Positron Emission Tomography (PET) in Oncology

Abstract
:1. FDG-PET/CT for Tumor Staging
1.1. Lung Cancer
1.1.1. T Staging
1.1.2. N Staging
1.1.3. M Staging
1.2. Colorectal Cancer (CRC)
1.3. Esophageal Cancer
1.4. Gastric and Gastroesophagal Cancer
1.5. Pancreatic Cancer
1.6. Head and Neck Squamous Cell Carcinoma
1.7. Breast Cancer
1.8. Other Gynecological Malignancies
1.8.1. Ovarian Cancer
1.8.2. Uterine Cervical Cancer
1.8.3. Melanoma
1.8.4. Lymphoma

{kind=link}
| Tumor Type | Diagnosis | Staging | Prognosis |
|---|---|---|---|
| Lung | ++ (solitary lung nodule) − (bronchoalveolar cell carcinoma, carcinoid tumor = low FDG avidity) | T: +/− N: + (EBUS/TBNA, EUS/FNA or histology often required) M: ++ | + (SUVMax, MTV) |
| Breast | +/− (routinely not used) | N: +/− (SLNB = gold standard for early stage) M: ++ (if advanced stage or risk factors) | + (SUVMax: correlation with histopathology, distant metastasis) |
| Ovarian cancer | − (lack of sensitivity) | Initial: − routinely not used, discussed in advanced disease/suspicion of peritoneal carcinomatosis Recurrence: ++ (CA125 elevation) | + (?), more data needed (MTV, SUVMax) |
| Cervical carcinoma | − | T: − (MRI better) N: ++ in advanced disease (but surgical staging generally required if PET negative) M: ++ (advanced stage) | + (SUVMax, lymph node involvement localization) |
| HNSCC | ++ (cervical lymph node of unknown primary tumor) | T: + N: + (if PET negative, surgical staging generally requires) M: ++ | + (more in treatment response evaluation) |
| Colorectal cancer | − | − (routinely not used) + discussed if potentially operable metastasis, problem solving or CEA elevation (recurrence) | + (?) more data needed |
| Esophageal cancer | − | squamous cell cancer: +/− adenocarcinoma: + | + |
| Gastric cancer | − (lower FDG avidity for diffuse type histology (mucinous, signet ring)) | − | More data needed |
| Pancreatic cancer | + (differentiating benign/malignant, IPMN) | +/− (not routinely used, might be discussed) | + (SUVMax, MTV, TGL) |
| Melanoma | − | ++ (advanced stage) ++ (surveillance if advanced stage) | + |
2. FDG-PET/CT in Solitary Pulmonary Nodule (SPN)
3. PET for Interim Tumor Response Assessment
| Tumor | Initial Staging | Interim Assessment |
|---|---|---|
| Breast | +(+) | ++ |
| Lung (NSCLC) | +(+) | ++ |
| Colorectal | −− | ++ |
| HNSCC | ++ | + |
| Esophagus | ++ | ++ |
3.1. Lymphoma
3.2. Breast Cancer
3.3. Colorectal Cancer
3.4. Head and Neck Squamous Cell Carcinoma
3.5. Non-Small Cell Lung Cancer
3.6. Esophageal Cancer
4. PET for Tumor Response
4.1. Radiological Imaging for Tumor Response
4.2. The Problem of Residual Mass at the End of Treatment
4.3. Functional Imaging for Tumor Response
| Response Assessment at Interim | PET-CT Findings at Interim | Remission Assessment at End-of-Treatment | PET-CT Findings at End of Treatment |
|---|---|---|---|
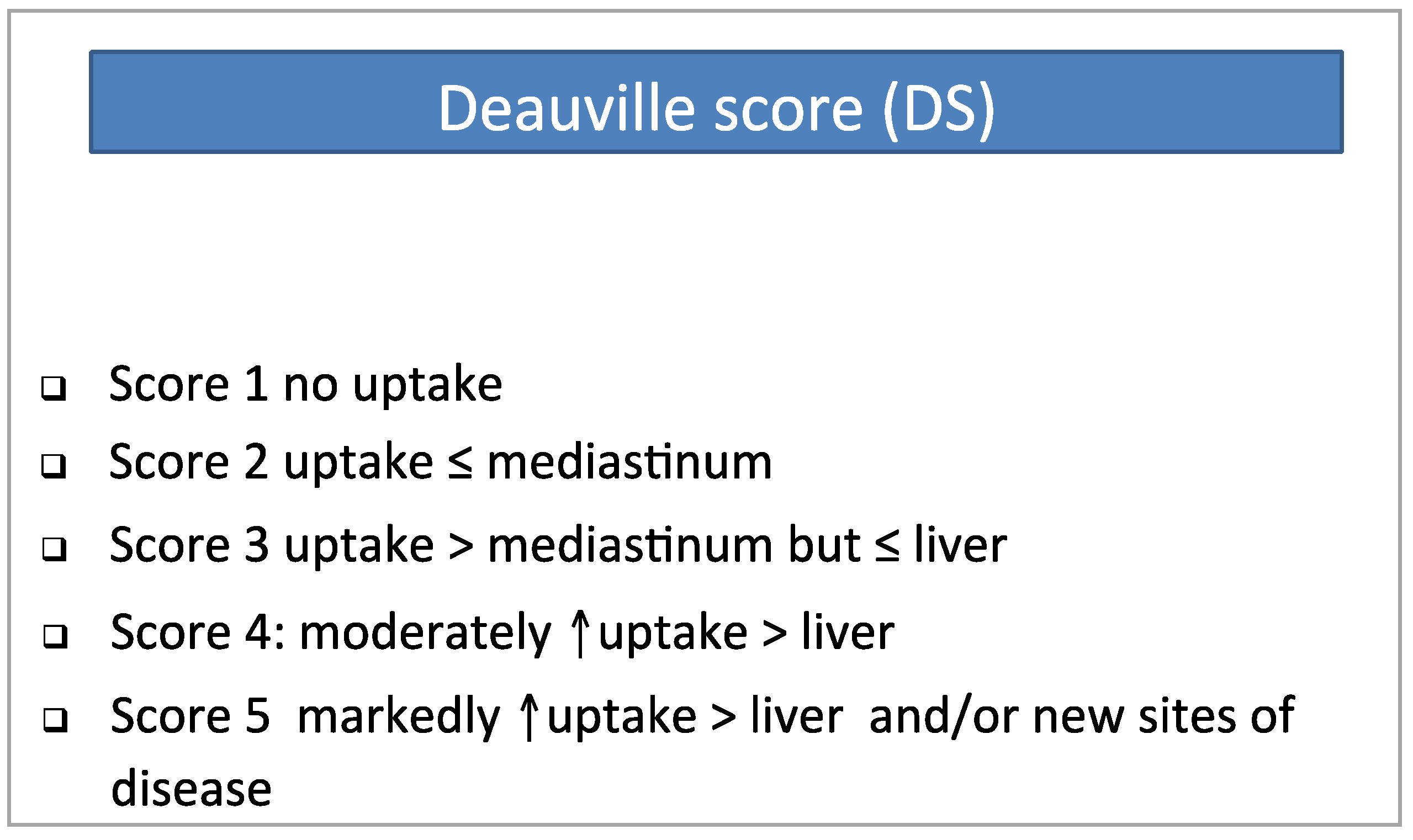
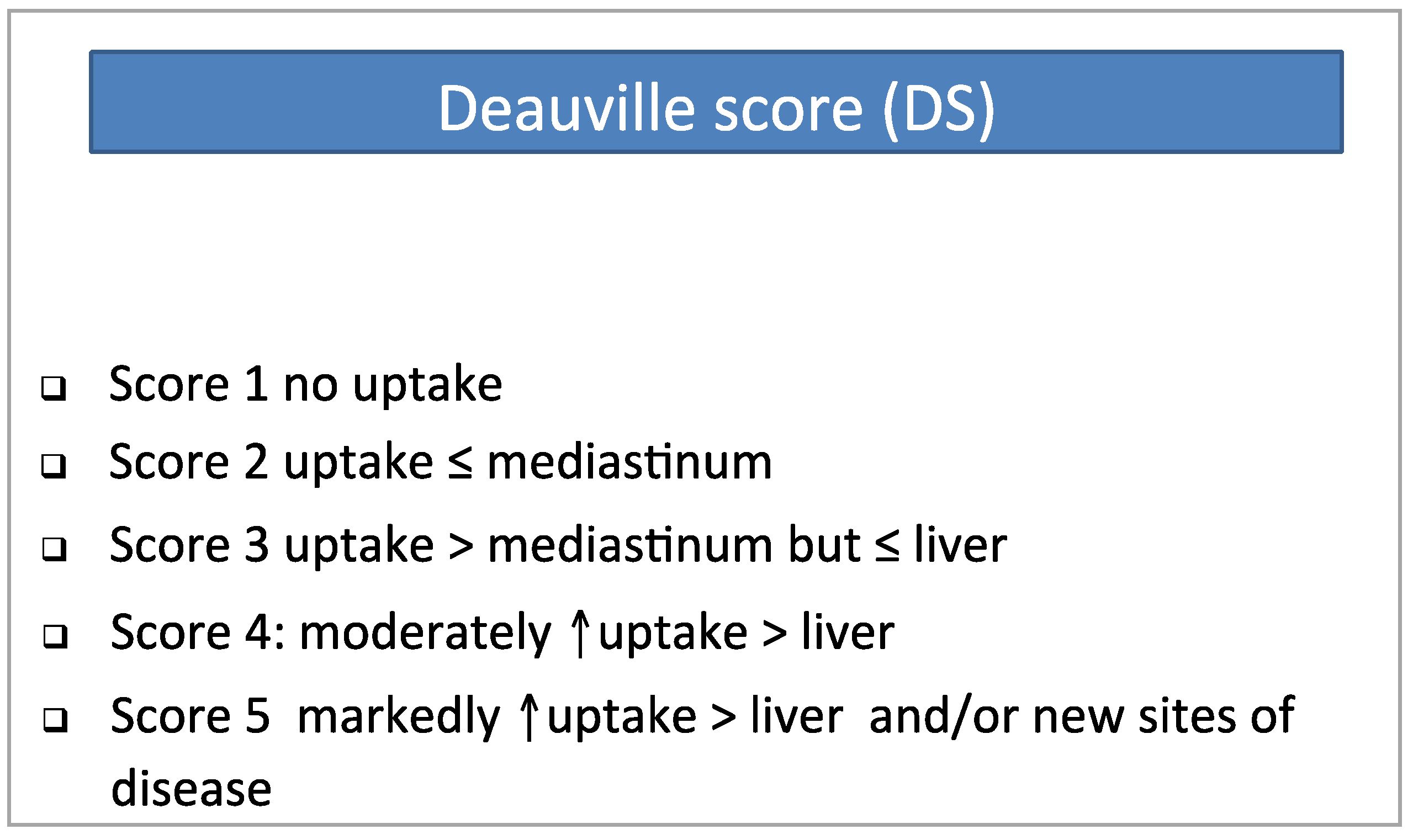
| Complete Metabolic Response (CMR) | Score 1, 2 Score 3 also likely represents a good response at interim but an end-of-treatment scan is recommended for further evaluation. | Complete Metabolic Response (CMR) | Residual mass of any size and Score 1, 2. Score 3 should be interpreted according to the clinical context and pre-treatment prognosis but in many patients indicates a good prognosis/CMR with standard treatment. For trials where de-escalation strategies are being investigated, it may be preferable to consider score 3 as inadequate response to avoid under-treatment. |
| Partial metabolic response (PMR) | Score 4 or 5 & reduced uptake from baseline | Residual metabolic disease (RMD) | Score 4 or 5, with reduced uptake from baseline & residual mass of any size (but no new lesions) |
| No metabolic response or Progressive Metabolic Disease (NMR/PMD) | Score 5 & no significant decrease in uptake or new FDG avid foci consistent with lymphoma | No Metabolic Response or Progressive metabolic disease (NMR/PMD) | Score 4 or 5 & no significant change in uptake from baseline or new FDG avid foci consistent with lymphoma or increase in uptake in previous disease foci |
4.4. Breast Cancer
4.5. Colorectal Cancer
4.6. Non-Small-Cell Lung Cancer
4.7. Head and Neck Squamous Cell Carcinoma
4.8. Epithelial Ovarian Cancer
5. MTV in Oncology
5.1. The Visual or Gradient Segmentation Method: The First One Applied and Still Widely Used
5.2. Fixed-Percentage Threshold Segmentation Method
5.3. Maximal Intensity Threshold
5.4. Adaptive Threshold Segmentation Method
5.5. Methods of Tumor Contour
5.6. Other Methods
6. FDG-PET and Multiple Myeloma
7. FDG-PET/CT in Surveillance of Cancer
8. New PET Technologies and Tracers
9. Conclusions
Abbreviations
| FDG | 18-Fluorodeoxyglucose |
| PET | Positron Emission Tomography |
| CT | Computed Tomography |
| FDG-PET/CT | Combined Positron Emission Tomography and Computed Tomography |
| SPECT | Single-photon Emission Computed Tomography |
| MRI | Magnetic Resonance Imaging |
| US | Ultrasound |
| EUS | Endoscopy Ultrasound |
| BS | Bone Scintigraphy |
| SUV | Standardized Uptake Value |
| SUVMax | Maximal SUV Value |
| SUVMean | Median SUV Value |
| SUVPeak | SUV value in a1-cm3 volume spherical ROI |
| ΔSUV | reduction in SUVMax |
| ROI | Region Of Interest |
| MTV | Metabolic Tumor Volume |
| TLG | Total Lesion Glycolysis |
| CeCT | Contrast-Enhanced Computed Tomography |
| BMB | Bone Marrow Biopsy |
| B/BM | Bone and Bone Marrow |
| PPV | Positive Predictive Value |
| NPV | Negative Predictive Value |
| AUC | Area Under Curve |
| ROC | Receiver Operating Charateristic |
Conflicts of Interest
References
- Avril, N.; Sassen, S.; Roylance, R. Response to therapy in breast cancer. J. Nucl. Med. 2009, 50, 55S–63S. [Google Scholar]
- Strauss, L.G.; Conti, P.S. The applications of PET in clinical oncology. J. Nucl. Med. 1991, 32, 623–648. [Google Scholar]
- Zasadny, K.R.; Wahl, R.L. Standardized uptake values of normal tissues at PET with 2-[fluorine-18]-fluoro-2-deoxy-D-glucose: Variations with body weight and a method for correction. Radiology 1993, 189, 847–850. [Google Scholar]
- American Joint Committee on Cancer. AJCC Cancer Staging Manual, 6th ed.; Springer: New York, NY, USA, 2002. [Google Scholar]
- Adebonojo, S.A.; Bowser, A.N.; Moritz, D.M.; Corcoran, P.C. Impact of revised stage classification of lung cancer on survival: A military experience. Chest 1999, 115, 1507–1513. [Google Scholar]
- Mountain, C.F. Revisions in the International System for Staging Lung Cancer. Chest 1997, 111, 1710–1717. [Google Scholar]
- Tylski, P.; Stute, S.; Grotus, N.; Doyeux, K.; Hapdey, S.; Gardin, I.; Vanderlinden, B.; Buvat, I. Comparative assessment of methods for estimating tumor volume and standardized uptake value in (18)F-FDG PET. J. Nucl. Med. 2010, 51, 268–276. [Google Scholar]
- Larson, S.M.; Erdi, Y.; Akhurst, T.; Mazumdar, M.; Macapinlac, H.A.; Finn, R.D.; Casilla, C.; Fazzari, M.; Srivastava, N.; Yeung, H.W. Tumor Treatment Response Based on Visual and Quantitative Changes in Global Tumor Glycolysis Using PET-FDG Imaging. The Visual Response Score and the Change in Total Lesion Glycolysis. Clin. Positron Imaging 1999, 2, 159–171. [Google Scholar]
- Obara, P.; Pu, Y. Prognostic value of metabolic tumor burden in lung cancer. Chin. J. Cancer Res. (Chung-Kuo Yen Cheng Yen Chiu) 2013, 25, 615–622. [Google Scholar]
- Weng, E.; Tran, L.; Rege, S.; Safa, A.; Sadeghi, A.; Juillard, G.; Mark, R.; Santiago, S.; Brown, C.; Mandelkern, M. Accuracy and clinical impact of mediastinal lymph node staging with FDG-PET imaging in potentially resectable lung cancer. Am. J. Clin. Oncol. 2000, 23, 47–52. [Google Scholar]
- Changlai, S.P.; Tsai, S.C.; Chou, M.C.; Ho, Y.J.; Kao, C.H. Whole body 18F-2-deoxyglucose positron emission tomography to restage non-small cell lung cancer. Oncol. Rep. 2001, 8, 337–339. [Google Scholar]
- Taus, A.; Aguilo, R.; Curull, V.; Suarez-Pinera, M.; Rodriguez-Fuster, A.; Rodriguez de Dios, N.; Zuccarino, F.; Vollmer, I.; Sánchez-Font, A.; Belda-Sanchis, J.; et al. Impact of 18F-FDG PET/CT in the Treatment of Patients With Non-Small Cell Lung Cancer. Arch. Bronconeumol. 2014, 50, 99–104. [Google Scholar]
- Maziak, D.E.; Darling, G.E.; Inculet, R.I.; Gulenchyn, K.Y.; Driedger, A.A.; Ung, Y.C.; Miller, J.D.; Gu, C.S.; Cline, K.J.; Evans, W.K.; et al. Positron emission tomography in staging early lung cancer: A randomized trial. Ann. Internal Med. 2009, 151, 221–228, W-48. [Google Scholar]
- Fischer, B.; Lassen, U.; Mortensen, J.; Larsen, S.; Loft, A.; Bertelsen, A.; Ravn, J.; Clementsen, P.; Høgholm, A.; Larsen, K.; et al. Preoperative staging of lung cancer with combined PET-CT. N. Engl. J. Med. 2009, 361, 32–39. [Google Scholar]
- Imai, K.; Minamiya, Y.; Saito, H.; Motoyama, S.; Sato, Y.; Ito, A.; Yoshino, K.; Kudo, S.; Takashima, S.; Kawaharada, Y.; et al. Diagnostic imaging in the preoperative management of lung cancer. Surg. Today 2014, 44. [Google Scholar] [CrossRef]
- De Wever, W.; Ceyssens, S.; Mortelmans, L.; Stroobants, S.; Marchal, G.; Bogaert, J.; Verschakelen, J.A. Additional value of PET-CT in the staging of lung cancer: Comparison with CT alone, PET alone and visual correlation of PET and CT. Eur. Radiol. 2007, 17, 23–32. [Google Scholar]
- Chao, F.; Zhang, H. PET/CT in the staging of the non-small-cell lung cancer. J. Biomed. Biotechnol. 2012, 2012, 783739. [Google Scholar]
- Shim, S.S.; Lee, K.S.; Kim, B.T.; Chung, M.J.; Lee, E.J.; Han, J.; Choi, J.Y.; Kwon, O.J.; Shim, Y.M.; Kim, S. Non-small cell lung cancer: Prospective comparison of integrated FDG PET/CT and CT alone for preoperative staging. Radiology 2005, 236, 1011–1019. [Google Scholar]
- Bille, A.; Pelosi, E.; Skanjeti, A.; Arena, V.; Errico, L.; Borasio, P.; Mancini, M.; Ardissone, F. Preoperative intrathoracic lymph node staging in patients with non-small-cell lung cancer: Accuracy of integrated positron emission tomography and computed tomography. Eur. J. Cardio-Thoracic Surg. 2009, 36, 440–445. [Google Scholar]
- Li, S.; Zheng, Q.; Ma, Y.; Wang, Y.; Feng, Y.; Zhao, B.; Yang, Y. Implications of False Negative and False Positive Diagnosis in Lymph Node Staging of NSCLC by Means of (18)F-FDG PET/CT. PLoS One 2013, 8, e78552. [Google Scholar]
- Tandberg, D.J.; Gee, N.G.; Chino, J.P.; D’Amico, T.A.; Ready, N.E.; Coleman, R.E.; Kelsey, C.R. Are discordant positron emission tomography and pathological assessments of the mediastinum in non-small cell lung cancer significant? J. Thoracic Cardiovasc. Surg. 2013, 146, 796–801. [Google Scholar]
- Adams, K.; Shah, P.L.; Edmonds, L.; Lim, E. Test performance of endobronchial ultrasound and transbronchial needle aspiration biopsy for mediastinal staging in patients with lung cancer: Systematic review and meta-analysis. Thorax 2009, 64, 757–762. [Google Scholar]
- Eschmann, S.M.; Friedel, G.; Paulsen, F.; Budach, W.; Harer-Mouline, C.; Dohmen, B.M.; Bares, R. FDG PET for staging of advanced non-small cell lung cancer prior to neoadjuvant radio-chemotherapy. Eur. J. Nucl. Med. Mol. Imaging 2002, 29, 804–808. [Google Scholar]
- Seltzer, M.A.; Yap, C.S.; Silverman, D.H.; Meta, J.; Schiepers, C.; Phelps, M.E.; Gambhir, SS.; Rao, J.; Valk, P.E.; Czernin, J. The impact of PET on the management of lung cancer: The referring physician’s perspective. J. Nucl. Med. 2002, 43, 752–756. [Google Scholar]
- Erasmus, J.J.; Patz, E.F., Jr.; McAdams, H.P.; Murray, J.G.; Herndon, J.; Coleman, R.E.; Goodman, P.C. Evaluation of adrenal masses in patients with bronchogenic carcinoma using 18F-fluorodeoxyglucose positron emission tomography. AJR Am. J. Roentgenol. 1997, 168, 1357–1360. [Google Scholar]
- Stone, W.Z.; Wymer, D.C.; Canales, B.K. Fluorodeoxyglucose-positron-emission tomography/computed tomography imaging for adrenal masses in patients with lung cancer: Review and diagnostic algorithm. J. Endourol. 2014, 28, 104–111. [Google Scholar]
- DiPerna, C.A.; Wood, D.E. Surgical management of T3 and T4 lung cancer. Clin. Cancer Res. 2005, 11, 5038s–5044s. [Google Scholar]
- Tagliabue, L. The emerging role of FDG PET/CT in rectal cancer management: Is it time to use the technique for early prognostication? Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 652–656. [Google Scholar]
- NCCN version 4.2013. Available online: http://www.NCCN.org (accessed on 25 July 2014).
