Traffic Priority-Aware Adaptive Slot Allocation for Medium Access Control Protocol in Wireless Body Area Network

Abstract
:1. Introduction
- Firstly, a reduced contention adaptive slot allocation algorithm is presented, to minimize contention rounds during the transmission of data from BMSs to the body coordinator.
- Secondly, a low threshold vital signs criticality-based adaptive slot allocation algorithm is developed to resolve slot allocation conflicts among high priority data.
- Thirdly, a high threshold vital signs criticality-based adaptive slot allocation algorithm is designed to resolve slot allocation conflicts among low priority data.
- Simulations are performed in realistic biomedical environments, to comparatively evaluate the performance of the proposed protocol with state-of-the-art MAC protocols.
2. Related Works
- ■
- IEEE 802.15.4 provides limited 16 (0–15) channels.
- ■
- All BMSs perform contention and repeats the previous rounds of contention in the current rounds to access the channel in the CAP period.
- ■
- Allocation of the CFP channels only to those BMSs that obtained a channel access in the CAP period.
- ■
- During contention to access the channel, there is no priority-basis slot allocated to emergency data, and there is no differentiation between normal, periodic, and emergency data to assign the first slot based on priority during life critical situations.
- ■
- Due to contention, BMSs consume a higher amount of energy and drop patient data by exceeding the threshold values of contention.
- ■
- In TDMA, each BMS transmits sensory data in the fixed length of time and drops data if it has a large amount of data (frame). For instance, the report of the ECG is comprised of long sensory information.
3. Traffic Priority-Aware Adaptive Slot Allocation for Medium Access Control
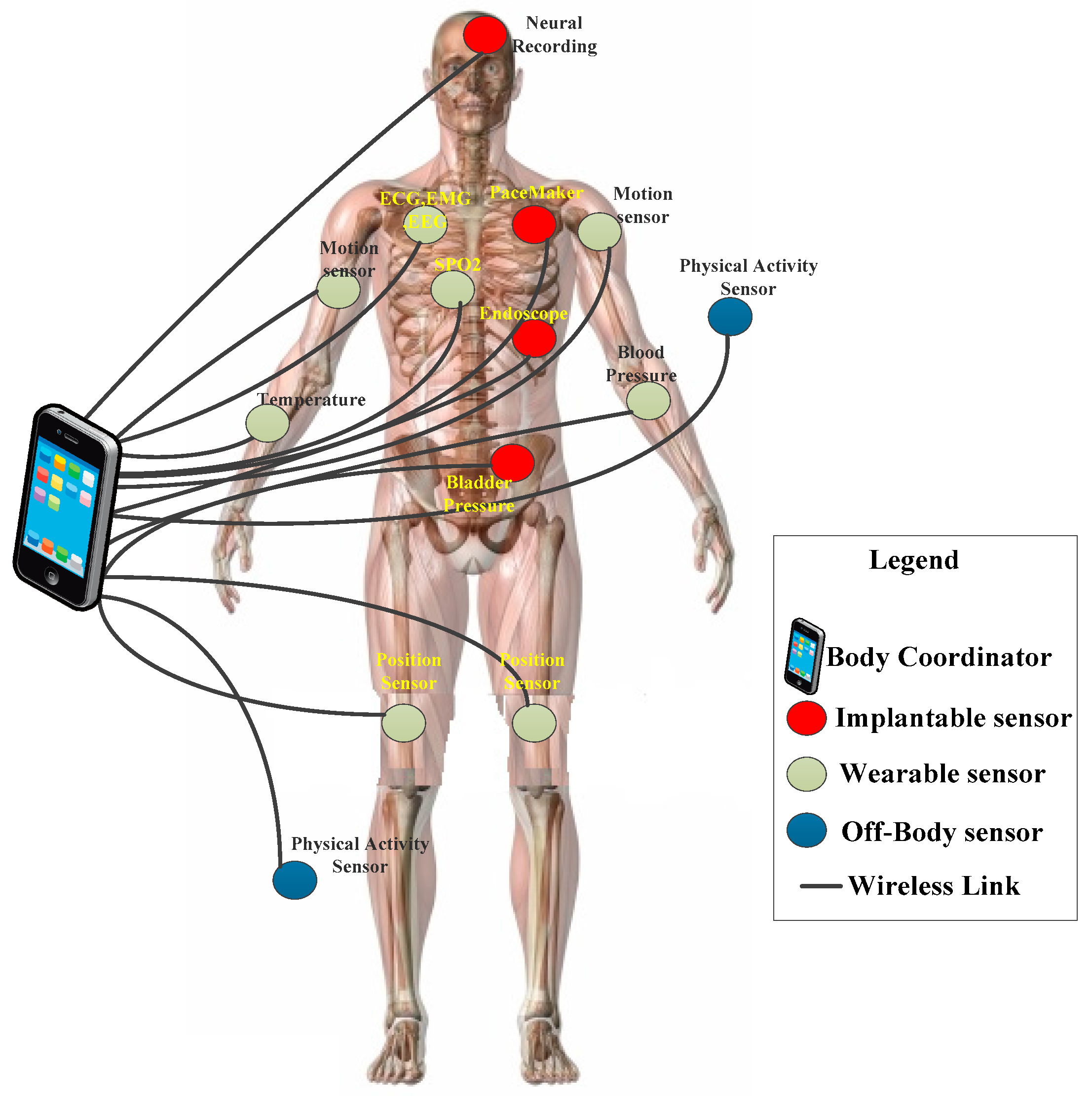
3.1. Network Model
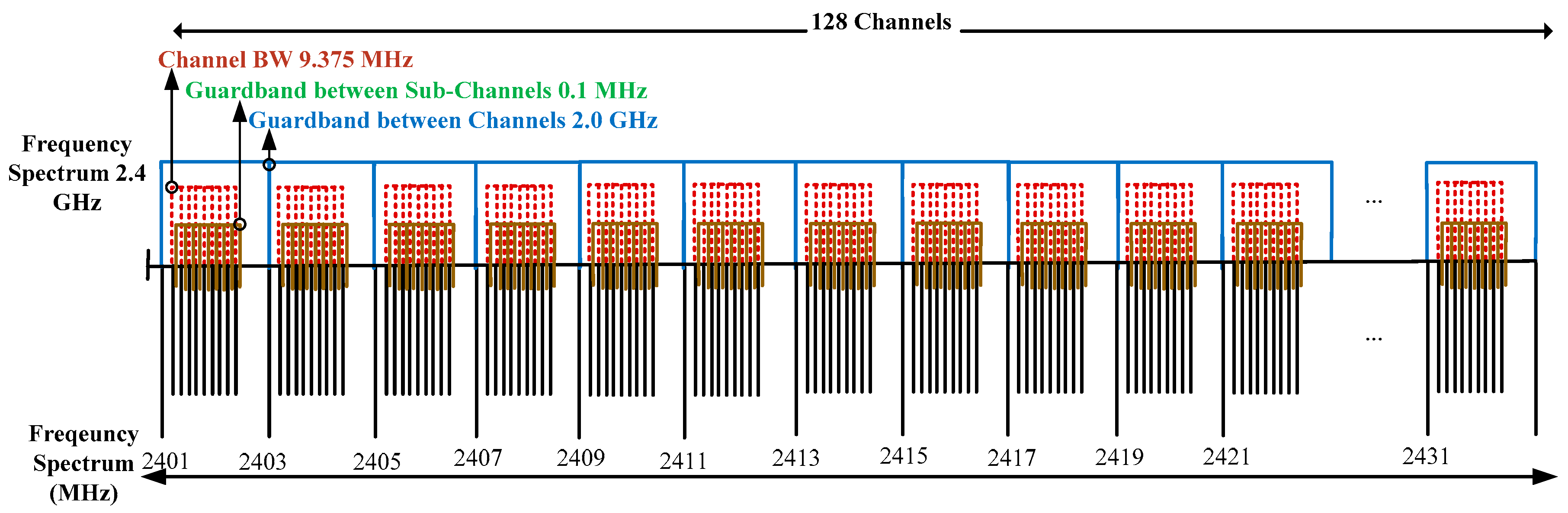
- This study proposes Superframe structure of the TraySL-MAC protocol and provides sufficient channels by classifying the operating frequency into sub-frequencies.
- The sub-frequencies avoid the channel interferences, and BMSs transmit the long report of ECG with a sufficient time period of BI.
- The proposed ReCAL-CSMA/CA mechanism reduces the repetition in rounds of contention of non-emergency-based BMSs and does not drop the patient’s data.
- Emergency-based BMSs do not contend to access the CAP channel, but they transmit alert signals to the dedicated emergency beacons. For this purpose, this study proposes a delay-aware mechanism, known as VSCAS.
- The proposed TraySL-MAC protocol and other mechanisms improve throughput and packet delivery ratio (PDR), and reduces energy consumption and packet delivery delay.
