Utility of MRI Diffusion Techniques in the Evaluation of Tumors of the Head and Neck

Abstract
:1. Introduction
2. Physical Basis of DWI and Technical Aspects of DWI in the Neck
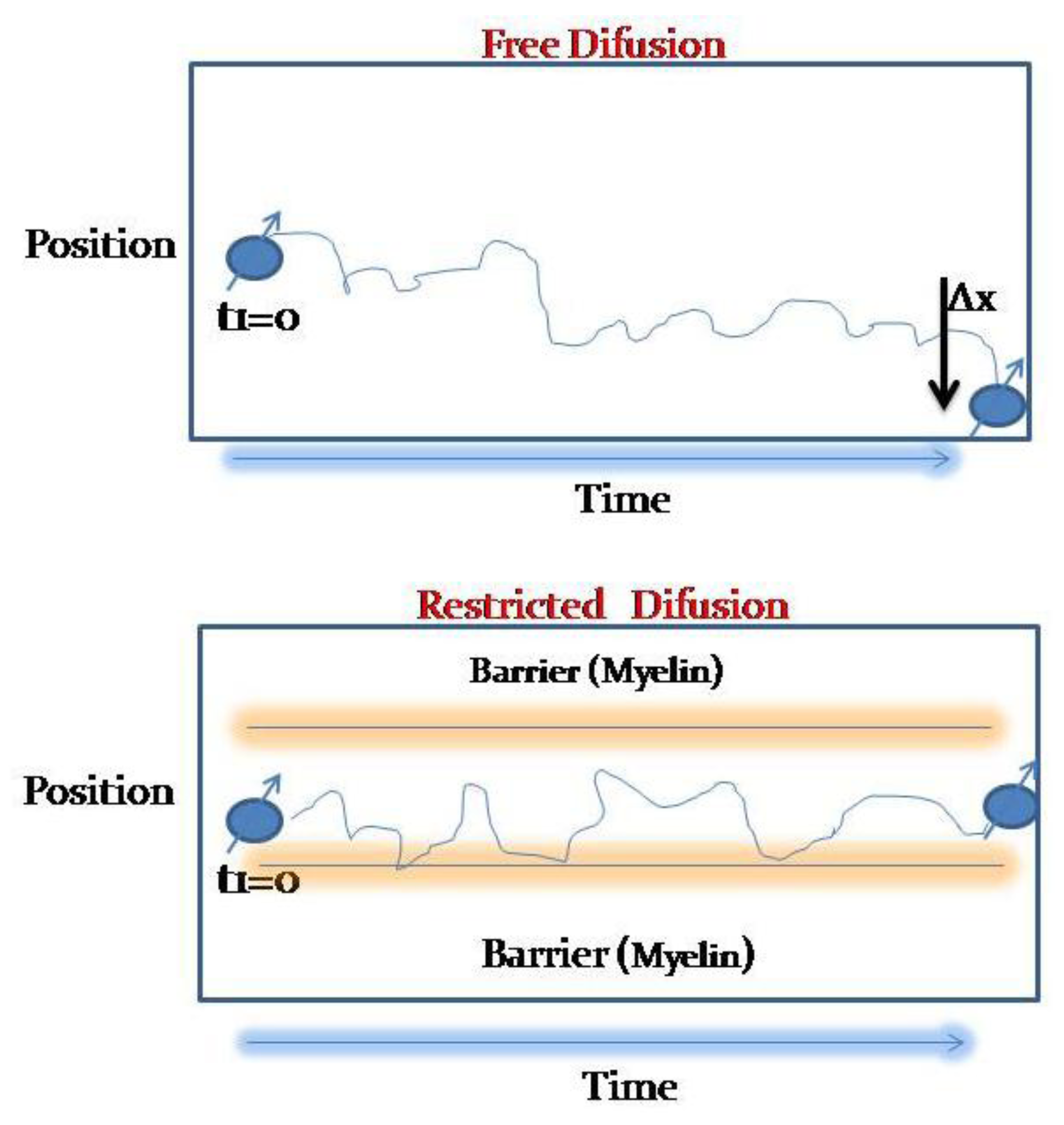
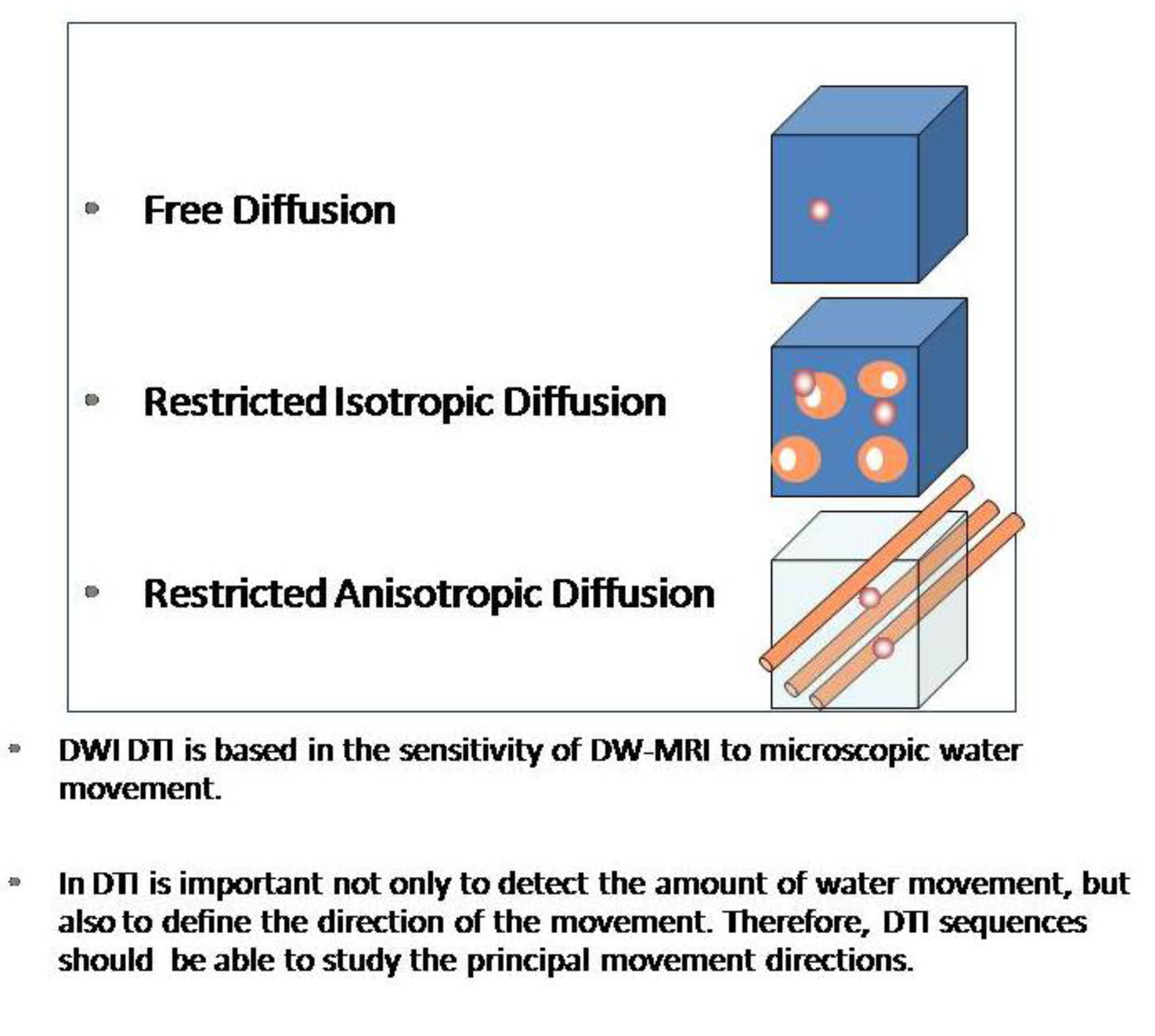
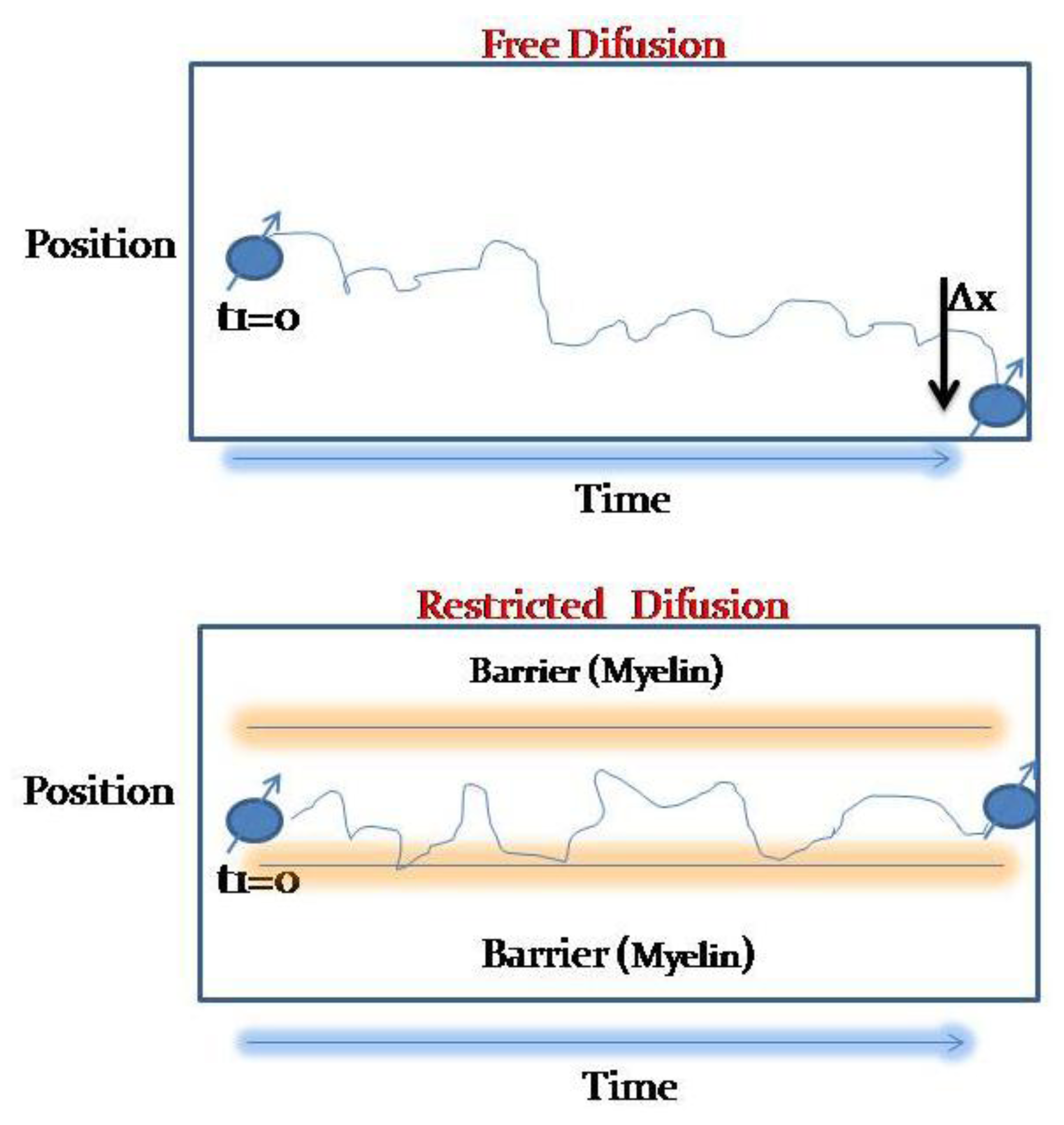
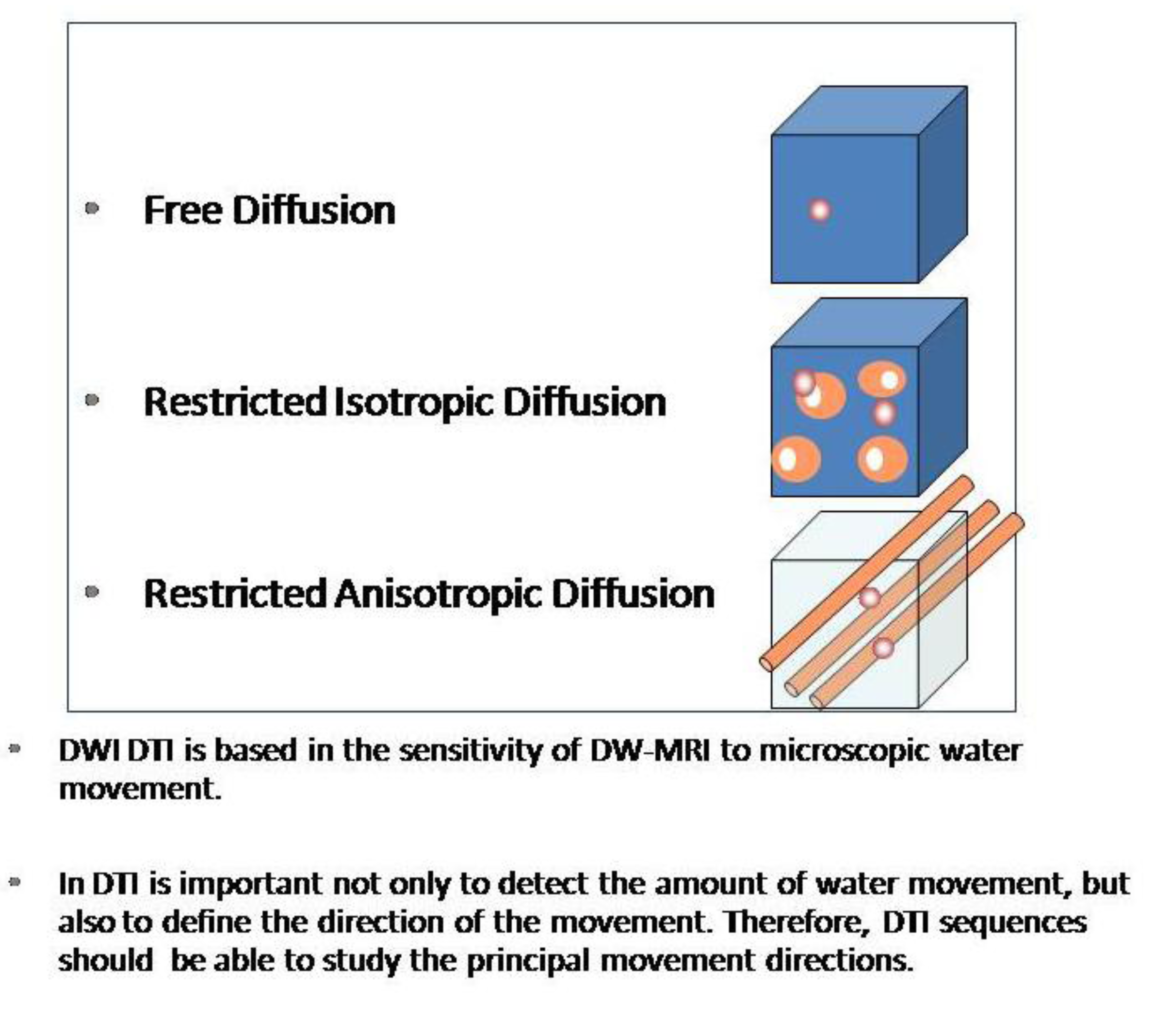
2.1. Physical Basis of DWI
2.2. Technical Aspects of DWI in the Neck

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Minimize T1 saturation | TR (repetition time) should be long enough to avoid T1 saturation effects |
|---|---|
| Use short TE (echo time) | Increasing the bandwidth (up to a maximum of 1,500 MHz) using parallel imaging (SENSE factor up to 2) and by increasing the gradient intensity in the gradient lobes |
| Increase the number of adquisitions (NEX) | Noise is disruptive and the signal is additive |
| Decrease the field of view (FOV) | Minimum in phase encoding direction. |
| Do not increase the resolution in plane to levels where the noise increases | It will decrease the quality of ADC maps; enlarging the FOV may have a similar result |
| Use fat supression sequences | Increase the dynamic range of the DWI |
2.3. Measurement Approach of ADC Values in the Head and Neck
3. Clinical Applications of MRI-DWI in Head Neck Neoplastic Lesions
3.1. Detection and Evaluation of Primary Malignancies of the Upper Respiratory Tract and Malignant Lymph Nodes
3.2. Salivary Gland Tumors, Orbitary and Pediatric Lesions
4. Conclusions
Acknowledgments
Conflict of Interest
References