- Kekelidze, M.; D’Errico, L.; Pansini, M.; Tyndall, A.; Hohmann, J. Colorectal cancer: Current imaging methods and future perspectives for the diagnosis, staging and therapeutic response evaluation. World J. Gastroenterol. 2013, 19, 8502–8514. [Google Scholar]
- Bipat, S.; Niekel, M.C.; Comans, E.F.; Nio, C.Y.; Bemelman, W.A.; Verhoef, C.; Stoker, J. Imaging modalities for the staging of patients with colorectal cancer. Neth. J. Med. 2012, 70, 26–34. [Google Scholar]
- Tsunoda, Y.; Ito, M.; Fujii, H.; Kuwano, H.; Saito, N. Preoperative diagnosis of lymph node metastases of colorectal cancer by FDG-PET/CT. Jpn. J. Clin. Oncol. 2008, 38, 347–353. [Google Scholar]
- Niekel, M.C.; Bipat, S.; Stoker, J. Diagnostic imaging of colorectal liver metastases with CT, MR imaging, FDG PET, and/or FDG PET/CT: A meta-analysis of prospective studies including patients who have not previously undergone treatment. Radiology 2010, 257, 674–684. [Google Scholar]
- Bamba, Y.; Itabashi, M.; Kameoka, S. Value of PET/CT imaging for diagnosing pulmonary metastasis of colorectal cancer. Hepatogastroenterology 2011, 58, 1972–1974. [Google Scholar]
- Briggs, R.H.; Chowdhury, F.U.; Lodge, J.P.; Scarsbrook, A.F. Clinical impact of FDG PET-CT in patients with potentially operable metastatic colorectal cancer. Clin. Radiol. 2011, 66, 1167–1174. [Google Scholar]
- Kochhar, R.; Liong, S.; Manoharan, P. The role of FDG PET/CT in patients with colorectal cancer metastases. Cancer Biomarkers 2010, 7, 235–248. [Google Scholar]
- Grassetto, G.; Fornasiero, A.; Bonciarelli, G.; Banti, E.; Rampin, L.; Marzola, M.C.; Massaro, A; Galeotti, F.; del Favero, G.; Pasini, F. Additional value of FDG-PET/CT in management of “solitary” liver metastases: Preliminary results of a prospective multicenter study. Mol. Imaging Biol. 2010, 12, 139–144. [Google Scholar]
- Bonanni, L.; De’liguori Carino, N.; Deshpande, R.; Ammori, B.J.; Sherlock, D.J.; Valle, J.W.; Tam, E.; O’Reilly, D.A. A comparison of diagnostic imaging modalities for colorectal liver metastases. Eur. J. Surg. Oncol. 2014, 40, 545–550. [Google Scholar]
- Brush, J.; Boyd, K.; Chappell, F.; Crawford, F.; Dozier, M.; Fenwick, E.; Glanville, J.; McIntosh, H.; Renehan, A.; Weller, D.; et al. The value of FDG positron emission tomography/computerised tomography (PET/CT) in pre-operative staging of colorectal cancer: A systematic review and economic evaluation. Health Technol. Assess. 2011, 15, 1–192, iii–iv. [Google Scholar]
- Lutz, M.P.; Zalcberg, J.R.; Ducreux, M.; Ajani, J.A.; Allum, W.; Aust, D.; Bang, Y.J.; Cascinu, S.; Hölscher, A.; Jankowski, J.; et al. Highlights of the EORTC St. Gallen International Expert Consensus on the primary therapy of gastric, gastroesophageal and oesophageal cancer—Differential treatment strategies for subtypes of early gastroesophageal cancer. Eur. J. Cancer 2012, 48, 2941–2953. [Google Scholar]
- Tangoku, A.; Yamamoto, Y.; Furukita, Y.; Goto, M.; Morimoto, M. The new era of staging as a key for an appropriate treatment for esophageal cancer. Ann. Thoracic Cardiovasc. Surg. 2012, 18, 190–199. [Google Scholar]
- Karaosmanoglu, A.D.; Blake, M.A. Applications of PET-CT in patients with esophageal cancer. Diagn. Int. Radiol. 2012, 18, 171–182. [Google Scholar]
- Okada, M.; Murakami, T.; Kumano, S.; Kuwabara, M.; Shimono, T.; Hosono, M.; Shiozaki, H. Integrated FDG-PET/CT compared with intravenous contrast-enhanced CT for evaluation of metastatic regional lymph nodes in patients with resectable early stage esophageal cancer. Ann. Nucl. Med. 2009, 23, 73–80. [Google Scholar]
- Vazquez-Sequeiros, E.; Foruny-Olcina, J.R. Linear EUS: The clinical impact of N staging in esophageal carcinoma. Minerva Med. 2007, 98, 313–319. [Google Scholar]
- Shi, W.; Wang, W.; Wang, J.; Cheng, H.; Huo, X. Meta-analysis of 18FDG PET-CT for nodal staging in patients with esophageal cancer. Surg. Oncol. 2013, 22, 112–116. [Google Scholar]
- Manabe, O.; Hattori, N.; Hirata, K.; Itoh, K.; Hosokawa, M.; Takahashi, H.; Oyama-Manabe, N.; Tamaki, N. Diagnostic accuracy of lymph node metastasis depends on metabolic activity of the primary lesion in thoracic squamous esophageal cancer. J. Nucl. Med. 2013, 54, 670–676. [Google Scholar]
- Van Vliet, E.P.; Heijenbrok-Kal, M.H.; Hunink, M.G.; Kuipers, E.J.; Siersema, P.D. Staging investigations for oesophageal cancer: A meta-analysis. Br. J. Cancer 2008, 98, 547–557. [Google Scholar]
- Hsu, P.K.; Lin, K.H.; Wang, S.J.; Huang, C.S.; Wu, Y.C.; Hsu, W.H. Preoperative positron emission tomography/computed tomography predicts advanced lymph node metastasis in esophageal squamous cell carcinoma patients. World J. Surg. 2011, 35, 1321–1326. [Google Scholar]
- Barber, T.W.; Duong, C.P.; Leong, T.; Bressel, M.; Drummond, E.G.; Hicks, R.J. 18F-FDG PET/CT has a high impact on patient management and provides powerful prognostic stratification in the primary staging of esophageal cancer: A prospective study with mature survival data. J. Nucl. Med. 2012, 53, 864–871. [Google Scholar]
- Sun, G.; Tian, J.; Gorospe, E.C.; Johnson, G.B.; Hunt, C.H.; Lutzke, L.S.; Leggett, C.L.; Iyer, P.G.; Wang, K.K. Utility of baseline positron emission tomography with computed tomography for predicting endoscopic resectability and survival outcomes in patients with early esophageal adenocarcinoma. J. Gastroenterol. Hepatol. 2013, 28, 975–981. [Google Scholar]
- Chan, D.S.; Fielding, P.; Roberts, S.A.; Reid, T.D.; Ellis-Owen, R.; Lewis, W.G. Prognostic significance of 18-FDG PET/CT and EUS-defined tumour characteristics in patients with oesophageal cancer. Clin. Radiol. 2013, 68, 352–357. [Google Scholar]
- Shum, W.Y.; Ding, H.J.; Liang, J.A.; Yen, K.Y.; Chen, S.W.; Kao, C.H. Use of pretreatment metabolic tumor volumes on PET-CT to predict the survival of patients with squamous cell carcinoma of esophagus treated by curative surgery. Anticancer Res. 2012, 32, 4163–4168. [Google Scholar]
- Sehdev, A.; Catenacci, D.V. Gastroesophageal cancer: Focus on epidemiology, classification, and staging. Discov. Med. 2013, 16, 103–111. [Google Scholar]
- Stahl, A.; Ott, K.; Weber, W.A.; Becker, K.; Link, T.; Siewert, J.R.; Schwaiger, M.; Fink, U. FDG PET imaging of locally advanced gastric carcinomas: Correlation with endoscopic and histopathological findings. Eur. J. Nucl. Med. Mol. Imaging 2003, 30, 288–295. [Google Scholar]
- Nath, J.; Moorthy, K.; Taniere, P.; Hallissey, M.; Alderson, D. Peritoneal lavage cytology in patients with oesophagogastric adenocarcinoma. Br. J. Surg. 2008, 95, 721–726. [Google Scholar]
- Dibble, E.H.; Karantanis, D.; Mercier, G.; Peller, P.J.; Kachnic, L.A.; Subramaniam, R.M. PET/CT of cancer patients: Part 1, pancreatic neoplasms. AJR Am. J. Roentgenol. 2012, 199, 952–967. [Google Scholar]
- Wang, Z.; Chen, J.Q.; Liu, J.L.; Qin, X.G.; Huang, Y. FDG-PET in diagnosis, staging and prognosis of pancreatic carcinoma: A meta-analysis. World J. Gastroenterol. 2013, 19, 4808–4817. [Google Scholar]
- Hu, S.L.; Yang, Z.Y.; Zhou, Z.R.; Yu, X.J.; Ping, B.; Zhang, Y.J. Role of SUV(max) obtained by 18F-FDG PET/CT in patients with a solitary pancreatic lesion: Predicting malignant potential and proliferation. Nucl. Med. Commun. 2013, 34, 533–539. [Google Scholar]
- Choi, H.J.; Kang, C.M.; Lee, W.J.; Song, S.Y.; Cho, A.; Yun, M.; Lee, J.D.; Kim, J.H.; Lee, J.H. Prognostic value of 18F-fluorodeoxyglucose positron emission tomography in patients with resectable pancreatic cancer. Yonsei Med. J. 2013, 54, 1377–1383. [Google Scholar]
- Moon, S.Y.; Joo, K.R.; So, Y.R.; Lim, J.U.; Cha, J.M.; Shin, H.P.; Yang, Y.J. Predictive value of maximum standardized uptake value (SUVmax) on 18F-FDG PET/CT in patients with locally advanced or metastatic pancreatic cancer. Clin. Nucl. Med. 2013, 38, 778–783. [Google Scholar]
- Xu, H.X.; Chen, T.; Wang, W.Q.; Wu, C.T.; Liu, C.; Long, J.; Xu, J.; Zhang, Y.J.; Chen, R.H.; Liu, L.; et al. Metabolic tumour burden assessed by F-FDG PET/CT associated with serum CA19-9 predicts pancreatic cancer outcome after resection. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1093–1102. [Google Scholar]
- Kim, Y.I.; Kim, S.K.; Paeng, J.C.; Lee, H.Y. Comparison of F-18-FDG PET/CT findings between pancreatic solid pseudopapillary tumor and pancreatic ductal adenocarcinoma. Eur. J. Radiol. 2014, 83, 231–235. [Google Scholar]
- Kato, K.; Nihashi, T.; Ikeda, M.; Abe, S.; Iwano, S.; Itoh, S.; Shimamoto, K.; Naganawa, S. Limited efficacy of (18)F-FDG PET/CT for differentiation between metastasis-free pancreatic cancer and mass-forming pancreatitis. Clin. Nucl. Med. 2013, 38, 417–421. [Google Scholar]
- Matsumoto, I.; Shirakawa, S.; Shinzeki, M.; Asari, S.; Goto, T.; Ajiki, T.; Fukumoto, T.; Kitajima, K.; Ku, Y. 18-Fluorodeoxyglucose positron emission tomography does not aid in diagnosis of pancreatic ductal adenocarcinoma. Clin. Gastroenterol. Hepatol. 2013, 11, 712–718. [Google Scholar]
- Nagamachi, S.; Nishii, R.; Wakamatsu, H.; Mizutani, Y.; Kiyohara, S.; Fujita, S.; Futami, S.; Sakae, T.; Furukoji, E.; Tamura, S. The usefulness of (18)F-FDG PET/MRI fusion image in diagnosing pancreatic tumor: Comparison with (18)F-FDG PET/CT. Ann. Nucl. Med. 2013, 27, 554–563. [Google Scholar]
- Baiocchi, G.L.; Bertagna, F.; Gheza, F.; Grazioli, L.; Calanducci, D.; Giubbini, R.; Giubbini, R.; Portolani, N.; Giulini, S.M. Searching for indicators of malignancy in pancreatic intraductal papillary mucinous neoplasms: The value of 18FDG-PET confirmed. Ann. Surg. Oncol. 2012, 19, 3574–3580. [Google Scholar]
- Bertagna, F.; Treglia, G.; Baiocchi, G.L.; Giubbini, R. F18-FDG-PET/CT for evaluation of intraductal papillary mucinous neoplasms (IPMN): A review of the literature. Jpn. J. Radiol. 2013, 31, 229–236. [Google Scholar]
- Javery, O.; Shyn, P.; Mortele, K. FDG PET or PET/CT in patients with pancreatic cancer: When does it add to diagnostic CT or MRI? Clin. Imaging 2013, 37, 295–301. [Google Scholar]
- Topkan, E.; Parlak, C.; Yapar, A.F. FDG-PET/CT-based restaging may alter initial management decisions and clinical outcomes in patients with locally advanced pancreatic carcinoma planned to undergo chemoradiotherapy. Cancer Imaging 2013, 13, 423–428. [Google Scholar]
- Pauwels, E.K.; Coumou, A.W.; Kostkiewicz, M.; Kairemo, K. [18F]fluoro-2-deoxy-d-glucose positron emission tomography/computed tomography imaging in oncology: Initial staging and evaluation of cancer therapy. Med. Princ. Pract. 2013, 22, 427–437. [Google Scholar]
- Haerle, S.K.; Strobel, K.; Ahmad, N.; Soltermann, A.; Schmid, D.T.; Stoeckli, S.J. Contrast-enhanced 18F-FDG-PET/CT for the assessment of necrotic lymph node metastases. Head Neck 2011, 33, 324–329. [Google Scholar]
- Carlson, E.R.; Schaefferkoetter, J.; Townsend, D.; McCoy, J.M.; Campbell, P.D., Jr.; Long, M. The use of multiple time point dynamic positron emission tomography/computed tomography in patients with oral/head and neck cancer does not predictably identify metastatic cervical lymph nodes. J. Oral Maxillofac. Surg. 2013, 71, 162–177. [Google Scholar]
- Connell, C.A.; Corry, J.; Milner, A.D.; Hogg, A.; Hicks, R.J.; Rischin, D.; Peters, L.J. Clinical impact of, and prognostic stratification by, F-18 FDG PET/CT in head and neck mucosal squamous cell carcinoma. Head Neck 2007, 29, 986–995. [Google Scholar]
- Roh, J.L.; Yeo, N.K.; Kim, J.S.; Lee, J.H.; Cho, K.J.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. Utility of 2-[18F] fluoro-2-deoxy-D-glucose positron emission tomography and positron emission tomography/computed tomography imaging in the preoperative staging of head and neck squamous cell carcinoma. Oral Oncol. 2007, 43, 887–893. [Google Scholar]
- Gao, S.; Li, S.; Yang, X.; Tang, Q. FDG PET-CT for distant metastases in patients with recurrent head and neck cancer after definitive treatment. A meta-analysis. Oral Oncol. 2013, 50, 163–167. [Google Scholar]
- Xu, G.Z.; Guan, D.J.; He, Z.Y. (18)FDG-PET/CT for detecting distant metastases and second primary cancers in patients with head and neck cancer. A meta-analysis. Oral Oncol. 2011, 47, 560–565. [Google Scholar]
- Bourgeois, A.C.; Warren, L.A.; Chang, T.T.; Embry, S.; Hudson, K.; Bradley, Y.C. Role of positron emission tomography/computed tomography in breast cancer. Radiol. Clin. N. Am. 2013, 51, 781–798. [Google Scholar]
- Garami, Z.; Hascsi, Z.; Varga, J.; Dinya, T.; Tanyi, M.; Garai, I.; Damjanovich, L.; Galuska, L. The value of 18-FDG PET/CT in early-stage breast cancer compared to traditional diagnostic modalities with an emphasis on changes in disease stage designation and treatment plan. Eur. J. Surg. Oncol. 2012, 38, 31–37. [Google Scholar]
- Bernsdorf, M.; Berthelsen, A.K.; Wielenga, V.T.; Kroman, N.; Teilum, D.; Binderup, T.; Tange, U.B.; Andersson, M.; Kjær, A.; Loft, A.; et al. Preoperative PET/CT in early-stage breast cancer. Ann. Oncol. 2012, 23, 2277–2282. [Google Scholar]
- Adejolu, M.; Huo, L.; Rohren, E.; Santiago, L.; Yang, W.T. False-positive lesions mimicking breast cancer on FDG PET and PET/CT. AJR Am. J. Roentgenol. 2012, 198, W304–W314. [Google Scholar]
- Koolen, B.B.; Vrancken Peeters, M.J.; Wesseling, J.; Lips, E.H.; Vogel, W.V.; Aukema, T.S.; van Werkhoven, E.; Gilhuijs, K.G.; Rodenhuis, S.; Rutgers, E.J.; et al. Association of primary tumour FDG uptake with clinical, histopathological and molecular characteristics in breast cancer patients scheduled for neoadjuvant chemotherapy. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 1830–1838. [Google Scholar]
- Groheux, D.; Giacchetti, S.; Moretti, J.L.; Porcher, R.; Espie, M.; Lehmann-Che, J.; de Roquancourt, A.; Hamy, A.S.; Cuvier, C.; Vercellino, L.; et al. Correlation of high 18F-FDG uptake to clinical, pathological and biological prognostic factors in breast cancer. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 426–435. [Google Scholar]
