
Application of Augmented Reality Interventions for Children with Autism Spectrum Disorder (ASD): A Systematic Review

 ,
,
Abstract
:1. Introduction
1.1. Research Question and Objects
- Systematically review the existing literature on augmented reality interventions for children with autism spectrum disorder (ASD);
- Evaluate the effectiveness of augmented reality interventions in rehabilitating and training individuals with ASD across various domains, including social interaction, emotion recognition, cooperation, learning, cognitive skills, and living skills;
- Identify the strengths and limitations of the current research designs, control groups, sample sizes, and assessment and feedback methods used in the reviewed studies.
1.2. Contributions and Organization
- We conducted a systematic search for studies evaluating the types of intervention on the ASD population and analyze the efficacy of AR intervention on a variety of functions, such as social and communication, emotion management, daily living, and cognitive skills;
- We discussed the limitations and future works of the existing research.
2. A Brief Overview of The Related Concepts
2.1. Autism Spectrum Disorder
2.2. Augmented Reality
3. Methodology
3.1. Search Strategy and Data Sources
3.2. Search Strings
3.3. Inclusion and Exclusion Criteria
3.4. Data Extraction
4. Results
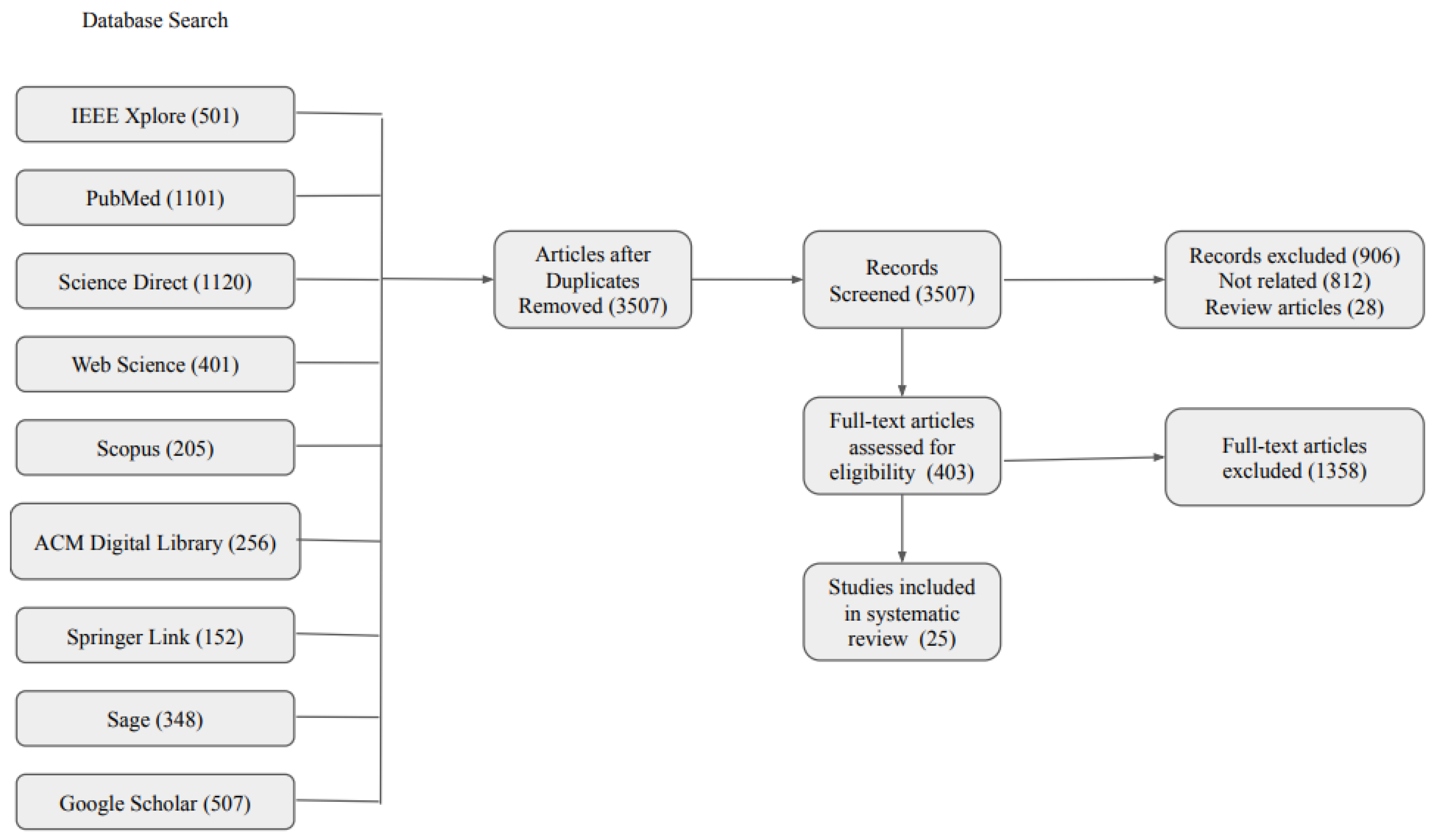
4.1. Data Selection
4.2. Descriptive Characteristics of The Selected Studies
4.2.1. System Protocol Design
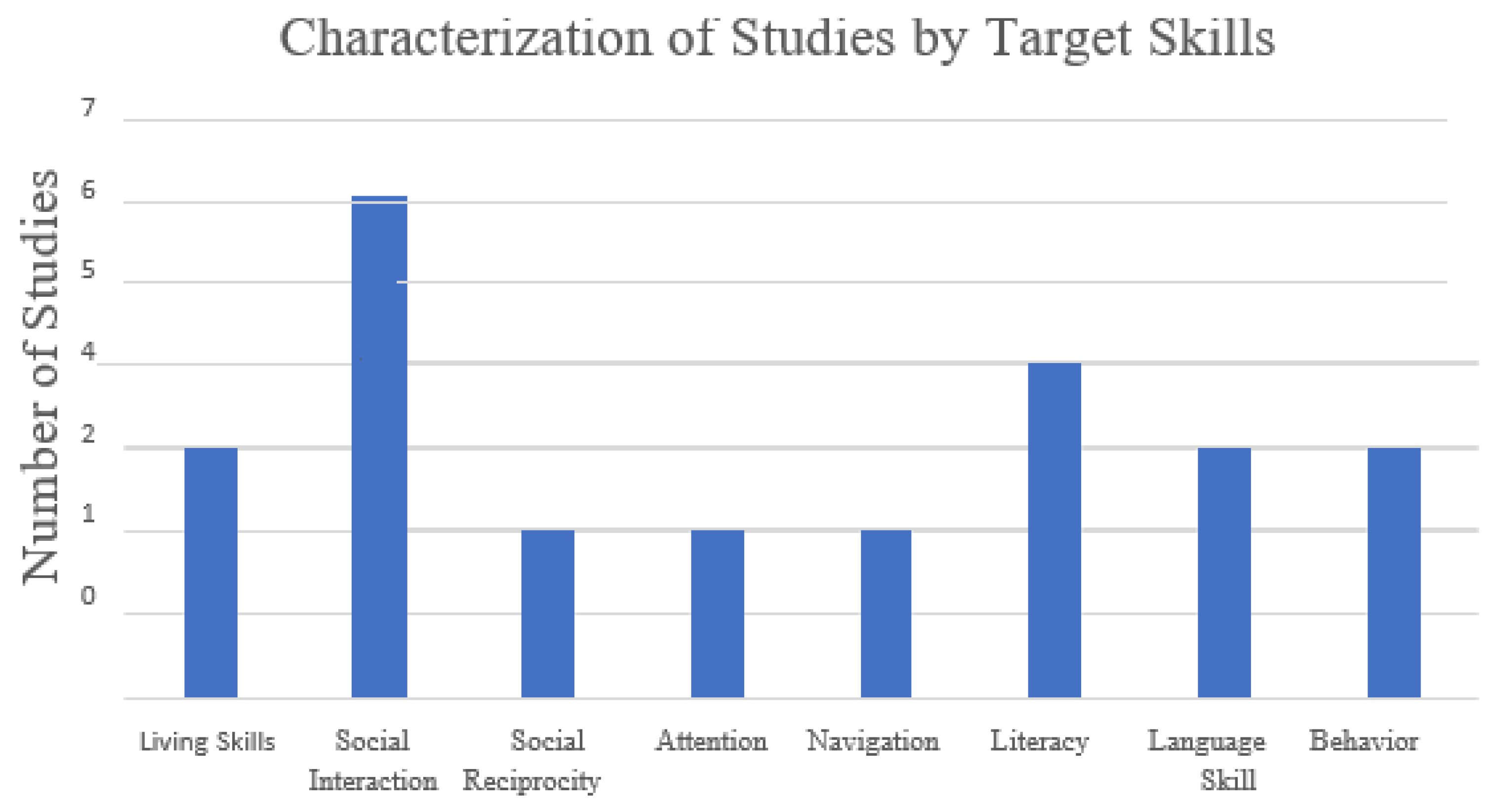
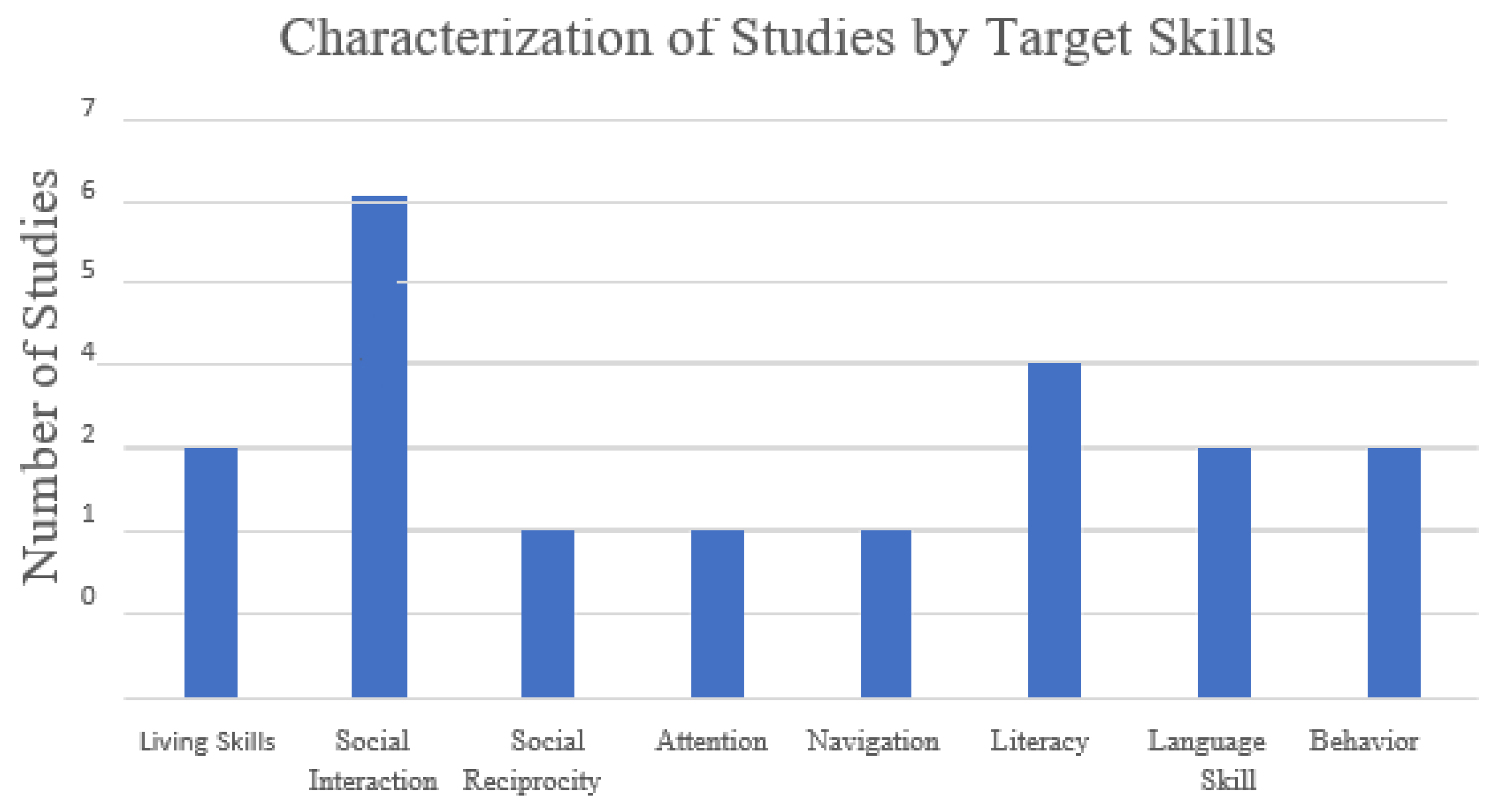
4.2.2. Target Skills
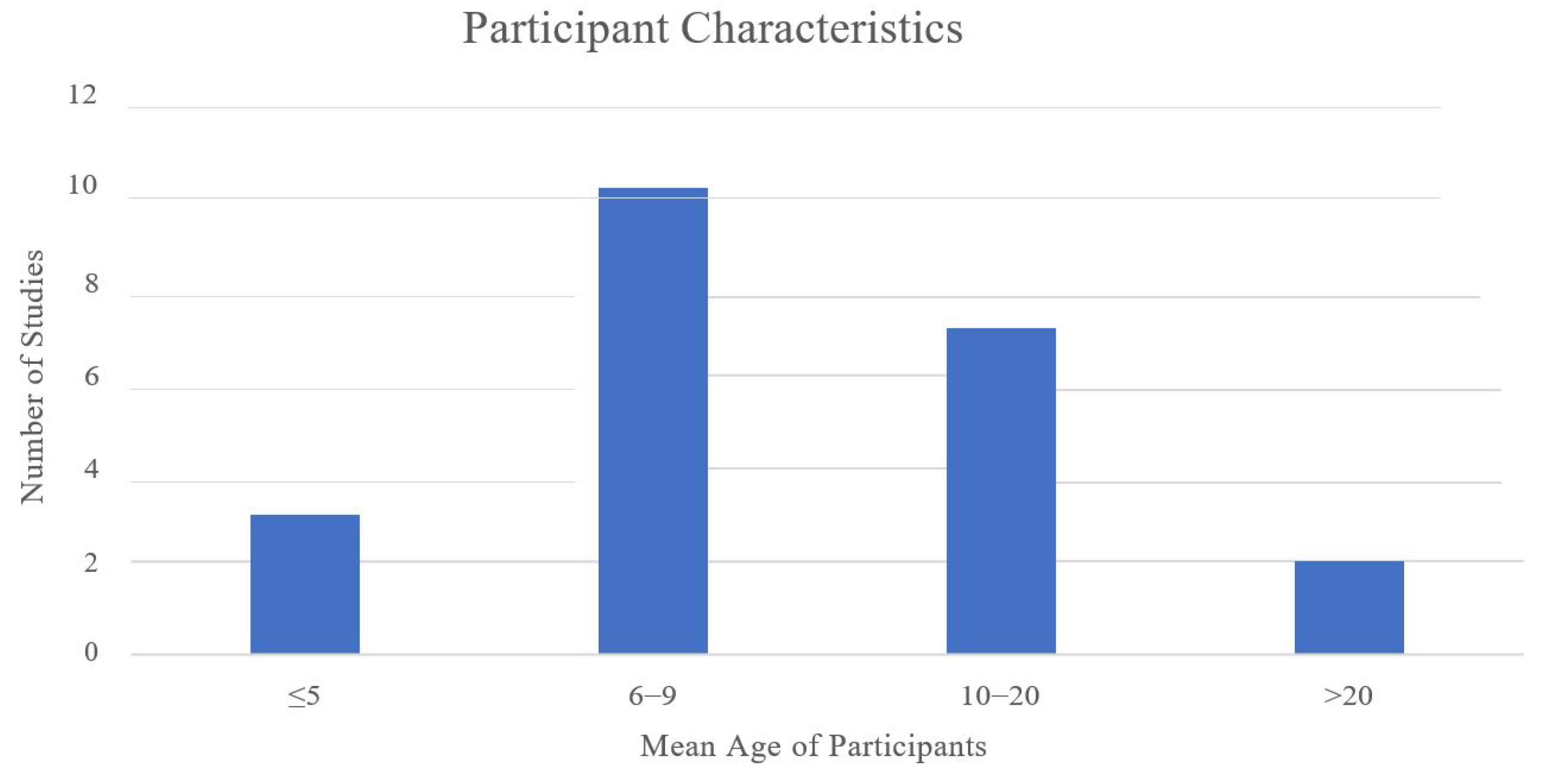
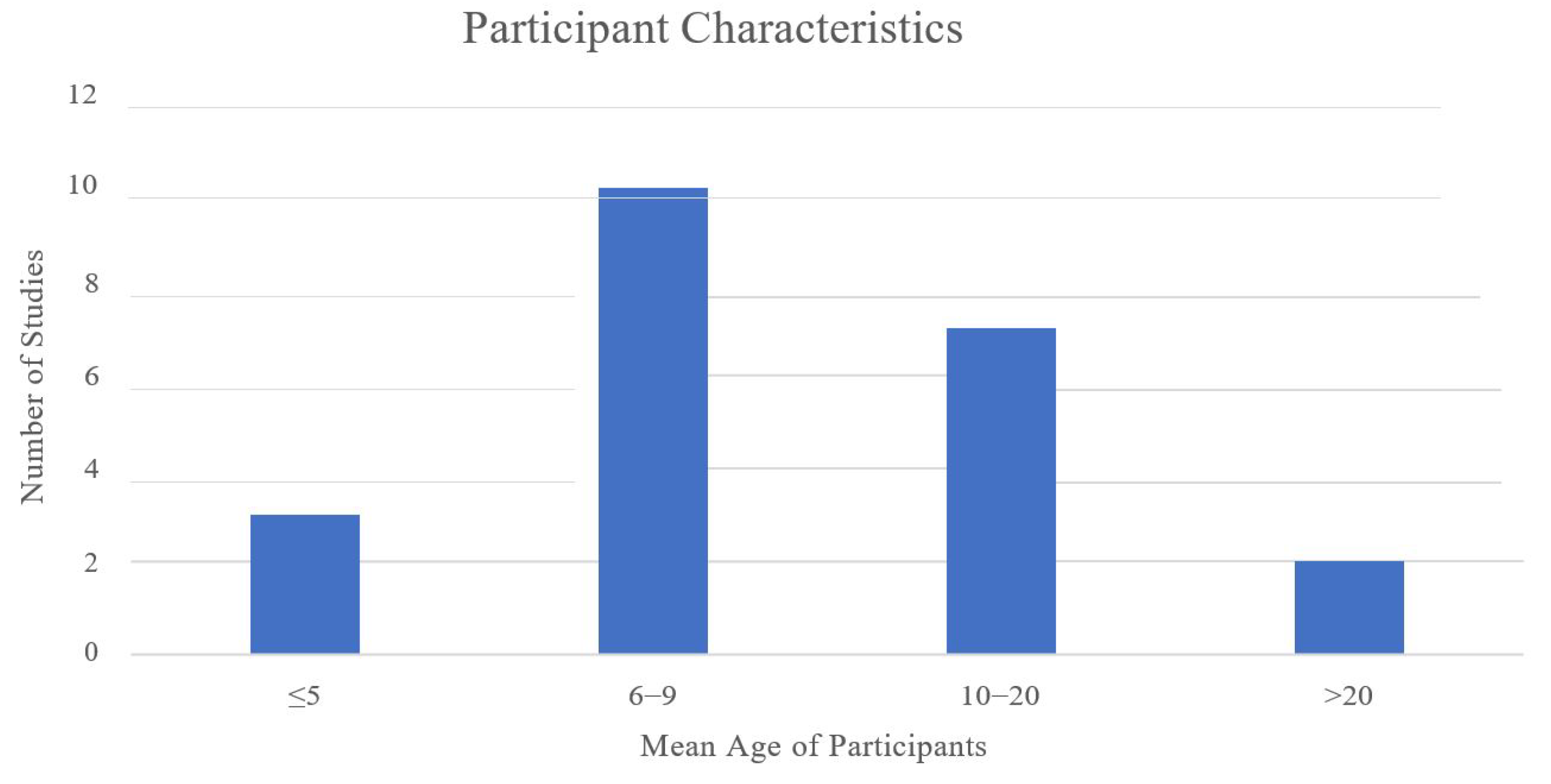
4.2.3. Participant Characteristics
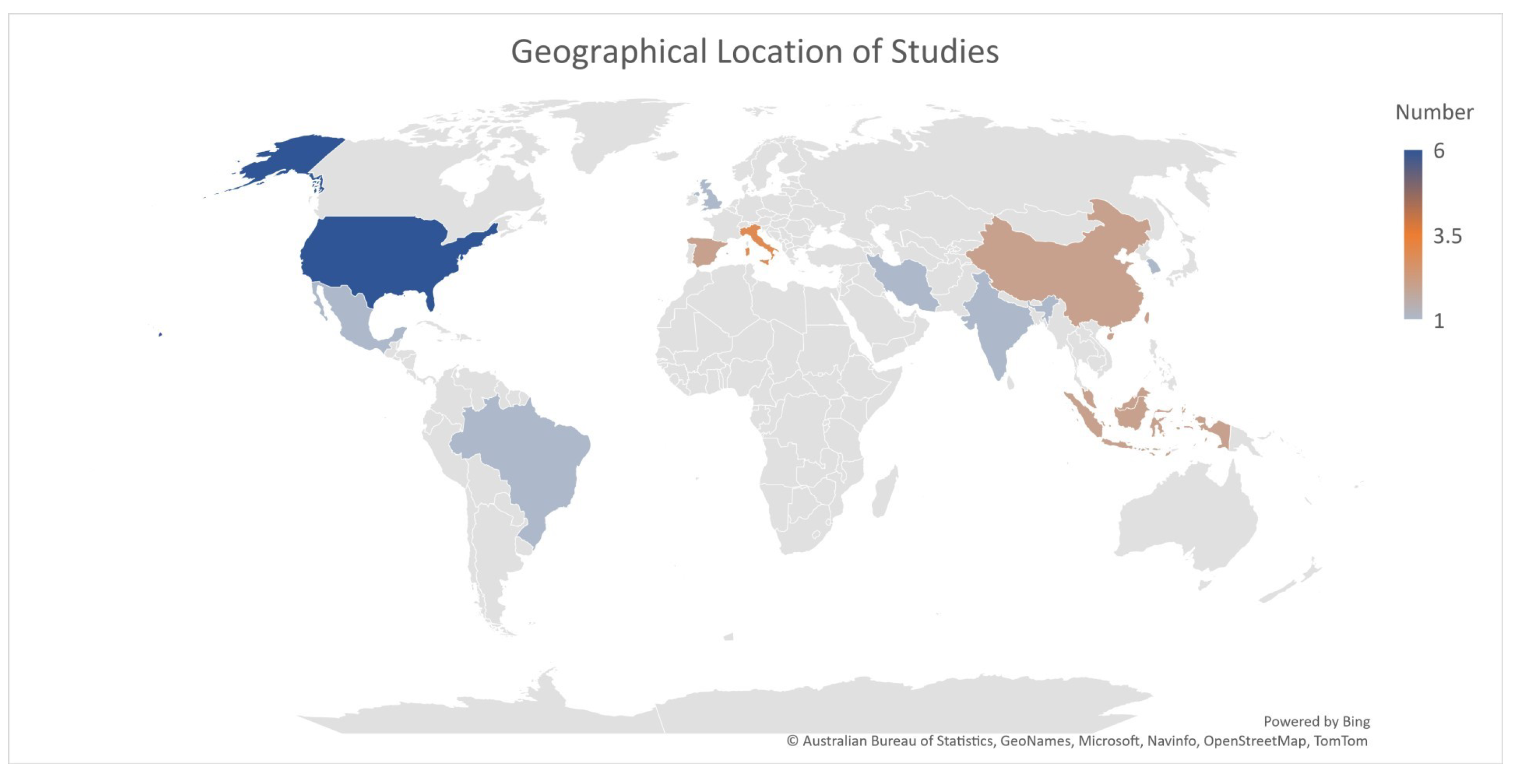
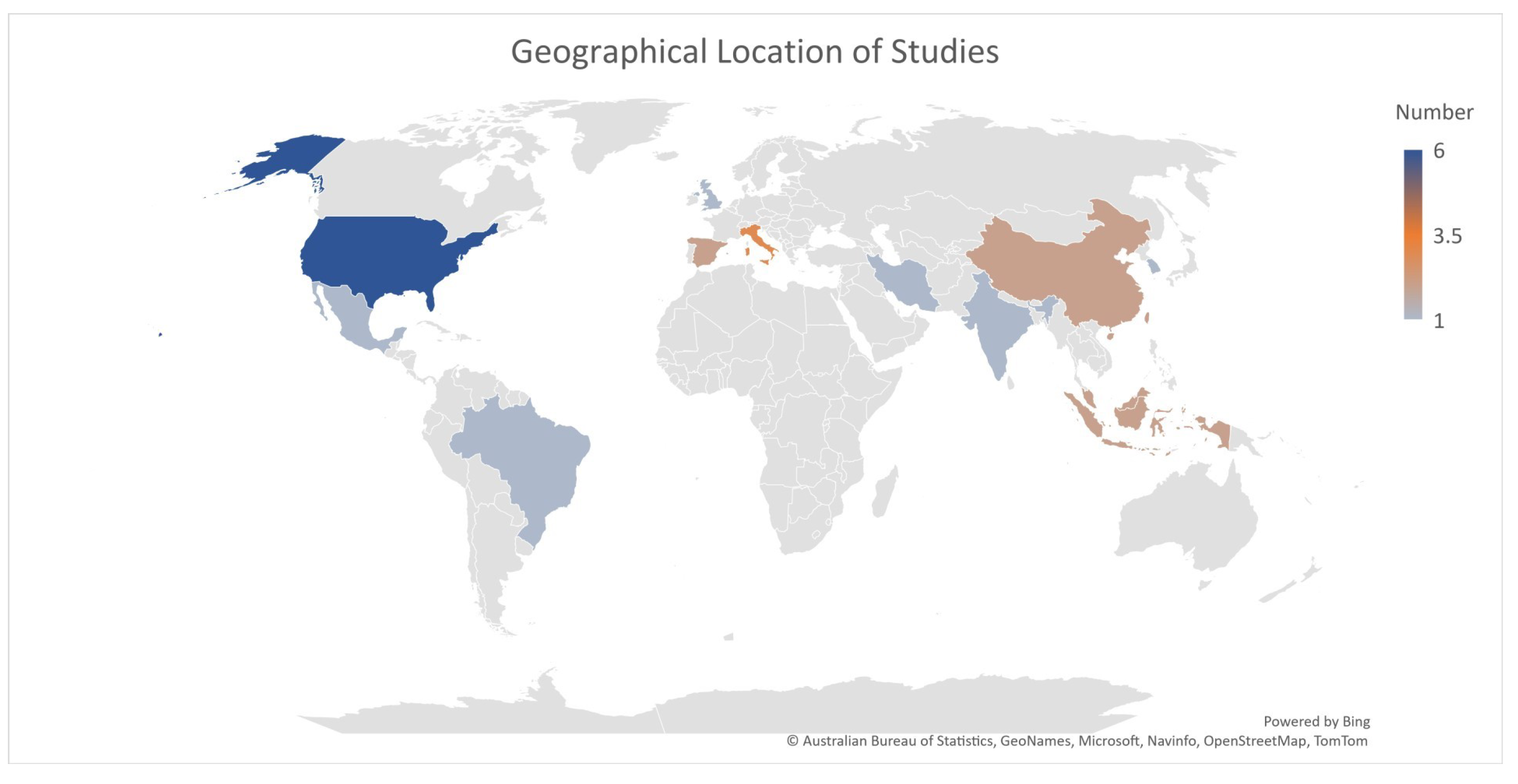
4.2.4. Region of Experimentation
4.2.5. Quality Assessment of the Articles
5. Discussion
6. Conclusions and Future Work
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| AR | Augmented Reality |
| ASD | Autism Spectrum Disorder |
| GPS | Global Positioning System |
| HCI | Human-Computer Interaction |
| ICTs | Information and Communication Technologies |
| IoT | Internet of Things |
| MAR | Mobile Augmented Reality |
| SLR | Systematic Literature Review |
| SUS | System Usability Scale |
| PHR | Personal Health Record |
| TBI | Technology-based Intervention |
| VM | Video Modeling |
| VR | Virtual Reality |
References
- Sharma, N.; Mishra, R.; Mishra, D. The fifth edition of diagnostic and statistical manual of mental disorders (dsm-5): What is new for the pediatrician. Indian Pediatr. 2015, 52, 141–143. [Google Scholar] [CrossRef] [PubMed]
- Zeidan, J.; Fombonne, E.; Scorah, J.; Ibrahim, A.; Durkin, M.S.; Saxena, S.; Yusuf, A.; Shih, A.; Elsabbagh, M. Global prevalence of autism: A systematic review update. Autism Res. 2022, 15, 778–790. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Meeting Report: Autism Spectrum Disorders and Other Developmental Disorders: From Raising Awareness to Building Capacity: World Health Organization, Geneva, Switzerland 16–18 September 2013; WHO: Geneva, Switzerland, 2013.
