
Reducing the Cost of Proton Radiation Therapy: The Feasibility of a Streamlined Treatment Technique for Prostate Cancer

Abstract
:1. Introduction
2. Methods and Materials
2.1. Patient Cohort
2.2. Treatment Planning

2.3. Monte Carlo Simulations
2.4. Calculations of Lifetime Risk of Neutron-Induced Second Cancer of the Bladder and Rectum
2.5. Determination of Equivalent Photon and Proton Prescription Doses
3. Results
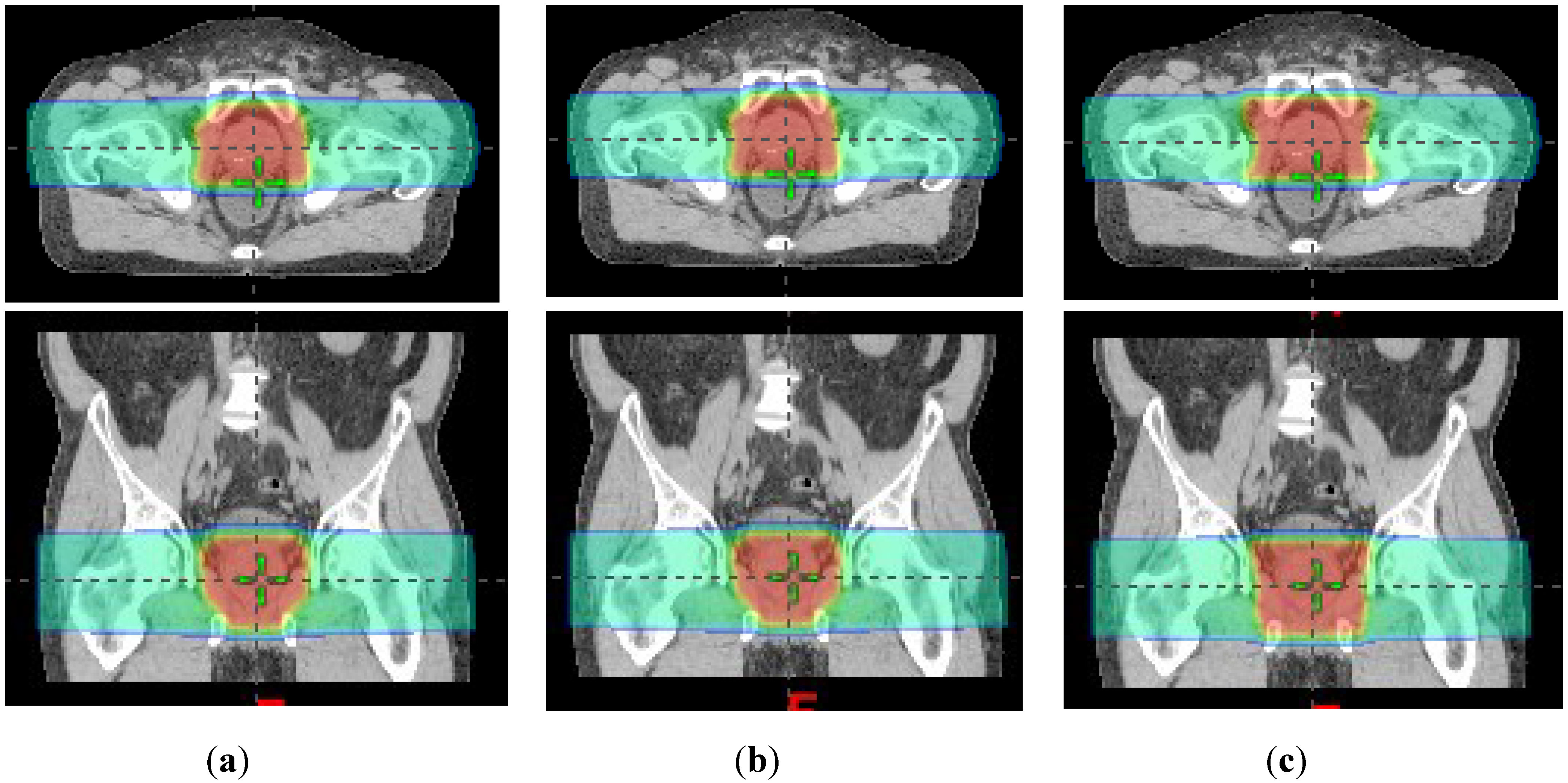
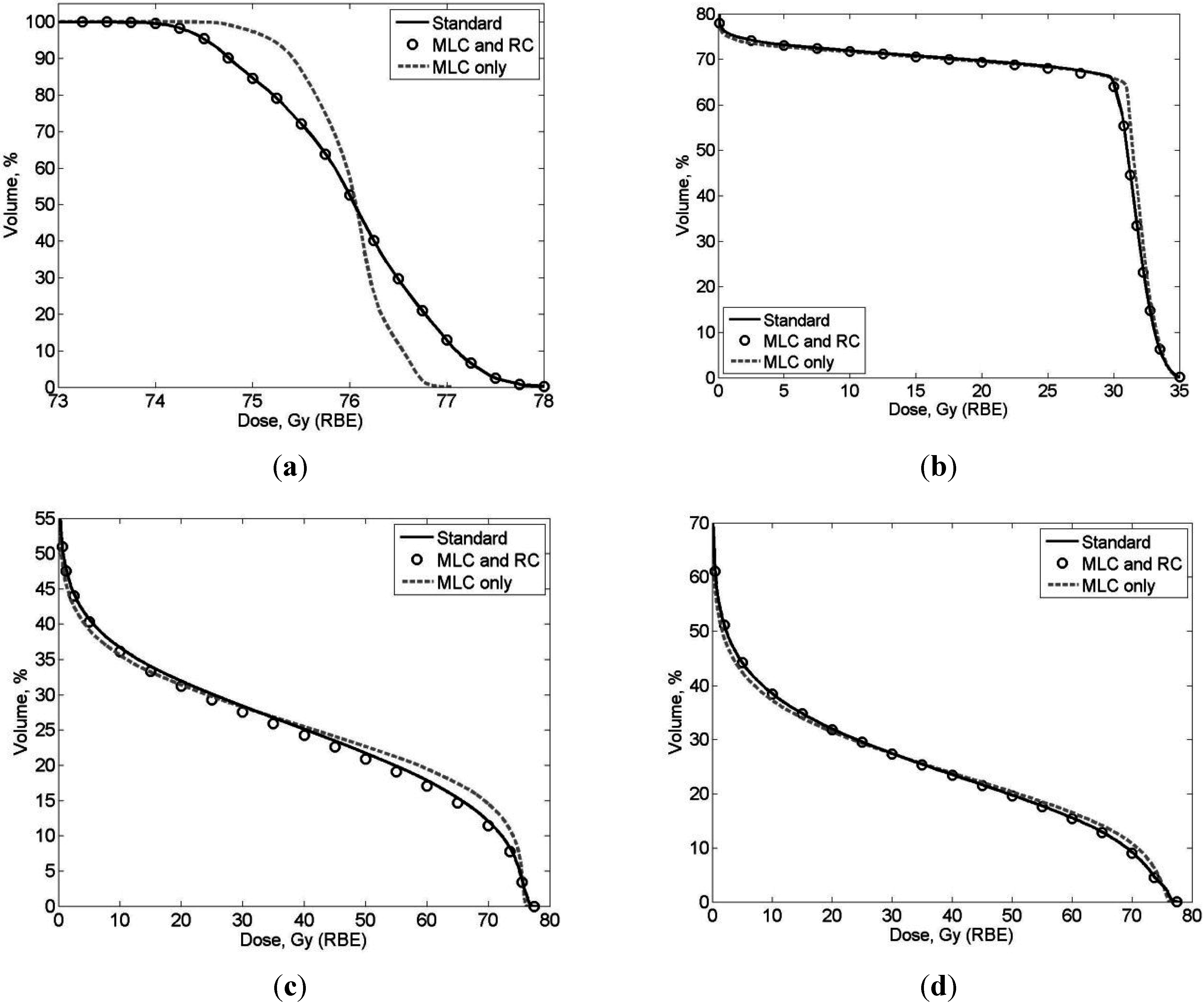
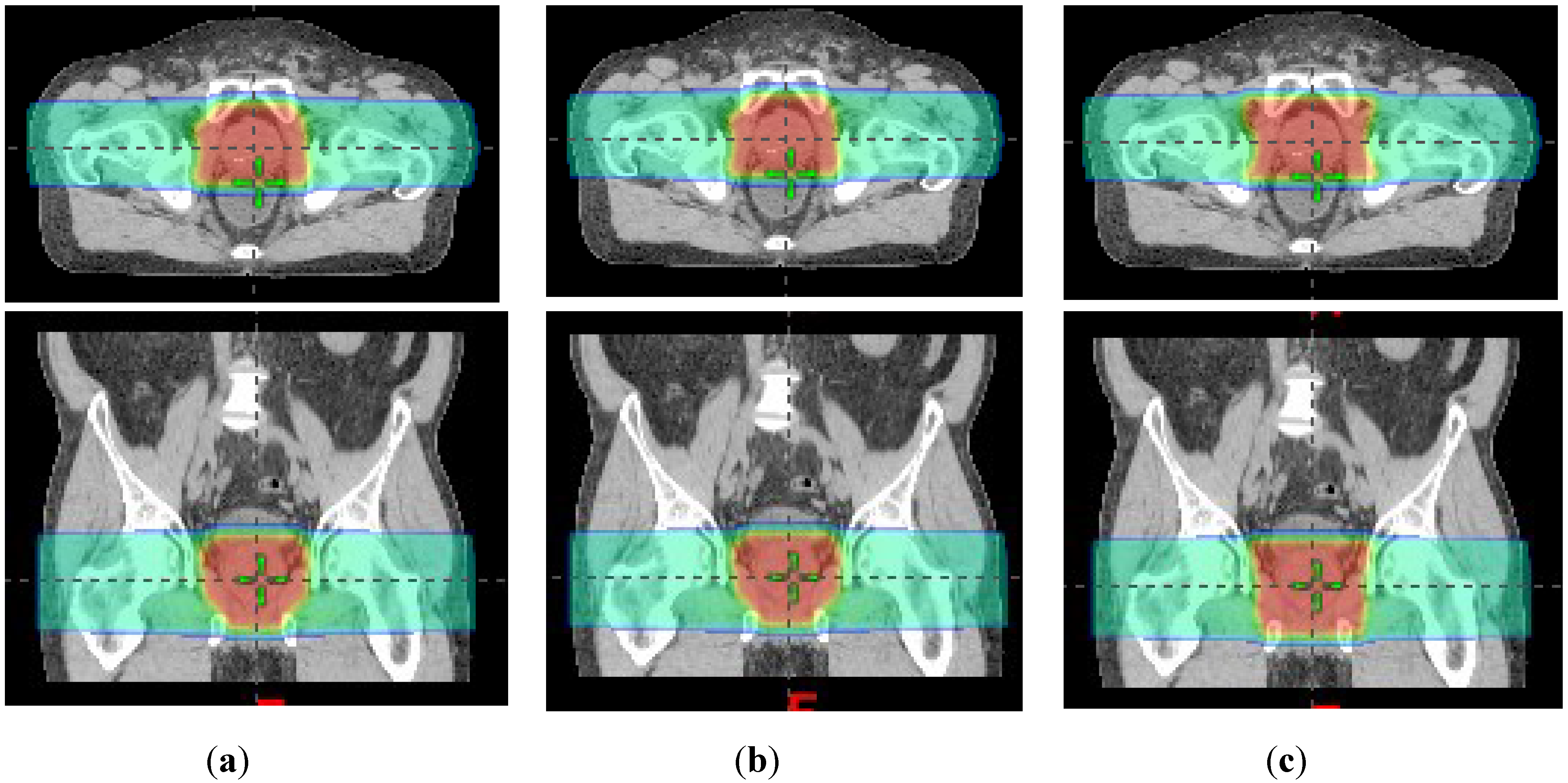
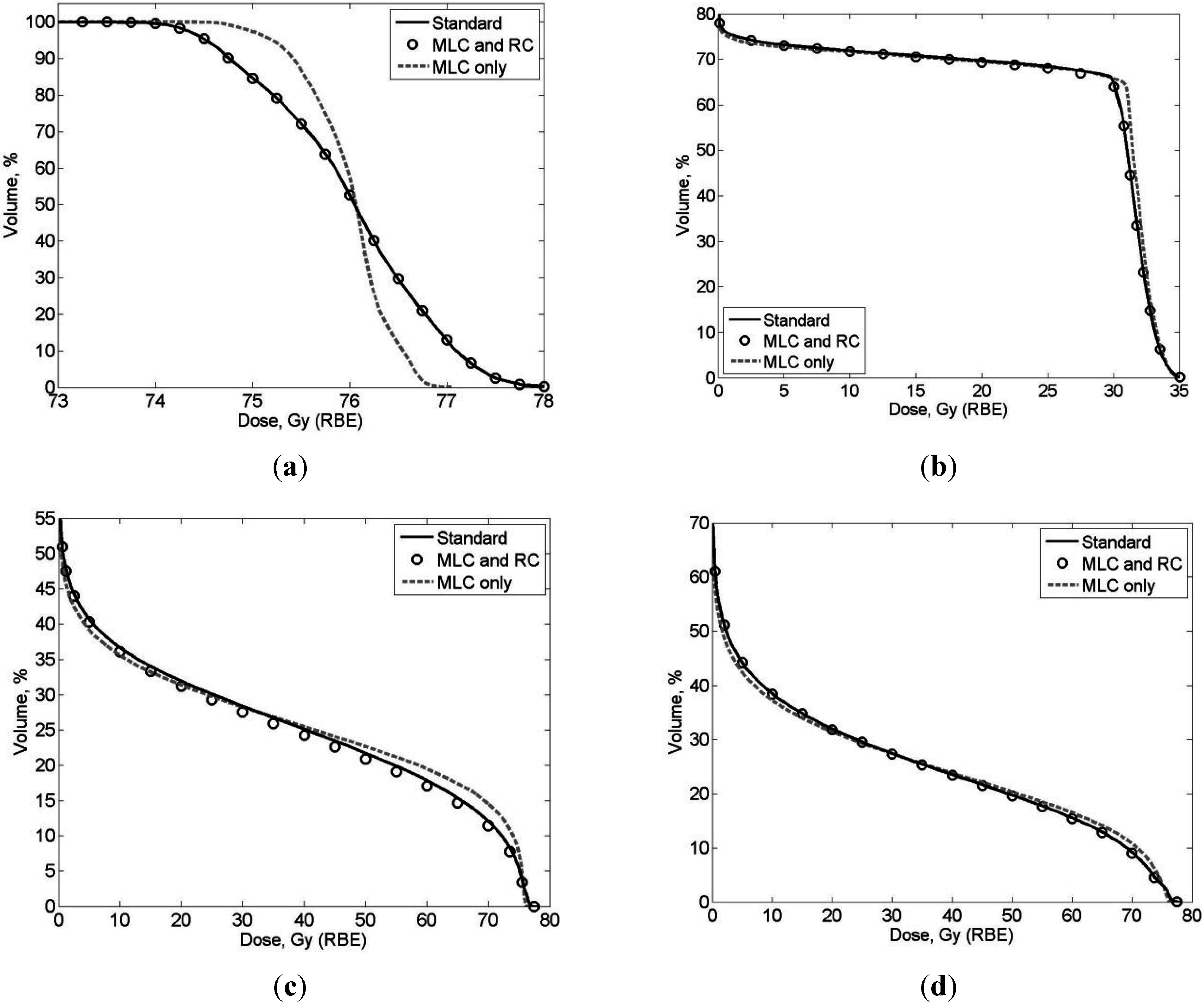
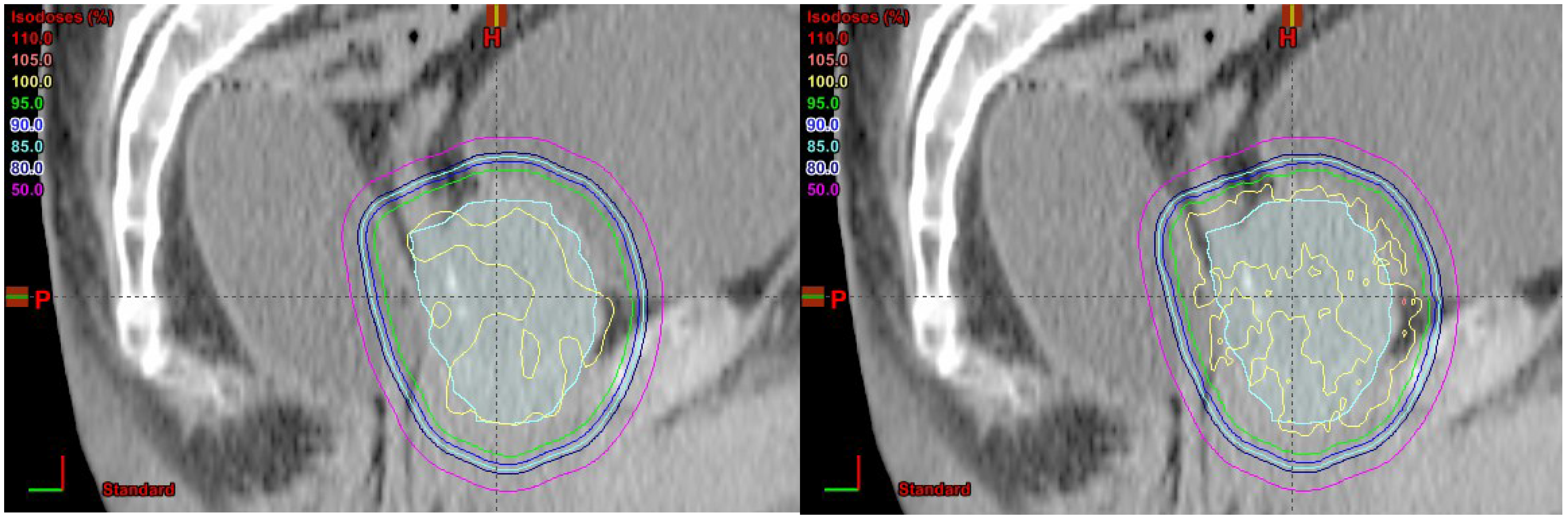
3.1. Comparison of SOC Treatment Plans to MLC + RC and MLC-only Treatment Plans

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Organ | SOC | MLC + RC | MLC Only | |||
|---|---|---|---|---|---|---|
| Max | Mean | Max | Mean | Max | Mean | |
| Anterior Rectal Wall | 76.77 | 39.48 | 76.89 | 75.90 | 76.89 | 75.90 |
| Bladder | 77.09 | 12.87 | 76.35 | 12.18 | 76.35 | 12.06 |
| CTV | 77.63 | 75.90 | 76.89 | 75.90 | 76.89 | 75.90 |
| Distal Seminal Vesicles | 75.37 | 67.63 | 75.87 | 68.74 | 75.80 | 68.29 |
| Femoral Heads | 36.94 | 25.28 | 42.16 | 25.38 | 42.15 | 25.30 |
| Proximal Seminal Vesicles | 76.92 | 75.83 | 76.46 | 75.85 | 76.45 | 75.83 |
| Rectum | 76.81 | 16.73 | 76.34 | 16.81 | 76.33 | 16.76 |

| Organ/Tissue | SOC | MLC Only | ||||
|---|---|---|---|---|---|---|
| External | Internal | Total | External | Internal | Total | |
| Anterior Rectal Wall | 228 | 561 | 788 | 174 | 641 | 815 |
| Bladder | 222 | 363 | 585 | 170 | 413 | 582 |
| CTV | 228 | 840 | 1067 | 172 | 938 | 1110 |
| Distal Seminal Vesicles | 233 | 691 | 924 | 173 | 787 | 960 |
| Femoral Heads | 280 | 531 | 811 | 217 | 572 | 789 |
| Prostate | 227 | 841 | 1068 | 173 | 941 | 1113 |
| Proximal Seminal Vesicles | 239 | 814 | 1053 | 169 | 873 | 1042 |
| Rectum | 223 | 425 | 648 | 171 | 481 | 652 |
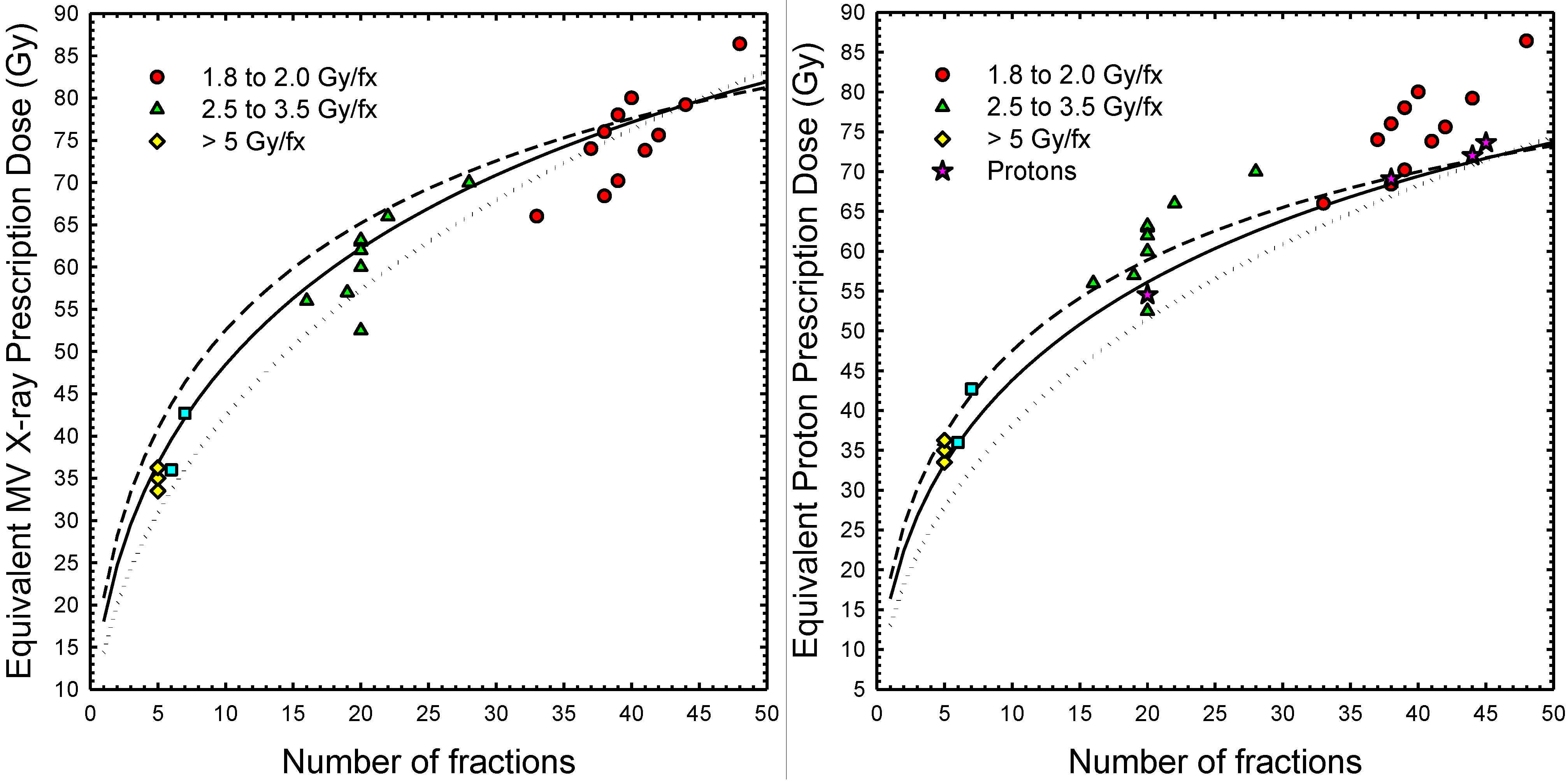
3.2. RBE Effects in Conventional and Hypofractionated Proton Treatments
| n | Fraction Size (Gy) | Total Dose (Gy) | Ratio | ||||
|---|---|---|---|---|---|---|---|
| min | mid | max | min | mid | max | max/min | |
| 1 | 13.0 | 16.4 | 18.9 | 13.0 | 16.4 | 18.9 | 1.45 |
| 3 | 7.3 | 8.9 | 10.1 | 22.0 | 26.8 | 30.3 | 1.38 |
| 5 | 5.6 | 6.7 | 7.4 | 27.9 | 33.3 | 37.0 | 1.33 |