- Lyman, G.H.; Giuliano, A.E.; Somerfield, M.R.; Benson, A.B., 3rd; Bodurka, D.C.; Burstein, H.J.; Cochran, A.J.; Cody, H.S., 3rd; Edge, S.B.; Galper, S.; et al. American Society of Clinical Oncology guideline recommendations for sentinel lymph node biopsy in early-stage breast cancer. J. Clin. Oncol. 2005, 23, 7703–7720. [Google Scholar]
- Cooper, K.L.; Meng, Y.; Harnan, S.; Ward, S.E.; Fitzgerald, P.; Papaioannou, D.; Wyld, L.; Ingram, C.; Wilkinson, I.D.; Lorenz, E. Positron emission tomography (PET) and magnetic resonance imaging (MRI) for the assessment of axillary lymph node metastases in early breast cancer: Systematic review and economic evaluation. Health Technol. Assess. 2011, 15, iii–iv. 1–134. [Google Scholar]
- Koolen, B.B.; Valdes Olmos, R.A.; Elkhuizen, P.H.; Vogel, W.V.; Vrancken Peeters, M.J.; Rodenhuis, S.; Rutgers, E.J. Locoregional lymph node involvement on 18F-FDG PET/CT in breast cancer patients scheduled for neoadjuvant chemotherapy. Breast Cancer Res. Treat. 2012, 135, 231–240. [Google Scholar]
- Koolen, B.B.; Vogel, W.V.; Vrancken Peeters, M.J.; Loo, C.E.; Rutgers, E.J.; Valdes Olmos, R.A. Molecular Imaging in Breast Cancer: From Whole-Body PET/CT to Dedicated Breast PET. J. Oncol. 2012, 2012, 438647. [Google Scholar]
- Peare, R.; Staff, R.T.; Heys, S.D. The use of FDG-PET in assessing axillary lymph node status in breast cancer: A systematic review and meta-analysis of the literature. Breast Cancer Res. Treat. 2010, 123, 281–290. [Google Scholar]
- Riegger, C.; Herrmann, J.; Nagarajah, J.; Hecktor, J.; Kuemmel, S.; Otterbach, F.; Hahn, S.; Bockisch, A.; Lauenstein, T.; Antoch, G.; et al. Whole-body FDG PET/CT is more accurate than conventional imaging for staging primary breast cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 852–863. [Google Scholar]
- Piccardo, A.; Altrinetti, V.; Bacigalupo, L.; Puntoni, M.; Biscaldi, E.; Gozza, A.; Cabria, M.; Iacozzi, M.; Pasa, A.; Morbelli, S.; et al. Detection of metastatic bone lesions in breast cancer patients: Fused (18)F-Fluoride-PET/MDCT has higher accuracy than MDCT. Preliminary experience. Eur. J. Radiol. 2012, 81, 2632–2638. [Google Scholar]
- Hahn, S.; Heusner, T.; Kummel, S.; Koninger, A.; Nagarajah, J.; Muller, S.; Boy, C.; Forsting, M.; Bockisch, A.; Antoch, G.; et al. Comparison of FDG-PET/CT and bone scintigraphy for detection of bone metastases in breast cancer. Acta Radiol. 2011, 52, 1009–1014. [Google Scholar]
- Berland, L.L.; Silverman, S.G.; Gore, R.M.; Mayo-Smith, W.W.; Megibow, A.J.; Yee, J.; Brink, J.A.; Baker, M.E.; Federle, M.P.; Foley, W.D.; et al. Managing incidental findings on abdominal CT: White paper of the ACR incidental findings committee. J. Am. Coll. Radiol. 2010, 7, 754–773. [Google Scholar]
- Tatsumi, M.; Cohade, C.; Mourtzikos, K.A.; Fishman, E.K.; Wahl, R.L. Initial experience with FDG-PET/CT in the evaluation of breast cancer. Eur. J. Nucl. Med. Mol. Imaging 2006, 33, 254–262. [Google Scholar]
- Havrilesky, L.J.; Kulasingam, S.L.; Matchar, D.B.; Myers, E.R. FDG-PET for management of cervical and ovarian cancer. Gynecol. Oncol. 2005, 97, 183–191. [Google Scholar]
- Zimny, M.; Siggelkow, W. Positron emission tomography scanning in gynecologic and breast cancers. Curr. Opin. Obst. Gynecol. 2003, 15, 69–75. [Google Scholar]
- Zimny, M.; Siggelkow, W.; Schroder, W.; Nowak, B.; Biemann, S.; Rath, W.; Buell, U. 2-[Fluorine-18]-fluoro-2-deoxy-d-glucose positron emission tomography in the diagnosis of recurrent ovarian cancer. Gynecol. Oncol. 2001, 83, 310–315. [Google Scholar]
- Menzel, C.; Dobert, N.; Hamscho, N.; Zaplatnikov, K.; Vasvatekis, S.; Matic, V.; Wördehoff, N.; Grünwald, F. The influence of CA 125 and CEA levels on the results of (18)F-deoxyglucose positron emission tomography in suspected recurrence of epithelial ovarian cancer. Strahlenther. Onkol. 2004, 180, 497–501. [Google Scholar]
- Fulham, M.J.; Carter, J.; Baldey, A.; Hicks, R.J.; Ramshaw, J.E.; Gibson, M. The impact of PET-CT in suspected recurrent ovarian cancer: A prospective multi-centre study as part of the Australian PET Data Collection Project. Gynecol. Oncol. 2009, 112, 462–468. [Google Scholar]
- Rieber, A.; Nussle, K.; Stohr, I.; Grab, D.; Fenchel, S.; Kreienberg, R.; Reske, S.N.; Brambs, H.J. Preoperative diagnosis of ovarian tumors with MR imaging: Comparison with transvaginal sonography, positron emission tomography, and histologic findings. AJR Am. J. Roentgenol. 2001, 177, 123–129. [Google Scholar]
- Hynninen, J.; Auranen, A.; Carpen, O.; Dean, K.; Seppanen, M.; Kemppainen, J.; Lavonius, M.; Lisinen, I.; Virtanen, J.; Grénman, S. FDG PET/CT in staging of advanced epithelial ovarian cancer: Frequency of supradiaphragmatic lymph node metastasis challenges the traditional pattern of disease spread. Gynecol. Oncol. 2012, 126, 64–68. [Google Scholar]
- Bats, A.S.; Hugonnet, F.; Huchon, C.; Bensaid, C.; Pierquet-Ghazzar, N.; Faraggi, M.; Lécuru, L. Prognostic significance of mediastinal 18F-FDG uptake in PET/CT in advanced ovarian cancer. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 474–480. [Google Scholar]
- Yoshida, Y.; Kurokawa, T.; Kawahara, K.; Tsuchida, T.; Okazawa, H.; Fujibayashi, Y.; Yonekura, Y.; Kotsuji, F. Incremental benefits of FDG positron emission tomography over CT alone for the preoperative staging of ovarian cancer. AJR Am. J. Roentgenol. 2004, 182, 227–233. [Google Scholar]
- Castellucci, P.; Perrone, A.M.; Picchio, M.; Ghi, T.; Farsad, M.; Nanni, C.; Messa, C.; Meriggiola, M.C.; Pelusi, G.; Al-Nahhas, A.; et al. Diagnostic accuracy of 18F-FDG PET/CT in characterizing ovarian lesions and staging ovarian cancer: Correlation with transvaginal ultrasonography, computed tomography, and histology. Nucl. Med. Commun. 2007, 28, 589–595. [Google Scholar]
- De Iaco, P.; Musto, A.; Orazi, L.; Zamagni, C.; Rosati, M.; Allegri, V.; Cacciari, N.; Al-Nahhas, A.; Rubello, D.; Venturoli, S.; et al. FDG-PET/CT in advanced ovarian cancer staging: Value and pitfalls in detecting lesions in different abdominal and pelvic quadrants compared with laparoscopy. Eur. J. Radiol. 2011, 80, e98–e103. [Google Scholar]
- Turlakow, A.; Yeung, H.W.; Salmon, A.S.; Macapinlac, H.A.; Larson, S.M. Peritoneal carcinomatosis: Role of (18)F-FDG PET. J. Nucl. Med. 2003, 44, 1407–1412. [Google Scholar]
- Kim, H.W.; Won, K.S.; Zeon, S.K.; Ahn, B.C.; Gayed, I.W. Peritoneal carcinomatosis in patients with ovarian cancer: Enhanced CT versus 18F-FDG PET/CT. Clin. Nucl. Med. 2013, 38, 93–97. [Google Scholar]
- Suzuki, A.; Kawano, T.; Takahashi, N.; Lee, J.; Nakagami, Y.; Miyagi, E.; Hirahara, F.; Togo, S.; Shimada, H.; Inoue, T. Value of 18F-FDG PET in the detection of peritoneal carcinomatosis. Eur. J. Nucl. Med. Mol. Imaging 2004, 31, 1413–1420. [Google Scholar]
- Sanli, Y.; Turkmen, C.; Bakir, B.; Iyibozkurt, C.; Ozel, S.; Has, D.; Yilmaz, E.; Topuz, S.; Yavuz, E.; Unal, S.N.; et al. Diagnostic value of PET/CT is similar to that of conventional MRI and even better for detecting small peritoneal implants in patients with recurrent ovarian cancer. Nucl. Med. Commun. 2012, 33, 509–515. [Google Scholar]
- Drieskens, O.; Stroobants, S.; Gysen, M.; Vandenbosch, G.; Mortelmans, L.; Vergote, I. Positron emission tomography with FDG in the detection of peritoneal and retroperitoneal metastases of ovarian cancer. Gynecol. Obst. Investig. 2003, 55, 130–134. [Google Scholar]
- Ebina, Y.; Watari, H.; Kaneuchi, M.; Takeda, M.; Hosaka, M.; Kudo, M.; Yamada, H.; Sakuragi, N. Impact of FDG PET in optimizing patient selection for cytoreductive surgery in recurrent ovarian cancer. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 446–451. [Google Scholar]
- Fruscio, R.; Sina, F.; Dolci, C.; Signorelli, M.; Crivellaro, C.; Dell’Anna, T.; Cuzzocrea, M.; Guerra, L.; Milani, R.; Messa, C. Preoperative 18F-FDG PET/CT in the management of advanced epithelial ovarian cancer. Gynecol. Oncol. 2013, 131, 689–693. [Google Scholar]
- Risum, S.; Loft, A.; Engelholm, S.A.; Hogdall, E.; Berthelsen, A.K.; Nedergaard, L.; Lundvall, L.; Høgdall, C. Positron emission tomography/computed tomography predictors of overall survival in stage IIIC/IV ovarian cancer. Int. J. Gynecol. Cancer 2012, 22, 1163–1169. [Google Scholar]
- Chung, H.H.; Kwon, H.W.; Kang, K.W.; Park, N.H.; Song, Y.S.; Chung, J.K.; Kang, S.B.; Kim, J.W. Prognostic value of preoperative metabolic tumor volume and total lesion glycolysis in patients with epithelial ovarian cancer. Ann. Surg. Oncol. 2012, 19, 1966–1972. [Google Scholar]
- Patel, C.N.; Nazir, S.A.; Khan, Z.; Gleeson, F.V.; Bradley, K.M. 18F-FDG PET/CT of cervical carcinoma. AJR Am. J. Roentgenol. 2011, 196, 1225–1233. [Google Scholar]
- Chung, H.H.; Cheon, G.J.; Kang, K.W.; Kim, J.W.; Park, N.H.; Song, Y.S. Preoperative PET/CT FDG standardized uptake value of pelvic lymph nodes as a significant prognostic factor in patients with uterine cervical cancer. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 674–681. [Google Scholar]
- Kidd, E.A.; Siegel, B.A.; Dehdashti, F.; Grigsby, P.W. Pelvic lymph node F-18 fluorodeoxyglucose uptake as a prognostic biomarker in newly diagnosed patients with locally advanced cervical cancer. Cancer 2010, 116, 1469–1475. [Google Scholar]
- Wright, J.D.; Dehdashti, F.; Herzog, T.J.; Mutch, D.G.; Huettner, P.C.; Rader, J.S.; Gibb, R.K.; Powell, M.A.; Gao, F.; Siegel, B.A.; et al. Preoperative lymph node staging of early-stage cervical carcinoma by [18F]-fluoro-2-deoxy-d-glucose-positron emission tomography. Cancer 2005, 104, 2484–2491. [Google Scholar]
- Sironi, S.; Buda, A.; Picchio, M.; Perego, P.; Moreni, R.; Pellegrino, A.; Colombo, M.; Mangioni, C.; Messa, C.; Fazio, F. Lymph node metastasis in patients with clinical early-stage cervical cancer: Detection with integrated FDG PET/CT. Radiology 2006, 238, 272–279. [Google Scholar]
- Herrera, F.G.; Prior, J.O. The role of PET/CT in cervical cancer. Front. Oncol. 2013, 3, 34. [Google Scholar]
- Gouy, S.; Morice, P.; Narducci, F.; Uzan, C.; Gilmore, J.; Kolesnikov-Gauthier, H.; Querleu, D.; Haie-Meder, C.; Leblanc, E. Nodal-staging surgery for locally advanced cervical cancer in the era of PET. Lancet Oncol. 2012, 13, e212–e220. [Google Scholar]
- Choi, H.J.; Roh, J.W.; Seo, S.S.; Lee, S.; Kim, J.Y.; Kim, S.K.; Kang, K.W.; Lee, J.S.; Jeong, J.Y.; Park, S.Y. Comparison of the accuracy of magnetic resonance imaging and positron emission tomography/computed tomography in the presurgical detection of lymph node metastases in patients with uterine cervical carcinoma: A prospective study. Cancer 2006, 106, 914–922. [Google Scholar]
- Kitajima, K.; Yamasaki, E.; Kaji, Y.; Murakami, K.; Sugimura, K. Comparison of DWI and PET/CT in evaluation of lymph node metastasis in uterine cancer. World J. Radiol. 2012, 4, 207–214. [Google Scholar]
- Im, H.J.; Yoon, H.J.; Lee, E.S.; Kim, T.S.; Kim, J.Y.; Chung, J.K.; Park, S.Y. Prognostic implication of retrocrural lymph node involvement revealed by (18)F-FDG PET/CT in patients with uterine cervical cancer. Nucl. Med. Commun. 2014, 35, 268–275. [Google Scholar]
- Zhao, Q.; Feng, Y.; Mao, X.; Qie, M. Prognostic value of fluorine-18-fluorodeoxyglucose positron emission tomography or PET-computed tomography in cervical cancer: A meta-analysis. Int. J. Gynecol. Cancer 2013, 23, 1184–1190. [Google Scholar]
- Gouy, S.; Morice, P.; Narducci, F.; Uzan, C.; Martinez, A.; Rey, A.; Bentivegna, E.; Pautier, P.; Deandreis, D.; Querleu, D.; et al. Prospective multicenter study evaluating the survival of patients with locally advanced cervical cancer undergoing laparoscopic para-aortic lymphadenectomy before chemoradiotherapy in the era of positron emission tomography imaging. J. Clin. Oncol. 2013, 31, 3026–3033. [Google Scholar]
- Margulies, A.L.; Peres, A.; Barranger, E.; Perreti, I.; Brouland, J.F.; Toubet, E.; Sarda-Mantel, L.E.; Thoury, A.; Chis, C.; Walker, F.; et al. Selection of patients with advanced-stage cervical cancer for para-aortic lymphadenectomy in the era of PET/CT. Anticancer Res. 2013, 33, 283–286. [Google Scholar]
- Liu, F.Y.; Yen, T.C.; Chen, M.Y.; Lai, C.H.; Chang, T.C.; Chou, H.H.; Hong, J.H.; Chen, Y.R.; Ng, K.K. Detection of hematogenous bone metastasis in cervical cancer: 18F-fluorodeoxyglucose-positron emission tomography versus computed tomography and magnetic resonance imaging. Cancer 2009, 115, 5470–5480. [Google Scholar]
- Akkas, B.E.; Demirel, B.B.; Vural, G.U. Clinical impact of 18F-FDG PET/CT in the pretreatment evaluation of patients with locally advanced cervical carcinoma. Nucl. Med. Commun. 2012, 33, 1081–1088. [Google Scholar]
- Keu, K.V.; Iagaru, A.H. The clinical use of PET/CT in the evaluation of melanoma. Methods Mol. Biol. 2014, 1102, 553–580. [Google Scholar]
- Danielsen, M.; Hojgaard, L.; Kjaer, A.; Fischer, B.M. Positron emission tomography in the follow-up of cutaneous malignant melanoma patients: A systematic review. Am. J. Nucl. Med. Mol. Imaging 2013, 4, 17–28. [Google Scholar]
- Eigtved, A.; Andersson, A.P.; Dahlstrom, K.; Rabol, A.; Jensen, M.; Holm, S.; Sørensen, S.S.; Drzewiecki, K.T.; Højgaard, L.; Friberg, L. Use of fluorine-18 fluorodeoxyglucose positron emission tomography in the detection of silent metastases from malignant melanoma. Eur. J. Nucl. Med. 2000, 27, 70–75. [Google Scholar]
- Rinne, D.; Baum, R.P.; Hor, G.; Kaufmann, R. Primary staging and follow-up of high risk melanoma patients with whole-body 18F-fluorodeoxyglucose positron emission tomography: Results of a prospective study of 100 patients. Cancer 1998, 82, 1664–1671. [Google Scholar]
- Holder, W.D., Jr.; White, R.L., Jr.; Zuger, J.H.; Easton, E.J., Jr.; Greene, F.L. Effectiveness of positron emission tomography for the detection of melanoma metastases. Ann. Surg. 1998, 227, 764–771. [Google Scholar]
- Kwee, T.C.; Kwee, R.M.; Nievelstein, R.A. Imaging in staging of malignant lymphoma: A systematic review. Blood 2008, 111, 504–516. [Google Scholar]
- Munker, R.; Glass, J.; Griffeth, L.K.; Sattar, T.; Zamani, R.; Heldmann, M.; Shi, R.; Lilien, D.L. Contribution of PET imaging to the initial staging and prognosis of patients with Hodgkin’s disease. Ann. Oncol. 2004, 15, 1699–1704. [Google Scholar]