- WHO. Book Mental Health Action Plan 2013–2020; WHO: Geneva, Switzerland, 2013.
- World Health Organization. Global Technical Strategy for Malaria 2016–2030; WHO: Geneva, Switzerland, 2015.
- World Health Organization. Nurturing Care for Early Childhood Development: A Framework for Helping Children Survive and Thrive to Transform Health and Human Potential; WHO: Geneva, Switzerland, 2018.
- Eldevik, S.; Hastings, R.P.; Hughes, J.C.; Jahr, E.; Eikeseth, S.; Cross, S. Meta-analysis of early intensive behavioral intervention for children with autism. J. Clin. Child Adolesc. Psychol. 2009, 38, 439–450. [Google Scholar] [CrossRef] [PubMed]
- McConnell, S.R. Interventions to facilitate social interaction for young children with autism: Review of available research and recommendations for educational intervention and future research. J. Autism Dev. Disord. 2002, 32, 351–372. [Google Scholar] [CrossRef] [PubMed]
- Axe, J.B.; Evans, C.J. Using video modeling to teach children with pdd-nos to respond to facial expressions. Res. Autism Spectr. Disord. 2012, 6, 1176–1185. [Google Scholar] [CrossRef]
- Bellini, S.; Akullian, J. A meta-analysis of video modeling and video self-modeling interventions for children and adolescents with autism spectrum disorders. Except. Child. 2007, 73, 264–287. [Google Scholar] [CrossRef]
- Khowaja, K.; Salim, S.S. A systematic review of strategies and computer-based intervention (cbi) for reading comprehension of children with autism. Res. Autism Spectr. Disord. 2013, 7, 1111–1121. [Google Scholar] [CrossRef]
- Pennisi, P.; Tonacci, A.; Tartarisco, G.; Billeci, L.; Ruta, L.; Gangemi, S.; Pioggia, G. Autism and social robotics: A systematic review. Autism Res. 2016, 9, 165–183. [Google Scholar] [CrossRef]
- Ramdoss, S.; Mulloy, A.; Lang, R.; O’Reilly, M.; Sigafoos, J.; Lancioni, G.; Didden, R.; Zein, F.E. Use of computer-based interventions to improve literacy skills in students with autism spectrum disorders: A systematic review. Res. Autism Spectr. Disord. 2011, 5, 1306–1318. [Google Scholar] [CrossRef]
- Fletcher-Watson, S. A targeted review of computer-assisted learning for people with autism spectrum disorder: Towards a consistent methodology. Rev. J. Autism Dev. Disord. 2014, 1, 87–100. [Google Scholar] [CrossRef]
- Lorenzo, G.; Lledó, A.; Arráez-Vera, G.; Lorenzo-Lledó, A. The application of immersive virtual reality for students with asd: A review between 1990–2017. Educ. Inf. Technol. 2019, 24, 127–151. [Google Scholar] [CrossRef]
- Mesa-Gresa, P.; Gil-Gómez, H.; Lozano-Quilis, J.-A.; Gil-Gómez, J.-A. Effectiveness of virtual reality for children and adolescents with autism spectrum disorder: An evidence-based systematic review. Sensors 2018, 18, 2486. [Google Scholar] [CrossRef] [PubMed]
- Kagohara, D.M.; Meer, L.v.; Ramdoss, S.; O’Reilly, M.F.; Lancioni, G.E.; Davis, T.N.; Rispoli, M.; Lang, R.; Marschik, P.B.; Sutherland, D.; et al. Using ipods® and ipads® in teaching programs for individuals with developmental disabilities: A systematic review. Res. Dev. Disabil. 2013, 34, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Noor, H.A.M.; Shahbodin, F.; Pee, N.C. Serious game for autism children: Review of literature. Int. J. Psychol. Behav. Sci. 2012, 6, 554–559. [Google Scholar]
- Zakari, H.M.; Ma, M.; Simmons, D. A review of serious games for children with autism spectrum disorders (asd). In International Conference on Serious Games Development and Applications; Springer: Berlin/Heidelberg, Germany, 2014; pp. 93–106. [Google Scholar]
- Krevelen, D.V.; Poelman, R. A survey of augmented reality technologies, applications and limitations. Int. J. Virtual Real. 2010, 9, 1–20. [Google Scholar] [CrossRef]
- Goh, E.S.; Sunar, M.S.; Ismail, A.W.; Andias, R. An inertial device-based user interaction with occlusion-free object handling in a handheld augmented reality. Int. J. Integr. Eng. 2018, 10, 6. [Google Scholar]
- Bai, Z.; Blackwell, A.F.; Coulouris, G. Using augmented reality to elicit pretend play for children with autism. IEEE Trans. Vis. Comput. Graph. 2014, 21, 598–610. [Google Scholar] [CrossRef]
- Goh, E.S.; Sunar, M.S.; Ismail, A.W. 3d object manipulation techniques in handheld mobile augmented reality interface: A review. IEEE Access 2019, 7, 40581–40601. [Google Scholar] [CrossRef]
- O’Nions, E.; Happé, F.; Evers, K.; Boonen, H.; Noens, I. How do parents manage irritability, challenging behaviour, non-compliance and anxiety in children with autism spectrum disorders? A meta-synthesis. J. Autism Dev. Disord. 2018, 48, 1272–1286. [Google Scholar] [CrossRef]
- Bagatell, N. The routines and occupations of families with adolescents with autism spectrum disorders. Focus Autism Other Dev. Disabil. 2016, 31, 49–59. [Google Scholar] [CrossRef]
- Lopez-Herrejon, R.E.; Poddar, O.; Herrera, G.; Sevilla, J. Customization support in computer-based technologies for autism: A systematic mapping study. Int. J. Human–Comput. Interact. 2020, 36, 1273–1290. [Google Scholar] [CrossRef]
- Bhatt, S.; Leon, N.D.; Al-Jumaily, A. Augmented reality game therapy for children with autism spectrum disorder. Int. J. Smart Sens. Intell. Syst. 2017, 7, 519–536. [Google Scholar] [CrossRef]
- Lee, I.-J. Kinect-for-windows with augmented reality in an interactive roleplay system for children with an autism spectrum disorder. Interact. Learn. Environ. 2021, 29, 688–704. [Google Scholar] [CrossRef]
- Marto, A.; Almeida, H.A.; Gonçalves, A. Using augmented reality in patients with autism: A systematic review. In ECCOMAS Thematic Conference on Computational Vision and Medical Image Processing; Springer: Berlin/Heidelberg, Germany, 2019; pp. 454–463. [Google Scholar]
- Karagiannidis, C. The application of augmented reality for intervention to people with autism spectrum disorders. IOSR J. Mob. Comput. Appl. (IOSR-JMCA) 2017, 4, 42–51. [Google Scholar]
- Adnan, N.H.; Ahmad, I.; Abdullasim, N. Systematic review on augmented reality application for autism children. J. Adv. Res. Dyn. Control Syst 2018, 10, 26–32. [Google Scholar]
- Khowaja, K.; Banire, B.; Al-Thani, D.; Sqalli, M.T.; Aqle, A.; Shah, A.; Salim, S.S. Augmented reality for learning of children and adolescents with autism spectrum disorder (asd): A systematic review. IEEE Access 2020, 8, 78779–78807. [Google Scholar] [CrossRef]
- Berenguer, C.; Baixauli, I.; Gómez, S.; Andrés, M.d.E.P.; Stasio, S.D. Exploring the impact of augmented reality in children and adolescents with autism spectrum disorder: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 6143. [Google Scholar] [CrossRef]
- Mullick, M.S.I.; Goodman, R. The prevalence of psychiatric disorders among 5–10 year olds in rural, urban and slum areas in bangladesh: An exploratory study. Soc. Psychiatry Psychiatr. Epidemiol. 2005, 40, 633–671. [Google Scholar] [CrossRef]
- Jahan, N.; Rahman, A.; Choudhury, S.; Chowdhury, K.; Wahab, M.; Rahman, F. Prevalence of mental disorders, mental retardation, epilepsy and substance abuse in children. Bang. J. Psychiatry 2009, 23, 11–52. [Google Scholar]
- Aggarwal, R.; Singhal, A. Augmented reality and its effect on our life. In Proceedings of the 2019 9th International Conference on Cloud Computing, Data Science & Engineering (Confluence), Uttar Pradesh, India, 10–11 January 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 510–515. [Google Scholar]
- Akçayır, M.; Akçayır, G. Advantages and challenges associated with augmented reality for education: A systematic review of the literature. Educ. Res. Rev. 2017, 20, 1–11. [Google Scholar] [CrossRef]
