty adjustment preference of young and old individuals?
- H1.
- Flow refers to an equilibrium between challenge presented by the game and respective skill set of players where maximum enjoyment is achieved. For example, in Wii Sports Tennis, players experience flow when the skill level of the non-playable characters (NPC) are on par with their own. Since controlling player skill is a mundane task, we achieve flow by adjusting game difficulty and modifying game elements such as NPC speed, health, gameplay duration, or power-up frequency. Traditional methods used for these adjustments follow a steady increase in difficulty, mostly in steps represented as game levels. Growth or amount of the adjustment depends on player’s self-assessment of his perceived skill and selection of difficulty from a given set of choices such as easy, normal, and hard. This schema causes a decline in flow and leads to a diminished gaming experience [18,46,47,50,62]. Accordingly we form our first hypothesis as follows: Constant difficulty will fail to provide a satisfactory exergaming experience compared to ramping, performance-based, and biofeedback-based difficulty adjustments.
- H2.
- Aging-related changes have become a central topic in exergame design for older individuals. As an example, diminished motor control and neural functions affect various aspects of designing exergame experiences for this specific target group. However, effects of these changes on difficulty adjustment preference are still not clearly defined. We think that technology experience and gaming perception of young and old generations differ significantly, which is likely to have a substantial effect on preferred level of difficulty. Combined with varying game preferences, we believe that exergaming experience of young and old generations will demonstrate a considerable amount of dissimilarity under same conditions. Based on this background, our second hypothesis is: Measured exergaming experience of the two age groups will show a significant difference based on Jackson and Marsh’s Flow State Scale (FSS) [67].
- H3.
- Based upon the first and second hypotheses, we predict significant differences between difficulty adjustment preference of the two age groups. Building upon this interaction, we form our final hypothesis as follows: The two age groups will favor different difficulty adjustment methods.
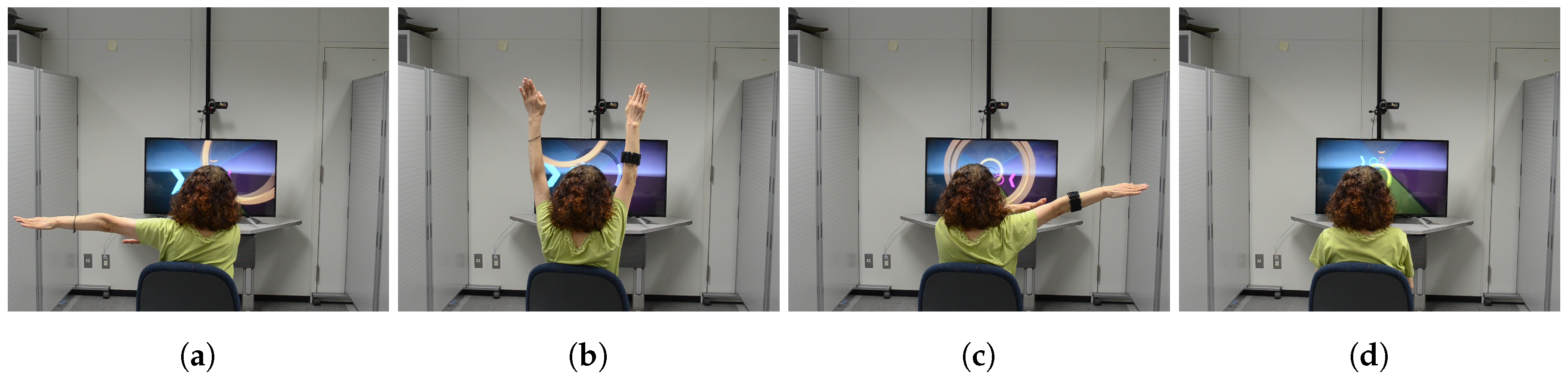
3.2. Exergame Design
3.3. Measures
3.4. Experiment Procedure
3.5. Apparatus
3.6. Environmental Settings
3.7. Participant Profile
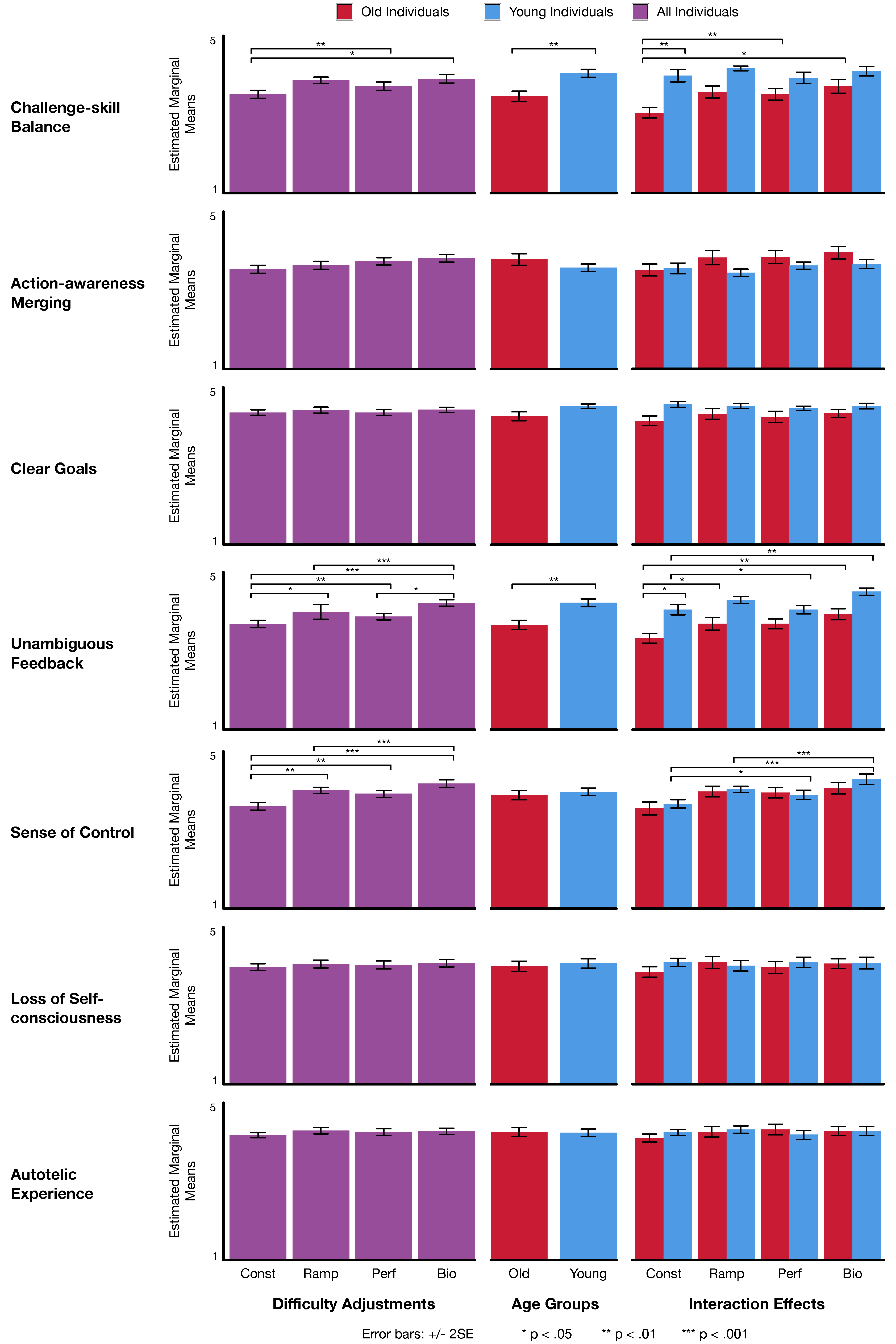
4. Results
4.1. Challenge-Skill Balance
4.2. Action-awareness Merging
4.3. Clear Goals
4.4. Unambiguous Feedback
4.5. Sense of Control
4.6. Loss of Self-Consciousness
4.7. Autotelic Experience
5. Discussion
5.1. General Examination of Results
5.2. Post-Experiment Discussions
5.3. Deployment at a Rehabilitation Hospital
5.4. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| JSPS | Japan Society for the Promotion of Science |
| MIC | Ministry of Internal Affairs and Communications |