- Grégorie, V.; Lefebvre, J.L.; Licitra, F.; Felip, E.; EHNS-ESMO-ESTRO Guidelines Working Group. Squamous cell carcinoma of the head and neck: EHNS-ESMO-ESTRO Clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2010, 21, 184–186. [Google Scholar] [CrossRef]
- Franca, C.; Levin-Plotnik, D.; Sehgal, V.C.; Chen, G.; Ramsey, R.G. Use of three-dimensional spiral computed tomography imaging for staging and surgical planning of head and neck cancer. J. Digit. Imaging 2000, 13, 24–32. [Google Scholar] [CrossRef]
- Sauter, A.W.; Spira, D.; Schulze, M.; Pfannenberg, C.; Hetzel, J.; Reimold, M.; Klotz, E.; Claussen, C.D.; Horger, M.S. Correlation between [(18)F]FDG PET/CT and volume perfusion CT in primary tumours and mediastinal lymph nodes of non-small-cell lung cancer. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 677–684. [Google Scholar] [CrossRef]
- Veit-Haibach, P.; Schmid, D.; Strobel, K.; Soyka, J.D.; Schaefer, N.G.; Haerle, S.K.; Huber, G.; Studer, G.; Seifert, B.; Hany, T.F. Combined PET/CT-perfusion in patients with head and neck cancers. Eur. Radiol. 2013, 23, 163–173. [Google Scholar] [CrossRef]
- Trojanowska, A.; Trojanowski, P.; Bisdas, S.; Staśkiewicz, G.; Drop, A.; Klatka, J.; Bobek-Billewicz, B. Squamous cell cancer of hypopharynx and larynx—Evaluation of metastatic nodal disease based on computed tomography perfusion studies. Eur. J. Radiol. 2012, 81, 1034–1039. [Google Scholar] [CrossRef]
- Hermans, R.; de keyzer, F.; Vandecaveye, V.; Carp, L. Imaging techniques. In Head and Neck Cancer Imaging; Springer: Berlin/Heidelberg, Germany, 2012; pp. 33–54. [Google Scholar]
- Akter, M.; Hirai, T.; Minoda, R.; Murakami, R.; Saiki, S.; Okuaki, T.; Kitajima, M.; Fukuoka, H.; Sasao, A.; Nishimura, S.; et al. Diffusion tensor tractography in the head-and-neck region using a clinical 3-T MR scanner . Acad. Radiol. 2009, 16, 858–865. [Google Scholar]