- Kellems, R.O.; Yakubova, G.; Morris, J.R.; Wheatley, A.; Chen, B.B. Using augmented and virtual reality to improve social, vocational, and academic outcomes of students with autism and other developmental disabilities. In Research Anthology on Inclusive Practices for Educators and Administrators in Special Education; IGI Global: Hershey, PA, USA, 2022; pp. 737–756. [Google Scholar]
- Cakir, R.; Korkmaz, O. The effectiveness of augmented reality environments on individuals with special education needs. Educ. Inf. Technol. 2019, 24, 1631–1659. [Google Scholar] [CrossRef]
- Baragash, R.S.; Al-Samarraie, H.; Moody, L.; Zaqout, F. Augmented reality and functional skills acquisition among individuals with special needs: A meta-analysis of group design studies. J. Spec. Educ. Technol. 2022, 37, 74–81. [Google Scholar] [CrossRef]
- Hashim, H.U.; Yunus, M.M.; Norman, H. ’Areal-vocab’: An augmented reality English vocabulary mobile application to cater to mild autism children in response towards sustainable education for children with disabilities. Sustainability 2022, 14, 4831. [Google Scholar] [CrossRef]
- Nekar, D.M.; Kang, H.; Alao, H.; Yu, J. Feasibility of using multiplayer game-based dual-task training with augmented reality and personal health record on social skills and cognitive function in children with autism. Children 2022, 9, 1398. [Google Scholar] [CrossRef]
- Pérez-Fuster, P.; Herrera, G.; Kossyvaki, L.; Ferrer, A. Enhancing joint attention skills in children on the autism spectrum through an augmented reality technology-mediated intervention. Children 2022, 9, 258. [Google Scholar] [CrossRef] [PubMed]
- Root, J.R.; Cox, S.K.; Davis, K.; Gonzales, S. Using augmented reality and modified schema-based instruction to teach problem solving to students with autism. Remedial Spec. Educ. 2022, 43, 301–313. [Google Scholar] [CrossRef]
- Wang, C.-P.; Tsai, C.-H.; Lee, Y.-L. Requesting help module interface design on key partial video with action and augmented reality for children with autism spectrum disorder. Appl. Sci. 2022, 12, 8527. [Google Scholar] [CrossRef]
- Luca, R.D.; Leonardi, S.; Portaro, S.; Cause, M.L.; Domenico, C.D.; Colucci, P.V.; Pranio, F.; Bramanti, P.; Calabrò, R.S. Innovative use of virtual reality in autism spectrum disorder: A case-study. Appl. Neuropsychol. Child 2021, 10, 90–100. [Google Scholar] [CrossRef]
- Zheng, Z.K.; Sarkar, N.; Swanson, A.; Weitlauf, A.; Warren, Z.; Sarkar, N. Cheerbrush: A novel interactive augmented reality coaching system for tooth-brushing skills in children with autism spectrum disorder. ACM Trans. Access. Comput. (TACCESS) 2021, 14, 1–20. [Google Scholar] [CrossRef]
- Antão, J.Y.F.d.L.; Abreu, L.C.d.; Barbosa, R.T.d.A.; Crocetta, T.B.; Guarnieri, R.; Massetti, T.; Antunes, T.P.C.; Tonks, J.; Monteiro, C.B.d.M. Use of augmented reality with a motion-controlled game utilizing alphabet letters and numbers to improve performance and reaction time skills for people with autism spectrum disorder. Cyberpsychol. Behav. Soc. Netw. 2020, 23, 16–22. [Google Scholar] [CrossRef]
- Arpaia, P.; Bravaccio, C.; Corrado, G.; Duraccio, L.; Moccaldi, N.; Rossi, S. Robotic autism rehabilitation by wearable brain-computer interface and augmented reality. In Proceedings of the 2020 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Bari, Italy, 1 June–1 July 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 1–6. [Google Scholar]
- López-Faican, L.; Jaen, J. Emofindar: Evaluation of a mobile multi-player augmented reality game for primary school children. Comput. Educ. 2020, 149, 149. [Google Scholar] [CrossRef]
- Kung-Teck, W.; Hanafi, H.F.; Abdullah, N.; Noh, N.M.; Hamzah, M. A prototype of augmented reality animation (ara) ecourseware: An assistive technology to assist autism spectrum disorders (asd) students master in basic living skills. Int. J. Innov. Technol. Explor. Eng. (IJITEE) 2019, 9, 3487–3492. [Google Scholar]
- Sahin, N.T.; Abdus-Sabur, R.; Keshav, N.U.; Liu, R.; Salisbury, J.P.; Vahabzadeh, A. Case study of a digital augmented reality intervention for autism in school classrooms: Associated with improved social communication, cognition, and motivation via educator and parent assessment. Front. Educ. 2018, 3, 57. [Google Scholar] [CrossRef]
- Magrini, M.; Curzio, O.; Carboni, A.; Moroni, D.; Salvetti, O.; Melani, A. Augmented interaction systems for supporting autistic children. evolution of a multichannel expressive tool: The semi project feasibility study. Appl. Sci. 2019, 9, 3081. [Google Scholar] [CrossRef]
- Singh, K.; Shrivastava, A.; Achary, K.; Dey, A.; Sharma, O. Augmented reality-based procedural task training application for less privileged children and autistic individuals. In Proceedings of the 17th International Conference on Virtual-Reality Continuum and its Applications in Industry, Brisbane, QLD, Australia, 14–16 November 2019; pp. 1–10. [Google Scholar]
- Tang, T.Y.; Xu, J.; Winoto, P. An augmented reality-based word-learning mobile application for children with autism to support learning anywhere and anytime: Object recognition based on deep learning. In International Conference on Human-Computer Interaction; Springer: Berlin/Heidelberg, Germany, 2019; pp. 182–192. [Google Scholar]
- Vahabzadeh, A.; Keshav, N.U.; Salisbury, J.P.; Sahin, N.T. Improvement of attention-deficit/hyperactivity disorder symptoms in school-aged children, adolescents, and young adults with autism via a digital smartglasses-based socioemotional coaching aid: Short-term, uncontrolled pilot study. JMIR Ment. Health 2018, 5, e9631. [Google Scholar] [CrossRef]
- Taryadi; Kurniawan, I. The improvement of autism spectrum disorders on children communication ability with pecs method multimedia augmented reality-based. J. Phys. Conf. Ser. 2018, 947, 012009. [Google Scholar] [CrossRef]
- Syahputra, M.F.; Sari, P.P.; Arisandi, D.; Abdullah, D.; Napitupulu, D.; Setiawan, M.I.; Albra, W.; Asnawi; Andayani, U. Implementation of augmented reality to train focus on children with s pecial needs. J. Phys. Conf. Ser. 2018, 978, 012109. [Google Scholar] [CrossRef]
- Chen, C.-H.; Lee, I.-J.; Lin, L.-Y. Augmented reality-based video- modeling storybook of nonverbal facial cues for children with autism spectrum disorder to improve their perceptions and judgments of facial expressions and emotions. Comput. Hum. Behav. 2016, 55, 477–485. [Google Scholar] [CrossRef]
- Cihak, D.F.; Moore, E.J.; Wright, R.E.; McMahon, D.D.; Gibbons, M.M.; Smith, C. Evaluating augmented reality to complete a chain task for elementary students with autism. J. Spec. Educ. Technol. 2016, 31, 99–108. [Google Scholar] [CrossRef]
- Hosseini, E.; Foutohi-Ghazvini, F. Play therapy in augmented reality children with autism. J. Mod. Rehabil. 2016, 10, 110–115. [Google Scholar]
- McMahon, D.D.; Cihak, D.F.; Wright, R.E.; Bell, S.M. Augmented reality for teaching science vocabulary to postsecondary education stu- dents with intellectual disabilities and autism. J. Res. Technol. Educ. 2016, 48, 38–56. [Google Scholar] [CrossRef]
- Escobedo, L.; Tentori, M. Mobile augmented reality to support teachers of children with autism. In International Conference on Ubiquitous Computing and Ambient Intelligence; Springer: Berlin/Heidelberg, Germany, 2014; pp. 60–67. [Google Scholar]
- Escobedo, L.; Nguyen, D.H.; Boyd, L.; Hirano, S.; Rangel, A.; Rosas, D.G.; Tentori, M.; Hayes, G. Mosoco: A mobile assistive tool to support children with autism practicing social skills in real-life situations. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Austin, TX, USA, 5–10 May 2012; pp. 2589–2598. [Google Scholar]
- Critical Appraisal Skills Programme. “CASP Checklists”, CASP–Critical Appraisal Skills Programme. 2022. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 23 July 2023).