| 10 | 3.8 | 4.4 | 4.8 | 38.2 | 43.8 | 47.5 | 1.25 |
| 15 | 3.0 | 3.4 | 3.6 | 45.6 | 50.8 | 54.2 | 1.19 |
| 20 | 2.6 | 2.8 | 2.9 | 51.5 | 56.1 | 58.9 | 1.14 |
| 25 | 2.3 | 2.4 | 2.5 | 56.5 | 60.4 | 62.6 | 1.11 |
| 30 | 2.0 | 2.1 | 2.2 | 60.9 | 63.9 | 65.5 | 1.08 |
| 35 | 1.9 | 1.9 | 1.9 | 64.8 | 66.8 | 68.0 | 1.05 |
| 38 | 1.8 | 1.8 | 1.8 | 66.9 | 68.4 | 69.2 | 1.03 |
| 40 | 1.7 | 1.7 | 1.8 | 68.3 | 69.4 | 70.0 | 1.03 |
| 44 | 1.6 | 1.6 | 1.6 | 70.8 | 71.2 | 71.4 | 1.01 |
| 45 | 1.6 | 1.6 | 1.6 | 71.5 | 71.7 | 71.8 | 1.00 |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Newhauser, W.D.; Fontenot, J.D.; Mahajan, A.; Kornguth, D.; Stovall, M.; Zheng, Y.; Taddei, P.J.; Mirkovic, D.; Mohan, R.; Cox, J.D.; et al. The risk of developing a second cancer after receiving craniospinal proton irradiation. Phys. Med. Biol. 2009, 54, 2277–2291. [Google Scholar] [CrossRef] [PubMed]
- Gragoudas, E.S. Current approaches in the management of uveal melanomas. Int. Ophthalmol. Clin. 1992, 32, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Zietman, A.L. The Titanic and the Iceberg: Prostate proton therapy and health care economics. J. Clin. Oncol. 2007, 25, 3565–3566. [Google Scholar] [CrossRef] [PubMed]
- Widesott, L.; Pierelli, A.; Fiorino, C.; Dell’oca, I.; Broggi, S.; Cattaneo, G.M.; di Muzio, N.; Fazio, F.; Calandrino, R.; Schwarz, M. Intensity-modulated proton therapy versus helical tomotherapy in nasopharynx cancer: Planning comparison and NTCP evaluation. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Widesott, L.; Amichetti, M.; Schwarz, M. Proton therapy in lung cancer: Clinical outcomes and technical issues. A systematic review. Radiother. Oncol. 2008, 86, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Sugahara, S.; Tokuuye, K.; Okumura, T.; Nakahara, A.; Saida, Y.; Kagei, K.; Ohara, K.; Hata, M.; Igaki, H.; Akine, Y. Clinical results of proton beam therapy for cancer of the esophagus. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Lomax, A.J.; Cella, L.; Weber, D.; Kurtz, J.M.; Miralbell, R. Potential role of intensity-modulated photons and protons in the treatment of the breast and regional nodes. Int. J. Radiat. Oncol. Biol. Phys. 2003, 55, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Rutz, H.P.; Weber, D.C.; Goitein, G.; Ares, C.; Bolsi, A.; Lomax, A.J.; Pedroni, E.; Coray, A.; Hug, E.B.; Timmermann, B. Postoperative spot-scanning proton radiation therapy for chordoma and chondrosarcoma in children and adolescents: Initial experience at paul scherrer institute. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Schaffner, B. Proton dose calculation based on in-air fluence measurements. Phys. Med. Biol. 2008, 53, 1545–1562. [Google Scholar] [CrossRef] [PubMed]
- International Commission on Radiation Units and Measurements. Prescribing, Recording, and Reporting Proton-Beam Therapy ICRU Report 78; Oxford University Press: Oxford, UK, 2007. [Google Scholar]
- Newhauser, W.D.; Ding, X.; Giragosian, D.; Nill, S.; Titt, U. Neutron radiation area monitoring system for proton therapy facilities. Radiat. Prot. Dosim. 2005, 115, 149–153. [Google Scholar] [CrossRef]
- Newhauser, W.D.; Durante, M. Assessing the risk of second malignancies after modern radiotherapy. Nat. Rev. Cancer 2011, 11, 438–448. [Google Scholar] [CrossRef] [PubMed]
- Coutrakon, G.B. Accelerators for heavy-charged-particle radiation therapy. Technol. Cancer Res. Treat. 2007, 6, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Newhauser, W.D.; Zhang, R. The physics of proton therapy. Phys. Med. Biol. 2015. [Google Scholar] [CrossRef]
- Pedroni, E.; Bearpark, R.; Bohringer, T.; Coray, A.; Duppich, J.; Forss, S.; George, D.; Grossmann, M.; Goitein, G.; Hilbes, C.; et al. The PSI Gantry 2: A second generation proton scanning gantry. Z. Med. Phys. 2004, 14, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Lomax, A.J.; Boehringer, T.; Coray, A.; Egger, E.; Goitein, G.; Grossmann, M.; Juelke, P.; Lin, S.; Pedroni, E.; Rohrer, B.; et al. Intensity modulated proton therapy: A clinical example. Med. Phys. 2001, 28, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Goitein, M.; Jermann, M. The relative costs of proton and X-ray radiation therapy. Clin. Oncol. 2003, 15, S37–S50. [Google Scholar] [CrossRef]
- Peeters, A.; Grutters, J.P.; Pijls-Johannesma, M.; Reimoser, S.; de Ruysscher, D.; Severens, J.L.; Joore, M.A.; Lambin, P. How costly is particle therapy? Cost analysis of external beam radiotherapy with carbon-ions, protons and photons. Radiother. Oncol. 2010, 95, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Parthan, A.; Pruttivarasin, N.; Davies, D.; Taylor, D.C.; Pawar, V.; Bijlani, A.; Lich, K.H.; Chen, R.C. Comparative cost-effectiveness of stereotactic body radiation therapy versus intensity-modulated and proton radiation therapy for localized prostate cancer. Front. Oncol. 2012. [Google Scholar] [CrossRef]