| SCOPE | Strategic Information and Communications R&D Promotion Programme |
| DDA | Dynamic Difficulty Adjustments |
| FSS | Flow State Scale |
| HRV | Heart Rate Variability |
| Const | Constant |
| Ramp | Ramping |
| Perf | Performance-based |
| Bio | Biofeedback-based |
Appendix A


References
- World Health Organization. Fact Sheet on Physical Activity; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- World Health Organization. Physical Inactivity: A Global Public Health Problem; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. Can. Med. Assoc. J. 2006, 174, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of exercise is a major cause of chronic diseases. Compr. Physiol. 2018, 2, 1143–1211. [Google Scholar]
- Ding, D.; Lawson, K.D.; Kolbe-Alexander, T.L.; Finkelstein, E.A.; Katzmarzyk, P.T.; van Mechelen, W.; Pratt, M. The economic burden of physical inactivity: A Global Analysis of major non-communicable diseases. Lancet 2016, 388, 1311–1324. [Google Scholar] [CrossRef]
- King, A.; Castro, C.; Wilcox, S.; Eyler, A.; Sallis, J.F.; Brownson, R.C. Personal and environmental factors associated with physical inactivity among different racial-ethnic groups of US middle-aged older-aged women. Health Psychol. 2000, 19, 354–364. [Google Scholar] [CrossRef] [PubMed]
- Cecchini, M.; Sassi, F.; Lauer, J.A.; Lee, Y.Y.; Guajardo-Barron, V.; Chisholm, D. Tackling of unhealthy diets, physical inactivity, and obesity: Health effects and cost-effectiveness. Lancet 2010, 376, 1775–1784. [Google Scholar] [CrossRef]
- Nedeltcheva, A.V.; Kessler, L.; Imperial, J.; Penev, P.D. Exposure to recurrent sleep restriction in the setting of high caloric intake and physical inactivity results in increased insulin resistance and reduced glucose tolerance. J. Clin. Endocrinol. Metab. 2009, 94, 3242–3250. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.H.; Dorn, L. Stress, fatigue, health, and risk of road traffic accidents among professional drivers: The contribution of physical inactivity. Annu. Rev. Public Health 2006, 27, 371–391. [Google Scholar] [CrossRef] [PubMed]
- Paddon-Jones, D. Interplay of stress and physical inactivity on muscle loss: Nutritional countermeasures. J. Nutr. 2006, 136, 2123–2126. [Google Scholar] [CrossRef] [PubMed]
- Kohl, H.W., III; Cook, H.D. Educating the Student Body: Taking Physical Activity and Physical Education to School; National Academies Press: Washington, DC, USA, 2013. [Google Scholar]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Baker, J.S.; dos Santos, L.; Davies, B.; Ciolac, E.G.; Bocalini, D.S. Approaches in physical activity: From basic to applied research. BioMed Res. Int. 2016, 2016, 6498624. [Google Scholar] [CrossRef] [PubMed]
- Kharrazi, H.; Lu, A.S.; Gharghabi, F.; Coleman, W. A scoping review of health game research: Past, present, and future. Games Health 2012, 1, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Marston, H.R.; Freeman, S.; Bishop, K.A.; Beech, C.L. A scoping review of digital gaming research involving older adults aged 85 and older. Games Health J. 2016, 5, 157–174. [Google Scholar] [CrossRef] [PubMed]