3.2. Frequency Bands
3.3. Patient’s Traffic Classification
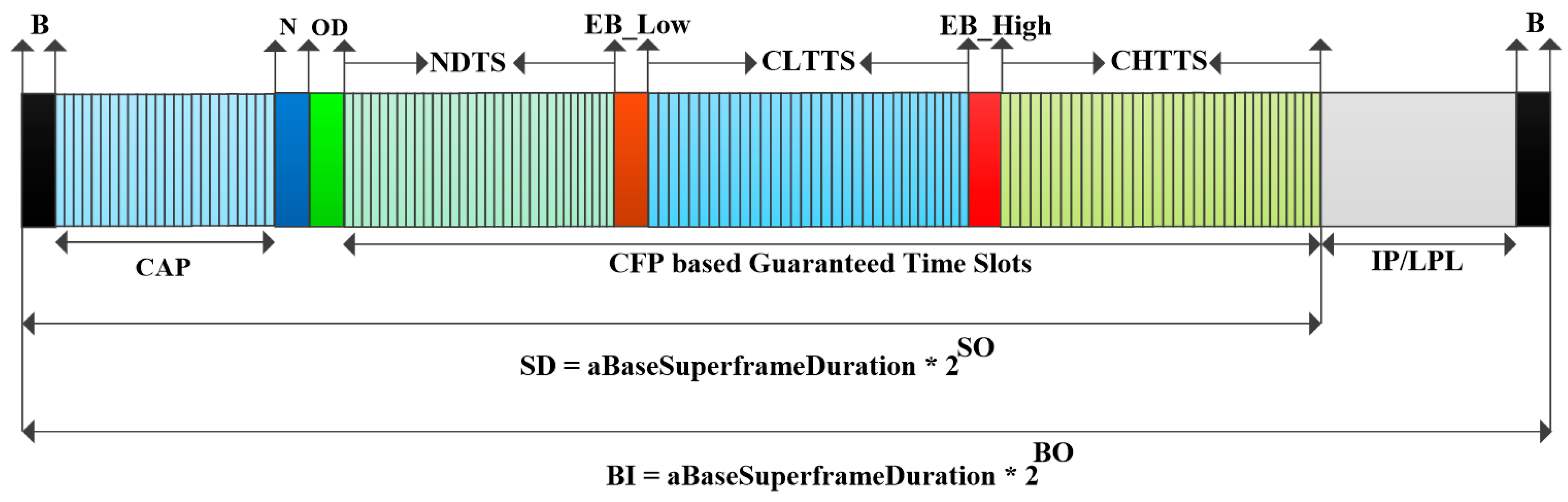
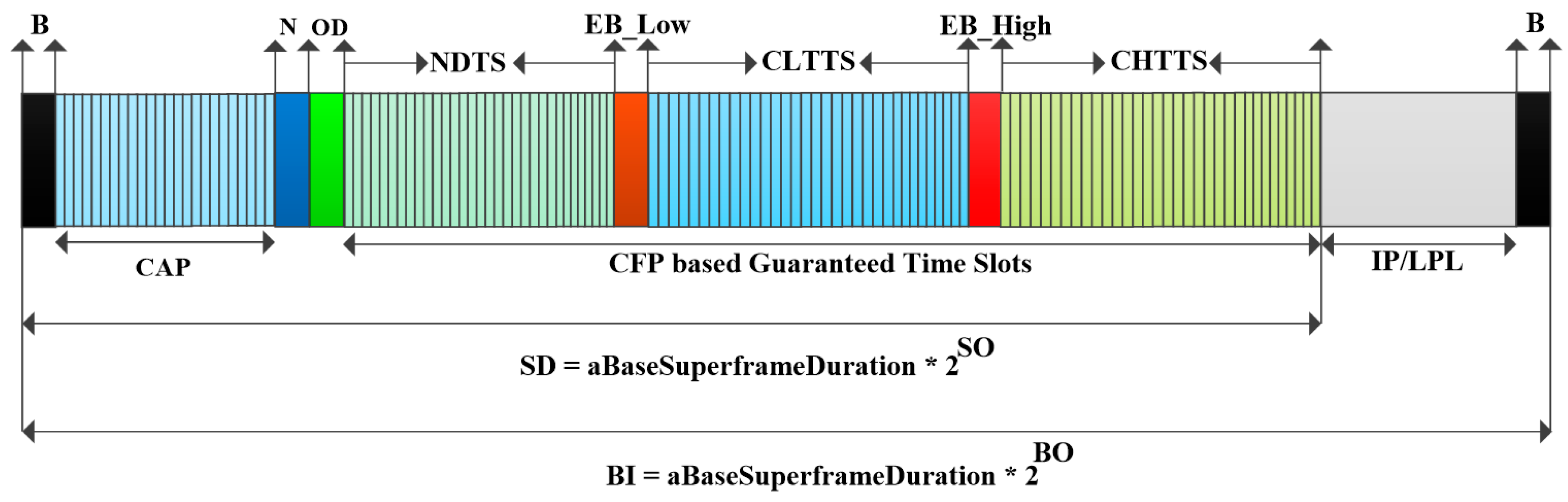
3.4. The Superframe Structure of TraySL-MAC
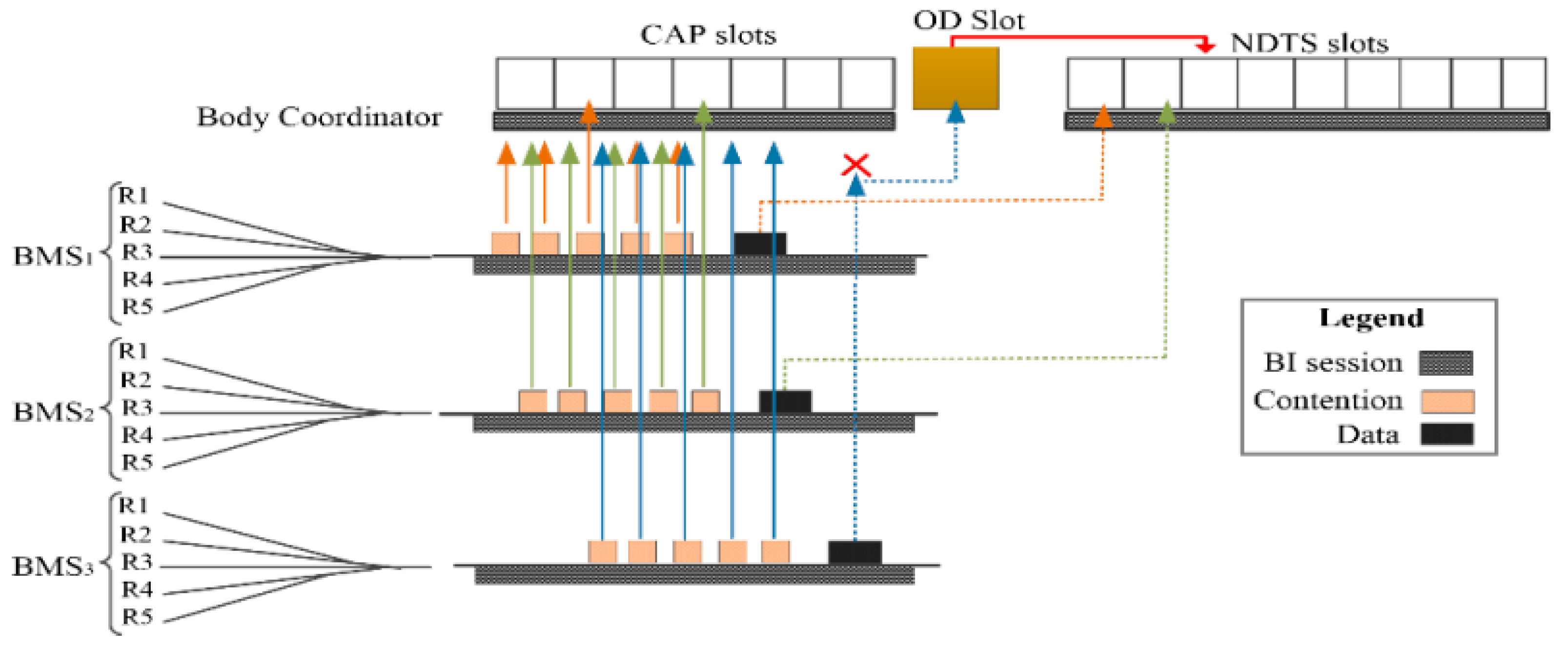
3.5. Reduced Contention Adaptive Slot Allocation CSMA/CA Scheme
| Algorithm 1. ReCAL-CSMA/CA: Reduced contention adaptive slot allocation CSMA-CA scheduling access scheme. | |
| Notations | |
| : Contention window size | |
| : Number of back-offs | |
| CCA: Clear Channel Assessment | |
| Be: Back-off Exponential | |
| MacMinBe: First round for contention | |
| MACb: Second round for contention | |
| MACMinb: Third round for contention | |
| MacMedb: Fourth round for contention | |
| aMaxb: fifth round for contention | |
| : Minimum Be | |
| : Maximum Be | |
| Process | |
| 1. | Set = 2, = 0, Be = 1 |
| 2. | if (BMS_i ∈ operates on Fixed Battery Power OR Not operates on Fixed Battery) |
| Set Be ← min (1, MacMinBe) | |
| else | |
| Set Be ← 1 | |
| end if | |
| 3. | Locate Backoff Period boundary |
| Set ← (0 To 2Be − 1) | |
| Set BMS_i ← perform CCA on backoff period boundary of | |
| 4. | if (channel_of_CAP = idle) |
| Set Decrement ( ← − 1) | |
| if ( = 0 && slot is available in CAP period) | |
| Transmit | |
| else | |
| CCA expires and Go to [Step 4] | |
| end if | |
| 5. | else // in case of channel busy |
| Set ← 2 | |
| Set Be ← Be + 1; | |
| Set Be ← min (Be + 1, aMaxb) | |
| end if | |
| 6. | if ( > aMaxb) |
| //Here to add OD slot to access NDTS slots of CFP period | |
| Set perform CCA 2 Times to find status of OD_slot | |
| if (status_of_OD_Slot = idle) | |