- Lievens, Y.; Pijls-Johannesma, M. Health economic controversy and cost-effectiveness of proton therapy. Semin. Radiat. Oncol. 2013, 23, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Bues, M.; Newhauser, W.D.; Titt, U.; Smith, A.R. Therapeutic step and shoot proton beam spot-scanning with a multi-leaf collimator: A Monte Carlo study. Radiat. Prot. Dosim. 2005, 115, 164–169. [Google Scholar] [CrossRef]
- Diffenderfer, E.S.; Ainsley, C.G.; Kirk, M.L.; McDonough, J.E.; Maughan, R.L. Comparison of secondary neutron dose in proton therapy resulting from the use of a tungsten alloy MLC or a brass collimator system. Med. Phys. 2011, 38, 6248–6256. [Google Scholar] [CrossRef] [PubMed]
- Moskvin, V.; Cheng, C.W.; Das, I.J. Pitfalls of tungsten multileaf collimator in proton beam therapy. Med. Phys. 2011, 38, 6395–6406. [Google Scholar] [CrossRef] [PubMed]
- Gottschalk, B. Multileaf collimators, air gap, lateral penumbra, and range compensation in proton radiotherapy. Med. Phys. 2011. [Google Scholar] [CrossRef]
- Daartz, J.; Bangert, M.; Bussiere, M.R.; Engelsman, M.; Kooy, H.M. Characterization of a mini-multileaf collimator in a proton beamline. Med. Phys. 2009, 36, 1886–1894. [Google Scholar] [CrossRef] [PubMed]
- Svensson, R.; Larsson, S.; Gudowska, I.; Holmberg, R.; Brahme, A. Design of a fast multileaf collimator for radiobiological optimized IMRT with scanned beams of photons, electrons, and light ions. Med. Phys. 2007, 34, 877–888. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.R. Prostate cancer and the hypofractionation hypothesis. J. Clin. Oncol. 2013, 31, 3849–3851. [Google Scholar] [CrossRef] [PubMed]
- Tree, A.C.; Alexander, E.J.; van As, N.J.; Dearnaley, D.P.; Khoo, V. Biological dose escalation and hypofractionation: What is there to be gained and how will it best be done? Clin. Oncol. 2013, 25, 483–498. [Google Scholar] [CrossRef]
- Kim, Y.J.; Cho, K.H.; Pyo, H.R.; Lee, K.H.; Moon, S.H.; Kim, T.H.; Shin, K.H.; Kim, J.Y.; Lee, S.B.; Nam, B.H. A phase II study of hypofractionated proton therapy for prostate cancer. Acta Oncol. 2013, 52, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Newhauser, W.D.; Giebeler, A.; Langen, K.M.; Mirkovic, D.; Mohan, R. Can megavoltage computed tomography reduce proton range uncertainties in treatment plans for patients with large metal implants? Phys. Med. Biol. 2008, 53, 2327–2344. [Google Scholar] [CrossRef] [PubMed]