- Padhani, A.R.; Liu, G.; Mu-Kon, D.; Chenevert, T.L.; Thoeny, H.C.; Takahara, T.; Dzik-Jurasz, A.; Ross, B.D.; van Cauteren, M.; Collins, D.; et al. Diffusion-Weighted Magnetic Resonance Imaging as a Cancer Biomarker: Consensus and Recommendations. Neoplasia 2009, 11, 102–125. [Google Scholar]
- Varoquaux, A.; Rager, O.; Lovblad, K.O.; Masterson, K.; Dulguerov, P.; Ratib, O.; Becker, C.D. Functional imaging of head and neck squamous cell carcinoma with diffusion-weighted MRI and FDG PET/CT: Quantitative analysis of ADC and SUV. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 842–852. [Google Scholar] [CrossRef]
- Stadlbauer, A.; Bernt, R.; Gruber, S.; Bogner, W.; Pinker, K.; van der Riet, W.; Haller, J.; Salomonowitz, E. Diffusion-weighted MR imaging with background body signal suppression (DWIBS) for the diagnosis of malignant and benign breast lesions. Eur. Radiol. 2009, 19, 2349–2356. [Google Scholar] [CrossRef]
- Rodriguez, I.; Martin, I.; Luna, A. Role of DWI in the evaluation of tumors of the head and neck and in the assessment of lymph nodes. In Diffusion MRI outside the Brain; Luna, A., Ribes, R., Soto, J.A., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 307–337. [Google Scholar]
- Huisman, T.A.G.M.; Loenneker, T.; Barta, G.; Bellemann, M.E.; Hennig, J.; Fischer, J.E.; Il’yasov, K.A. Quantitative diffusion tensor MR imaging of the brain: Field strength related variance of apparent diffusion coefficient (ADC) and fractional anisotropy (FA) scalars. Eur. Radiol. 2006, 16, 1651–1658. [Google Scholar] [CrossRef]