| Set OD_Slot ← BMS_i transmits an alert signal | |
| BMS_i ←BC_Allocates_ NDTS _slot (Xi) | |
| NDTS _slot (Xi) ← BMS_i | |
| else | |
| Wait for next beacon interval or Drop | |
| end if | |
| 7. | else |
| if (= MACb) | |
| Set MACb ← 2 | |
| Set Be ← MACb | |
| Delay for random [Compute =2(Be -1) To 2 Be – 1] Backoffs | |
| Go to [Step 4] | |
| else if ( = MACMinb) | |
| Set MACMinb ← 3 | |
| Set Be ← MACMinb | |
| Delay for random [Compute =2(Be -1) To 2 Be – 1] Backoffs | |
| Go to [Step 4] | |
| else if ( = MACMedb) | |
| Set MACMedb ← 4 | |
| Set Be ← MACMedb | |
| Delay for random [Compute =2(Be -1) To 2 Be – 1] Backoffs | |
| Go To & Perform CCA [Step 4] | |
| else | |
| Set aMaxb ← 5 | |
| Set Be ← aMaxb | |
| Delay for random [Compute =2(Be -1) To 2 Be – 1] Backoffs | |
| Go To & Perform CCA [Step 4] | |
| else | |
| Set perform CCA 2 times for OD_slot | |
| Allocate NDTS slots | |
| end if | |
| end if | |
| 8. | End |
| Output: Minimization in rounds of contentions, delay, packet loss, energy consumption and allocation of CAP slots to BMSs | |
3.5.1. Explanation of Steps of ReCal-CSMA/CA Algorithm
3.5.2. Complexity Analysis
3.6. Slot Allocation Based on the Criticalities of Threshold Values
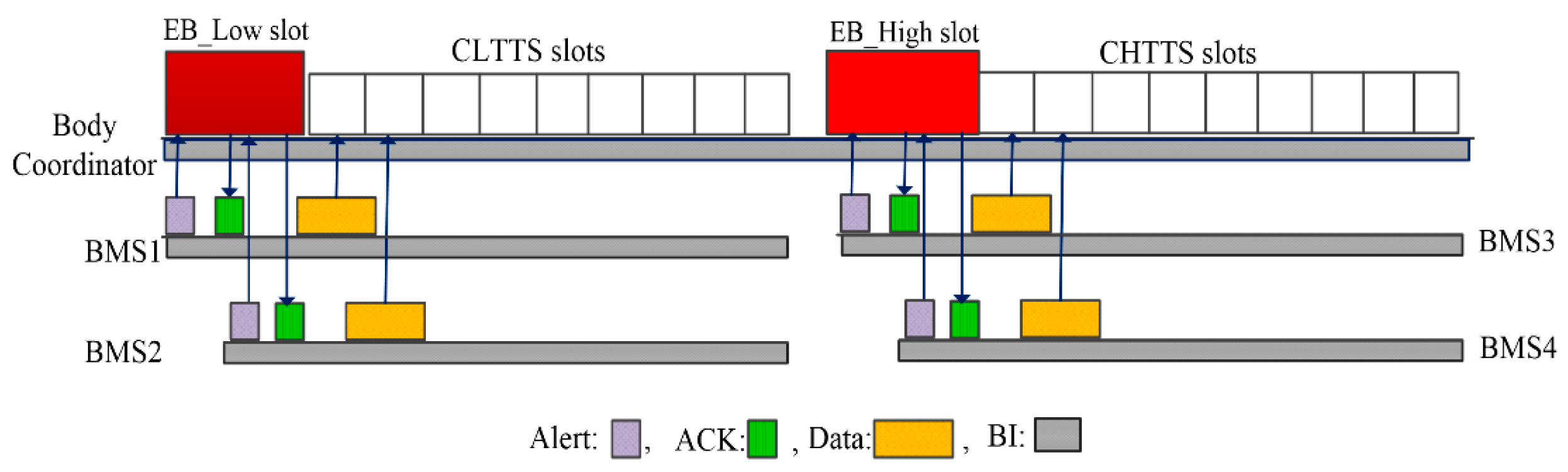
3.6.1. Low Threshold Vital Signs Criticalities-Based Adaptive Slot Allocation
| Algorithm 2. (LT-VSCAS): The body coordinator calculates the criticalities of low threshold values and assigns CLTTS slots on the priority-basis to vital signs. | |
| Notations | |
| Vital_signs_Monitor: vital signs of a patient. | |