- Newhauser, W.D.; Jones, T.; Swerdloff, S.; Newhauser, W.; Cilia, M.; Carver, R.; Halloran, A.; Zhang, R. Anonymization of DICOM electronic medical records for radiation therapy. Comput. Biol. Med. 2014, 53, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Newhauser, W.; Fontenot, J.; Zheng, Y.; Polf, J.; Titt, U.; Koch, N.; Zhang, X.; Mohan, R. Monte Carlo simulations for configuring and testing an analytical proton dose-calculation algorithm. Phys. Med. Biol. 2007, 52, 4569–4584. [Google Scholar] [CrossRef] [PubMed]
- Fontenot, J.D.; Lee, A.K.; Newhauser, W.D. Risk of secondary malignant neoplasms from proton therapy and intensity-modulated x-ray therapy for early-stage prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 616–622. [Google Scholar] [CrossRef] [PubMed]
- Newhauser, W.D.; Zheng, Y.; Taddei, P.J.; Mirkovic, D.; Fontenot, J.D.; Giebeler, A.; Zhang, R.; Titt, U.; Mohan, R. Monte Carlo proton radiation therapy planning calculations. Trans. Am. Nucl. Soc. 2008, 99, 63–64. [Google Scholar]
- Hendricks, J.S.; McKinney, G.W.; Durkee, J.W.; Finch, J.P.; Fensin, M.L.; James, M.R.; Johns, R.C.; Pelowitz, D.B.; Waters, L.S.; Gallmeier, F.X. MCNPX, Version 26c; Los Alamos National Laboratory: Los Alamos, NM, USA, 2006. [Google Scholar]
- Taddei, P.J.; Mirkovic, D.; Fontenot, J.D.; Giebeler, A.; Zheng, Y.; Kornguth, D.; Mohan, R.; Newhauser, W.D. Stray radiation dose and second cancer risk for a pediatric patient receiving craniospinal irradiation with proton beams. Phys. Med. Biol. 2009, 54, 2259–2275. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Fontenot, J.; Mirkovic, D.; Hendricks, J.; Newhauser, D. Advantages of MCNPX-based lattice tally over mesh tally in high-speed Monte Carlo dose reconstruction for proton radiotherapy. Nucl. Technol. 2013, 183, 101–106. [Google Scholar] [PubMed]
- Fontenot, J.; Taddei, P.; Zheng, Y.; Mirkovic, D.; Jordan, T.; Newhauser, W. Equivalent dose and effective dose from stray radiation during passively scattered proton radiotherapy for prostate cancer. Phys. Med. Biol. 2008, 53, 1677–1688. [Google Scholar] [CrossRef] [PubMed]