- Gerling, K.M.; Schild, J.; Masuch, M. Exergame design for elderly users: The case study of SilverBalance. In Proceedings of the Advances in Computer Entertainment Technology, Taipei, Taiwan, 17–19 November 2010; pp. 66–69. [Google Scholar]
- Brox, E.; Luque, L.F.; Evertsen, G.J.; Hernández, J.E.G. Exergames for elderly: Social exergames to persuade seniors to increase physical activity. In Proceedings of the 2011 5th International Conference on Pervasive Computing Technologies for Healthcare (PervasiveHealth) and Workshops, Dublin, Ireland, 23–26 May 2011; pp. 546–549. [Google Scholar]
- Gerling, K.M.; Livingston, I.J.; Nacke, L.E.; Mandryk, R.L. Full-body motion-based game interaction for older adults. In Proceedings of the Human Factors in Computing Systems, Austin, TX, USA, 5–10 May 2012; pp. 1873–1882. [Google Scholar]
- Daley, A.J. Can exergaming contribute to improving physical activity levels and health outcomes in children? Pediatrics 2009, 124, 763–771. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.; Lin, J.H.; Crouse, J. Is playing exergames really exercising? A meta-analysis of energy expenditure in active video games. Cyberpsychol. Behav. Soc. Netw. 2011, 14, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Larsen, L.H.; Schou, L.; Lund, H.H.; Langberg, H. The physical effect of exergames in healthy elderly—A systematic review. Games Health J. 2013, 2, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Barry, G.; Galna, B.; Rochester, L. The role of exergaming in Parkinson’s disease rehabilitation: A systematic review of the evidence. J. Neuroeng. Rehabil. 2014, 11, 33. [Google Scholar] [CrossRef] [PubMed]
- Staiano, A.E.; Calvert, S.L. Exergames for physical education courses: Physical, social, and cognitive benefits. Child Dev. Perspect. 2011, 5, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Staiano, A.E.; Abraham, A.A.; Calvert, S.L. Competitive versus cooperative exergame play for African American adolescents’ executive function skills: Short-term effects in a long-term training intervention. Dev. Psychol. 2012, 48, 337. [Google Scholar] [CrossRef] [PubMed]
- Staiano, A.E.; Abraham, A.A.; Calvert, S.L. Adolescent exergame play for weight loss and psychosocial improvement: A controlled physical activity intervention. Obesity 2013, 21, 598–601. [Google Scholar] [CrossRef] [PubMed]
- Staiano, A.E.; Flynn, R. Therapeutic uses of active videogames: A systematic review. Games Health J. 2014, 3, 351–365. [Google Scholar] [CrossRef] [PubMed]
- Fox News. Exercise, lose weight with ‘Exergaming’. Fox News, 20 January 2005. [Google Scholar]
- Nintendo. Financial results briefing for the three-month period ended June 2009. Available online: https://www.nintendo.co.jp/ir/pdf/2009/090731e.pdf (accessed on 6 November 2018).
- De Moraes, V.B.; de Andrade, M.M.A.; Toyoda, C.Y.; Araujo, R.D.C.T. The use of Nintendo Wii as therapeutic resource for elderly: An activity analysis from the occupational therapy perspective. Cad. Ter. Ocup. 2016, 24, 705–714. [Google Scholar]
- Fain, E.A.; Kennell, B. Nintendo® Wii™ and a physical activity routine: Effective therapeutic interventions in the older adult population? Open J. Nurs. 2014, 4, 577–582. [Google Scholar] [CrossRef]