- Oke, A.E.; Arowoiya, V.A. Critical barriers to augmented reality technology adoption in developing countries: A case study of Nigeria. J. Eng. Des. Technol. 2022, 20, 1320–1333. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category 1 | Category 2 | Category 3 |
|---|---|---|
| Autism | Augmented Reality | Mobile |
| Autism Spectrum Disorder | AR | Tablet |
| ASD | Mobile Augmented Reality | Smartphone |
| Autistic | Augmented | Toolkit |
| Autistic Children | Inclusive Digital Technologies | Smartglass |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| In1: Studies published between January 2010 and November 2022, spanning the last ten years | Ex1: Studies with an exclusively medical focus or a focus on the diagnosis of autism spectrum disorder |
| In2: Journal articles | Ex2: Not peer-reviewed (i.e., commentaries, letters to the editor, opinion articles, lectures) |
| In3: Studies with a focus on AR technology for ASD patients | Ex3: Studies that involve AR but do not include ASD exclusively |
| In4: Studies related to the usage of technology | Ex4: Studies that take into account usability and accessibility in contexts where technology is not involved |
| In5: Authors reported intervention impact, generalization, or maintenance | Ex5: Descriptive case studies with no reported research design or participant outcome. |
| In6: Empirically based studies employing single-subject, qualitative, quantitative, or mixed methodologies | Ex6: Studies that do not directly attempt to aid individuals with autism spectrum disorder, but rather their caregivers |
| No. | Study | Study Design | Study Purpose | Functional Skills/Observed Improvements | No. of Participants/Consent Taken | Groups (Sex/Age) | Geographic Location/ Ethnicity | Duration of AR |
|---|---|---|---|---|---|---|---|---|
| 01. | Hashim (2022) [41] | Design and development | Assist children with mild autism in acquiring English vocabulary | Learning/significant improvements in learning | Total: 6 (M:5, F:1)/yes | Mildly ASD children; age: 5–12 years | Malaysia/Malaysian | 15–20 h in total |
| 02. | Nekar (2022) [42] | Single group;pre-test–post-test | Evaluate multiplayer games with dual-task exercise employing AR and a personal health record (PHR) system for autistic children’s social skills and cognitive function | Social skills/promising improvement in social skills | Total: 14 (M:11, F:3)/yes | ASD children; age: 6–16 | South Korea/Korean | 3 h in total |
| 03. | Perez (2022) [43] | Multiple baseline single-subject experimental design | Improve responding to joint attention (RJA) skills such as gaze tracking and pointing | Joint attention/moderate engagement | Total: 6 (M:5, F:1)/did not mention | ASD children; age: 3–8 years old | Spain/Spanish | 30 min per session |
| 04. | Root (2022) [44] | Program evaluation | Analyze the effectiveness of a multi-component intervention using AR and modified schema-based instruction (MSBI) | Living skills/moderate improvements | Total: 4/did not mention | Age: 21 | USA | Did not mention |
| 05. | Wang (2022) [45] | AR intervention study | Using support modules, dynamic video, and AR in (key partial video) KPV, enhance the communication of youngsters with ASD. | Social interaction, verbal/non-verbal communication, facial emotion recognition, attention | Total: 5 (M:4, F:1)/yes | 2 TD male 3 ASD (2 male and 1 female); mean age: 7 | China/Taiwanese | Did not mention |
| 06. | Lee (2021) [28] | Multiple baseline across single-subjects design | Help children with autism recognize social greetings and body gestures so they can respond appropriately | Social reciprocal skills/improvement observed | Total: 3 (M:2, F:1)/yes | ASD children; age: 7–9 years old (mean age = 8.1 years) | Taiwan/Taiwanese | Did not mention |
| 07. | Luca (2021) [46] | Single-subject design | Determine the feasibility and effectiveness of VR gadget in improving cognitive and behavioral skills of an ASD-affected boy | Cognitive and behavioral skills/indeterminate | Total: 1 (M:1)/did not mention | Male; age: 16 | Italy/Italian | 40 min per session |
| 08. | Zheng (2021) [47] | Feasibility study | Interactive AR coaching system, CheerBrush, to improve the tooth-brushing skills of children with ASD | Living skills/improved living skills | Total: 12/did not mention | (6 with ASD, 6 TD); 3–6 years | USA/American | Did not mention |
| 09. | Anto (2020) [48] | Pre-test–post-test | Employment of alphabet letters and numbers in AR environment and its influence on reaction time | Learning/significant improvement | Total: 96/yes | (48 with ASD, 48 TD); mean age | Brazil/Brazilian | Did not mention |
| 10. | Arpaia (2020) [49] | Case study | Design a system for ASD rehabilitation combining AR smart glasses and SSVEP brain–computer interface | Social interaction/significant improvement | Total: 3/Did not mention | Untrained ASD/ADHD children; Age: 8–10 years old | Italy/Italian | Did not mention |
| 11. | Lopez (2020) [50] | Program evaluation | To improve interaction, communication, and emotional intelligence in elementary school students, build a multiplayer game using marker-less MAR. | Social, emotional, social interaction/satisfactory results | Total: 38/yes | Age: 9–11 years (mean = 10.42, SD = 0.59) | Spain/Spanish | Did not mention |
| 12. | Kung (2019) [51] | Prototype, pre–post quasi-experimental design | A pre–post experimental research design named BLS (Basic Living Skills) E-courseware to help in teaching | Education/significant improvements | Total: 4/did not mention | Not mentioned | Malaysia/Malaysian | Did not mention |
| 13. | Sahin (2018) [52] | Single-case experimental design | Feasibility study of Empowered Brain Face2Face module, a social communication intervention using smart glasses | Social skills/moderate improvements | Total: 1 (M:1)/Yes | Fully-verbal ASD boy; age: 13 years | USA/American | 20 min daily for 3 weeks |
| 14. | Magrini (2019) [53] | Feasibility study | Create interactive games that are adjusted for a child’s sensory preferences and level of challenge. Children’s gross and fine motor capabilities, imitation skills, social interaction, and personal autonomy will all be improved by the prototype. | Social interaction, emotional intelligence/improved | Total: 10/yes | Subjects with ASD and dyspraxia; age: 6–10 years | Italy/Italian | 45 min per session |
| 15. | Singh (2019) [54] | Within-subject user study | Using AR applications to enhance learning experiences for less privileged autistic children. | Acquisition of certain skills/indeterminate | Total: 12 (M:6, F:6)/Did not mention | (6 boys, 6 girls); age: 9–12 years | India/Indian | Did not mention |
| 16. | Tang (2019) [55] | Pilot study | Design a lightweight AR-based mobile vocabulary study application for autistic children, particularly for outdoor and home use | Education/significant improvements | Study one: did not mention; study two: five/did not mention | Age: one under 5; another 6–8 years | China/Chinese | Did not mention |
| 17. | Vahabzadeh (2018) [56] | Short-term, uncontrolled pilot study | Empowered Brain, an AR smart glasses tool for behavioral and social communication, was used to assess ADHD-related symptom changes in ASD children and adolescents. | Social skills/significant improvements | Total: 8 (M:7, F:1)/yes | ASD individuals (male to female ratio of 7:1); mean age: 15 years | USA/American | Did not mention |
| 18. | Kurniawan (2018) [57] | Program evaluation | Examine the use of multimedia PECS (Picture Exchange Communication System)-based AR as an alternative learning tool for autism children’s communication training | Social interaction/significant improvements | Total: 12/did not mention | Autistic children | Indonesia/Indonesian | Did not mention |
| 19. | Syahputra (2018) [58] | Pilot study | Design an AR system using leap motion controller to help train the focus of autistic individuals | Emotional intelligence/indeterminate | N/A/did not mention | N/A | Indonesia/Indonesian | N/A |
| 20. | Chen (2016) [59] | Single-subject with multiple baseline design | Improve ASD children’ attention to nonverbal social cues | Social-emotional reciprocity/improved | Total: 6 (M:5, F:1)/yes | 5 boys and 1 girl and Age: 11–13 years; mean: 11.53 years | Taiwan/Taiwanese | Did not mention |
| 21. | Cihak (2016) [60] | Group-experimental design | Evaluate AR intervention in teaching a chain task to elementary students with ASD | Living skills/indeterminate | Total: 3 (M:3)/Yes | Male with ASD | USA/American | Did not mention |