- Committee to Assess Health Risks from Exposure to Low Levels of Ionizing Radiation; Board on Radiation Effects Research; Division on Earth and Life Studies; National Research Council. Health Risks from Exposure to Low Levels of Ionizing Radation: BEIR VII-Phase 2; Nation Research Council of the National Academies: Washington, DC, USA, 2006. [Google Scholar]
- Rechner, L.A.; Howell, R.M.; Zhang, R.; Etzel, C.; Lee, A.K.; Newhauser, W.D. Risk of radiogenic second cancers following volumetric modulated arc therapy and proton arc therapy for prostate cancer. Phys. Med. Biol. 2012, 57, 7117–7132. [Google Scholar] [CrossRef] [PubMed]
- ICRP. Basic anatomical and physiological data for use in radiological protection: Reference values: ICRP report 89. Ann. ICRP 2002, 32, 1–277. [Google Scholar]
- Stewart, R.D.; Li, X.A. BGRT: Biologically guided radiation therapy-the future is fast approaching! Med. Phys. 2007, 34, 3739–3751. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.J.; Curtis, R.E.; Hall, E.J.; Ron, E. Second malignancies in prostate carcinoma patients after radiotherapy compared with surgery. Cancer 2000, 88, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Taddei, P.J.; Fontenot, J.D.; Zheng, Y.; Mirkovic, D.; Lee, A.K.; Titt, U.; Newhauser, W.D. Reducing stray radiation dose to patients receiving passively scattered proton radiotherapy for prostate cancer. Phys. Med. Biol. 2008, 53, 2131–2147. [Google Scholar] [CrossRef] [PubMed]
- Paganetti, H. Relative biological effectiveness (RBE) values for proton beam therapy. Variations as a function of biological endpoint, dose, and linear energy transfer. Phys. Med. Biol. 2014, 59, R419–R472. [Google Scholar] [CrossRef] [PubMed]
- Titt, U.; Zheng, Y.; Vassiliev, O.N.; Newhauser, W.D. Monte Carlo investigation of collimator scatter of proton-therapy beams produced using the passive scattering method. Phys. Med. Biol. 2008, 53, 487–504. [Google Scholar] [CrossRef] [PubMed]
- Isacsson, U.; Hagberg, H.; Johansson, K.A.; Montelius, A.; Jung, B.; Glimelius, B. Potential advantages of protons over conventional radiation beams for paraspinal tumours. Radiother. Oncol. 1997, 45, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Oelfke, U.; Bortfeld, T. Intensity modulated radiotherapy with charged particle beams: Studies of inverse treatment planning for rotation therapy. Med. Phys. 2000, 27, 1246–1257. [Google Scholar] [CrossRef] [PubMed]