- Clark, R.A.; Bryant, A.L.; Pua, Y.; McCrory, P.; Bennell, K.; Hunt, M. Validity and reliability of the Nintendo Wii Balance Board for assessment of standing balance. Gait Posture 2010, 31, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Skjæret-Maroni, N.; Vonstad, E.K.; Ihlen, E.A.; Tan, X.C.; Helbostad, J.L.; Vereijken, B. Exergaming in older adults: Movement characteristics while playing stepping games. Front. Psychol. 2016, 7, 964. [Google Scholar] [CrossRef] [PubMed]
- Sato, K.; Kuroki, K.; Saiki, S.; Nagatomi, R. Improving walking, muscle strength, and balance in the elderly with an exergame using Kinect: A randomized controlled trial. Games Health 2015, 4, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Kamel Boulos, M.N. Xbox 360 Kinect exergames for health. Games Health 2012, 1, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Webster, D.; Celik, O. Systematic review of Kinect applications in elderly care and stroke rehabilitation. J. Neuroeng. Rehabil. 2014, 11, 108. [Google Scholar] [CrossRef] [PubMed]
- Galna, B.; Jackson, D.; Schofield, G.; McNaney, R.; Webster, M.; Barry, G.; Mhiripiri, D.; Balaam, M.; Olivier, P.; Rochester, L. Retraining function in people with Parkinson’s disease using the Microsoft Kinect: Game design and pilot testing. J. Neuroeng. Rehabil. 2014, 11, 60. [Google Scholar] [CrossRef] [PubMed]
- Yim, J.; Graham, T.N. Using games to increase exercise motivation. In Proceedings of the 2007 Conference on Future Play, Toronto, ON, Canada, 14–17 November 2007; pp. 166–173. [Google Scholar]
- Ijsselsteijn, W.; Nap, H.H.; de Kort, Y.; Poels, K. Digital game design for elderly users. In Proceedings of the Future Play, Toronto, ON, Canada, 3–5 November 2008; pp. 17–22. [Google Scholar]
- Russell, W.D.; Newton, M. Short-term psychological effects of interactive video game technology exercise on mood and attention. Educ. Technol. Soc. 2008, 11, 294–308. [Google Scholar]
- Lange, B.; Flynn, S.; Proffitt, R.; Chang, C.Y.; Rizzo, A. Development of an interactive game-based rehabilitation tool for dynamic balance training. Top. Stroke Rehabil. 2010, 17, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Nits, J.; Kuys, S.; Isles, R.; Fu, S. Is the Wii Fit (TM) a new-generation tool for improving balance, health and well-being? A pilot study. Climacteric 2010, 13, 487–491. [Google Scholar] [CrossRef] [PubMed]
- De Groot, G.; Lindgren, C.; Fagerström, L. Older adults’ motivating factors and barriers to exercise to prevent falls. Scand. J. Occup. Ther. 2011, 18, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Kosse, N.M.; Caljouw, S.R.; Vuijk, P.J.; Lamoth, C.J.C. Exergaming: Interactive balance training in healthy community-dwelling older adults. Cyber Ther. Rehabil. 2011, 4, 399–407. [Google Scholar]
- Keyani, P.; Hsieh, G.; Mutlu, B.; Matthew, E.; Forlizzi, J. DanceAlong: Supporting positive social exchange and exercise for the elderly through dance. In Extended Abstracts on Human Factors in Computing Systems; ACM: New York, NY, USA, 2005; pp. 1541–1544. [Google Scholar]