| TH_Val: Threshold values of a vital sign | |
| BMSm… + in: Number of different BMSs to monitor vital signs of a patient. | |
| BC: The Body Coordinator who is responsible for the allocation of CLTTS slots. | |
| EB_Low: Emergency beacon for Low threshold values to receive alerts during emergency situation. | |
| CLTTS: “critical low threshold transfer slots” designated to allocate during transmission of low threshold values. | |
| BC: The body coordinator is to allocate CLTTS slots | |
| G_Ea: Earlier generation time of detection of threshold value. | |
| G_Re: Recently generation time of detection of threshold value. | |
| PktS: The packet size of the detected vital sign. | |
| BC_Allc_CLTTS: The body Coordinator allocates CLTTS slots to sensors of detected low threshold values. | |
| PKts_m: the data packet belongs to BMS m | |
| PKts_n: the data packet belongs to BMS n | |
| C_L1: Low threshold is represented by Criticality level (L1). | |
| C_L2: Low threshold is represented by Criticality level (L2). | |
| Input | |
| Classification of the low threshold values into L1 and L2. L1 is more critical as it approaches towards zero value as compared to L2 which is far away from L1 value. | |
| Process | |
| START | |
| 1. ← | |
| 2. for (each BMS transmit Th_Val belongs to Low) do | |
| 3. then | |
| 4. | |
| 5. Low_Th_Vals && ∈ ) == ← S () && ← S () | |
| 6. else > ← S () && ← S () | |
| 7. else ← S () && ← S () | |
| 8. else ← S () && ← S () | |
| 9. == ←S () && ←S () | |
| 10. else > ←S () && ← S () | |
| 11. else ←S () && ← S () | |
| 12. else ←S () && ← S () | |
| 13. == ← S () && ← S () | |