- Le Bihan, D.; Breton, E.; Lallemand, D.; Aubin, M.L.; Vignaud, J.; Laval-Jeantet, M. Separation of diffusion and perfusion in intravoxel incoherent motion MR Imaging. Radiology 1998, 168, 497–505. [Google Scholar]
- Lu, Y.; Jansen, J.F.; Mazaheri, Y.; Stambuk, H.E.; Koutcher, J.A.; Shukla-Dave, A. Extension of the intravoxel incoherent motion model to non-gaussian diffusion in head and neck cancer. J. Magn. Reson. Imaging 2012, 36, 1088–1096. [Google Scholar] [CrossRef]
- Rheinheimer, S.; Stieltjes, B.; Schneider, F.; Simon, D.; Pahernik, S.; Kauczor, H.U.; Hallscheidt, P. Investigation of renal lesions by diffusion-weighted magnetic resonance imaging applying intravoxel incoherent motion-derived parameters—Initial experience. Eur. J. Radiol. 2012, 81, 310–316. [Google Scholar] [CrossRef]
- Guiu, B.; Cercueil, J.P. Liver diffusion-weighted MR imaging: The tower of babel? Eur. Radiol. 2011, 21, 463–467. [Google Scholar]
- Döpfert, J.; Lemke, A.; Weidner, A.; Schad, LR. Investigation of prostate cancer using diffusion-weighted intravoxel incoherent motion imaging. Magn. Reson. Imaging 2011, 29, 1053–1058. [Google Scholar] [CrossRef]
- Hauser, T.; Essi, M.; Jensen, A.; Gerigk, L.; Laun, F.B.; Münter, M.; Simon, D.; Stieltjes, B. Characterization and therapy monitoring of head and neck carcinomas using diffusion-imaging-based intravoxel incoherent motion parameters-preliminary results. Neuroradiology 2013, 55, 527–536. [Google Scholar] [CrossRef]
- Sumi, M.; Nakamura, T. Head and neck tumors: Assessment of perfusion-related parameters and diffusion coefficients based on the intravoxel incoherent motion model. Am. J. Neuroradiol. 2013, 34, 410–416. [Google Scholar] [CrossRef]