| 22. | Hosseini (2016) [61] | Quasi-experimental study | PECS method implemented, and program was for training and orientation of objects of the real world | Communication skills/indeterminate | Did not mention/N/A | 6–11 years | Iran/Iranian | Did not mention |
| 23. | McMahon (2016) [62] | Multiple probes across behaviors design | Assess AR intervention for teaching science vocabulary to college students with intellectual disabilities and ASD. | Education/improved navigation | Total: 4 (M:1, F:3)/yes | Three students with ID and one with ASD; age: 19–25 years | USA/American | Did not mention |
| 24. | Bai (2014) [22] | Within-subject experiment | Design an interactive method to visualize pretense in an open-ended play environment using AR | Emotional intelligence using games/significant improvement | Total: 12 (M:10, F:2)/N/A | ASC; 10 male and 2 female; 4–7 | UK/British | Did not mention |
| 25. | Escobedo (2014) [63] | Deployment study | Help teachers lessen the burden and workload of administering therapies by allowing children to use tangible objects | Education/enables multitasking abilities | Total: 21/did not mention | (7 teachers, 14 students); age of students (3–7, m = 5.08, sd = 0.90) | Mexico/Mexican | Did not mention |
| No. | Study | Assessment of Inclusion Criteria | Possible Covariates |
|---|---|---|---|
| 01. | Hashim (2022) [41] | N/A | N/A |
| 02. | Nekar (2022) [42] | (1) Having been diagnosed with autism, (2) the ability to see, hear, and understand basic instructions, (3) the ability to read and understand Korean (the main language used in the game contents) | N/A |
| 03. | Perez (2022) [43] | N/A | N/A |
| 04. | Root (2022) [44] | (1) Educational or medical classification of ASD, (2) enrolled in a public school transition program, (3) researcher observation of prerequisite skills via screening tool. | N/A |
| 05. | Wang (2022) [45] | N/A | N/A |
| 06. | Lee (2021) [28] | (1) A clinical diagnosis of ASD based on DSM-IV-TR criteria, (2) no other specific disabilities, (3) not taking medications for physician or self-diagnosed illnesses, (4) no physician-diagnosed comorbidities, (5) not undergoing any other therapies at the time of the testing, (6) an FIQ > 90. | N/A |
| 07. | Luca (2021) [46] | N/A | N/A |
| 08. | Zheng (2021) [47] | (1) Height of at least 3 feet for successful Kinect recognition; (2) age 3–6 years; and, for children with ASD, (3) a documented diagnosis of ASD by a licensed clinical provider | N/A |
| 09. | Anto (2020) [48] | N/A | N/A |
| 10. | Arpaia (2020) [49] | N/A | N/A |
| 11. | Lopez (2020) [50] | N/A | H0h-P2Obs1-Sustaining mutual understanding, H0i-P2Obs2-Dialogue management, H0j-P2Obs3-Information pooling, H0k-P2Obs4-Reaching consensus, H0l-P2Obs5-Task division, H0m-P2Obs6-Time management, H0n-P2Obs7-Technical coordination, H0o-P2Obs8-Reciprocal interaction, H0p-P2Obs9-Individual task orientation. |
| 12. | Kung (2019) [51] | N/A | Basic Living Skills (BLS) e-courseware prototypes (Augmented Reality Animation) and Basic Living Skills (Static graphic) |
| 13. | Sahin (2018) [52] | N/A | N/A |
| 14. | Magrini (2019) [53] | N/A | N/A |
| 15. | Singh (2019) [54] | N/A | Training Time, solve time, correct placements, subjective questionnaire. |
| 16. | Tang (2019) [55] | N/A | N/A |
| 17. | Vahabzadeh (2018) [56] | N/A | N/A |
| 18. | Kurniawan (2018) [57] | N/A | N/A |
| 19. | Syahputra (2018) [58] | N/A | N/A |
| 20. | Chen (2016) [59] | (1) A clinical diagnosis of ASD based on DSM-IV-TR criteria, (2) not undergoing any other therapies/medication at the time of the testing, (3) no other disabilities, (4) an FIQ > 90. | N/A |
| 21. | Cihak (2016) [60] | N/A | N/A |
| 22. | Hosseini (2016) [61] | N/A | N/A |
| 23. | McMahon (2016) [62] | N/A | N/A |
| 24. | Bai (2014) [22] | N/A | N/A |
| 25. | Escobedo (2014) [63] | N/A | N/A |
| No. | Study | Did the Paper Address a Clearly Focused Question? | Did the Authors Look for the Right Type of Papers? | Do You Think All the Important, Relevant Studies Were Included? | Did the Paper’s Authors Do Enough to Assess Quality of the Included Studies? | If the Results of the Paper Have Been Combined, Was It Reasonable to Do So? |
|---|---|---|---|---|---|---|
| 01. | Hashim (2022) [41] | Yes | Yes | Yes | Yes | Yes |
| 02. | Nekar (2022) [42] | Yes | Yes | No | Indeterminate | Yes |
| 03. | Perez (2022) [43] | Yes | Yes | Yes | Yes | Yes |
| 04. | Root (2022) [44] | Yes | Yes | Yes | Yes | Yes |
| 05. | Wang (2022) [45] | Yes | Yes | Yes | Yes | Yes |
| 06. | Lee (2021) [28] | Yes | Yes | Yes | Yes | Yes |
| 07. | Luca (2021) [46] | Yes | Yes | No | Yes | Yes |
| 08. | Zheng (2021) [47] | Yes | Yes | Yes | Yes | Yes |
| 09. | Anto (2020) [48] | Yes | Yes | Yes | Yes | Yes |
| 10. | Arpaia(2020) [49] | Yes | Yes | Yes | Yes | Yes |
| 11. | Lopez (2020) [50] | Yes | Yes | Yes | Yes | Yes |
| 12. | Kung (2019) [51] | Yes | Yes | Yes | Yes | Yes |
| 13. | Sahin (2018) [52] | Yes | Yes | Yes | Yes | Yes |
| 14. | Magrini (2019) [53] | Yes | Yes | Yes | Yes | Yes |
| 15. | Singh (2019) [54] | Yes | Yes | Yes | Yes | Yes |
| 16. | Tang(2019) [55] | Yes | Yes | No | Indeterminate | Indeterminate |
| 17. | Vahabzadeh (2018) [56] | Yes | Yes | Yes | Yes | Yes |
| 18. | Kurniawan (2018) [57] | Yes | No | No | Yes | Indeterminate |
| 19. | Syahputra (2018) [58] | No | No | No | Indeterminate | Indeterminate |
| 20. | Chen (2016) [59] | No | Yes | Yes | Yes | Yes |
| 21. | Cihak (2016) [60] | Yes | Yes | Yes | Yes | Yes |
| 22. | Hosseini (2016) [61] | Yes | Yes | Yes | Yes | Yes |
| 23. | McMahon (2016) [62] | Yes | Yes | Yes | Yes | Yes |
| 24. | Bai (2014) [22] | Yes | Yes | Yes | Yes | Yes |
| 25. | Escobedo (2014) [63] | Yes | Yes | No | No | No |
| No. | Study | What Are the Overall Results of the Paper? | How Precise Are the Results? | Can the Results Be Applied to the Local Population? | Were All Important Outcomes Considered? | Are the Benefits Worth the Harms and Costs? |
|---|---|---|---|---|---|---|
| 01. | Hashim (2022) [41] | Did not mention clearly | Did not mention | Indeterminate | Indeterminate | Indeterminate |
| 02. | Nekar (2022) [42] | Despite no statistically significant result in social communication and restricted interests and repetitive behavior, a decrease in the mean was observed when compared to the baseline data. | p < 0.05 | Yes | Yes | Yes |
| 03. | Perez (2022) [43] | An overall PAND of 98% was obtained for v2 and an overall PAND of 96% was measured for v3. This shows that the intervention was highly effective (PAND > 90%) for enhancing the abilities of gaze following and pointing to the target object in six autistic children. | p < 0.01 | Indeterminate | Yes | Yes |
| 04. | Root (2022) [44] | The combination of MSBI and video-based instruction delivered via AR helped four adult students with ASD improve in their ability to solve percentage of change problems (i.e., tip) | Did Not Mention | Yes | Yes | Yes |
| 05. | Wang (2022) [45] | ASD improved from baseline 1 at 83% when using the AOM to 98% at intervention 2 when using KPV with AR | p < 0.05 | Indeterminate | Yes | Indeterminate |
| 06. | Lee (2021) [28] | Baseline mean: 19.16% | p < 0.05 | Yes | Yes | Yes |
| 07. | Luca (2021) [46] | Significant increase in attention processes | Did not mention | Indeterminate | Indeterminate | Yes |
| 08. | Zheng (2021) [47] | ASD Baseline: 98.89 | The HR and SCL differences of ASD group reached and was near statistically significant, respectively | Indeterminate | Yes | Yes |
| 09. | Anto (2020) [48] | ASD Total Points: 54.5 | p < 0.05 | Indeterminate | Yes | Yes |
| 10. | Arpaia (2020) [49] | Positive feedback on the device acceptance and attentional performance were offered after tests on three ASD patients (with three different CGI scores) between 8 and 10 years | Did not mention | Yes | Yes | Yes |
| 11. | Lopez (2020) [50] | A total of 95% of the children participated actively in the search for the solution to end the game | p < 0.05 | Yes | Yes | Yes |
| 12. | Kung (2019) [51] | Improvement in academic performance | Did not mention | Yes | Indeterminate | Yes |
| 13. | Sahin (2018) [52] | SRS measure baseline raw score: 92 | Did not mention | Yes | Yes | Yes |
| 14. | Magrini (2019) [53] | Children embraced experiments, showing improved attention, and response times | Did not mention | Yes | Indeterminate | Yes |
| 15. | Singh (2019) [54] | More training time compared to desktop and in-person | Did not mention | Yes | Indeterminate | Yes |