- Rigacci, L.; Vitolo, U.; Nassi, L.; Merli, F.; Gallamini, A.; Pregno, P.; Alvarez, I.; Salvi, F.; Sancetta, R.; Castagnoli, A.; et al. Positron emission tomography in the staging of patients with Hodgkin’s lymphoma. A prospective multicentric study by the Intergruppo Italiano Linfomi. Ann. Hematol. 2007, 86, 897–903. [Google Scholar]
- Hutchings, M.; Loft, A.; Hansen, M.; Pedersen, L.M.; Berthelsen, A.K.; Keiding, S.; D'Amore, F.; Boesen, A.M.; Roemer, L.; Specht, L. Position emission tomography with or without computed tomography in the primary staging of Hodgkin’s lymphoma. Haematologica 2006, 91, 482–489. [Google Scholar]
- Cheson, B.D. Role of functional imaging in the management of lymphoma. J. Clin. Oncol. 2011, 29, 1844–1854. [Google Scholar]
- Rodriguez-Vigil, B.; Gomez-Leon, N.; Pinilla, I.; Hernandez-Maraver, D.; Coya, J.; Martin-Curto, L.; Madero, R. PET/CT in lymphoma: Prospective study of enhanced full-dose PET/CT versus unenhanced low-dose PET/CT. J. Nucl. Med. 2006, 47, 1643–1648. [Google Scholar]
- Chalaye, J.; Luciani, A.; Enache, C.; Beaussart, P.; Lhermite, C.; Evangelista, E.; Sasanelli, M.; Safar, V.; Meignan, M.; Haioun, C.; et al. Clinical impact of contrast-enhanced CT combined with low-dose F-FDG PET/CT on routine lymphoma patient management. Leuk. Lymphoma 2014. [Google Scholar] [CrossRef]
- Pinilla, I.; Gomez-Leon, N.; del Campo-Del Val, L.; Hernandez-Maraver, D.; Rodriguez-Vigil, B.; Jover-Diaz, R.; Coya, J. Diagnostic value of CT, PET and combined PET/CT performed with low-dose unenhanced CT and full-dose enhanced CT in the initial staging of lymphoma. Q. J. Nucl. Med. Mol. Imaging 2011, 55, 567–575. [Google Scholar]
- Elstrom, R.L.; Leonard, J.P.; Coleman, M.; Brown, R.K. Combined PET and low-dose, noncontrast CT scanning obviates the need for additional diagnostic contrast-enhanced CT scans in patients undergoing staging or restaging for lymphoma. Ann. Oncol. 2008, 19, 1770–1773. [Google Scholar]
- El-Galaly, T.C.; d’Amore, F.; Mylam, K.J.; de Nully Brown, P.; Bogsted, M.; Bukh, A.; Specht, L.; Loft, A.; Iyer, V.; Hjorthaug, K.; et al. Routine bone marrow biopsy has little or no therapeutic consequence for positron emission tomography/computed tomography-staged treatment-naive patients with Hodgkin lymphoma. J. Clin. Oncol. 2012, 30, 4508–4514. [Google Scholar]
- Khan, A.B.; Barrington, S.F.; Mikhaeel, N.G.; Hunt, A.A.; Cameron, L.; Morris, T.; Carr, R. PET-CT staging of DLBCL accurately identifies and provides new insight into the clinical significance of bone marrow involvement. Blood 2013, 122, 61–67. [Google Scholar]
- Avigdor, A. Staging DLBCL: Bone marrow biopsy or PET-CT? Blood 2013, 122, 4–5. [Google Scholar]
- Le Dortz, L.; de Guibert, S.; Bayat, S.; Devillers, A.; Houot, R.; Rolland, Y.; Cuggia, M.; Le Jeune, F.; Bahri, H.; Barge, M.L.; et al. Diagnostic and prognostic impact of 18F-FDG PET/CT in follicular lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 2307–2314. [Google Scholar]
- Luminari, S.; Biasoli, I.; Arcaini, L.; Versari, A.; Rusconi, C.; Merli, F.; Spina, M.; Ferreri, A.J.; Zinzani, P.L.; Gallamini, A.; et al. The use of FDG-PET in the initial staging of 142 patients with follicular lymphoma: A retrospective study from the FOLL05 randomized trial of the Fondazione Italiana Linfomi. Ann. Oncol. 2013, 24, 2108–2112. [Google Scholar]
- Bodet-Milin, C.; Touzeau, C.; Leux, C.; Sahin, M.; Moreau, A.; Maisonneuve, H.; Morineau, N.; Jardel, H.; Moreau, P.; Gallazini-Crépin, C.; et al. Prognostic impact of 18F-fluoro-deoxyglucose positron emission tomography in untreated mantle cell lymphoma: A retrospective study from the GOELAMS group. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 1633–1642. [Google Scholar]
- Karam, M.; Ata, A.; Irish, K.; Feustel, P.J.; Mottaghy, F.M.; Stroobants, S.G.; Verhoef, G.E.; Chundru, S.; Douglas-Nikitin, V.; Oliver Wong, C.Y.; et al. FDG positron emission tomography/computed tomography scan may identify mantle cell lymphoma patients with unusually favorable outcome. Nucl. Med. Commun. 2009, 30, 770–778. [Google Scholar]
- Barrington, S.F.; Mikhaeel, N.G.; Kostakoglu, L.; Meignan, M.; Hutchings, M.; MÜeller, S.P.; Lawrence, H.S.; Zucca, E.; Fisher, R.I.; Trotman, J.; et al. Role of Imaging in the Staging and Response Assessment of Lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group. J. Clin. Oncol. 2014. [Google Scholar] [CrossRef]
- Sim, Y.T.; Poon, F.W. Imaging of solitary pulmonary nodule-a clinical review. Quant. Imaging Med. Surg. 2013, 3, 316–326. [Google Scholar]
- Erasmus, J.J.; McAdams, H.P.; Connolly, J.E. Solitary pulmonary nodules: Part II. Evaluation of the indeterminate nodule. Radiographics 2000, 20, 59–66. [Google Scholar]
- Gurney, J.W.; Lyddon, D.M.; McKay, J.A. Determining the likelihood of malignancy in solitary pulmonary nodules with Bayesian analysis. Part II. Application. Radiology 1993, 186, 415–422. [Google Scholar]
- Bryant, A.S.; Cerfolio, R.J. The maximum standardized uptake values on integrated FDG-PET/CT is useful in differentiating benign from malignant pulmonary nodules. Ann. Thoracic Surg. 2006, 82, 1016–1020. [Google Scholar]
- Lowe, V.J.; Fletcher, J.W.; Gobar, L.; Lawson, M.; Kirchner, P.; Valk, P.; Karis, J.; Hubner, K.; Delbeke, D.; Heiberg, E.V.; et al. Prospective investigation of positron emission tomography in lung nodules. J. Clin. Oncol. 1998, 16, 1075–1084. [Google Scholar]
- Hashimoto, Y.; Tsujikawa, T.; Kondo, C.; Maki, M.; Momose, M.; Nagai, A.; Ohnuki, T.; Nishikawa, T.; Kusakabe, K. Accuracy of PET for diagnosis of solid pulmonary lesions with 18F-FDG uptake below the standardized uptake value of 2.5. J. Nucl. Med. 2006, 47, 426–431. [Google Scholar]
- Nguyen, N.C.; Kaushik, A.; Wolverson, M.K.; Osman, M.M. Is there a common SUV threshold in oncological FDG PET/CT, at least for some common indications? A retrospective study. Acta Oncol. 2011, 50, 670–677. [Google Scholar]
- Kim, S.K.; Allen-Auerbach, M.; Goldin, J.; Fueger, B.J.; Dahlbom, M.; Brown, M.; Czernin, J.; Schiepers, C. Accuracy of PET/CT in characterization of solitary pulmonary lesions. J. Nucl. Med. 2007, 48, 214–220. [Google Scholar]
- Deppen, S.; Putnam, J.B., Jr.; Andrade, G.; Speroff, T.; Nesbitt, J.C.; Lambright, E.S.; Massion, P.P.; Walker, R.; Grogan, E.L. Accuracy of FDG-PET to diagnose lung cancer in a region of endemic granulomatous disease. Ann. Thoracic Surg. 2011, 92, 428–433. [Google Scholar]
- Gould, M.K.; Maclean, C.C.; Kuschner, W.G.; Rydzak, C.E.; Owens, D.K. Accuracy of positron emission tomography for diagnosis of pulmonary nodules and mass lesions: A meta-analysis. JAMA 2001, 285, 914–924. [Google Scholar]
- Orlacchio, A.; Schillaci, O.; Antonelli, L.; D’Urso, S.; Sergiacomi, G.; Nicoli, P.; Simonetti, G. Solitary pulmonary nodules: Morphological and metabolic characterisation by FDG-PET-MDCT. La Radiol. Med. 2007, 112, 157–173. [Google Scholar]
- Zhang, L.; Wang, Y.; Lei, J.; Tian, J.; Zhai, Y. Dual time point 18FDG-PET/CT versus single time point 18FDG-PET/CT for the differential diagnosis of pulmonary nodules: A meta-analysis. Acta Radiol. 2013, 54, 770–777. [Google Scholar]
- Gould, M.K.; Fletcher, J.; Iannettoni, M.D.; Lynch, W.R.; Midthun, D.E.; Naidich, D.P.; Ost, D.E.; American College of Chest Physicians. Evaluation of patients with pulmonary nodules: When is it lung cancer? ACCP evidence-based clinical practice guidelines (2nd edition). Chest 2007, 132, 108S–130S. [Google Scholar]
- Wahl, R.L.; Jacene, H.; Kasamon, Y.; Lodge, M.A. From RECIST to PERCIST: Evolving considerations for PET Response Criteria in Solid Tumors. J. Nucl. Med. 2009, 50, 122S–150S. [Google Scholar]
- Weber, W.A. Assessing Tumor Response to Therapy. J. Nucl. Med. 2009, 50, 1S–10S. [Google Scholar]
- Minn, H.; Paul, R.; Ahonen, A. Evaluation of treatment response to radiotherapy in head and neck cancer with fluorine-18 fluorodeoxyglucose. J. Nucl. Med. 1988, 29, 1521–1525. [Google Scholar]
- Wahl, R.L.; Zasadny, K.; Helvie, M.; Hutchins, G.D.; Weber, B.; Cody, R. Metabolic monitoring of breast cancer chemo-hormonotherapy using positron emission tomography: Initial evaluation. J. Clin. Oncol. 1993, 11, 2101–2111. [Google Scholar]
- Hoekstra, O.S.; van Lingen, A.; Ossenkoppele, G.J.; Golding, R.; Teule, G.J. Early response monitoring in malignant lymphoma using fluorine-18 fluorodeoxyglucose single-photon emission tomography. Eur.J. Nucl. Med. 1993, 20, 1214–1217. [Google Scholar]
- Mikhaeel, N.G.; Hutchings, M.; Fields, P.A.; O’Doherty, M.J.; Timothy, A.R. FDG-PET after two to three cycles of chemotherapy predicts progression-free and overall survival in high-grade non-Hodgkin lymphoma. Ann. Oncol. 2005, 16, 1514–1523. [Google Scholar]
- Hutchings, M.; Loft, A.; Hansen, M.; Pedersen, L.M.; Buhl, T.; Jurlander, J.; Buus, S.; Keiding, S.; D’Amore, F.; Boesen, A.M.; et al. FDG-PET after two cycles of chemotherapy predicts treatment failure and progression-free survival in Hodgkin lymphoma. Blood 2006, 107, 52–59. [Google Scholar]
- Gallamini, A.; Rigacci, L.; Merli, F.; Nassi, L.; Bosi, A.; Capodanno, I.; Vitolo, U.; Sancetta, R.; Iannitto, E.; Trentin, L.; et al. The predictive value of positron emission tomography scanning performed after two courses of standard therapy on treatment outcome in advanced stage Hodgkin’s disease. Haematologica 2006, 91, 475–481. [Google Scholar]
- Cerci, J.J.; Pracchia, L.F.; Linardi, C.C.; Delbeke, D.; Izaki, M.; Trindade, E.; Soares, J., Jr; Buccheri, V.; Meneghetti, J.C. 18F-FDG PET after 2 cycles of ABVD predicts event-free survival in early and advanced Hodgkin lymphoma. J. Nucl. Med. 2010, 51, 1337–1343. [Google Scholar]
- Casasnovas, R.O.; Meignan, M.; Berriolo-Riedinger, A.; Bardet, S.; Julian, A.; Thieblemont, C.; Vera, P.; Bologna, S.; Brière, J.; Jais, J.P.; et al. SUVmax reduction improves early prognosis value of interim positron emission tomography scans in diffuse large B-cell lymphoma. Blood 2011, 118, 37–43. [Google Scholar]
- Terasawa, T.; Lau, J.; Bardet, S.; Couturier, O.; Hotta, T.; Hutchings, M.; Nihashi, T.; Nagai, H. Fluorine-18-fluorodeoxyglucose positron emission tomography for interim response assessment of advanced stage Hodgkin’s lymphoma and diffuse large B-cell lymphoma: A systematic review. J. Clin. Oncol. 2009, 27, 1906–1914. [Google Scholar]
- Meignan, M.; Gallamini, A.; Haioun, C.; Polliack, A. Report on the Second International Workshop on interim positron emission tomography in lymphoma held in Menton, France, 8–9 April 2010. Leuk. Lymphoma 2010, 51, 217111–217180. [Google Scholar]
- Meignan, M.; Itti, E.; Gallamini, A.; Hioun, C. Interim 18F-fluorodeoxyglucose positron emission tomography in diffuse large B-cell lymphoma: Qualitative or quantitative Interpretation—Where do we stand? Leuk. Lymphoma 2009, 50, 1753–1756. [Google Scholar]
- Gallamini, A.; Fiore, F.; Sorasio, R.; Meignan, M. Interim positron emission tomography scan in Hodgkin lymphoma: Definitions, interpretation rules, and clinical validation. Leuk. Lymphoma 2009, 50, 1761–1764. [Google Scholar]
- Gallamini, A. Positron emission tomography scanning: A new paradigm for the management of Hodgkin’s lymphoma. Haematologica 2010, 95, 1046–1048. [Google Scholar]
- Facey, K.; Bradbury, I.; Laking, G.; Payne, E. Overview of the clinical effectiveness of positron emission tomography imaging in selected cancers. Health Technol. Assess. 2007, 11, 44. [Google Scholar]
- Fletcher, J.W.; Djulbegovic, B.; Soares, H.P.; Siegel, B.A.; Lowe, V.J.; Lyman, G.H.; Coleman, R.E.; Wahl, R.; Paschold, J.C.; Avril, N.; et al. Recommendations on the use of 18 F-FDG PET in oncology. J. Nucl. Med. 2008, 49, 480–508. [Google Scholar]
- Shankar, L.K.; Hoffman, J.M.; Bacharach, S.; Graham, M.M.; Karp, J.; Lammertsma, A.A.; Larson, S.; Mankoff, D.A.; Siegel, B.A.; van den Abbeele, A.; et al. Consensus recommendations for the use of 18F-FDG PET as an indicator of therapeutic response in patients in National Cancer Institute trials. J. Nucl. Med. 2006, 47, 1059–1066. [Google Scholar]
- Young, H.; Baum, R.; Cremerius, U.; Herholz, K.; Hoekstra, O.; Lammertsma, A.A.; Pruim, J.; Price, P. Measurement of clinical and subclinical tumour response using [18F]-fluorodeoxyglucose and positron emission tomography: Review and 1999 EORTC recommendations. European Organization for Research and Treatment of Cancer (EORTC) PET Study Group. Eur. J. Cancer 1999, 35, 1773–1782. [Google Scholar]
- Contractor, K.B.; Aboagye, E.O. Monitoring predominantly cytostatic treatment response with 18F-FDG PET. J. Nucl. Med. 2009, 50, 97S–105S. [Google Scholar]
- Castell, F.; Cook, G.J. Quantitative techniques in 18 FDG PET scanning in oncology. Br. J. Cancer 2008, 98, 1597–1601. [Google Scholar]
- Keyes, J.W., Jr. SUV: Standard uptake or silly useless value? J. Nucl. Med. 1995, 36, 1836–1839. [Google Scholar]
- Kostakoglu, L.; Goldsmith, S.J.; Leonard, J.P.; Christos, P.; Furman, R.R.; Atasever, T.; Chandramouly, A.; Verma, S.; Kothari, P.; Coleman, M. FDG-PET after 1 cycle of therapy predicts outcome in diffuse large cell lymphoma and classic Hodgkin disease. Cancer 2006, 107, 2678–2687. [Google Scholar]
- Zinzani, P.L.; Rigacci, L.; Stefoni, V.; Broccoli, A.; Puccini, B.; Castagnoli, A.; Vaggelli, L.; Zanoni, L.; Argnani, L.; Baccarani, M.; et al. Early interim 18 F-FDG PET in Hodgkin’s lymphoma: Evaluation on 304 patients. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 4–12. [Google Scholar]
- Hutchings, M.; Mikhaeel, N.G.; Fields, P.A.; Nunan, T.; Timothy, A.R. Prognostic value of interim FDG-PET after two or three cycles of chemotherapy in Hodgkin lymphoma. Ann. Oncol. 2005, 16, 1160–1168. [Google Scholar]