- Flynn, R.T.; Barbee, D.L.; Mackie, T.R.; Jeraj, R. Comparison of intensity modulated X-ray therapy and intensity modulated proton therapy for selective subvolume boosting: A phantom study. Phys. Med. Biol. 2007, 52, 6073–6091. [Google Scholar] [CrossRef] [PubMed]
- Caporaso, G.J.; Mackie, T.R.; Sampayan, S.; Chen, Y.J.; Blackfield, D.; Harris, J.; Hawkins, S.; Holmes, C.; Nelson, S.; Paul, A.; et al. A compact linac for intensity modulated proton therapy based on a dielectric wall accelerator. Phys. Med. 2008, 24, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Sandison, G.A.; Papiez, E.; Bloch, C.; Morphis, J. Phantom assessment of lung dose from proton arc therapy. Int. J. Radiat. Oncol. Biol. Phys. 1997, 38, 891–897. [Google Scholar] [CrossRef] [PubMed]
- Brodin, N.P.; Vogelius, I.R.; Bjork-Eriksson, T.; Munck Af Rosenschold, P.; Maraldo, M.V.; Aznar, M.C.; Specht, L.; Bentzen, S.M. Optimizing the radiation therapy dose prescription for pediatric medulloblastoma: Minimizing the life years lost attributable to failure to control the disease and late complication risk. Acta Oncol. 2014, 53, 462–470. [Google Scholar] [CrossRef] [PubMed]
- Rechner, L.A.; Eley, J.G.; Howell, R.M.; Zhang, R.; Mirkovic, D.; Newhauser, W.D. Risk-optimized proton therapy to minimize radiogenic second cancers. Phys. Med. Biol. 2015, in press. [Google Scholar]
- Pugh, T.J.; Munsell, M.F.; Choi, S.; Nguyen, Q.N.; Mathai, B.; Zhu, X.R.; Sahoo, N.; Gillin, M.; Johnson, J.L.; Amos, R.A.; et al. Quality of life and toxicity from passively scattered and spot-scanning proton beam therapy for localized prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 946–953. [Google Scholar] [CrossRef] [PubMed]
- Engelsman, M.; Schwarz, M.; Dong, L. Physics controversies in proton therapy. Semin. Radiat. Oncol. 2013, 23, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Schippers, J.M.; Lomax, A.J. Emerging technologies in proton therapy. Acta Oncol. 2011, 50, 838–850. [Google Scholar] [CrossRef] [PubMed]
- Titt, U.; Mirkovic, D.; Sawakuchi, G.O.; Perles, L.A.; Newhauser, W.D.; Taddei, P.J.; Mohan, R. Adjustment of the lateral and longitudinal size of scanned proton beam spots using a pre-absorber to optimize penumbrae and delivery efficiency. Phys. Med. Biol. 2010, 55, 7097–7106. [Google Scholar] [CrossRef] [PubMed]