| 14. else > ← S () && ← S () | |
| 15. else ← S () && ← S () | |
| 16. else ← S () && ← S () | |
| 17. == ← S () && ← S () | |
| 18. else > ← S () && ← S () | |
| 19. else ← S () && ← S () | |
| 20. else ( ← S () && ← S () | |
| else Go to sleep or monitor the vital sign | |
| END | |
| Output: Allocation of CLTTS slots to low threshold values based on the criticalities of vital signs | |
3.6.2. Explanation of Steps of LT_VSCAS Algorithm
3.6.3. High Threshold Vital Signs Criticalities-Based Adaptive Slot Allocation
| Algorithm 3. (HT-VSCAS): The body coordinator calculates the criticalities of high threshold values and assigns CHTTS slots on the priority-basis to vital signs. | |
| Notations | |
| Vital_signs_Monitor: vital signs of a patient. | |
| TH_Val: Threshold values of a vital sign | |
| BMSm… + in: Number of different BMSs to monitor vital signs of a patient. | |
| BC: Body Coordinator who is responsible for the allocation of CHTTS slots. | |
| EB_High: Emergency beacon for High threshold values to receive alerts during emergency situation. | |
| CHTTS: “critical high threshold transfer slots” designated to allocate during transmission of high threshold values. | |
| G_Ea: Earlier generation time of detection of threshold value. | |
| G_Re: Recently generation time of detection of threshold value. | |
| PktS: The packet size of the detected vital sign. | |
| BC_Allc_CHTTS: The body Coordinator allocates CHTTS slots to sensors of detected high threshold values. | |
| PKts_m: the data packet belongs to BMS m | |
| PKts_n: the data packet belongs to BMS n | |