- Gallamini, A.; Hutchings, M.; Rigacci, L.; Specht, L.; Merli, F.; Hansen, M.; Patti, C.; Loft, A.; di Raimondo, F.; D’Amore, F.; et al. Early interim 2-[18F]fluoro-2-deoxy-D glucose positron emission tomography is prognostically superior to international prognostic score in advanced-stage Hodgkin’s lymphoma: A report from a joint Italian-Danish study. J. Clin. Oncol. 2007, 25, 3746–3752. [Google Scholar]
- Lin, C.; Itti, E.; Haioun, C.; Petegnief, Y.; Luciani, A.; Dupuis, J.; Talbot, J.N.; Rahmouni, A.; Meignan, M. Early 18F-FDG PET for prediction of prognosis in patients with diffuse large B-Cell lymphoma: SUV-based assessment versus visual analysis. J. Nucl. Med. 2007, 48, 1626–1632. [Google Scholar]
- Moskowitz, C.H.; Schoder, H.; Teruya-Feldstein, J.; Sima, C.; Iasonos, A.; Portlock, C.S.; Straus, D.; Noy, A.; Palomba, M.L.; O’Connor, O.A.; et al. Risk adapted dose-dense immunochemoterapy determined by interim FDG-PET in advanced stage diffuse large B-cell lymphoma. J. Clin. Oncol. 2010, 28, 1896–1903. [Google Scholar]
- Pregno, P.; Chiappella, A.; Bello, M.; Botto, B.; Ferrero, S.; Franceschetti, S.; Giunta, F.; Ladetto, M.; Limerutti, G.; Menga, M.; et al. Interim 18-FDG-PET/CT failed to predict the outcome in diffuse large B-cell lymphoma patients treated at the diagnosis with rituximab-CHOP. Blood 2012, 119, 2066–2073. [Google Scholar]
- Cashen, A.F.; Dehdashti, F.; Luo, J.; Homb, A.; Siegel, B.A.; Bartlett, N.L. 18-FDG-PET/CT for early response assessment in diffuse large B-cell lymphoma: Poor predictive value of international harmonization project interpretation. J. Nucl. Med. 2011, 52, 386–392. [Google Scholar]
- Gallamini, A.; Kostakoglu, L. Interim FDG-PET in Hodgkin lymphoma: A compass for a safe navigation in clinical trials? Blood 2012, 120, 4913–4920. [Google Scholar]
- Dupuis, J.; Berriolo-Riedinger, A.; Julian, A.; Brice, P.; Tychyj-Pinel, C.; Tilly, H.; Mounier, N.; Gallamini, A.; Feugier, P.; Soubeyran, P.; et al. Impact of [(18)F]fluorodeoxyglucose positron emission tomography response evaluation in patients with high tumor burden follicular lymphoma treated with immunochemotherapy: A prospective study from the Groupe d’Etudes des Lymphomes de l’Adulte and GOELAMS. J. Clin. Oncol. 2012, 30, 4317–4322. [Google Scholar]
- Pellegrini, C.; Casadei, B.; Derenzini, E.; Stefoni, V.; Derenzini, E.; Gandolfi, L.; Casadei, B.; Maglie, R.; Pileri, S.; Zinzani, P.L. Prognostic Value of Interim Positron Emission Tomography in Patients With Peripheral T-Cell Lymphoma. Oncologist 2014, 19, 746–750. [Google Scholar]
- Meignan, M.; Gallamini, A.; Haioun, C. Report on the first international workshop on interim-PET scan in Lymphoma. Leuk. Lymphoma 2009, 50, 1257–1260. [Google Scholar]
- Biggi, A.; Gallamini, A.; Chauvie, S.; Hutchings, M.; Kostakoglu, L.; Gregianin, M.; Meignan, M.; Malkowski, B.; Hofman, M.S.; Barrington, S.F.; et al. International validation study for interim PET in ABVD-treated, advanced-stage Hodgkin lymphoma: Interpretation criteria and concordance rate among reviewers. J. Nucl. Med. 2013, 54, 683–690. [Google Scholar]
- Gallamini, A.; Barrington, S.F.; Biggi, A.; Chauvie, S.; Kostakoglu, L.; Gregianin, M.; Meignan, M.; Mikhaeel, G.N.; Loft, A.; Zaucha, J.M.; et al. The predictive role of interim Positron Emission Tomography on Hodgkin lymphoma treatment outcome is confirmed using the 5-point scale interpretation criteria. Haematologica 2014, 99, 1107–1113. [Google Scholar]
- Schwarz-Dose, J.; Untch, M.; Tiling, R.; Sassen, S.; Mahner, S.; Kahlert, S.; Harbeck, N.; Lebeau, A.; Brenner, W.; Schwaiger, M.; et al. Monitoring primary systemic therapy of large and locally advanced breast cancer by using sequential positron emission tomography imaging with [18F] fluorodeoxyglucose. J. Clin. Oncol. 2009, 27, 535–541. [Google Scholar]
- Martoni, A.A.; Zamagni, C.; Quercia, S.; Rosati, M.; Cacciari, N.; Bernardi, A.; Musto, A.; Fanti, S.; Santini, D.; Taffurelli, M. Early (18)F-2-fluoro-2-deoxy-D-glucose positron emission tomography may identify a subset of patients with estrogen receptor-positive breast cancer who will not respond optimally to preoperative chemotherapy. Cancer 2010, 116, 805–813. [Google Scholar]
- Keam, B.; Im, S.A.; Koh, Y.; Han, S.W.; Oh, D.Y.; Cho, N.; Kim, J.H.; Han, W.; Kang, K.W.; Moon, W.K.; et al. Early metabolic response using FDG PET/CT and molecular phenotypes of breast cancer treated with neoadjuvant chemotherapy. BMC Cancer 2011, 11, 452. [Google Scholar]
- Schelling, M.; Avril, N.; Nahrig, J.; Kuhn, W.; Römer, W.; Sattler, D.; Werner, M.; Dose, J.; Jänicke, F.; Graeff, H.; et al. Positron emission tomography using [18F]fluorodeoxyglucose for monitoring primary chemotherapy in breast cancer. J. Clin. Oncol. 2000, 18, 1689–1695. [Google Scholar]
- Smith, I.C.; Welch, A.E.; Hutcheon, A.W.; Miller, I.D.; Payne, S.; Chilcott, F.; Waikar, S; Whitaker, T.; Ah-See, A.K.; Eremin, O.; et al. Positron emission tomography using [18F]-fluorodeoxy-D-glucose to predict the pathologic response of breast cancer to primary chemotherapy. J. Clin. Oncol. 2000, 18, 1676–1688. [Google Scholar]
- Rousseau, C.; Devillers, A.; Sagan, C.; Ferrer, L.; Bridji, B.; Campion, L.; Ricaud, M.; Bourbouloux, E.; Doutriaux, I.; Clouet, M.; et al. Monitoring of early response to neoadjuvant chemotherapy in stage II and III breast cancer by [18F]fluorodeoxyglucose positron emission tomography. J. Clin. Oncol. 2006, 24, 5366–5372. [Google Scholar]
- Hendlisz, A.; Golfinopoulos, V.; Deleporte, A.; Paesmans, M.; El Mansy, H.; Garcia, C.; Peeters, M.; Annemans, L.; Vandeputte, C.; Maetens, M.; et al. Preoperative chemosensitivity testing as predictor of treatment benefit in adjuvant stage III colon cancer (PePiTA): Protocol of a prospective BGDO (Belgian Group for Digestive Oncology) multicentric study. BMC Cancer 2013, 13, 190–199. [Google Scholar]
- De Geus-Oei, L.F.; van Laarhoven, H.W.; Visser, E.P.; Hermsen, R.; van Hoorn, B.A.; Kamm, Y.J.; Krabbe, P.F.; Corstens, F.H.; Punt, C.J.; Oyen, W.J. Chemotherapy response evaluation with FDG–PET in patients with colorectal cancer. Ann. Oncol. 2008, 19, 348–352. [Google Scholar]
- Byström, P.; Berglund, A.; Garske, U.; Jacobsson, H.; Sundin, A.; Nygren, P.; Frödin, J.E.; Glimelius, B. Early prediction of response to first-line chemotherapy by sequential [18 F]-2-fluoro-2-deoxy-D-glucose positron emission tomography in patients with advanced colorectal cancer. Ann. Oncol. 2009, 20, 1057–1061. [Google Scholar]
- Kim, J.; Choi, S.; Yi, H.; Lim, J.; Lee, M.; Hyun, I.; Kim, C. Prediction of response to chemotherapy using sequential F-18-fluorodeoxyglucose (FDG) positron emission tomography (PET) in patients with metastatic colorectal cancer. J. Clin. Oncol. 2007, 25, 2536. [Google Scholar]
- Hendlisz, A.; Golfinopoulos, V.; Garcia, C.; Covas, A.; Emonts, P.; Ameye, L.; Paesmans, M.; Deleporte, A.; Machiels, G.; Toussaint, E.; et al. Serial FDG-PET/CT for early outcome prediction in patients with metastatic colorectal cancer undergoing chemotherapy. Ann. Oncol. 2012, 23, 1687–1693. [Google Scholar]
- Yoon, D.H.; Cho, Y.; Kim, S.Y.; Nam, S.Y.; Choi, S.H.; Roh, J.L.; Lee, S.W.; Song, S.Y.; Lee, J.H.; Kim, J.S.; et al. Usefulness of interim FDG-PET after induction chemotherapy in patients with locally advanced squamous cell carcinoma of the head and neck receiving sequential induction chemotherapy followed by concurrent chemoradiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 118–125. [Google Scholar]
- Ceulemans, G.; Voordeckers, M.; Farrag, A.; Verdriers, D.; Storme, G.; Everaert, H. Can 18-FDG-PET during radiotherapy replace post-therapy scanning for detection/demonstration of tumor response in head and neck cancer? Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 938–942. [Google Scholar]
- Goldstraw, P.; Crowley, J.; Chansky, K.; Giroux, D.J.; Groome, P.A.; Rami-Porta, R.; Postmus, P.E.; Rusch, V.; Sobin, L.; International Association for the Study of Lung Cancer International Staging Committee; et al. The IASLC Lung Cancer Staging Project: Proposals for the revision of the TNM stage groupings in the forthcoming (seventh) ed. of the TNM Classification of malignant tumours. J. Thorac. Oncol. 2007, 2, 706–714. [Google Scholar]
- Aukema, T.S.; Kappers, I.; Valdés Olmos, R.A.; Codrington, H.E.; van Tinteren, H.; van Pel, R.; Klomp, H.M.; NEL Study Group. Is 18F-FDG PET/CT useful for the early prediction of histopathologic response to neoadjuvant erlotinib in patients with non-small cell lung cancer? J. Nucl. Med. 2010, 51, 1344–1348. [Google Scholar]
- Hoekstra, C.J.; Stroobants, S.G.; Smit, E.F.; Vansteenkiste, J.; van Tinteren, H.; Postmus, P.E.; Golding, R.P.; Biesma, B.; Schramel, F.J.; van Zandwijk, N.; et al. Prognostic relevance of response evaluation using [18F]-2-fluoro-2-deoxy-d-glucose positron emission tomography in patients with locally advanced non-small-cell lung cancer. J. Clin. Oncol. 2005, 23, 8362–8370. [Google Scholar]
- Lee, D.H.; Kim, S.K.; Lee, H.Y.; Lee, S.Y.; Park, S.H.; Kim, H.Y.; Kang, K.W.; Han, J.Y.; Kim, H.T.; Lee, J.S. Early prediction of response to first-line therapy using integrated 18F-FDG PET/CT for patients with advanced/metastatic non-small cell lung cancer. J. Thorac. Oncol. 2009, 4, 816–821. [Google Scholar]
- Decoster, L.; Schallier, D.; Everaert, H.; Nieboer, K.; Meysman, M.; Neyns, B.; de Mey, J.; de Grève, J. Complete metabolic tumour response, assessed by 18-fluorodeoxyglucose positron emission tomography (18FDGPET), after induction chemotherapy predicts a favourable outcome in patients with locally advanced non-small cell lung cancer (NSCLC). Lung Cancer 2008, 62, 55–61. [Google Scholar]
- Jemal, A.; Murray, T.; Ward, E.; Samuels, A.; Tiwari, R.C.; Ghafoor, A.; Feuer, E.J.; Thun, M.J. Cancer statistics. CA Cancer. J. Clin. 2005, 55, 10–30. [Google Scholar]
- Miyata, M.; Yamasaki, M.; Takahashi, T.; Murakami, K.; Tanaka, K.; Yukinori, K.; Nakajima, K.; Takiguchi, S.; Morii, E.; Hatazawa, J.; et al. Determinants of response to neoadjuvant chemotherapy for esophageal cancer using 18F-fluorodeoxiglucose Positron Emission Tomography (18F-FDG-PET). Ann. Surg. Oncol. 2013. [Google Scholar] [CrossRef]
- Weber, W.A.; Ott, K.; Becker, K.; Dittler, H.J.; Helmberger, H.; Avril, N.E.; Meisetschläger, G.; Busch, R.; Siewert, J.R.; Schwaiger, M.; et al. Prediction of response to preoperative chemotherapy in adenocarcinomas of the esophagogastric junction by metabolic imaging. J. Clin. Oncol. 2001, 19, 3058–3065. [Google Scholar]
- Lordick, F.; Ott, K.; Krause, B.J.; Weber, W.A.; Becker, K.; Stein, H.J.; Lorenzen, S.; Schuster, T.; Wieder, H.; Herrmann, K.; et al. PET to assess early metabolic response and to guide treatment of adenocarcinoma of the oesophagogastric junction: The MUNICON phase II trial. Lancet Oncol. 2007, 8, 797–805. [Google Scholar]
- Krause, B.J.; Herrmann, K.; Wieder, H.; Meyer zum Buschenfelde, C. 18F-FDG PET and 18F-FDG PET/CT for assessing response to therapy in esophageal cancer. J. Nucl. Med. 2009, 50, 89S–96S. [Google Scholar]
- Miller, A.B.; Hoogstraten, B.; Staquet, M.; Winkler, A. Reporting results of cancer treatment. Cancer 1981, 47, 207–214. [Google Scholar]
- Therasse, P.; Arbuck, S.G.; Eisenhauer, E.A.; Wanders, J.; Kaplan, R.S.; Rubinstein, L.; Verweij, J.; van Glabbeke, M.; van Oosterom, A.T.; Christian, M.C.; et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J. Natl. Cancer Inst. 2000, 92, 205–216. [Google Scholar]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumors: Revised RECIST guideline (version1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar]
- Moertel, C.G.; Hanley, J.A. The effect of measuring error on the results of therapeutic trials in advanced cancer. Cancer 1976, 38, 388–394. [Google Scholar]
- Karrison, T.G.; Maitland, M.L.; Stadler, W.M.; Ratain, M.J. Design of phase II cancer trials using a continuous endpoint of change in tumor size: Application to a study of sorafenib and erlotinib in non small-cell lung cancer. J. Natl. Cancer Inst. 2007, 99, 1455–1461. [Google Scholar]
- Michaelis, L.C.; Ratain, M.J. Measuring response in a post-RECIST world: From black and white to shades of grey. Nat. Rev. Cancer 2006, 6, 409–414. [Google Scholar]
- Radford, J.A.; Cowan, R.A.; Flanagan, M.; Dunn, G.; Crowther, D.; Johnson, R.J.; Eddleston, B. The significance of residual mediastinal abnormality on the chest radiograph following treatment for Hodgkin’s disease. J. Clin. Oncol. 1988, 6, 940–946. [Google Scholar]
- Surbone, A.; Longo, D.L.; de Vita, V.T., Jr.; Ihde, D.C.; Duffey, P.L.; Jaffe, E.S.; Solomon, D.; Hubbard, S.M.; Young, R.C. Residual abdominal masses in aggressive non-Hodgkin’s lymphoma after combination chemotherapy: Significance and management. J. Clin. Oncol. 1988, 6, 1832–1837. [Google Scholar]
- Naumann, R.; Vaic, A.; Beuthien-Baumann, B.; Bredow, J.; Kropp, J.; Kittner, T.; Franke, W.G.; Ehninger, G. Prognostic value of positron emission tomography in the evaluation of post-treatment residual mass in patients with Hodgkin’s disease and non-Hodgkin’s lymphoma. Br. J. Haematol. 2001, 115, 793–800. [Google Scholar]
- Canellos, G.P. Residual mass in lymphoma may not be residual disease. J. Clin. Oncol. 1988, 6, 931–933. [Google Scholar]
- Cheson, B.D.; Horning, S.J.; Coiffier, B.; Fisher, R.I.; Connors, J.M.; Lister, T.A.; Vose, J.; Grillo-López, A.; Hagenbeek, A.; et al. Report of an international workshop to standardize response criteria for non-Hodgkin’s lymphomas. NCI Sponsored International Working Group. J. Clin. Oncol. 1999, 17, 1244. [Google Scholar]
- Porceddu, S.V.; Pryor, D.I.; Burmeister, E.; Burmeister, B.H.; Poulsen, M.G.; Foote, M.C.; Panizza, B.; Coman, S.; McFarlane, D.; Coman, W.; et al. Results of a prospective study of positron emission tomography-directed management of residual nodal abnormalities in node-positive head and neck cancer after definitive radiotherapy with or without systemic therapy. Head Neck 2011, 33, 1675–1682. [Google Scholar]
- Van den Abbeele, A.D. The Lessons of GIST—PET and PET/CT: A New Paradigm for Imaging. Oncologist 2008, 13, 8–13. [Google Scholar]