| 16. | Tang (2019) [55] | Did not mention clearly | N/A | Indeterminate | Indeterminate | Indeterminate |
| 17. | Vahabzadeh (2018) [56] | Baseline mean: 5.5 | Did not mention | Yes | Yes | Yes |
| 18. | Kurniawan (2018) [57] | The increase achieved an average of 76% in the communication skills of children before treatment. | Did not mention | Yes | Yes | Yes |
| 19. | Syahputra (2018) [58] | With an average percentage of 83% on a Likert scale, respondents strongly agree that the app can train the child’s focus. | Did not mention | Indeterminate | Indeterminate | Indeterminate |
| 20. | Chen (2016) [59] | baseline range: 86.66–94.28% | Yes | No | Yes | Yes |
| 21. | Cihak (2016) [60] | Students’ independent performance immediate increased when augmented reality was introduced with 98% non-overlapping data. | Did not mention | Indeterminate | Indeterminate | Yes |
| 22. | Hosseini (2016) [61] | Data obtained results using Wilcoxon test of 0.007 | p < 0.05 | Yes | Yes | Yes |
| 23. | McMahon (2016) [62] | Baseline scores on the vocabulary assessments for the students indicated that the students had very low initial knowledge of the science vocabulary words across the three-word lists | Did not mention | Yes | No | Yes |
| 24. | Bai (2014) [22] | Did not mention clearly | Did not mention | Indeterminate | Indeterminate | Indeterminate |
| 25. | Escobedo (2014) [63] | Mobile Object Identification System helped teachers to attend to multiple students (n > 1) during the therapy | Did not mention | Yes | No | Yes |
| No. | Study | Software | Hardware | Setting | Phase | Duration | Method Followed/Feedback Method | Survey Questions Availability |
|---|---|---|---|---|---|---|---|---|
| 01. | Hashim (2022) [41] | Smartphone application, called ‘AReal-Vocab’ | Flashcards containing words | Home and Classroom | Five 30 to 40 min sessions | 5 weeks | Kohan Cappa Analysis/interviews and field notes | Yes |
| 02. | Nekar (2022) [42] | Kinect | Tablet | Local social welfare center | Baseline, intervention, post-intervention Survey | Three weeks | 3 Wilcoxon signed-rank test/System Usability Scale (SUS)-based survey | Yes |
| 03. | Perez (2022) [43] | Pictogram Room | LCD Projector, Interactive Digital Whiteboard, Computer, Kinect, and Samsung SCC-301P Video camera | School classroom | Pre-baseline phase, pre-assessments, baseline phase, learning phase, intervention phase, post-intervention phase, post-assessments, follow-up assessments | 12 Weeks | Social Communication Questionnaire, Leiter International Performance Scale, Autism Diagnostic Observation Schedule Second Edition (ADOS-2), Early Social Communication Scales (ESCS)/N/A | Yes |
| 04. | Root (2022) [44] | Calculator application, HP Reveal, and First-Then Visual Schedule HD | Worksheet and iPod | Classroom, Campus coffee and snack shop | Baseline, intervention, generalization, and maintenance | N/A | N/A | No |
| 05. | Wang (2022) [45] | HP Reveal, Unity Vuforia, AR Kit, MAKAR, KPV | Paper-based picture cards, vocabulary textbooks, tablet | Teacher-selected computer classrooms in elementary schools | Two phases: the first phase comprises the A1 baseline and B1 treatment periods, and the second phase includes the C1 reversal and B2 treatment periods | 4 Months | t-test/N/A | No |
| 06. | Lee (2021) [28] | KST System | Computer | Classroom | Baseline, Intervention, Maintenance | 6 weeks | Kolmogorov– Smirnov test, Likert scale/Verbal | No |
| 07. | Luca (2021) [46] | N/A | Medical Device named BTS-N | Clinic | Two different trainings: CBT according to standardized approach, CBT in a VR environment (Total 48 sessions) | One month | Raven’s Matrices test, Modified Little Bell Test, developmental test of visual–motor integration, Gilliam Autism Rating Scale/ Questionnaire | No |
| 08. | Zheng (2021) [47] | Virtual Avatar | Mechatronic toothbrush and Microsoft Kinect V2 Camera and Sensor, E4 | N/A | Baseline, pre-test, coaching, post-test | N/A | p-values/ Questionnaire, Likert Scale | Yes |
| 09. | Anto (2020) [48] | Computer game MoviLetrando | Laptop computer | Classroom | Pre-test, post-test | N/A | Mann–Whitney U test, Wilcoxon signed-rank test/N/A | No |
| 10. | Arpaia (2020) [49] | A SSVEP-based single-channel BCI | Smart glasses | Social interaction | N/A | N/A | N/A | No |
| 11. | Lopez (2020) [50] | EmoFindAR application | Smartphone | Classroom | Gender: did not mention | N/A | Questionnaire/ N/A | Yes |
| 12. | Kung (2019) [51] | Smartphone application | Smartphone and flashcards | Classroom | Pre-test and post-test | N/A | N/A/ Questionnaire | No |
| 13. | Shanin (2018) [52] | N/A | Empowered Brain Face2Face module | Classroom | N/A Baseline and intervention | 2 weeks | N/A/Social Responsiveness Scale2 (SRS-2) school-age form | No |
| 14. | Magrini (2019) [53] | Kinect SDK | Computer, Sensor | N/A | Four phases: repeat the movements, guess the movements, connect the dots and guess the card | 6 weeks | Time and score for each exercise/verbal | No |
| 15. | Singh (2019) [54] | Desktop-based Application | Tangram Puzzle and Desktop Computer and Webcam | Classroom | Training and Testing | N/A | Time required to solve a Tangram puzzle/ Questionnaire | Yes |
| 16. | Tang (2019) [55] | Deep learning platform, TensorFlow and simple lightweight mobile application | N/A | Special education school and university campus | N/A | N/A | No/verbal | No |
| 17. | Kurniawan (2018) [57] | Mobile application | Smartphone | Classroom | Baseline, Intervention after 24 and 48 h | N/A | Qualitative, visual analysis/interview | No |
| 18. | Vahabzadeh (2018) [56] | Empowered Brain System | Google Glass | N/A | Baseline, Intervention after 24 and 48 h | 48 h | Social Communication Questionnaire (SCQ), ABC-H/N/A | No |
| 19. | Syahputra (2018) [58] | Leap Motion Controller | Camera, 3D object marker, Computer | N/A | N/A | N/A | Detection/ Questionnaire | No |
| 20. | Chen (2016) [59] | Application | Tablet and AR-based video modeling storybook | School | Baseline, intervention, maintenance | 4 weeks | No/questionnaires and interviews after each phase | No |
| 21. | Hosseini (2016) [61] | Mobile application | Smartphone | School | N/A | N/A | Wilcoxon test for data collection/N/A | No |
| 22. | Bai (2014) [22] | Goblin XNA | Webcam, Bluetooth keyboard, and play materials consisting of AR items (three foam blocks and a box with connected markers) and non-AR physical props (three cotton balls, two paper tubes, three popsicle sticks, three pen tops, three strings and a piece of cloth) | Home | N/A | N/A | CARS2, BPVS3, play frequency, play time/ questionnaire | No |
| 23. | Cihak (2016) [60] | AR application | iPod, toothbrush, paper cup | Classroom | Baseline, pretraining, AR intervention, maintenance | 9 weeks | Likert scale, percentage of steps/no | No |
| 24. | McMahon (2016) [62] | Mobile app Aurasma | Book | Computer lab in a university campus | Baseline, training, intervention | N/A | Number of vocabulary items defined and labeled correctly/Likert-type survey | Yes |
| 25. | Escobedo (2014) [63] | MOBIS, an AR application | Smartphone | Specialized clinic | Pre-deployment (2 weeks), deployment (5 weeks), and post-deployment (1 week) | 8 weeks | Weekly interview; LSA and ANOVA/group interview, survey | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doulah, A.B.M.S.U.; Rasheduzzaman, M.; Arnob, F.A.; Sarker, F.; Roy, N.; Ullah, M.A.; Mamun, K.A. Application of Augmented Reality Interventions for Children with Autism Spectrum Disorder (ASD): A Systematic Review. Computers 2023, 12, 215. https://doi.org/10.3390/computers12100215
Doulah ABMSU, Rasheduzzaman M, Arnob FA, Sarker F, Roy N, Ullah MA, Mamun KA. Application of Augmented Reality Interventions for Children with Autism Spectrum Disorder (ASD): A Systematic Review. Computers. 2023; 12(10):215. https://doi.org/10.3390/computers12100215
Chicago/Turabian StyleDoulah, A. B. M. S. U., Mirza Rasheduzzaman, Faed Ahmed Arnob, Farhana Sarker, Nipa Roy, Md. Anwar Ullah, and Khondaker A. Mamun. 2023. "Application of Augmented Reality Interventions for Children with Autism Spectrum Disorder (ASD): A Systematic Review" Computers 12, no. 10: 215. https://doi.org/10.3390/computers12100215
APA StyleDoulah, A. B. M. S. U., Rasheduzzaman, M., Arnob, F. A., Sarker, F., Roy, N., Ullah, M. A., & Mamun, K. A. (2023). Application of Augmented Reality Interventions for Children with Autism Spectrum Disorder (ASD): A Systematic Review. Computers, 12(10), 215. https://doi.org/10.3390/computers12100215