| C_H1: High threshold represents by Criticality level (H1) as it is more critical as compared to H2. | |
| C_H2: High threshold represents by Criticality level (H2). | |
| Input | |
| Classification of the High threshold values in H1 and H2. H1 contains more critical data as compared to H2 because the ranges of H1 is greater than H2. | |
| Process | |
| START | |
| 1. ← | |
| 2. for (each BMS transmit Th_Val belongs to high) do | |
| 3. then | |
| 4. | |
| 5. | |
| 6. High_Th_Val && ∈ ) | |
| 7. ← S () && ← S () | |
| 8. else > ← S () && ← S () | |
| 9.else ← S () && ← S () | |
| 10. else = = ← S () && ← S () | |
| 11. else = = ← S () && ← S () | |
| 12. else > ← S () && ← S () | |
| 13. else ← S () && ← S ( ) | |
| 14. else = = ← S () && ← S () | |
| 15. else = = ← S () && ← S () | |
| 16. else > ← S () && ← S () | |
| 17. else ← S () && ← S () | |
| 18. else = = ← S () && ← S () | |
| 19. else = = ← S () && ← S () | |
| 20. else > ( ← S () && ← S () | |
| 21. else < ( ← S () && ← S () | |
| 22. else = = ( ← S () && ← S () | |
| else Go to sleep or monitor the vital sign | |
| end for | |
| END | |
| Output: Allocation of CHTTS slots to high threshold values based on the criticalities of vital signs | |
3.6.4. Explanation of Steps of HT_VSCAS Algorithm
3.6.5. Complexity Analysis of LT_VSCAS and HT_VSCAS Algorithms
4. Performance Evaluation
4.1. Evaluation of ReCAL-CSMA/CA
4.2. Comparative Evaluation
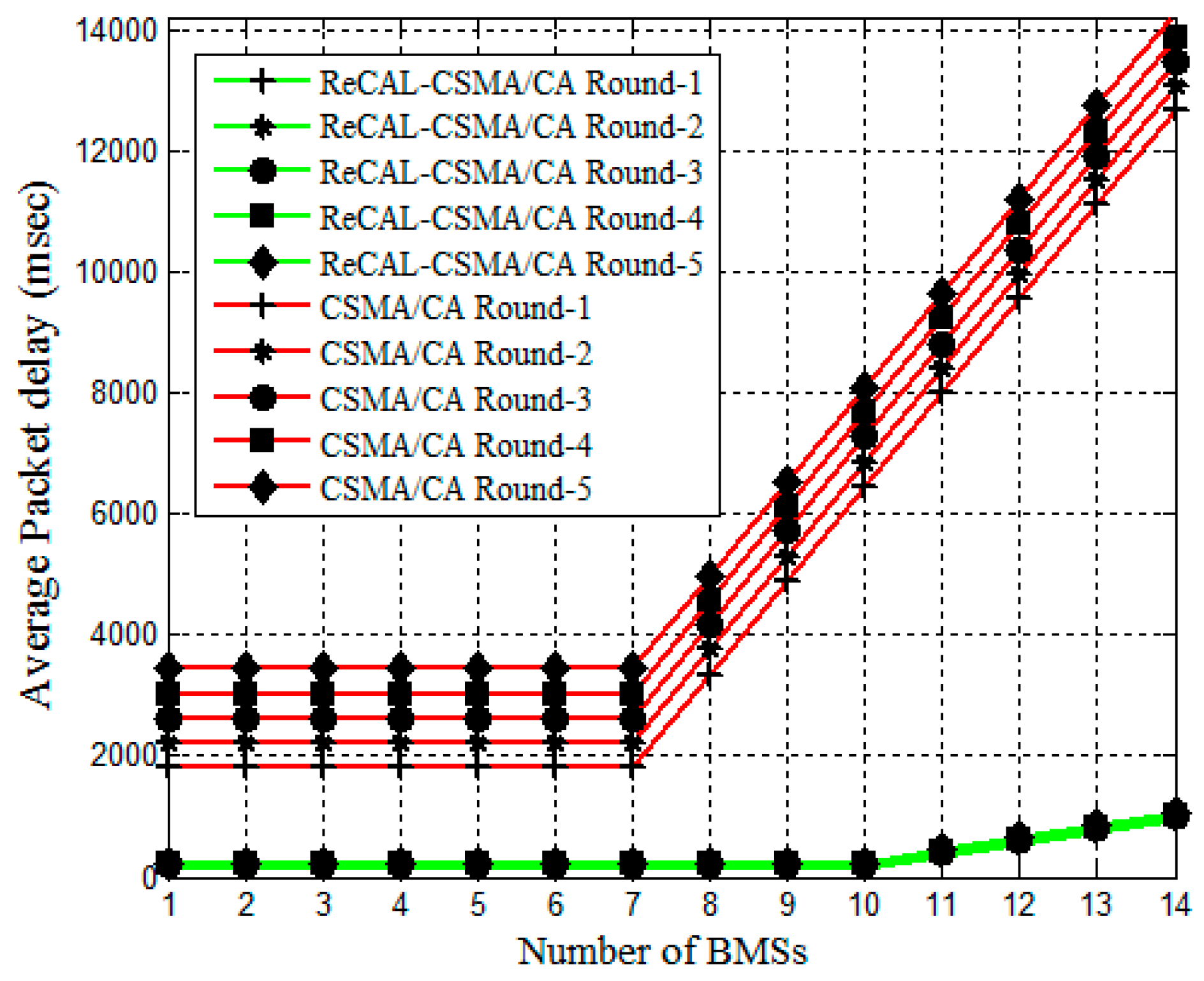
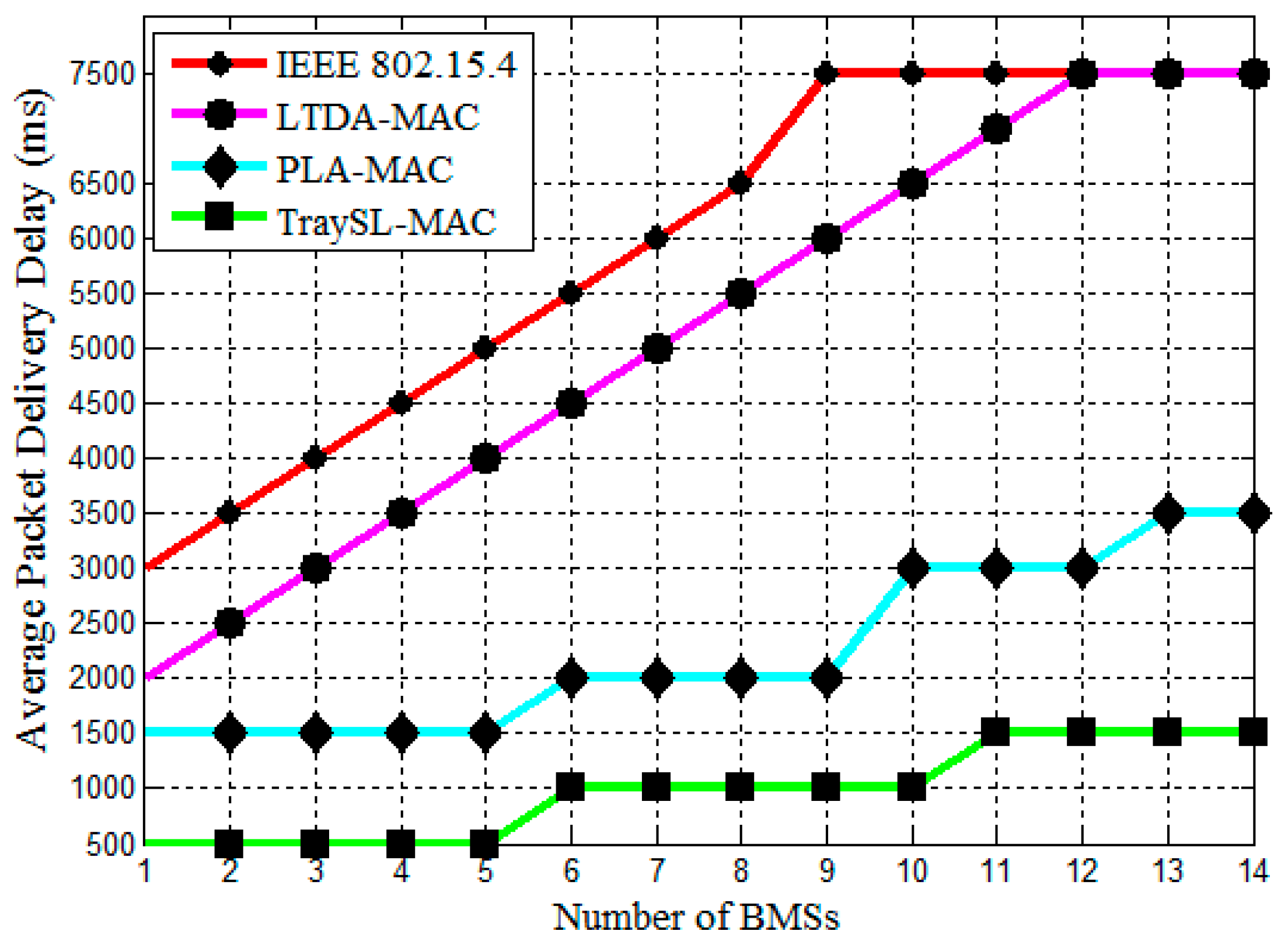
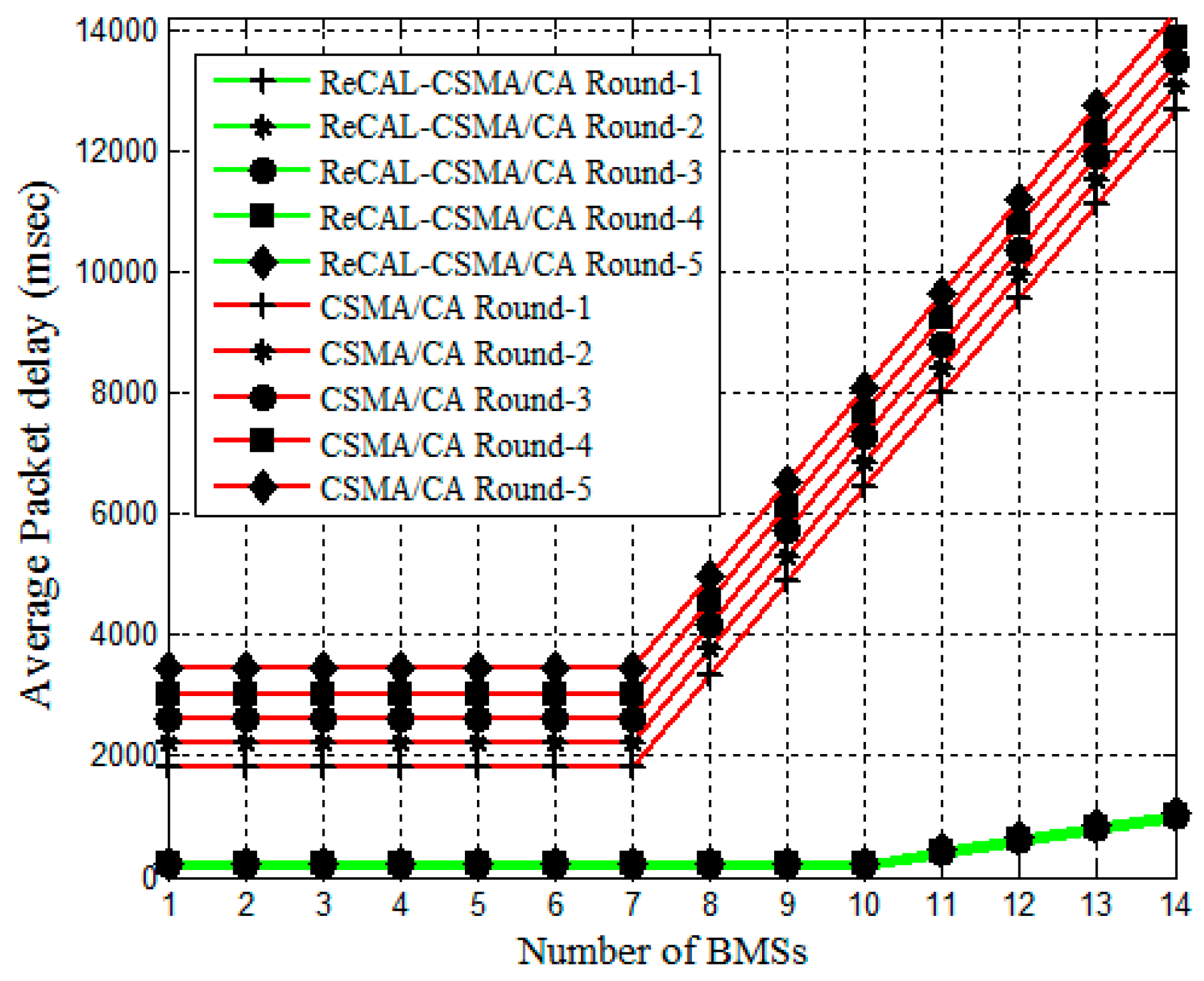
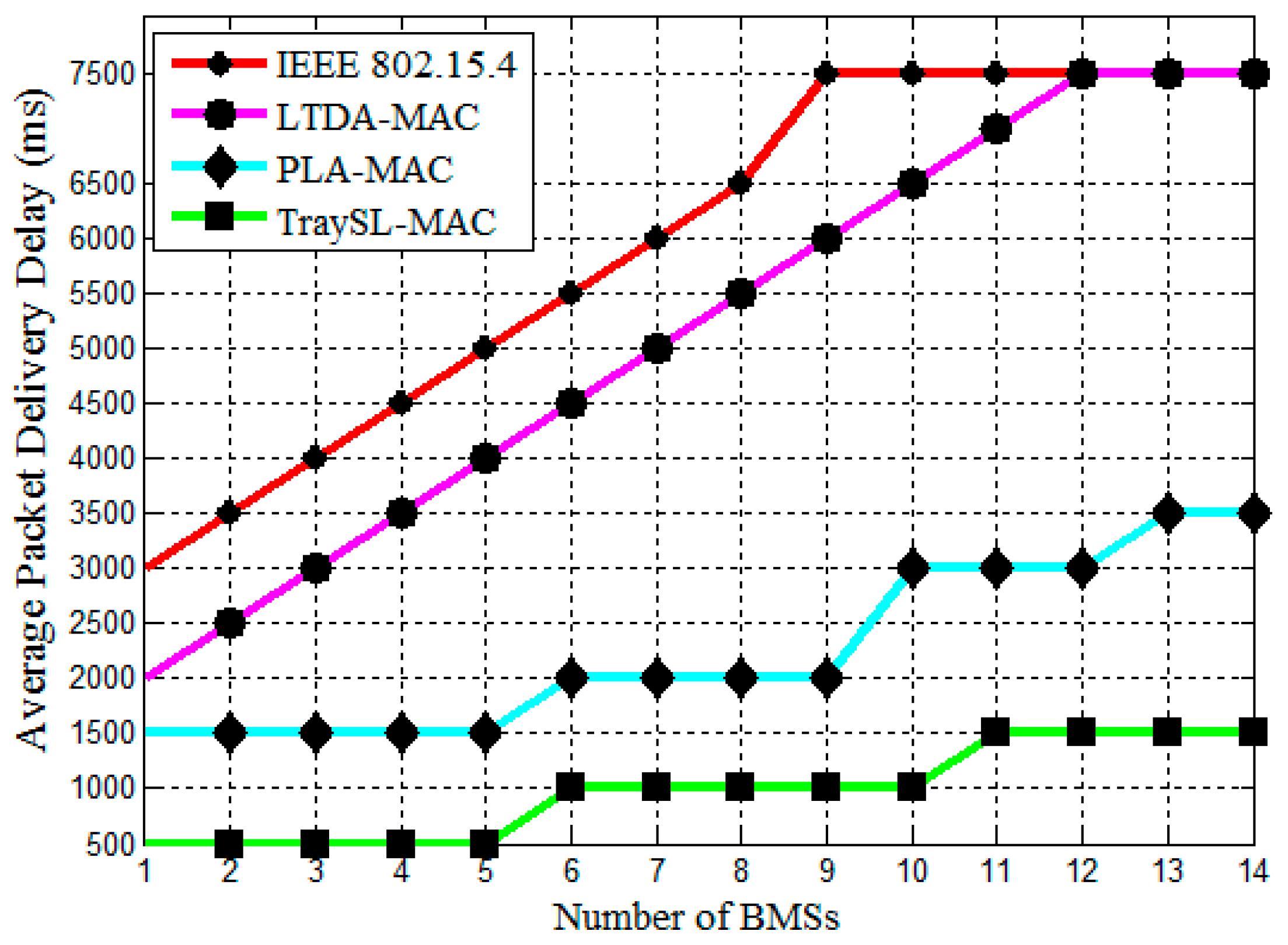