- Forner, A.; Ayuso, C.; Varela, M.; Rimola, J.; Hessheimer, A.J.; de Lope, C.R.; Reig, M.; Bianchi, L.; Llovet, J.M.; Bruix, J. Evaluation of tumor response after locoregional therapies in hepatocellular carcinoma: Are response evaluation criteria in solid tumors reliable? Cancer 2009, 115, 616–623. [Google Scholar]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar]
- André, N.; Fabre, A.; Colavolpe, C.; Jacob, T.; Gaudart, J.; Coze, C.; Paris, M.; Gentet, J.C.; Guedj, E.; Michel, G.; et al. FDG PET and evaluation of posttherapeutic residual tumors in pediatric oncology: Preliminary experience. J. Pediatr. Hematol. Oncol. 2008, 30, 343–346. [Google Scholar]
- Jadvar, H.; Connolly, L.P.; Fahey, F.H.; Shulkin, B.L. PET and PET/CT in Pediatric Oncology. Semin. Nucl. Med. 2007, 37, 316–331. [Google Scholar]
- Brucher, B.L.; Weber, W.; Bauer, M.; Fink, U.; Avril, N.; Stein, H.J.; Werner, M.; Zimmerman, F.; Siewert, J.R.; Schwaiger, M. Neoadjuvant therapy of esophageal squamous cell carcinoma: Response evaluation by positron emission tomography. Ann. Surg. 2001, 233, 300–309. [Google Scholar]
- Vansteenkiste, J.F.; Stroobants, S.G.; de Leyn, P.R.; Dupont, P.J.; Verbeken, E.K. Potential use of FDG-PET scan after induction chemotherapy in surgically staged IIIa-N2 non-small-cell lung cancer: A prospective pilot study. The Leuven Lung Cancer Group. Ann. Oncol. 1998, 9, 1193–1198. [Google Scholar]
- Bryant, A.S.; Cerfolio, R.J.; Klemm, K.M.; Ojha, B. Maximum standard uptake value of mediastinal lymph nodes on integrated FDG-PET-CT predicts pathology in patients with non-small cell lung cancer. Ann. Thorac. Surg. 2006, 82, 417–422. [Google Scholar]
- Dooms, C.; Verbeken, E.; Stroobants, S.; Nackaerts, K.; de Leyn, P.; Vansteenkiste, J. Prognostic stratification of stage IIIA-N2 non-small-cell lung cancer after induction chemotherapy: A model based on the combination of morphometric pathologic response in mediastinal nodes and primary tumor response on serial 18-fluoro-2-deoxy-glucose positron emission tomography. J. Clin. Oncol. 2008, 26, 1128–1134. [Google Scholar]
- Kasamon, Y.L.; Wahl, R.L. FDG PET and risk-adapted therapy in Hodgkin and non-Hodgkin’s lymphoma. Curr. Opin. Oncol. 2008, 20, 206–219. [Google Scholar]
- Kasamon, Y.L.; Jones, R.J.; Wahl, R.L. Integrating PET and PET/CT into the risk adapted therapy of lymphoma. J. Nucl. Med. 2007, 48, 19S–27S. [Google Scholar]
- Humm, J.L.; Rosenfeld, A.; del Guerra, A. From PET detectors to PET scanners. Eur. J. Nucl. Med. Mol. Imaging 2003, 30, 1574–1597. [Google Scholar]
- Tatsumi, M.; Cohade, C.; Nakamoto, Y.; Fishman, E.K.; Wahl, R.L. Direct comparison of FDG PET and CT findings in patients with lymphoma: Initial experience. Radiology 2005, 237, 1038–1045. [Google Scholar]
- Boellaard, R.; Oyen, W.J.; Hoekstra, C.J.; Hoekstra, O.S.; Visser, E.P.; Willemsen, A.T.; Arends, B.; Verzijlbergen, F.J.; Zijlstra, J.; Paans, A.M.; et al. The Netherlands protocol for standardisation and quantification of FDG whole body PET studies in multicenter trials. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 2320–2333. [Google Scholar]
- Ziai, D.; Wagner, T.; El Badaoui, A.; Hitzel, A.; Woillard, J.B.; Melloni, B.; Monteil, J. Therapy response evaluation with FDG-PET/CT in small cell lung cancer: A prognostic and comparison study of the PERCIST and EORTC criteria. Cancer Imaging 2013, 13, 73–80. [Google Scholar]
- Skougaard, K.; Nielsen, D.; Vittrup Jensen, B.; Westergren Hendel, H. Comparison of EORTC Criteria and PERCIST for PET/CT Response Evaluation of Patients with Metastatic Colorectal Cancer Treated with Irinotecan and Cetuximab. J. Nucl. Med. 2013, 54, 1026–1031. [Google Scholar]
- Maffione, A.M.; Ferretti, A.; Chondrogiannis, S.; Rampin, L.; Marzola, M.C.; Grassetto, G.; Capirci, C.; Colletti, P.M.; Rubello, D. Proposal of a new 18F-FDG PET/CT predictor of response in rectal cancer treated by neoadjuvant chemoradiation therapy and comparison with PERCIST criteria. Clin. Nucl. Med. 2013, 38, 795–797. [Google Scholar]
- Costelloe, C.M.; Chuang, H.H.; Madewell, J.E.; Ueno, N.T. Cancer Response Criteria and Bone Metastases: RECIST 1.1, MDA and PERCIST. J. Cancer 2010, 1, 80–92. [Google Scholar]
- Cheson, B.D.; Pfistner, B.; Juweid, M.E.; Gascoyne, R.D.; Specht, L.; Horning, S.J.; Coiffier, B.; Fisher, R.I.; Hagenbeek, A.; Zucca, E.; et al. Revised response criteria for malignant lymphoma. J. Clin. Oncol. 2007, 25, 579–586. [Google Scholar]
- Juweid, M.E.; Stroobants, S.; Hoekstra, O.S.; Mottaghy, F.M.; Dietlein, M.; Guermazi, A.; Wiseman, G.A.; Kostakoglu, L.; Scheidhauer, K.; Buck, A.; et al. Use of Positron Emission Tomography for Response Assessment of Lymphoma: Consensus of the Imaging Subcommittee of International Harmonization Project in Lymphoma. J. Clin. Oncol. 2007, 25, 571–578. [Google Scholar]
- Juweid, M.E.; Cheson, B.D. Role of positron emission tomography in lymphoma. J. Clin. Oncol. 2005, 23, 4577–4580. [Google Scholar]
- Fabel, M.; von Tengg-Kobligk, H.; Giesel, F.L.; Bornemann, L.; Dicken, V.; Kopp-Schneider, A.; Moser, C.; Delorme, S.; Kauczor, H.U. Semi-automated volumetric analysis of lymph node metastases in patients with malignant melanoma stage III/IV—A feasibility study. Eur. Radiol. 2008, 18, 1114–1122. [Google Scholar]
- Barrington, S.F.; Qian, W.; Somer, E.J.; Franceschetto, A.; Bagni, B.; Brun, E.; Almquist, H.; Loft, A.; Højgaard, L.; Federico, M.; et al. Concordance between four European centres of PET reporting criteria designed for use in multicentre trials in Hodgkin lymphoma. Eur. J. Nucl. Med.Mol. Imaging. 2010, 37, 1824–1833. [Google Scholar]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for initial evaluation, staging and response assessment of Hodgkin and non-Hodgkin lymphoma—The lugano classification. J. Clin. Oncol. 2014. [Google Scholar] [CrossRef]
- Galow, J.R.; Burstein, H.J.; Wood, W.; Hortobagyi, G.N.; Gianni, L.; von Minckwitz, G.; Buzdar, A.U.; Smith, I.E.; Symmans, W.F.; Singh, B.; et al. Preoperative therapy in invasive breast cancer: Pathologic assessment and systemic therapy issues in operable disease. J. Clin. Oncol. 2008, 26, 814–819. [Google Scholar]
- Mauri, D.; Pavlidis, N.; Ioannidis, J.P. Neoadjuvant versus adjuvant systemic treatment in breast cancer: A meta-analysis. J. Natl. Cancer Inst. 2005, 97, 188–194. [Google Scholar]
- Bear, H.D.; Anderson, S.; Smith, R.E.; Geyer, C.E., Jr.; Mamounas, E.P.; Fisher, B.; Brown, A.M.; Robidoux, A.; Margolese, R.; Kahlenberg, M.S.; et al. Sequential preoperative or postoperative docetaxel added to preoperative doxorubicin plus cyclophosphamide for operable breast cancer: National Surgical Adjuvant Breast and Bowel Project Protocol B-27. J. Clin. Oncol. 2006, 24, 2019–2027. [Google Scholar]
- Bonadonna, G.; Valagussa, P.; Brambilla, C.; Ferrari, L.; Moliterni, A.; Terenziani, M.; Zambetti, M. Primary chemotherapy in operable breast cancer: Eight-year experience at the Milan Cancer Institute. J. Clin. Oncol. 1998, 16, 93–100. [Google Scholar]
- Fisher, E.R.; Wang, J.; Bryant, J.; Fisher, B.; Mamounas, E.; Wolmark, N. Pathobiology of preoperative chemotherapy: Findings from the National Surgical Adjuvant Breast and Bowel (NSABP) protocol B-18. Cancer 2002, 95, 681–695. [Google Scholar]
- Honkoop, A.H.; van Diest, P.J.; de Jong, J.S.; Linn, S.C.; Giaccone, G.; Hoekman, K.; Wagstaff, J.; Pinedo, H.M. Prognostic role of clinical, pathological and biological characteristics in patients with locally advanced breast cancer. Br. J. Cancer 1998, 77, 621–626. [Google Scholar]
- Fisher, B.; Bryant, J.; Wolmark, N.; Mamounas, E.; Brown, A.; Fisher, E.R.; Wickerham, D.L.; Begovic, M.; DeCillis, A.; Robidoux, A.; et al. Effect of preoperative chemotherapy on the outcome of women with operable breast cancer. J. Clin. Oncol. 1998, 16, 2672–2685. [Google Scholar]
- Chollet, P.; Amat, S.; Cure, H.; de Latour, M.; Le Bouedec, G.; Mouret-Reynier, M.A.; Ferriere, J.P.; Achard, J.L.; Dauplat, J.; Penault-Llorca, F. Prognostic significance of a complete pathological response after induction chemotherapy in operable breast cancer. Br. J. Cancer 2002, 86, 1041–1046. [Google Scholar]
- Gonzalez-Angulo, A.M.; McGuire, S.E.; Buchholz, T.A.; Tucker, S.L.; Kuerer, H.M.; Rouzier, R.; Kau, S.W.; Huang, E.H.; Morandi, P.; Ocana, A.; et al. Factors predictive of distant metastases in patients with breast cancer who have a pathologic complete response after neoadjuvant chemotherapy. J. Clin. Oncol. 2005, 23, 7098–7104. [Google Scholar]
- Isasi, C.R.; Moadel, R.M.; Blaufox, M.D. A meta-analysis of FDG-PET for the evaluation of breast cancer recurrence and metastases. Breast Cancer Res. Treat. 2005, 90, 105–112. [Google Scholar]
- Du, Y.; Cullum, I.; Illidge, T.M.; Ell, P.J. Fusion of metabolic function and morphology: Sequential [18F]fluorodeoxyglucose positron-emission tomography/computed tomography studies yield new insights into the natural history of bone metastases in breast cancer. J. Clin. Oncol. 2007, 25, 3440–3447. [Google Scholar]
- Hinshaw, J.L.; Lee, F.T., Jr. Cryoablation for liver cancer. Tech. Vasc. Interv. Radiol. 2007, 10, 47–57. [Google Scholar]
- Wood, T.F.; Rose, D.M.; Chung, M.; Allegra, D.P.; Foshag, L.J.; Bilchik, A.J. Radiofrequency ablation of 231 unresectable hepatic tumors: Indications, limitations, and complications. Ann. Surg. Oncol. 2000, 7, 593–600. [Google Scholar]
- Sharma, R.A.; Van Hazel, G.A.; Morgan, B.; Berry, D.P.; Blanshard, K.; Price, D.; Bower, G.; Shannon, J.A.; Gibbs, P.; Steward, W.P. Radioembolization of liver metastases from colorectal cancer using Yttrium-90 microspheres with concomitant systemic oxaliplatin, fluorouracil, and leucovorin chemotherapy. J. Clin. Oncol. 2007, 25, 1099–1106. [Google Scholar]
- Bester, L.; Meteling, B.; Pocock, N.; Saxena, A.; Chua, T.C.; Morris, D.L. Radioembolisation with Yttrium-90 microspheres: An effective treatment modality for unresectable liver metastases. J. Med. Imaging Radiat. Oncol. 2013, 57, 72–80. [Google Scholar]
- Langenhoff, B.S.; Oyen, W.J.; Jager, G.J.; Strijk, S.P.; Wobbes, T.; Corstens, F.H.; Ruers, T.J. Efficacy of fluorine-18-deoxyglucose positron emission tomography in detecting tumor recurrence after local ablative therapy for liver metastases: A prospective study. J. Clin. Oncol. 2002, 20, 4453–4458. [Google Scholar]
- Joosten, J.; Jager, G.; Oyen, W.; Wobbes, T.; Ruers, T. Cryosurgery and radiofrequency ablation for unresectable colorectal liver metastases. Eur. J. Surg. Oncol. 2005, 31, 1152–1159. [Google Scholar]
- Donckier, V.; van Laethem, J.L.; Goldman, S.; van Gansbeke, D.; Feron, P.; Ickx, B.; Wikler, D.; Gelin, M. [F-18] fluorodeoxyglucose positron emission tomography as a tool for early recognition of incomplete tumor destruction after radiofrequency ablation for liver metastases. J. Surg. Oncol. 2003, 84, 215–223. [Google Scholar]
- Blokhuis, T.J.; van der Schaaf, M.C.; van den Tol, M.P.; Comans, E.F.; Manoliu, R.A.; van der Sijp, J.R. Results of radio frequency ablation of primary and secondary liver tumors: Long-term follow-up with computed tomography and positron emission tomography-18F-deoxyfluoroglucose scanning. Scand. J. Gastroenterol. Suppl. 2004, 241, 93–97. [Google Scholar]
- Veit, P.; Antoch, G.; Stergar, H.; Bockisch, A.; Forsting, M.; Kuehl, H. Detection of residual tumor after radiofrequency ablation of liver metastasis with dual modality PET/CT: Initial results. Eur. Radiol. 2006, 16, 80–87. [Google Scholar]
- Salem, R.; Lewandowski, R.J.; Gates, V.L.; Nutting, C.W.; Murthy, R.; Rose, S.C.; Soulen, M.C.; Geschwind, J.F.; Kulik, L.; Kim, Y.H.; et al. Research reporting standards for radioembolization of hepatic malignancies. J. Vasc. Interv. Radiol. 2011, 22, 265–278. [Google Scholar]
- Shen, S.; DeNardo, G.L.; Yuan, A.; DeNardo, D.A.; DeNardo, S.J. Planar gamma camera imaging and quantitation of yttrium-90 bremsstrahlung. J. Nucl. Med. 1994, 35, 1381–1389. [Google Scholar]
- Rault, E.; Clementel, E.; Vandenberghe, S.; D’Asseler, Y.; van Holen, R.; de Beenhouwer, J.; Staelens, S. Comparison of yttrium-90 SPECT and PET images. J. Nucl. Med. 2010, 51, 125. [Google Scholar]
- Elschot, M.; Nijsen, J.F.; Dam, A.J.; de Jong, H.W. Quantitative evaluation of scintillation camera imaging characteristics of isotopes used in liver radioembolization. PLoS One 2011, 6, e26174. [Google Scholar]
- Selwyn, R.G.; Nickles, R.J.; Thomadsen, B.R.; DeWerd, L.A.; Micka, J.A. A new internal pair production branching ratio of 90Y: The development of a non-destructive assay for 90Y and 90Sr. Appl. Radiat. Isot. 2007, 65, 318–327. [Google Scholar]
- Lhommel, R.; van Elmbt, L.; Goffette, P.; van den Eynde, M.; Jamar, F.; Pauwels, S.; Walrand, S. Feasibility of 90Y TOF PET-based dosimetry in liver metastasis therapy using SIR-spheres. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 1654–1662. [Google Scholar]
- Van Elmbt, L.; Vandenberghe, S.; Walrand, S.; Pauwels, S.; Jamar, F. Comparison of yttrium-90 quantitative imaging by TOF and non-TOF PET in a phantom of liver selective internal radiotherapy. Phys. Med. Biol. 2011, 56, 6759–6777. [Google Scholar]
- Walrand, S.; Flux, G.D.; Konijnenberg, M.W.; Valkema, R.; Krenning, E.P.; Lhommel, R.; Pauwels, S.; Jamar, F. Dosimetry of yttrium-labelled radiopharmaceuticals for internal therapy: 86Y or 90Y imaging? Eur. J. Nucl. Med. Mol. Imaging 2011, 38, S57–S68. [Google Scholar]
- Wong, R.K.; Tandan, V.; de Silva, S.; Figueredo, A. Pre-operative radiotherapy and curative surgery for the management of localized rectal carcinoma. Cochrane Database Syst. Rev. 2007, CD002102. [Google Scholar]
- Bosset, J.F.; Collette, L.; Calais, G.; Maingon, P.; Radosevic-Jelic, L.; Daban, A.; Bardet, E.; Beny, A.; Ollier, J.C. Chemotherapy with preoperative radiotherapy in rectal cancer. N. Engl. J. Med. 2006, 355, 1114–1123. [Google Scholar]