- Herneth, A.M.; Mayerhoefer, M.; Schernthaner, R.; Ba-Ssalamah, A.; Czerny, C.; Fruehwald-Pallamar, J. Diffusion weighted imaging: Lymph nodes. Eur. J. Radiol. 2010, 76, 398–405. [Google Scholar] [CrossRef]
- Park, J.K.; Kim, S.E.; Trieman, G.S.; Parker, D.; Jeong, E.K. High-resolution diffusion-weighted imaging of neck lymph nodes using 2D-single-shot interleaved multiple inner volume imaging diffusion-weighted echo-planar imaging at 3T. Am. J. Neuroradiol. 2011, 32, 1173–1177. [Google Scholar] [CrossRef]
- Verhappen, M.H.; Pouwels, P.J.; Ljumanovic, R.; van der Putten, L.; Knol, D.L.; de Bree, R.; Castelijns, J.A. Diffusion-weighted MR imaging in head and neck cancer: Comparison between half-fourier acquired single-shot turbo spin-echo and EPI techniques. Am. J. Neuroradiol. 2012, 33, 1239–1246. [Google Scholar] [CrossRef]
- Maeda, M.; Maier, S.E. Usefulness of diffusion-weighted imaging and the apparent diffusion coefficient in the assessment of head and neck tumors. J. Neuroradiol. 2008, 35, 71–78. [Google Scholar] [CrossRef]
- Maeda, M.; Kato, H.; Sakuma, H.; Maier, S.E.; Takeda, K. Usefulness of the apparent diffusion coefficient in line scan diffusion-weighted imaging for distinguishing between squamous cell carcinomas and malignant lymphomas of the head and neck. AJNR Am. J. Neuroradiol. 2005, 2, 1186–1192. [Google Scholar]
- Sumi, M.; Sakihama, N.; Sumi, T.; Morikawa, M.; Uetani, M.; Kabasawa, H.; Shigeno, K.; Hayashi, K.; Takahashi, H.; Nakamura, T. Discrimination of metastatic cervical lymph modes with diffusion-weithed MR Imaging in patiens with head and neck cancer. AJNR Am. J. Neuroradiol. 2003, 24, 1627–1634. [Google Scholar]