4.2.1. Analysis of Packet Delivery Delay
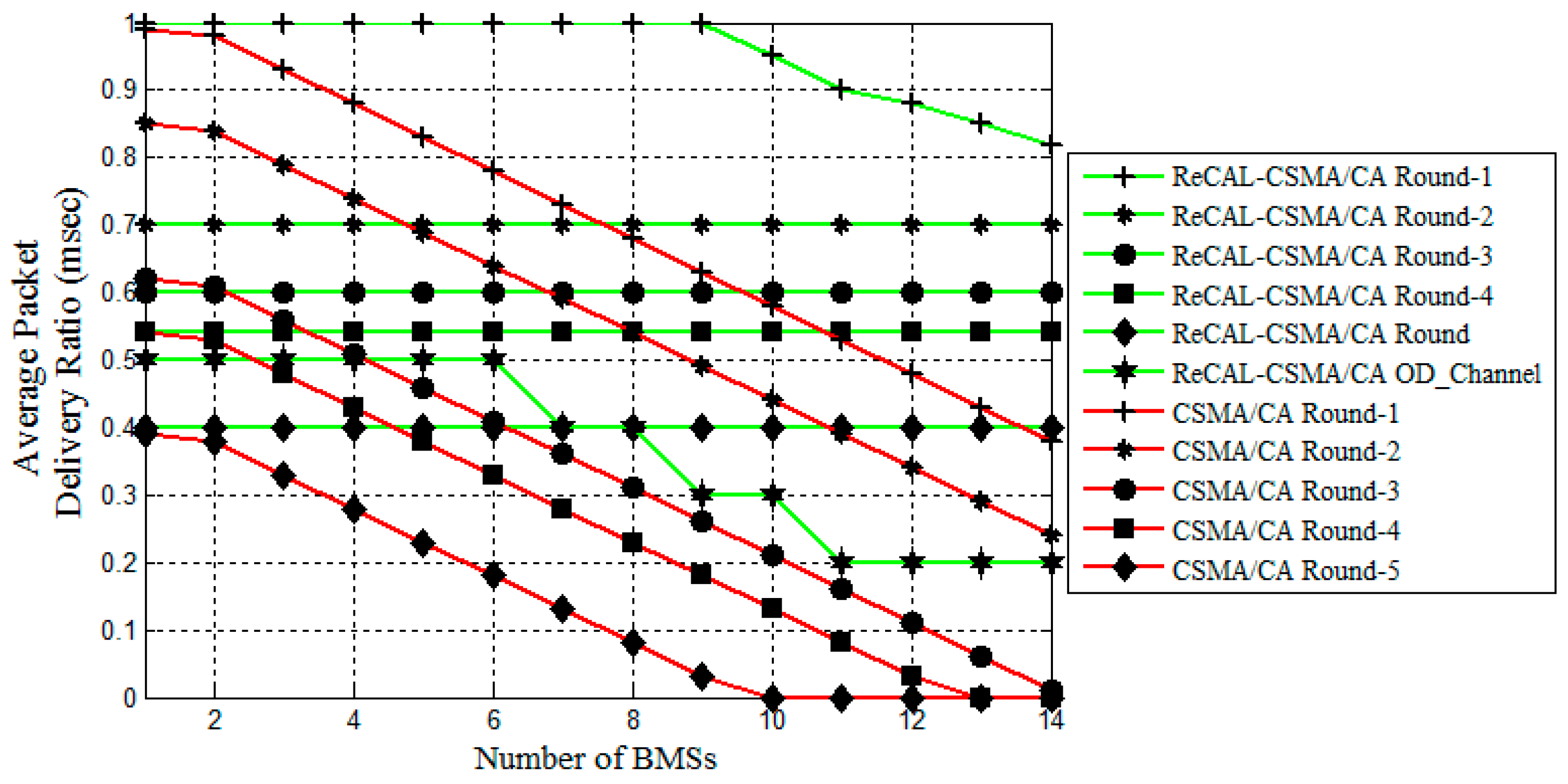
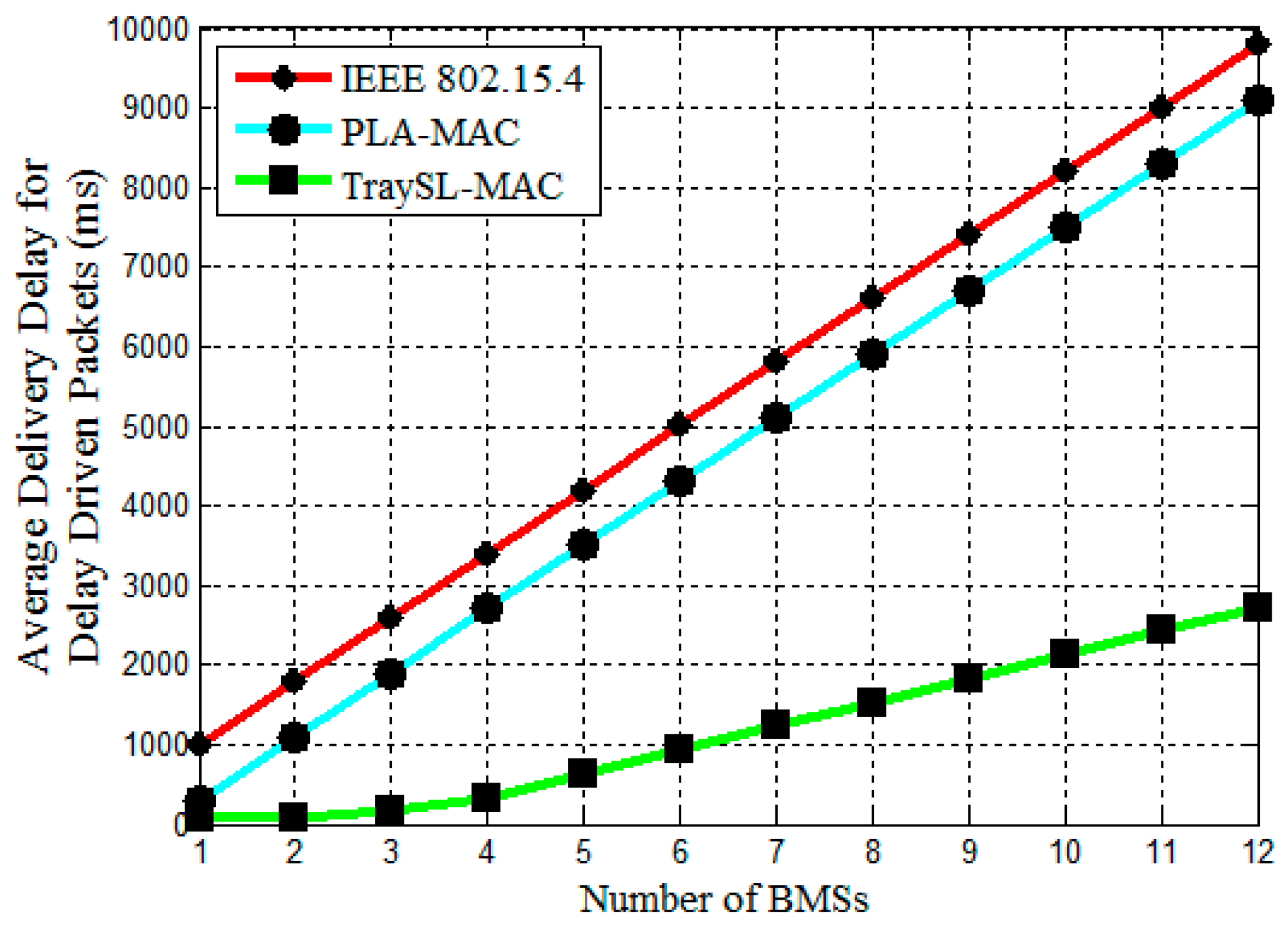
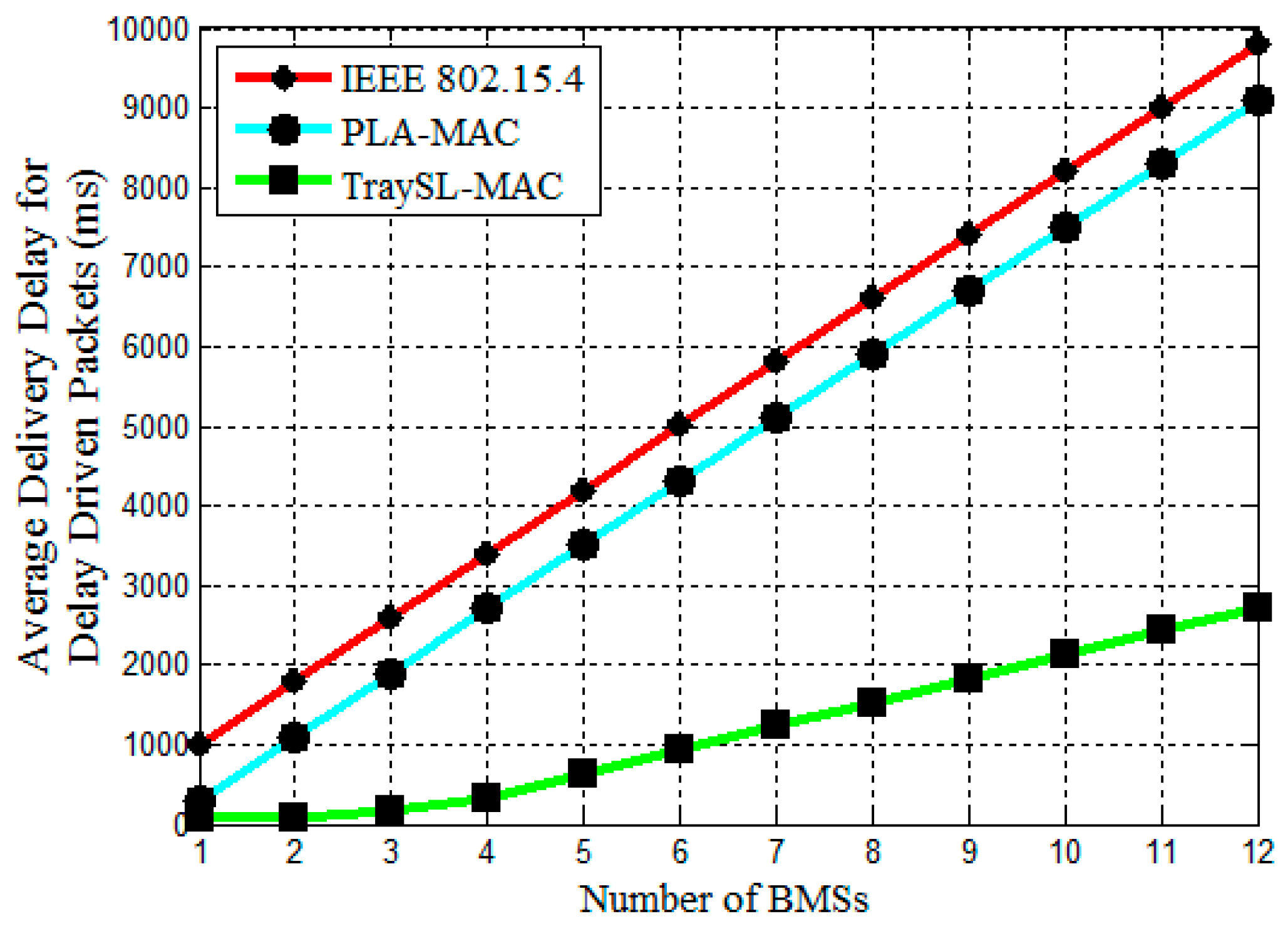
4.2.2. Analysis of Delivery Delay for Delay Driven Packets
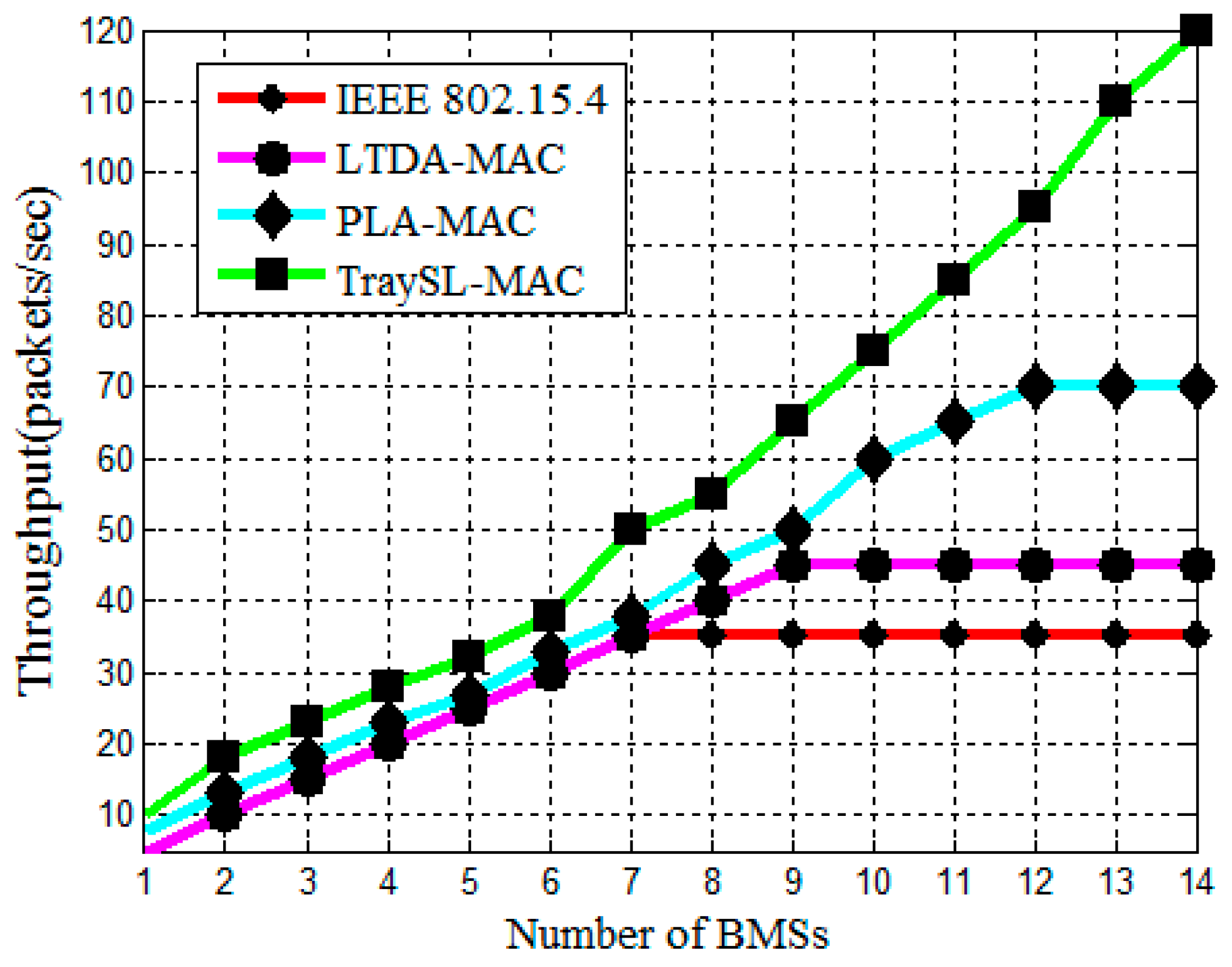
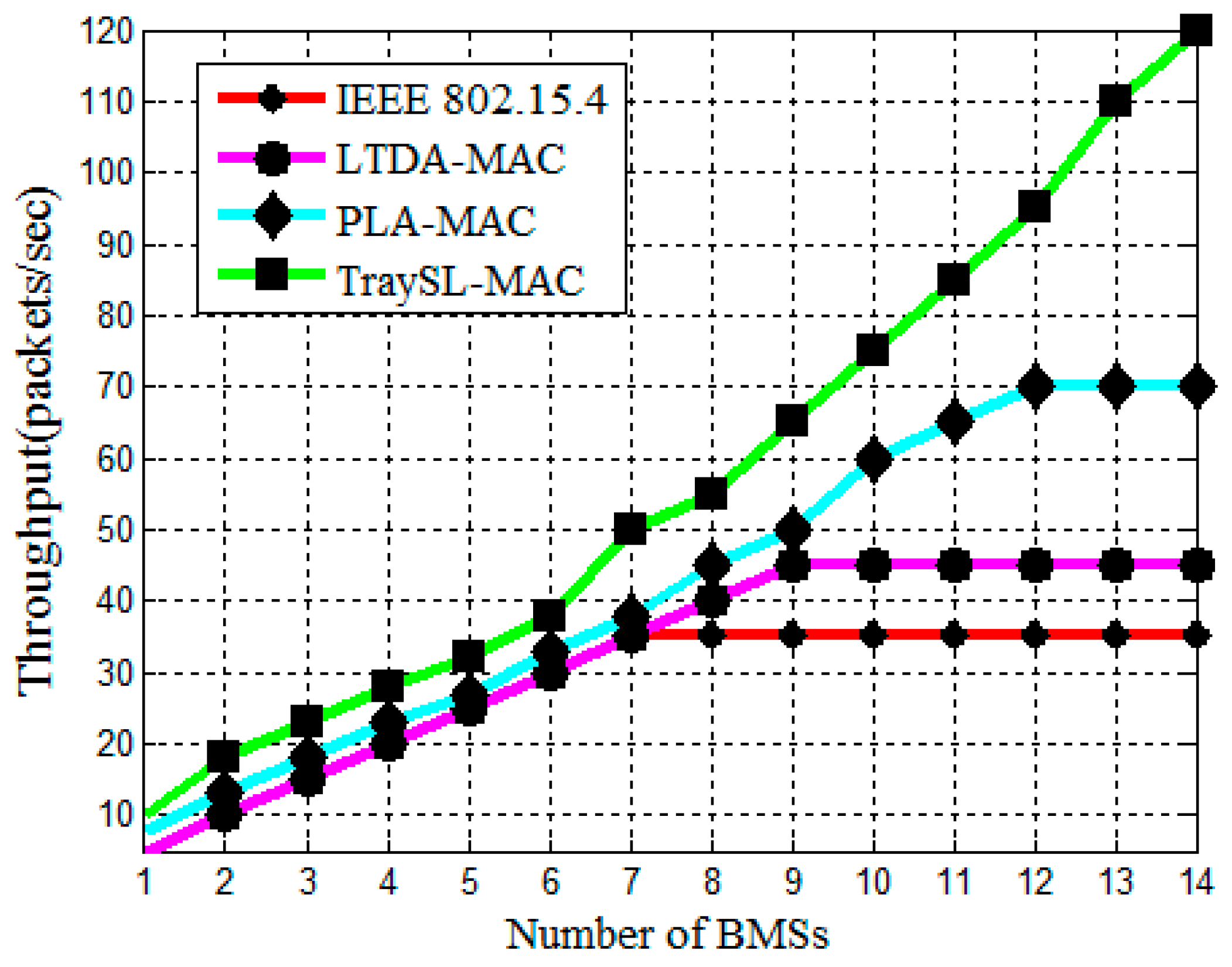
4.2.3. Analysis of Throughput
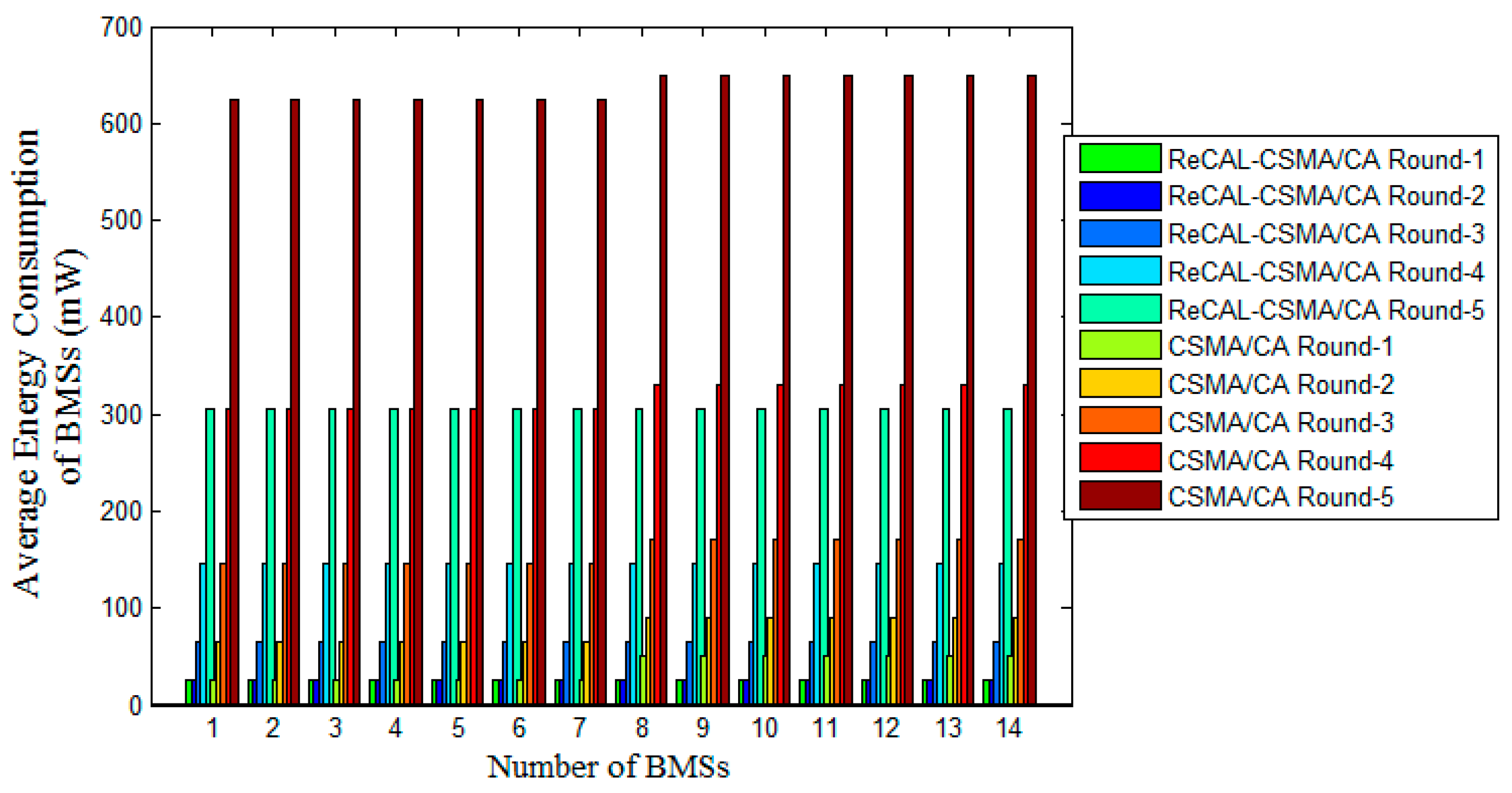
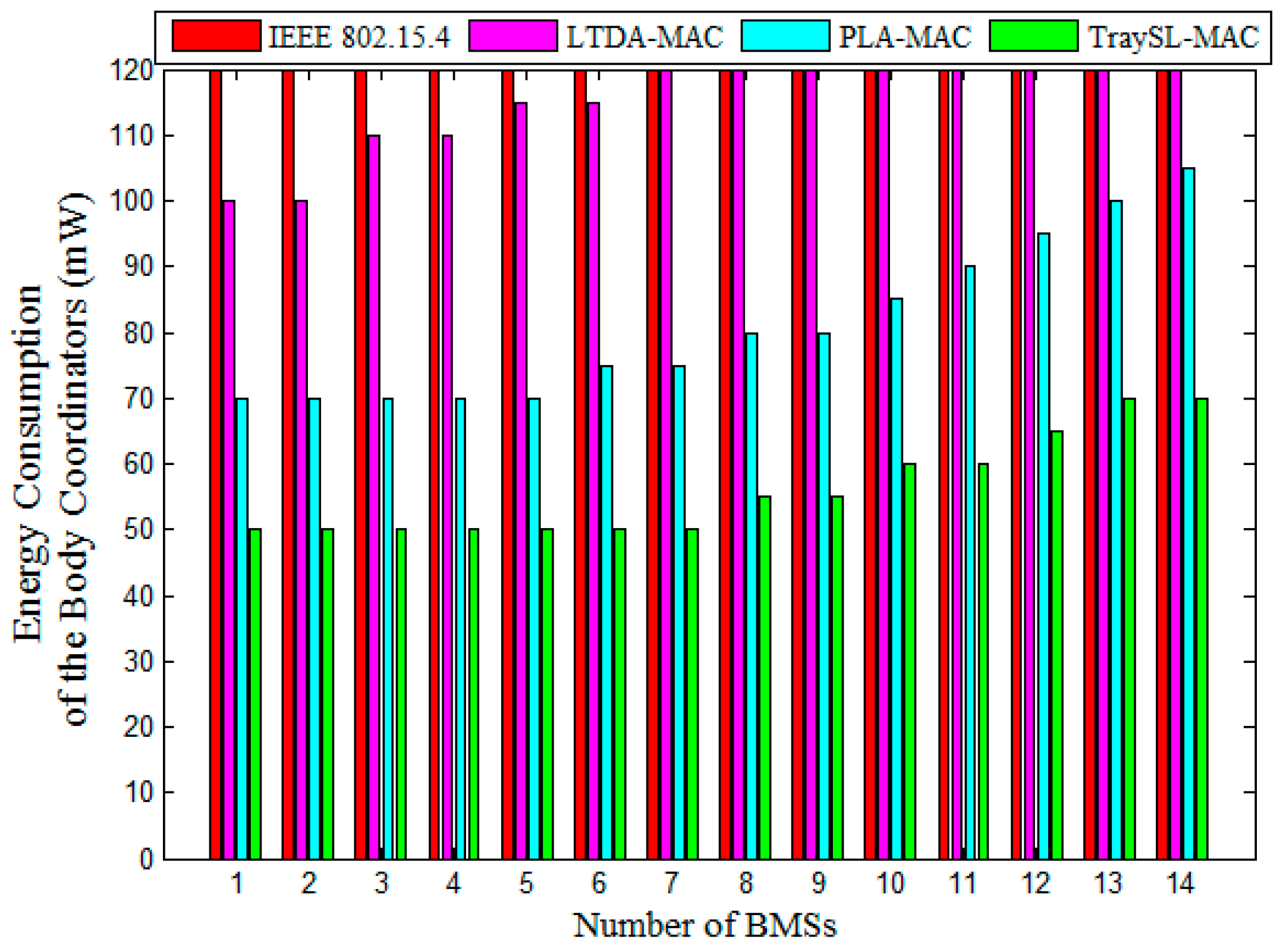
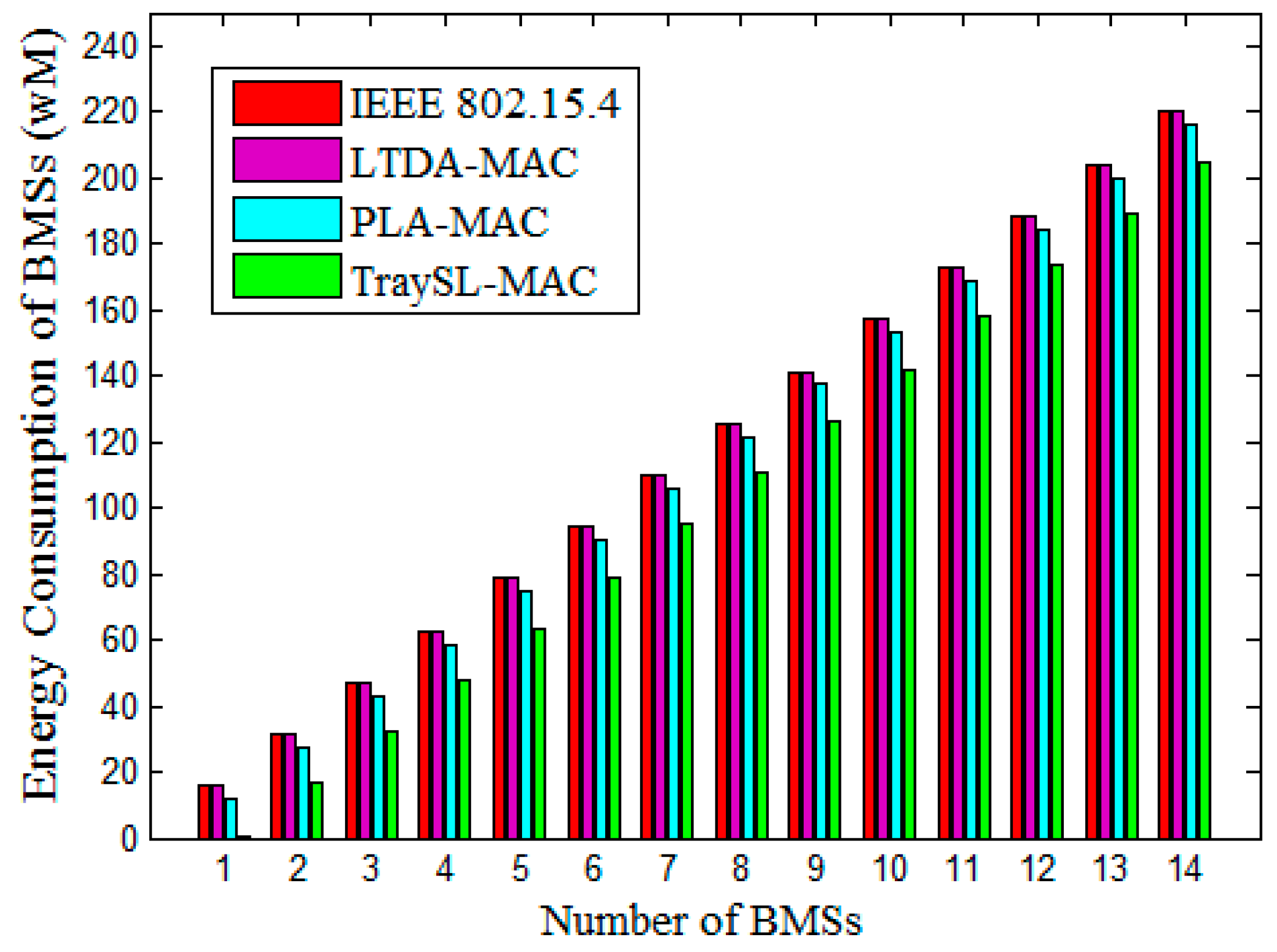
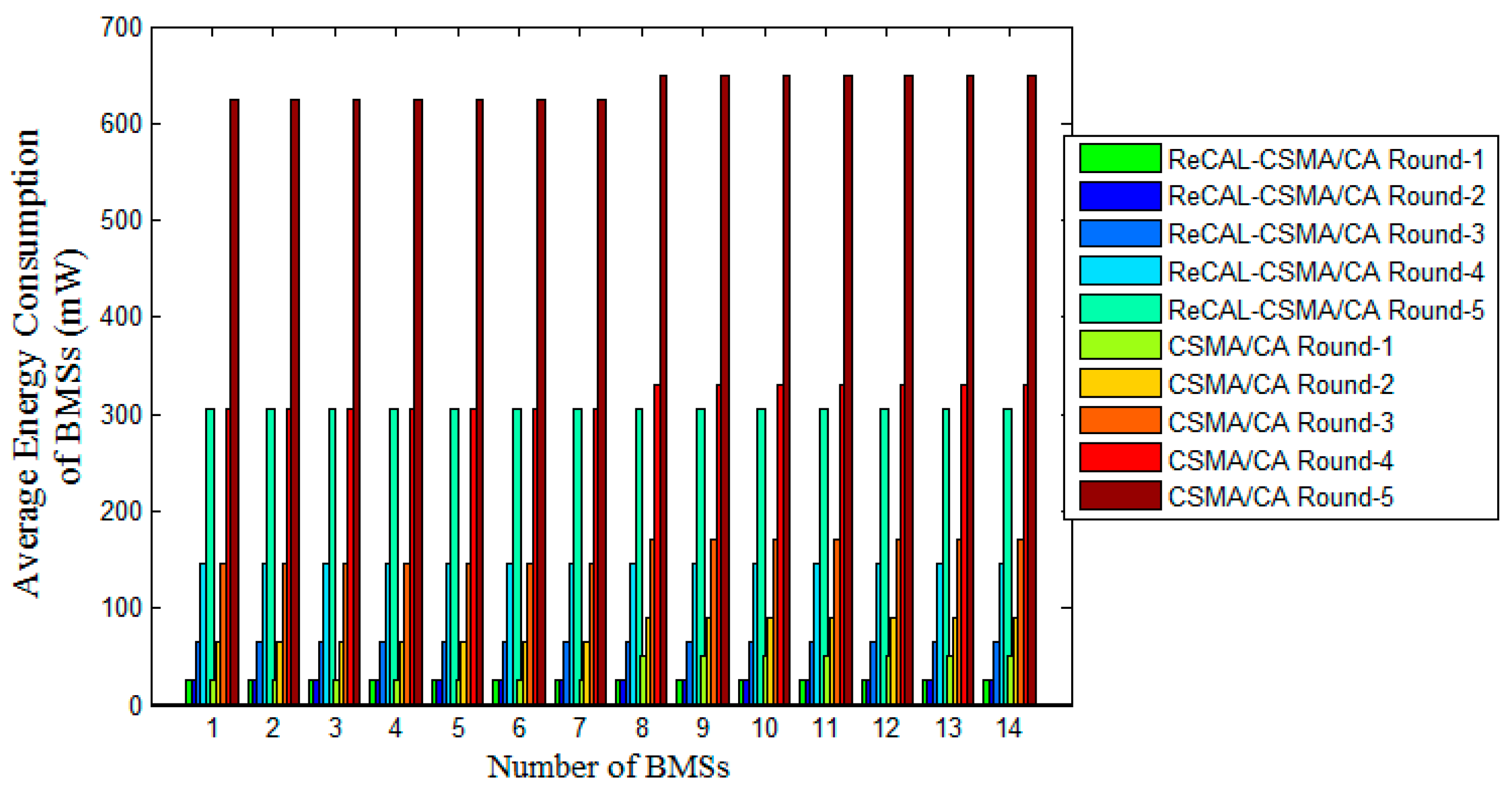
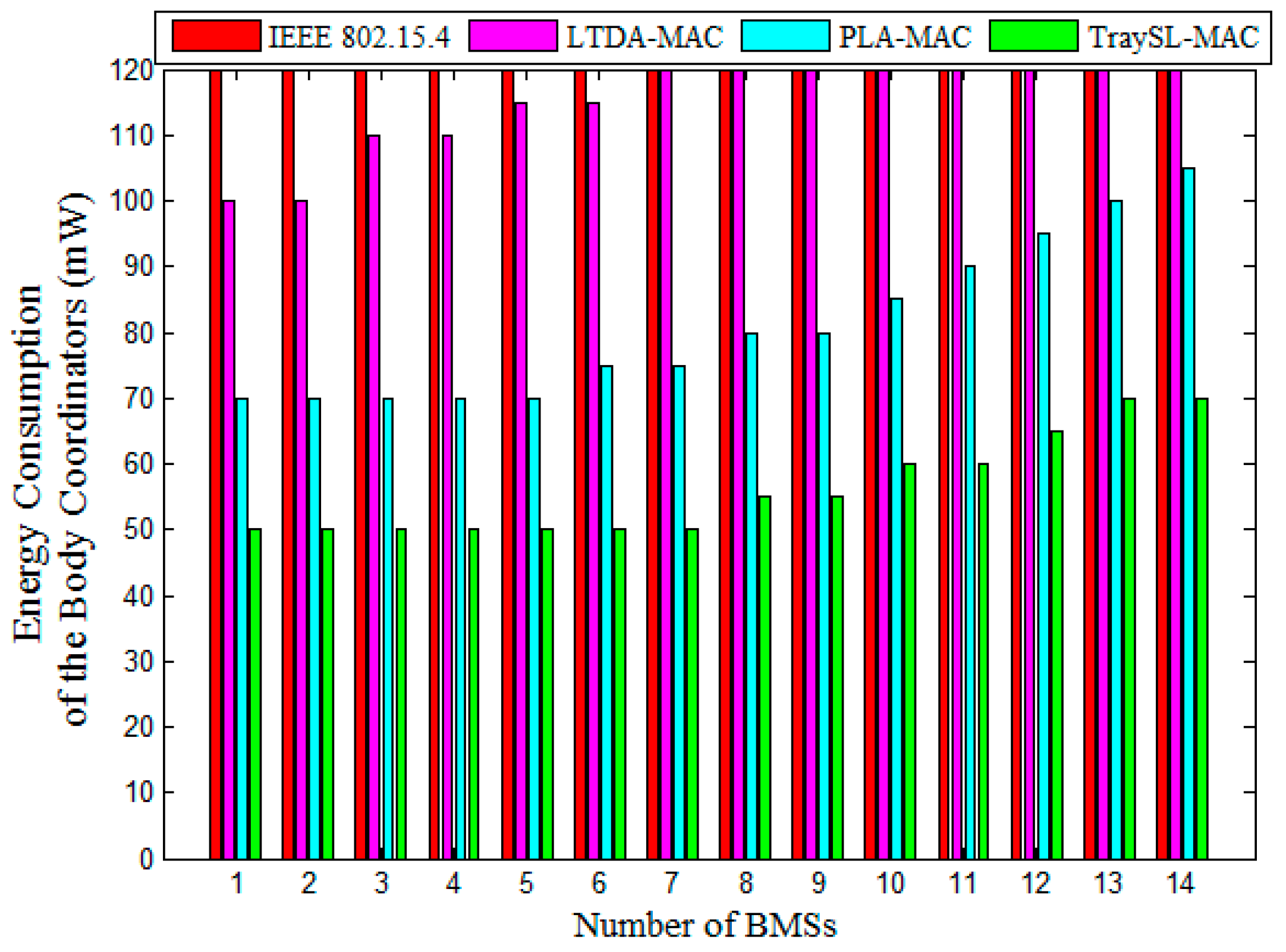
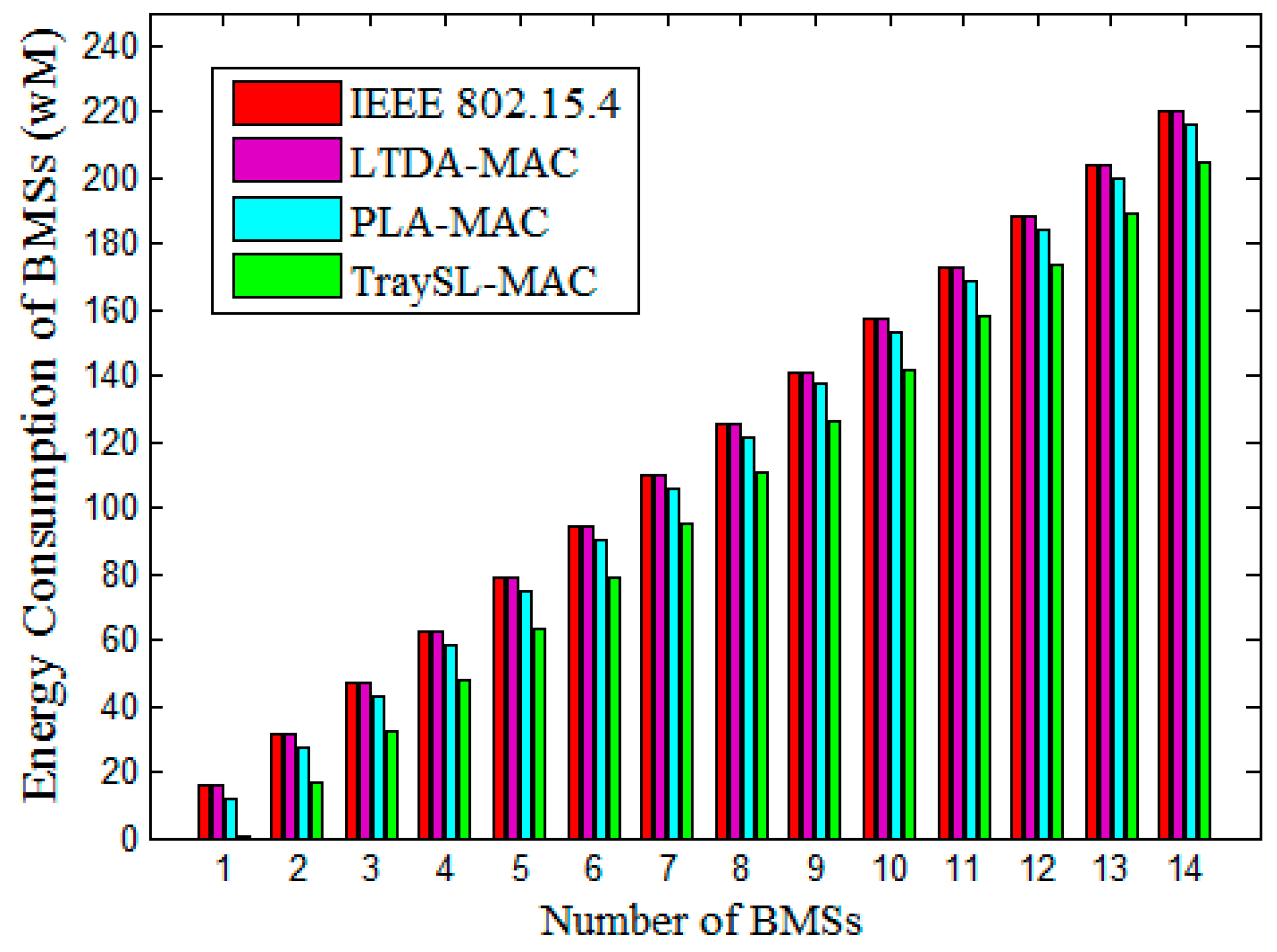
4.2.4. Analysis of Energy Consumption
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Yu, L.; Guo, L.; Deng, H.; Lin, K.; Yu, L.; Gao, W.; Saeed, I.A. Research on Continuous Vital Signs Monitoring Based on WBAN. In Proceedings of the International Conference on Smart Homes and Health Telematics, Wuhan, China, 25–27 May 2016; pp. 371–382.
- Chen, M.; Member, S.; Wan, J.; Gonz, S.; Liao, X.; Leung, V.C.M. A Survey of Recent Developments in Home M2M Networks. IEEE Commun. Surv. Tutor. 2014, 16, 98–114. [Google Scholar] [CrossRef]
- Alam, M.M.; Hamida, E.B. Surveying wearable human assistive technology for life and safety critical applications: Standards, challenges and opportunities. Sensors 2014, 14, 9153–9209. [Google Scholar] [CrossRef] [PubMed]
- Quwaider, M.; Biswas, S. Probabilistic Routing in on-Body Sensor Networks with Postural Disconnections. In Proceedings of the 7th ACM international symposium on Mobility management and wireless access (MobiWAC ’09), Canary Islands, Spain, 27–30 October 2009; pp. 149–158.