- Rechner, L.A.; Howell, R.M.; Zhang, R.; Newhauser, W.D. Impact of margin size on the predicted risk of radiogenic second cancers following proton arc therapy and volumetric modulated arc therapy for prostate cancer. Phys. Med. Biol. 2012, 57, N469–N479. [Google Scholar] [CrossRef] [PubMed]
- Hyer, D.E.; Hill, P.M.; Wang, D.; Smith, B.R.; Flynn, R.T. A dynamic collimation system for penumbra reduction in spot-scanning proton therapy: Proof of concept. Med. Phys. 2014. [Google Scholar] [CrossRef]
- Dowdell, S.J.; Clasie, B.; Depauw, N.; Metcalfe, P.; Rosenfeld, A.B.; Kooy, H.M.; Flanz, J.B.; Paganetti, H. Monte Carlo study of the potential reduction in out-of-field dose using a patient-specific aperture in pencil beam scanning proton therapy. Phys. Med. Biol. 2012, 57, 2829–2842. [Google Scholar] [CrossRef] [PubMed]
- Kirk, M.; Ainsley, C.; McDonough, J. Comparison of proton MLC with non-divergent brass and tungsten apertures. Med. Phys. 2010, 37, 3280. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Newhauser, W.D.; Zhang, R.; Jones, T.G.; Giebeler, A.; Taddei, P.J.; Stewart, R.D.; Lee, A.; Vassiliev, O. Reducing the Cost of Proton Radiation Therapy: The Feasibility of a Streamlined Treatment Technique for Prostate Cancer. Cancers 2015, 7, 688-705. https://doi.org/10.3390/cancers7020688
Newhauser WD, Zhang R, Jones TG, Giebeler A, Taddei PJ, Stewart RD, Lee A, Vassiliev O. Reducing the Cost of Proton Radiation Therapy: The Feasibility of a Streamlined Treatment Technique for Prostate Cancer. Cancers. 2015; 7(2):688-705. https://doi.org/10.3390/cancers7020688
Chicago/Turabian StyleNewhauser, Wayne D., Rui Zhang, Timothy G. Jones, Annelise Giebeler, Phillip J. Taddei, Robert D. Stewart, Andrew Lee, and Oleg Vassiliev. 2015. "Reducing the Cost of Proton Radiation Therapy: The Feasibility of a Streamlined Treatment Technique for Prostate Cancer" Cancers 7, no. 2: 688-705. https://doi.org/10.3390/cancers7020688
APA StyleNewhauser, W. D., Zhang, R., Jones, T. G., Giebeler, A., Taddei, P. J., Stewart, R. D., Lee, A., & Vassiliev, O. (2015). Reducing the Cost of Proton Radiation Therapy: The Feasibility of a Streamlined Treatment Technique for Prostate Cancer. Cancers, 7(2), 688-705. https://doi.org/10.3390/cancers7020688