- Kim, J.K.; Kim, K.A.; Park, B.W.; Kim, N.; Cho, K.S. Feasibility of diffusion-weighted imaging in the differentiation of metastatic from nonmetastatic lymph nodes: Early experience. J. Magn. Reson. Imaging 2008, 28, 714–719. [Google Scholar] [CrossRef]
- King, A.D.; Ahuja, A.T.; Yeung, D.K.; Fong, D.K.; Lee, Y.Y.; Lei, K. Malignant cervical lymphadenopathy: Diagnostic accuracy of diffusion-weighted MR imaging. Radiology 2007, 245, 806–813. [Google Scholar] [CrossRef]
- Kwee, T.C.; Takahara, T.; Luijten, P.R.; Nievelstein, R.A.J. ADC measurements of lymph nodes: Inter- and intra-observer reproducibility study and an overview of the literature. Eur. J. Radiol. 2010, 75, 215–220. [Google Scholar] [CrossRef]
- Herneth, A.M.; Mayerhoefer, M.; Schernthaner, R. Diffusion weighted imaging: Lymph nodes. Eur. J. Radiol. 2010, 76, 398–406. [Google Scholar] [CrossRef]
- Thoeny, H.C.; de Keyzer, F.; King, A.D. Diffusion-Weighted MR Imaging in head and Neck. Radiology 2012, 263, 19–32. [Google Scholar] [CrossRef]
- Chawla, S.; Kim, S.; Wang, S.; Poptani, H. Diffusion-weighted imaging in head and neck cancers. Future Oncol. 2009, 5, 959–975. [Google Scholar] [CrossRef]
- Fong, D.; Bhatia, K.S.; Yeung, D.; King, A.D. Diagnostic accuracy of diffusion-weighted MR imaging for nasopharyngeal carcinoma, head and neck lymphoma and squamous cell carcinoma at the primary site. Oral Oncol. 2010, 46, 603–606. [Google Scholar] [CrossRef]