- Romero, N.; Sturm, J.; Bekker, T.; De Valk, L.; Kruitwagen, S. Playful persuasion to support older adults’ social and physical activities. Interact. Comput. 2010, 22, 485–495. [Google Scholar] [CrossRef]
- Baldwin, A.; Johnson, D.; Wyeth, P.A. The effect of multiplayer dynamic difficulty adjustment on the player experience of video games. In Extended Abstracts on Human Factors in Computing Systems; ACM: New York, NY, USA, 2014; pp. 1489–1494. [Google Scholar]
- Smeddinck, J.D.; Siegel, S.; Herrlich, M. Adaptive difficulty in exergames for Parkinson’s disease patients. In Proceedings of the Regina Graphics Interface, Regina, SK, Canada, 29–31 May 2013; pp. 141–148. [Google Scholar]
- Gerling, K.M.; Miller, M.; Mandryk, R.L.; Birk, M.V.; Smeddinck, J.D. Effects of balancing for physical abilities on player performance, experience and self-esteem in exergames. In Proceedings of the Human Factors in Computing Systems, Regina, SK, Canada, 29–31 May 2013; pp. 2201–2210. [Google Scholar]
- Stach, T.; Graham, N.; Yim, J.; Rhodes, R. Heart rate control of exercise video games. In Proceedings of the Graphics Interface, Kelowna, BC, Canada, 25–27 May 2009; pp. 125–132. [Google Scholar]
- Liu, C.; Agrawal, P.; Sarkar, N.; Chen, S. Dynamic difficulty adjustment in computer games through real-time anxiety-based affective feedback. Int. J. Hum.-Comput. Interact. 2009, 25, 506–529. [Google Scholar] [CrossRef]
- Mueller, F.; Edge, D.; Vetere, F.; Gibbs, M.R.; Agamanolis, S.; Bongers, B.; Sheridan, J.G. Designing sports: A framework for exertion games. In Proceedings of the Human Factors in Computing Systems, Vancouver, BC, Canada, 7–12 May 2011; pp. 2651–2660. [Google Scholar]
- Straker, L.; Abbott, R. Effect of screen-based media on energy expenditure and heart rate in 9-to 12-year-old children. Pediatr. Exerc. Sci. 2007, 19, 459–471. [Google Scholar] [CrossRef] [PubMed]
- Graves, L.E.; Ridgers, N.D.; Williams, K.; Stratton, G.; Atkinson, G.; Cable, N.T. The physiological cost and enjoyment of Wii Fit in adolescents, young adults, and older adults. J. Phys. Act. Health 2010, 7, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Althoff, T.; White, R.W.; Horvitz, E. Influence of Pokémon Go on physical activity: Study and implications. J. Med. Internet Res. 2016, 18, e315. [Google Scholar] [CrossRef] [PubMed]
- Douris, P.C.; McDonald, B.; Vespi, F.; Kelley, N.C.; Herman, L. Comparison between Nintendo Wii Fit aerobics and traditional aerobic exercise in sedentary young adults. J. Strength Cond. Res. 2012, 26, 1052–1057. [Google Scholar] [CrossRef] [PubMed]
- Phillips, E.M.; Schneider, J.C.; Mercer, G.R. Motivating elders to initiate and maintain exercise. Arch. Phys. Med. Rehabil. 2004, 85, 52–57. [Google Scholar] [CrossRef]
- Billis, A.; Konstantinidis, E.; Mouzakidis, C.; Tsolaki, M.; Pappas, C.; Bamidis, P. A game-like interface for training seniors’ dynamic balance and coordination. In Proceedings of the Mediterranean Conference on Medical and Biological Engineering and Computing, Chalkidiki, Greece, 27–30 May 2010; pp. 691–694. [Google Scholar]