- Hospers, G.A.; Punt, C.J.; Tesselaar, M.E.; Cats, A.; Havenga, K.; Leer, J.W.; Marijnen, C.A.; Jansen, E.P.; van Krieken, H.H.; Wiggers, T.; et al. Preoperative chemoradiotherapy with capecitabine and oxaliplatin in locally advanced rectal cancer: A phase I-II multicenter study of the Dutch Colorectal Cancer Group. Ann. Surg. Oncol. 2007, 14, 2773–2779. [Google Scholar]
- De Geus-Oei, L.F.; Vriens, D.; van Laarhoven, H.W.M.; van der Graaf, W.T.A.; Oyen, W.J.G. Monitoring and Predicting Response to Therapy with 18F-FDG PET in Colorectal Cancer: A Systematic Review. J. Nucl. Med. 2009, 50, 43S–54S. [Google Scholar]
- Bipat, S.; Glas, A.S.; Slors, F.J.; Zwinderman, A.H.; Bossuyt, P.M.; Stoker, J. Rectal cancer: Local staging and assessment of lymph node involvement with endoluminal US, CT, and MR imaging—A meta-analysis. Radiology 2004, 232, 773–783. [Google Scholar]
- Kwok, H.; Bissett, I.P.; Hill, G.L. Preoperative staging of rectal cancer. Int. J. Colorectal. Dis. 2000, 15, 9–20. [Google Scholar]
- Kubota, R.; Yamada, S.; Kubota, K.; Ishiwata, K.; Tamahashi, N.; Ido, T. Intratumoral distribution of fluorine-18-fluorodeoxyglucose in vivo: High accumulation in macrophages and granulation tissues studied by microautoradiography. J. Nucl. Med. 1992, 33, 1972–1980. [Google Scholar]
- Larson, S.M. Cancer or inflammation? A Holy Grail for nuclear medicine. J. Nucl. Med. 1994, 35, 1653–1655. [Google Scholar]
- Amthauer, H.; Denecke, T.; Rau, B.; Hildebrandt, B.; Hünerbein, M.; Ruf, J.; Schneider, U.; Gutberlet, M.; Schlag, P.M.; Felix, R.; et al. Response prediction by FDG-PET after neoadjuvant radiochemotherapy and combined regional hyperthermia of rectal cancer: Correlation with endorectal ultrasound and histopathology. Eur. J. Nucl. Med. Mol. Imaging 2004, 31, 811–819. [Google Scholar]
- Janssen, M.H.M.; Ollers, M.C.; van Stiphout, R.G.P.M.; Riedl, R.G.; van den Bogaard, J.; Buijsen, J.; Lambin, P.; Lammering, G. PET-based treatment response evaluation in rectal cancer: Prediction andvalidation. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 871–876. [Google Scholar]
- Mandard, A.M.; Dalibard, F.; Mandard, J.C.; Marnay, J.; Henry-Amar, M.; Petiot, J.F.; Roussel, A.; Jacob, J.H.; Segol, P.; Samama, G.; et al. Pathologic assessment of tumor regression after preoperative chemoradiotherapy of esophageal carcinoma. Clinicopathologic correlations. Cancer 1994, 73, 2680–2686. [Google Scholar]
- Jemal, A.; Thun, M.J.; Ries, L.A.; Howe, H.L.; Weir, H.K.; Center, M.M.; Ward, E.; Wu, X.C.; Eheman, C.; Anderson, R.; et al. Annual report to the Nation on the status of cancer, 1975–2005, featuring trends in lung cancer, tobacco use, and tobacco control. J. Natl. Cancer Inst. 2008, 100, 1672–1694. [Google Scholar]
- Brundage, M.D.; Davies, D.; Mackillop, W.J. Prognostic factors in non-small cell lung cancer: A decade of progress. Chest 2002, 122, 1037–1057. [Google Scholar]
- Wright, G.; Manser, R.L.; Byrnes, G.; Hart, D.; Campbell, D.A. Surgery for non-small cell lung cancer: Systematic review and meta-analysis of randomised controlled trials. Thorax 2006, 61, 597–603. [Google Scholar]
- MacManus, M.P.; Hicks, R.J.; Matthews, J.P.; McKenzie, A.; Rischin, D.; Salminen, E.K.; Ball, D.L. Positron emission tomography is superior to computed tomography scanning for response-assessment after radical radiotherapy or chemoradiotherapy in patients with non-small-cell lung cancer. J. Clin. Oncol. 2003, 21, 1285–1292. [Google Scholar]
- Benz, M.R.; Herrmann, K.; Walter, F.; Garon, E.B.; Reckamp, K.L.; Figlin, R.; Phelps, M.E.; Weber, W.A.; Czernin, J.; Allen-Auerbach, M.S. (18)FFDG PET/CT for monitoring treatment responses to the epidermal growth factor receptor inhibitor erlotinib. J. Nucl. Med. 2011, 52, 1684–1689. [Google Scholar]
- Prestwich, R.J.; Subesinghe, M.; Gilbert, A.; Chowdhury, F.U.; Sen, M.; Scarsbrook, A.F. Delayed response assessment with FDGPET-CT following (chemo) radiotherapy for locally advanced head and neck squamous cell carcinoma. Clin. Radiol. 2012, 67, 966–975. [Google Scholar]
- Ghanooni, R.; Delpierre, I.; Magremanne, M.; Vervaet, C.; Dumarey, N.; Remmelink, M.; Lacroix, S.; Trotta, N.; Hassid, S.; Goldman, S. FDG PET/CT and MRI in the follow-up of head and neck squamous cell carcinoma. Contrast. Media Mol. Imaging 2011, 6, 260–266. [Google Scholar]
- McGuire, W.P.; Hoskins, W.J.; Brady, M.F.; Kucera, P.R.; Partridge, E.E.; Look, K.Y.; Clarke-Pearson, D.L.; Davidson, M. Cyclophosphamide and Cisplatin Compared with Paclitaxel and Cisplatin in Patients with Stage III and Stage IV Ovarian Cancer. N. Engl. J. Med. 1996, 334, 1–6. [Google Scholar]
- Marcus, C.S.; Maxwell, G.L.; Darcy, K.M.; Hamilton, C.A.; McGuire, W.P. Current Approaches and Challenges in Managing and Monitoring Treatment Response in Ovarian Cancer. J. Cancer 2014, 5, 25–30. [Google Scholar]
- Von Georgi, R.; Schubert, K.; Grant, P.; Munstedt, K. Post-therapy surveillance and after-care in ovarian cancer. Eur. J. Obst. Gynecol. Reprod. Biol. 2004, 114, 228–233. [Google Scholar]
- Geurts, S.M.; de Vegt, F.; van Altena, A.M.; Tjan-Heijnen, V.C.; Massuger, L.F.; Adang, E.M.; van Dijck, J.A.; Verbeek, A.L. Impact of routine follow-up examinations on life expectancy in ovarian cancer patients: A simulation study. Int. J. Gynecol. Cancer 2012, 22, 1150–1157. [Google Scholar]
- Kew, F.; Galaal, K.; Bryant, A.; Naik, R. Evaluation of follow-up strategies for patients with epithelial ovarian cancer following completion of primary treatment. Cochrane Database Syst. Rev. 2011. [Google Scholar] [CrossRef]
- Miller, R.E.; Rustin, G.J. How to follow-up patients with epithelial ovarian cancer. Curr. Opin. Oncol. 2010, 22, 498–502. [Google Scholar]
- Gadducci, A.; Cosio, S. Surveillance of patients after initial treatment of ovarian cancer. Crit. Rev. Oncol. Hematol. 2009, 71, 43–52. [Google Scholar]
- Javitt, M.C. ACR Appropriateness Criteria on staging and follow-up of ovarian cancer. J. Am. Coll. Radiol. 2007, 4, 586–589. [Google Scholar]
- Thrall, M.M.; DeLoia, J.A.; Gallion, H.; Avril, N. Clinical use of combined positron emission tomography and computed tomography (FDG-PET/CT) in recurrent ovarian cancer. Gynecol. Oncol. 2007, 105, 17–22. [Google Scholar]
- Colombo, N.; Peiretti, M.; Parma, G.; Lapresa, M.; Mancari, R.; Carinelli, S.; Sessa, C.; Castiglione, M. Newly diagnosed and relapsed epithelial ovarian carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2010, 21, v23–v30. [Google Scholar]
- Bhosale, P.; Peungjesada, S.; Wei, W.; Levenback, C.F.; Schmeler, K.; Rohren, E.; Macapinlac, H.A.; Iyer, R.B. Clinical utility of positron emission tomography/computed tomography in the evaluation of suspected recurrent ovarian cancer in the setting of normal CA-125 levels. Int. J. Gynecol. Cancer 2010, 20, 936–944. [Google Scholar]
- Bharwani, N.; Reznek, R.H.; Rockall, A.G. Ovarian Cancer Management: The role of imaging and diagnostic challenges. Eur. J. Radiol. 2011, 78, 41–51. [Google Scholar]
- Hoekstra, C.J.; Paglianiti, I.; Hoekstra, O.S.; Smit, E.F.; Postmus, P.E.; Teule, G.J.; Lammertsma, A.A. Monitoring response to therapy in cancer using [18f]-2-fluoro-2-deoxy-d-glucose and positron emission tomography: An overview of different analytical methods. Eur. J. Nucl. Med. 2000, 27, 731–743. [Google Scholar]
- Tomasi, G.; Turkheimer, F.; Aboagye, E. Importance of quantification for the analysis of PET data in oncology: Review of current methods and trends for the future. Mol. Imaging Biol. 2012, 14, 131–146. [Google Scholar]
- Hoekstra, C.J.; Hoekstra, O.S.; Stroobants, S.G.; Vansteenkiste, J.; Nuyts, J.; Smit, E.F.; Boers, M.; Twisk, J.W.; Lammertsma, A.A. Methods to monitor response to chemotherapy in nonsmall cell lung cancer with 18F-FDG PET. J. Nucl. Med. 2002, 43, 1304–1309. [Google Scholar]
- Daisne, J.F.; Duprez, T.; Weynand, B.; Lonneux, M.; Hamoir, M.; Reychler, H.; Grégoire, V. Tumor volume in pyafyngolaryngeal squamous cell carcinoma: Comparison at CT, MR imaging and FGD PET and validation with surgical specimen. Radiology 2004, 233, 93–100. [Google Scholar]
- Geets, X.; Lee, J.A.; Bol, A.; Lonneux, M.; Gregoire, V. A gradient-based method for segmenting FDG-PET images: Methodology and validation. Eur. J. Nucl. Med. Mol. Imaging 2007, 34, 1427–1438. [Google Scholar]
- Werner-Wasik, M.; Nelson, A.D.; Choi, W.; Arai, Y.; Faulhaber, P.F.; Kang, P.; Almeida, F.D.; Xiao, Y.; Ohri, N.; Brockway, K.D.; et al. What is the best way to contour lung tumors on PET scans? Multiobserver validation of a gradient-based method using a NSCLC digital PET phantom. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 1164–1171. [Google Scholar]
- Riegel, A.C.; Berson, A.M.; Destian, S.; Ng, T.; Tena, L.B.; Mitnick, R.J,; Wong, P.S. Variability of gross tumor volume delineation in head-and-neck cancer using CT and PET/CT fusion. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 726–732. [Google Scholar]
- Nestle, U.; Schaefer-Schuler, A.; Kremp, S.; Groeschel, A.; Hellwig, D.; Rübe, C.; Kirsch, C.M. Target volume definition for 18F-FDG PET-positive lymph nodes in radiotherapy of patients with non-small cell lung cancer. Eur. J. Nucl. Med. Mol. Imaging 2007, 34, 453–462. [Google Scholar]
- Schinagl, D.A.; Vogel, W.V.; Hoffmann, A.L.; van Dalen, J.A.; Oyen, W.J.; Kaanders, J.H. Comparison of five segmentation tools for 18F-Fluoro-deoxy-glucosepositron emission tomography-based target volume definition in head and neck cancer. Int. J. Radiat. Oncol. Biol. Phys. 2007, 69, 1282–1289. [Google Scholar]
- Erdy, Y.E.; Mawlawi, O.; Larson, S.M.; Imbiaco, M.; Yeung, H.; Finn, R.; Humm, J.L. Segmentation of lung lesion volume by adaptive positron emission tomography image thresholding. Cancer 1997, 80, 2505–2509. [Google Scholar]
- Nakamoto, Y.; Zasadny, K.R.; Minn, H.; Wahl, R.L. Reproducibility of common semi-quantitative parameters for evaluating lung cancer glucose metabolism with positron emission tomography using 2-deoxy-2-[18f]fluoro-d-glucose. Mol. Imaging Biol. 2002, 4, 171–178. [Google Scholar]
- Van Dalen, J.A. A novel iterative method for lesion delineation and volumetric quantification with FDG PET. Nucl. Med. Commun. 2007, 28, 485–493. [Google Scholar]
- Daisne, J.F.; Sibomana, M.; Bol, A.; Doumont, T.; Lonneux, M.; Grégoire, V. Tri-dimensional automatic segmentation of PET volumes based on measured source-to-background ratios: Influence of reconstruction algorithms. Radiother. Oncol. 2003, 69, 247–250. [Google Scholar]
- Schaefer, A.; Kremp, S.; Hellwig, D.; Rübe, C.; Kirsch, C.M.; Nestle, U. A contrast-oriented algorithm for FDG-PET-based delineation of tumour volumes for the radiotherapy of lung cancer: Derivation from phantom measurements and validation in patient data. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 1989–1999. [Google Scholar]
- Zaidi, H.; El Naqa, I. PET-guided delineation of radiation therapy treatment volumes: A survey of image segmentation techniques. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 2165–2187. [Google Scholar]
- El Naqa, I.; Yang, D.; Apte, A.; Khullar, D.; Mutic, S.; Zheng, J.; Bradley, J.D.; Grigsby, P.; Deasy, J.O. Concurrent multimodality image segmentation by active contours for radiotherapy treatment planning. Med. Phys. 2007, 34, 4738–4749. [Google Scholar]
- Li, H.; Thorstad, W.L.; Biehl, K.J.; Laforest, R.; Su, Y.; Shoghi, K.I.; Donnelly, E.D.; Low, D.A.; Lu, W. A novel PET tumor delineation method based on adaptive region-growing and dual-front active contours. Med. Phys. 2008, 35, 3711–3721. [Google Scholar]
- Yu, H.; Caldwell, C.; Mah, K.; Mozeg, D. Coregistered FDG PET/CT-based textural characterization of head and neck cancer for radiation treatment planning. IEEE Trans. Med. Imaging 2009, 28, 374–383. [Google Scholar]
- Belhassen, S.; Zaidi, H. A novel fuzzy c-means algorithm for unsupervised heterogeneous tumor quantification in PET. Med. Phys. 2010, 37, 1309–1324. [Google Scholar]
- Murchison, J.T. TNM staging update for lung cancer: Why is this important? World. J. Radiol. 2012, 4, 126–127. [Google Scholar]
- Van de Wiele, C.; Kruse, V.; Smeets, P.; Shathekge, M.; Maes, A. Predictive and prognostic value of metabolic tumor volume and total lesion glycolysis in solid tumors. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 290–231. [Google Scholar]
- Van der Schroeff, M.P.; Baatenburg de Jong, R.J. Staging and prognosis in head and neck cancer. Oral Oncol. 2009, 45, 356–360. [Google Scholar]
- Chung, M.K.; Jeong, H.S.; Son, Y.I.; So, Y.K.; Park, G.Y.; Choi, J.Y.; Hyun, S.H.; Kim, H.J.; Ko, Y.H.; Baek, C.H. Metabolic tumor volumes by [18F]-fluorodeoxyglucose PET/CT correlate with occult metastasis in oral squamous cell carcinoma of the tongue. Ann. Surg. Oncol. 2009, 16, 3111–3117. [Google Scholar]
- Dibble, E.H.; Alvarez, A.C.; Truong, M.T.; Mercier, G.; Cook, E.F.; Subramaniam, R.M. 18F-FDG metabolic tumor volume and total glycolytic activity of oral cavity and oropharyngeal squamous cell cancer: Adding value to clinical staging. J. Nucl. Med. 2012, 53, 709–715. [Google Scholar]
- Chan, S.C.; Chang, J.T.; Lin, C.Y.; Ng, S.H.; Wang, H.M.; Liao, C.T.; Chang, C.J.; Lin, S.Y.; Yen, T.C. Clinical utility of 18F-FDG PET parameters in patients with advanced nasopharyngeal carcinoma: Predictive role for different survival endpoints and impact on prognostic stratification. Nucl. Med. Commun. 2011, 32, 989–996. [Google Scholar]
- De Geus-Oei, L.F.; van der Heijden, H.F.; Corstens, F.H.; Oyen, W.J. Predictive and prognostic value of FDG-PET in nonsmall-cell lung cancer: A systematic review. Cancer 2007, 110, 1654–1664. [Google Scholar]
- Lee, P.; Weerasuriya, D.K.; Lavori, P.W.; Quon, A.; Hara, W.; Maxim, P.G.; Le, Q.T.; Wakelee, H.A.; Donington, J.S.; Graves, E.E.; et al. Metabolic tumor burden predicts for disease progression and death in lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2007, 69, 328–333. [Google Scholar]