- Vandecaveye, V.; Dirix, P.; de Keyzer, F.; de Beeck, K.O.; Vander Poorten, V.; Roebben, I.; Nuyts, S.; Hermans, R. Predictive value of diffusion-weighted magnetic resonance imaging during chemoradiotherapy for head and neck squamous cell carcinoma. Eur. Radiol. 2010, 20, 1703–1715. [Google Scholar] [CrossRef]
- Kim, S.; Loevner, L.; Quon, H.; Sherman, E.; Weinstein, G.; Kilger, A.; Poptani, H. Diffusion-weighted magnetic resonance imaging for predicting and detecting early response to chemoradiation therapy of squamous cell carcinomas of the head and neck. Clin. Cancer Res. 2009, 15, 986–994. [Google Scholar] [CrossRef]
- Hermans, R. Diffusion-weighted MRI in head and neck cancer. Curr. Opin. Otoralyngol. Head Neck Surg. 2010, 18, 72–78. [Google Scholar] [CrossRef]
- Wang, J.; Takashima, S.; Takayama, F.; Kawakami, S.; Saito, A.; Matsushita, T.; Momose, M.; Ishiyama, T. Head and Neck Lesions: Characterization with Diffusion-weithed Echo planar MR Imaging. Radiology 2001, 220, 621–630. [Google Scholar] [CrossRef]
- Razek, A.A.; Megahed, A.S.; Denewer, A.; Motamed, A.; Tawfik, A.; Nada, N. Role of diffusion-weighted magnetic resonance imaging in differentiation between the viable and necrotic parts of head and neck tumors. Acta Radiol. 2008, 49, 364–370. [Google Scholar] [CrossRef]
- Eida, S.; Sumi, M.; Sakihama, N.; Takahashi, H.; Nakamura, T. Apparent Diffusion Coefficient Mapping of Salivary Gland Tumors: Prediction of the Benignancy and Malignancy. AJNR Am. J. Neuroradiol. 2007, 28, 116–121. [Google Scholar]
- Razek, A.; Gaballa, G.; Elhawarey, G.; Megahed, A.S.; Hafez, M.; Nada, N. Characterization of pediatric head and neck masses with diffusion-weitghed MR imaging. Eur. Radiol. 2009, 19, 201–208. [Google Scholar] [CrossRef]