- Ijsselsteijn, W.A.; Kort, Y.D.; Westerink, J.; Jager, M.D.; Bonants, R. Virtual fitness: Stimulating exercise behavior through media technology. Presence-Teleoper. Virtual Env. 2006, 15, 688–698. [Google Scholar] [CrossRef]
- Durick, J.; Robertson, T.; Brereton, M.; Vetere, F.; Nansen, B. Dispelling ageing myths in technology design. In Proceedings of the Australian Computer-Human Interaction Conference, Adelaide, Australia, 25–29 November 2013; pp. 467–476. [Google Scholar]
- Skjæret, N.; Nawaz, A.; Ystmark, K.; Dahl, Y.; Helbostad, J.L.; Svanæs, D. Designing for movement quality in exergames: Lessons learned from observing senior citizens playing stepping games. Gerontology 2015, 61, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Gerling, K.M.; Schulte, F.P.; Masuch, M. Designing and evaluating digital games for frail elderly persons. In Proceedings of the Advances in Computer Entertainment Technology, Lisbon, Portugal, 8–11 November 2011; pp. 62–69. [Google Scholar]
- Baldwin, A.; Johnson, D.; Wyeth, P.; Sweetser, P. A framework of dynamic difficulty adjustment in competitive multiplayer video games. In Proceedings of the 2013 IEEE International Games Innovation Conference (IGIC), Vancouver, BC, Canada, 23–25 September 2013; pp. 16–19. [Google Scholar]
- Hunicke, R. The case for dynamic difficulty adjustment in games. In Proceedings of the Human Factors in Computing Systems, Valencia, Spain, 15–17 June 2005; pp. 429–433. [Google Scholar]
- Jennings-Teats, M.; Smith, G.; Wardrip-Fruin, N. Polymorph: Dynamic difficulty adjustment through level generation. In Proceedings of the Workshop on Procedural Content Generation in Games, Monterey, CA, USA, 18 June 2010; p. 11. [Google Scholar]
- Lange, B.; Flynn, S.; Chang, C.Y.; Liang, W.; Si, Y.; Nanavati, C.; Chieng, C.L. Development of an interactive stepping game to reduce falls in older adults. Disabil. Hum. Dev. 2011, 10, 331–335. [Google Scholar] [CrossRef]
- Uzor, S.; Baillie, L. Investigating the long-term use of exergames in the home with elderly fallers. In Proceedings of the Human Factors in Computing Systems, Toronto, ON, Canada, 26 April–1 May 2014; pp. 2813–2822. [Google Scholar]
- Jackson, S.A.; Marsh, H.W. Development and validation of a scale to measure optimal experience: The flow state scale. J. Sport Exerc. Psychol. 1996, 18, 17–35. [Google Scholar] [CrossRef]
- Gamberini, L.; Raya, M.A.; Barresi, G.; Fabregat, M.; Ibanez, F.; Prontu, L. Cognition, technology and games for the elderly: An introduction to ELDERGAMES Project. PsychNol. J. 2006, 4, 285–308. [Google Scholar]
- Bruckman, A. Can educational be fun. In Proceedings of the Game Developers Conference, San Jose, CA, USA, 15–19 March 1999; Volume 99, pp. 75–79. [Google Scholar]
- Karvonen, M.J. The effects of training on the heart rate. Ann. Med. Exp. Biol. Fenn. 1957, 35, 307–315. [Google Scholar] [PubMed]
- Csikszentmihalyi, M. Flow: The Psychology of Optimal Experience; Harper & Row: New York, NY, USA, 1990; pp. 209–226. [Google Scholar]
- Thomas, S.; Reading, J.; Shephard, R.J. Revision of the physical activity readiness questionnaire (PAR-Q). Can. J. Sport Sci. 1992, 17, 338–345. [Google Scholar] [PubMed]