- Jemal, A.; Siegel, R.; Ward, E.; Hao, Y.; Xu, J.; Thun, M. Cancer statistics. CA Cancer J. Clin. 2009, 59, 225–249. [Google Scholar]
- Pennathur, A.; Luketich, J. Resection of esophageal cancer: Strategies for optimal management. Ann. Thorac. Surg. 2008, 85, 751–756. [Google Scholar]
- Sagar, P.M.; Gauperaa, T.; Sue-Ling, H.; McMahon, M.J.; Johnston, D. An audit of the treatment of cancer of the oesophagus. Gut 1994, 35, 941–945. [Google Scholar]
- Lordick, F.; Ott, K.; Sendler, A. Gastric cancer and adenocarcinoma of the esophagogastric junction: Principles of neoadjuvant therapy. Chirurg 2011, 82, 968–973. [Google Scholar]
- Jayachandran, P.; Pai, R.K.; Quon, A.; Graves, E.; Krakow, T.E.; La, T.; Loo, B.W., Jr.; Koong, A.C.; Chang, D.T. Postchemoradiotherapy positron emission tomography predicts pathologic response and survival in patients with esophageal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, 471–477. [Google Scholar]
- Zhong, X.; Yu, J.; Zhang, B.; Mu, D.; Zhang, W.; Li, D.; Han, A.; Song, P.; Li, H.; Yang, G.; et al. Using 18F-fluorodeoxyglucose positron emission tomography to estimate the length of gross tumor in patients with squamous cell carcinoma of the esophagus. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 136–141. [Google Scholar]
- Mamede, M.; El Fakhri, G.; Abreu-e-Lima, P.; Gandler, W.; Nosé, V.; Gerbaudo, V.H. Pre-operative estimation of esophageal tumor metabolic length in FDG-PET images with surgical pathology confirmation. Ann. Nucl. Med. 2007, 21, 553–562. [Google Scholar]
- Roedl, J.B.; Harisinghani, M.G.; Colen, R.R.; Fischman, A.J.; Blake, M.A.; Mathisen, D.J.; Mueller, P.R. Assessment of treatment response and recurrence in esophageal carcinoma based on tumor length and standardized uptake value on positron emission tomography-computed tomography. Ann. Thorac. Surg. 2008, 86, 1131–1138. [Google Scholar]
- Eifel, P.J.; Winter, K.; Morris, M.; Levenback, C.; Grigsby, P.W.; Cooper, J.; Rotman, M.; Gershenson, D.; Mutch, D.G. Pelvic irradiation with concurrent chemotherapy versus pelvic and para-aortic irradiation for high-risk cervical cancer: An update of radiation therapy oncology group trial (RTOG) 90-01. J. Clin. Oncol. 2004, 22, 872–880. [Google Scholar]
- Kidd, E.A.; Thomas, M.; Siegel, B.A.; Dehdashti, F.; Grigsby, P.W. Changes in cervical cancer FDG uptake during chemoradiation and association with response. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 116–122. [Google Scholar]
- Malpas, J.S.; Caroll, J.J. Myeloma: Clinical presentation and diagnosis. In Myeloma: Biology and Management; Malpas, J.S., Bergsagel, D.E., Kyle, R.A., Eds.; Oxford University Press: New York, NY, USA, 1995; p. 169. [Google Scholar]
- Drach, J.; Sagaster, V.; Ackermann, J.; Kaufmann, H. Prognostic factors for multiple myeloma. Hematology 2006, 2, 196–200. [Google Scholar]
- Kyle, R.A.; Rajkumar, S.V. Criteria for diagnosis, staging, risk stratification and response assessment of multiple myeloma. Leukemia 2009, 23, 3–9. [Google Scholar]
- Durie, B.G.; Salmon, S.E. A clinical staging system for multiple myeloma: Correlation of measured myeloma cells with presenting clinical features, response to treatment and survival. Cancer 1975, 36, 842–854. [Google Scholar]
- Durie, B.G.M. The role of anatomical and functional staging myeloma: Description of Durie/Salmon plus staging system. Eur. J. Cancer 2006, 42, 1539–1543. [Google Scholar]
- Zamagni, E.; Patriarca, F.; Nanni, C.; Zannetti, B.; Englaro, E.; Pezzi, A.; Tacchetti, P.; Buttignol, S.; Perrone, G.; Brioli, A.; et al. Prognostic relevance of 18-F FDG PET/CT in newly diagnosed multiple myeloma patients treated with up-front autologous transplantation. Blood 2011, 118, 5989–5995. [Google Scholar]
- Fonti, L.; Larobina, M.; del Vecchio, S.; de Luca, S.; Fabbricini, R.; Catalano, L.; Pane, F.; Salvatore, M.; Pace, L. Metabolic Tumor Volume assessed by 18 F-FDG PET/CT for the prediction of outcome in patients with multiple myeloma. J. Nucl. Med. 2012, 53, 1829–1835. [Google Scholar]
- Special Report: Positron Emission Tomography for the Indication of Post-Treatment Surveillance of Cancer. Available online: http://www.bcbs.com/blueresources/tec/press/special-report-positron.html (accessed on 25 July 2014).
- Podoloff, D.A.; Advani, R.H.; Allred, C.; Benson, A.B., 3rd; Brown, E.; Burstein, H.J.; Carlson, R.W.; Coleman, R.E.; Czuczman, M.S.; Delbeke, D.; et al. NCCN task force report: Positron emission tomography (PET)/computed tomography (CT) scanning in cancer. J. Natl. Compr. Cancer Netw. 2007, 5, S1–S23. [Google Scholar]
- Patel, K.; Hadar, N.; Lee, J.; Siegel, B.A.; Hillner, B.E.; Lau, J. The lack of evidence for PET or PET/CT surveillance of patients with treated lymphoma, colorectal cancer, and head and neck cancer: A systematic review. J. Nucl. Med. 2013, 54, 1518–1527. [Google Scholar]
- Lee, A.I.; Zuckerman, D.S.; van den Abbeele, A.D.; Aquino, S.L.; Crowley, D.; Toomey, C.; Lacasce, A.S.; Feng, Y.; Neuberg, D.S.; Hochberg, E.P. Surveillance imaging of Hodgkin lymphoma patients in first remission: A clinical and economic analysis. Cancer 2010, 116, 3835–3842. [Google Scholar]
- Sobhani, I.; Tiret, E.; Lebtahi, R.; Aparicio, T.; Itti, E.; Montravers, F.; Vaylet, C.; Rougier, P.; André, T.; Gornet, J.M.; et al. Early detection of recurrence by 18FDG-PET in the follow-up of patients with colorectal cancer. Br. J. Cancer 2008, 98, 875–880. [Google Scholar]
- Hicks, R.J.; Hofman, M.S. Is there still a role for SPECT-CT in oncology in the PET-CT era? Nat. Rev. Clin. Oncol. 2012, 9, 712–720. [Google Scholar]
- Beauregard, J.M.; Williams, S.G.; Degrado, T.R.; Roselt, P.; Hicks, R.J. Pilot comparison of F-fluorocholine and F-fluorodeoxyglucose PET/CT with conventional imaging in prostate cancer. J. Med. Imaging Radiat. Oncol. 2010, 54, 325–332. [Google Scholar]
- Evangelista, L.; Zattoni, F.; Guttilla, A.; Saladini, G.; Zattoni, F.; Colletti, P.M.; Rubello, D. Choline PET or PET/CT and biochemical relapse of prostate cancer: A systematic review and meta-analysis. Clin. Nucl. Med. 2013, 38, 305–314. [Google Scholar]
- Von Eyben, F.E.; Kairemo, K. Meta-analysis of (11)C-choline and (18)F-choline PET/CT for management of patients with prostate cancer. Nucl. Med. Commun. 2014, 35, 221–230. [Google Scholar]
- Treglia, G.; Ceriani, L.; Sadeghi, R.; Giovacchini, G.; Giovanella, L. Relationship between prostate-specific antigen kinetics and detection rate of radiolabelled choline PET/CT in restaging prostate cancer patients: A meta-analysis. Clin. Chem. Lab. Med. 2014, 52, 725–733. [Google Scholar]
- Umbehr, M.H.; Muntener, M.; Hany, T.; Sulser, T.; Bachmann, L.M. The role of 11C-choline and 18F-fluorocholine positron emission tomography (PET) and PET/CT in prostate cancer: A systematic review and meta-analysis. Eur. Urol. 2013, 64, 106–117. [Google Scholar]
- Evangelista, L.; Guttilla, A.; Zattoni, F.; Muzzio, P.C.; Zattoni, F. Utility of choline positron emission tomography/computed tomography for lymph node involvement identification in intermediate- to high-risk prostate cancer: A systematic literature review and meta-analysis. Eur. Urol. 2013, 63, 1040–1048. [Google Scholar]
- Varrone, A.; Asenbaum, S.; Vander Borght, T.; Booij, J.; Nobili, F.; Nagren, K.; Darcourt, J.; Kapucu, O.L.; Tatsch, K.; Bartenstein, P.; et al. EANM procedure guidelines for PET brain imaging using [18F]FDG, version 2. Eur. J. Nucl. Med. Mol. Imaging 2009, 36, 2103–2110. [Google Scholar]
- Spence, A.M.; Muzi, M.; Mankoff, D.A.; O’Sullivan, S.F.; Link, J.M.; Lewellen, T.K.; Lewellen, B.; Pham, P.; Minoshima, S.; Swanson, K.; et al. 18F-FDG PET of gliomas at delayed intervals: Improved distinction between tumor and normal gray matter. J. Nucl. Med. 2004, 45, 1653–1659. [Google Scholar]
- Prieto, E.; Marti-Climent, J.M.; Dominguez-Prado, I.; Garrastachu, P.; Diez-Valle, R.; Tejada, S.; Aristu, J.J.; Peñuelas, I.; Arbizu, J. Voxel-based analysis of dual-time-point 18F-FDG PET images for brain tumor identification and delineation. J. Nucl. Med. 2011, 52, 865–872. [Google Scholar]
- Mehrkens, J.H.; Popperl, G.; Rachinger, W.; Herms, J.; Seelos, K.; Tatsch, K.; Tonn, J.C.; Kreth, F.W. The positive predictive value of O-(2-[18F]fluoroethyl)-L-tyrosine (FET) PET in the diagnosis of a glioma recurrence after multimodal treatment. J. Neurooncol. 2008, 88, 27–35. [Google Scholar]
- Fueger, B.J.; Czernin, J.; Cloughesy, T.; Silverman, D.H.; Geist, C.L.; Walter, M.A.; Schiepers, C.; Nghiemphu, P.; Lai, A.; Phelps, M.E.; et al. Correlation of 6-18F-fluoro-L-dopa PET uptake with proliferation and tumor grade in newly diagnosed and recurrent gliomas. J. Nucl. Med. 2010, 51, 1532–1538. [Google Scholar]
- Karunanithi, S.; Sharma, P.; Kumar, A.; Khangembam, B.C.; Bandopadhyaya, G.P.; Kumar, R.; Gupta, D.K.; Malhotra, A.; Bal, C. 18F-FDOPA PET/CT for detection of recurrence in patients with glioma: Prospective comparison with 18F-FDG PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 1025–1035. [Google Scholar]
- Lizarraga, K.J.; Allen-Auerbach, M.; Czernin, J.; DeSalles, A.A.; Yong, W.H.; Phelps, M.E.; Chen, W. (18)F-FDOPA PET for differentiating recurrent or progressive brain metastatic tumors from late or delayed radiation injury after radiation treatment. J. Nucl. Med. 2014, 55, 30–36. [Google Scholar]
- Kratochwil, C.; Combs, S.E.; Leotta, K.; Afshar-Oromieh, A.; Rieken, S.; Debus, J.; Haberkorn, U.; Giesel, F.L. Intra-individual comparison of (1)(8)F-FET and (1)(8)F-DOPA in PET imaging of recurrent brain tumors. Neuro-Oncology 2014, 16, 434–440. [Google Scholar]
- Bacca, A.; Chiacchio, S.; Zampa, V.; Carrara, D.; Duce, V.; Congregati, C.; Simi, P.; Taddei, S.; Materazzi, G.; Volterrani, D.; et al. Role of 18F-DOPA PET/CT in diagnosis and follow-up of adrenal and extra-adrenal paragangliomas. Clin. Nucl. Med. 2014, 39, 14–20. [Google Scholar]
- Wong, K.K.; Waterfield, R.T.; Marzola, M.C.; Scarsbrook, A.F.; Chowdhury, F.U.; Gross, M.D.; Rubello, D. Contemporary nuclear medicine imaging of neuroendocrine tumours. Clin. Radiol. 2012, 67, 1035–1050. [Google Scholar]
- Tehrani, O.S.; Shields, A.F. PET imaging of proliferation with pyrimidines. J. Nucl. Med. 2013, 54, 903–912. [Google Scholar]
- Bading, J.R.; Shields, A.F. Imaging of cell proliferation: Status and prospects. J. Nucl. Med. 2008, 49, 64S–80S. [Google Scholar]
- Segall, G.; Delbeke, D.; Stabin, M.G.; Even-Sapir, E.; Fair, J.; Sajdak, R.; Smith, G.T. SNM practice guideline for sodium 18F-fluoride PET/CT bone scans 1.0. J. Nucl. Med. 2010, 51, 1813–1820. [Google Scholar]
- Hofman, M.S.; Kong, G.; Neels, O.C.; Eu, P.; Hong, E.; Hicks, R.J. High management impact of Ga-68 DOTATATE (GaTate) PET/CT for imaging neuroendocrine and other somatostatin expressing tumours. J. Med. Imaging radiat. Oncol. 2012, 56, 40–47. [Google Scholar]
- Hofmann, M.; Maecke, H.; Borner, R.; Weckesser, E.; Schoffski, P.; Oei, L.; Schumacher, J.; Henze, M.; Heppeler, A.; Meyer, J.; et al. Biokinetics and imaging with the somatostatin receptor PET radioligand (68)Ga-DOTATOC: Preliminary data. Eur. J. Nucl. Med. 2001, 28, 1751–1757. [Google Scholar]
- Ambrosini, V.; Campana, D.; Tomassetti, P.; Fanti, S. (6)(8)Ga-labelled peptides for diagnosis of gastroenteropancreatic NET. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, S52–S60. [Google Scholar]
- Drzezga, A.; Souvatzoglou, M.; Eiber, M.; Beer, A.J.; Furst, S.; Martinez-Moller, A.; Nekolla, S.G.; Ziegler, S.; Ganter, C.; Rummeny, E.J.; et al. First clinical experience with integrated whole-body PET/MR: Comparison to PET/CT in patients with oncologic diagnoses. J. Nucl. Med. 2012, 53, 845–855. [Google Scholar]
- Tian, J.; Fu, L.; Yin, D.; Zhang, J.; Chen, Y.; An, N.; Xu, B. Does the Novel Integrated PET/MRI Offer the Same Diagnostic Performance as PET/CT for Oncological Indications? PLoS One 2014, 9, e90844. [Google Scholar]
- Al-Nabhani, K.Z.; Syed, R.; Michopoulou, S.; Alkalbani, J.; Afaq, A.; Panagiotidis, E.; O’Meara, C.; Groves, A.; Ell, P.; Bomanji, J. Qualitative and quantitative comparison of PET/CT and PET/MR imaging in clinical practice. J. Nucl. Med. 2014, 55, 88–94. [Google Scholar]
- Wetter, A.; Lipponer, C.; Nensa, F.; Heusch, P.; Rubben, H.; Schlosser, T.W.; Pöppel, T.D.; Lauenstein, T.C.; Nagarajah, J. Quantitative evaluation of bone metastases from prostate cancer with simultaneous [F] choline PET/MRI: Combined SUV and ADC analysis. Ann. Nucl. Med. 2014, 28, 405–410. [Google Scholar]
- Queiroz, M.A.; Hullner, M.; Kuhn, F.; Huber, G.; Meerwein, C.; Kollias, S.; von Schulthess, G.; Veit-Haibach, P. PET/MRI and PET/CT in follow-up of head and neck cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1066–1045. [Google Scholar]
- Littooij, A.S.; Kwee, T.C.; Barber, I.; Granata, C.; Vermoolen, M.A.; Enriquez, G.; Zsíros, J.; Soh, S.Y.; de Keizer, B.; Beek, F.J.; et al. Whole-body MRI for initial staging of paediatric lymphoma: Prospective comparison to an FDG-PET/CT-based reference standard. Eur. Radiol. 2014, 24, 1153–1165. [Google Scholar]
- Yoon, S.H.; Goo, J.M.; Lee, S.M.; Park, C.M.; Seo, H.J.; Cheon, G.J. Positron emission tomography/magnetic resonance imaging evaluation of lung cancer: Current status and future prospects. J. Thorac. Imaging 2014, 29, 4–16. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gallamini, A.; Zwarthoed, C.; Borra, A. Positron Emission Tomography (PET) in Oncology. Cancers 2014, 6, 1821-1889. https://doi.org/10.3390/cancers6041821
Gallamini A, Zwarthoed C, Borra A. Positron Emission Tomography (PET) in Oncology. Cancers. 2014; 6(4):1821-1889. https://doi.org/10.3390/cancers6041821
Chicago/Turabian StyleGallamini, Andrea, Colette Zwarthoed, and Anna Borra. 2014. "Positron Emission Tomography (PET) in Oncology" Cancers 6, no. 4: 1821-1889. https://doi.org/10.3390/cancers6041821
APA StyleGallamini, A., Zwarthoed, C., & Borra, A. (2014). Positron Emission Tomography (PET) in Oncology. Cancers, 6(4), 1821-1889. https://doi.org/10.3390/cancers6041821