- Freling, N.J.; Merks, J.H.; Saeed, P.; Balm, A.J.; Bras, J.; Pieters, B.R.; Adam, J.A.; van Rijn, R.R. Imaging findings in craniofacial childhood rhabdomyosarcoma. Pediatr. Radiol. 2010, 40, 1723–1738. [Google Scholar]
- Viets, R.; Parsons, M.; van Stavern, G.; Hildebolt, C.; Sharma, A. Hyperintense optic nerve heads on diffusion-weighted imaging: a potential imaging sign of papilledema. AJNR Am. J. Neuroradiol. 2013. [Google Scholar] [CrossRef]
- Fatima, Z.; Motosugi, U.; Muhi, A.; Hori, M.; Ishigame, K.; Araki, T. Diffusion-weighted imaging in optic neuritis. Assoc. Radiol. J. 2013, 64, 51–55. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Martínez Barbero, J.P.; Rodríquez Jiménez, I.; Martin Noguerol, T.; Luna Alcalá, A. Utility of MRI Diffusion Techniques in the Evaluation of Tumors of the Head and Neck. Cancers 2013, 5, 875-889. https://doi.org/10.3390/cancers5030875
Martínez Barbero JP, Rodríquez Jiménez I, Martin Noguerol T, Luna Alcalá A. Utility of MRI Diffusion Techniques in the Evaluation of Tumors of the Head and Neck. Cancers. 2013; 5(3):875-889. https://doi.org/10.3390/cancers5030875
Chicago/Turabian StyleMartínez Barbero, José Pablo, Inmaculada Rodríquez Jiménez, Teodoro Martin Noguerol, and Antonio Luna Alcalá. 2013. "Utility of MRI Diffusion Techniques in the Evaluation of Tumors of the Head and Neck" Cancers 5, no. 3: 875-889. https://doi.org/10.3390/cancers5030875
APA StyleMartínez Barbero, J. P., Rodríquez Jiménez, I., Martin Noguerol, T., & Luna Alcalá, A. (2013). Utility of MRI Diffusion Techniques in the Evaluation of Tumors of the Head and Neck. Cancers, 5(3), 875-889. https://doi.org/10.3390/cancers5030875