- Chakraborty, C.; Gupta, B.; Ghosh, S.K. Tele-Wound Monitoring through Smartphone. In Proceedings of the 2014 International Conference on Medical Imaging, m-Health and Emerging Communication Systems (MedCom), Greater Noida, India, 7–8 November 2014; pp. 197–201.
- Kumar, P.; Lee, H.-J. Security issues in healthcare applications using wireless medical sensor networks: A survey. Sensors 2012, 12, 55–91. [Google Scholar] [CrossRef] [PubMed]
- IEEE 802.15.4. IEEE Standard for Information Technology 802.15.4, Wireless Medium Access Control (MAC) and Physical Layer (PHY) Specifications for Low-Rate Wireless Personal Area Networks (LR-WPANs); The Institue of Electrical and Electronics Engineers, Inc.: New York, NY, USA, 2006; Volume 2006. [Google Scholar]
- Okdem, S. A real-time noise resilient data link layer mechanism for unslotted IEEE 802.15.4 networks. Int. J. Commun. Syst. 2017, 30, e2955. [Google Scholar] [CrossRef]
- Shu, M.; Yuan, D.; Zhang, C.; Wang, Y.; Chen, C. A MAC Protocol for Medical Monitoring Applications of Wireless Body Area Networks. Sensors 2015, 15, 12906–12931. [Google Scholar] [CrossRef] [PubMed]
- Anjum, I.; Alam, N.; Razzaque, M.A.; Hassan, M.M.; Alamri, A. Traffic Priority and Load Adaptive MAC Protocol for QoS Provisioning in Body Sensor Networks. Int. J. Distrib. Sens. Netw. 2013, 2013, 1–9. [Google Scholar] [CrossRef]
- Yoon, J.S.; Ahn, G.-S.; Joo, S.-S.; Lee, M.J. PNP-MAC: Preemptive Slot Allocation and Non-Preemptive Transmission for Providing QoS in Body Area Networks. In Proceedings of the 2010 7th IEEE Consumer Communications and Networking Conference, Las Vegas, NV, USA, 9–12 January 2010; pp. 1–5.
- Li, C.; Hao, B.; Zhang, K.; Liu, Y.; Li, J. A novel medium access control protocol with low delay and traffic adaptivity for wireless body area networks. J. Med. Syst. 2011, 35, 1265–1275. [Google Scholar] [CrossRef] [PubMed]
- Rezvani, S.; Ghorashi, S.A. Context aware and channel-based resource allocation for wireless body area networks. IET Wirel. Sens. Syst. 2013, 3, 16–25. [Google Scholar] [CrossRef]
- Nepal, S.; Pudasaini, A.; Pyun, J.; Hwang, S.; Lee, C.G.; Shin, S. A New MAC Protocol for Emergency Handling in Wireless Body Area Networks. In Proceedings of the 2016 Eighth International Conference on Ubiquitous and Future Networks (ICUFN), Vienna, Austria, 5–8 July 2016; pp. 588–590.
- Bhandari, S.; Moh, S. A Priority-Based Adaptive MAC Protocol for Wireless Body Area Networks. Sensors 2016, 16, 401. [Google Scholar] [CrossRef] [PubMed]
- IEEE 802.11. Available online: http://ieee802.org/11/ (accessed on 17 Octobar 2016).
- IEEE 802.15 WPAN. Available online: http://www.ieee802.org/15/pub/index_TG3e.html (accessed on 26 November 2016).
- Rashwand, S.; Mišić, J. Effects of access phases lengths on performance of IEEE 802.15.6 CSMA/CA. Comput. Netw. 2012, 56, 2832–2846. [Google Scholar] [CrossRef]
- Ullah, S.; Higgins, H.; Shen, B.; Kwak, K.S. On the implant communication and MAC protocols for WBAN. Commun. Syst. 2010, 23, 982–999. [Google Scholar] [CrossRef]
- Qadri, S.F.; Awan, S.A.; Amjad, M.; Anwar, M.; Shehzad, S. Applications, Challenges, Security of Wireless Body Area Networks (Wbans) and Functionality of IEEE 802.15.4/ZIGBEE. Sci. Int. Lahore 2013, 25, 697–702. [Google Scholar]
- Khan, Z.A.; Rasheed, M.B.; Javaid, N.; Robertson, B. Effect of Packet Inter-arrival Time on the Energy Consumption of Beacon Enabled MAC Protocol for Body Area Networks. Procedia Comput. Sci. 2014, 32, 579–586. [Google Scholar] [CrossRef]
- Xia, F.; Hao, R.; Li, J.; Xiong, N.; Yang, L.T.; Zhang, Y. Adaptive GTS allocation in IEEE 802.15.4 for real-time wireless sensor networks. J. Syst. Arch. 2013, 59, 1231–1242. [Google Scholar] [CrossRef]
- Zhou, J.; Guo, A.; Xu, J.; Su, S. An optimal fuzzy control medium access in wireless body area networks. Neurocomputing 2014, 142, 107–114. [Google Scholar] [CrossRef]
- Shuai, J.; Zou, W.; Zhou, Z. Priority-Based Adaptive Timeslot Allocation Scheme for Wireless Body Area Network. In Proceedings of the 2013 13th International Symposium on Communications and Information Technologies (ISCIT), Surat Thani, Thailand, 4–6 September 2013; pp. 609–614.
- Li, C.; Zhang, B.; Yuan, X.; Ullah, S.; Vasilakos, A.V. MC-MAC: A multi-channel based MAC scheme for interference mitigation in WBANs. Wirel. Netw. 2016, 1–15. [Google Scholar] [CrossRef]
- Yuan, X.; Li, C.; Yang, L.; Yue, W.; Zhang, B.; Ullah, S. A token-based dynamic scheduled MAC protocol for health monitoring. EURASIP J. Wirel. Commun. Netw. 2016, 2016, 1–18. [Google Scholar] [CrossRef]
- Sarkar, S.; Misra, S. From Micro to Nano: The Evolution of Wireless Sensor-Based Health Care. IEEE Pulse 2016, 7, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Ullah, S.; Shen, B.; Islam, S.M.R.; Khan, P.; Saleem, S.; Kwak, K.S. A study of MAC protocols for WBANs. Sensors 2010, 10, 128–145. [Google Scholar] [CrossRef]
- Naranjo-Hernández, D.; Roa, L.M.; Reina-Tosina, J.; Estudillo-Valderrama, M.A.; Barbarov, G. Low-Power Platform and Communications for the Development of Wireless Body Sensor Networks. Int. J. Distrib. Sens. Netw. 2015, 2015, 1–13. [Google Scholar] [CrossRef]
- Djenouri, D.; Balasingham, I. New QoS and Geographical Routing in Wireless Biomedical Sensor Networks. In Proceedings of the 6th International ICST Conference on Broadband Communications, Networks, and Systems, Madrid, Spain, 14–16 September 2009; pp. 1–8.
- Fletcher, G.F.; Ades, P.A.; Kligfield, P.; Arena, R.; Balady, G.J.; Bittner, V.A.; Coke, L.A.; Fleg, J.L.; Forman, D.E.; Gerber, T.C.; et al. Exercise Standards for Testing and Training: A Scientific Statement From the American Heart Association. Circulation 2013, 128, 873–934. [Google Scholar] [CrossRef] [PubMed]
- Guazzi, M.; Arena, R.; Halle, M.; Piepoli, M.F.; Myers, J.; Lavie, C.J. 2016 Focused Update: Clinical Recommendations for Cardiopulmonary Exercise Testing Data Assessment in Specific Patient Populations. Circulation 2016, 133, e694–e711. [Google Scholar] [CrossRef] [PubMed]
- WebMD. Counting Respiration Rate. 2016. Available online: http://www.webmd.com/lung/counting-respiration-rate (accessed on 10 Octobar 2016).
- WikiHow. Breathing Rate (Rate of Respiration). 2016. Available online: http://www.wikihow.com/Check-Someone’s-Breathing-Rate-(Rate-of-Respiration) (accessed on 2 November 2016).
- Advisor, N.H. Blood_Pressure_Equation. 2016. Available online: http://www.newhealthadvisor.com/blood-pressure-equation.html (accessed on 25 November 2016).
- Ready, P.; Steady, P. How various medications affect the blood pressure equation. 2016. Available online: http://cardeneiv.com/c2_cardeneiv_ov_ma.shtml (accessed on 18 December 2016).
- Tutorvista. Temperature Formula. 2016. Available online: http://formulas.tutorvista.com/physics/temperature-formula.html (accessed on 15 Demeber 2016).
- WebMD. Body Temperature. 2016. Available online: http://www.webmd.com/first-aid/body-temperature?page=6 (accessed on 18 November 2016).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vital Sign | Normal Values | Low Values | High Values | ||
|---|---|---|---|---|---|
| Low1 (L1) | Low2 (L2) | High1 (H1) | High2 (H2) | ||
| HR | 51–119 beats/min | 0–25 beats/min | 26–50 beats/min | 141–180 beats/min | 120–140 beats/min |
| RR | 12–19 breaths/min | 0–6 breaths/min | 7–11 breaths/min | 41–60 breaths/min | 20–40 breaths/min |
| BP (Systolic/Diastolic) mm Hg | (90–120)/(60–80) | (70–90)/(40–60) | (140–190)/(90–100) | ||
| Temperature | 37 °C | N/A | 40 °C & above | 38 °C to 39.9 °C | |
| Parameter | Value | Parameter | Value |
|---|---|---|---|
| Operating Carrier Frequency | 2.4 GHz | aBaseSlot_Duration | 60 symbols |
| Channel Rate | 250 kbps | Sending Data Rates | 20 kbps |
| Number of channels in the proposed TraySL-MAC and PLA-MAC Superframe structure | 128 | MAC Payload size | 1920 bytes |
| Number of channels in IEEE 802.15.4 and LTDA-MAC | 16 and 32 | Buffer size of the Body Coordinator | 2000 bytes |
| BO set for all MAC protocols | 10 | Buffer size of a BMS | 1920 bytes |
| SO set for all MAC protocols | 9 | Max PHY Packet Size | 127 bytes |
| A Slot Duration | 1.536 s | TurnaroundTime | 12 Symbols |
| CCA Time | 8 symbols | UnitBackoffPeriod | 20 symbols |
| Max Frame Retries | 4 | macAckWaitDuration | 54 |
| Carrier sense sensitivity | −97 mW | macMinBE—for Standard IEEE 802.15.4 | 3 |
| Receiver sense sensitivity | −97 mW | BI in seconds | 393.216 s |
| Time of Superframe Duration (SD) | 196.608 s | BI in Symbols | 7864320 symbols |
| Low data generation rate | 0.5 ms | Data generation rate | 1.5 ms |
| Traffic Type | CBR | Power Consumed in Sleep state | 0.005 mW |
| Power Consumed in Transmission state | 27–220 mW | Power Consumed in Receive state | 1.8 mW |
| Duration of Turn-On radio to Transmit/Receive data | 0.8 ms | Power required for radio to switch from transmitting state to receive state & vice versa | 0.4 ms |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ullah, F.; Abdullah, A.H.; Kaiwartya, O.; Arshad, M.M. Traffic Priority-Aware Adaptive Slot Allocation for Medium Access Control Protocol in Wireless Body Area Network. Computers 2017, 6, 9. https://doi.org/10.3390/computers6010009
Ullah F, Abdullah AH, Kaiwartya O, Arshad MM. Traffic Priority-Aware Adaptive Slot Allocation for Medium Access Control Protocol in Wireless Body Area Network. Computers. 2017; 6(1):9. https://doi.org/10.3390/computers6010009
Chicago/Turabian StyleUllah, Fasee, Abdul Hanan Abdullah, Omprakash Kaiwartya, and Marina Md Arshad. 2017. "Traffic Priority-Aware Adaptive Slot Allocation for Medium Access Control Protocol in Wireless Body Area Network" Computers 6, no. 1: 9. https://doi.org/10.3390/computers6010009
APA StyleUllah, F., Abdullah, A. H., Kaiwartya, O., & Arshad, M. M. (2017). Traffic Priority-Aware Adaptive Slot Allocation for Medium Access Control Protocol in Wireless Body Area Network. Computers, 6(1), 9. https://doi.org/10.3390/computers6010009