- Lu, A.S. Narrative in exergames: Thoughts on procedure, mechanism, and others. Games Health 2015, 4, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Social cognitive theory: An agentic perspective. Annu. Rev. Psychol. 2001, 52, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.R.; Ishii-Kuntz, M. Social interaction, loneliness, and emotional well-being among the elderly. Res. Aging 1987, 9, 459–482. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, R.; Luszczynska, A.; Ziegelmann, J.P.; Scholz, U.; Lippke, S. Social-Cognitive Predictors of Physical Exercise Adherence: Three Longitudinal Studies in Rehabilitation; American Psychological Association: Washington, DC, USA, 2008; Volume 27, pp. S54–S63. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Modification | Distance (in Seconds) | ||
|---|---|---|---|
| Young | Old | ||
| Constant | Fixed | 1.0″, 0.75″, 0.5″ | 1.5″, 1.0″, 0.5″ |
| Ramping | Reduced over time | 1.0″∼0.5″ | 1.5″∼0.5″ |
| Performance-based | Reduced on success | 1.0″∼0.5″ | 1.5″∼0.5″ |
| Biofeedback-based | Dynamic based on HRV | 1.0″∼0.5″ | 1.5″∼0.5″ |
| Male | Female | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| N | Mean | St.Dev. | N | Mean | St.Dev. | N | Mean | St.Dev. | |
| Old | 10 | 72.30 | 2.91 | 4 | 72.50 | 3.70 | 14 | 72.36 | 3.00 |
| Young | 10 | 27.10 | 3.03 | 5 | 26.20 | 1.64 | 15 | 26.80 | 2.62 |
| Total | 20 | 49.70 | 23.37 | 9 | 46.78 | 24.53 | 29 | 48.79 | 23.33 |
| αconst | αramp | αperf | αbio | |
|---|---|---|---|---|
| Challenge-skill Balance | 0.916 | 0.931 | 0.899 | 0.891 |
| Action-awareness Merging | 0.818 | 0.885 | 0.902 | 0.854 |
| Clear Goals | 0.943 | 0.947 | 0.938 | 0.874 |
| Unambiguous Feedback | 0.874 | 0.852 | 0.902 | 0.891 |
| Concentration on Task at Hand | 0.740 | 0.649 | 0.701 | 0.805 |
| Sense of Control | 0.883 | 0.877 | 0.869 | 0.923 |
| Loss of Self-consciousness | 0.828 | 0.789 | 0.825 | 0.730 |
| Transformation of Time | 0.506 | 0.642 | 0.728 | 0.827 |
| Autotelic Experience | 0.827 | 0.933 | 0.911 | 0.899 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaplan, O.; Yamamoto, G.; Taketomi, T.; Plopski, A.; Sandor, C.; Kato, H. Exergame Experience of Young and Old Individuals Under Different Difficulty Adjustment Methods. Computers 2018, 7, 59. https://doi.org/10.3390/computers7040059
Kaplan O, Yamamoto G, Taketomi T, Plopski A, Sandor C, Kato H. Exergame Experience of Young and Old Individuals Under Different Difficulty Adjustment Methods. Computers. 2018; 7(4):59. https://doi.org/10.3390/computers7040059
Chicago/Turabian StyleKaplan, Oral, Goshiro Yamamoto, Takafumi Taketomi, Alexander Plopski, Christian Sandor, and Hirokazu Kato. 2018. "Exergame Experience of Young and Old Individuals Under Different Difficulty Adjustment Methods" Computers 7, no. 4: 59. https://doi.org/10.3390/computers7040059
APA StyleKaplan, O., Yamamoto, G., Taketomi, T., Plopski, A., Sandor, C., & Kato, H. (2018). Exergame Experience of Young and Old Individuals Under Different Difficulty Adjustment Methods. Computers, 7(4), 59. https://doi.org/10.3390/computers7040059